
Abstract
Background
Colorectal cancer (CRC) is a frequent cancer worldwide with varied survival outcomes.
Objective
We aimed to develop a nomogram model to predict the overall survival (OS) of CRC patients after surgery.
Design
This is a retrospective study.
Setting
This study was conducted from 2015 to 2016 in a single tertiary center for CRC.
Patients
CRC patients who underwent surgery between 2015 and 2016 were enrolled and randomly assigned into the training (n = 480) and validation (n = 206) groups. The risk score of each subject was calculated based on the nomogram. All participants were categorized into two subgroups according to the median value of the score.
Main outcome measures
The clinical characteristics of all patients were collected, significant prognostic variables were determined by univariate analysis. Least absolute shrinkage and selection operator (LASSO) regression was applied for variable selection. The tuning parameter (λ) for LASSO regression was determined by cross-validation. Independent prognostic variables determined by multivariable analysis were used to establish the nomogram. The predictive capacity of the model was assessed by risk group stratification.
Results
Infiltration depth, macroscopic classification, BRAF, carbohydrate antigen 19 − 9 (CA-199) levels, N stage, M stage, TNM stage, carcinoembryonic antigen levels, number of positive lymph nodes, vascular tumor thrombus, and lymph node metastasis were independent prognostic factors. The nomogram established based on these factors exhibited good discriminatory capacity. The concordance indices for the training and validation groups were 0.796 and 0.786, respectively. The calibration curve suggested favorable agreement between predictions and observations. Moreover, the OS of different risk subgroups was significantly different.
Limitations
The limitations of this work included small sample size and single-center design. Also, some prognostic factors could not be included due to the retrospective design.
Conclusions
A prognostic nomogram for predicting the OS of CRC patients after surgery was developed, which might be helpful for evaluating the prognosis of CRC patients.
Similar content being viewed by others


Introduction
Colorectal cancer (CRC) is the third most diagnosed carcinoma and the leading cause of cancer-related death worldwide. It is the third most common cancer in women and the second in men [1, 2]. Globally, there were over 1 million newly diagnosed cases and approximately 500,000 deaths per year [3]. In China, the incidence and mortality of CRC continue to increase [4, 5].
Surgical intervention remains the main treatment strategy for CRC and adjuvant therapy is recommended for high-risk patients. The TNM staging system is widely applied to predict the prognosis for CRC patients. However, significant heterogeneity in the survival outcomes of patients at the same TNM stage has been observed due to the diversity of cancer biology and clinicopathological characteristics [6, 7]. Moreover, the TNM alone cannot provide enough individualized predictions for postoperative CRC patients [8, 9]. Hence, it is necessary to develop a prognostic model for personalized probabilistic predictions.
Nomograms are statistical tools that calculate the probability of individual clinical events based on determinants and prognostic characteristics [10]. Nomogram prediction models provide individualized probability estimates of death for each patient. Several studies have established nomogram models to predict overall postoperative survival of colorectal cancer patients [11,12,13]. Some variables are included in these nomogram models, such as age and sex. However, it is worth noting that these studies are characterized by long time span of data sets and few variables included. New pathologic and molecular markers such as perineuronal infiltration, mismatch repair status, and RAS/RAF mutation status were not included in the data analysis. As a result, these columns are not applicable to the current patient. In this study, these new pathological and molecular markers were also incorporated into the data analysis. This will help predict survival rates for colon cancer patients more accurately.
In this study, a prognostic nomogram model for personalized probabilistic predictions of the overall survival (OS) of CRC patients after surgery was developed using tumor-related factors and patient-related factors (e.g. age, diabetes, hypertension). This model may help physicians predict the OS of each patient without incurring additional costs.
Materials and methods
Subjects and ethical approval
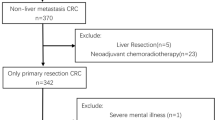
In this retrospective, single-center study, CRC patients who underwent surgery in our hospital between April 2015 and December 2016. The inclusion criteria: (1) the diagnosis of CRC was made in our department and confirmed by pathological findings; (2) patients underwent radical surgical excision to remove primary tumors. The following cases were excluded: (1) patients with unknown prognosis or incomplete follow-up data; (2) patients who had received radiotherapy, chemotherapy, or chemoradiotherapy prior to enrollment; (3) patients with other primary malignant tumors, acute infection, or severe liver disease; (4) patients who have died from non-cancer causes. Finally, 686 patients were enrolled. The case registration process is shown in Fig. 1. The start of the follow-up was the patient’s diagnosis time, the end of the follow-up was on July 9, 2020, the follow-up duration was 7 to 75 months, and the median follow-up duration was 27.00 months.

The Research flow chart for this study
This work was registered at China Clinical Trial Registry (Registration No. ChiCTR 2,100,043,775) and approved by local ethics committee (Approval No. 2020kt417). Informed consent was waived because of the retrospective design.
Clinical data
The clinical characteristics of all patients were collected, including sex, age, BRAF type, KRAS type, MLH1 type, MSH2 type, MSH6 type, PMS2 type, tumor site, history of diabetes, history of hypertension, history of aspirin use, carbohydrate antigen 19 − 9 (CA-199) levels, CA-724 levels, carcinoembryonic antigen (CEA) levels, WBC count (i.e. leukocytes and white blood cells), neutrophil count, platelet count, platelet to lymphocyte ratio (PLR), pathological type, degree of differentiation, infiltration depth, lymphocyte count, neutrophil to lymphocyte ratio (NLR), vascular tumor thrombus, nerve invasion, N stage, M stage, number of positive lymph node (LN), TNM stage, LN metastasis, macroscopic classification, tumor size (long diameter) and Chemotherapy.
Variable selection
Univariate Cox regression analysis was used to explore the clinical characteristics that associated with the OS of CRC patients significantly. Least absolute shrinkage and selection operator (LASSO) regression is a shrinkage method that can reduce the likelihood of overfitting by actively selecting from a large set of variables and decreasing the regression coefficient [14, 15]. In this study, significant variables identified by univariate analysis were selected by LASSO regression using the R package “glmnet”. Dummy variables were generated for categorical variables. The tuning parameter λ was determined by cross-validation. Finally, multivariate Cox regression analysis was performed to identify independent risk or protective factors for the OS of patients. P < 0.05 indicated statistical significance.
Nomogram construction
The R package “rms” was used to construct the nomogram model. Independent risk or protective factors were included in the nomogram and 1-, 3-, and 5-year OS were predicted.
Nomogram validation
The concordance index (C-index; range: 0.5–1.0) was calculated using the R software to validate the nomogram. The closer to 1 the value, the higher the discriminatory capacity of the model. The C-indices were calculated by Cox regression models and the discrimination for nomogram models were estimated by C-index. Calibration curves were used to assess the difference between actual observations and predictions by the nomogram, in which a 45-degree line indicated perfect agreement between observed and predicted probabilities. C-index is between 0.5 and 1. 0.5 is completely random, indicating that the model has no predictive effect, and 1 is completely consistent, indicating that the prediction results of the model are completely consistent with reality. Previous studies believed that C-index between 0.50 and 0.70 was low accuracy; between 0.71 and 0.90 was moderate accuracy; and higher than 0.90 was high accuracy [16,17,18]. Decision curve analysis (DCA) is a widely used method to measure clinical utility [19, 20]. In this study, the threshold probability and net benefit of the nomogram and TNM stage were determined by DCA using the R package “rmda”. The sensitivity and specificity of nomogram was determined by receiver operating characteristics (ROC) curves.
Risk group stratification
The risk score of each subject was calculated using the formula:
The ORi was the OR value in multivariate Cox regression analysis and xi was the z-score-transformed value of each factor in nomogram. All participants were categorized into high-risk and low-risk group according to the median value of the score. Score distribution in all patients and the number of patients with low or high scores were assessed.
Statistical analysis
R software (version 4.0.1) and SPSS (version 20.0; Chicago, IL, USA) were used for data analysis. Independent t test or Mann-Whitney U test were used for continuous variables, and Fisher’s exact test or Chi-square test were used for categorical variables to evaluate the differences in clinical features among each group. Three or more groups were compared using Analysis of variance (ANOVA) and Kruskal-Wallis H test. Survival curves were generated by Kaplan–Meier method and compared by two-sided log-rank test. P < 0.05 indicated statistical significance.
Results
Patients
A total of 686 CRC patients (403 males; 283 females) were enrolled and randomly assigned into two groups at a ratio of 7:3 (training group, n = 480; validation group, n = 206). The clinical characteristics of both groups are shown in Table 1.
Variable selection
Univariate Cox regression analysis was used to explore the clinical characteristics that associated with the OS of CRC patients significantly. And in the univariate analysis, 12 variables had P values less than 0.05, which were shown in Table 2. Moreover, the survival curves of 12 variables was shown in Fig. 2.

The survival curves of 12 variables had P values less than 0.05. (A) Infiltration depth (B) Macroscopic classification (C) BRAF (D) Vascular tumor thrombus (E) CA-199 (F) Lymph node metastasis (G) CEA (H) N stage (I) TNM stage (J) Number of positive lymph nodes (K) Metastasis (L) Chemotherapy
The most appropriate tuning parameter (λ) for LASSO regression was 0.12 when partial likelihood binomial deviation reached its minimum value (Fig. 3A). Furthermore, seven characteristics with were selected by LASSO regression, including BRAF, number of positive lymph nodes, CEA levels, CA-199 levels, M stage, TNM stage, and macroscopic classification (Fig. 3B). Multivariate analysis was then applied and five independent risk or protective factors were identified, including CEA levels (OR = 1.00, P = 0.001), CA-199 levels (OR = 1.00, P = 0.041), TNM stage (OR = 2.09, P = 0.004), number of positive LN (OR = 1.15, P < 0.001), and macroscopic classification (OR = 0.54, P = 0.043) (Fig. 3C). The above variables were used to construct the nomogram. As metastasis state is a well-recognized risk factor for the prognosis of CRC patients, M stage was also included in the nomogram model.

Variables selection using LASSO and multivariate Cox regression analysis. (A, B) Selection of the most appropriate penalty parameter (λ) for LASSO regression, and the LASSO regression selected seven variables. (C). Forrest plot of multivariate Cox regression analysis
Nomogram construction and performance
The nomogram was developed using variables selected by multivariate analysis (Fig. 4). A vertical line was drawn from the point on the top row and a point was assigned for each variable. By drawing a vertical line from the points to the result axis, the predicted survival probability can be obtained. For training group, the C-index was 0.796, suggesting well discriminatory capacity. Calibration curve showed favorable agreement between actual observations and predictions (Fig. 5). The high-risk threshold, standardized net benefit, and benefit ratio of the nomogram were determined by DCA (Fig. 6). The threshold probability for 3- and 5-year survival was > 0, indicating that the use of the nomogram provided more benefits than treatment/non-treatment for predicting the survival. Nomogram model also showed more benefits for predicting the 3- and 5-year OS of these patients than TNM stage. The area under the ROC curve for 1-, 3-, and 5-survival of the training group was 0.840, 0.778, and 0.871, respectively (Fig. 7A).

Nomogram model for predicting the survival rate of patients at 1, 3, and 5 years in in the training group

Calibration curves for 1, 3 and 5-year overall survival prediction. (A) The consistency test of the 1-year survival rate of the training group (B) The consistency test of the 3-years survival rate of the training group (C) The consistency test of the 5-year survival rate of the training group. (D) The consistency test of the 1-year survival rate of the validation group (E) The consistency test of the 3-years survival rate of the validation group (F) The consistency test of the 5-years survival rate of the validation group

The results of the decision curve analysis (DCA) for nomogram. (A) DCA of 1-year OS using training group. (B) DCA of 3-years OS using training group. (C) DCA of 5-years OS using training group. (D) DCA of 1-year OS using validation group. (E) DCA of 3-years OS using validation group. (F) DCA of 5-years OS using validation group

ROC curve and Kaplan-Meier analysis for evaluating the reliability of the prediction model, and distribution of the risk value and survival status. (A) ROC curve of 1、3 and 5-year survival rate predictions on the training group.(B) Kaplan-Meier analysis of the risk value of the training group.(C) ROC curve of 1、3 and 5-year survival rate predictions on the validation group.(D) Kaplan-Meier analysis of the risk value of the validation group.(E)The distribution of the risk value and survival status of the patients in the training group.(F)The distribution of the risk value and survival status of the patients in the validation group
Nomogram validation
The validation group was used for nomogram validation. The C-index for this group was 0.786, suggesting well discrimination. Calibration curve indicated good concordance between actual prognosis and predicted probabilities (Fig. 5). The DCA curve showed that the use of the nomogram provided more benefits than treatment/non-treatment and TNM stage for predicting the 3- and 5-year OS of all CRC patients (Fig. 6). The area under the ROC for 1-, 3-, and 5-year survival of the training group was 0.774, 0.828, and 0.803, respectively (Fig. 7). The above data suggested that the nomogram was also accurate in the validation group.
Risk group stratification
Patients were then categorized into two subgroups based on the median of riskscore. In both training and validation sets, high-risk subgroups showed significantly worse OS (Fig. 7B, D). Moreover, the actual 5-year survival rate of the high-risk group was also lower than that of the low-risk group (80.7% vs. 60.4%, P = 3.01e-06). The score distribution and the numbers of patients in different subgroups are shown in Fig. 7.
Discussion
Colorectal cancer is one of the most common cancers diagnosed in men and women, which remains a major cause of cancer-related death worldwide. Surgery is the main curative treatment for patients with colorectal cancer [21]. The OS of CRC patients after surgical resection varies significantly [22]. The TNM stage has currently been applied to predict the prognosis of postoperative CRC patients but with insufficient accuracy [23, 24]. Thus, it is necessary to develop a prognostic model for personalized probabilistic predictions. In the present study, a nomogram model for predicting the OS of CRC patients following surgery was constructed and validated.
The raw data of recruited patients were complete and of high quality. Univariate analysis was applied to identify prognostic variables. LASSO regression was used to select clinical features and reduce the likelihood of overfitting [25]. Over-fitting means that the established model performs too well in the training samples, resulting in poor performance in the validation data set and the test data set. Through LASSO regression and multivariate analysis, we distinguished number of positive LN, CEA levels, CA-199 levels, M stage, TNM stage, and macroscopic classification as prognostic factors.
CEA is a potential biomarker for tumor stage and the prognosis of CRC patients. Preoperative serum CEA levels were positively associated with LN invasion, vascular invasion, and perineural invasion [26]. Moreover, Hermunen et al. reported that patients with elevated postoperative CEA levels had worse OS and disease-free survival [27]. Serum CA-199 levels were positively correlated with early recurrence of CRC and negatively associated with the OS for CRC patients [28]. Also, high preoperative serum CA-199 levels could pridict worse 3-year OS and relapse-free survival [29], suggesting that CA-199 is an unfavorable prognostic factor for the survival of CRC patients. The number of positive LN is also considered a key prognostic factor for CRC patients after curative resection [30,31,32]. However, studies have shown that the log of the ratio of numbers of positive and negative LN is a more accurate prognostic indicator than the number of positive LN [33, 34], which therefore would be included in our upcoming studies. Macroscopic classification is another independent risk factor for recurrence of Stage II CRC [35]. Li et al. showed that macroscopic classification was an independent prognostic factor for stage I-III CRC and infiltrative CRC subtype was correlated to poor OS of stage III CRC patients [36]. Collectively, infiltrative CRC subtype is an unfavorable prognostic factor for the survival of CRC patients. The TNM staging system plays a critical role in predicting the prognosis [37]. Consistently, our study showed that TNM stage and M stage and were significantly associated with the OS of CRC patients. However, previous literature indicated that CRC patients with the same M or TNM stage had different OS and TNM stage cannot predict the prognosis of individual patients [23, 24, 38]. Here, M and TNM stage were included in the nomogram, which predicted the prognosis of each patient more accurately. Hence, inclusion of these characteristics into our nomogram was consistent with previous results.
The nomogram was constructed using characteristics selected by multivariate analysis of the training group. C-index, calibration curve, DCA, and ROC analysis were performed to evaluate nomogram performance. Then, CRC patients were categorized into high- and low-risk subgroups. For those in the high-risk subgroup, additional treatments and follow-up care may improve their prognosis. Validation is a key step in nomogram studies, which determines the generalizability of the nomogram [39]. Here, the C-indices suggesting that the nomogram model had good discriminatory capacity. The calibration curves of the training group indicated a favorable agreement between predictions and observations of 3- and 5-year outcomes, but not 1-year survival. The calibration of the validation group also suggested a favorable agreement in 3- and 5-years outcomes. These data proved the reliability and repeatability of this model for 3- and 5-year OS. Furthermore, DCA indicated that the nomogram model provided more benefits than treatment/non-treatment and TNM stage for predicting the 3- or 5-year OS of all CRC patients, indicating decent predictive and discriminatory capacity of this model. However, the prediction of 1-year survival was not accurate enough, probably due to insufficient sample size. Additionally, high-risk subgroups had significantly worse OS, suggesting satisfactory predictive performance of the nomogram.
In addition, many researchers have established nomograms for the prognosis of patients undergoing colon cancer surgery. Shuanhu Wang et al. develop and validate a prognostic nomogram for patients with resectable colon cancer, and indicate that age, race, primary site, grade, T stage, N stage, chemotherapy, and CEA level were independent predictors of OS [11]. Moreover, CEA levels (OR = 1.00, P = 0.001) was also independent predictors of OS in our study. This proves that CEA has an important effect on the prognosis of CRC patients. Y. Kanemitsu et al. develop a nomogram to predict survival of patients radical resection of colon cancer [12]. Predictors of OS were: age, gender, depth of tumour invasion, lymphatic invasion, CEA level, number of metastatic lymph nodes, number of lymph nodes examined and extent of lymphadenectomy. CEA level and number of metastatic lymph nodes were also included in our nomogram. This proves that the above variables are crucial for predicting the prognosis of patients. Chaoran Yu et al. established a nomogram model of overall survival in elderly colorectal cancer (ECRC) patients (Age ≥ 70) based on SEER database, and indicate that sex, gender, marital status, grade, AJCC TNM, metastasis and tumor size was independent predictors of OS [13]. Age and sex were independent predictors of OS in the study of Y. Kanemitsu and Chaoran Yu et al., and were included in the nomogram. And in this study, they were not included in the nomogram. This may be due to the insufficient sample size in our study. However, it is worth noting that these studies have the characteristics of long data set time span and few included variables. This raises the question of whether these nomogram can be applied to current patients. In this study, novel pathological and molecular markers, such as perineuronal infiltration, mismatch repair status, and RAS/RAF mutation status, were incorporated into the data analysis. This will help predict the survival rate of colon cancer patients more accurately.
The limitations of this work included small sample size and single-center design. Also, some prognostic factors could not be included due to the retrospective design. Data from multiple institutions will be used for external validation in future studies.
Conclusion
A nomogram for predicting the OS of CRC patients after surgery was developed and validated, which may help clinicians predict the survival of each CRC patient and identify high-risk patients who may need more aggressive treatments.
Data availability
The datasets generated and analysed during the current study are not publicly available due to the protection of patient privacy but are available from the corresponding author on reasonable request.
References
Baidoun F, Elshiwy K, Elkeraie Y, et al. Colorectal Cancer epidemiology: recent Trends and Impact on Outcomes. Curr Drug Targets. 2021;22(9):998–1009.
Song M. Global epidemiology and prevention of colorectal cancer. Lancet Gastroenterol Hepatol. 2022;7(7):588–90.
Sung H, Ferlay J, Siegel RL, et al. Global Cancer Statistics 2020: GLOBOCAN estimates of incidence and Mortality Worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209–49.
Li N, Lu B, Luo C, et al. Incidence, mortality, survival, risk factor and screening of colorectal cancer: a comparison among China, Europe, and northern America. Cancer Lett. 2021;522:255–68.
Qu R, Ma Y, Zhang Z, Fu W. Increasing burden of colorectal cancer in China. Lancet Gastroenterol Hepatol. 2022;7(8):700.
Glynne-Jones R, Glynne-Jones S. The concept and use of the neoadjuvant rectal score as a composite endpoint in rectal cancer. Lancet Oncol. 2021;22(7):e314–26.
Wang L, Chang N, Wu L, et al. A nomogram-based immunoprofile predicts clinical outcomes for stage II and III human colorectal cancer. Mol Clin Oncol. 2021;15(6):257.
Wu J, Lu L, Chen H, et al. Prognostic nomogram to predict the overall survival of patients with early-onset colorectal cancer: a population-based analysis. Int J Colorectal Dis. 2021;36(9):1981–93.
Liu Z, Lu T, Li J, et al. Clinical significance and Inflammatory Landscape of aNovel Recurrence-Associated Immune signature in Stage II/III Colorectal Cancer. Front Immunol. 2021;12:702594.
Wang X, Lu J, Song Z, Zhou Y, Liu T, Zhang D. From past to future: bibliometric analysis of global research productivity on nomogram (2000–2021). Front Public Health. 2022;10:997713.
Wang S, Liu Y, Shi Y, Guan J, Liu M, Wang W. Development and external validation of a nomogram predicting overall survival after curative resection of colon cancer. J Int Med Res. 2021;49(5):3000605211015023.
Kanemitsu Y, Shida D, Tsukamoto S, et al. Nomograms predicting survival and recurrence in colonic cancer in the era of complete mesocolic excision. BJS Open. 2019;3(4):539–48.
Yu C, Zhang Y. Establishment of prognostic nomogram for elderly colorectal cancer patients: a SEER database analysis. BMC Gastroenterol. 2020;20(1):347.
Wu L, Zhou B, Liu D et al. LASSO Regression-Based Diagnosis of Acute ST-Segment Elevation Myocardial Infarction (STEMI) on Electrocardiogram (ECG). J Clin Med. 2022. 11(18).
Hu P, Liu Y, Li Y, et al. A comparison of LASSO Regression and Tree-Based models for delayed cerebral ischemia in Elderly patients with subarachnoid hemorrhage. Front Neurol. 2022;13:791547.
Harrell FE Jr, Califf RM, Pryor DB, Lee KL, Rosati RA. Evaluating the yield of medical tests. JAMA. 1982;247(18):2543–6.
Pencina MJ, D’Agostino RB. Overall C as a measure of discrimination in survival analysis: model specific population value and confidence interval estimation. Stat Med. 2004;23(13):2109–23.
Kang L, Chen W, Petrick NA, Gallas BD. Comparing two correlated C indices with right-censored survival outcome: a one-shot nonparametric approach. Stat Med. 2015;34(4):685–703.
Vickers AJ, Holland F. Decision curve analysis to evaluate the clinical benefit of prediction models. Spine J. 2021;21(10):1643–8.
Chalkou K, Vickers AJ, Pellegrini F, Manca A, Salanti G. Decision Curve Analysis for Personalized Treatment Choice between Multiple Options. Med Decis Making. 2022: 272989X221143058.
Kuipers EJ, Grady WM, Lieberman D, et al. Colorectal cancer. Nat Rev Dis Primers. 2015;1:15065.
Miller KD, Nogueira L, Mariotto AB, et al. Cancer treatment and survivorship statistics, 2019. CA Cancer J Clin. 2019;69(5):363–85.
Liu J, Huang X, Yang W, et al. Nomogram for predicting overall survival in stage II-III colorectal cancer. Cancer Med. 2020;9(7):2363–71.
Zhang J, Gong Z, Gong Y, Guo W. Development and validation of nomograms for prediction of overall survival and cancer-specific survival of patients with stage IV colorectal cancer. Jpn J Clin Oncol. 2019;49(5):438–46.
Tibshirani R. The lasso method for variable selection in the Cox model. Stat Med. 1997;16(4):385–95.
Gao Y, Wang J, Zhou Y, Sheng S, Qian SY, Huo X. Evaluation of serum CEA, CA19-9, CA72-4, CA125 and ferritin as diagnostic markers and factors of clinical parameters for Colorectal Cancer. Sci Rep. 2018;8(1):2732.
Hermunen K, Soveri LM, Boisen MK, et al. Postoperative serum CA19-9, YKL-40, CRP and IL-6 in combination with CEA as prognostic markers for recurrence and survival in colorectal cancer. Acta Oncol. 2020;59(12):1416–23.
Tang S, Chen Y, Tian S, Wang Y. Predictive nomogram for the prediction of early recurrence of Colorectal Cancer. Int J Gen Med. 2021;14:4857–66.
Ozawa T, Ishihara S, Kawai K, et al. Prognostic significance of preoperative serum Carbohydrate Antigen 19 – 9 in patients with stage IV Colorectal Cancer. Clin Colorectal Cancer. 2016;15(4):e157–63.
Johnson PM, Porter GA, Ricciardi R, Baxter NN. Increasing negative lymph node count is independently associated with improved long-term survival in stage IIIB and IIIC colon cancer. J Clin Oncol. 2006;24(22):3570–5.
Berger AC, Sigurdson ER, LeVoyer T, et al. Colon cancer survival is associated with decreasing ratio of metastatic to examined lymph nodes. J Clin Oncol. 2005;23(34):8706–12.
Lei P, Ruan Y, Liu J, Zhang Q, Tang X, Wu J. Prognostic Impact of the Number of Examined Lymph Nodes in Stage II Colorectal Adenocarcinoma: A Retrospective Study. Gastroenterol Res Pract. 2020. 2020: 8065972.
Persiani R, Cananzi FC, Biondi A, et al. Log odds of positive lymph nodes in colon cancer: a meaningful ratio-based lymph node classification system. World J Surg. 2012;36(3):667–74.
Scarinci A, Di Cesare T, Cavaniglia D, et al. The impact of log odds of positive lymph nodes (LODDS) in colon and rectal cancer patient stratification: a single-center analysis of 323 patients. Updates Surg. 2018;70(1):23–31.
Hashimoto T, Itabashi M, Ogawa S, et al. Sub-classification of stage II colorectal cancer based on clinicopathological risk factors for recurrence. Surg Today. 2014;44(5):902–5.
Li X, Zhao Q, An B, et al. Prognostic and predictive value of the macroscopic growth pattern in patients undergoing curative resection of colorectal cancer: a single-institution retrospective cohort study of 4,080 chinese patients. Cancer Manag Res. 2018;10:1875–87.
Gunderson LL, Jessup JM, Sargent DJ, Greene FL, Stewart AK. Revised TN categorization for colon cancer based on national survival outcomes data. J Clin Oncol. 2010;28(2):264–71.
Li C, Pei Q, Zhu H et al. Survival nomograms for stage III colorectal cancer. Medicine (Baltimore). 2018. 97(49): e13239.
Iasonos A, Schrag D, Raj GV, Panageas KS. How to build and interpret a nomogram for cancer prognosis. J Clin Oncol. 2008;26(8):1364–70.
Acknowledgements
Not available.
Funding
This work was supported by the Hebei Provincial Natural Science Foundation Precision Medicine Joint Project (H2020206485), Youth Science and Technology Project of the Hebei Health Commission (20210453), and Hebei Provincial Department of Science and Technology Key Project (206Z7705G). Study design and registration, and follow-up data collection were supported by all three funding bodies. Data storage and management were supported by the Hebei Provincial Natural Science Foundation Precision Medicine Joint Project. Manuscript publication was supported by the Hebei Provincial Department of Science and Technology Key Project.
Author information
Authors and Affiliations
Contributions
Guo Peiyuan and Hu xuhua wrote the main manuscript text. Wang Guiying, Guo Peiyuan, Guo Ganlin and Yin Xu prepared Figs. 1, 2 and 3. Yu bin, Hu xuhua, Liu Zining and Han Jiachao prepared Figs. 4, 5, 6 and 7. All authors reviewed the manuscript.
Corresponding authors
Ethics declarations
Disclosure of any commercial interest
None of the authors had a commercial conflict or were the source of any financial or material support. All the disclosure forms have been submitted to the editorial department.
Ethical statement and consent to participate
This study was approved by the Ethical Committee of the Fourth Hospital of Hebei Medical University (Approval No. 2020kt417) and performed in following the 1964 Helsinki Declaration. The requirement for informed consent was waived by the Ethics Committee of the Fourth Hospital of Hebei Medical University because of the retrospective nature of the study.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Peiyuan, G., xuhua, H., Ganlin, G. et al. Construction and validation of a nomogram model for predicting the overall survival of colorectal cancer patients. BMC Surg 23, 182 (2023). https://doi.org/10.1186/s12893-023-02018-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12893-023-02018-2