
Abstract
Purpose
To explore the effect of sarcopenia on recurrent fractures of adjacent vertebra after percutaneous kyphoplasty (PKP).
Methods
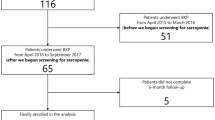
A total of 376 osteoporotic vertebral compression fractures (OVCFs) patients over 55 years old who were admitted to the Hospital from August 2020 to January 2021 were selected. Among them, 38 patients with recurrent fractures in adjacent vertebra after PKP were selected as the refracture group (RG), and the remaining 338 patients were selected as the non-refracture group (NRG). The age, gender, grip strength, body mass index (BMI), bone mineral density (BMD), visual analogue scale (VAS) of pain before and one month after surgery, Oswestry disability index (ODI) before and one month after surgery and the occurrence of sarcopenia were compared between the two groups. Logistic regression analysis was used to evaluate the effect of related risk factors on refracture after vertebral PKP.
Results
The results of t-test and Chi-square test showed that there were no obvious differences in gender, BMI, preoperative VAS score (t=-0.996, P = 0.320) and ODI (t=-0.424, P = 0.671), one month postoperative VAS score (t=-0.934, P = 0.355) and ODI score (t=-0.461, P = 0.645). while the age and grip strength showed significant differences between the two groups. Logistic regression analysis showed that BMI and gender had no significant effect on refracture after PKP, while sarcopenia and advanced age were independent risk factors for refracture after PKP. Also, increased BMD was a protective factor for refracture after PKP.
Conclusion
Sarcopenia is an independent risk factor for recurrent fractures after PKP in OVCF patients. The screening and diagnosis of sarcopenia should be strengthened. At the same time, anti-sarcopenia treatment should be actively performed after surgery.
Similar content being viewed by others


Background
With the development of the social economy and medical security system, the degree of aging is constantly developing, and the incidence of osteoporotic vertebral compression fractures also shows a trend of increasing [1]. At present, percutaneous kyphoplasty is usually the main method of treatment for osteoporotic vertebral compression fractures(OVCFs) patients. percutaneous kyphoplasty(PKP) can relieve symptoms, restore vertebral height and improve the prognosis. However, for patients with OVCF, PKP can only improve the diseased vertebrae, and restore the height of the vertebral body [2,3,4]; due to the loss of bone mass in patients, PKP is difficult to effectively prevent vertebra fractures adjacent to the diseased vertebrae. Therefore, refracture of adjacent vertebra after PKP is still an urgent problem to be solved [5]. Sarcopenia is a progressive and systemic disorder that primarily refers to the destruction of skeletal muscle shape and function, it is characterized by the loss of muscle mass and quantity, and leads to a number of adverse outcomes, including increased risk of falls, decreased limb function, physical weakness or even death [6]. Some researchers have pointed out that sarcopenia is closely related to the occurrence of osteoporosis [7, 8], so the effect of sarcopenia on refractures of adjacent vertebra in patients with OVCF deserves further investigation. This study is based on the study of patients with refractures of adjacent vertebra after PKP, and further explores the effect of sarcopenia on refractures of adjacent vertebra, in order to improve the prevention strategy of OVCF high-risk groups and prevent the occurrence of refractures.
Methods
1. This study retrospectively analyzed OVCF patients over 55 years old who were admitted to the First Affiliated Hospital of Soochow University from August 2020 to January 2021. This study was approved by the Ethics Committee of the First Affiliated Hospital of Soochow University. Inclusion criteria: 1)age ≥ 55 years; 2)Vertebral compression fracture (including instability of vertebral body, fresh fracture, delayed union) ; 3)patients with PKP; 4)BMD T value <-2.5SD; 5)refusal to stay in bed for conservative treatment; 6)no congenital lower limb deformity or dysfunction; Exclusion criteria: 1)patients with spinal cord injury; 2)vertebral fractures caused by violent violence; 3)neurological diseases affecting limb sensation and function; 4)severe cardiovascular or cerebrovascular diseases, and poorly controlled malignant hypertension; 5)diabetes with complications; 6)refusal of surgery or intolerance Recipients; 7)primary or metastatic tumors of the spine. According to the inclusion and exclusion criteria, a total of 376 patients were included in this study, and they were divided into 2 groups according to whether they had recurrent fractures after PKP. There were 38 cases in the refracture group (RG) and 338 cases in the non-refracture group (NRG). There were 71 males and 305 females. Their mean age was 70.37. Among them, 32 patients had confirmed diagnoses of sarcopenia in RG, and 145 patients in NRG were diagnosed as sarcopenia. Besides, all the patients have received anti-osteoporotic therapy, including the use of Calcium, vitamin D, denosumab and bisphosphonate since their first fracture.
Diagnostic criteria and surgery
Diagnosis
The diagnostic criteria for sarcopenia refer to the latest guidelines [6] recommended by the European Sarcopenia Working Group(EWGSOP) in 2019:grip strength :male<27 kg, female<16 kg; For the patients with reduced grip strength, we calculated the skeletal muscle indices (SMI), which sum measured by muscle area divided by the square of the patient’s height. Muscle area calculation method: On the CT image at the level of the pedicle of the thoracic 12 vertebrae, the measurement includes the erector spinae, latissimus dorsi, internal oblique, external oblique, rectus abdominis, external intercostal muscle and intercostal muscle (Fig. 1). The diagnostic value for SMI at the thoracic 12 level proposed by Nemec [9] et al.:<42.6cm2/m2(male) and<30.6cm2/m2(female). All data were independently measured by two physicians with more than 3 years of work experience. The patient’s grip strength and SMI value were both less than the diagnostic value to be diagnosed as sarcopenia, otherwise it was diagnosed as non-sarcopenia. The bone mineral density(BMD) was detected using dual-energy X-rays, we measured the bone density of L1-L4 and then averaged it.

Calculate the muscle area On the CT image at the level of the pedicle of the thoracic 12 vertebrae
Percutaneous kyphoplasty
After successful anesthesia and sterilization, we positioned the puncture point, and then hammered into the vertebra with the puncture needle; after the working cannula was placed; the balloons were also placed through the working cannula, then we expanded the balloon. After the bone cement was prepared, the balloon was taken out and push into the bone cement through the working cannula. X-ray showed that the bone cement was well distributed in the vertebra and the operation was completed.
Evaluation and follow-up
Basic information such as age, gender, height, weight, BMD and sarcopenia were recorded. The main indicators for evaluating the efficacy of surgery included: preoperative VAS [10, 11] score and ODI [12], postoperative VAS score and ODI one month after operation.
Statistics analysis
The t-test and Chi-square test was used to analyze the general conditions and surgery-related indicators of the patients in the refracture group and the non-refracture group. At the same time, logistic regression analysis was used to clarify the influence of gender, age, BMI, BMD and sarcopenia on refractures of adjacent vertebra after PKP.SPSS21(IBM Corp., Armonk, NY, USA) was used for statistical processing. Continuous variables were expressed as “mean ± standard deviation”, P < 0.05(★) was considered statistically significant, and “ns” was used to indicate that there is no statistical difference.
Results
-
1.
The results of t-test and Chi-square test showed that there were no obvious differences in gender(X2 = 0.264, P = 0.607) and BMI(t=-1.726,P = 0.085), while the age(t = 4.560,P = 0.001) and grip strength(t=-10.247,P = 0.001) showed significant differences between the two groups (Table 1). Besides, preoperative VAS score (t=-0.996, P = 0.320) and ODI (t=-0.424, P = 0.671), one month postoperative VAS score(t=-0.934, P = 0.355) and ODI score(t=-0.461,P = 0.645) (Table 1).
-
2.
Logistic regression analysis was performed on data such as gender, age, BMI, BMD, and sarcopenia (Table 2). The results showed that gender and BMI had no significant effect on refracture after PKP, while sarcopenia and advanced age were independent risk factors for refracture after PKP. Also, increased BMD was a protective factor for refracture after PKP (Fig. 2).

Results of the logistic regression analysis for sarcopenia, BMI, BMD, gender and age
-
3.
Here is a typical case. It was a woman who is 76 years old. Figure 3a and g showed her first OVCF in T12 before KP, and during her hospitalization, she was diagnosed as sarcopenia; Fig. 3h and i showed the Post-operative review results. Then Fig. 3j and p showed her second OVCF in T9 before the surgery, and Fig. 3q and r showed the follow-up results 3 months after the surgery (Fig. 3).

A typical case: a 76 years old women who was diagnosed as sarcopenia got OVCF twice within one year
Discussion
Sarcopenia was first proposed by Rosenberg [13] in the 1980s, it is a degenerative disease characterized by a decrease in the relative mass of skeletal muscle and decreased skeletal muscle strength. Sarcopenia currently occurs in 4.4-23% of people aged 65 and older worldwide [14,15,16]. According to the 2019 report of the Asian Sarcopenia Working Group (AWGS), the prevalence of sarcopenia in the elderly population in Asia is 5.5-25.7%, of which the prevalence of males is 5.1-21.0%, while the prevalence of females is 4.1 -16.3% [17]. In this study, we found that the BMI of sarcopenic patients is usually lower than that of non-sarcopenic patients, but there is no clear correspondence between them, that means patients with the same BMI may have a huge difference in SMI, which suggests that the skeletal muscle level of patients cannot be screened only by BMI.
Osteoporosis (OP) is the most common bone disease, which is mainly characterized by decreased bone mass, damage to the microstructure of bone tissue, increased bone fragility, and prone to fractures [18]. Common sites of osteoporotic fractures include vertebra, hip, distal forearm, proximal humerus, and pelvis, among which vertebra fractures are the most common [19]. For patients with OVCFs, PKP has become the first choice for many patients due to its rapid symptom relief, good vertebral height recovery, short operation time and lower price. In this study, the postoperative VAS and scores of the patients were significantly improved compared with those before the operation, which also confirmed the good effect of PKP on pain relief and functional recovery. However, since the patient’s osteoporosis has not been fundamentally improved, refractures of adjacent vertebra after PKP occur frequently. Nolan et al. also proposed that the occurrence of osteoporosis significantly increases the risk of recurrent fractures of adjacent vertebral bodies after PKP [20].
Since the concept of sarcopenia was proposed in 1989, researchers have gradually discovered the influence of metabolic factors, genetic factors and environmental factors on sarcopenia. Hirschfeld [21] et al. proposed that, based on the infiltration of adipose tissue into bone and muscle, obese patients usually need to consider the possibility of both osteoporosis and sarcopenia. The basic research on sarcopenia also pointed out that the relationship between bone and muscle not only has mechanical interaction, but also affects each other’s physiological processes through endocrine and paracrine pathways [22, 23]. This allows us to further understand the relationship between osteoporosis and sarcopenia. In the present study, sarcopenia was closely associated with refractures after PKP in OVCF patients. Of the 376 patients, 38 had recurrent fractures in adjacent vertebra after PKP. We performed logistic regression analysis on these 376 cases and found that sarcopenia significantly increased the risk of refractures in adjacent vertebra after PKP. Therefore, clinicians should pay attention to formulating an individualized plan for patients after PKP, strengthen the screening of sarcopenia, and concentrate on the supplementation of limb function exercise and nutritional diet. In this study, although we have analyzed some potential risk factors, the amount is limited. Some risk factors, such as claudication and history of glucocorticoid use, were needed a further comparison between two groups and a longer period of follow-up.
Conclusions
Sarcopenia is an independent risk factor for recurrent fractures after PKP in OVCF patients; it is necessary to strengthen the screening and diagnosis of sarcopenia. and perform anti-sarcopenia treatment after surgery, so as to reduce the risk of refractures.
Data availability
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- PKP:
-
percutaneous kyphoplasty
- OVCF:
-
osteoporotic vertebral compression fractures
- RG:
-
refracture group
- NRG:
-
non-refracture group
- BMI:
-
body mass index
- BMD:
-
bone mineral density
- VAS:
-
visual analogue scale
- ODI:
-
Oswestry disability index
- SMI:
-
skeletal muscle indices
References
Ling XU, Cummings SR, Mingwei Q et al. Vertebral Fractures in Beijing, China: The Beijing Osteoporosis Project.; 2000.
Ma XL, Xing D, Ma JX, Xu WG, Wang J, Chen Y. Balloon kyphoplasty versus percutaneous vertebroplasty in treating osteoporotic vertebral compression fracture: grading the evidence through a systematic review and meta-analysis. Eur Spine J. 2012;21(9):1844–59. https://doi.org/10.1007/s00586-012-2441-6.
Ko BS, Cho KJ, Park JW. Early adjacent vertebral fractures after balloon kyphoplasty for osteoporotic vertebral compression fractures. Asian Spine J. 2019;13(2):210–5. https://doi.org/10.31616/ASJ.2018.0224.
Liang L, Chen X, Jiang W, et al. Balloon kyphoplasty or percutaneous vertebroplasty for osteoporotic vertebral compression fracture? An updated systematic review and meta-analysis. Ann Saudi Med. 2016;36(3):165–74. https://doi.org/10.5144/0256-4947.2016.165.
Lee BG, Choi JH, Kim DY, Choi WR, Lee SG, Kang CN. Risk factors for newly developed osteoporotic vertebral compression fractures following treatment for osteoporotic vertebral compression fractures. Spine J. 2019;19(2):301–5. https://doi.org/10.1016/j.spinee.2018.06.347.
Cruz-Jentoft AJ, Bahat G, Bauer J, et al. Sarcopenia: revised European consensus on definition and diagnosis. Age Ageing. 2019;48(1):16–31. https://doi.org/10.1093/ageing/afy169.
Reiss J, Iglseder B, Alzner R, et al. Sarcopenia and osteoporosis are interrelated in geriatric inpatients. Z Gerontol Geriatr. 2019;52(7):688–93. https://doi.org/10.1007/s00391-019-01553-z.
Kirk B, Phu S, Brennan-Olsen SL, Bani Hassan E, Duque G. Associations between osteoporosis, the severity of Sarcopenia and fragility fractures in community-dwelling older adults. Eur Geriatr Med. 2020;11(3):443–50. https://doi.org/10.1007/s41999-020-00301-6.
Nemec U, Heidinger B, Sokas C, Chu L, Eisenberg RL. Diagnosing Sarcopenia on thoracic computed tomography: quantitative Assessment of skeletal muscle Mass in patients undergoing transcatheter aortic valve replacement. Acad Radiol. 2017;24(9):1154–61. https://doi.org/10.1016/j.acra.2017.02.008.
Bond MR, Pilowsky I. SUBJECTIVE ASSESSMENT OF PAIN AND ITS RELATIONSHIP TO THE ADMINISTRATION OF ANALGESICS IN PATIENTS WITH ADVANCED CANCER*. Vol 10.; 1966.
Heller GZ, Manuguerra M, Chow R. How to analyze the Visual Analogue Scale: myths, truths and clinical relevance. Scand J Pain. 2016;13:67–75. https://doi.org/10.1016/j.sjpain.2016.06.012.
Fairbank JCT, Pynsent PB. The Oswestry Disability Index. Vol 25.
Hankin JH. Development of a Diet History Questionnaire for Studies of Older Persons1-3. Vol 50.; 1989.
Trajanoska K, Schoufour JD, Darweesh SKL, et al. Sarcopenia and its clinical correlates in the General Population: the Rotterdam Study. J Bone Miner Res. 2018;33(7):1209–18. https://doi.org/10.1002/jbmr.3416.
Marty E, Liu Y, Samuel A, Or O, Lane J. A review of Sarcopenia: enhancing awareness of an increasingly prevalent disease. Bone. 2017;105:276–86. https://doi.org/10.1016/j.bone.2017.09.008.
Sánchez-Rodríguez D, Marco E, Ronquillo-Moreno N, et al. Prevalence of malnutrition and sarcopenia in a post-acute care geriatric unit: applying the new ESPEN definition and EWGSOP criteria. Clin Nutr. 2017;36(5):1339–44. https://doi.org/10.1016/j.clnu.2016.08.024.
Chen LK, Woo J, Assantachai P, et al. Asian Working Group for Sarcopenia: 2019 Consensus Update on Sarcopenia diagnosis and treatment. J Am Med Dir Assoc. 2020;21(3):300–307e2. https://doi.org/10.1016/j.jamda.2019.12.012.
Ensrud KE, Crandall CJ, Osteoporosis. Ann Intern Med. 2017;167(3):ITC17–ITC31. https://doi.org/10.7326/AITC201708010.
Siris ES, Adler R, Bilezikian J, et al. The clinical diagnosis of osteoporosis: a position statement from the National Bone Health Alliance Working Group. Osteoporos Int. 2014;25(5):1439–43. https://doi.org/10.1007/s00198-014-2655-z.
Nolan EK, Chen HY. A comparison of the Cox model to the Fine-Gray model for survival analyses of re-fracture rates. Arch Osteoporos. 2020;15(1). https://doi.org/10.1007/s11657-020-00748-x.
Hirschfeld HP, Kinsella R, Duque G. Osteosarcopenia: where bone, muscle, and fat collide. Osteoporos Int. 2017;28(10):2781–90. https://doi.org/10.1007/s00198-017-4151-8.
Tagliaferri C, Wittrant Y, Davicco MJ, Walrand S, Coxam V. Muscle and bone, two interconnected tissues. Ageing Res Rev. 2015;21:55–70. https://doi.org/10.1016/j.arr.2015.03.002.
Karsenty G, Olson EN. Bone and muscle endocrine functions: unexpected paradigms of inter-organ communication. Cell. 2016;164(6):1248–56. https://doi.org/10.1016/j.cell.2016.02.043.
Acknowledgements
Not applicable.
Funding
This work was supported by Suzhou Science and Technology Plan Project-Medical Devices and New Medicine (Clinical Trials)-Medicine-Industrial Collaborative Innovation Research Project “Study on clinical test method of robotic positioning system for minimally invasive spine surgery“(SLJ201902).
Author information
Authors and Affiliations
Contributions
JCN designed this study; WHZ and LP collected the data; JCN and WHZ made the statics analysis and wrote the manuscript; All authors reviewed the final manuscript. All authors agreed to be accountable for all aspects of the work. The author(s) read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was approved by the Medical Research Ethics Committee of the First Affiliated Hospital of Soochow University. This research was conducted in full compliance with the codes of ethical conduct from the Declaration of Helsinki. Written informed consent were obtained from the patients before they were enrolled in the study.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Jing, C., Wang, H., Liu, P. et al. Effect of sarcopenia on refractures of adjacent vertebra after percutaneous kyphoplasty. BMC Musculoskelet Disord 25, 210 (2024). https://doi.org/10.1186/s12891-024-07295-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12891-024-07295-3