
Abstract
Background
The Swedish Fracture Register (SFR) is a national quality register for all types of fractures in Sweden. Spine fractures have been included since 2015 and are classified using a modified AOSpine classification. The aim of this study was to determine the accuracy of the classification of thoracolumbar burst fractures in the SFR.
Methods
Assessments of medical images were conducted in 277 consecutive patients with a thoracolumbar burst fracture (T10-L3) identified in the SFR. Two independent reviewers classified the fractures according to the AOSpine classification, with a third reviewer resolving disagreement. The combined results of the reviewers were considered the gold standard. The intra- and inter-rater reliability of the reviewers was determined with Cohen’s kappa and percent agreement. The SFR classification was compared with the gold standard using positive predictive values (PPV), Cohen’s kappa and percent agreement.
Results
The reliability between reviewers was high (Cohen’s kappa 0.70–0.97). The PPV for correctly classifying burst fractures in the SFR was high irrespective of physician experience (76–89%), treatment (82% non-operative, 95% operative) and hospital type (83% county, 95% university). The inter-rater reliability of B-type injuries and the overall SFR classification compared with the gold standard was low (Cohen’s kappa 0.16 and 0.17 respectively).
Conclusions
The SFR demonstrates a high PPV for accurately classifying burst fractures, regardless of physician experience, treatment and hospital type. However, the reliability of B-type injuries and overall classification in the SFR was found to be low. Future studies on burst fractures using SFR data where classification is important should include a review of medical images to verify the diagnosis.
Similar content being viewed by others

Background
Burst fractures are compression fractures of the spine involving injury to the posterior wall of the vertebral body and at least one end plate [1]. They often occur in the thoracolumbar transition due to the biomechanical forces being highest in this area [2].
The Swedish Fracture Register (SFR) is a nationwide quality register that collect data on all types of orthopedic fractures [3]. Data collected include the date and cause of injury, fracture classifications, treatment, reoperations, and patient-reported outcome measures. The SFR uses a simplified AO/OTA classifications [4] with the aid of pictures to guide the registering physician. Registrations in SFR are made by physicians of different levels of experience, including interns, residents, emergency physicians and orthopedic surgeons.
Spine fractures have been included in the SFR since 2015 [5]. As physicians of any expertise may register the fracture, the accuracy of the classifications, and in turn, the reliability of the data in the SFR may be compromised.
Methods
Aim
The aim of this study was to determine the reliability of the classification of thoracolumbar burst fractures in the SFR.
Study design
This study is retrospective on prospectively collected data.
Study population
Patients in working age, 18–66 years, with a single-level thoracolumbar fracture from the tenth thoracic vertebra to the third lumbar vertebra classified as a burst fracture were identified in the SFR.
Data in the SFR during the time period included the majority of trauma and orthopedic departments in Sweden, including university hospitals and county hospitals [3]. Data is entered by the physician treating the patient in the web based platform, often by specialist or resident in orthopedics [5], but may be registered by even less experienced physicians [6]. Registrations is optimally entered already in the emergency department, but subsequent treatments can be added later [6]. Details concerning the registration process are described in the Appendix.
Thoracic and lumbar fractures in the SFR are classified using a modified version of the 2013 version of AO spine injury classification (AOSpine classification) by Reinhold et al. [7]. The physician selects the fracture level, neurological function, and the type of fracture with the assistance of pictures and information by text. As opposed to the original classification, the SFR classification doesn’t distinguish between incomplete and complete burst fractures [8]. Compression fractures are divided in three categories: simple compression fractures (A1), pincer fractures (A2) and burst fractures (A3/4). The physician then asked to add whether there is a concomitant injury to the posterior tension band (B-type injury). Finally, the physician is asked to decide if there are signs of ankylotic spinal disorder in the fractured area. A detailed description of the modified AOSpine classification is available in the Appendix.
The flow chart of the study is presented in Fig. 1. In this study, patients with factors that influence the decision for or against operative treatment were excluded. These factors included injury to the spinal cord or cauda equina, open fractures, pathological fractures, fractures on multiple levels and low-energy injuries (defined as a fall from standing height or less). Patients were collected from the inception of spine fracture registrations in the SFR, starting in 2015, until February 2019.

Flow chart of the study
Patients with any type of medical imaging within two weeks from the time of injury, as well as before surgery for the operatively treated patients, were eligible for the study. Computed tomography (CT), magnetic resonance imaging (MRI) or conventional radiograph of the spine were collected from the treating hospitals. If more than one modality was available, CT and MRI were prioritized.
Medical imaging assessment
Medical images were reviewed and classified independently by two physicians (SB and FB) and by a third physician (PG) where disagreement on classification occurred. The radiographs were anonymized, and the reviewers only had information about the patient’s birthdate and treatment. No information about patient history, cause of injury, sex and the radiologist evaluation were available. The fracture level was identified, and the fracture type was classified according to the AOSpine classification by Reinhold et al. [7]. The three reviewers had different levels of experience (SB orthopedic resident with training in the AOSpine classification, FB specialist in orthopedic surgery and PG specialist in orthopedics and experienced spine surgeon). The combined results of the three reviewers were considered the gold standard.
Agreement
To evaluate the intra-rater reliability, the reviewers SB and FB assessed a subset of 52 patients, 3 to 6 months after the first classification. For assessing the inter-rater reliability between reviewers SB and FB the initial classification was used. Finally, the inter-rater reliability between the gold standard and the SFR classification was performed.
Statistics
Data are presented with means, medians, quantiles, minimum, maximum and standard deviations for continuous variables, and numbers and percentages for categorical variables. The intra- and inter-rater reliability was determined with percentages of agreement and weighted Cohen’s kappa. The reliability was interpreted using the criteria first proposed by Landis and Koch [9], with kappa coefficients of 0.0–0.2 representing slight reliability, 0.2–0.4 as fair, 0.4–0.6 as moderate, 0.6–0.8 as substantial, and > 0.8 as excellent. The positive predictive value (PPV) was calculated to determine the accuracy of the classifications. Comparisons were made based on experience of the registering physician, choice of treatment (operative vs. non-operative), and hospital type. Statistical significance was set to p < 0.05.
RStudio software version 4.1.0 for Windows (R Foundation for Statistical Computing) was used for all statistical analyses.
Results
Patients and descriptive data
The patient characteristics are summarized in Table 1.
Comparisons between the SFR classification and the gold standard classification are displayed in Table 2. The accuracy and agreement of the fracture level in comparison to the gold standard was excellent (95%). The number of A1 compression fractures misclassified as a burst fracture was significantly greater for non-operatively treated patients compared to operatively treated (25 (15%), 3 (3%) respectively). There was a significant difference in experience in registrations between operatively and non-operatively treated patients with the majority of operatively treated patients being registered by a spine surgeon (85%), while the non-operative patients were registered by physicians of varying level of experience.
Intra- and inter-rater reliability
The intra- and inter-rater reliability of the reviewers are presented in Table 3. The percentage of agreement comparing classifications made by the reviewers on different occasions were excellent (83 − 99%). The intra-rater reliability was substantial to excellent, with the exception for B type injuries for reviewer 2 which had fair reliability (kappa 0.28).
Third review assessment
Of the total of 277 patients, 71 patients were assessed by the third reviewer. 10 patients were reviewed due to disagreement on the fracture level. 47 patients were reviewed for disagreement in the classification of type A-injury. Among these, 19 cases were reviewed for disagreement whether there was a wedge compression (A1) or an incomplete burst fracture (A3), and 17 cases for whether there was an incomplete (A3) or a complete (A4) burst fracture. The remaining 11 cases had disagreement whether there was a simple compression (A1) or a pincer fracture (A2) (3 patients), wedge compression (A1) or a complete burst fracture (A4) (3 patients), a pincer fracture (A2) or a complete burst fracture (A4) (1 patient), a fracture that should not be classified as A-type (4 patients). 8 (of 277) patients were reviewed for disagreement in the classification of type B-injures.
The inter-rater reliability between reviewers and gold standard were substantial to excellent across all sub-classifications (Table 3).
Comparison between SFR and the gold standard
Accuracy
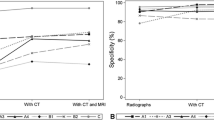
The accuracy determined by the PPV for correctly classifying patients having a burst fracture remained high regardless of the experience of the physician, for non-operatively and operatively treated patients and type of hospital (Table 4). However, the classification of B-type injuries was notably less accurate with PPV ranging from 0 to 40%.
Agreement between the SFR with the gold standard
The percentage of agreement and inter-rater reliability of the SFR classifications compared with the gold standard are summarized in Table 5. The estimation of Cohen’s kappa for A-type fractures was not possible for this dataset, as all reviewed fractures were determined to be burst fractures according to the SFR. The reliability of the fracture level was excellent (kappa 0.94). The reliability for B-type injuries were only slight (Cohen’s kappa 0.15). When ignoring the subtype of B injury, the reliability slightly improved (kappa 0.34). The overall reliability of the AOSpine classification with the SFR modification was slight (Cohen’s kappa 0.08) even when ignoring the subtype of B-injury registered (kappa 0.23). The inter-rater reliability did not change when analyzing subgroups by age, sex, treatment, registering physician or fracture severity (A3 vs. A4).
Discussion
The accuracy of correctly classifying a burst fracture in the SFR is excellent regarding level of fracture and type A injury regardless of the experience of the registering physician. However, the classification of B-type injuries in the SFR is far less reliable, with a significant number misclassification even among spine surgeons.
The SFR, being a national quality register that collects data on all types of orthopedic fractures, is a valuable resource for observational research on patients with thoracolumbar burst fractures to identify factors associated with treatment outcomes. Furthermore, as SFR expands to register-based randomized controlled trials, it is important that the classification of burst fractures is reliable [10]. The present study focused on investigating the reliability of classifications for thoracolumbar burst fractures in selected patients where both operative and non-operative options both are considered valid. This is a group of patients that may be registered and classified by physicians with a wide range of experience based on the local tradition of how they are usually treated.
The intra-rater and inter-rater reliability of the AOSpine classification as assessed by the reviewers in our study demonstrated substantial to excellent reliability. This is in accordance with previous reliability studies made on the classification system which have shown moderate to substantial reliability [11,12,13,14]. In a previous study by Morgonsköld et al., the reliability of spine fractures in the SFR was considered acceptable with moderate agreement [8]. In the study, physicians of varying experience levels were involved, all of whom had previous knowledge of the different classification systems used in the SFR, including AOSpine classification. Their gold standard was determined through the consensus of two experienced physicians and accuracy was measured using Cohen’s kappa. However, no direct comparison was made with the recorded classifications in the SFR. In practice, fractures may be registered by physicians without specific training in the classification systems being used.
Based on our results the likelihood that a burst fracture is correctly registered as a burst fracture in the SFR is high regardless of the level of experience in the registering physician. Although the percentage of agreement and PPV was high amongst all levels of experience, the number of simple compression fractures was substantially larger for non-operatively treated patients. Most registrations of operatively treated spine fractures were classified by surgeons themselves, whereas non-operatively treated spine fractures were registered by physicians of varying expertise, which explains the difference. In addition, the proportion of complete burst fractures (A4) compared to incomplete (A3) was higher in the operative group, which is also reasonable, as surgeons are likely to be more inclined to choose operative treatment options in patients with more severe fractures. Because the SFR classification do not distinguish between incomplete and complete burst fractures, simple comparisons between treatment groups may be erroneous, as the groups are not completely similar. The correct identification of complete burst fractures (A4) has been demonstrated to be challenging even among spine surgeons [14]. Consequently, opting not to separate burst fractures into incomplete and complete in the SFR is reasonable, considering the wide range of expertise among the registering physicians.
However, it is necessary to draw attention to the inter-rater reliability for B-type injuries, which was comparatively lower when comparing the gold standard with the classification in the SFR. Previous studies have shown that the inter-rater reliability of posterior tension band injuries tends to be lower compared to type A and C injuries [15,16,17]. Surprisingly, our study demonstrated an even lower level of reliability in this respect. A significant number of the fractures were misclassified as B1. This discrepancy may be explained by the accompanying textual descriptions with the pictures in the SFR that describes B1 as a “fracture through the vertebral body and rupture of the posterior tension band structures through bone” and B2 as “Rupture of the posterior tension band with or without skeletal injury”. It may not immediately apparent that a B1 fracture signifies a monosegmental osseous failure to a physician without knowledge of the classification system. This finding was also unexpectedly common for spine surgeons who should be familiar with the concept of the posterior tension band. According to our results, most physicians have registered any skeletal injury to the posterior structures of the lamina, including non-distraction type injuries such as vertical laminar fractures, as B-injuries. It should be noted that B3 type injuries according to the latest version of the AOSpine classification [16] is classified as C1 in the SFR classification, similarly to the classification presented by Reinhold et al. [7]. The absence of B3 injuries in our material can be explained by the fact that we excluded patients with ankylosing disorders given their increased likelihood of presenting with unstable fractures necessitating surgical fixation [18], and considering that the distinct injury mechanism associated with B3 injuries are primarily characterized by hyperextension [16] in contrast to axial compression for burst fractures [1].
To improve the reliability of B-type injury classifications in the SFR, we suggest that the register consider adding further choices with images depicting various types of fractures to the lamina, including vertical and horizontal spinous fractures. Additionally, it could prompt users to specify whether the horizontal spinous fracture is at the same level as the vertebral body fracture or not. These enhancements may help reduce misclassifications, ultimately improving the reliability of data collected in the SFR.
For thoracolumbar fracture to be reliably classified a CT is the imaging modality of choice [19]. In Swedish medical care where a fracture of the spine is considered a CT is the modality performed and conventional radiography has more or less become obsolete. The SFR doesn’t specify which imaging modality has been used for making the diagnosis. In our material most patients had undergone a CT, which was expected. 11 patients only had a conventional radiography. We chose to not exclude the patients with only conventional radiography as we aimed at determining the reliability of thoracolumbar burst fractures in the register. Excluding the cases with only a conventional radiography may have improved the reliability slightly. In 4 cases we only retrieved an MRI at the time of injury. In all 4 cases the patients underwent surgery and postoperative CT where available. We expect these cases to be patients from smaller hospitals that had been referred to the university hospital, although we have no possibility to verify this assumption. We chose to include these patients as the MRI was sufficient to determine whether a burst fracture was present or not, even though MRI is not the modality of choice determining skeletal injury [19].
In our study, most patients had not undergone an MRI within two weeks of injury. MRI plays an important role regarding soft tissue injuries and previous studies have shown that the classification of thoracolumbar fractures can change in 10 to 30% of cases [19,20,21,22,23]. The limited utilization of MRI may have implications for the accuracy of the true fracture classification, especially regarding B-type injuries although the clinical implications regarding a change in treatment with routine MRI are still questionable [19, 23].
Strengths
The collection of consecutive patients from multiple centers and comparison with the classifications made in the SFR by physicians of different levels of experience under real-life conditions constitute the strengths of this study.
Limitations
There are some limitations of this study that should be acknowledged. The cohort was prospectively collected but the analysis and classification of medical images was carried out retrospectively. We did not have clinical information about the patients, such as symptoms, levels of pain and comorbidities. Only burst fractures were collected and reviewed, which meant that the inter-rater reliability of A type injuries between the gold standard and SFR could not be made. We only reviewed selected patients where both operative and non-operative treatment are both valid options.
The patients identified for this study are likely to be only a fraction of the true number of patients in Sweden with a thoracolumbar burst fracture during this period. Since then, the coverage of SFR has increased SFR [6]. Despite this limitation, our study provides valuable insights to the SFR’s classification reliability of thoracolumbar burst fractures, emphasizing the need for further considerations in future research in this area.
Conclusions
The accuracy of classifying thoracolumbar burst fractures in the SFR is high regardless of the level of experience by the physician, treatment allocation and treating hospital. However, the inter-rater reliability of the AOSpine classifications of thoracolumbar burst fractures in the SFR is low when compared to reviewers with specific training in the classification system, particularly concerning B-type injuries. There are noticeable differences between operatively and non-operatively treated patients, and simple comparisons between treatments with data from the SFR without further review of medical images may lead to erroneous results. Future register-based studies on burst fractures with data from the SFR where classifications are of importance and when comparisons between operatively and non-operatively treated patients are made should include a review of medical images to verify the registered diagnosis.
Availability of data and materials
The data used for the analyses in this manuscript are available in the supplementary material.
Abbreviations
- CT:
-
Computed tomography
- MRI:
-
Magnetic resonance imaging
- PPV:
-
Positive predictive value
- SFR:
-
Swedish Fracture Register
References
Holdsworth F. Fractures, dislocations, and fracture-dislocations of the spine. J Bone Joint Surg Am. 1970;52(8):1534–51.
Wood KB, Li W, Lebl DR, Ploumis A. Management of thoracolumbar spine fractures. Spine J. 2014;14(1):145–64.
Möller M, Wolf O, Bergdahl C, Mukka S, Rydberg EM, Hailer NP, et al. The Swedish fracture register - ten years of experience and 600,000 fractures collected in a national quality register. BMC Musculoskelet Disord. 2022;23(1):141.
No authors listed. Fracture and dislocation compendium. Orthopaedic trauma association committee for coding and classification. J Orthop Trauma. 1996;10 Suppl 1:v-ix, 1–154.
Wennergren D, Ekholm C, Sandelin A, Möller M. The Swedish fracture register: 103,000 fractures registered. BMC Musculoskelet Disord. 2015;16:338.
Wennergren D, Möller M. Implementation of the Swedish fracture register. Unfallchirurg. 2018;121(12):949–55.
Reinhold M, Audigé L, Schnake KJ, Bellabarba C, Dai LY, Oner FC. AO spine injury classification system: a revision proposal for the thoracic and lumbar spine. Eur Spine J. 2013;22(10):2184–201.
Morgonsköld D, Warkander V, Savvides P, Wihlborg A, Bouzereau M, Möller H, et al. Inter- and intra-rater reliability of vertebral fracture classifications in the Swedish fracture register. World J Orthop. 2019;10(1):14–22.
Landis JR, Koch GG. The measurement of observer agreement for categorical data. Biometrics. 1977;33(1):159–74.
Blixt S, Mukka S, Försth P, Westin O, Gerdhem P. Study protocol: the SunBurst trial-a register-based, randomized controlled trial on thoracolumbar burst fractures. Acta Orthop. 2022;93:256–63.
Yacoub AR, Joaquim AF, Ghizoni E, Tedeschi H, Patel AA. Evaluation of the safety and reliability of the newly-proposed AO spine injury classification system. J Spinal Cord Med. 2017;40(1):70–5.
Schnake KJ, Schroeder GD, Vaccaro AR, Oner C. AOSpine classification systems (subaxial, thoracolumbar). J Orthop Trauma. 2017;31 Suppl 4:S14-s23.
Urrutia J, Zamora T, Yurac R, Campos M, Palma J, Mobarec S, et al. An independent interobserver reliability and intraobserver reproducibility evaluation of the new AOSpine thoracolumbar spine injury classification system. Spine (Phila Pa 1976). 2015;40(1):E54-58.
Kepler CK, Vaccaro AR, Koerner JD, Dvorak MF, Kandziora F, Rajasekaran S, et al. Reliability analysis of the AOSpine thoracolumbar spine injury classification system by a worldwide group of naïve spinal surgeons. Eur Spine J. 2016;25(4):1082–6.
Barcelos AC, Joaquim AF, Botelho RV. Reliability of the evaluation of posterior ligamentous complex injury in thoracolumbar spine trauma with the use of computed tomography scan. Eur Spine J. 2016;25(4):1135–43.
Vaccaro AR, Oner C, Kepler CK, Dvorak M, Schnake K, Bellabarba C, et al. AOSpine thoracolumbar spine injury classification system: fracture description, neurological status, and key modifiers. Spine (Phila Pa 1976). 2013;38(23):2028–37.
Kaul R, Chhabra HS, Vaccaro AR, Abel R, Tuli S, Shetty AP, et al. Reliability assessment of AOSpine thoracolumbar spine injury classification system and thoracolumbar injury classification and severity score (TLICS) for thoracolumbar spine injuries: results of a multicentre study. Eur Spine J. 2017;26(5):1470–6.
Westerveld LA, Verlaan JJ, Oner FC. Spinal fractures in patients with ankylosing spinal disorders: a systematic review of the literature on treatment, neurological status and complications. Eur Spine J. 2009;18(2):145–56.
Rajasekaran S, Vaccaro AR, Kanna RM, Schroeder GD, Oner FC, Vialle L, et al. The value of CT and MRI in the classification and surgical decision-making among spine surgeons in thoracolumbar spinal injuries. Eur Spine J. 2017;26(5):1463–9.
Leferink VJ, Veldhuis EF, Zimmerman KW, ten Vergert EM, ten Duis HJ. Classificational problems in ligamentary distraction type vertebral fractures: 30% of all B-type fractures are initially unrecognised. Eur Spine J. 2002;11(3):246–50.
Pizones J, Izquierdo E, Alvarez P, Sánchez-Mariscal F, Zúñiga L, Chimeno P, et al. Impact of magnetic resonance imaging on decision making for thoracolumbar traumatic fracture diagnosis and treatment. Eur Spine J. 2011;20 Suppl 3(Suppl 3):390–6.
Winklhofer S, Thekkumthala-Sommer M, Schmidt D, Rufibach K, Werner CM, Wanner GA, et al. Magnetic resonance imaging frequently changes classification of acute traumatic thoracolumbar spine injuries. Skeletal Radiol. 2013;42(6):779–86.
Aly MM, Al-Shoaibi AM, Abduraba Ali S, Al Fattani A, Eldawoody H. How Often Would MRI Change the Thoracolumbar Fracture Classification or Decision-Making Compared to CT Alone? Global Spine J. 2024;14(1):11–24.
Acknowledgements
We appreciate all patients and physicians contributing to the data collected in this study. We thank the case manager Jonas Lekander (Centre of Registers Västra Götaland) for the help acquiring data from the Swedish Fracture Register. We thank Christina Pettersson and Gül Kilickiran at the radiological department at Karolinska University Hospital in Huddinge for the help acquiring the images.
Funding
Open access funding provided by Uppsala University. The work for this study was funded by a grant from CIMED/Karolinska Institutet and the Swedish Research Council (number 2020 − 00493). Paul Gerdhem was supported by Uppsala University and Region Stockholm. The funding sources had no influence on this work.
Author information
Authors and Affiliations
Contributions
SB and FB reviewed all medical images. PG reviewed the cases where disagreement in classification occurred. SB wrote the main manuscript text, preparation of tables and figures. All authors contributed to the study concept and design, analysis of results and the reviewing of the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was conducted in accordance with the ethical principles of the Helsinki Declaration and was approved by the Swedish Ethical Review Authority (Approval No: 2021-00011). Consent from participants was waived by the Swedish Ethical Review Authority, as it is not necessary for this particular type of Swedish national quality register study. Following registration in the SFR, the patients are informed of their inclusion in the SFR and have the option to request the deletion of their registered information.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Blixt, S., Burmeister, F., Mukka, S. et al. Reliability of thoracolumbar burst fracture classification in the Swedish Fracture Register. BMC Musculoskelet Disord 25, 281 (2024). https://doi.org/10.1186/s12891-024-07395-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12891-024-07395-0