
Abstract
Background
Surgical site infections (SSIs) represent ~ 20% of all hospital-acquired infections in surgical patients and are associated with prolonged hospital stay, admission to intensive care, and mortality. We conducted a systematic review with economic and environmental models to assess whether triclosan-coated sutures (Plus Sutures) provide benefits over non-coated sutures in the reduction of SSI risk.
Methods
Searches were conducted in fifteen databases. A total of 1,991 records were retrieved. Following deduplication and screening by two independent reviewers, 31 randomized controlled trials in adults and children were included in the review.
Similarity of the studies was assessed by narrative review and confirmed by quantitative assessment. A fixed effects meta-analysis of SSI incidence model including all groups of patients estimated a risk ratio of 0.71 (95% confidence interval: 0.64 to 0.79) indicating those in the Plus Sutures group had a 29% reduction in the risk of developing an SSI compared with those in the control group (p < 0.001). Safety outcomes were analysed qualitatively.
Results
The economic model estimated the use of Plus Sutures to result in average cost savings of £13.63 per patient. Plus Sutures remained cost-saving in all subgroup analyses with cost-savings ranging between £11 (clean wounds) and £140 (non-clean wounds).
The environmental impact of SSI is substantial, and the model suggests that the introduction of Plus Sutures could result in potential environmental benefits.
Conclusions
The evidence suggests that Plus Sutures are associated with a reduced incidence of SSI across all surgery types alongside cost savings when compared with standard sutures.
Similar content being viewed by others


Explore related subjects
Find the latest articles, discoveries, and news in related topics.Background
Surgical site infections (SSIs) represent around 20% of all hospital-acquired infections in patients undergoing surgery and are associated with prolonged hospital stay and increased risk of admission to intensive care, morbidity and mortality [1, 2]. Alongside the negative impact on patients, SSI poses a significant financial and resource burden for hospitals. In the United States, the annual cost to the health care system of treating SSI has been estimated to be $3.3 billion [3], and a recent study estimated the additional hospital inpatient cost associated with SSI at between $3.7 and $5.5 billion [4]. In the UK, the average cost of managing an SSI is reported to be over £6,000 (accounting for inflation) [5] for National Health Service (NHS) hospitals. These costs do not include any potential litigation costs arising from acquisition of SSI during a hospital stay [6].
SSI is multifactorial and it has been estimated that 40% to 60% of cases may be preventable [7, 8]. Reducing the risk of SSI requires an evidence-based surgical care bundle approach, including management of patient risk factors for infection, appropriate skin antisepsis, instrument sterilisation, environmental control within the operating theatre, infection prevention and control measures, and antibacterial devices [9, 10].
Suture material is a risk factor for SSI. Bacteria can colonize on the suture developing a polymicrobial biofilm which increases the likelihood of an SSI [11,12,13,14,15,16,17]. Plus Antibacterial Sutures (Ethicon, Johnson & Johnson Medical Ltd), a range of synthetic, absorbable sutures, were developed to address this risk factor. Plus Sutures are coated with medical-grade triclosan, IRGACARE® MP, a broad-spectrum antibacterial agent that actively inhibits the colonization of bacteria on the suture and is effective against the most common organisms associated with SSI [18,19,20]. The use of triclosan-coated sutures to prevent SSIs has been recommended internationally by the World Health Organization (WHO), the National Institute for Health and Care Excellence (NICE) in the UK, the European Network for Health Technology Assessment (EUnetHTA), the Centers for Disease Control (CDC), the American College of Surgeons and the Surgical Infection Society, the Canadian Agency for Drugs and Technologies in Health (CADTH), and the Australian Guidelines for the Prevention and Control of Infection in Healthcare, among others [9, 10, 21,22,23].
The aim of this work was to synthesise the available published evidence around Plus Suture to prevent SSI in terms of clinical outcomes and estimate the effectiveness in terms of cost and environmental impact. This review and analyses also formed part of a submission for Plus Sutures to the NICE Medical Technologies Evaluation Programme (MTEP) [24]. NICE is an executive non-departmental public body that produces guidelines and advice for commissioners, practitioners and managers throughout the NHS and other public health and social care services in the UK [25]. As part of the MTEP process, the findings presented here were reviewed and corroborated by independent reviewers based at an External Assessment Centre [24].
Methods
The population was adults and children needing wound closure after a surgical procedure in any country, in whom absorbable sutures are an appropriate option.
The intervention was triclosan-coated sutures, with a focus on the Plus Antibacterial Sutures range that included:
-
▪ Coated VICRYL™ Plus Antibacterial (polyglactin 910) Suture, a synthetic absorbable multifilament suture (multiple braided threads).
-
▪ MONOCRYL™ Plus Antibacterial (poliglecaprone 25) Suture, a synthetic absorbable monofilament suture (solid and smooth thread).
-
▪ PDS™ Plus Antibacterial (polydioxanone) Suture, a synthetic absorbable monofilament suture (solid and smooth thread).
-
▪ STRATAFIX™ Knotless Tissue Control Devices, a barbed suture material to allow tissue approximation without the need to tie surgical knots. The STRATAFIX range includes the:
-
STRATAFIX™ Symmetric PDS Plus Knotless Tissue Control Device.
-
STRATAFIX™ Spiral PDS Plus Knotless Tissue Control Device.
-
STRATAFIX™ Spiral MONOCRYL Plus Knotless Tissue Control Device.
-
Studies that did not disclose the specific triclosan-coated suture product assessed or used “triclosan-coated sutures” as a generic term, were also eligible for inclusion.
The comparator was sutures that do not contain an antibacterial agent. This was intended to capture all studies comparing against sutures used in clinical practice across the wide range of geographical settings eligible for inclusion in the review.
The outcomes of interest as defined in the review protocol were:
-
▪ Incidence of SSI, as defined by authors of the included studies (primary outcome).
-
▪ Length of post-operative stay in hospital relating to SSI.
-
▪ Readmission related to SSI, as reported in the included studies.
-
▪ Antibiotics use for SSI (including prescription, duration and dose).
-
▪ Severity of SSI using any validated scoring systems such as ASEPSIS (additional treatment, serous discharge, erythema, purulent exudate, separation of tissues, isolation of bacteria, stay duration as an inpatient) wound score.
-
▪ Device-related adverse events.
Systematic review methods
This systematic review was undertaken following the principles of systematic reviewing embodied in the Cochrane handbook [26] and is reported following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines [27]. The scope of the review was guided by the decision problem published by NICE for the health technology assessment (HTA) of Plus Sutures in the UK [24].
The PRISMA checklist is presented in Supplementary Sect. 8. The review protocol was registered on the Open Science Foundation database to ensure transparency [28]. Full details of the eligibility criteria are presented in Table 1.
Searches for the systematic review
The searches for the NICE submission were conducted between 01 February 2021 and 08 February 2021 in multiple databases and information resources (see Table 2). These included: databases covering biomedical healthcare and nursing journal literature; databases of controlled trials, systematic reviews and health technology assessments; databases containing conference abstracts; and databases containing information on ongoing trials. The full search strategy for MEDLINE (Supplementary Fig. 1) was translated appropriately for the other databases (Supplementary Appendix A).
Searches of economic databases were included because search results were also considered for use in the cost-effectiveness model of Plus Sutures.
Reference lists of any relevant systematic reviews published in the last five years were checked for any eligible studies that may have been missed by the database searches, and the manufacturer provided details of any ongoing or unpublished trials with which they were associated.
Screening, selection and data extraction
Results were downloaded into Endnote bibliographic software [29], deduplicated using several algorithms, and the duplicate references held in a separate EndNote database. A single researcher assessed the search results according to their relevance in providing information on the clinical efficacy and safety of the intervention and comparator and removed the obviously irrelevant records.
Two reviewers independently assessed the titles and abstracts of remaining records for relevance against the eligibility criteria, with disagreements adjudicated by a third reviewer. Assessment of full texts was then conducted by the same three reviewers; two reviewers independently assessed the records, and the third reviewer adjudicated any disagreements.
The first reviewer extracted data from the eligible studies and the second reviewer quality checked all the data points against the papers to ensure accuracy. Data were extracted as reported by study authors, with calculations performed only where the required data were not presented in the format required for the meta-analyses. Calculations were minimal and were based only on reported data.
As recommended by Cochrane guidance [30], timepoints at which data were to be extracted were specified prior to starting the review. One timepoint per study was extracted (the optimum timepoint for each surgery type was either 30 or 90 days post-surgery); if a paper reported data at more than one timepoint, CDC guidance [3] was used to select the most appropriate timepoint.
The NICE Risk of Bias tool [31] was used to quality assess each of the included studies, with one researcher completing the assessment and a second verifying this. This tool considers seven different criteria.
Synthesis
A high-level assessment of the similarity of studies and availability of data was performed, guided by the Australian Pharmaceutical Benefits Advisory Committee criteria [32]. Where meta-analysis was possible, i.e. sufficient homogenous studies reported suitable data, statistical methods were used to analyse and summarise the results of the included studies.
For outcomes for which meta-analysis was not possible, a narrative summary exploring the quality of the studies, the relationship between studies and any patterns discerned in the data were presented.
Meta-analysis methods
Where meta-analysis was deemed appropriate, results were statistically pooled for the outcomes of interest using both fixed- and random-effects models, both of which produced estimated risk ratios. Further details are presented in Supplementary Sect. 2. Robustness of the model chosen, model assumptions and susceptibility to outliers were assessed. Potential sources of heterogeneity were defined a priori and were evaluated through sensitivity and subgroup analyses. All statistical analyses were conducted using R version 4.0.2 [33], with additional R packages meta (v.4.16–2 [34]) and dmetar (v.0.0.9000 [35]). Results were presented as forest plots, and the significance level was set at p ≤ 0.05.
The primary outcome for the meta-analysis was the relative risk (RR) of developing an SSI between the intervention (Plus Sutures) and control group.
Subgroup and sensitivity analyses
The base case analysis included all studies that provided sufficient data. Subgroup analysis considered four subgroups as defined in the NICE scope (adults only, children only, patients classified as having clean wounds, and patients classified as having non-clean wounds). Studies in which the authors did not explicitly state wound type were mapped to the subgroups by surgery type. Finally, a sensitivity analysis was carried out removing Stratafix Plus as an intervention to explore its potential effect on heterogeneity.
For the subgroup analyses by wound type, we recorded authors’ descriptions of the status of the wounds assessed in each study. Where the authors did not explicitly report this information, the independent opinion of three clinicians was sought as to the likely wound status following the surgery detailed in each of the studies. The categorisation of the wound status was then compared across the clinicians and any divergence of opinion discussed before a consensus was reached. The decisions reached determined which subgroup analysis each study would contribute to.
Modelling methods
Model structure
A decision-tree model was developed to estimate changes in healthcare costs (from the perspective of the NHS) associated with the use of Plus Sutures compared with conventional sutures in people undergoing a surgical procedure. The population considered in the model was all people undergoing a surgical procedure with subgroup analysis conducted for adults (≥ 18 years of age), children, clean and non-clean wounds. Following their surgical procedure people enter the model and receive either Plus Sutures or conventional sutures and then follow the pathway of SSI or no SSI, followed by survival or death. The model structure is presented in Fig. 1.

Structure of the model
Patients who developed an incisional SSI accrued additional mortality risk and costs which incorporated hospital readmission, increased length of stay plus other resource use required during SSI treatment. Given that no system changes were anticipated to implement the technology and no additional training was required for health care professionals to use Plus Sutures, no additional resource costs were included in the model.
Adverse events related to sutures were not included in the model because no events were identified from the clinical review that were judged to have a substantial impact on health-related quality of life (HRQoL) or health care resource use. Those reported were considered unlikely to be related to the Plus technology.
The model structure was aligned with the clinical pathway and other SSI models in the published literature as well as those developed or assessed by NICE, where the risk of SSI in both arms was captured and the cost of this applied [36,37,38,39,40,41,42,43,44,45]. The input parameters were not aligned with these studies; rather the best available evidence relevant to the NHS at the time of constructing the model (March 2021) was used instead, to ensure the model was current and relevant to the UK.
Model inputs
The model inputs are presented in Supplementary Table 1. In addition to the searches run to inform the systematic review, reports of adverse events associated with the technology were sought via searches of the Manufacturer and User Facility Device Experience (MAUDE) database and Medicines and Healthcare products Regulatory Agency (MHRA) resources. Results of these searches did not inform the systematic review but were used to check for any adverse events not reported in the published literature that might need to be considered in the model.
Baseline infection risk
Baseline infection risk of 1.04% with comparator sutures was derived from UK Health Security Agency (previously Public Health England; PHE) [46] surveillance data on SSI. The baseline infection risk of 1.04% was also used for the adult and children subgroups. This was judged to be reasonable based on data from the literature [47,48,49,50]. No alternative data were identified that were judged to be more representative of these subgroups.
For the baseline risk of infection in clean (0.8%) and non-clean (6.8%) subgroups the PHE data was also used. Surgical categories were split into those most likely to result in a clean and unclean wound in line with Troughton 2018 et al. [51].
Surgical Site Infection risk with Plus Sutures
The post-surgery SSI risk with Plus Sutures was calculated by applying the RR of infection derived from the meta-analysis to the base case SSI risk from PHE. The RR derived from the fixed effects model was used. RRs for each of the subgroups (children, adults, clean wounds and non-clean wounds) were used for each of the subgroup analyses.
Cost of SSI
The cost for SSI used in the base case was £6,016 based on Jenks et al. 2014 [5] (inflated from 2011/12 to 2019/20 [52]). This was used in the base case and for the adult and children subgroups. Jenks et al. 2014 reports a different median cost attributable to SSI for each category of surgery. These were used to calculate a cost of SSI for the clean and non-clean subgroups in line with Troughton 2018 [51].
Model outputs
The model generated the total per patient costs in each arm over a one-year time horizon. The incremental cost per patient is presented as well as a cost per SSI averted and the cost per death averted.
Subgroup and sensitivity analysis
One-way deterministic sensitivity analysis was conducted to explore the impact of varying individual parameters and identify key drivers of the analysis. Threshold/breakeven analysis was conducted around the baseline SSI incidence with comparator sutures, the cost of SSI, the RR reduction of SSI incidence with Plus Sutures, and the number of sutures. A tornado diagram (see Fig. 4) was used to present one-way analysis for all model inputs. Ranges reported were taken from the literature, and where unavailable, clinical opinion or assumptions were used.
Probabilistic sensitivity analysis (PSA) was conducted to explore second order uncertainty in the results using 1,000 iterations to ensure model stability.
The ranges considered in the sensitivity analyses are presented in Supplementary Table 1.
Subgroup analysis was conducted as described throughout for adults, children, clean and non-clean wounds.
Environmental sustainability model
An environmental sustainability model was developed to evaluate the environmental impact of SSI and the environmental benefits of SSI reductions. The model structure is shown in Supplementary Fig. 2. Patients who developed an SSI were associated with a 10 day longer length of hospital stay, 4.1 additional outpatient appointments, and 22% more A&E visits compared with patients without an SSI [5, 53]. Environmental impact per SSI for the additional length of stay in general and intensive care wards, additional outpatient and A&E visits and associated travel was calculated through the application of the environmental sustainability reference information provided in the Sustainable Care Pathways Guidance [54]. The model inputs are presented in Supplementary Table 2. The environmental impact of antibiotic prescriptions, GP/community care appointments, and community care home visits were not included as these data were not available [5, 46, 51, 53,54,55,56]. The model calculated the environmental impact of SSI using three environmental metrics in accordance with the Sustainable Care Pathway Guidance: greenhouse gas (GHG) emissions, freshwater use, and waste generation. Following this, the potential environmental benefit of reduction in SSI with the use of Plus Sutures was computed by applying the RR of infection derived from the meta-analysis to the base case SSI risk from PHE. The sustainability analysis underwent independent validation.
Results
Results of the systematic review
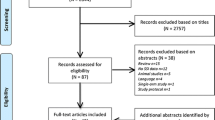
The searches retrieved a total of 1,991 records. Following deduplication, 1,229 unique records remained, and 186 publications and trial records proceeded to full text review, which excluded 108 documents (see Supplementary Table 3). Thirty-one studies (reported in 54 documents) were eligible for this review, and a further 21 ongoing or unpublished studies (reported in 24 documents) were listed for information. Figure 2 shows the PRISMA flow diagram, Table 3 presents a summary of the risk of bias assessment, and Supplementary Tables 4 to 7 present full details of the included studies. An overview of the study characteristics of the included studies is presented in Table 4. All but two studies [57, 58] explicitly stated that the sutures assessed were part of the Plus suture range (see Table 4), which uses medical-grade triclosan, IRGACARE® MP.

PRISMA flow diagram for the review
Of the 31 studies included in the review, three studies [61, 73, 84] were judged to be at a ‘low’ risk of bias, and two further studies [70, 79] were considered to have an overall ‘unclear’ risk of bias (Table 3). The remaining 26 studies were judged to have possible ‘methodological concerns’, most of which related to the adequacy of blinding of individuals involved in the trial and whether an appropriate intention-to-treat (ITT) analysis was conducted.
Results of outcomes not suitable for meta-analysis
All outcomes, except incidence of SSI, were unsuitable for assessment using meta-analysis. The main reason was a lack of reporting of the outcomes; when reported, the information was often incomplete. A summary of the reported outcomes, including safety outcomes, is presented in Supplementary Sect. 5.1.
The included studies reported minimal adverse events related to triclosan-coated sutures. Since adverse events are likely to emerge within the follow-up time of the RCTs, the evidence seems robust enough to exclude the possibility of significant adverse events related to the triclosan-coated sutures.
Results of the meta-analysis
Incidence of SSI was reported in all but one [81] of the 31 included studies. The similarity assessment to determine suitability of the trials for inclusion in the meta-analysis indicated that overall there was homogeneity between the studies. All but two studies [67, 72] reported outcomes at a timepoint of one month or longer, meaning that all SSI as described by the CDC definition [3] should have been captured by the studies. These two studies were excluded from the meta-analysis due to the potential impact of their short follow up: Karip 2016 [67] assessed infection rates at two weeks after surgery, and Rasic 2011 [72] only monitored outcomes during the hospitalization period (mean of 13.2 and 21.4 days for the intervention and comparator arms, respectively).
Similarity of the studies was confirmed by quantitative assessment. A Baujat diagnostic plot (Supplementary Fig. 3) showed that no study highly influenced the pooled effect size while also highly contributing to the overall heterogeneity of the meta-analysis, and a Leave-One-Out analysis (Supplementary Fig. 4) showed that no single study highly influenced heterogeneity or the pooled effect size with I2 ranging from 33 to 41% and the pooled effect size ranging from 0.67 to 0.70. Removal of Karip 2016 [67] and Rasic 2011 [72] did not unduly influence the primary outcome.
Selection of data for analyses
Thimour-Bergström 2013 [83] contributed two datasets to the meta-analysis; further details of these data can be found in the Supplementary Sect. 2.
Meta-analysis results
The fixed effects model for SSI including all groups of patients estimated a RR of 0.71 (95% confidence interval (CI): 0.64 to 0.79) indicating those in the triclosan-coated sutures (including Stratafix Plus) group had a 29% reduction in the risk of developing an SSI compared to those in the control group (p < 0.001). The random effects model estimated a RR of 0.70 (95% CI: 0.58 to 0.84; p < 0.001). These results are presented in Fig. 3 and are based on 6,852 and 6,969 total patients, and 503 and 708 events in the triclosan-coated sutures (including Stratafix Plus) and control arm, respectively. No outliers or substantial publication bias (see Supplementary Fig. 5) were noted during the analysis.

Meta- analysis results—All SSI incidence studies
Triclosan-coated sutures were found to be associated with a significant reduction in the risk of developing an SSI compared with those in the control group in all analyses conducted (25% to 48% reduction using fixed effects models across main analysis and subgroups). Full details of subgroups are presented in Supplementary Fig. 6a to d. Consistent findings were reported when Stratafix Plus was removed from the analyses (28% reduction; Supplementary Fig. 7).
Results of the economic model
The base case model results are presented in Table 5. The use of triclosan-coated sutures was estimated to result in average cost savings of £13.63 per patient. Triclosan-coated sutures remained cost saving in all subgroup analyses with cost savings estimated ranging between £11 (clean) and £140 (non-clean). Further details are presented in Supplementary Sect. 7.
As shown in the tornado plot (Fig. 4), use of triclosan-coated sutures remained the cost saving treatment strategy across all parameters that were changed individually within plausible ranges. The main driver of the analysis is the baseline risk of SSI with comparator sutures, followed by the RR of SSI with triclosan-coated sutures, and the cost of SSI.

Tornado plot presenting one-way sensitivity analysis
The probabilistic sensitivity analysis demonstrated that the results are robust when varying all input parameters simultaneously around pre-specified distributions that aimed to reflect the uncertainty in each parameter. These distributions were either based on uncertainty estimates from the literature or plausible assumptions where data were not available. All parameters were varied in the PSA with the majority of distributions based on confidence intervals reported in the literature or as per the meta-analysis, particularly for those parameters that are key drivers of the results (baseline risk of SSI, RR of SSI with triclosan-coated sutures and cost of SSI). 99.8% of iterations were cost saving when 1,000 iterations of the model were run.
Results of the sustainability model
The environmental model results are presented in Table 6. The environmental impact of an SSI was estimated to incur 576 kg CO2e GHG emissions (equivalent to return flights from London to Rome for two people) [87], 872 m3 water use and 65 kg waste generation. The use of triclosan-coated sutures, through reduction of SSI risk, was estimated to result in the environmental savings to NHS England of 1.74 tCO2e (equivalent to return flights from London to Rome for six people) [87], 2,629 m3 water use (equivalent to 25 times the annual drinking water use of an average European household) [88] and 0.2 tonnes of waste (equivalent to over four times the monthly waste generation of an average European person) [89], per 1,000 patients.
Discussion
Clinical outcomes
Thirty-one RCTs, including 13,754 patients and 1,211 episodes of SSI were eligible for this systematic review.
Results of the overall population meta-analysis indicated that patients in the triclosan-coated sutures (including Stratafix Plus) group had a 29% reduction in the risk of developing an SSI compared with those in the control group. All analyses showed a statistically significant reduction (between 25 to 48% depending on subgroup) in incidence of SSI with the use of Plus Sutures. Overall, the meta-analysis incorporated a homogenous group of studies (assessed using both quantitative and qualitative methods) and supports the use of Plus Sutures in reducing the risk of SSI [24]. Furthermore, these findings support the results of previous systematic reviews and meta-analyses which evaluated SSI risk in triclosan-coated sutures against standard sutures [90,91,92,93]. While the existing meta-analyses were informed by older searches [90, 91] or differed in focus and scope from this review (Otto-Lambertz 2023 limited to clean and clean-contaminated procedures only), the results consistently show a benefit for triclosan-coated sutures of between 24% [93] and 28% [91].
However, we note that a recently published systematic review [94] (searches in September 2021) concluded that there were no differences between triclosan-coated and uncoated sutures. The 2021 review had a restricted PICO (clean wounds and children excluded) and the meta-analysis only included studies deemed to have a low risk of bias as judged by an unvalidated tool (adapted specifically for SSI from the Cochrane risk of bias-2 tool, with input from the review authors and clinicians).
Efficacy outcomes other than SSI were not reported consistently in the published primary studies, and where they were reported, the strength of the evidence varied. More consistent reporting of these important outcomes is recommended in line with NICE recommendations [95].
The included studies reported minimal device-related adverse events. Since adverse events were likely to emerge within the follow-up time of the RCTs, the evidence seems robust enough to exclude the possibility of significant adverse events related to the triclosan-coated sutures [24].
Strengths and limitations of the clinical evidence
The clinical evidence is drawn from a good number of RCTs (31) including a high number of SSIs (1,211) across a wide range of surgery types. In 27 of the included studies, incidence of SSI was the primary outcome, with most studies using a commonly accepted definition of SSI and a clearly defined patient population.
As Plus Sutures were the only triclosan-coated sutures on the market at the time of conducting the review [J&J to provide citation as detailed above], these analyses reflect the available evidence base and may not be applicable to any future antibiotic suture products that may come to market.
The 31 studies represented eight middle income and eleven high income countries. This range of countries provides good generalisability to the middle / high income global context, although low income countries are not represented in this review. The FALCON trial [96] (published after searches for this review were conducted) has recently suggested that in 54 hospitals located in low and middle income countries (Benin, Ghana, India, Mexico, Nigeria, Rwanda and South Africa) the use of triclosan-coated sutures did not reduce the risk of SSI. Some of the pragmatic choices made in the conduct of the trial limit the generalizability of the results. Among them, (i) allowing for different techniques of skin closure, (ii) use of triclosan-coated sutures only for fascia closure and not for skin closure, (iii) compliance with the individual component of the WHO checklist [10] was not mandated and (iv) no standard postoperative management of the wounds was prescribed. SSI are multifactorial and the absence of clear standardisation in pre-, intra-, and post-operative management of the wounds in the trial raises the risk that the effect of single components (like the use of Plus Sutures) is obscured by other non-controlled factors. This risk may be heightened in emergency procedures which comprised over 60% of the cases in FALCON. The results of FALCON may therefore not be applicable outside the geographical context, the surgical technique used, and the population included in the trial.
A recent systematic review and analysis of 29 trials in clean and clean-contaminated procedures, including FALCON (Otto-Lambertz 2023 [93]), found a significant 24% reduction in postoperative wound infection rate with the use of triclosan-coated sutures.
An exploratory analysis (reported in Supplementary Fig. 8) was conducted to assess the impact of the FALCON trial on the meta-analysis described in this paper, and found similar results to those of Otto-Lambertz. No publication bias was identified, and the fixed effects model indicated that patients in the triclosan-coated sutures (including Stratafix Plus) group had a 18% reduction in the risk of developing an SSI compared with those in the control group. This reduces the effect of the main analysis, which showed a 29% reduction of risk, but still suggests benefits associated with the triclosan-coated sutures compared to standard sutures.
Studies included in this review covered a wide range of surgical interventions, both emergency and planned, as laid out in Table 4. Most of the studies included patients with comorbidities including diabetes, chronic obstructive pulmonary disease (COPD), malignant diseases, chronic renal insufficiency, anaemia, and people living with obesity or malnourishment. This large heterogeneity in patient population in conjunction with the positive result and low heterogeneity of the meta-analysis suggests that the intervention can be recommended to a wide population of patients.
Not all studies were blinded in the same way; 15 of the studies were double-blind and the remaining 16 were either single-blind, open label, or not clearly reported. In addition, the studies were conducted in a wide range of countries over a fifteen-year date span (from 2005 to 2020). During this time, the clinical pathways are likely to have changed. Despite these factors, heterogeneity across studies was not substantial, and the use of random effects models accounted for any variability.
As recommended by Cochrane to increase precision of the results [97], the current review incorporated evidence from all available trials without removing the high-risk of bias studies. We acknowledge that only limited number of RCTs (three of the total 31 included in the review) were deemed to have a low risk of bias.
Economic evidence
The economic model indicates that the use of triclosan-coated sutures results in estimated cost savings of almost £14 per patient if introduced in the NHS. This equates to an estimated cost saving for an average UK NHS hospital of around £13,000 based on 954 surgical procedures per year [98]. Cost savings result from a reduction in SSI (as demonstrated in the clinical evidence) and, therefore, a reduction in the healthcare related costs and resources associated with treating SSI. The increase (~ £4.50 per patient) in costs of using triclosan-coated sutures compared with alternative sutures is outweighed by savings from a reduction in SSI incidence. Results were robust to changes in individual input parameters as demonstrated in the sensitivity analyses. Plus Sutures remained cost saving in all subgroup analyses with cost savings estimated between £11 (clean wound procedures) and £140 (non-clean wound procedures) per patient.
The results of the economic model are consistent with other literature which also demonstrates cost savings with the introduction of Plus Sutures compared with sutures that do not contain an antibacterial agent [38,39,40,41,42,43,44,45]. Only one study [40] was identified which adopted the same UK perspective and this estimated greater cost savings with the introduction of Plus Sutures compared than those reported in this work (£91 vs £14). The assumptions used in the current economic model presented a conservative case for the introduction of Plus Sutures. Therefore, the model outputs and cost savings are likely to be lower than those reported in other literature. Leaper and colleagues [40] also reported cost savings of £57 per clean wound procedures and £248 per non-clean wound procedures. These savings are greater than those estimated in this model. Leaper and colleagues [40] did not report the model inputs used, thus making direct comparisons challenging. However, it appears that the cost of SSI and the baseline risk of SSI with comparator sutures used in the Leaper model may have been higher than in the current study.
The baseline risk used for incidence of SSI with comparator sutures in this model is likely to underestimate the true incidence in the NHS due to lack of robust SSI surveillance and the fact that Plus Sutures are currently used in the UK. The PHE registry is likely to be subject to important selection biases that may produce lower estimates of SSI incidence than are observed in practice [36]. Data submission to the registry is mostly voluntary and is unlikely to identify SSIs arising in the community after discharge. These issues have also been acknowledged in published literature [99, 100]. Using a higher value for the incidence of SSI with comparator sutures increased the estimated cost savings with Plus Sutures. For example, where the higher baseline risk of SSI (1.97%) reported by Jenks et al. is used [5], the cost savings with Plus Sutures are estimated to be £30 per patient. Strengths of the economic analysis include that:
-
▪ The structure, inputs and results are aligned with previously published models and with models used in the UK’s health technology assessment agency guidance (NICE) [36, 37].
-
▪ The RR of SSI with triclosan-coated sutures was identified through a systematic review and meta-analysis and is based on a sizable body of RCTs with statistically significant confidence intervals estimated, and was judged to accurately reflect the range of patients and procedures within the NHS.
-
▪ Extensive sensitivity analyses were conducted, and the model results were robust to plausible changes in input parameters.
-
▪ Conservative parameter estimates/assumptions were used. Therefore, the uncertainty in the model is minimised and robust estimates of the cost savings associated with the use of Plus Sutures within the NHS are presented.
Limitations of the cost analysis include that:
-
▪ The source used for the baseline risk of SSI is widely accepted to underreport the incidence of SSI in the NHS. Therefore, the cost savings in the model may be underestimated.
-
▪ The source used for the cost of SSI is potentially outdated; however, a more suitable source could not be identified. If the average cost of SSI is higher than that reported by Jenks et al. [5], then the cost savings in the model may be underestimated. It was noted that several changes in clinical practice which have occurred since publication of the Jenks study. These changes include the number of infections caused by multi-drug resistant bacteria, which could result in longer duration of IV antibiotics and longer admissions in hospital, and the increase in complexity of care due to multi-morbidity of the population, which suggest the costs of SSI may have increased.
-
▪ QoL was not considered in the model (in line with the NICE MTEP methods guide [101]. However, it is very likely that a reduction in the incidence of SSI will impact on patient’s QoL [36, 102, 103].
Overall, the results of the cost analysis are likely to provide a good reflection of the impact of introducing Plus Sutures into routine care in the NHS. However, it is expected that these results underestimate the true savings that could be released within clinical practice from adoption of Plus Sutures across the NHS.
Although this analysis was conducted from a UK NHS perspective it is expected that the findings would generalise and Plus Sutures would lead to cost savings in other settings and countries. Indeed these results are in line with existing published cost analyses [38, 39, 41,42,43,44,45] of Plus Sutures conducted in other countries, which used varying methods to estimate costs across a range of patient populations and settings but all found the technology to be cost saving. The studies were conducted in Italy [38], Austria [39], the US [41, 44, 45], India [42] and Japan [43].
Environmental impact
The sustainability analysis demonstrated that the environmental impact of SSI is substantial. Furthermore, this analysis highlighted that the use of Plus Sutures, through a lowered risk of SSI, could result in potential environmental benefits to the healthcare systems. Although this analysis was consistent with the methods described in the SHC guidance and provided a reasonable estimate of the environmental impact, the identification of more specific data relating to some of the care pathway activities could enhance the overall accuracy of the environmental impact assessment.
Impacts associated with energy consumption for care pathway activities were sourced from the Sustainable Care Pathways Guidance [54], which is based on the UK government emission factor data. Therefore, climate impacts from energy consumption for other countries could vary, due to differences in national electricity grid mixes. However, it is likely that the general findings of this study regarding the contribution that specific activities of the pathway make to the overall environmental impact are likely applicable to wider settings.
Through reducing risk of SSI and subsequent antibiotic prescribing, Plus Sutures has potential to deliver a direct positive contribution to environmental sustainability across healthcare systems. A recent European Public Health Alliance report [104] states that antimicrobial resistance (AMR) jeopardises the achievement of sustainable development goals and includes a focus on infection prevention and control to reduce the need for antibiotics and consequently decreasing risk of antimicrobial resistance.
Triclosan has been used since the 1970s in consumer and professional products [105]. Its safety and effectiveness in consumer antiseptic washes and healthcare handwashes, scrubs, and skin preps was questioned because of insufficient data [106, 107]. However, Plus Sutures have been shown in vivo and in vitro to be non-toxic, non-irritating, non-carcinogenic, and non-teratogenic [105]. The small amount of triclosan used in Plus Sutures does not accumulate in the body and it is metabolized and excreted in a neutralised form [105]. Despite the theoretical possibility of resistance to Triclosan, there is no known clinical connection to antibiotic cross-resistance [108, 109]. In addition the Scientific Committee on Consumer Safety (SCCS) clearly states that “there is no evidence that using triclosan leads to an increase in antibiotic resistance…to preserve the role of triclosan in infection control and hygiene, SCCS can only recommend its prudent use, for instance limited to applications where a health benefit can be demonstrated…” [110]. There is a likely reduction of antibiotic prescribing as a consequence of the prevention of SSI with the routine use of Plus Suture [111]. In the opinion of the authors, this could have a beneficial impact and reduce the development of antimicrobial resistance.
This was the first time that an environmental sustainability analysis was included in a NICE MTEP submission and formed a key part of the final report. Given the increased interest and importance of assessing the impact on the environment, the methodology illustrated in this work can serve as an example to guide future evaluation of interventions.
Conclusions
Overall, the available evidence demonstrates that triclosan-coated sutures are associated with a reduced incidence of SSI across all surgery types. A qualitative analysis of safety outcomes found that no significant harms were reported, while the economic model indicated cost savings for Plus Sutures when compared with non-coated sutures that do not contain an antimicrobial agent. Furthermore, the environmental impact of SSI is substantial, and the introduction of Plus Sutures could result in potential environmental benefits.
More robust trials with standardized surgical protocols (in particular we would advocate the use of triclosan sutures for both fascia and skin closure), especially in low-income countries, are still needed to further validate the SSI incidence in these challenging environments. Safety outcomes should be more consistently reported across trials, as existing evidence around safety is weak.
Considering the available evidence, Plus Sutures appear to be a useful device to minimise the risk of SSI. This is aligned with recommendations included in global guidelines, including NICE SSI Guidelines [112], WHO Global guidelines [10] and the 2017 CDC guidelines [9] all of which recommend the use of triclosan-coated sutures for the purpose of reducing the risk of SSI, independent of the type of surgery.
Availability of data and materials
The protocol for this review was registered with the Open Science Foundation and can be accessed at https://osf.io/yvjna. The datasets used and/or analysed during the current study may be available from the corresponding author on reasonable request.
Abbreviations
- AMR:
-
Antimicrobial resistance
- ASEPSIS:
-
Additional treatment, serous discharge, erythema, purulent exudate, separation of tissues, isolation of bacteria, stay duration as an inpatient
- CADTH:
-
Canadian Agency for Drugs and Technologies in Health
- CDC:
-
Centers for Disease Control
- CI:
-
Confidence interval
- COPD:
-
Chronic obstructive pulmonary disease
- EUnetHTA:
-
European Network for Health Technology Assessment
- GHG:
-
Greenhouse gas
- HRQoL:
-
Health-related quality of life
- HTA:
-
Health technology assessment
- ITT:
-
Intention-to-treat
- MAUDE:
-
Manufacturer and User Facility Device Experience
- MHRA:
-
Medicines and Healthcare products Regulatory Agency
- MTEP:
-
Medical Technologies Evaluation Programme
- NHS:
-
National Health Service
- NICE:
-
National Institute for Health and Care Excellence
- PHE:
-
Public Health England
- PRISMA:
-
Preferred Reporting Items for Systematic Reviews and Meta-Analyses
- PSA:
-
Probabilistic sensitivity analysis
- RCT:
-
Randomized controlled trial
- RR:
-
Risk ratio
- SCCS:
-
Scientific Committee on Consumer Safety
- SSI:
-
Surgical site infection
- WHO:
-
World Health Organization
References
Leaper DJ. Surgical-site infection. Br J Surg. 2010;97(11):1601–2.
Owens CD, Stoessel K. Surgical site infections: epidemiology, microbiology and prevention. J Hosp Infect. 2008;70(Suppl 2):3–10.
National Healthcare Safety Network. Surgical Site Infection Event (SSI). Atlanta: Center for Disease Control; 2021. Available from: https://www.cdc.gov/nhsn/pdfs/pscmanual/9pscssicurrent.pdf.
Forrester JD, Maggio PM, Tennakoon L. Cost of health care-associated infections in the United States. J Patient Saf. 2022;18(2):e477–9.
Jenks PJ, Laurent M, McQuarry S, Watkins R. Clinical and economic burden of surgical site infection (SSI) and predicted financial consequences of elimination of SSI from an English hospital. J Hosp Infect. 2014;86(1):24–33.
NHS Resolution. Hospital acquired infections: fredom of information request [Webpage]. 2019. Last updated 2019. Cited September 2021. Available from: https://resolution.nhs.uk/foi-disclosure-log/hospital-acquired-infections/.
Kirkland KB, Briggs JP, Trivette SL, Wilkinson WE, Sexton DJ. The impact of surgical-site infections in the 1990s: attributable mortality, excess length of hospitalization, and extra costs. Infect Control Hosp Epidemiol. 1999;20(11):725–30.
Institute for Healthcare Improvement (IHI). Changes to prevent surgical site infection [webpage]. Boston, MA: IHI; 2021. [cited August 2021]. Available from: http://www.ihi.org/resources/Pages/Changes/ChangestoPreventSurgicalSiteInfection.aspx.
Berrios-Torres SI, Umscheid CA, Bratzler DW, Leas B, Stone EC, Kelz RR, et al. Centers for disease control and prevention guideline for the prevention of surgical site infection, 2017. JAMA Surg. 2017;152(8):784–91.
World Health Organization. Preventing surgical site infections: implementation approaches for evidence-based recommendations. Geneva: World Health Organization; 2018. Available from: https://www.who.int/publications/i/item/9789241514385.
Edmiston CE Jr, Krepel CJ, Marks RM, Rossi PJ, Sanger J, Goldblatt M, et al. Microbiology of explanted suture segments from infected and noninfected surgical patients. J Clin Microbiol. 2013;51(2):417–21.
Barker JC, Khansa I, Gordillo GM. A formidable foe is sabotaging your results: what you should know about biofilms and wound healing. Plast Reconstr Surg. 2017;139(5):1184e-e1194.
Robert Koch-Institute. Prevention of postoperative wound infections recommendation of the Commission for Hospital Hygiene and Infection Prevention (KRINKO) at the Robert Koch-Institute. Bundesgesundheitsbla. 2018;61(4):448–73.
Ling ML, Apisarnthanarak A, Abbas A, Morikane K, Lee KY, Warrier A, et al. APSIC guidelines for the prevention of surgical site infections. Antimicrob Resist Infect Control. 2019;8:174.
Ohge H, Mayumi T, Haji S, Kitagawa Y, Kobayashi M, Kobayashi M, et al. The Japan Society for Surgical Infection: guidelines for the prevention, detection, and management of gastroenterological surgical site infection, 2018. Surg Today. 2021;51(1):1–31.
De Simone B, Sartelli M, Coccolini F, Ball CG, Brambillasca P, Chiarugi M, et al. Intraoperative surgical site infection control and prevention: a position paper and future addendum to WSES intra-abdominal infections guidelines. World J Emerg Surg. 2020;15(1):10.
Lohsiriwat V, Chinswangwatanakul V, Lohsiriwat D, Rongrungruang Y, Malathum K, Ratanachai P, et al. Guidelines for the prevention of surgical site infection: the surgical infection society of Thailand recommendations (executive summary). J Med Assoc Thai. 2020;103(1):99–105.
Ming X, Rothenburger S, Yang D. In vitro antibacterial efficacy of MONOCRYL Plus antibacterial suture (Poliglecaprone 25 with triclosan). Surg Infect (Larchmt). 2007;8(2):201–8.
Rothenburger S, Spangler D, Bhende S, Burkley D. In vitro antimicrobial evaluation of Coated VICRYL* Plus antibacterial suture (coated polyglactin 910 with triclosan) using zone of inhibition assays. Surg Infect (Larchmt). 2002;3(suppl 1):S79-87.
Ming X, Rothenburger S, Nichols MM. In vivo and in vitro antibacterial efficacy of PDS plus (polidioxanone with triclosan) suture. Surg Infect (Larchmt). 2008;9(4):451–7.
Ban KA, Minei JP, Laronga C, Harbrecht BG, Jensen EH, Fry DE, et al. American College of Surgeons and Surgical Infection Society: surgical site infection guidelines, 2016 update. J Am Coll Surg. 2017;224(1):59–74.
Allegranzi B, Zayed B, Bischoff P, Kubilay NZ, de Jonge S, de Vries F, et al. New WHO recommendations on intraoperative and postoperative measures for surgical site infection prevention: an evidence-based global perspective. Lancet Infect Dis. 2016;16(12):e288–303.
National Health and Medical Research Council, Australian Commission on Safety and Quality in Healthcare. Australian guidelines for the prevention and control of infection in healthcare (2019). Canberra: National Health and Medical Research Council; 2019. Available from: https://www.nhmrc.gov.au/about-us/publications/australian-guidelines-prevention-and-control-infection-healthcare-2019.
National Institute for Health and Care Excellence (NICE). Plus Sutures for preventing surgical site infection. Medical technologies guidance [MTG59] [Webpage]. London & Manchester: NICE; 2021. Cited August 2021. Available from: https://www.nice.org.uk/guidance/mtg59.
National Institute for Health and Care Excellence (NICE). What we do [Webpage]. London & Manchester: NICE; 2022. Cited July 2022. Available from: https://www.nice.org.uk/about/what-we-do.
Higgins JPT, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, et al., editors. Cochrane handbook for systematic reviews of interventions [2nd edition] [updated October 2019]. https://training.cochrane.org/handbook/current: The Cochrane Collaboration; 2019. Available from: www.cochrane-handbook.org.
Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71.
Open Science Foundation. Open Science Foundation (OSF) database. Charlottesville: Center for Open Science; 2021. Cited February 2021. Available from: https://osf.io/.
Clarivate Analytics. Endnote [X9 for Windows & Mac]. [program] Philadelphia: Clarivate Analytics; 2018. Available from: http://endnote.com/.
Li T HJ, Deeks JJ. Chapter 5: Collecting data. In: Higgins JPT TJ, Chandler J, Cumpston M, Li T, Page MJ, Welch VA, editors. Cochrane Handbook for Systematic Reviews of Interventions version 6.1. London: Cochrane; 2020.
National Institute for Health and Care Excellence (NICE). Single technology appraisal: user guide for company evidence submission template [Webpage]. London & Manchester: NICE; 2021. Cited August 2021. Available from: https://www.nice.org.uk/process/pmg24/chapter/clinical-effectiveness.
Australian Government Department of Health and Ageing Pharmaceutical Benefits Advisory Committee (PBAC). Guidelines for preparing submissions to the Pharmaceutical Benefits Advisory Committee (version 5.0) Appendix 4. Canberra, Australia: PBAC; 2016. Available from: https://pbac.pbs.gov.au/content/information/files/pbac-guidelines-version-5.pdf.
R Core Team. A language and environment for statistical computing. Vienna: R Foundation for Statistical Computing; 2020. Cited February 2021. Available from: https://www.r-project.org/.
Balduzzi S, Rucker G, Schwarzer G. How to perform a meta-analysis with R: a practical tutorial. Evid Based Ment Health. 2019;22(4):153–60.
Harrer M, Cuijpers P, Furukawa T, Ebert DD. dmetar: Companion R package for the guide 'Doing meta-analysis in R,' R package version 0.0.9000. Erlangen: ProjectLab; 2019. Cited February 2021. Available from: http://dmetar.protectlab.org/.
National Institute for Health and Care Excellence. Surgical site infections: prevention and treatment. Health economic model report. England: 2019. Available from: https://www.nice.org.uk/guidance/ng125/evidence/health-economic-model-report-pdf-6727106989.
National Institute for Health and Care Excellence. Leukomed sorbact for preventing surgical site infection. England: 2021. Available from: https://www.nice.org.uk/guidance/mtg55.
Ceresoli M, Carissimi F, Piemontese A, Paragò V, Galvain T, Tommaselli GA, et al. The clinical and economic value of triclosan-coated surgical sutures in abdominal surgery. Appl Sci. 2020;10(3):1090.
Fleck T, Moidl R, Blacky A, Fleck M, Wolner E, Grabenwoger M, et al. Triclosan-coated sutures for the reduction of sternal wound infections: economic considerations. Ann Thorac Surg. 2007;84(1):232–6.
Leaper DJ, Edmiston CE Jr, Holy CE. Meta-analysis of the potential economic impact following introduction of absorbable antimicrobial sutures. Br J Surg. 2017;104(2):e134–44.
Leaper DJ, Holy CE, Spencer M, Chitnis A, Hogan A, Wright GWJ, et al. Assessment of the risk and economic burden of surgical site infection following colorectal surgery using a US longitudinal database: is there a role for innovative antimicrobial wound closure technology to reduce the risk of infection? Dis Colon Rectum. 2020((Leaper) Department of Surgery, University of Newcastle, Australia):1628–38.
Mahajan N, Pillai R, Chopra H, Grover A, Kohli A. An economic model to assess the value of triclosan-coated sutures in reducing the risk of surgical-site infection in coronary artery bypass graft in India. J Indian Coll Cardiol. 2020;10(2):79–84.
Nakamura T, Kashimura N, Noji T, Suzuki O, Ambo Y, Nakamura F, et al. Triclosan-coated sutures reduce the incidence of wound infections and the costs after colorectal surgery: a randomized controlled trial. Surgery. 2013;153(4):576–83.
Singh A, Bartsch SM, Muder RR, Lee BY. An economic model: value of antimicrobial-coated sutures to society, hospitals, and third-party payers in preventing abdominal surgical site infections. Infect Control Hosp Epidemiol. 2014;35(8):1013–20.
Stone J, Gruber TJ, Rozzelle CJ. Healthcare savings associated with reduced infection rates using antimicrobial suture wound closure for cerebrospinal fluid shunt procedures. Pediatr Neurosurg. 2010;46(1):19–24.
Public Health England. Surveillance of surgical site infections in NHS hospitals in England: April 2019 to March 2020. London: Public Health England; 2020. Available from: https://www.gov.uk/government/publications/surgical-site-infections-ssi-surveillance-nhs-hospitals-in-england.
Wong JLC, Ho CWY, Scott G, Machin JT, Briggs TWR. Getting It Right First Time: the national survey of surgical site infection rates in NHS trusts in England. Ann R Coll Surg Engl. 2019;101(7):463–71.
Danwang C, Bigna JJ, Tochie JN, Mbonda A, Mbanga CM, Nzalie RNT, et al. Global incidence of surgical site infection after appendectomy: a systematic review and meta-analysis. BMJ Open. 2020;10(2):e034266.
Boomer LA, Cooper JN, Deans KJ, Minneci PC, Leonhart K, Diefenbach KA, et al. Does delay in appendectomy affect surgical site infection in children with appendicitis? J Pediatr Surg. 2014;49(6):1026–9 (discussion 29).
Collaborative GlobalSurg. Surgical site infection after gastrointestinal surgery in children: an international, multicentre, prospective cohort study. BMJ Glob Health. 2020;5(12):e003429.
Troughton R, Birgand G, Johnson AP, Naylor N, Gharbi M, Aylin P, et al. Mapping national surveillance of surgical site infections in England: needs and priorities. J Hosp Infect. 2018;100(4):378–85.
Personal Social Services Research Unit (PSSRU). Unit costs of health & social care 2020. Canterbury: PSSRU; 2020. Available from: https://www.pssru.ac.uk/project-pages/unit-costs/.
Perencevich EN, Sands KE, Cosgrove SE, Guadagnoli E, Meara E, Platt R. Health and economic impact of surgical site infections diagnosed after hospital discharge. Emerg Infect Dis. 2003;9(2):196–203.
Coalition for Sustainable Pharmaceuticals and Medical Devices. Care pathways: guidance on appraising sustainability. Cambridge: NHS Sustainable Development Unit; 2015. Cited February 2021. Available from: https://www.sduhealth.org.uk/areas-of-focus/carbon-hotspots/pharmaceuticals/cspm/sustainable-care-pathways-guidance.aspx.
Coello R, Charlett A, Wilson J, Ward V, Pearson A, Borriello. Adverse impact of surgical site infections in English hospitals. J Hosp Infect. 2005;60(2):93–103.
Shepard J, Ward W, Milstone A, Carlson T, Frederick J, Hadhazy E, et al. Financial impact of surgical site infections on hospitals: the hospital management perspective. JAMA Surg. 2013;148(10):907–14.
Ruiz-Tovar J, Alonso N, Morales V, Llavero C. Association between Triclosan-Coated Sutures for Abdominal Wall Closure and Incisional Surgical Site Infection after Open Surgery in Patients Presenting with Fecal Peritonitis: A Randomized Clinical Trial. Surg Infect (Larchmt). 2015;16(5):588–94.
Soomro R, Khurshaidi N, Rahman SSU, Hassan R. Does antibiotic coated polyglactin helps in reducing surgical site infection in clean surgery? Medical Forum Monthly. 2017;28(2):23–6.
Arslan NC, Atasoy G, Altintas T, Terzi C. Effect of triclosan-coated sutures on surgical site infections in pilonidal disease: prospective randomized study. Int J Colorectal Dis. 2018;33(10):1445–52.
Baracs J, Huszar O, Sajjadi SG, Horvath OP. Surgical site infections after abdominal closure in colorectal surgery using triclosan-coated absorbable suture (PDS Plus) vs. uncoated sutures (PDS II): a randomized multicenter study. Surg Infect (Larchmt). 2011;12(6):483–9.
Diener MK, Knebel P, Kieser M, Schuler P, Schiergens TS, Atanassov V, et al. Effectiveness of triclosan-coated PDS Plus versus uncoated PDS II sutures for prevention of surgical site infection after abdominal wall closure: the randomised controlled PROUD trial. Lancet. 2014;384(9938):142–52.
Ford HR, Jones P, Gaines B, Reblock K, Simpkins DL. Intraoperative handling and wound healing: controlled clinical trial comparing coated VICRYL plus antibacterial suture (coated polyglactin 910 suture with triclosan) with coated VICRYL suture (coated polyglactin 910 suture). Surg Infect (Larchmt). 2005;6(3):313–21.
Galal I, El-Hindawy K. Impact of using triclosan-antibacterial sutures on incidence of surgical site infection. Am J Surg. 2011;202(2):133–8.
Ichida K, Noda H, Kikugawa R, Hasegawa F, Obitsu T, Ishioka D, et al. Effect of triclosan-coated sutures on the incidence of surgical site infection after abdominal wall closure in gastroenterological surgery: a double-blind, randomized controlled trial in a single center. Surgery. 2018;164(1):91–5.
Isik I, Selimen D, Senay S, Alhan C. Efficiency of antibacterial suture material in cardiac surgery: a double-blind randomized prospective study. Heart Surg Forum. 2012;15(1):E40-45.
Justinger C, Slotta JE, Ningel S, Graber S, Kollmar O, Schilling MK. Surgical-site infection after abdominal wall closure with triclosan-impregnated polydioxanone sutures: results of a randomized clinical pathway facilitated trial (NCT00998907). Surgery. 2013;154(3):589–95.
Karip AB, Celik K, Aydin T, Yazicilar H, Iscan Y, Agalar C, et al. Effect of triclosan-coated suture and antibiotic prophylaxis on infection and recurrence after karydakis flap repair for pilonidal disease: a randomized parallel-arm double-blinded clinical trial. Surg Infect (Larchmt). 2016;17(5):583–8.
Lin S-J, Chang F-C, Huang T-W, Peng K-T, Shih HN, Lee MS. Temporal change of interleukin-6, C-ceactive protein, and skin temperature after total knee arthroplasty using triclosan-coated sutures. Biomed Res Int. 2018:9136208.
Mattavelli I, Rebora P, Doglietto G, Dionigi P, Dominioni L, Luperto M, et al. Multi-center randomized controlled trial on the effect of triclosan-coated sutures on surgical site infection after colorectal surgery. Surg Infect (Larchmt). 2015;16(3):226–35.
Mingmalairak C, Ungbhakorn P, Paocharoen V. Efficacy of antimicrobial coating suture coated polyglactin 910 with tricosan (Vicryl Plus) compared with polyglactin 910 (Vicryl) in reduced surgical site infection of appendicitis, double blind randomized control trial, preliminary safety report. J Med Assoc Thai. 2009;92(6):770–5.
Olmez T, Berkesoglu M, Turkmenoglu O, Colak T. Effect of triclosan-coated suture on surgical site infection of abdominal fascial closures. Surg Infect (Larchmt). 2019;20(8):658–64.
Rasic Z, Schwarz D, Adam VN, Sever M, Lojo N, Rasic D, et al. Efficacy of antimicrobial triclosan-coated polyglactin 910 (Vicryl* Plus) suture for closure of the abdominal wall after colorectal surgery. Coll Antropol. 2011;35(2):439–43.
Renko M, Paalanne N, Tapiainen T, Hinkkainen M, Pokka T, Kinnula S, et al. Triclosan-containing sutures versus ordinary sutures for reducing surgical site infections in children: a double-blind, randomised controlled trial. Lancet Infect Dis. 2017;17(1):50–7.
Rozzelle CJ, Leonardo J, Li V. Antimicrobial suture wound closure for cerebrospinal fluid shunt surgery: a prospective, double-blinded, randomized controlled trial. J Neurosurg Pediatrics. 2008;2(2):111–7.
Ruiz-Tovar J, Llavero C, Jimenez-Fuertes M, Duran M, Perez-Lopez M, Garcia-Marin A. Incisional Surgical Site Infection after Abdominal Fascial Closure with Triclosan-Coated Barbed Suture vs Triclosan-Coated Polydioxanone Loop Suture vs Polydioxanone Loop Suture in Emergent Abdominal Surgery: A Randomized Clinical Trial. J Am Coll Surg. 2020;230(5):766–74.
Santos PSF, Santos M, Colafranceschi AS, Pragana ANdS, Correia MG, Simoes HH, et al. Effect of Using Triclosan-Impregnated Polyglactin Suture to Prevent Infection of Saphenectomy Wounds in CABG: A Prospective, Double-Blind, Randomized Clinical Trial. Braz. 2019;34(5):588–95.
Seim BE, Tonnessen T, Woldbaek PR. Triclosan-coated sutures do not reduce leg wound infections after coronary artery bypass grafting. Interact Cardiovasc Thorac Surg. 2012;15(3):411–5.
Sprowson AP, Jensen C, Parsons N, Partington P, Emmerson K, Carluke I, et al. The effect of triclosan-coated sutures on the rate of surgical site infection after hip and knee arthroplasty: a double-blind randomized controlled trial of 2546 patients. Bone Joint J. 2018;100-B(3):296–302.
Sukeik M, George D, Gabr A, Kallala R, Wilson P, Haddad FS. Randomised controlled trial of triclosan coated vs uncoated sutures in primary hip and knee arthroplasty. World J Orthop. 2019;10(7):268–77.
Sundaram K, Warren J, Klika A, Piuzzi N, Mont M, Krebs V. Barbed sutures reduce arthrotomy closure duration compared to interrupted conventional sutures for total knee arthroplasty: a randomized controlled trial. Musculoskelet Surg. 2020a. Available from: https://link.springer.com/article/10.1007/s12306-020-00654-y.
Sundaram K, Piuzzi NS, Klika AK, Molloy RM, Higuera-Rueda CA, Krebs VE, et al. Barbed sutures reduce arthrotomy closure duration and suture utilisation compared to interrupted conventional sutures for primary total hip arthroplasty: a randomised controlled trial. Hip Int. 2020b: 1120700020911891. Available from: https://journals.sagepub.com/doi/pdf/10.1177/1120700020911891.
Tabrizi R, Mohajerani H, Bozorgmehr F. Polyglactin 910 suture compared with polyglactin 910 coated with triclosan in dental implant surgery: randomized clinical trial. Int J Oral Maxillofac Surg. 2019;48(10):1367–71.
Thimour-Bergstrom L, Roman-Emanuel C, Schersten H, Friberg O, Gudbjartsson T, Jeppsson A. Triclosan-coated sutures reduce surgical site infection after open vein harvesting in coronary artery bypass grafting patients: a randomized controlled trial. Eur J Cardiothorac Surg. 2013;44(5):931–8.
Turtiainen J, Saimanen EIT, Makinen KT, Nykanen AI, Venermo MA, Uurto IT, et al. Effect of triclosan-coated sutures on the incidence of surgical wound infection after lower limb revascularization surgery: a randomized controlled trial. World J Surg. 2012;36(10):2528–34.
Williams N, Sweetland H, Goyal S, Ivins N, Leaper DJ. Randomized trial of antimicrobial-coated sutures to prevent surgical site infection after breast cancer surgery. Surg Infect (Larchmt). 2011;12(6):469–74.
Zhang Z-T, Zhang H-W, Fang X-D, Wang L-M, Li X-X, Li Y-F, et al. Cosmetic outcome and surgical site infection rates of antibacterial absorbable (Polyglactin 910) suture compared to Chinese silk suture in breast cancer surgery: a randomized pilot research. Chin Med J. 2011;124(5):719–24.
International Civil Aviation Organization (ICAO). ICAO carbon emissions calculator [Webpage]. ICAO; 2016. Cited September 2021. Available from: https://www.icao.int/environmental-protection/carbonoffset/pages/default.aspx.
EurEau. Europe’s water in figures: an overview of the European drinking water and waste water sectors. Brussels, Belgium: EurEau; 2021. Available from: https://www.eureau.org/resources/publications/eureau-publications/5824-europe-s-water-in-figures-2021/file.
EUROSTAT Statistics Explained. Municipal waste statistics. Luxembourg: EUROSTAT; December 2021. Available from: https://ec.europa.eu/eurostat/statistics-explained/index.php?title=Municipal_waste_statistics.
Ahmed I, Boulton AJ, Rizvi S, Carlos W, Dickenson E, Smith NA, et al. The use of triclosan-coated sutures to prevent surgical site infections: a systematic review and meta-analysis of the literature. BMJ Open. 2019;9(9):e029727.
De Jonge SW, Atema JJ, Solomkin JS, Boermeester MA. Meta-analysis and trial sequential analysis of triclosan-coated sutures for the prevention of surgical-site infection. Br J Surg. 2017;104(2):e118–33.
Onesti MG, Carella S, Scuderi N. Effectiveness of antimicrobial-coated sutures for the prevention of surgical site infection: a review of the literature. Eur Rev Med Pharmacol Sci. 2018;22(17):5729–39.
Otto-Lambertz C, Decker L, Adams A, Yagdiran A, Eysel P. Can triclosan-coated sutures reduce the postoperative rate of wound infection? Data from a systematic review and meta-analysis. Surgery. 2023;174(3):638–46.
National Institute of Health Research Unit on Global Surgery. Alcoholic chlorhexidine skin preparation or triclosan-coated sutures to reduce surgical site infection: a systematic review and meta-analysis of high-quality randomised controlled trials. Lancet Infect Dis. 2022;22(8):1242–51.
National Institute for Health and Care Excellence. Plus Sutures for preventing surgical site infection: Medtech innovation briefing [MIB204]. London: NICE; 2020. Available from: https://www.nice.org.uk/advice/mib204.
Nihr Global Research Health Unit on Global Surgery. Reducing surgical site infections in low-income and middle-income countries (FALCON): a pragmatic, multicentre, stratified, randomised controlled trial. Lancet. 2021;398(10312):1687–99.
Boutron I, Page M, Higgins J, Altman D, Lundh A, Hróbjartsson A. Chapter 7.6.2: Including risk-of-bias assessments in analyses. In: Higgins JPT, Green S, editors. Cochrane Handbook for Systematic Reviews of Interventions Version 6.3 (updated 2022). The Cochrane Collaboration. 2022. Available from: https://training.cochrane.org/handbook/current/chapter-07#section-7-6.
Public Health England. Surveillance of surgical site infections in NHS hospitals in England. England: 2020. Available from: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/945712/SSI_Annual_Report_2019_20.pdf.
Singh S, Davies J, Sabou S, Shrivastava R, Reddy S. Challenges in reporting surgical site infections to the national surgical site infection surveillance and suggestions for improvement. Ann R Coll Surg Engl. 2015;97(6):460–5.
Tanner J, Padley W, Kiernan M, Leaper D, Norrie P, Baggott R. A benchmark too far: findings from a national survey of surgical site infection surveillance. J Hosp Infect. 2013;83(2):87–91.
National Institute for Health and Care Excellence (NICE). Medical technologies evaluation programme methods guide: process and methods [PMG33] [Webpage]. London & Manchester: NICE; 2017. Cited August 2021. Available from: https://www.nice.org.uk/process/pmg33/chapter/introduction.
Matza LS, Kim KJ, Yu H, Belden KA, Chen AF, Kurd M, et al. Health state utilities associated with post-surgical staphylococcus aureus infections. Eur J Health Econ. 2019;20(6):819–27.
Gheorghe A, Moran G, Duffy H, Roberts T, Pinkney T, Calvert M. Health utility values associated with surgical site infection: a systematic review. Value Health. 2015;18(8):1126–37.
Vettore G. Roadmap for action on antimicrobial resistance (AMR). Brussels: European Public Health Alliance; 2019. Cited February 2021. Available from: https://epha.org/roadmap-for-action-on-antimicrobial-resistance-amr/.
Barbolt TA. Chemistry and safety of triclosan, and its use as an antimicrobial coating on Coated VICRYL* Plus antibacterial suture (coated polyglactin 910 suture with triclosan). Surg Infect (Larchmt). 2002;3(Suppl 1):S45-53.
Food and Drug Administration (FDA). Safety and effectiveness of consumer antiseptics; topical antimicrobial drug products for over-the-counter human use [Webpage]. FederalRegister.gov; 2016. Last updated 06 Sept 2016. Cited 05 April 2022. Available from: https://www.federalregister.gov/documents/2016/09/06/2016-21337/safety-and-effectiveness-of-consumer-antiseptics-topical-antimicrobial-drug-products-for.
Food and Drug Administration (FDA). Safety and effectiveness of health care antiseptics; topical antimicrobial drug products for over-the-counter human use [Webpage]. FederalRegister.gov; 2017. Last updated 20 Dec 2017. Cited 05 April 2022. Available from: https://www.federalregister.gov/documents/2017/12/20/2017-27317/safety-and-effectiveness-of-health-care-antiseptics-topical-antimicrobial-drug-products-for.
Leaper D, Wilson P, Assadian O, Edmiston C, Kiernan M, Miller A, et al. The role of antimicrobial sutures in preventing surgical site infection. Ann R Coll Surg Engl. 2017;99(6):439–43.
Cole EC, Addison RM, Rubino JR, Leese KE, Dulaney PD, Newell MS, et al. Investigation of antibiotic and antibacterial agent cross-resistance in target bacteria from homes of antibacterial product users and nonusers. J Appl Microbiol. 2003;95(4):664–76.
European Commission, Scientific Committee on Consumer Safety. Triclosan and Antibiotics resistance [Webpage]. Brussels, Belgium: 2010. Cited 05 April 2022. Available from: https://ec.europa.eu/health/scientific_committees/opinions_layman/triclosan/en/index.htm.
National Institute for Health and Care Excellence (NICE). Medical technologies guidance: MT507 Plus sutures for preventing surgical site infection. Supporting documentation - committee papers [Webpage]. London: National Institute for Health and Care Excellence; 2021. Cited 05 April 2022. Available from: https://www.nice.org.uk/guidance/mtg59/documents/supporting-documentation.
National Institute for Health and Care Excellence. Surgical site infections: prevention and treatment [NG125]. London: NICE; 2020. Available from: https://www.nice.org.uk/guidance/ng125.
Acknowledgements
The authors with to thank the following individuals for their contributions to the review and analyses.
J&J: Gianluca Casali, Meagen Hicks, Brian Chen, Suzi Patel
YHEC: Joe Moss (statistician), Emily Gregg (medical writer), Mick Arber (information specialist), Michelle Jenks (economic modelling), Emma Carr and Deborah Watkins (research assistants)
Funding
This systematic review and meta-analysis was funded by Johnson & Johnson Medical Devices and conducted by York Health Economics Consortium.
The funders contributed to the design of the protocol for the systematic review and analyses, as well as the decision to publish the results and the writing of the manuscript. Searches, study se-lection, data extraction and qualitative analysis were conducted independently by YHEC, with search strategies and data collection forms approved by J&J.
Author information
Authors and Affiliations
Contributions
Conceptualisation, TG and WD; methodology, SG, ME, TG, MK and JS; investigation, SG, ME, TG, MK and JS; data curation, ME, SG, TG, MK and JS; software, TG, MK and JS; formal analysis, SG, ME, TG, MK and JS; writing—original draft preparation, ME, SG, JS, TG, WD, MK; writing—review and editing, ME, SG, JS, TG, WD, MK, DP, DB and KJH; supervision, TG, WD and SG; project administration, TG, WD and SG. All authors have read and agreed to the published version of the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Ethics approval was not applicable to this work as the analyses synthesise existing aggregate data.
Consent for publication
Not applicable.
Competing interests
SG and ME are employees of YHEC and were commissioned by J&J to plan and conduct the systematic review, feasibility assessment, and qualitative analysis of results described in this publication. JS was an employee of YHEC at the time of conducting the review and analyses and writing the manuscript.
TG, WD, AK and NDS are employees of J&J.
DJP, DB and KJH provided independent clinical support for the project. DJP has been funded by the Royal College of Surgeons of England. He receives consulting fees from Johnson & Johnson and Novo Nordisk and payments for lectures, presentations, and educational events from Johnson & Johnson, Medtronic, and Novo Nordisk. DB and KJH have no competing interests to declare.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: Supplementary Figure 1.
Search strategies. Supplementary Table 1. Model inputs. Supplementary Figure 2. Structure of the environmental model. Supplementary Table 2. Environmental sustainability model inputs. Supplementary Table 3. Documents excluded at full text review (n = 108). Supplementary Table 4. Studies included in the review. Supplementary Table 5. Summary of review included study characteristics. Supplementary Table 6. Summary of review included study population details. Supplementary Table 7. Risk of bias assessment of studies included in the review. Supplementary Table 8. Antibiotic use for SSI (presenting only those studies reporting eligible data by arm). Supplementary Table 9. Hospital stay (presenting only those studies reporting eligible data by arm). Supplementary Table 10. Severity of SSIs (presenting only those studies reporting eligible data by arm). Supplementary Figure 3. Baujat diagnostic plot. Supplementary Figure 4. Leave-One-Out analysis. Supplementary Figure 5. Publication bias: funnel plot. Supplementary Figure 6a. Meta- analysis results – Adult only SSI incidence studies (with Stratafix). Supplementary Figure 6b. Meta- analysis results – Children only SSI incidence studies (with Stratafix). Supplementary Figure 6c. Meta- analysis results – Clean wound only SSI incidence studies (with Stratafix). Supplementary Figure 6d. Meta- analysis results – Non-clean wound only SSI incidence studies (with Stratafix). Supplementary Figure 7. Meta- analysis results – Without Stratafix sensitivity analysis. Supplementary Figure 8. Meta- analysis results – including Falcon trial. Supplementary Figure 9. Labbe plot – including Falcon trial. Supplementary Figure 10. Baujat plot – including Falcon trial. Supplementary Figure 11. Left-one-out plot – including Falcon trial. Supplementary Figure 12. Funnel plot – including Falcon trial. Supplementary Table 11. Threshold/breakeven analyses results. Supplementary Table 12. Subgroup analyses for adults only. Supplementary Table 13. Subgroup analyses for children only. Supplementary Table 14. Subgroup analyses for clean wounds only. Supplementary Table 15. Subgroup analyses for non-clean wounds only. PRISMA 2020 Checklist. Supplementary Appendix A. Full Search Strategies for the Systematic Review.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Edwards, M., Graziadio, S., Shore, J. et al. Plus Sutures for preventing surgical site infection: a systematic review of clinical outcomes with economic and environmental models. BMC Surg 23, 300 (2023). https://doi.org/10.1186/s12893-023-02187-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12893-023-02187-0