
Abstract
Background
Robotic transanal minimally invasive surgery (R-TAMIS) is an appealing alternative to transanal minimally invasive surgery (TAMIS) and transanal endoscopic microsurgery (TEM) for benign and early malignant rectal lesions that are not amenable to traditional open transanal excision. However, no studies to our knowledge have directly compared the three techniques. This study sought to compare peri-operative and pathologic outcomes of the three approaches.
Methods
The records of 29 consecutive patients who underwent TEM, TAMIS, or R-TAMIS at a single academic center between 2016 and 2020 were reviewed. Intra-operative details, pathological diagnosis and margins, and post-operative outcomes were recorded. The three groups were compared using chi-square and Kruskal–Wallis tests.
Results
Overall, 16/29 patients were women and the median age was 57 (interquartile range (IQR): 28–81). Thirteen patients underwent TEM, six had TAMIS, and 10 had R-TAMIS. BMI was lower in the R-TAMIS patients (24.7; IQR 23.8–28.7), than in TEM (29.3; IQR 19.9–30.2), and TAMIS (30.4; IQR 26.6–32.9) patients. High grade dysplasia and/or invasive cancer was more common in TAMIS (80%) and R-TAMIS (66.7%) patients than in TEM patients (41.7%). The three groups did not differ significantly in tumor type or distance from the anal verge. No R-TAMIS patients had a positive surgical margin compared to 23.1% in the TEM group and 16.7% in the TAMIS group. Length of stay (median 1 day for TEM and R-TAMIS patients, 0 days for TAMIS patients) and 30-day readmission rates (7.7% of TEM, 0% of TAMIS, 10% of R-TAMIS patients) also did not differ among the groups. Median operative time was 110 min for TEM, 105 min for TAMIS, and 76 min for R-TAMIS patients.
Conclusions
R-TAMIS may have several advantages over other advanced techniques for transanal excisions. R-TAMIS tended to be faster and to more often result in negative surgical margins compared to the two other techniques.
Similar content being viewed by others


Background
Transanal local excision is indicated for benign rectal lesions, malignant rectal T1 adenocarcinomas that are moderately and well differentiated, without lymphovascular or perineural invasion, and small neuroendocrine tumors of the rectum [1]. When traditional open transanal excision is not feasible because the lesion is located in the mid to proximal rectum, two other techniques are transanal endoscopic microsurgery (TEM) and laparoscopic transanal minimally invasive surgery (TAMIS). More recently, robotic transanal minimally invasive surgery (R-TAMIS) has become an increasingly appealing alternative. Although the benefits of transabdominal pelvic robotic surgery over laparoscopic surgery are just emerging [2, 3] whether these benefits translate to transanal robotic surgery is unclear. Another advantage of robotic surgery is improved surgeon ergonomics during pelvic and abdominal surgeries [4, 5], but whether this holds for transanal robotic surgery is not well established.
Robotic surgery for transanal excision of rectal lesions is a relatively new approach. In the largest series to date at a single institution, 58 patients underwent R-TAMIS, 55 of whom had negative surgical margins. Of those 55, three patients developed local recurrence at a mean follow-up of 12 months, requiring salvage surgery [6]. The authors concluded that R-TAMIS improved surgeon ergonomics and enabled tumor removal from all quadrants [6]. There is still a lack of studies directly comparing R-TAMIS, TAMIS, and TEM [7]. We sought to address this gap by comparing operative, perioperative, and pathological outcomes of these three distinct approaches at a single tertiary academic institution.
Methods
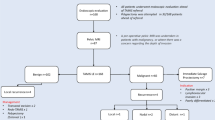
Data from all adult patients (> 21 years old) who underwent advanced transanal excision of a rectal lesion at a single academic center (University of California San Francisco) were retrospectively collected from a database of consecutive patients undergoing colorectal surgery from 2016 to 2020. In our clinical practice, patients were considered for advanced transanal excision if lesions were not amenable to traditional transanal excision and were one of the following: (1) the biopsy of the lesion was benign (adenomatous polyps) with no evidence of deep invasion on MRI, or (2) the biopsy showed rectal adenocarcinoma which, on preoperative magnetic resonance imaging (MRI) or endoscopic ultrasound (EUS) was read as a T1/T2 N0 lesion, or (3) rectal neuroendocrine tumors < 2 cm. [1] For those in whom pre-operative MRI was unable to distinguish between T1 and T2, patients underwent a local excision with the understanding that a T2 lesion on final pathology would require a subsequent radical resection. All lesions had to be within 13 cm of the anal verge. Two colorectal surgeons (CH, AS) performed all the operations. Before May 2018, all patients were offered TEM. From May 2018 to December 2019, patients were offered TAMIS, and from January 2020, all patients were offered R-TAMIS with the Da Vinci Robotic Surgical System Xi (Intuitive Surgical, Inc., Sunnyvale, CA). Thus, no selection criteria were used to determine use of one technique versus another; the surgical approach received was dependent on when the patient presented to our practice. The R-TAMIS procedure started at proctoscopy, followed by the Gelpoint being placed and the robot being docked.
Patients’ electronic medical records were retrospectively reviewed for demographics and clinical diagnosis; intra-operative details such as operative time, lesion location and size; pathological diagnosis, intactness of specimen, and margins; and post-operative complications and outcomes with follow-up time ranging from 3 months to 5 years. The direct cost of each operation was collected from the hospital’s cost accounting management system, linked to the patient’s encounter within the electronic medical record system.
Data are summarized as medians and interquartile ranges (IQR). The three groups were compared using the chi-square test for categorical variables and the Kruskal–Wallis test for continuous variables. Statistical significance was defined as a p ≤ 0.05. Statistical analyses were completed using Stata/IC version 16.1 (StataCorp, LLC, College Station, TX).
A video compilation was created of some of the robotic cases included in this study, to illustrate the key steps of this operation in different types of tumors that can be resected by R-TAMIS. This study was approved by the Institutional Review Board at the University of California, San Francisco (UCSF): Study Number 18-26677.
Results
Patient demographics
A total of 29 patients were included in our review: 13 TEM, 6 TAMIS, 10 R-TAMIS (Table 1). A video compilation of the key steps in four different patients treated with R-TAMIS is presented in Additional file 1. The median cohort age was 57 (IQR 28–81) and there were 16 women. Twenty-two (76%) patients identified as White. There were no significant demographic differences among the three groups. Patients who underwent R-TAMIS tended to have a lower body mass index (BMI) than patients in the other groups. American Society of Anesthesiologist (ASA) classification differed significantly: most TAMIS patients were ASA class 3, whereas most TEM and R-TAMIS patients were ASA Class 2 (p = 0.004). One hundred percent of the TAMIS and R-TAMIS patients underwent pre-operative antibiotic bowel preparation, whereas only 61.5% of TEM patients did so (p = 0.02).
Tumor characteristics
A higher proportion of patients who underwent TAMIS (80%) and R-TAMIS (66.7%) had high grade dysplasia or invasive cancer than those who had TEM (41.7%), though the difference was not statistically significant. Tumor type or distance from the anal verge did not differ significantly among the three procedures (Table 2). Positive surgical margins were seen in 3/13 of the TEM patients, 1/6 of TAMIS and 0/10 of the R-TAMIS patients (Table 3).
Intra-operative details: The median time in the operating room and the median procedure duration was lowest in the R-TAMIS group (Table 3). Forty percent of the TAMIS and R-TAMIS patients were placed in prone position versus 30.8% of the TEM patients (Fig. 1). The direct cost was higher in the R-TAMIS group ($9226, IQR $7835–$10,224) than in the other groups ($6362, IQR $5286–$6721 in TEM, $6428, IQR $5177–$8060 in TAMIS).

Intra-operative photos of transanal rectal excision using R-TAMIS. A Patient positioned prone jackknife. B Set-up of Gelpoint path port, through which the robotic ports are placed, and monitor. C Robotic trocars and airseal insufflator placement through Gelport. D Rectal lesion specimen oriented for pathological evaluation
Post-operative outcomes
Postoperative length of stay did not differ among the groups (Table 3). One patient in the TEM group was readmitted for pain control. One patient in the TAMIS group was readmitted due to a concern for a pelvic abscess, was brought back to the OR, and no abscess was found. In the TEM group, 4/13 patients required further surgery: one patient was found to have a T2 lesion on final pathology and underwent a robotic low anterior resection (LAR), one patient had positive surgical margins and was recommended to follow up to discuss surgical options but was lost to follow up, one patient’s TEM was aborted due to the location and underwent an LAR one month later, and one patient had a recurrence one year later thus was scheduled for an abdominoperineal resection (APR). In the TAMIS group, 4/6 patients required further surgery: two patients were found to have a T2 lesion on final pathology and underwent LAR, one patient developed a rectal stricture requiring exams under anesthesia with dilations, and one patient with HSIL in the setting of ulcerative colitis underwent a total colectomy one year later. In the R-TAMIS group, 1/10 patients was found to have a T2 lesion on final pathology and was scheduled for an LAR.
Discussion
As robotic TAMIS gains traction as a technique for transanal excision of benign and early malignant rectal lesions, a handful of series have described the outcomes [6,7,8,9,10], but none compared R-TAMIS to TAMIS and TEM. Our study directly compared these three groups at a single tertiary academic institution with respect to perioperative and pathological outcomes. The results suggest a tendency for R-TAMIS to be faster, have a higher frequency of negative surgical margins, and lower requirement for further surgery, compared to TEM and laparoscopic TAMIS. We present a video compilation of different R-TAMIS cases to illustrate the benefits of this technique for different types of tumor.
In terms of patient positioning, our experience with R-TAMIS is similar to that of other authors. Case series of patients undergoing R-TAMIS for rectal lesions have described several advantages including better 3D visualization, improved surgeon ergonomics, and the ability to position the patient in a consistent position regardless of the tumor location [11]. This is due to the Da Vinci’s 7 degrees of freedom, which enable the circumferential resection of lesions regardless of patient positioning. Authors of a study of two tertiary referral centers advocated for the lithotomy position (used in 32/34 of their patients) because of the additional time needed to position the patient in a prone or jackknife position [9]. In our study, 40% of patients in all three groups were in the prone position. We found a non-significant tendency for lower operative time in the R-TAMIS group, which leads us to recommend considering jackknife positioning for R-TAMIS. The advantage of using the prone approach is that the legs of the patient do not interfere with the positioning of the robotic arms and there is less risk of positioning or mechanical injury to the legs. Although the robot enables the surgeon to operate in all quadrants, we believe that the operation is faster and more straightforward if the lesion is positioned to be inferior on the screen. Others have expressed theoretical concerns for anesthetic concerns in jackknife positioning especially if the patient is under general anesthesia [7], but this has not been our experience. Moreover, the safety of this positioning for anorectal surgeries of similar duration has been well established. [12].
With R-TAMIS, we could reach tumors at a median 8 cm from the anal verge. Compared to TEM, which is rigid and therefore allows only a limited field of view at one time making excision of large lesions difficult and closure of large defects challenging, the robotic platform allows 360 degrees of view due to its flexible platform. In addition, the robot aids in suturing high in the rectum as it does not ergonomically limit the surgeon at the console even though instrument movement may be somewhat restricted similar to TEM or L-TAMIS. Others have also advocated for the ability to reach very low-lying tumors due to the articulation of the wrist [11] although these lesions may not require any advanced instrumentation. None of our robot excisions required conversion to a different approach, a finding similar to the experience of others [9]. Our median operative time of 76 min and median distance of the tumor from the anal verge (8 cm) were also similar to what others have reported. [6]
In our study, pre-operative antibiotic bowel preparation was significantly more common in the TAMIS and R-TAMIS groups than in the TEM group. This is likely a reflection of how practices have evolved over time. It is encouraging that patients in all three groups received few to no opioids during their hospitalization.
We also found no positive surgical margins in the R-TAMIS group. In other case series of only R-TAMIS patients, negative margin rates have ranged from 0% [11] to 8.7% [8]. In our series, while limited by the small number of patients, there was no significant difference in positive margins between the three groups. In other larger studies of each technique, TEM was associated with up to 17% rate of positive margins [13] and TAMIS with 7% [14]. However, only our study directly compared the three techniques.
The median direct cost of R-TAMIS in our study was higher than that of TEM and TAMIS, although this was not statistically significant (median $9,226 in R-TAMIS group, $6,362 in TEM group, and $6,428 in TAMIS group). Another study that compared the cost of R-TAMIS to TAMIS also found that the median direct cost was unsurprisingly higher in R-TAMIS ($4441 versus $3562) [15]. The median length of stay in all three of our groups was one day, but the significantly lower number of patients requiring further surgery after R-TAMIS due to better margins may offset the higher direct cost of the initial operation. We found no significant differences in 30 day readmissions among the three groups.
The limitations of this study include the small sample size and retrospective design. The primary surgeon had completed 30 prior transanal procedure at another institution prior to this work and the techniques were introduced based on available technology. As such the role of learning curve was minimal. There was no selection bias towards robotic surgery in this study as any patients who met criteria for a transanal excision was offered surgery and the technique offered was based on the available technology at the time. No selection towards one or other technique was made based on patient characteristics. The short follow-up time also limits our knowledge of the long-term oncologic and functional outcomes. The BMI of the R-TAMIS group tended to be lower than in the other groups, which may have contributed to the shorter operative time for that group. Others have found that a higher BMI was associated with longer R-TAMIS times. [9]
Conclusions
Our comparison of R-TAMIS, TAMIS, and TEM at a single tertiary academic institution shows that R-TAMIS may have several advantages over conventional endoscopic and laparoscopic excision of transanal lesions. Larger studies with longer follow-up times are needed to confirm these findings and clarify the role of robotic TAMIS in the care of patients with rectal lesions.
Availability of data and materials
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- ASA:
-
American Society of Anesthesiologist classification
- BMI:
-
Body mass index
- OME:
-
Oral morphine equivalents
- IQR:
-
Interquartile range
- R-TAMIS:
-
Robotic transanal minimally invasive surgery
- TAMIS:
-
Transanal minimally invasive surgery
- TEM:
-
Transanal endoscopic microsurgery
References
Monson JR, Weiser MR, Buie WD, et al. Practice parameters for the management of rectal cancer (revised). Dis Colon Rectum. 2013;56(5):535–50.
Wang Y, Liu Y, Han G, et al. The severity of postoperative complications after robotic versus laparoscopic surgery for rectal cancer: A systematic review, meta-analysis and meta-regression. PLoS ONE. 2020;15(10):e0239909.
Kowalewski KF, Seifert L, Ali S, et al. Functional outcomes after laparoscopic versus robotic-assisted rectal resection: a systematic review and meta-analysis. Surg Endosc. 2021;35(1):81–95.
van der Schatte Olivier RH, Van’t Hullenaar CD, Ruurda JP, et al. Ergonomics, user comfort, and performance in standard and robot-assisted laparoscopic surgery. Surg Endosc. 2009;23(6):1365–71.
Tarr ME, Brancato SJ, Cunkelman JA, et al. Comparison of postural ergonomics between laparoscopic and robotic sacrocolpopexy: a pilot study. J Minim Invasive Gynecol. 2015;22(2):234–8.
Tomassi MJ, Taller J, Yuhan R, et al. Robotic transanal minimally invasive surgery for the excision of rectal neoplasia: clinical experience with 58 consecutive patients. Dis Colon Rectum. 2019;62(3):279–85.
Yao HL, Ngu JC, Lin YK, et al. Robotic transanal minimally invasive surgery for rectal lesions. Surg Innov. 2020;27(2):181–6.
Huang YJ, Huang YM, Wang WL, et al. Surgical outcomes of robotic transanal minimally invasive surgery for selected rectal neoplasms: A single-hospital experience. Asian J Surg. 2020;43(1):290–6.
Liu S, Suzuki T, Murray BW, et al. Robotic transanal minimally invasive surgery (TAMIS) with the newest robotic surgical platform: a multi-institutional North American experience. Surg Endosc. 2019;33(2):543–8.
Baker EJ, Waters PS, Peacock O, et al. Robotic transanal minimally invasive surgery—technical, oncological and patient outcomes from a single institution. Colorectal Dis. 2020;22(10):1422–8.
Lo KW, Blitzer DN, Shoucair S, et al. Robotic transanal minimally invasive surgery: a case series. Surg Endosc. 2021. https://doi.org/10.1007/s00464-020-08257-1.
Cheema F, Lee S, Zebrower M, Poggio J. Safety of prone jackknife position in ambulatory anorectal surgery. World J Colorectal Surg. 2018;7(1):16.
Moore JS, Cataldo PA, Osler T, et al. Transanal endoscopic microsurgery is more effective than traditional transanal excision for resection of rectal masses. Dis Colon Rectum. 2008;51(7):1026–30 (discussion 30-1).
Lee L, Burke JP, deBeche-Adams T, et al. Transanal minimally invasive surgery for local excision of benign and malignant rectal neoplasia: outcomes from 200 consecutive cases with midterm follow up. Ann Surg. 2018;267(5):910–6.
Lee SG, Russ AJ, Casillas MA Jr. Laparoscopic transanal minimally invasive surgery (L-TAMIS) versus robotic TAMIS (R-TAMIS): short-term outcomes and costs of a comparative study. Surg Endosc. 2019;33(6):1981–7.
Acknowledgements
We thank Pamela Derish in the UCSF Department of Surgery for editorial review of the manuscript.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Author information
Authors and Affiliations
Contributions
MES contributed to the design of study, data collection, and manuscript writing. SH contributed to data collection and analysis, and manuscript writing. SW contributed to data collection, video creation, and manuscript revisions. HC contributed to data interpretation and manuscript revisions. MV contributed to data interpretation and manuscript revisions. AS contributed to the conception and design of the study, data collection, and manuscript revisions. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This research was performed in accordance with the Declaration of Helsinki. This study was approved by the Institutional Review Board (IRB) at the University of California, San Francisco (UCSF): Study Number 18-26677. Per our IRB committee, consent (written or oral) was not obtained.
Consent for publication
Not applicable.
Competing interests
MES: spouse is an employee of Intuitive Surgical. None of the other authors have anything to disclose.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1. R-TAMIS video.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Schwab, M.E., Hernandez, S., Watanaskul, S. et al. Comparison of advanced techniques for local excision of rectal lesions: a case series. BMC Surg 22, 117 (2022). https://doi.org/10.1186/s12893-022-01543-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12893-022-01543-w