
Abstract
Objective
Osteoarthritis (OA) of the knee is one of the most common global joint disorders, especially in aging population, and is among leading health-related concerns of societies. Therefore, this systematic review and meta-analysis was done to investigate the results related to the effects of exercise interventions on knee repositioning sense in patients with knee OA.
Methods
An extensive search was independently performed in electronic databases including PubMed, MEDLINE, Web of Science, SCOPUS, and Google Scholar, to identify randomized clinical trials (RCTs) conducted on knee OA and to evaluate knee repositioning sense before and after different exercise interventions. After extracting relevant data from eligible studies, results of the studies were pooled using a random-effects model of meta-analysis. The Physiotherapy Evidence Database (PEDro) of clinical trials was used for quality assessment of eligible studies.
Results
Among 2702 studies identified in the initial search, 17 studies were eligible for final systematic review and meta-analysis. The results showed that the patients who participated in different exercise interventions had significantly less knee repositioning error (mean differences: -1.141 degrees (95%CI: -1.510, -0.772, P < .001) compared to those who did not undergo exercise interventions. The eligible studies exhibited publication bias (Intercept: -6.69, P = .002), and the data showed significant heterogeneity (I2 = 85.633%, Q = 153.125, P < .001). Moreover, meta regression showed more prolonged exercise duration might have more effects on knee repositioning error (Coefficient=-0.860, 95% CI=-1.705, -0.016, Z=-2.00, P = .045).
Conclusion
There is strong evidence that exercise interventions may effectively reduce knee repositioning error. Moreover, it seems that more prolonged exercise duration may be associated with the greater effect size.
Similar content being viewed by others


Introduction
Osteoarthritis (OA) is one of the most common global joint disorders, especially in aging population, and is among leading health-related concerns in different communities [1]. In addition, financial burden of this disease has been estimated around tens of billions of dollars for governments to cure and tackle disease’s substantial consequences [2]. Knee OA is accompanied by various physical symptoms including pain, joint stiffness, limitations in physical activities, and loss of joint mobility [3]. It seems that, the OA patients’ walking quality and speed will be adversely influenced, and they will face with difficulties in ascending stairs and standing up from a chair [4]. In order to reduce the complications, several approaches are suggested for management of patients with knee OA [3, 5, 6]. Some of them include surgical approaches, such as arthroscopy and osteotomy and joint-replacement procedures [7]. There are also non-surgical treatments like orthotic devices [8] and improving individual’s lifestyle [3], of which exercise-based interventions are believed to play an essential role in management of patients with knee OA [9,10,11]. On the other hand, it seems that impaired proprioceptive sense of the knee may be present in patients with knee OA as well [12].
Proprioception plays a critical role in keeping humans҆ balance and movement control during daily activities. Any flaws in proprioceptive function may cause balance problems, leading to an increased risk of falling (9). It had been shown that different bodily processes, including muscular, sensory, cognitive, and psychosocial ones, change with aging. So, the loss of proprioceptive function is associated with aging in human beings [13]. Age-related loss of proprioception may alter the neuromuscular control of the limbs and the biomechanics of joints, impairing balance and increasing the risk of falls [3]. Moreover, it seems that the age-related loss of proprioception can be slowed by appropriate and proper physical activity [14]. In this line, some evidence suggests that knee repositioning sense may be impaired in patients with knee Osteoarthritis OA [12], and participating in exercise protocols may improve it (15). Previous studies have evaluated the effects of different exercise protocols on proprioceptive functions in patients with knee OA like Tai-chi and Baduanjin Qigong [16,17,18], balance and proprioceptive-based exercises [19,20,21,22], sensorimotor exercises [15, 23], computer-based exercises [24], Pilates [25], and different kinds of strengthening protocols [22, 26,27,28].
Previous studies have shown that exercise protocols may positively influence knee repositioning sense in patients with knee OA; however, there are controversial results regarding effectiveness of some exercise protocols [26, 29, 30]. So, it seems that running a systematic review with pooled meta-analysis would clarify strength regarding the effect of such exercises on repositioning sense in patients with knee OA. Therefore, this systematic review and meta-analysis was done to investigate the results on the effect of exercise interventions on knee repositioning sense in patients with knee OA.
Materials & methods
Search strategy of the literature
This study conducted in accordance with PRISMA guidelines [31]. The database of abstracts of reviews of effects (DARE) and the Cochrane Library were searched to find any systematic review and meta-analysis on this topic, but no systematic review and meta-analysis was found. Two independent investigators (MD and RS) performed an extensive review in electronic databases including PubMed, MEDLINE, Web of Science, and SCOPUS, and Google Scholar. A combination of the following keywords was used to search in the databases: [1] “sense of position”, “position sense”, repositioning, proprioception, [2] knee, hip, “lower extremity”, [3] osteoarthritis, osteoarthrosis, “degenerative joint disease”, and DJD. The “AND” and “OR” operators were used for between and within keyword groups, respectively. The search was performed from inception to 27 December 2022. All the searched citations with their abstracts were imported to the EndNote X7 software for more detailed checks.
Selection criteria
Both reviewers (MD and RS) assessed the studies with respect to inclusion criteria. Only clinical trials that had administered any exercise training type for knee repositioning sense in the patients with knee OA were selected by screening titles and abstracts of the searched citations. Then, data on trial design and outcomes were extracted and summarized in a table. Any disagreements were resolved by consensus. The full texts of potentially eligible studies were retrieved and reviewed to determine whether they meet the inclusion criteria.
Only clinical trials that had been published in English peer-reviewed journals and had control groups were selected. There was no limitation about type of exercise training used or measurement tool to assess knee repositioning sense. Studies could be included regardless of repositioning sense being the primary or secondary outcome. Studies that had not included exercise groups or those that had combined exercise training with other interventions, such as manual therapy were excluded from the present research. The control group should not have performed exercise training, so studies, in which the control group had received no treatment or conventional treatments, were included. If any study had reported different measures for repositioning sense (e.g., different test angles, passive or active movements), the test results reporting the largest knee flexion range of motion -between 60 and 90 degrees- and active movements were only selected for data synthesis. No criterion was considered in terms of evaluation method and tests of the studies.
Data extraction
The data extracted from eligible studies are summarized in Table 1. Table 1 shows the information including the first author names and years of publication, general characteristics of participants, available information about interventions and groups of study, quality assessment score of each study, the main utilized tools and methods, and the main results of the retrieved studies. The aim of the current study was to examine the effect of various exercise protocols on knee reposition sense.
Quality assessment and level of evidence
The Physiotherapy Evidence Database (PEDro) of clinical trials and its guidelines were used for quality assessment of eligible studies. According to Sackett et al., level of evidence was also determined [32].
Statistical analysis
The relevant data were extracted from eligible studies (including pretest and posttest means and standard deviations, P-values, sample sizes, and also possible mean differences and standard deviations). Then, results of the studies were pooled using a random-effects model of meta-analysis and the forest plot of the standard differences in means and estimated standardized Hedge’s g effect size with 95% confidence interval (CI). Q-test was applied to investigate data heterogeneity, while I2 was used to determine magnitude of possible data heterogeneity. In the case of data heterogeneity, meta-regression was run to identify the potential effect of exercise duration on meta-analysis results. Both funnel plot and Egger’s tests were used to check publication bias. The trim-and-fill method was used to evaluate the effect of adding possible random studies on the results if needed. Statistical analysis was performed using comprehensive meta-analysis (CMA) software version 3.0 (Biostat Inc, Englewood, New Jersey).
Results
Search results
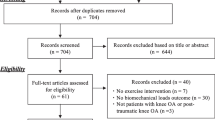
A total of 2702 studies were found in the initial search. Nine hundred eighty-one duplicated citations were removed from the list. After reviewing abstracts/titles, 1681 studies did not meet the inclusion criteria, so they were excluded from the study. Then, the full texts of 40 studies were assessed in more detail. Again, 22 studies did not also meet the inclusion criteria.
Moreover, 5 studies had provided no sufficient data to be included in the study. Also, 4 studies were eligible for analysis from other sources including eligible studies obtained from citations and searches through Google Scholar database. Finally, 17 studies were selected to enter meta-analysis (Fig. 1). The information of eligible studies is summarized in Table 1.

Flow diagram for eligible studies
Study characteristics
Duration of the prescribed exercises ranged from 3 to 24 weeks, with 2–5 exercise sessions per week. Several types of exercise training had been prescribed in the studies including 3 studies on Thai-Chi and Baduanjin Qigong [16,17,18], 4 studies on proprioceptive exercises [19,20,21,22], 6 studies on resistance and strength training exercises [22, 26,27,28], 2 studies on sensorimotor training [15, 23], one study on Pilates [25], one study on aquatic therapy [33], one study on computer-based exercise [24], one study on backward walking [34], one study on proprioceptive neuromuscular facilitation [35], and 3 studies on other exercises including conventional therapeutic exercises, electromyographic (EMG) biofeedback, and a combination of EMG biofeedback and isokinetic exercises [25, 26]. Totally, 17 eligible studies had included 847 participants, as shown in Table 1.
Description of the selected variables
Criteria for diagnosis of DJD of the Knee: Overall, 15 studies had used x-ray to evaluate knees [15,16,17,18,19,20,21,22, 24,25,26,27,28, 34, 35], and 2 studies had used clinical presentations only [23, 33]. Regarding knee OA severity, eligible studies recruited patients with different degrees of knee OA based on the Kellgren Lawrence scoring system. Patients with Grades 1–3 of knee OA had been examined in 5 studies [17, 22, 24, 27, 35], patients with Grades 2 and 3 of knee OA had been examined in 4 studies [15, 18, 19, 26], one study had investigated patients with Grades 3 and 4 of knee OA [20], one study had investigated patients with Grade 4 or lower of knee OA [25], one research had studied patients with Grade 4 of knee OA [21], one study studied the participants with at least grade 1 of OA [34], and 2 studies had not reported degree of knee OA [28, 33].
Knee repositioning error had been assessed using several tools including electronic goniometer in 3 studies [21, 22, 24], the CYBEX computerized dynamometer in one study [19], a custom-made JOBST air splint in one study [28], the Biodex system in one study [25], the Biodex 4 isokinetic device in one study [26], the shuttle mini-clinic device in one study [27], the CYBEX-NORM dynamometer in one study [20], the Prokin system in two studies [18, 34], the Biodex 3 pro-multi-joint isokinetic dynamometer in one study [23], Proprioception test devices [35], and the biometrics electro goniometer in one study [16].
Data synthesis
In this meta-analysis study, meta-analysis was run using the standardized mean differences between intervention and control groups calculated in beginning and end of the exercise protocols for knee repositioning sense.
Knee repositioning sense
Meta-analysis was performed on 17 eligible studies [15,16,17,18,19,20,21,22,23,24,25,26,27,28, 33,34,35] that had obtained data on knee repositioning sense among a total of 847 participants with knee OA. The pooled estimated standard difference was − 1.141 degrees (95%CI: -1.510, -0.772, P < .001). The results showed that the patients who participated in different exercise protocols had significantly less knee repositioning error than control groups (Fig. 2). A funnel plot was used to assess the presence of the possible publication bias. Also, value of Egger’s test was significant (Intercept: -6.69, P = .002). The trim- and- fill method was used to investigate the effect of adding possible random publications to right side of the plot. The results showed that the main finding did not change, so it seems that publication bias might have no apparent effect on meta-analysis results (Fig. 3). Furthermore, significant heterogeneity was observed in data (I2 = 85.633%, Q = 153.125, P < .001).
Possibly, the presence of data with high levels of heterogeneity may be attributed to different durations of the studies; so, meta-regression was run by adding the number of exercise training weeks as a covariate in meta-analysis. The results showed that the regression model was significant, and more prolonged exercise duration might have more effects on knee repositioning error (Coefficient=-0.860, 95% CI=-1.705, -0.016, Z=-2.00, P = .045). No significant associations were found between age, BMI, and OA severity variables and the effect size of exercise training in Meta regression to report (P > .05). The regression model is illustrated in Fig. 4.
As there were 6 high–quality studies [16,17,18, 21, 22, 27] showing the positive effects of exercise training on knee repositioning sense, strong evidence was assigned to this finding.

Forest plot regarding the effect of exercise on knee repositioning sense (favors A: Exercise, favors B: Control). CI: Confidence interval

Funnel plot assessing the presence of publication bias in meta-analysis for knee repositioning sense. White-filled circles indicate the observed studies, while the gray-filled circles show the imputed studies

Meta-regression results that show longer exercise duration may have more effects on knee repositioning error
Discussion
To the best of our knowledge, this study is the first systematic review and meta-analysis regarding the effect of different exercise interventions on knee repositioning sense in patients with knee OA. The results showed a strong evidence indicating that exercise intervention may be effective to decrease knee repositioning error (SD mean differences-1.141 degrees (95%CI: -1.510, -0.772, P < .001)).
According to our results, different exercise interventions can decrease knee repositioning sense in patients with knee OA. Moreover, it seems that more prolonged exercise duration may be associated with the greater effect size. It has been shown that mechanoreceptor contents of the knee meniscuses and ligaments are decreased in patients with knee OA [36]. On the other hand, knee repositioning sense not only relies on joint mechanoreceptors but also on periarticular tissues, such as tendons, capsules, and muscles [9]. So, it seems that an improvement in knee repositioning sense might result from muscle and neurophysiological adaptations to mechanical loadings [4] of different exercise regimens. Also, it appears that with more prolonged exercise duration, the body may have more chance to adapt to exercise [37], so showing the greater effect sizes in knee repositioning sense. Furthermore, our finding demonstrated that the effects of exercise therapy on proprioception was irrespective of age, BMI and OA severity. Generally, it seems that participating in any exercise program may improve knee repositioning sense in patients with knee OA of various ages, BMIs, or OA severity.
With regard to the existing heterogeneity among the eligible studies, as mentioned in the methods section, different tools were used for examining knee reposition sense. But the scale of all of them was in degrees. So standard differences in means were used to pool data. But the accuracy and reliability of various tools are different in examining the knee repositioning sense [38,39,40]. On the other hand, various exercise protocols were prescribed in eligible studies. We should remember that various exercises may have different impacts on knee repositioning sense in knee OA patients. Moreover, the participants had OA of varying severity. It is also to be expected that the different severity of the disease may impact the change in joint reposition sense. Accordingly, it seems that the different measurement tools and the prescribed exercises may result in heterogeneity among eligible studies.
The findings of this study should be evaluated with respect to several limitations. Firstly, the study included only original papers in English peer-reviewed journals. Here, a strong level of evidence was found regarding the positive effects of exercise therapy on knee repositioning sense. Still, high levels of data heterogeneity highlight the need for caution in generalizing and interpreting these results to all forms of exercise or all exercise durations. This study protocol has not been prospectively registered in advance in any registration database. Finally, the eligible studies were included regardless of repositioning sense being the primary or secondary outcome, so it should be remembered that included studies are not being powered to show improvement in repositioning sense.
Conclusion
The results showed strong evidence stating that exercise intervention might reduce knee repositioning error. Moreover, it seems that more prolonged exercise duration may be associated with the greater effect size. Because of high levels of data heterogeneity among the reviewed studies, more studies are needed to clarify the effects of different types of exercise or durations on patients with knee OA.
Data Availability
The datasets generated and analysed during the current study are available in the supplementary file 1 in the journal.
References
Spitaels D, Mamouris P, Vaes B, Smeets M, Luyten F, Hermens R, et al. Epidemiology of knee osteoarthritis in general practice: a registry-based study. BMJ open. 2020;10(1):e031734–e. https://doi.org/10.1136/bmjopen-2019-031734. PubMed PMID: 31964664.
Abbott H, Wilson R. The projected burden of knee osteoarthritis in New Zealand: healthcare expenditure and total joint provision-a response. N Z Med J. 2020;133(1509):77–8. Epub 2020/02/07. PubMed PMID: 32027642.
Ferlinc A, Fabiani E, Velnar T, Gradisnik L. The importance and role of Proprioception in the Elderly: a short review. Materia socio-medica. 2019;31(3):219–21. https://doi.org/10.5455/msm.2019.31.219-221. Epub 2019/11/26.
Basso JC, Suzuki WA. The Effects of Acute Exercise on Mood, Cognition, Neurophysiology, and Neurochemical Pathways: A Review. Brain Plasticity. 2017;2:127–52. https://doi.org/10.3233/BPL-160040.
Song Q, Shen P, Mao M, Sun W, Zhang C, Li L. Proprioceptive neuromuscular facilitation improves pain and descending mechanics among elderly with knee osteoarthritis. 2020;30(9):1655–63. https://doi.org/10.1111/sms.13709. PubMed PMID: 32407583.
Fischer AG, Erhart-Hledik JC, Asay JL, Andriacchi TP. Intermittent vibrational stimulation enhances mobility during stair navigation in patients with knee pain. Gait Posture. 2021;86. https://doi.org/10.1016/j.gaitpost.2021.03.013. Epub 2021/03/16. :125 – 31.
Chen L, Duan X, Xing F, Liu G, Gong M, Li L, et al. Effects of pulsed electromagnetic field therapy on pain, stiffness and physical function in patients with knee osteoarthritis: a systematic review and meta-analysis of randomized controlled trials. J Rehabil Med. 2019;51(11):821–7. Epub 2019/10/05. PubMed PMID: 31583420.
Farrokhi S, Jayabalan P, Gustafson JA, Klatt BA, Sowa GA, Piva SR. The influence of continuous versus interval walking exercise on knee joint loading and pain in patients with knee osteoarthritis. Gait Posture. 2017;56:129–33. https://doi.org/10.1016/j.gaitpost.2017.05.015. Epub 05/17. PubMed PMID: 28544950.
Tuthill JC, Azim E, Proprioception. Curr Biol. 2018;28(5):R194–R203. https://doi.org/10.1016/j.cub.2018.01.064.
de Zwart AH, Dekker J. High-intensity versus low-intensity resistance training in patients with knee osteoarthritis: a randomized controlled trial. 2022;36(7):952–67. https://doi.org/10.1177/02692155211073039. PubMed PMID: 35331018.
Babur MN, Siddiqi FA, Tassadaq N, Arshad Tareen MA, Osama M. Effects of glucosamine and chondroitin sulfate supplementation in addition to resistance exercise training and manual therapy in patients with knee osteoarthritis: a randomized controlled trial. JPMA The Journal of the Pakistan Medical Association. 2022;72(7):1272–7. https://doi.org/10.47391/jpma.2444. Epub 2022/09/27.
van Tunen JA, Dell’Isola A, Juhl C, Dekker J, Steultjens M, Thorlund JB et al. Association of Malalignment, muscular dysfunction, proprioception, laxity and abnormal joint loading with tibiofemoral knee Osteoarthritis-A systematic review and Meta-analysis. 2018.
Henry M, Baudry S. Age-related changes in leg proprioception: implications for postural control. J NEUROPHYSIOL. 2019;122(2):525 – 38. https://doi.org/10.1152/jn.00067.2019. PubMed PMID: 31166819.
Ribeiro F, Oliveira J. Aging effects on joint proprioception: the role of physical activity in proprioception preservation. Eur Rev Aging Phys Activity. 2007;4(2):71–6. https://doi.org/10.1007/s11556-007-0026-x.
Tsauo J, Cheng P, Yang R. The effects of sensorimotor training on knee proprioception and function for patients with knee osteoarthritis: a preliminary report. Clin Rehabil. 2008;22(5):448.
Schmid A, McAlindon T, Schmid CH, Wang C. The influence of Tai Chi exercise on proprioception in patients with knee osteoarthritis: results from a pilot randomized controlled trial. Int J Integr Med. 2013;1.
Zhu QQ, Huang LY, Li JX, Mao LJ, Zhang YY, Min F, et al. Effect of Taijiquan practice versus wellness education on knee proprioception in patients with knee osteoarthritis: a randomized controlled trial. J Tradit Chin Med. 2017;37(6):774–81. PubMed PMID: WOS:000423497600006.
Ye JJ, Simpson MW, Liu Y, Lin W, Zhong WH, Cai SH, et al. The Effects of Baduanjin Qigong on Postural Stability, Proprioception, and symptoms of patients with knee osteoarthritis: a Randomized Controlled Trial. Front Med. 2020;6. https://doi.org/10.3389/fmed.2019.00307. PubMed PMID: WOS:000509281600001.
Sekir U, Gür H. A multi-station proprioceptive exercise program in patients with bilateral knee osteoarthrosis: functional capacity, pain and sensoriomotor function. A randomized controlled trial. J Sports Sci Med. 2005;4(4):590–603. Epub 2005/12/01. PubMed PMID: 24501572; PubMed Central PMCID: PMCPmc3899676.
Duman I, Taskaynatan M, Mohur H, Tan A. Assessment of the impact of proprioceptive exercises on balance and proprioception in patients with advanced knee osteoarthritis. Rheumatol Int. 2012;32(12):3793.
Kumar S, Kumar A, Kumar R. Proprioceptive training as an adjunct in osteoarthritis of knee. J Musculoskelet Res. 2013;16(1). https://doi.org/10.1142/S0218957713500024.
Lin DH, Lin CHJ, Lin YF, Jan MH. Efficacy of 2 non-weight-bearing interventions, proprioception training versus strength training, for patients with knee osteoarthritis: a randomized clinical trial. J ORTHOP SPORTS PHYS THER. 2009;39(6):450–7. https://doi.org/10.2519/jospt.2009.2923.
Ahmed AF. Effect of sensorimotor training on balance in elderly patients with knee osteoarthritis. J Adv Res. 2011;2(4):305–11. https://doi.org/10.1016/j.jare.2011.02.001.
Jan M, Tang P, Lin J, Tseng S, Lin Y, Lin D. Efficacy of a target-matching foot-stepping exercise on proprioception and function in patients with knee osteoarthritis. J Orthop Sports Phys Ther. 2008;38(1):19.
Mazloum V, Rabiei P, Rahnama N, Sabzehparvar E. The comparison of the effectiveness of conventional therapeutic exercises and pilates on pain and function in patients with knee osteoarthritis. Complement Ther Clin Pract. 2018;31:343–8. Epub 2018/10/15. https://doi.org/10.1016/j.ptsp.2018.10.001. https://doi.org/10.1016/j.ctcp.2017.10.008. PubMed PMID: 29108873.
Raj NB, Saha S, Saha S, Razali H, Othman NYH, US MR. Does Proprioception of knee improve after various forms of training in osteoarthritis of knee? Res J Pharm Technol. 2019;12(9):4379–86.
Jan M, Lin C, Lin Y, Lin J, Lin D. Effects of weight-bearing versus nonweight-bearing exercise on function, walking speed, and position sense in participants with knee osteoarthritis: a randomized controlled trial. Arch Phys Med Rehabil. 2009;90(6):897.
Topp R, Pifer M. A preliminary study into the effect of 2 resistance training modes on proprioception of subjects with knee osteoarthritis. 2017.
Miller KJ, Mesagno C, McLaren S, Grace F, Yates M, Gomez R, Exercise. Mood, Self-Efficacy, and Social Support as Predictors of depressive symptoms in older adults: Direct and Interaction Effects. Front Psychol. 2019;10(2145). https://doi.org/10.3389/fpsyg.2019.02145.
Bieler T, Siersma V, Magnusson SP, Kjaer M, Beyer N. Exercise induced effects on muscle function and range of motion in patients with hip osteoarthritis. Physiother Res Int. 2018;23(1). https://doi.org/10.1002/pri.1697. PubMed PMID: 28971551. Epub 2017/10/04.
Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. https://doi.org/10.1136/bmj.n71.
Sackett DL, Straus SE, Richardson WS, Rosenberg W, Haynes RB. Evidence-based medicine: how to practice and teach EBM (Straus, evidence-based medicine). Volume 2. ed: Edinburgh and London: Churchill Livingstone; 2000.
Hale L, Waters D, Herbison P. A randomized controlled trial to investigate the effects of water-based exercise to improve falls risk and physical function in older adults with lower-extremity osteoarthritis. Arch Phys Med Rehabil. 2012;93(1):27.
Chen Z, Ye X, Wang Y, Shen Z. The efficacy of Backward walking on Static Stability, Proprioception, Pain, and physical function of patients with knee osteoarthritis: a Randomized Controlled Trial. 2021;2021:5574966. https://doi.org/10.1155/2021/5574966. PubMed PMID: 34221078.
Shen P, Li L, Song Q, Sun W, Zhang C, Fong DTP, et al. Proprioceptive neuromuscular facilitation improves symptoms among older adults with knee osteoarthritis during Stair Ascending: a Randomized Controlled Trial. Am J Phys Med Rehabil. 2022;101(8):753–60. https://doi.org/10.1097/phm.0000000000001906. Epub 2021/10/24.
Hassan BS, Mockett S, Doherty M. Static postural sway, proprioception, and maximal voluntary quadriceps contraction in patients with knee osteoarthritis and normal control subjects. Ann Rheum Dis. 2001;60(6):612–8. https://doi.org/10.1136/ard.60.6.612. PubMed PMID: 11350851.
Arribat Y, Broskey NT, Greggio C, Boutant M, Alonso SC, Kulkarni SS, et al. Distinct patterns of skeletal muscle Mitochondria Fusion, Fission and Mitophagy upon Duration of Exercise Training. Acta Physiologica (Oxford England). 2019;225(2):e13179.
Busch A, Bangerter C, Mayer F, Baur H. Reliability of the active knee joint position sense test and influence of limb dominance and sex. Sci Rep. 2023;13(1):152. https://doi.org/10.1038/s41598-022-26932-2.
Romero-Franco N, Montaño-Munuera JA, Fernández-Domínguez JC, Jiménez-Reyes P. Validity and reliability of a Digital Inclinometer to assess knee joint position sense in an Open Kinetic Chain. J Sport Rehabil. 2019;28(4):332–8. https://doi.org/10.1123/jsr.2017-0221. Epub 2017/12/19.
Jebreen M, Sole G, Arumugam A. Test-retest reliability of a Passive Joint position sense Test after ACL Reconstruction: influence of Direction, Target Angle, Limb, and Outcome Measures. Orthop J Sports Med. 2023;11(3):23259671231157351. PubMed PMID: 36970320; PubMed Central PMCID: PMCPmc10034299.
Acknowledgements
Not Applicable.
Funding
No funding was obtained for this study
Author information
Authors and Affiliations
Contributions
RS, MD, HP, SS and MS contributed to study design and data collection. MD, RS, HP and MS drafted the manuscript and made critical revisions to the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval, guidelines and consent to participate
Not Applicable.
Consent for publication
Not Applicable.
Competing interests
There is no conflict of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Sheikhhoseini, R., Dadfar, M., Shahrbanian, S. et al. The effects of exercise training on knee repositioning sense in people with knee osteoarthritis: a systematic review and meta-analysis of clinical trials. BMC Musculoskelet Disord 24, 592 (2023). https://doi.org/10.1186/s12891-023-06712-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12891-023-06712-3