
Abstract
Taping is increasingly used to manage proprioceptive deficits, but existing reviews on its impact have shortcomings. To accurately assess the effects of taping, a separate meta-analyses for different population groups and tape types is needed. Therefore, both between- and within-group meta-analyses are needed to evaluate the influence of taping on proprioception. According to PRISMA guidelines, a literature search was conducted across seven databases (Web of Science, PEDro, Pubmed, EBSCO, Scopus, ERIC, SportDiscus, Psychinfo) and one register (CENTRAL) using the keywords “tape” and “proprioception”. Out of 1372 records, 91 studies, involving 2718 individuals, met the inclusion criteria outlined in the systematic review. The meta-analyses revealed a significant between and within-group reduction in repositioning errors with taping compared to no tape (Hedge’s g: -0.39, p < 0.001) and placebo taping (Hedge’s g: -1.20, p < 0.001). Subgroup and sensitivity analyses further confirmed the reliability of the overall between and within-group analyses. The between-group results further demonstrated that both elastic tape and rigid tape had similar efficacy to improve repositioning errors in both healthy and fatigued populations. Additional analyses on the threshold to detection of passive motion and active movement extent discrimination apparatus revealed no significant influence of taping. In conclusion, the findings highlight the potential of taping to enhance joint repositioning accuracy compared to no tape or placebo taping. Further research needs to uncover underlying mechanisms and refine the application of taping for diverse populations with proprioceptive deficits.
Similar content being viewed by others


Introduction
Over the past decade, taping has become a focal point in rehabilitation and performance science [1]. The increased application of this intervention is partly fueled by its enhanced viability [2], ease of application [3], availability [4], cost-effectiveness [5, 6], and sometimes just a fashion statement [7, 8]. Owing to these factors, the application of taping in the existing literature extends endlessly across different medical conditions [9,10,11,12,13,14,15,16], and sports [17,18,19].
The literature has proposed several mechanisms to explain the effects of taping [14, 20,21,22,23,24]. However, enhancing joint proprioception is one of the significant mechanisms of taping that is considered to facilitate recovery and performance [25, 26]. Proprioception refers to an individual's ability to integrate sensory input from mechanoreceptors within musculoskeletal structures to determine the position of a body segment in space [27]. Deficiencies in proprioception are known to negatively affect joint biomechanics and neuromuscular control, increasing the risks of injury [28,29,30]. Therefore, stimulating proprioception during training is crucial for rehabilitation, as its enhancement could not only promote coordinated movements, joint stability, and control, but also reduce the likelihood of injuries [31,32,33]. In the context of taping, research has indicated that the tactile stimulation from taping can activate mechanoreceptors that eventually augment the afferent input via the central pathways to augment proprioception [34,35,36]. Eventually, this increased afferent input is thought to further facilitate the efferent neuromuscular response, which increases both the speed and the quality of the muscle reaction [37,38,39]. Y Konishi [34] suggested that injury-induced damage to musculoskeletal structures could impair proprioception by deteriorating mechanoreceptors' ability to provide regular afferent feedback, crucial for modulating motor units. Under these conditions, tactile stimulation via taping might rescue alpha motor activity [34], while a "skin stretch" effect from taping could enhance proprioception by altering musculoskeletal kinetics [40,41,42,43]. Taping has demonstrated benefits in improving proprioception and preventing injuries by enhancing joint position sense and resisting harmful movements [44,45,46]. Additionally, taping may boost motor performance by enhancing neural activity, as shown in neuroimaging studies indicating increased activation in brain areas related to coordination and sensation [14, 47, 48].
Despite this mounting evidence suggesting the beneficial influence of taping on joint proprioception and its gaining popularity, a lack of consensus exists in the literature regarding its efficacy. For instance, while some individual trials have suggested the beneficial influence of taping on proprioception [49,50,51,52,53,54,55,56], others have suggested no effect [57,58,59,60,61,62,63], or even a detrimental effect [64,65,66,67,68]. Similarly, reviews [23, 63, 69, 70], and meta-analyses [71, 72], have reported inconclusive evidence regarding the overall efficacy of taping on joint proprioception. Within the meta-analyses, while one has reported no effect of taping on proprioception in people with a recurrent ankle sprain [71], the other reported a beneficial influence of taping on ankle repositioning in the same population group [72]. Likewise, the four systematic reviews also stated an inconclusive impact of tape on proprioceptive performance [23, 63, 69, 70].
Besides the mixed findings, several limitations of the existent meta-analyses warrant an improved systematic review and meta-analysis [73]. The existing reviews are limited from both analytical and methodological points of view on several accounts. First, these reviews do not include several existing high-quality trials [48,49,50,51,52, 57, 64, 74,75,76,77,78,79,80,81,82,83]. This lack of sufficient data could diminish the power of these meta-analyses and increase the probability that the observed results occurred due to a type II error. Second, none of these reviews conducted both between- and within-group meta-analyses. These findings could be significant because the between-group analyses can explain the differential outcome of taping compared to no-tape/placebo tape. In contrast, the within-group analyses could explain the magnitude of change in proprioceptive parameters before and after the taping. Findings on both, between- and within-group effects are needed to deduce appropriate training dosages or perform comparative evaluations with existing interventions in their training regimens. Third, it was observed that none of the existing meta-analyses analyzed the results differently among randomized controlled and controlled clinical trials. Such a differential analysis would allow for the classification of studies in a meta-analysis according to their inherent level of bias. Fourth, no review has differentiated the outcomes of taping according to an individual's health status. The two meta-analyses published to date have only evaluated the influence of taping on individuals with ankle instability [71, 72]. Even though trials have reported the impact of taping among healthy individuals and individuals with stroke [77, 84], osteoarthritis [85, 86], anterior cruciate ligament injury/reconstruction [78, 87, 88], no review has attempted to differentially synthesize the efficacy of taping according to the health status of an individual. Evaluating this outcome is important to quantify the effectiveness of taping in different health conditions and could be helpful for both clinicians and patient population groups. Finally, no review has yet examined how the elasticity of tapes, including elastic and rigid tape, influences joint proprioceptive performance [89, 90]. Elastic tapes, such as Kinesio and dynamic tape, are known to enhance proprioception due to their high stretch capabilities, allowing them to move and stretch with the body's natural movements and provide constant feedback to sensory receptors in the skin and underlying tissues [91]. In contrast, rigid tapes like athletic and Leuko tape prioritize support and stability over range of motion (47). A comparative assessment of elastic and rigid tapes could offer useful insights for clinicians, patients, and tape manufacturers on how tensile strength affects proprioceptive performance.
Research aims and questions
In this systematic review and meta-analysis, a between-group analysis (i.e., taping vs placebo/no tape) and a within-group (i.e., pre-vs post-test) was conducted to determine the influence taping has on proprioception in healthy and patient population groups. The goal of the study is to allow clinicians to understand tape's overall impact while simultaneously allowing them to compare its efficacy with existing interventions. The main aims of this study are:
-
1.
To evaluate the effect of taping on repositioning accuracy from between- and within-group analyses.
-
2.
To evaluate the effect of taping on the threshold to detect passive movement from both between- and within-group analyses.
-
3.
To evaluate the effect of taping on active movement extent discrimination accuracy from between- and within-group analyses.
-
4.
To perform subgroup meta-analyses between individual studies according to the elasticity of tape (i.e., elastic, rigid tape), health status (i.e., healthy, patient population groups), and study design (i.e., randomized and non-randomized trials).
Material and methods
The PRISMA-SR 2020 guidelines were followed to conduct this systematic review and meta-analysis. The checklist is presented in Table S1. This systematic review was pre-registered at the PROSPERO (CRD42022344452).
Sources of data and search strategy
The systematic literature search was performed across seven databases (Web of Science, PEDro, Pubmed, EBSCO, Scopus, ERIC, SportDiscus, Psychinfo) and one register (Cochrane Central Register of Controlled Trials) for the publication period from January 1970 until August 2023. These databases were chosen on the basis of access provided by the academic organization. The authors also conducted an extra search of the reference section of the included studies.
The review's criteria for study inclusion were established following the PICOS approach (Population, Intervention, Comparator, Outcome of Interest, Study Design). Two researchers (S.G, I.G) determined the inclusion criteria, which were as follows:
-
1.
Healthy population groups.
-
2.
Population groups with musculoskeletal disorders (e.g., sprains, strains, tendinitis, repetitive stress injuries, degenerative joint diseases, traumatic injuries).
-
3.
Population groups with neurological disorders (e.g., stroke, Parkinson's disease, cerebral palsy, multiple sclerosis, traumatic brain injury, degenerative neurological disorders).
-
4.
Studies assessing the impact of taping on joint proprioception.
-
5.
Proprioception acuity evaluated through joint repositioning tests, threshold to detect passive motion (TTDPM), active movement extent discrimination apparatus (AMEDA) (for detailed test explanations, refer to [27]).
-
6.
Studies comparing taping intervention outcomes with no taping or placebo tape.
-
7.
All types of quantitative clinical studies, including randomized controlled trials, controlled clinical trials, crossover trials, cross-sectional studies, cohort studies, and feasibility studies.
-
8.
Studies published in peer-reviewed academic journals, theses, and conference proceedings.
-
9.
Studies published in English, French, German, or Hindi.
Two authors independently screened the titles, abstracts, and full texts of the articles. In instances of disagreement regarding the selection of pertinent studies, the two authors engaged in discussions. The subsequent data were extracted from the articles: author names, country of research, participant details (age, sample size, gender distribution, health status), evaluated joint, taping method, taping technique, taping applicator, assessment durations, taping frequency, and outcomes.
Assessment of the methodological quality
The quality of the studies included in the review was assessed using the PEDro quality appraisal scale [92]. The interpretation of PEDro scale scores is as follows: studies scoring between 9 to 11 are considered "excellent quality," 6 to 8 are deemed "good quality," 4 to 5 are classified as "fair quality," and scores less than or equal to 3 are labeled "poor quality" [93]. Two researchers (SG, IG) independently conducted the appraisal of the studies.
Data analysis
In the present review, a between-group (taping vs. no taping comparator and taping vs. placebo comparator) and a within-group (pre- vs. post-taping) random effect meta-analysis was conducted with Comprehensive meta-analysis (V 4.0) [94]. The data for the meta-analysis was separately distributed and analyzed for each proprioceptive outcome (i.e., re-positioning accuracy, the threshold to detect motion passively, active movement extent discrimination accuracy). Furthermore, subgroup analyses were conducted based on study design (i.e., randomized controlled trial, controlled clinical trial), type of taping (i.e., elastic, rigid tape), and health status (i.e., healthy, musculoskeletal injury, neurological injury), and health status receiving different types of tape (elastic/rigid). The reported outcomes of the meta-analysis included weighted and adjusted effect size (i.e., Hedge’s g), 95% C.I., and significance level. The threshold for the interpretation of effect size is as follows: > 0.16 to < 0.38 is considered a small effect, ≥ 0.38 to < 0.76 as a medium effect, and ≥ 0.76 as a large effect [95]. Forest plots were generated to illustrate the overall results.
Besides, the presence of heterogeneity was assessed using I2 statistics. The threshold for interpreting the heterogeneity with I2 statistics is as follows: between 0 to 25% considered negligible heterogeneity, 25% to 75% as moderate heterogeneity, and > 75% as substantial heterogeneity [96]. Additionally, “leave-one-out” sensitivity analyses were conducted to test the robustness of the findings. The method systematically removes each study from the meta-analysis and re-analyzes the data to assess the influence of individual studies on the overall results. This helps to identify studies that may be driving the results and assess the robustness of the findings [97]. Additionally, an assessment of publication bias was carried out according to the trim and fill procedure by Duval and Tweedie [98]. The alpha level for the study was set at 5%.
Results
Characteristics of included studies
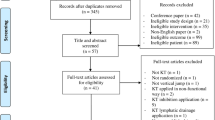
The initial search across the seven databases and one registry yielded a total of 1372 articles, which after implementing the PICOS inclusion criteria, were reduced to 73 articles. Furthermore, during the examination of the citations within these included articles, 98 relevant articles were encountered. These additional articles underwent another round of screening, ultimately resulting in the inclusion of another 18, in total 91 articles. A PRISMA flow chart illustrates the entire selection process in Fig. 1 [99]. Thereafter, qualitative data were extracted from all included studies.

PRISMA flowchart (developed from an R package and Shiny application from [99])
Study design
Of the 91 included studies (Table S 2), 35 were randomized controlled trials [54, 55, 57, 60, 62, 67, 74,75,76,77,78, 80, 82, 83, 85, 100,101,102,103,104,105,106,107,108,109,110,111,112,113,114,115,116,117,118,119], 29 were randomized cross over design [48, 51, 52, 56, 59, 61, 66, 81, 84, 90, 120,121,122,123,124,125,126,127,128,129,130,131,132,133,134,135,136,137,138], 12 were pre-test post-test quasi experimental design [53, 64, 139,140,141,142,143,144,145,146,147,148], 10 were crossover trials [36, 39, 50, 58, 68, 88, 149,150,151,152], two were non-randomized controlled design [65, 153], one was a cross-sectional design [154], and one was a retrospective cohort study [87]. Additionally, one study presented data from two different studies in which one was a pre-test post-test quasi experimental design and a randomized controlled design [86].
Risk of bias
The individual PEDro scoring for each included study has been tabulated in Table 1. The average PEDro quality score of the 91 included studies was (5.2 ± 1.6), suggesting the overall quality of the included studies to be “fair”. Individually, 3% of studies scored 9, 5% scored 8, 10% scored 7, 26% scored 6, 22% scored 5, 18% scored 4, 11% scored 3, and 4% scored 2. As mentioned before, one study presented data from two different study in which one was a pre-test post-test quasi experimental design and a randomized controlled design [86]. The risk for bias for this study was appraised as 3 for the pre-test post-test quasi experimental design, and 8 for the randomized controlled design. The risk of bias scoring across the studies has also been illustrated in Fig. 2.

Illustrating the presence/absence of risk of bias according to the PEDro scale
Publication bias
The incidence of publication bias according to Duval and Tweedie’s trim and fill procedure for the primary outcome of absolute error during joint position sense has been demonstrated in Fig. 3. The method identified five missing studies on the left side of the mean effect, whereas no study was missing on the right side. In the analysis, under the random effect model, the point estimate and the 95% C.I. for the combined studies was -0.39 (-0.54 to -0.24). Using the trim and fill procedure, the imputed point estimates were -0.48 (-0.64 to -0.32).

A trim and fill funnel plot illustrating the publication bias. Each study is represented by an individual blue circle, whereas a unique red circle represents the imputed studies. The funnel plot area covers 95% of the pseudo-confidence intervals. The vertical midline represents the estimated overall effect size (i.e., empirical studies + imputed studies)
Systematic review report
Participants
From the 91 included studies, data from a total of 2718 (1043F, 1123M) people was reported. Fourteen of the included studies did not report the sex distribution of their sample [36, 50, 55, 62, 66, 76, 82, 102, 110, 118, 119, 134, 147, 154]. Likewise, seven studies did not report the age description [50, 52, 60, 65, 114, 142, 154]. In the rest of the 91 studies, the average of the sample was 29.7 ± 12.8 years.
In the entire study sample of 2718 individuals, 2166 (812F, 938M) individuals had received the taping. The discrepancy in the sex distribution is because 14 studies, as mentioned before, had failed to report sex distribution in their respective studies. The average age of the sample receiving taping was 29.4 ± 13 years. Additionally, 13 studies compared the taping intervention's efficacy with a placebo taping [57, 75,76,77, 85, 100,101,102,103, 105, 111,112,113, 116, 118]. Here, data were reported for a total of 279 (115F, 100M) individuals. The discrepancy in the sex distribution was again because three studies did not mention the sex distribution of their participants [76, 102, 118]. The average age in this sample was 35.7 ± 16.6 years. Likewise, 17 studies performed a comparative evaluation by comparing the effectiveness of taping in a group that was subjected to no intervention [54, 55, 60, 67, 74, 78, 82, 101, 104,105,106,107, 110, 114, 115, 117, 134]. Here, data were reported from a total of 273 (116F, 85M) individuals. Five studies had not reported their sex distribution [55, 60, 82, 110, 134], and two studies had not reported the age descriptive of the group that did not receive taping [60, 114]. The average age in this sample was 26.1 ± 3.7 years.
Health status
Table 2 shows a detailed description of the health status of the participants included in this review.
Type of tape
Fourteen different types of tapes were utilized in the included studies (Table S2). The tapes were classified as either rigid or elastic tapes based on the description provided in the respective studies. Overall, sixty studies had utilized elastic tapes [48, 50,51,52,53,54, 56,57,58, 65,66,67, 74,75,76,77,78,79, 81, 82, 84, 85, 87, 88, 90, 100,101,102, 105,106,107,108, 111, 113, 114, 116,117,118, 120, 123, 124, 126, 129,130,131,132, 137,138,139,140,141,142,143,144,145,146,147, 153, 154], and 33 studies had used rigid tapes [36, 39, 55, 59,60,61,62, 64, 80, 83, 86, 103, 104, 110, 115, 119, 122, 125, 127, 128, 133,134,135,136, 148,149,150,151,152]. Additionally, four studies had compared the efficacy across two different tapes. Here, two studies had compared the efficacy between elastic and rigid tapes [90, 109], whereas one study each had evaluated the efficacy between two different types of elastic [56], and rigid tapes [68].
Proprioceptive assessment
Seven different types of proprioceptive assessments were used in the included studies to evaluate proprioceptive performance. Here, 71 of the included studies had used joint sense tests [36, 39, 48, 50, 54,55,56,57,58,59,60,61, 65,66,67,68, 74,75,76,77,78, 81,82,83,84,85,86,87,88, 100,101,102,103,104,105,106,107, 109, 110, 112,113,114,115,116, 118, 119, 122, 124,125,126, 128, 129, 131, 132, 134, 136,137,138,139,140, 142,143,144,145,146,147,148,149,150, 152, 153], four studies had used threshold to detect of passive motion test [62, 111, 127, 133], four had used active movement extent discrimination accuracy test [51, 52, 80, 90], one had used proprioceptive feedback index (i.e., derived from repositioning error and the correlation between instant movement and prototype instant movement) [130], one study had used active displacement test [154], one study had added proprioceptive test accuracy scores (i.e., moving target program on an isokinetic dynamometer) [120], one had used proprioceptive index (i.e., x, y, rotation values) [141], and one had evaluated the percentage of exact joint position sense trial [123]. Additionally, seven studies had performed assessment of joint position sense as well as threshold to detection of passive motion [53, 64, 79, 108, 117, 135, 151].
Outcome
The outcomes of individual studies, categorized by the type of proprioceptive assessment used, are summarized as follows:
-
1.
Joint position sense: Among the 78 studies assessing the impact of taping on joint position sense 47 reported a significant improvement in repositioning accuracy [36, 39, 48, 50, 53, 54, 56, 64, 75,76,77,78,79, 83,84,85, 87, 88, 102, 103, 106,107,108, 110, 112,113,114,115,116, 119, 124, 132, 134,135,136, 139, 140, 143, 144, 146,147,148, 150, 151, 153], 27 reported no difference [55, 57, 59,60,61, 65, 67, 81, 82, 86, 100, 101, 104, 105, 109, 117, 118, 122, 125, 126, 128, 129, 131, 137, 138, 142, 145, 149, 152], and four reported a significant decline in repositioning accuracy with taping [58, 66, 68, 74].
-
2.
Threshold to detection of passive motion: In the 11 studies examining the effect of taping on the threshold to detection of passive motion, two studies observed a significant improvement [64, 117], one study reported significant deterioration [133], while eight studies found no significant impact of taping [53, 61, 62, 108, 111, 121, 127, 151].
-
3.
Active movement extent discrimination apparatus: Three studies indicated a significant improvement in active movement extent discrimination [51, 52, 80], while one study found no difference in discrimination capabilities with taping [90].
-
4.
Active displacement test: One study assessing the influence of taping on active displacement outcomes reported a significant improvement in displacement capabilities with taping [154].
-
5.
Percentage of exact joint position sense trials: In one study, no significant effect of taping on the ability to perform exact joint repositioning trials was reported [123].
-
6.
Proprioceptive feedback index: A study evaluating the impact of taping on the proprioceptive feedback index reported a significant improvement with taping.
-
7.
Proprioceptive index: One study assessing the influence of taping on the proprioceptive index reported a significant improvement with taping [141].
-
8.
Proprioceptive test accuracy: One study reported no significant effect of taping on proprioceptive test accuracy trials [120].
Meta-analysis report
Table 3 provides comprehensive insights into the meta-analysis results for absolute repositioning error, threshold to detection of passive motion, and discrimination of active movement extent apparatus. It offers a thorough examination of the between-group analysis comparing taping, placebo, and no comparators. Similarly, Table 4 illustrates the outcomes of the meta-analysis within each group.

Forest plot illustrating the between group effect of taping on repositioning error. Black boxes: individual weighted effect sizes (Hedge's g), whiskers: 95% confidence intervals, red diamond: pooled weighted effect size and 95% CI, positive effect size: reduced repositioning error for the placebo/no-taping group, negative effect size: reduced repositioning error for the taping group
Sensitivity analysis
A summary of the leave-one-out sensitivity analysis has been provided in Table 5. Specifically, studies were reported if the overall analysis yielded a p-value less than 0.05, and the removal of a specific study increased the p-value above this threshold. Conversely, studies were also reported if the overall analysis yielded a p-value greater than 0.05 and the removal of any particular study decreased the p-value below this threshold.
Discussion
This systematic review and meta-analysis aimed to synthesize the current state of knowledge regarding the influence of taping on joint proprioception in healthy and patient population groups. The findings from the review suggest a positive influence of taping on improving joint repositioning accuracy against both placebo and no comparator groups.
To date, only two meta-analyses have quantified the influence of taping on proprioceptive accuracy [71, 72]. In the initial review, five studies reported medium effect enhancements (Hedge’s g: 0.25) in proprioceptive accuracy among individuals with ankle instability [72]. In an additional analysis with two studies, the authors reported trivial deterioration (g: -0.10) in knee proprioception among individuals with patellofemoral pain syndrome. In the second review, the authors included a total of seven studies and reported a positive influence of taping/bracing on joint position sense (0.20º) but not the threshold to movement detection (-0.24º) [71]. However, it is essential to note that the authors merged the outcomes of studies and did not differentiate the results between taping and bracing. This merged reporting of effects could be an essential factor that biases the understanding concerning the overall influence of taping on joint proprioception. The present study, through a review of 91 studies, represents a significant advancement over previous reviews. Firstly, unlike prior studies that merged various joint stabilizers, such as taping and bracing [71], the present study focused solely on taping, allowing for a more precise evaluation of taping’s efficacy. Secondly, deliberate analyses based on the type of assessment ensured distinct between-group and within-group comparisons, a modification absent in prior research. Thirdly, the review extended beyond previous studies by systematically differentiating outcomes according to study design i.e., distinguishing between randomized and non-randomized designs. Fourth, the study explored nuanced variations in taping outcomes across different health statuses, providing valuable insights for clinicians and patients. Fifth, the evaluation of tape elasticity, encompassing both elastic and rigid varieties, sheds light on how different tape properties influence joint proprioception. Overall, these additions enrich the existing literature and expand understanding concerning the taping's impact on proprioception.
In line with the previous findings, a medium-to-large effect improvement in joint repositioning accuracy was observed with taping in the between group analyses against no comparator (Hedge’s g: -0.39), placebo comparator (g: -1.20) and in the within-group (-0.65) analyses. While the magnitude of improvement for the joint position sense tests was larger for the placebo group compared to the no taping group, it's crucial to note that both of these improvements were statistically significant (p < 0.05). This suggests that regardless of the intervention (placebo or no taping), there was a substantial enhancement in repositioning accuracy. Moreover, the analysis revealed a notable difference in the number of studies included, with 48 studies in the no taping analysis compared to 25 studies in the placebo analysis. This variance in the number of studies might have influenced the observed difference in magnitude [155]. For instance, a larger pool of studies in the no taping analysis could potentially dilute the effect size, whereas a smaller number of studies in the placebo analysis might result in a more pronounced effect size. Therefore, despite the varying magnitudes of improvement, the consistent statistical significance across both groups underscores the importance of the observed enhancement in joint position sense accuracy. These effects were also visible in subsequent subgroup analyses, where the outcomes between RCTs and non-RCTs were differentially analyzed. Moreover, the robustness of these findings was confirmed through leave-one-out sensitivity analyses (see Table 5). This approach involved systematically removing individual data points from each study and rerunning the analysis to evaluate the consistency and stability of the results. By iteratively testing the impact of each data point on the overall outcome, leave-one-out sensitivity analysis provided valuable insights into the reliability of the statistical conclusions. Specifically, it allowed us to determine whether the findings were dependent on specific data points or if they held true across the entire dataset. The consistent patterns observed across multiple iterations of the analysis therefore indicated the robustness of the results. Furthermore, when it comes to the threshold to detect passive motion, no significant effect of taping (-0.02) was observed as compared to no comparator, but a significant effect was observed as compared to placebo comparator (-1.35). During the within-group analysis, a medium effect (-0.36) improvement was observed in the threshold to perceive passive motion. The change in the threshold to detect passive motion is a crucial measure in assessing proprioception because the test evaluates the ability to perceive passive motion, incorporating passive proprioceptive signals which may differ from consciously perceived tests of proprioception. This assessment is particularly valuable in cases of ACL-deficient knees [156], or individuals with rotator cuff tears [157], as it can identify subtle proprioceptive alterations commonly observed in such conditions. Moreover, the sensitivity and precision of the threshold to detect passive motion provide insights into prognostic outcomes and guide treatment planning. For instance, individuals with higher threshold values may exhibit greater functional impairment, signaling the need for more targeted interventions to improve proprioception and enhance joint stability. Furthermore, a between-group analysis was conducted to evaluate the influence of taping on active movement extent discrimination apparatus. However, no significant influence of taping was observed. This lack of effect on the ability to actively discriminate movements could perhaps be as a result of the high level of ecological validity demonstrated by the active movement extent discrimination apparatus [158]. The test reportedly assesses proprioception functions in conditions more analogous to natural settings [27]. Likewise, its ability to provide accurate and meaningful metrics, rooted in signal detection theory [159], is important as by analyzing response data amidst uncertainty using receiver operating characteristic analysis, the test offers a robust assessment of proprioception. This could potentially explain why modifications in joint position sense and threshold to detection of passive motion were observed, while none were noted in the active movement discrimination test. However, it's worth considering the impact of the number of studies included in the analysis. For instance, in the meta-analysis comparing joint position sense against no comparator, 48 studies were evaluated. In contrast, for threshold to detection of passive motion, eight studies were assessed, and for active movement discrimination apparatus, only two studies were evaluated. The lack of modification observed in active movement discrimination apparatus could be attributed to its reliability in assessing proprioception. However, it's also plausible that the limited number of studies prevented an effect from being observed, potentially due to a type II error [160].
Influence of taping on healthy and patient population groups
In line with the existing studies where the use of taping has been emphasized to manage deficit joint proprioception [50, 76,77,78], significant medium-to-large effect increments for the outcomes of repositioning accuracy with taping were found for healthy population groups (no comparator: -0.29, placebo comparator: -0.61). The increments in repositioning accuracy were also found in population groups with anterior cruciate ligament rupture (no comparator: -0.66), and in individuals with osteoarthritis (placebo comparator: -2.21). These improvements were however, not confirmed in the within-group analyses where non-significant improvement in repositioning accuracy was evident in healthy population groups (g: -0.55, p = 0.10). These findings contrast with existing literature suggesting that augmentation of proprioceptive afferent by taping is more beneficial for individuals with poorer inherent proprioception than individuals with good proprioception [161]. The reason behind being that taping augmented proprioceptive afferent information might overload the “inherently good” proprioceptive pathways in healthy individuals. In contrast, individuals with poorer proprioception (i.e., injuries) might benefit from augmented afferent information [126, 162]. Although this theory is widely supported [61, 126, 163], two reasons might explain this differential result in the meta-analysis. First, there was a large difference in the number of studies in the subgroup analysis that evaluated effects of taping on different population groups. For instance, in the within-group analysis, the influence of taping was evaluated on healthy individuals among 15 studies, whereas in the between group analysis with no taping comparator there were 32 studies that had evaluated the effect of taping on healthy individuals. Moreover, in the within group analysis only four, three, and two studies evaluated taping’s impact on ankle instability, stroke, and anterior cruciate ligament reconstruction, respectively. The difference between the number of studies incorporating healthy and patient population group was also evident in between-group meta-analyses (i.e., in no comparator analyses healthy: 32 studies, functional ankle instability: three, patellofemoral pain syndrome: two). Second, in the analyses of healthy population groups, separate sub-group analyses to evaluate the differential influence on individuals with excellent and poor inherent proprioception were not conducted. This analysis was not performed because only a few of the included studies had reported their data differentially according to the intrinsic proprioceptive capabilities of their sample [61, 126]. Future studies are strongly recommended to classify the proprioceptive level of their population groups, as it will help in understanding the actual influence of taping on proprioceptive accuracy among healthy individuals.
Influence of elastic and rigid tapes on proprioception
Various tapes had been used in the existing literature to influence proprioceptive outcomes in healthy and patient population groups (Table S2). However, seldomly some studies have directly compared the influence of different types of tapes on proprioceptive results [49, 56, 90]. In the meta-analyses different tapes were characterized as elastic or rigid tapes based on the description provided in the studies. All the between-group analysis revealed that both the elastic tape (no comparator: -0.40, placebo comparator: -1.13), and rigid tape (no comparator: -0.37, placebo comparator: -1.67) led to a significant improvement repositioning accuracy. The improvement in repositioning accuracy with elastic tape makes sense because previously published literature has demonstrated that tapes with low elastic modulus can support and stabilize the joints without restricting their range of motion [164,165,166]. Besides, owing to their better elasticity, tapes such as Kinesio tape have been reported to exert a pulling force on the skin, facilitating mechanoreceptors' stimulation [142]. Similarly, enhanced elasticity in the tape has been shown to provide better comfort as it aligns well with the contour of the body, and this could have led to an enhancement in proprioceptive performance [90]. With regards to the rigid tape, the higher elasticity modulus of such tapes could restrict the range of motion at a joint, thereby immobilizing its activity during the injury phase to facilitate healing [167, 168]. However, it's important to note that in some instances documented in the literature, certain rigid tapes have been reported to lose their elasticity rapidly, leading to inadequate restraint of joint motion [169,170,171].
The analysis did not report differences in the magnitude of effect between rigid (-0.70) and elastic (-0.63) tape during the within-group analyses as well. However, when evaluating the efficacy of these tapes in detecting passive motion thresholds, larger magnitude of improvements was noted in the threshold perception with the elastic tape (-0.26) as compared to the rigid tape (0.04). This difference in efficacy might stem from the restrictive nature of the rigid tapes, which while limiting ankle motion could affect joint forces higher up the kinetic chain, particularly in the knee joint [172]. Furthermore, subgroup analyses were conducted to evaluate the differential influence of elastic and rigid taping on proprioceptive outcomes in both healthy and injured population groups. Significant enhancement in joint proprioception was observed with both types of tape among in healthy individuals, with similar magnitudes of improvement noted for elastic (-0.30) and rigid tape (-0.29). However, among fatigued healthy individuals, although not statistically significant, there was a "medium" effect size improvement in repositioning accuracy with rigid tape (-0.72), contrasting with a "small" effect size improvement seen with elastic tape (-0.08). This difference in magnitude could be likely attributed to the fact that when a muscle or joint is fatigued, it becomes more susceptible to injury [173], and rigid tape can help to prevent this by limiting the range of motion and providing additional support. Likewise, rigid taping could have also restrained motion at the injured ligamentous tissue to its anatomical limits, and could have attenuated fatigue-induced instability, often associated with deficits in neuromuscular control, by improving the altered flow of afferent input to the central nervous system [38, 55, 174].
Limitations
Despite the novelty of the present meta-analysis, the study has a few limitations. The principal objective of this study was to elucidate the influence of taping on joint repositioning accuracy, the threshold to detection of passive motive, and active movement extent discrimination accuracy. However, upon further assessment of the studies, it was observed that while some of the included studies had evaluated the direct influence of taping [76, 120, 140, 153], others had assessed the influence of the prolonged application of taping on the outcomes of joint proprioception [75, 78, 87, 103, 119, 134]. As it was not the initial goal to evaluate how prolonged taping could influence joint proprioception, separate subgroup analyses to compare the effect of prolonged taping on proprioception were not conducted. Existing studies have suggested that prolonged taping could have a larger impact on movement kinematics and kinetics than immediately after taping [103, 119, 175]. Therefore, future studies are strongly recommended to evaluate the differential influence of the prolonged application of taping on joint proprioception. Secondly, the majority of the studies included in the analysis did not blind assessors, therapists, and subjects, as determined by the PEDro scale used to assess methodological quality. This lack of blinding could have significantly impacted the results, and even though subgroup analyses were conducted to account for the differences between studies with blinding and randomization versus those without, readers are urged to interpret the findings with caution. Thirdly, substantial heterogeneity was also prominent regarding the different taping application methods. For instance, some studies included in the review adhered to a specific taping technique, such as Kenzo Kase’s technique [50, 78, 85], and basket-weave technique [36, 134, 148], whereas the majority had applied taping without following any standardized approach [39, 59, 61, 76, 77, 110]. This heterogeneous approach to using tape complicates understanding of taping’s influence on joint proprioception. Future studies are recommended to adhere to standardized taping applications as they can help develop practical, evidence-based guidelines. Another major limitation of the study was that fewer studies were included in certain meta-analyses, such as between-group analyses of stroke population, individuals with ankle sprain (i.e., two studies), active movement extent discrimination apparatus (two studies), and within-group analysis of threshold to detect passive motion (three studies for overall analysis). The fewer studies could increase the chances of a type II error [176]. Lastly, as the present review mainly incorporated studies that evaluated the influence of taping on joint repositioning accuracy tests, it is important to understand the inherent constraints associated with joint position tests to grasp the overall impact of taping on proprioception [27, 177]. The literature suggests that joint re-positioning tests lack ecological validity because the testing conditions are significantly different from normal daily activities [27, 178]. For instance, conditions such as slow angular velocities, non/partial-weight bearing conditions, absence of auditory and visual feedback, and isolation of the joint under investigation mean that these tasks do not accurately reflect the normal performance of the proprioceptive system in real-world scenarios [27]. Additionally, since joint position sense tests heavily rely on memory and attention, the outcomes may not solely reflect an individual's proprioceptive ability [27, 177]. For example, in cases where an individual has good proprioception but suffers from memory deficits or attention issues, their performance on joint position sense tests may be adversely affected. This suggests that the results of joint position sense tests may not accurately isolate and evaluate proprioceptive function when other cognitive factors come into play. The reader is recommended to infer the results of this review in light of the aforementioned limitations.
Future directions
Although the number of studies incorporating taping for improving proprioception in healthy and patient population groups has increased in the past decade, a few aspects still warrant exploration. For instance, limited research has evaluated the long-term retention of proprioceptive accuracy after the application of taping [78, 103]. Conventionally, taping has been identified as a transient approach that facilitates performance transiently by guiding the movement when it is being worn. However, once it’s removed, the lack of guidance (see guidance hypothesis [179]) by taping forces improved accuracy back to initial levels [171]. An effective means by which this feedback dependency of taping could be countered by tapering the extent of tactile feedback provided over time. Here, perhaps reducing the length of taping applied [51], or even the tension with which taping is used could reduce the extent of feedback being provided to the performer and allow them to form robust internal feedback/feed-forward models concerning the task at hand. Future studies should try to evaluate these outcomes to ascertain if tactile stimulation via taping can also enhance learning as compared to performance.
Conclusion
The meta-analysis suggests a positive influence of taping on proprioceptive accuracy outcomes in healthy population groups. The increments for repositioning accuracy were confirmed to be higher in the between group analysis against both placebo and no taping comparators. Besides, subgroup analyses revealed that both elastic taping and rigid taping had similar efficacy in improving repositioning accuracy. Despite the sensitivity analyses confirming the robustness of the findings, readers are recommended to interpret these results cautiously as the studies included in the review were of "fair" methodological quality, and high levels of heterogeneity were observed in the meta-analyses. Nonetheless, the study provides evidence for incorporating taping to promote joint repositioning accuracy.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
References
Qin Y, Li M, Han J, Cui G, Du W, Yang K: Research hotspots and trends of Kinesio Taping from 2011 to 2020: a bibliometric analysis. Environ Sci Pollution Res. 2022.
Yoshida A, Kahanov L. The effect of kinesio taping on lower trunk range of motions. Res Sports Med. 2007;15(2):103–12.
Kim S-Y, Oh D-W, Kim T-Y. Functional Taping Technique for Chronic Back Pain and Lower Extremity Pain-McConnell’s Approach. J Korean Acad Orthop Manual Phys Ther. 2008;14(2):50–9.
Gardner MJ, Parada S, Routt MLC Jr. Internal rotation and taping of the lower extremities for closed pelvic reduction. J Orthop Trauma. 2009;23(5):361–4.
Franettovich MM, Murley GS, David BS, Bird AR. A comparison of augmented low-Dye taping and ankle bracing on lower limb muscle activity during walking in adults with flat-arched foot posture. J Sci Med Sport. 2012;15(1):8–13.
Bennell K, Coburn S, Wee E, Green S, Harris A, Forbes A, Buchbinder R. Efficacy and cost-effectiveness of a physiotherapy program for chronic rotator cuff pathology: A protocol for a randomised, double-blind, placebo-controlled trial. BMC Musculoskelet Disord. 2007;8(1):86.
Cai C, Au IPH, An W, Cheung RTH. Facilitatory and inhibitory effects of Kinesio tape: Fact or fad? J Sci Med Sport. 2016;19(2):109–12.
Kalron A, Bar-Sela S. A systematic review of the effectiveness of Kinesio Taping–fact or fashion. Eur J Phys Rehabil Med. 2013;49(5):699–709.
Parreira PdCS, Costa LdCM. Junior LCH, Lopes AD, Costa LOP: Current evidence does not support the use of Kinesio Taping in clinical practice: a systematic review. J Physiother. 2014;60(1):31–9.
Xue X, Chen Y, Mao X, Tu H, Yang X, Deng Z, Li N. Effect of kinesio taping on low back pain during pregnancy: a systematic review and meta-analysis. BMC Pregnancy Childbirth. 2021;21(1):1–11.
Tran L, Makram AM, Makram OM, Elfaituri MK, Morsy S, Ghozy S, Zayan AH, Nam NH, Zaki MMM, Allison EL: Efficacy of kinesio taping compared to other treatment modalities in musculoskeletal disorders: a systematic review and meta-analysis. Res Sports Med. 2021:1–24.
Kasawara KT, Mapa JMR, Ferreira V, Added MAN, Shiwa SR, Carvas N Jr, Batista PA. Effects of Kinesio Taping on breast cancer-related lymphedema: A meta-analysis in clinical trials. Physiother Theory Pract. 2018;34(5):337–45.
Jaraczewska E, Long C. Kinesio® taping in stroke: improving functional use of the upper extremity in hemiplegia. Top Stroke Rehabil. 2006;13(3):31–42.
Delahunt E, McGrath A, Doran N, Coughlan GF. Effect of taping on actual and perceived dynamic postural stability in persons with chronic ankle instability. Arch Phys Med Rehabil. 2010;91(9):1383–9.
Logan CA, Bhashyam AR, Tisosky AJ, Haber DB, Jorgensen A, Roy A, Provencher MT. Systematic review of the effect of taping techniques on patellofemoral pain syndrome. Sports Health. 2017;9(5):456–61.
Capecci M, Serpicelli C, Fiorentini L, Censi G, Ferretti M, Orni C, Renzi R, Provinciali L, Ceravolo MG. Postural rehabilitation and Kinesio taping for axial postural disorders in Parkinson’s disease. Arch Phys Med Rehabil. 2014;95(6):1067–75.
Kwon M, Lee S, Lee J, Lee A, Lee H. The Effects of Functional Ankle Taping on Postural Stability in Elite Judo Players. Appl Sci. 2022;12(21):10779.
Lau KK-L, Cheng KC-C: Effectiveness of taping on functional performance in elite athletes: A systematic review. J Biomechanics. 2019;90:16–23.
Sacco IdCN. Takahasi HY, Suda EY, Battistella LR, Kavamoto CA, Lopes JAF, Vasconcelos JCPd: Ground reaction force in basketball cutting maneuvers with and without ankle bracing and taping. Sao Paulo Med J. 2006;124:245–52.
Crossley K, Cowan SM, Bennell KL, McConnell J. Patellar taping: is clinical success supported by scientific evidence? Man Ther. 2000;5(3):142–50.
Bishop C, Arnold JB, May T. Effects of Taping and Orthoses on Foot Biomechanics in Adults with Flat-Arched Feet. Med Sci Sports Exerc. 2016;48(4):689–96.
Tobin S, Robinson G. The effect of McConnell’s vastus lateralis inhibition taping technique on vastus lateralis and vastus medialis obliquus activity. Physiotherapy. 2000;86(4):173–83.
Joscha K, Julian M. What is the current level of evidence and the efficacy of medical taping on circulation, muscle function, correction, pain, and proprioception? Amsterdam, the Netherlands, Professional Assignment Project, European School of Physiotherapy, Hogeschool van Amsterdam. 2010.
Kase K: Clinical therapeutic applications of the Kinesio taping method. Albuquerque. 2003.
Park Y-H, Lee J-H. Effects of proprioceptive sense-based Kinesio taping on walking imbalance. J Phys Ther Sci. 2016;28(11):3060–2.
Kneeshaw D. Shoulder taping in the clinical setting. J Bodyw Mov Ther. 2002;6(1):2–8.
Han J, Waddington G, Adams R, Anson J, Liu Y. Assessing proprioception: A critical review of methods. J Sport Health Sci. 2016;5(1):80–90.
Labanca L, Ciardulli F, Bonsanto F, Sommella N, Di Martino A, Benedetti MG. Balance and proprioception impairment, assessment tools, and rehabilitation training in patients with total hip arthroplasty: a systematic review. BMC Musculoskelet Disord. 2021;22(1):1055.
Van Tunen JAC, Dell’Isola A, Juhl C, Dekker J, Steultjens M, Thorlund JB, Lund H. Association of malalignment, muscular dysfunction, proprioception, laxity and abnormal joint loading with tibiofemoral knee osteoarthritis-a systematic review and meta-analysis. BMC Musculoskelet Disord. 2018;19:1–15.
Röijezon U, Clark NC, Treleaven J. Proprioception in musculoskeletal rehabilitation. Part 1: Basic science and principles of assessment and clinical interventions. Man Ther. 2015;20(3):368–77.
Chiaramonte R, D’Amico S, Caramma S, Grasso G, Pirrone S, Ronsisvalle MG, Bonfiglio M. The Effectiveness of Goal-Oriented Dual Task Proprioceptive Training in Subacute Stroke: A Retrospective Observational Study. Ann Rehabil Med. 2024;48(1):31.
Chiaramonte R, Bonfiglio M, Leonforte P, Coltraro GL, Guerrera CS, Vecchio M. Proprioceptive and Dual-Task Training: The Key of Stroke Rehabilitation, A Systematic Review. J Funct Morphol Kinesiol. 2022;7(3):53.
Chiaramonte R, Bonfiglio M, Chisari S: Multidisciplinary protocol for the management of fibromyalgia associated with imbalance. Our experience and literature review. Revista da Associação Médica Brasileira. 2019;65.
Konishi Y. Tactile stimulation with Kinesiology tape alleviates muscle weakness attributable to attenuation of Ia afferents. J Sci Med Sport. 2013;16(1):45–8.
Morrissey D. Proprioceptive shoulder taping. J Bodyw Mov Ther. 2000;4(3):189–94.
Jerosch J, Hoffstetter I, Bork H, Bischof M. The influence of orthoses on the proprioception of the ankle joint. Knee Surg Sports Traumatol Arthrosc. 1995;3(1):39–46.
Glick JM, Gordon RB, Nishimoto D. The prevention and treatment of ankle injuries. Am J Sports Med. 1976;4(4):136–41.
Karlsson J, Andreasson GO. The effect of external ankle support in chronic lateral ankle joint instability: an electromyographic study. Am J Sports Med. 1992;20(3):257–61.
Heit EJ, Lephart SM, Rozzi SL. The effect of ankle bracing and taping on joint position sense in the stable ankle. J Sport Rehabil. 1996;5(3):206–13.
Cimino SR, Beaudette SM, Brown SHM. Kinesio taping influences the mechanical behaviour of the skin of the low back: A possible pathway for functionally relevant effects. J Biomech. 2018;67:150–6.
Pamuk U, Yucesoy CA. MRI analyses show that kinesio taping affects much more than just the targeted superficial tissues and causes heterogeneous deformations within the whole limb. J Biomech. 2015;48(16):4262–70.
Kelly LA, Racinais S, Tanner CM, Grantham J, Chalabi H. Augmented Low Dye Taping Changes Muscle Activation Patterns and Plantar Pressure During Treadmill Running. J Orthop Sports Phys Ther. 2010;40(10):648–55.
Yam TTT, Or PPL, Ma AWW, Fong SSM, Wong MS. Effect of Kinesio taping on Y-balance test performance and the associated leg muscle activation patterns in children with developmental coordination disorder: A randomized controlled trial. Gait Posture. 2019;68:388–96.
Sarvestan J, Svoboda Z. Acute effect of ankle Kinesio and athletic taping on ankle range of motion during various agility tests in athletes with chronic ankle sprain. J Sport Rehabil. 2019;29(5):527–32.
Hunter LY. Braces and taping. Clin Sports Med. 1985;4(3):439–53.
Mostafavifar M, Wertz J, Borchers J. A systematic review of the effectiveness of kinesio taping for musculoskeletal injury. Phys Sportsmed. 2012;40(4):33–40.
Callaghan MJ, McKie S, Richardson P, Oldham JA. Effects of Patellar Taping on Brain Activity During Knee Joint Proprioception Tests Using Functional Magnetic Resonance Imaging. Phys Ther. 2012;92(6):821–30.
Lin Z-M, Yang J-F, Lin Y-L, Cheng Y-C, Hung C-T, Chen C-S, Chou L-W. Effect of Kinesio Taping on Hand Sensorimotor Control and Brain Activity. Appl Sci. 2021;11(22):10522.
Grütters K, Narciss S, Beaudette SM, Oppici L. Reducing lumbar flexion in a repetitive lifting task: Comparison of leukotape and kinesio tape and their effect on lumbar proprioception. 2022.
Chen H-S, Chang Y-Z, Fang C-M, Lin C-Y, Yang W-C: [論文摘要] Effect of Kinesio Taping on Lower Extremities Proprioception and Dynamic Balance in Taekwondo Poomsae Athletes. 物理治療. 2022;47(2):137–137.
Yu R, Yang Z, Witchalls J, Adams R, Waddington G, Han J. Kinesiology tape length and ankle inversion proprioception at step-down landing in individuals with chronic ankle instability. J Sci Med Sport. 2021;24(9):894–9.
Adams R, Ganderton C, Han J, Waddington G, Witchalls J, Yang Z. Effects of kinesiology tape with training shoes on ankle proprioception in individuals with chronic ankle instability during drop landing. J Sci Med Sport. 2021;24:S55–6.
Narasinta I, Masduchi RH, Kurniawati PM. Immediate Effect of Kinesio Taping Application on Joint Proprioception Function in Knee Osteoarthritis Patients. Surabaya Phys Med Rehabil J. 2019;1(1):1–5.
Dhahi M, Abdelsalam MS. Effect of Kinesio Tape on Ankle Joint Position Sense and Evertor Peak Torque in Football Players Following Exercise Induced Fatigue. Int J Adv Res. 2019;7(3):434–41.
Jahjah A, Seidenspinner D, Schüttler K, Klasan A, Heyse TJ, Malcherczyk D, El-Zayat BF. The effect of ankle tape on joint position sense after local muscle fatigue: a randomized controlled trial. BMC Musculoskelet Disord. 2018;19(1):1–8.
Brogden CM, Marrin K, Page RM, Greig M. The efficacy of elastic therapeutic tape variations on measures of ankle function and performance. Phys Ther Sport. 2018;32:74–9.
Göktaş HE, Çitaker S, Yurtsever ED. Acute Effects of Dynamic Taping on Pain, Range of Motion and Proprioception in Patients with Subacromial Impingement Syndrome. Int J Acad Med Pharm. 2022;4(2):35–41.
Wilson LM, Greig M. The efficacy of functional supports in mediating the effects of exercise on shoulder joint position sense. Isokinet Exerc Sci. 2017;25(2):127–34.
Callaghan MJ, Selfe J, McHenry A, Oldham JA. Effects of patellar taping on knee joint proprioception in patients with patellofemoral pain syndrome. Man Ther. 2008;13(3):192–9.
Cecchinato AL: The effectiveness of ankle taping and bracing on joint position sense of functionally unstable ankles following an exercise regime: University of New Hampshire Plymouth State College; 2003.
Callaghan MJ, Selfe J, Bagley PJ, Oldham JA. The effects of patellar taping on knee joint proprioception. J Athl Train. 2002;37(1):19.
Refshauge KM, Kilbreath SL, Raymond J. The effect of recurrent ankle inversion sprain and taping on proprioception at the ankle. Med Sci Sports Exerc. 2000;32(1):10–5.
Williams S, Whatman C, Hume PA, Sheerin K. Kinesio taping in treatment and prevention of sports injuries. Sports Med. 2012;42(2):153–64.
Bayu CG, Andriana M, Pawana A. Effect of McConnell Patelar Taping on Joint Position Sense and Threshold to Detection Passive Motion in Sub acute Stroke Patient. Int J Res Publications. 2022;94(1):8–8.
Ruggiero SA, Frost LR, Vallis LA, Brown SHM. Effect of short-term application of kinesio tape on the flexion-relaxation phenomenon, trunk postural control and trunk repositioning in healthy females. J Sports Sci. 2016;34(9):862–70.
Aarseth LM, Suprak DN, Chalmers GR, Lyon L, Dahlquist DT. Kinesio tape and shoulder-joint position sense. J Athl Train. 2015;50(8):785–91.
Miralles I, Monterde S, del Rio O, Valero S, Montull S, Salvat I: Has Kinesio Tape Effects on Ankle Proprioception? A Randomized Clinical Trial. Clinical Kinesiology (Online Edition). 2014;68(2).
Mumford K. The acute effects of taping on proprioception in the ankle with previous inversion sprain. 2003.
Hughes T, Rochester P. The effects of proprioceptive exercise and taping on proprioception in subjects with functional ankle instability: A review of the literature. Phys Ther Sport. 2008;9(3):136–47.
Varela Miranda M, Justo Cousiño LA, González González Y, Alonso Calvete A. Effect of the neuromuscular taping on proprioception and postural control. Systematic review. Archivos de Neurociencias. 2022;27(3).
Raymond J, Nicholson LL, Hiller CE, Refshauge KM. The effect of ankle taping or bracing on proprioception in functional ankle instability: a systematic review and meta-analysis. J Sci Med Sport. 2012;15(5):386–92.
Ghai S, Driller M, Ghai I. Effects of joint stabilizers on proprioception and stability: A systematic review and meta-analysis. Phys Ther Sport. 2017;25:65–75.
Parreira PdCS, Costa LdCM. Hespanhol Junior LC, Lopes AD, Costa LOP: Current evidence does not support the use of Kinesio Taping in clinical practice: a systematic review. J Physiother. 2014;60(1):31–9.
Saran M, Pawaria S, Kalra S. Kinesio taping with ballistic six plyometric training on speed, accuracy, target and joint proprioception in fast bowlers with glenohumeral instability. Comp Exer Physiol. 2022;18(4):357–63.
Saki F, Romiani H, Ziya M, Gheidi N. The effects of gluteus medius and tibialis anterior kinesio taping on postural control, knee kinematics, and knee proprioception in female athletes with dynamic knee valgus. Phys Ther Sport. 2022;53:84–90.
Mehta P, Prabhakar AJ, Eapen C. Effect of kinesio taping on shoulder maximal voluntary contraction, proprioception and upper limb reaction time in recreational badminton players: A randomized placebo controlled trial. Physiother Prac Res. 2022;43(Preprint):97–105.
Kim JH, Kim KH, Kim DH: Effects of Proprioception Training with Kinesio Taping of the Knee Joints on the Proprioception, Balance, and Gait in Stroke Patients: A Single-Blind Randomized Trials. Physikalische Medizin, Rehabilitationsmedizin, Kurortmedizin. 2022.
Kielė D, Solianik R: Four-Week Application of Kinesiotaping Improves Proprioception, Strength, and Balance in Individuals With Complete Anterior Cruciate Ligament Rupture. J Strength Conditioning Res. 2022:10–1519.
Boonkerd C, Thinchuangchan K, Chalarak N, Thonpakorb S, Wanasoonthontham R, Kitsuksan T, Laddawong T. Effect of Kinesio Tape on Proprioception, Static and Dynamic Balance in Individuals with Chronic Ankle Instability. Ann Appl Sport Sci. 2022:2476–4981.
Smyth E, Waddington G, Witchalls J, Newman P, Weissensteiner J, Hughes S, Niyonsenga T, Drew M. Does ankle tape improve proprioception acuity immediately after application and following a netball session? A randomised controlled trial. Phys Ther Sport. 2021;48:20–5.
Chen Y-S, Tseng W-C, Chen C-H, Lu Y-X. Moderate kinesio taping stretch tension produced good inter-day reliability of dosiflexion joint position sense measurement. Gazz Med Ital Arch Sci Med. 2021;180:35–42.
Binaei F, Hedayati R, Mirmohammadkhani M, Taghizadeh Delkhoush C, Bagheri R. Examining the Use of Kinesiology Tape During Weight Bearing Exercises on Proprioception in Participants With Functional Ankle Instability. Percept Mot Skills. 2021;128(6):2654–68.
Alawna M, Unver B, Yuksel E. Effect of ankle taping and bandaging on balance and proprioception among healthy volunteers. Sport Sci Health. 2021;17(3):665–76.
Santos GLd, Souza MB, Desloovere K, Russo TL. Elastic tape improved shoulder joint position sense in chronic hemiparetic subjects: a randomized sham-controlled crossover study. PloS one. 2017;12(1):e0170368.
Cho H-y. Kim E-H, Kim J, Yoon YW: Kinesio taping improves pain, range of motion, and proprioception in older patients with knee osteoarthritis: a randomized controlled trial. Am J Phys Med Rehabil. 2015;94(3):192–200.
Hinman RS, Crossley KM, McConnell J, Bennell KL. Does the application of tape influence quadriceps sensorimotor function in knee osteoarthritis? Rheumatology. 2004;43(3):331–6.
Liu K, Qian J, Gao Q, Ruan B: Effects of Kinesio taping of the knee on proprioception, balance, and functional performance in patients with anterior cruciate ligament rupture: A retrospective case series. Medicine. 2019;98(48).
Bischoff L, Babisch C, Babisch J, Layher F, Sander K, Matziolis G, Pietsch S, Röhner E. Effects on proprioception by Kinesio taping of the knee after anterior cruciate ligament rupture. Eur J Orthop Surg Traumatol. 2018;28(6):1157–64.
Vanti C, Bertozzi L, Gardenghi I, Turoni F, Guccione AA, Pillastrini P. Effect of Taping on Spinal Pain and Disability: Systematic Review and Meta-Analysis of Randomized Trials. Phys Ther. 2015;95(4):493–506.
Long Z, Wang R, Han J, Waddington G, Adams R, Anson J. Optimizing ankle performance when taped: Effects of kinesiology and athletic taping on proprioception in full weight-bearing stance. J Sci Med Sport. 2017;20(3):236–40.
McNeill W, Pedersen C. Dynamic tape. Is it all about controlling load? J Bodyw Mov Ther. 2016;20(1):179–88.
Moseley AM, Rahman P, Wells GA, Zadro JR, Sherrington C, Toupin-April K, Brosseau L. Agreement between the Cochrane risk of bias tool and Physiotherapy Evidence Database (PEDro) scale: a meta-epidemiological study of randomized controlled trials of physical therapy interventions. PLoS ONE. 2019;14(9):e0222770.
Cashin AG, McAuley JH. Clinimetrics: Physiotherapy Evidence Database (PEDro) Scale. J Physiother. 2020;66(1):59.
Borenstein M. Comprehensive meta‐analysis software. Systematic reviews in health research: meta‐analysis in context. 2022:535–548.
Brydges CR. Effect size guidelines, sample size calculations, and statistical power in gerontology. Innov Aging. 2019;3(4):igz036.
West SL, Gartlehner G, Mansfield AJ, Poole C, Tant E, Lenfestey N, Lux LJ, Amoozegar J, Morton SC, Carey TC: Comparative effectiveness review methods: Clinical heterogeneity. 2010.
Willis BH, Riley RD. Measuring the statistical validity of summary meta-analysis and meta-regression results for use in clinical practice. Stat Med. 2017;36(21):3283–301.
Duval S, Tweedie R. Trim and fill: a simple funnel-plot–based method of testing and adjusting for publication bias in meta-analysis. Biometrics. 2000;56(2):455–63.
Haddaway NR, Page MJ, Pritchard CC, McGuinness LA. PRISMA2020: An R package and Shiny app for producing PRISMA 2020-compliant flow diagrams, with interactivity for optimised digital transparency and Open Synthesis. Campbell Syst Rev. 2022;18(2):e1230.
Abbasi S, Hadian Rasanani M-R, Ghotbi N, Olyaei GR, Bozorgmehr A, Rasouli O. Short-term effect of kinesiology taping on pain, functional disability and lumbar proprioception in individuals with nonspecific chronic low back pain: a double-blinded, randomized trial. Chiropractic Manual Ther. 2020;28(1):1–10.
Ahn IK, Kim YL, Bae Y-H, Lee SM. Immediate effects of kinesiology taping of quadriceps on motor performance after muscle fatigued induction. Evid Based Complement Alternat Med. 2015;410526:1–7.
Alahmari KA, Reddy RS, Tedla JS, Samuel PS, Kakaraparthi VN, Rengaramanujam K, Ahmed I. The effect of Kinesio taping on cervical proprioception in athletes with mechanical neck pain—a placebo-controlled trial. BMC Musculoskelet Disord. 2020;21(1):1–9.
Alawna M, Mohamed AA. Short-term and long-term effects of ankle joint taping and bandaging on balance, proprioception and vertical jump among volleyball players with chronic ankle instability. Phys Ther Sport. 2020;46:145–54.
Allah NHN, Mohamed GA, Elhafez SM, Emran IM. Effect of rigid tape on hip joint proprioception in patients with sacroiliac joint dysfunction. Biosci Res. 2018;15(3):2686–92.
Aytar A, Ozunlu N, Surenkok O, Baltacı G, Oztop P, Karatas M. Initial effects of kinesio® taping in patients with patellofemoral pain syndrome: A randomized, double-blind study. Isokinet Exerc Sci. 2011;19(2):135–42.
Babakhani F, Heydarian M, Hatefi M. The immediate effect of kinesiotape and wobble board training on ankle joint position sense in athletes with functional ankle instability. J Adv Sport Technol. 2020;4(2):49–59.
Burfeind SM, Chimera N. Randomized control trial investigating the effects of kinesiology tape on shoulder proprioception. J Sport Rehabil. 2015;24(4):405–12.
Fazli F, Farsi A, Takamjani IE, Mansour S, Yousefi N, Azadinia F: Effect of Knee Orthosis and Kinesio Taping on Clinical and Neuromuscular Outcomes in Patients with Knee Osteoarthritis: A Randomized Clinical Trial. Life 2023;15:17.
Grütters K, Narciss S, Beaudette SM, Oppici L. Reducing lumbar flexion in a repetitive lifting task: Comparison of leukotape and kinesio tape and their effect on lumbar proprioception. Appl Sci. 2023;13(10):5908.
Iris M, Monterde S, Salvador M, Salvat I, Fernández-Ballart J, Judith B. Ankle taping can improve proprioception in healthy volunteers. Foot Ankle Int. 2010;31(12):1099–106.
Keenan KA, Akins JS, Varnell M, Abt J, Lovalekar M, Lephart S, Sell TC. Kinesiology taping does not alter shoulder strength, shoulder proprioception, or scapular kinematics in healthy, physically active subjects and subjects with Subacromial Impingement Syndrome. Phys Ther Sport. 2017;24:60–6.
Kurt EE, Büyükturan Ö, Erdem HR, Tuncay F, Sezgin H. Short-term effects of kinesio tape on joint position sense, isokinetic measurements, and clinical parameters in patellofemoral pain syndrome. J Phys Ther Sci. 2016;28(7):2034–40.
Saki F, Shayesteh A, Ramezani F, Shahheidari S. The Effects of Lower Leg Kinesio Taping on Ankle Proprioception, Static and Dynamic Balance in Athletes with Medial Tibial Stress Syndrome. J Adv Sport Technol. 2023;7(2):1–11.
Shahrokhi H, Miri H, Yekedehghan S. Comparison of the effect of 8 week taping and selected therapeutic exercises on range of motion, proprioception and pain in gymnasts with shoulder impingement syndrome. Stud Sport Med. 2020;11(26):127–46.
Shams F, Hadadnezhad M, Letafatkar A, Hogg J. Valgus Control Feedback and Taping Improves the Effects of Plyometric Exercises in Women With Dynamic Knee Valgus. Sports Health. 2022;14(5):747–57.
Shih YF, Lee YF, Chen WY. Effects of kinesiology taping on scapular reposition accuracy, kinematics, and muscle activity in athletes with shoulder impingement syndrome: A randomized controlled study. J Sport Rehabil. 2018;27(6):560–9.
Torres R, Trindade R, Gonçalves RS. The effect of kinesiology tape on knee proprioception in healthy subjects. J Bodyw Mov Ther. 2016;20(4):857–62.
Trost A: The Effects of Kinesio Tape™ on Proprioception and Balance in Individuals with and without Knee Pain. University of Hawai'i at Manoa; 2020.
Ucuzoglu ME, Unver B, Sarac DC, Cilga G. Similar effects of two different external supports on wrist joint position sense in healthy subjects: A randomized clinical trial. Hand Surgery Rehabil. 2020;39(2):96–101.
Bailey D, Firth P. Does kinesiology taping of the ankles affect proprioceptive control in professional football (soccer) players? Phys Ther Sport. 2017;25:94–8.
Boonkerd C, Thinchuangchan K, Chalarak N, Thonpakorb S, Wanasoonthontham R, Kitsuksan T, Laddawong T. Effect of Kinesio Tape on Proprioception, Static and Dynamic Balance in Individuals with Chronic Ankle Instability. Ann Appl Sport Sci. 2023:0–0.
Bradley T, Baldwick C, Fischer D, Murrell GAC. Effect of taping on the shoulders of Australian football players. Br J Sports Med. 2009;43(10):735–8.
Fratocchi G, Di Mattia F, Rossi R, Mangone M, Santilli V, Paoloni M. Influence of Kinesio Taping applied over biceps brachii on isokinetic elbow peak torque. A placebo controlled study in a population of young healthy subjects. J Sci Med Sport. 2013;16(3):245–9.
Han J-T. Immediate Effect of Calf Muscle Kinesio Taping on Ankle Joint Reposition Sense and Force Sense in Healthy Elderly. 대한물리치료학회지 (JKPT). 2020;32(4):193–197.
Hopper DM, Grisbrook TL, Finucane M, Nosaka K. Effect of ankle taping on angle and force matching and strength of the plantar flexors. Phys Ther Sport. 2014;15(4):254–60.
Hosp S, Bottoni G, Heinrich D, Kofler P, Hasler M, Nachbauer W. A pilot study of the effect of Kinesiology tape on knee proprioception after physical activity in healthy women. J Sci Med Sport. 2015;18(6):709–13.
Hubbard TJ, Kaminski TW. Kinesthesia is not affected by functional ankle instability status. J Athl Train. 2002;37(4):481.
Kaminski TW, Gerlach TM. The effect of tape and neoprene ankle supports on ankle joint position sense. Phys Ther Sport. 2001;2(3):132–40.
Li P, Wei Z, Zeng Z, Wang L. Acute effect of kinesio tape on postural control in individuals with functional ankle instability following ankle muscle fatigue. Front Physiol. 2022;13:980438.
Jj L. Hung CJ, Yang PL: The effects of scapular taping on electromyographic muscle activity and proprioception feedback in healthy shoulders. J Orthop Res. 2011;29(1):53–7.
Maqsood M, Váczi M. Immediate Effects of Quadriceps Muscle Kinesiology Taping on Joint Position Sense and Force Sense in Healthy Individuals. In: Preprints. Preprints; 2023.
Park S-Y, Kim M-J, Seol S-E, Hwang C, Hong J-S, Kim H, Shin W-S. Effects of dynamic taping on shoulder joint proprioception. Phys Ther Rehabil Sci. 2020;9(4):269–74.
Refshauge KM, Raymond J, Kilbreath SL, Pengel L, Heijnen I. The effect of ankle taping on detection of inversion-eversion movements in participants with recurrent ankle sprain. Am J Sports Med. 2009;37(2):371–5.
Robbins S, Waked E, Rappel R. Ankle taping improves proprioception before and after exercise in young men. Br J Sports Med. 1995;29(4):242–7.
Simoneau GG, Degner RM, Kramper CA, Kittleson KH. Changes in ankle joint proprioception resulting from strips of athletic tape applied over the skin. J Athl Train. 1997;32(2):141.
Weerakkody N, Allen T. The effects of fast bowling fatigue and adhesive taping on shoulder joint position sense in amateur cricket players in Victoria. Australia J Sports Sci. 2017;35(19):1954–62.
Wei Z, Wang X-X, Wang L. Effect of short-term kinesiology taping on knee proprioception and quadriceps performance in healthy individuals. Front Physiol. 2020;11:1501.
Zanca GG, Mattiello SM, Karduna AR. Kinesio taping of the deltoid does not reduce fatigue induced deficits in shoulder joint position sense. Clin Biomech. 2015;30(9):903–7.
Akbari M, Pahnabi G, Karimi H. Immediate Effect of Kinesio Taping on Knee Joint Position Sense after Anterior Cruciate Ligament Reconstruction. J Clin Physiother Res. 2016;2(4):162–8.
Bae Y-S. Effects of spiral taping on proprioception in subjects with unilateral functional ankle instability. J Phys Ther Sci. 2017;29(1):106–8.
Cho SH, Moon HJ. Effects of Kinesio-taping on balance abilities and proprioception sense. J Int Aca Phys Ther Res. 2017;8(2):1163–7.
Halseth T, John WM, Mark D. The effects of Kinesio TM Taping on proprioception at the ankle. J Spo Sci Med. 2004;3(1):1–7.
Momeni-lari H, Ghasemi M, Khademi-kalantari K, Akbarzadeh-baghban A. The Short-Term Effects of Kinesio Tape on Joint Position Sense, Sense of Force and Postural Control in Patients with Functional Ankle Instability. J Babol Univ Med Sci. 2018;20(8):51–5.
Niknam H, Sarmadi A, Salavati M, Madadi F. The effect of knee kinesiotaping on proprioception and weight bearing in ACL reconstructed patients. Daneshvar Med. 2011;19(2):33–42.
Poyraz İ, Vergili Ö. The impacts of Kinesio taping on muscular fatigue and proprioception following fatigue among adolescent basketball players. J Health Sci Med. 2023;6(3):623–9.
Rajabzadeh B, Amiri A, Vasaghi-Gharamaleki B, Saneii SH. The Effects of Shoulder Kinesio Taping on Shooting Accuracy and Joint Position Sense in Female Archery Athletes. Function Disability J. 2019;2(1):9–16.
Seo H-D, Kim M-Y, Choi J-E, Lim G-H, Jung S-I, Park S-H, Cheon S-H, Lee H-Y. Effects of Kinesio taping on joint position sense of the ankle. J Phys Ther Sci. 2016;28(4):1158–60.
Spanos S, Brunswic M, Billis E. The effect of taping on the proprioception of the ankle in a non-weight bearing position, amongst injured athletes. Foot. 2008;18(1):25–33.
Barbanera M. Mazuchi FdA, Batista JPB, Ultremare JdM, Iwashita JdS, Ervilha UF: Semi-rigid brace and taping decrease variability of the ankle joint position sense. Motriz. 2014;20:448–53.
Lee W-H, Kwon O-Y, Yi C-H, Jeon H-S, Ha S-M. Effects of taping on wrist extensor force and joint position reproduction sense of subjects with and without lateral epicondylitis. J Phys Ther Sci. 2011;23(4):629–34.
Mokhtarinia H, Ebrahimi TI, Salavati M, Goharpai S, Khosravi A. The effect of patellar taping on knee joint proprioception in patients with patellofemoral pain syndrome. 2008.
Schenker M. Tape versus mikros. Kranken Gymnastik. 1991;43(0010):01081–97.
Barzegar Ganji Z, Dehghan-Manshadi F, Khademi-Kalantari K, Ghasemi M, Tabatabaee SM. The immediate effect of kinesio tape on the variation of shoulder position sense at different angles in patients with impingement syndrome. Sci J Rehabil Med. 2015;4(2):37–45.
Kisa EP, Kaya BK. Does Taping Have an Immediate Effect on Shooting the Target? Percept Mot Skills. 2023;130(4):1609–23.
Turner RM, Bird SM, Higgins JPT. The Impact of Study Size on Meta-analyses: Examination of Underpowered Studies in Cochrane Reviews. PLoS ONE. 2013;8(3):e59202.
Roberts D, Ageberg E, Andersson G, Fridén T. Clinical measurements of proprioception, muscle strength and laxity in relation to function in the ACL-injured knee. Knee Surg Sports Traumatol Arthrosc. 2007;15(1):9–16.
Takahashi K, Shitara H, Ichinose T, Sasaki T, Hamano N, Hasegawa M, Yamaji T, Tazawa M, Chikuda H, Wada N. Delayed detection of passive motion in shoulders with a rotator cuff tear. J Orthop Res. 2022;40(6):1263–9.
Antcliff S, Welvaert M, Witchalls J, Wallwork SB, Waddington G. Using the Active Movement Extent Discrimination Apparatus to Test Individual Proprioception Acuity: Implications for Test Design. Percept Mot Skills. 2020;128(1):283–303.
Swets JA: Signal detection theory and ROC analysis in psychology and diagnostics: Collected papers: Psychology Press; 2014.
Stanley TD, Doucouliagos H, Ioannidis JPA. Beyond Random Effects: When Small-Study Findings Are More Heterogeneous. Adv Methods Pract Psychol Sci. 2022;5(4):25152459221120428.
Perlau R, Frank C, Fick G. The effect of elastic bandages on human knee proprioception in the uninjured population. Am J Sports Med. 1995;23(2):251–5.
Birmingham TB, Kramer JF, Inglis JT, Mooney CA, Murray LJ, Fowler PJ, Kirkley S. Effect of a neoprene sleeve on knee joint position sense during sitting open kinetic chain and supine closed kinetic chain tests. Am J Sports Med. 1998;26(4):562–6.
Ghai S, Ghai I, Narciss S. Influence of taping on force sense accuracy: a systematic review with between and within group meta-analysis. BMC Sports Sci Med Rehabil. 2023;15(1):138.
Alam S, Malhotra D, Munjal J, Chachra A. Immediate effect of Kinesio taping on shoulder muscle strength and range of motion in healthy individuals: A randomised trial. Hong Kong Physiother J. 2015;33(2):80–8.
Reynard F, Vuistiner P, Léger B, Konzelmann M. Immediate and short-term effects of kinesiotaping on muscular activity, mobility, strength and pain after rotator cuff surgery: a crossover clinical trial. BMC Musculoskelet Disord. 2018;19(1):305.
Franettovich Smith MM, Coates SS, Creaby MW. A comparison of rigid tape and exercise, elastic tape and exercise and exercise alone on pain and lower limb function in individuals with exercise related leg pain: a randomised controlled trial. BMC Musculoskelet Disord. 2014;15(1):328.
Shaheen AF, Bull AMJ, Alexander CM. Rigid and Elastic taping changes scapular kinematics and pain in subjects with shoulder impingement syndrome; an experimental study. J Electromyogr Kinesiol. 2015;25(1):84–92.
Bozkurt T, Kilic RT, Yosmaoglu HB. The effect of elastic therapeutic taping and rigid taping on pain, functionality, and tissue temperature in lumbar radiculopathy: a randomized controlled study. Somatosens Mot Res. 2021;38(4):373–80.
Best R, Mauch F, Böhle C, Huth J, Brüggemann P. Residual Mechanical Effectiveness of External Ankle Tape Before and After Competitive Professional Soccer Performance. Clin J Sport Med. 2014;24(1):51–7.
Oppici L, Grütters K, Garofolini A, Rosenkranz R, Narciss S. Deliberate Practice and Motor Learning Principles to Underpin the Design of Training Interventions for Improving Lifting Movement in the Occupational Sector: A Perspective and a Pilot Study on the Role of Augmented Feedback. Front Sports Act Living. 2021;3.
Pinto BL, Beaudette SM, Brown SHM. Tactile cues can change movement: An example using tape to redistribute flexion from the lumbar spine to the hips and knees during lifting. Hum Mov Sci. 2018;60:32–9.
Williams SA, Ng L, Stephens N, Klem N, Wild C. Effect of prophylactic ankle taping on ankle and knee biomechanics during basketball-specific tasks in females. Phys Ther Sport. 2018;32:200–6.
Miura K, Ishibashi Y, Tsuda E, Okamura Y, Otsuka H, Toh S. The effect of local and general fatigue on knee proprioception. Arthroscopy. 2004;20(4):414–8.
Hiemstra LA, Lo IKY, Fowler PJ. Effect of fatigue on knee proprioception: implications for dynamic stabilization. J Orthop Sports Phys Ther. 2001;31(10):598–605.
Kim J, Kim S, Lee J. Longer application of kinesio taping would be beneficial for exercise-induced muscle damage. J Exercise Rehabil. 2016;12(5):456.
Button KS, Ioannidis J, Mokrysz C, Nosek BA, Flint J, Robinson ESJ, Munafò MR. Power failure: why small sample size undermines the reliability of neuroscience. Nat Rev Neurosci. 2013;14(5):365–76.
Goble DJ. Proprioceptive acuity assessment via joint position matching: from basic science to general practice. Phys Ther. 2010;90(8):1176–84.
Laszlo JI: Chapter 2 Motor Control and Learning: How Far Do the Experimental Tasks Restrict Our Theoretical Insight? In: Advances in Psychology. Volume 84, edn. Edited by Summers JJ: North-Holland; 1992: 47–79.
Schmidt RA, Young DE, Swinnen S, Shapiro DC. Summary knowledge of results for skill acquisition: support for the guidance hypothesis. J Exp Psychol Learn Mem Cogn. 1989;15(2):352.
Acknowledgements
Not applicable.
Funding
Open access funding provided by Karlstad University. This work was partly funded by the German Research Foundation (DFG, Deutsche Forschungsgemeinschaft) as part of Germany's Excellence Strategy—EXC 2050/1—Project ID 390696704—Cluster of Excellence "Centre for Tactile Internet with Human-in-the-Loop" (CeTI) of Technische Universität Dresden. The open access funding was provided by Karlstad University.
Author information
Authors and Affiliations
Contributions
SG conceptualized the study and was responsible for designing and implementing the research. SG, IG acted as the independent reviewers and performed the statistical analysis. SG wrote the initial version of the manuscript. All authors read and approved the final version of the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Ghai, S., Ghai, I. & Narciss, S. Influence of taping on joint proprioception: a systematic review with between and within group meta-analysis. BMC Musculoskelet Disord 25, 480 (2024). https://doi.org/10.1186/s12891-024-07571-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12891-024-07571-2