
Abstract
Introduction
Low back pain (LBP) is a key social, economic, and public health problem in the world. The impact of LBP is given less priority and is empirically unrepresented in low- and middle-income countries as a result of the focus on more pressing and life-threatening health issues, including infectious diseases. In Africa, the prevalence of LBP is irregular and increasing among schoolteachers on account of teaching activities performed under suboptimal working conditions. Therefore, the objective of this review was to estimate the pooled prevalence and associated factors of LBP among school teachers in Africa.
Methods
This systematic review and meta-analysis was designed based on the PRISMA guidelines. A comprehensive systematic literature search focused on LBP in African school teachers was conducted using the PubMed/MEDLINE, CINAHL, and CABI databases, regardless of publication timelines, from October 20 to December 3, 2022. In addition, gray literature was searched using Google Scholar and Google Search. Data were extracted in Microsoft Excel by using the JBI data extraction checklist. The overall effect of LBP was estimated using a random effect model via DerSimonian-Laird weights. The pooled prevalence and odds ratio of associated factors with 95% CI were computed using STATA 14/SE software. The I2 test and Egger’s regression test were used to assess heterogeneity and publication bias, respectively.
Results
A total of 585 articles were retrieved, and 11 eligible studies involving a total of 5,805 school teachers were included in this systematic review and meta-analysis. The overall estimated pooled prevalence of LBP in African school teachers was found to be 59.0% (95% CI: 52.0%–65.0%). Being female [POR: 1.53; 95% CI (1.19, 1.98)], being older [POR: 1.58; 95% CI (1.04, 2.40)], being physically inactive [POR: 1.92; 95% CI (1.04, 3.52)], having sleep problems [POR: 2.03; 95% CI (1.19, 3.44)] and having a history of injury [POR: 1.92; 95% CI (1.67, 2.21)] were factors significantly associated with LBP.
Conclusions
The pooled prevalence of LBP was high among school teachers in Africa compared to developed nations. Sex (female), older age, physical inactivity, sleep problems, and a history of previous injury were predictors of LBP. It is suggested that policymakers and administrators ought to gain awareness of LBP and its risk factors to put existing LBP preventive and control measures into action. Prophylactic management and therapeutic strategies for people with LBP should also be endorsed.
Similar content being viewed by others

Introduction
Low back pain (LBP) is defined as pain or discomfort from the region of the twelfth (12th) rib to the region of the inferior gluteal folds, with or without accompanying leg pain [1]. LBP is the most widespread musculoskeletal condition as well as the leading cause of years lived with disability (YLDs) worldwide [2, 3]. As part of the Global Burden of Disease (GBD) study expert group, LBP is among the top ten high-burden diseases and injuries, with an average number of disability-adjusted life years (DALYs) higher than HIV, road injuries, tuberculosis, lung cancer, chronic obstructive pulmonary disease, and preterm birth complications [4]. As a result, the condition is a significant public health concern because it has a noticeable impact on healthcare systems and people’s quality of life (QoL) [5]. In contemporary workplaces, the occupational application of LBP is strong-minded in terms of direct and indirect costs, including lost productivity, activity limitation, time away from work, early retirement, and incurring a major economic burden in compensation costs and lost wages [6,7,8].
Low back pain is a major clinical and governmental health problem that has reached epidemic levels. It is estimated that about 90% of the global population suffers from LBP at some point in their lives [9]. LBP was identified by the WHO as one of the top three occupational health problems, and it has been estimated that occupational exposures accounted for 37% of the global burden of LBP [10, 11]. The prevalence of LBP is increasing globally at an estimated 30% to 80% among the general population [12]. It varies according to the type of activity performed [13,14,15,16] and affects adults of all ages, any gender, and any socioeconomic background [17].
School teachers are among the occupational groups most affected by LBP [14]. The prevalence of LBP is much higher in teaching staff compared to other occupational groups, ranging from 12 to 95% [18, 19]. The burden of LBP is greater in low- and middle-income countries (LMICs) like African nations [20, 21]. A sparse study conducted among teachers in Africa showed that the prevalence of LBP among teachers is irregular and increasing. In light of this, the prevalence of LBP among school teachers in Africa ranges from 53.2% in Egypt [22], 55.7% in Botswana [16], 62.7% in Nigeria [23], 64.98% in Kenya [24], 74.8% in Ethiopia [25], to 82.9% in Tanzania [18].
Several factors have been associated with the development of LBP in school teachers [26]. The work of a teacher is planning, organizing, and implementing an instructional program in a learning environment to guide students in developing and achieving their academic potential. The majority of a teacher's time is spent standing in the classroom, walking while teaching, writing on the blackboard, preparing lessons, grading assignments, and doing other administrative tasks with risky working postures for extended periods, all of which stress the musculoskeletal system and development of LBP [27, 28]. In Africa, almost all teaching activities are performed under unfavorable conditions, requiring teachers to use their physical, cognitive, and effective capabilities to achieve a teaching objective while over-demanding or generating effort for their psycho-physiological functions [29]. Psychosocial factors such as high workload, sleep disturbance, low job satisfaction, and job stress have been implicated as risk factors for LBP among school teachers [25, 30,31,32], while some factors like regular exercise and good job satisfaction act as protective effects against LBP in teachers [30, 33]. Socio-demographic factors, such as age, sex, work experience, and lifestyle factors, such as smoking and BMI, are other risk factors associated with LBP among school teachers [16, 24, 34, 35].
The impact of LBP is given less priority and is empirically unrepresented in low- and middle-income countries as a result of the focus on more pressing and life-threatening health issues like none communicable diseases and infectious diseases. In addition, most African countries are in the midst of socio-political crises, and as a result, almost all of each country's resources are diverted to dealing with these political crises rather than addressing public health problems, including the management of LBP [36, 37]. Teachers’ health has a substantial effect on a country's development since they are valuable resources for the socio-economic and cultural development of that country. As a result, an increase in the prevalence of LBP among teachers will affect every country's education system. In Africa, the prevalence of LBP is scattered and increasing in the teaching profession; however, there is a lack of studies to estimate the cumulative prevalence and associated risk factors of LBP among school teachers to provide strong evidence for policymakers and implementers to design effective prevention and control methods to protect teachers’ health and the quality of education that their students receive. Therefore, the objective of this review was to estimate the pooled prevalence and associated factors of LBP among school teachers in Africa. The review focused on nursery, primary or elementary, secondary, and preparatory school teachers.
Materials and methods
Registration and protocol
This systematic review and meta-analysis were done to compile the most recent evidence using published and gray literature on the prevalence and associated risk factors of LBP among school teachers in Africa. The protocol for this review was registered on the Prospective Register of Systematic Reviews (PROSPERO) international database (protocol registration number: CRD42022373366). For reporting, we followed the protocol of the Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) guidelines [38] (S1 File).
General characteristics of the reviewed articles
All studies primarily reporting on the prevalence of LBP among school teachers in African countries are included in the current review. As well, studies reported on the prevalence of MSDs as a whole, but they had to provide subgroup data for LBP prevalence, which could also be included in our systematic and meta-analytical review. Subjects in the studies could be of any race, gender, and people the age of 18 years and above.
Search strategies
A comprehensive systematic literature search was conducted using the PubMed/MEDLINE, CINAHL, and CABI databases, regardless of publication timelines, from October 20 to December 03, 2022, because there had been no systematic review and meta-analysis done before. The following key terms were used in combination with the Boolean operators "AND" and "OR". For the PubMed/MEDLINE search, the following key terms were used in combination with the Boolean operators "AND" and "OR". ((((((((((((((low back pain*[All Fields]) OR (lower back pain*[All Fields])) OR (back pain*[All Fields])) OR (back ache*[All Fields])) OR (Low Backache*[All Fields])) OR (Back Ache*[All Fields])) AND (Primary school teacher*[All Fields])) OR (Elementary school teacher*[All Fields])) OR (Middle School Teacher*[All Fields])) OR (Pre-School Teacher*[All Fields])) OR (Secondary school teacher*[All Fields])) OR (Preparatory school teacher*[All Fields])) OR (School teacher*[All Fields])))) OR (High school teacher*[All Fields]) AND (Algeria OR Angola OR Benin OR Botswana OR Burkina Faso OR Burundi OR Cameroon OR Cape Verde OR Central African Republic OR Chad OR Comoros OR Congo OR Ivory Coast OR Djibouti OR Egypt OR Equatorial Guinea OR Eritrea OR Ethiopia OR Gabon OR Gambia OR Ghana OR Guinea OR Guinea-Bissau OR Kenya OR Lesotho OR Liberia OR Libya OR Madagascar OR Malawi OR Mali OR Mauritania OR Mauritius OR Morocco OR Mozambique OR Namibia OR Niger OR Nigeria OR Rwanda OR Sao Tome and Principe OR Senegal OR Seychelles OR Sierra Leone OR Somalia OR South Africa OR Sudan OR Swaziland OR Tanzania OR Togo OR Tunisia OR Uganda OR Zambia OR and Zimbabwe). In addition to the electronic database search, gray literature was searched using direct Google Search and Google Scholar. Reference lists (bibliographies) of the included studies were also searched to obtain additional articles.
Eligibility criteria
Inclusion criteria
Articles that met the following determined inclusion criteria were included in this systematic review and meta-analysis: (a) were published and unpublished studies in any period (the study period was not restricted for inclusion), (b) examined the prevalence and/or associated factors of LBP, (c) were conducted in African countries, (d) studies that employed an observational study design, (e) were carried out on primary school teachers, elementary school teachers, middle school teachers, pre-school teachers, secondary school teachers, and/or preparatory school teachers, and (f) studies reported in the English language up to December 03, 2022, were included in our systematic review and meta-analysis.
Exclusion criteria
Qualitative studies, systematic reviews, editorial letters and reviews, short communications, and commentaries were excluded. In addition, articles that were not fully accessible after three or more personal email contacts with the corresponding author were also excluded.
Study selection
Two review authors (AHT & FMA) independently screened articles by their title, abstract, and full text to identify eligible articles using predetermined inclusion and exclusion criteria. The identified articles were then combined, exported, and managed using Endnote X9.2 (Thomson Reuters, Philadelphia, PA, USA) software. After the exclusion of duplicate studies, titles, and abstracts were independently screened for inclusion in the full-text appraisal, which was done by other review authors (AHT, GA, & FMA), and the disagreement between authors that arises during data abstraction and selection are solved based on evidence-based discussion and by the involvement of the remaining review authors (THM & AGJ).
Outcome measurements
The primary outcome of this systematic review and meta-analysis was the prevalence of LBP among school teachers in Africa, which indicates the number of people who reported the pain divided by the population number at a given point in time (in our case, 12 months) and presented as a prevalence or proportion. We used the authors’ reported definitions using standardized scales or questionnaires (e.g., standardized Nordic questionnaire, Dutch musculoskeletal questionnaire). The secondary outcomes of this review were to identify the risk factors for LBP (e.g., sociodemographic factors like sex, age, etc., personal or behavioral factors like physical exercise, BMI, smoking, etc., psychosocial factors, ergonomics factors, and workplace-related factors). We derived estimates from the number of cases and sample size provided in each study when the outcome of the results (e.g., proportion and 95% CI) were not directly reported and it was practical to do so. The measure of effect size was the odds ratio.
Data extraction and management
The data were extracted using the Joanna Briggs Institute (JBI) data extraction checklist. Three review authors (AHT, FMA, and GA) extracted the data independently using a Microsoft Excel spreadsheet. The differences between the three review authors were solved with discussion. Any discrepancies were resolved through a review by the other review authors (THM and AGJ). From each study, information such as the name of the first author, the year of publication, the study year, the study country, the study design, the total number of participants, the number of LBP cases among school teachers, the prevalence of LBP and its standard error, factors associated with LBP with their standard errors, and each study's measures of association were extracted.
Assessment of the methodological quality of the studies
The JBI quality appraisal tool for cross-sectional studies was used to assess the quality of included articles and the risk of bias in each study [39]. Three reviewer authors (AHT, GA, and FMA) independently assessed the quality of the included articles. The assessment tool contains eight criteria: (1) clear inclusion and exclusion criteria; (2) description of the study subject and study setting; (3) use of a valid and reliable method to measure the exposure; (4) standard criteria used for measurement of the condition; (5) identification of confounding factors; (6) development of strategies to deal with confounding factors; (7) use of a valid and reliable method to measure the outcomes; and (8) use of appropriate statistical analysis. It was evaluated using the JBI critical appraisal checklist options of "yes," "no," "unclear," and "not applicable." The risks for biases were classified as low (total score, 5 to 8) and high (total score, 0 to 4). The study scored 50% or higher on all quality-assessed items, which were considered low-risk and included in this review. Disagreements that arose during the full-text quality assessment were resolved through evidence-based discussion with the other review authors (THM and AGJ).
Data synthesis and analysis
The extracted data were exported from a Microsoft Excel spreadsheet to STATA version 14 for further analysis. We calculated the I2 statistic to determine study heterogeneity, which describes the percentage of total variation among studies that is due to heterogeneity rather than chance, in which 25%, 50%, and 75% represented low, moderate, and high heterogeneity, respectively [40]. The test statistic showed there is significant heterogeneity among the studies (I2 = 96.27%, p < 0.000). Therefore, the overall effect of LBP among African school teachers was estimated using a random effect model and measured by prevalence rates and odds ratios with 95% CI using DerSimonian-Laird weight [41]. We conducted a country-specific sub-group analysis. Furthermore, sensitivity analysis is performed to determine the impact of individual studies on the pooled estimate. Publication bias (the small study effect) was detected using the visual funnel plot test and Egger’s statistical test [42]. To estimate the relationship between LBP and factors, the odds ratio with a 95% confidence level was used, and a significance level of 0.05 was considered for the P-value. The results were presented using graphs, tables, texts, and a forest plot.
Results
Searching results
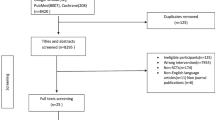
A total of 585 articles were retrieved from PubMed/MEDLINE, CINAHL, and CABI electronic databases, as well as from Google Scholar and Google Search. 463 duplicate articles were removed using EndNote citation manager; 104 articles were excluded after the title and abstract screening, and then 18 articles remained. After a careful inspection of 18 publications for the presence of the outcome variable, 7 papers were removed in compliance with the exclusion criteria, and finally, 11 articles remained. Accordingly, 11 eligible studies were incorporated for this systematic review and meta-analysis to estimate the pooled prevalence of LBP and its associated factors after quality assessment using the JBI quality assessment critical appraisal checklist. The overall study selection process was represented by the following flow diagram (Fig. 1).

PRISMA flow diagram describing the selection of studies for the systematic review and meta-analysis of low back pain and associated risk factors among school teachers in Africa, 2022
Description of included studies
The characteristics of the review, which include the publication year, sample size, study design, and study country, are all compiled in Table 1. All included studies were cross-sectional in study design, with sample sizes ranging from 153 in Nigeria [23] to 1747 in Botswana [16]. The studies were published from 2013 through 2022. The entire set of included studies counted for both genders and the recall periods for LBP were reported as a 12-month prevalence.
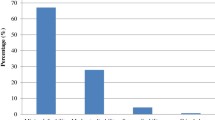
In this systematic review and meta-analysis, a total of 5,805 school teachers were included to estimate the pooled prevalence of LBP. The eleven studies were carried out across several African nations: Four (36.36%) articles [25, 30, 43, 44] were conducted in Ethiopia, two (18.18%) articles [24, 45] were conducted in Kenya; two (18.18%) articles [22, 46] were conducted in Egypt; and one (9.1%) article was conducted in each of Botswana [16], Nigeria [23], and Tanzania [18]. The lowest and highest prevalence of LBP among school teachers in Africa was 41% in Egypt [46] and 82.9% in Tanzania [18], respectively. All of the articles were re-evaluated by independent evaluators prior to any analysis, and the studies were fit in terms of quality (quality score ranged from 5 to above points). The description of the included studies is presented in Table 1.
Meta-analysis
Pooled prevalence of low back pain among school teachers in Africa
There were a total of 5,805 school teachers included in the eleven studies that were used to estimate the pooled prevalence of LBP for the current study. The forest plot result of the eleven included studies showed that the overall pooled prevalence of LBP among African school teachers was 59.0% (95% CI: 52.0–65.0%) (Fig. 2). In addition, the forest plot of our meta-analysis showed that the highest proportion (83.0%) of LBP was reported from a study done in Tanzania [18]. Whereas, the lowest proportion (41.0%) of LBP was reported in a study done in Egypt [46]. Nine (81.82%) of the eleven studies revealed that LBP affected more than 50% of school teachers. According to this review's I2 test statistics (I2 = 96.27%), the included studies showed high heterogeneity. Therefore, subgroup and univariate meta-regression analyses were conducted to identify the possible sources of heterogeneity.

Forest plot of the pooled prevalence of LBP among African school teachers, 2022
Subgroup analysis
The subgroup prevalence of LBP was estimated by considering the country where the studies were conducted. Accordingly, in the subgroup analysis, the overall pooled prevalence of LBP based on the country of the studies was 58.0% (95% CI: 51.0%, 66.0%). In addition, the pooled prevalence of LBP was widely varied across the country. As such, in the country subgroup analysis, Kenya had the highest pooled proportion of LBP at 62.0% (95% CI: 56.0%, 68.0%), followed by Ethiopia at 58.0% (95% CI: 44.0%, 72.0%), and Egypt at 47.0% (95% CI: 35.0%, 59.0%). Even if a single study was reported in Botswana, Nigeria, and Tanzania, the highest prevalence of LBP is reported in a study conducted in Tanzania out of all eleven studies included in this systematic review and meta-analysis (Fig. 3).

Forest plot of pooled low back pain among school teachers in Africa by country, 2022
Heterogeneity and small study effect test
All eleven included articles were assessed for heterogeneity and publication bias (small study effect). The presence of a possible small study effect was checked by using a funnel plot and the Egger test. Accordingly, the funnel plot (Fig. 4) showed an asymmetric distribution and presented evidence of heterogeneity. However, the result of the Egger regression test indicates that there is no evidence of publication bias (P-value = 0.920) (Fig. 5).

Funnel plot and Egger test of the eleven studies included in the meta-analysis of low back pain among school teachers in Africa, 2022

Egger graph to test for small study effect
Sensitivity analysis test
A sensitivity analysis of the eleven studies was conducted to test the effect of each study on the pooled result. This was carried out by excluding each study step by step (i.e., based on eleven studies). However, the results of the sensitivity analysis showed that there were no significant changes across all studies in the fitted meta-analytic model, as shown in Fig. 6.

Sensitivity analysis graph to examine the effect of each study on the pooled result
Factors associated with low back pain among school teachers in Africa
Factors associated with LBP were identified based on the pooled effect of two or more studies. Gender, age, physical activity, cigarette smoking, sleep problems, and a history of previous injury were identified as factors associated with LBP among African school teachers.
The pooled effect of our review analysis showed that female teachers were 1.53 times more likely to experience LBP compared to male teachers [POR: 1.53; 95% CI (1.19, 1.98)]. Similarly, school teachers who were in the age range of 30 or more years were more likely to have LBP compared to those in the age range of less than 30 years [POR: 1.58; 95% CI (1.04, 2.40)]. As well, the pooled effect of our analysis indicated that the likelihood of suffering from LBP was increased twofold among teachers who did not perform the physical exercise as compared to those who did [POR: 1.92; 95% CI (1.04, 3.52)]. Besides, teachers who had sleep problems were two times more likely to develop LBP compared to teachers who did not have sleep problems [POR: 2.03; 95% CI (1.19, 3.44)]. Furthermore, the odds of having LBP were 1.92 times higher among teachers who had a history of injury compared with those who did not [POR: 1.92; 95% CI (1.67, 2.21)]. However, there was no significant pooled effect size observed between cigarette smoking and LBP among school teachers in Africa in our analysis [POR: 2.86; 95% CI (0.24, 33.54)] (Table 2).
Discussion
Low back pain is the most common public health, economic, and social problem. LBP also has an indiscriminate impact on populations all over the world [47]. This first-of-its-kind systematic review and meta-analysis aimed to estimate the pooled prevalence of low back pain and its associated factors among school teachers in African countries. Overall, this review suggests that LBP pain in teachers is likely an under-researched topic but that the teaching profession itself poses a high risk for LBP. According to this meta-analysis, the overall annual pooled prevalence of LBP among school teachers was found to be 59.0% (95% CI: 52.0–65.0%). As well, based on the combined effects of two or more of the studies included in this meta-analysis, significant factors associated with LBP among school teachers in Africa included gender, age, physical activity, sleep problems, and a history of earlier injuries.
The current pooled prevalence of LBP is in line with a couple of systematic reviews and meta-analyses conducted in Ethiopia (54.2%) [48] and 54.05% [49], a systematic review conducted in Nigeria (55.39%) [50], a systematic review and meta-analysis conducted in India (51%) [51], prior working groups in African nations (57%) [52], as well as a study conducted in the United Arab Emirates (64.6%) [53]. However, the pooled prevalence of LBP in the present review is higher than a systematic review conducted in Latin America (31.3%) [54], a study conducted in the United Kingdom (36.1%) [55], and a study conducted in Spain (20%) [12]. Compared to estimates for the global prevalence of LBP, the African working population has a higher annual prevalence of LBP [12, 56, 57]. Our review finding also revealed that the pooled prevalence of LBP (59.0%) in our finding is higher than the global annual prevalence of LBP (38.5%) [56].
A plausible explanation for the higher pooled prevalence of LBP among African school teachers is that LBP is a low priority in impoverished African countries and receives less attention than other diseases because the governments of such countries concentrate on more urgent and life-threatening health issues, such as infectious diseases [58]. The other reason can be due to the fact that the ongoing COVID-19 epidemic, violent wars, and challenges linked to climate change have severely strained the African healthcare system. As a result, health systems in every African nation are overburdened by communicable and noncommunicable diseases, which makes LBP a lower-priority issue in African countries' health development plans [59, 60]. As well, in every African nation, there is an absence of national screening programs and surveillance data on musculoskeletal disorders (MSDs) and/or LBP, which supplants the existing fact of the absence of priority given to every working population in Africa. Furthermore, the high prevalence of LBP among African school teachers can also be attributed to the fact that these specific working groups are accustomed to working in subpar workplace environments with poor ergonomic circumstances, which exacerbate pain in the low back region [16, 61, 62]. Therefore, it is necessary to create and put into effect plans and policies that effectively address the burden of LBP in developing or underdeveloped nations, such as those in Africa [21].
The result of subgroup analysis by country showed that the pooled prevalence of LBP was almost similar across countries in Africa. Thus far, there has been a relatively higher pooled prevalence of LBP found in Kenya (62% with a 95% CI: 56%, 68%), followed by Ethiopia (58% with a 95% CI: 44%, 72%), and the highest prevalence of LBP is reported in a study conducted in Tanzania out of all eleven studies included in this systematic review and meta-analysis study.
Risk factors of low back pain among school teachers in Africa
Our systematic review and meta-analysis also tried to investigate factors associated with low back pain. Accordingly, female gender, advanced age, physical inactivity, sleeping problems, and a history of previous injury were the identified predictors for LBP among African school teachers.
This meta-analysis of risk factors showed that the odds of LBP among female teachers were 1.53 times higher when compared with male teachers [POR: 1.53; 95% CI (1.19, 1.98)]. This finding is in agreement with studies conducted in Malaysia [63], Brazil [11], China [27], Turkey [64], and Iran [65], which reported that being female in gender had higher odds of LBP than being male among teachers. As opposed to our findings, few studies in Filipino [31] and Slovenia [66] indicated female gender had no significant effect on LBP in teachers. The plausible reason for this gender difference could be that females have a lower threshold for pain than males [67]. As a result, females were more likely to report pain trouble than their counterparts. In addition, females’ lower physical strength, pregnancy, menstruation, and pain related to osteoporosis might be a possible explanation for the incongruity [33]. Moreover, females could carry out more heavy housework than males daily, and evidence [68] suggests that these differences in household task involvement may explain LBP differences between females and males. Furthermore, the physical stress of child-rearing and perimenopausal abdominal weight gain [69] and the physiologically low disk space in females [70] may also contribute to the occurrence of more LBP among females. This suggests that back pain prevention strategies in the workplace should give much emphasis on the female population.
School teachers who were in the age range of 30 or more years were found to be more likely to have LBP compared to those in the age range of less than 30 years. This finding is supported by previous studies conducted in the Philippines [71], Brazil [11], Turkey [72], Slovenia [66], China [73], and America [74]. Besides, the European Agency for Safety and Health at Work [75] highlighted advanced age as one of the most reported individual risk factors for LBP. This could be justified as teachers age; there is a gradual decline in muscle mass, and they lose connective tissue elasticity and undergo a diminishing of cartilage between joints. On the other hand, healing will slow down with advancing age [76]. In addition, with increasing age, the direct blood supply to the intervertebral disc will be reduced [77]. This will make lumbar discs easily susceptible to wear and tear or degeneration. Lumbar disc degeneration leads to lumbar spine instability. This unstable lumbar spine then imposes a higher biomechanical demand on the ligaments, capsules, muscles, and facets [78] and consequently develops pain in the lower back region. The older teachers might have a longer teaching service, and this increases the duration of exposure to risk factors. As a result, this cumulative effect can also explain the higher odds of LBP among older teachers than their younger colleagues [79].
As well, the pooled effect of this study indicated that the likelihood of experiencing LBP was increased by twofold among school teachers who did not perform the physical exercise as compared to those who did [POR: 1.92; 95% CI (1.04, 3.52)]. Previous study from Australia [80] have shown a similar association between no physical exercise and LBP. This could be due to the fact that not performing physical exercise might weaken muscles in the lower back and cause a misalignment of the spine, subsequently leading to the development of LBP in teachers [81, 82]. On the other way round, studies done in Tunisia [83], Southern Brazil [84], and China [85] indicated that performing regular physical activity can reduce LBP risk. Likewise, Hosam et al.'s systematic review and meta-analysis of a cross-sectional study corroborated this finding [86]. The possible explanation for this could be that regular physical exercise can enhance muscle strength and endurance, improve cardiovascular function, promote the diffusion of tissue fluid, ensure the absorption of nutrition by bone and muscle tissue, and alleviate muscle fatigue [87]. Therefore, performing regular physical exercise may reduce the risk of LBP [88]. Another reason could be that physical exercise increases blood flow to the spine, which supplies essential nutrients to the structure of the lower back region [89]. This implies that conducting regular physical exercise is imperative to prevent the development of LBP among teachers.
Moreover, the current systematic review and meta-analysis pooled effect size determined that teachers who had sleep problems were two times more likely to develop LBP compared to teachers who did not have sleep problems. This is supported by studies in China [27], India [81], Bangladesh [34], and France [90]. The reasons might be that teachers may have received insufficient rest as a result of insufficient sleep, which aggravated their lower back health issues by increasing their stress levels [81].
Furthermore, empirical evidence from Bangladesh [34], France [91], and elsewhere [74] indicated that a history of previous injury was associated with an increased risk of LBP. Similarly, our study found a significant association between previous injury and LBP in teachers. Congruently, a similar relationship was found between prior injury and back and upper extremity pain in Korean male steelworkers [92]. On top of that, a similar association has been shown among healthcare workers in Italy [93]. The plausible explanation could be that previous injuries weaken the stamina of the back region’s soft tissues, including tendons, cartilage, discs, and nerves, and degrade the natural auto-recovery capability of the musculoskeletal system. This, in turn, reduces the tolerance of the musculoskeletal system for risk factors; thereby easily experiencing LBP. This implies that teachers with a history of previous injury shall be given priority and protected from musculoskeletal disorder risk factors. Though several studies [94,95,96,97] found that cigarette smoking was a risk factor for LBP, in this systematic review and meta-analysis, however, no association was found between cigarette smoking and LBP among school teachers in Africa. The findings from a study among Malaysian teachers [98] and a study by Jegnie M et al. [99] mimics similar result.
This systematic review and meta-analysis study suggests that multifaceted intervention strategies targeting socio-demographic, behavioral, physical, and/or educational and ergonomic aspects have been shown to have the greatest improvement in the prevention and management of LBP. Explicitly, risk factors significantly associated with LBP, particularly those identified in this review, should be incorporated into algorithms for the preventive and curative management of LBP. In addition, emphasis should be placed on the implementation and enforcement of the LBP management and control strategy, particularly in developing countries such as Africa to curtail this menace. Above all, future research, especially in Africa, should focus on identifying the barriers to implementation and the effectiveness of ergonomic and other interventions for LBP in school settings, which could help to propose tailored, effective, low-cost, and reasonably simple intervention programs for LBP. A multiple interventions approach to LBP using the results of an intervention trial, such as a cluster randomized controlled trial among teachers and other populations, should also be rigorously implemented in Africa to curb the high levels of LBP.
Strengths and limitations of the study
This study was a first-of-its-kind systematic review and meta-analysis that estimated the pooled prevalence and associated risk factors of LBP among school teachers in Africa. However, the absence of studies from countries other than the included ones may limit the continental representativeness of the study. The use of only the English language may also limit the conclusiveness of the findings.
Conclusions and policy implications
In this review, a high pooled prevalence of LBP was found in African school teachers compared to both the global estimate and developed nations. Sex (female), older age, physical inactivity, sleep problems, and a history of previous injury were predictors of LBP. However, no significant pooled effect size was observed between cigarette smoking and LBP among school teachers in Africa. It is recommended that school teachers be provided with and trained on ergonomics, physical exercise, behavioral change, and sleep quality to lessen the impact of LBP. In addition, it is suggested that policymakers and administrators ought to gain awareness of LBP and its risk factors to put existing LBP preventive and control measures into action. Policymakers also need to integrate and strengthen LBP prevention and management strategies into the country's health system management guidelines and implement existing LBP prevention and control measures. Prophylactic management and therapeutic strategies for people with LBP should also be endorsed.
Availability of data and materials
All data generated or analyzed during this study are included in this published article [and its supplementary information files].
Abbreviations
- LBP:
-
Low back pain
- MSDs:
-
Musculoskeletal disorders
- POR:
-
Pooled odds ratio
- GBD:
-
Global burden of disease
- YLDs:
-
Years lived with disability
- DALYs:
-
Disability-adjusted life years
- QOL:
-
Quality of life
- PRISMA:
-
Preferred Reporting Items for Systematic Reviews and Meta-Analyses
References
Hoy D, March L, Brooks P, Woolf A, Blyth F, Vos T, Buchbinder R. Measuring the global burden of low back pain. Best Pract Res Clin Rheumatol. 2010;24(2):155–65.
Wu A, March L, Zheng X, Huang J, Wang X, Zhao J, Blyth FM, Smith E, Buchbinder R, Hoy D: Global low back pain prevalence and years lived with disability from 1990 to 2017: estimates from the Global Burden of Disease Study 2017. Ann Transl Med. 2020, 8(6):299.
Woolf AD, Pfleger B. Burden of major musculoskeletal conditions. Bull World Health Organ. 2003;81:646–56.
Vos T, Flaxman AD, Naghavi M, Lozano R, Michaud C, Ezzati M, Shibuya K, Salomon JA, Abdalla S, Aboyans V. Years lived with disability (YLDs) for 1160 sequelae of 289 diseases and injuries 1990–2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012;380(9859):2163–96.
Driscoll T, Jacklyn G, Orchard J, Passmore E, Vos T, Freedman G, Lim S, Punnett L. The global burden of occupationally related low back pain: estimates from the Global Burden of Disease 2010 study. Ann Rheum Dis. 2014;73(6):975–81.
Aldawsari SA, Alhammad AH, Alanazi ADS, Al-Rashidi N, Mohamed EY, Ahmed SM: A study of the prevalence of low back pain and associated risk factors among surgical staff in Sudair Area, Saudi Arabia.
Sritipsukho P, Siripakarn Y: Prevalence and risk factors of low back pain among the university staff. J Med Assoc Thai 2010. 93(suppl 7):S142-S141S148.
Di Donato M, Iles R, Lane T, Collie A. The impact of income support systems on healthcare quality and functional capacity in workers with low back pain: a realist review protocol. Syst Rev. 2019;8(1):1–11.
Freburger JK, Holmes GM, Agans RP, Jackman AM, Darter JD, Wallace AS, Castel LD, Kalsbeek WD, Carey TS. The rising prevalence of chronic low back pain. Arch Intern Med. 2009;169(3):251–8.
Prüss-Üstün A, Corvalán C. Preventing disease through healthy environments. Towards an estimate of the environmental burden of disease Geneva: World Health Organization; 2006.
Cardoso JP. Ribeiro IdQB, Araújo TMd, Carvalho FM, Reis EJFBd: Prevalence of musculoskeletal pain among teachers. Rev Bras Epidemiol. 2009;12:604–14.
Hoy D, Brooks P, Blyth F, Buchbinder R. The epidemiology of low back pain. Best Pract Res Clin Rheumatol. 2010;24(6):769–81.
Erick PN, Smith DR: The prevalence and risk factors for musculoskeletal disorders among school teachers in Botswana. Occupational Medicine & Health Affairs 2014:1–13.
Bandpei MAM, Ehsani F, Behtash H, Ghanipour M. Occupational low back pain in primary and high school teachers: prevalence and associated factors. J Manipulative Physiol Ther. 2014;37(9):702–8.
Badawood MA, Obaid H, Mohammed ME, Alrogi AJ: Impact of Low Back Pain on the work performance of male high school Saudi Teachers in Taif City. J Health Inform in Dev Countries. 2017, 11(2).
Erick PN, Smith DR. Low back pain among school teachers in Botswana, prevalence and risk factors. BMC Musculoskelet Disord. 2014;15(1):1–13.
Majid K, Truumees E: Epidemiology and natural history of low back pain. In: Seminars in Spine Surgery. Royal Oak: Elsevier. 2008;87–92.
Nilahi CD: Work-related lower back pain among primary school teachers in Dar es Salaam, Tanzania. 2014.
Kaleem RMW, Shahzad U, Shahzad H, Batool A. PREVALENCE OF LOW BACK PAIN IN PRIMARY FEMALE SCHOOL TEACHERS. PalArch’s J Archaeol Egypt/Egyptology. 2021;18(10):564–70.
Woolf AD, Erwin J, March L. The need to address the burden of musculoskeletal conditions. Best Pract Res Clin Rheumatol. 2012;26(2):183–224.
Woolf AD, Brooks P, Åkesson K, Mody GM. Prevention of musculoskeletal conditions in the developing world. Best Pract Res Clin Rheumatol. 2008;22(4):759–72.
Fahmy VF, Momen MAMT, Mostafa NS, Elawady MY. Prevalence, risk factors and quality of life impact of work-related musculoskeletal disorders among school teachers in Cairo, Egypt. BMC Public Health. 2022;22(1):1–17.
Sumaila FG, Mayana KI, Bello B, Sharif AM. Prevalence of low back pain and back ergonomics awareness among teachers of selected secondary schools in Kano Metropolis. Int J Physiother. 2015;2(6):999–1005.
Mwangi A, Downing R, Elias HE. Low back pain among primary school teachers in Rural Kenya: Prevalence and contributing factors. African J Primary Health Care Family Med. 2019;11(1):1–7.
Kebede A, Abebe SM, Woldie H, Yenit MK: Low back pain and associated factors among primary school teachers in Mekele City, North Ethiopia: a cross-sectional study. Occupational therapy international 2019, 2019.
Zamri EN, Hoe VCW, Moy FM. Predictors of low back pain among secondary school teachers in Malaysia: a longitudinal study. Ind Health. 2020;58(3):254–64.
Chong EY, Chan AH. Subjective health complaints of teachers from primary and secondary schools in Hong Kong. Int J Occup Saf Ergon. 2010;16(1):23–39.
Gupta G, Sharma A. Prevalence of low back pain among higher secondary school teachers of Kanpur, India. J Orthopaed Physiother. 2018;1:1–8.
Musa AI, Qutubuddin S. Ergonomics study of the incidence of musculoskeletal disorder among the school teachers in Egba division of Ogun state Nigeria. J Sci Technol Res. 2020;2(1):13–12.
Beyen TK, Mengestu MY, Zele YT. Low back pain and associated factors among teachers in Gondar Town, North Gondar, Amhara Region, Ethiopia. Occup Med Health Aff. 2013;1(5):1–8.
Atlas AP, Bondoc R, Garrovillas R, Lo RD, Recinto J, Yu K. PTRP M: Prevalence of low back pain among public high school teachers in the City of Manila. Philippine J Allied Health Sci. 2007;2(1):34–40.
Mohammadi G. Prevalence of low back pain and associated risk factors among high school teachers in Kerman, Iran. J Musculoskeletal Res. 2017;20(01):1750005.
Erick PN, Smith DR. A systematic review of musculoskeletal disorders among school teachers. BMC Musculoskelet Disord. 2011;12(1):1–11.
Akter J, Kamrujjaman M, Maleque A. Prevalence and factors associated with low back pain among school teachers residing in northern Dhaka city. MOJ Orthopedics Rheumatology. 2018;10(5):333–7.
Alghwiri A, Marchetti G. Occupational back pain among schoolteachers in Jordan: estimated prevalence and factors associated with self-reported pain and work limitations. Int J Occup Saf Ergon. 2018;24(3):341–6.
Kahere M, Hlongwa M, Ginindza TG. A scoping review on the epidemiology of chronic low back pain among adults in sub-Saharan Africa. Int J Environ Res Public Health. 2022;19(5):2964.
Buchbinder R, van Tulder M, Öberg B, Costa LM, Woolf A, Schoene M, Croft P, Hartvigsen J, Cherkin D, Foster NE. Low back pain: a call for action. Lancet. 2018;391(10137):2384–8.
Moher D, Shamseer L, Clarke M, Ghersi D, Liberati A, Petticrew M, Shekelle P, Stewart LA. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst Rev. 2015;4(1):1–9.
Institute JB: JBI Checklist for Analytical Cross Sectional Studies. JBI Global, 2020. In.
Higgins JP. Thompson SGJSim: Quantifying heterogeneity in a meta-analysis. 2002;21(11):1539–58.
DerSimonian R. Laird NJCct: Meta-analysis in clinical trials. 1986;7(3):177–88.
Egger M, Smith GD. Schneider M. Minder CJB: Bias in meta-analysis detected by a simple, graphical test. 1997;315(7109):629–34.
Gebreyesus T, Weldemariam S, Fasika S, Abebe E, Kifle M. Prevalence and associated factors of low back pain among school teachers in Mekelle City, Northern Ethiopia, 2016: a cross sectional study. World J Phys Med Rehab. 2019;1:1006.
Abebaw T-A, Weldegebriel MK, Gebremichael B, Abaerei AA. Prevalence and associated factors of low back pain among teachers working at governmental primary schools in Addis Ababa, Ethiopia: a cross sectional study. Biomed J. 2018;1(6):3.
Ndonye NA, Matara NJ, Muriithi IA: Predictors of work-related musculoskeletal disorders among primary school teachers in Machakos County, Kenya. Int J Ind Ergon 2019.
Mo E, Ebied E. Work-related musculoskeletal pain among primary school teachers: a recommended health promotion intervention for prevention and management. World J Nurs Sci. 2015;1(3):54–61.
Manchikanti L, Singh V, Datta S, Cohen SP, Hirsch JA. Comprehensive review of epidemiology, scope, and impact of spinal pain. Pain Physician. 2009;12(4):E35-70.
Mengistu DA, Mulugeta Demmu Y, Alemu A. Occupational related upper and low back pain among the working population of Ethiopia: systematic review and meta-analysis. Environmental health insights. 2021;15:11786302211067840.
Jegnie M, Afework M: Prevalence of self-reported work-related lower back pain and its associated factors in Ethiopia: a systematic review and meta-analysis. J Environ Public Health. 2021, 2021:6633271.
Bello B, Adebayo HB: A systematic review on the prevalence of low back pain in Nigeria. Middle East J Rehab Health. 2017, 4(2).
Shetty GM, Jain S, Thakur H, Khanna K: Prevalence of low back pain in India: a systematic review and meta-analysis. Work 2022(Preprint):1–24.
Morris LD, Daniels KJ, Ganguli B, Louw QA. An update on the prevalence of low back pain in Africa: a systematic review and meta-analyses. BMC Musculoskelet Disord. 2018;19(1):1–15.
BENER A. EL-RUFAIE OF, SIYAM A, ABUZEID MS, TOTH F, LOVASZ G: Epidemiology of low back pain in the United Arab Emirates. APLAR J Rheumatol. 2004;7(3):189–95.
Garcia JB, Hernandez-Castro JJ, Nunez RG, Pazos MA, Aguirre JO, Jreige A, Delgado W, Serpentegui M, Berenguel M, Cantisani AF: Prevalence of low back pain in Latin America: a systematic literature review. Pain Physician. 2014; 17: 379–391.
Raspe H, Matthis C, Croft P, O’Neill T, Group EVOS. Variation in back pain between countries: the example of Britain and Germany. Spine. 2004;29(9):1017–21.
Hoy D, Bain C, Williams G, March L, Brooks P, Blyth F, Woolf A, Vos T, Buchbinder R. A systematic review of the global prevalence of low back pain. Arthritis Rheum. 2012;64(6):2028–37.
Wang L, Ye H, Li Z, Lu C, Ye J, Liao M, Chen X. Epidemiological trends of low back pain at the global, regional, and national levels. Eur Spine J. 2022;31(4):953–62.
Froud R, Patterson S, Eldridge S, Seale C, Pincus T, Rajendran D, Fossum C, Underwood M. A systematic review and meta-synthesis of the impact of low back pain on people’s lives. BMC Musculoskelet Disord. 2014;15(1):1–14.
Sharma S, McAuley JH: Low Back Pain in Low-and Middle-Income Countries, Part 1: The Problem. In., vol. 52: JOSPT, Inc. JOSPT, 1033 North Fairfax Street, Suite 304, Alexandria, VA …; 2022: 233–235.
Kahere M, Ginindza T. Mapping evidence on the prevalence, incidence, risk factors and cost associated with chronic low back pain among adults in Sub-Saharan Africa: a systematic scoping review protocol. Syst Rev. 2020;9(1):1–9.
Alias AN, Karuppiah K, How V, Perumal V: Does prolonged standing at work among teachers associated with musculoskeletal disorders (MSDs)? Malaysian J Med Health Sci. 2020, 16(2):281.
Abdul Rahim AA, Jeffree MS, Ag Daud DM, Pang N, Sazali MF. Factors associated with musculoskeletal disorders among regular and special education teachers: a narrative review. Int J Environ Res Public Health. 2022;19(18):11704.
Nurul I, Haslinda A, Saidi M, Shamsul B, Zailina H. Prevalence of low back pain and its risk factors among school teachers. Am J Appl Sci. 2010;7(5):634–9.
Başkurt F, Başkurt Z, Gelecek N. Prevalence of self-reported musculoskeletal symptoms in teachers. Süleyman Demirel Üniversitesi Sağlık Bilimleri Dergisi. 2011;2(2):58–64.
Mohammadi G. Musculoskeletal complaints among high school teachers. J Musculoskelet Res. 2013;16(02):1350010.
Kovač M, Leskošek B, Hadžić V, Jurak G. Occupational health problems among Slovenian physical education teachers. Kinesiology. 2013;45(1):92–100.
Chiu TT, Lam T-H, Hedley AJ. Maximal isometric muscle strength of the cervical spine in healthy volunteers. Clin Rehabil. 2002;16(7):772–9.
Punnett L, Herbert R: Work-related musculoskeletal disorders: is there a gender differential, and if so, what does it mean? In: Women and Health. edn.: Elsevier; 2000: 474–492.
Bailey A. Risk factors for low back pain in women: still more questions to be answered. Menopause. 2009;16(1):3–4.
Wáng YXJ, Wáng J-Q, Káplár Z. Increased low back pain prevalence in females than in males after menopause age: evidences based on synthetic literature review. Quant Imaging Med Surg. 2016;6(2):199.
Ma L, Tm G. Prevalence and risk-factors of musculoskeletal disorders among provincial high school teachers in the Philippines. J UOEH. 2020;42(2):151–60.
Durmus D, Ilhanli I. Are there work-related musculoskeletal problems among teachers in Samsun, Turkey? J Back Musculoskelet Rehabil. 2012;25(1):5–12.
Jin K, Sorock GS, Courtney TK. Prevalence of low back pain in three occupational groups in Shanghai, People’s Republic of China. J Safety Res. 2004;35(1):23–8.
Chaffin DB. PARK KS: A longitudinal study of low-back pain as associated with occupational weight lifting factors. Am Ind Hyg Assoc J. 1973;34(12):513–25.
h a t W o r k EuropeanAgencyforSafetyandHealt: Introduction to work-related musculoskeletal disorders, Factsheet 71. In.; 2007.
Nilufer CK, Uur C, Emine AT. Musculoskeletal pain, associated risk factors and coping strategies in school teachers. Scientific Research and Essays. 2011;6(3):649–57.
THERESA STACK LTO, AND CHERYL A. WILHELMSEN: OCCUPATIONAL ERGONOMICS: A Practical Approach; 2016.
De Beeck RO, Hermans V. Work-related low back disorders. Spain: Bilbao; 2000.
Meucci RD, Fassa AG, Faria NMX. Prevalence of chronic low back pain: systematic review. Rev Saude Publica. 2015;49:73.
Hayes MJ, Smith DR, Cockrell D. An international review of musculoskeletal disorders in the dental hygiene profession. Int Dent J. 2010;60(5):343–52.
Behera S, Koley S. Low Back Pain And Its Associated Factors Among Secondary School Teachers In Cuttack, Odisha: A Cross-Sectional Study. IJMSDR. 2021;5(6):90–7.
Lemoyne J, Laurencelle L, Lirette M, Trudeau F. Occupational health problems and injuries among Quebec’s physical educators. Appl Ergon. 2007;38(5):625–34.
Ayed HB, Yaich S, Trigui M, Hmida MB, Jemaa MB, Ammar A, Jedidi J, Karray R, Feki H, Mejdoub Y. Prevalence, risk factors and outcomes of neck, shoulders and low-back pain in secondary-school children. Journal of research in health sciences. 2019;19(1): e00440.
Noll M, Candotti CT. Rosa BNd, Loss JF: Back pain prevalence and associated factors in children and adolescents: an epidemiological population study. Rev Saude Publica. 2016;50:31.
Yue P, Liu F, Li L. Neck/shoulder pain and low back pain among school teachers in China, prevalence and risk factors. BMC Public Health. 2012;12(1):1–8.
Alzahrani H, Mackey M, Stamatakis E, Zadro JR, Shirley D. The association between physical activity and low back pain: a systematic review and meta-analysis of observational studies. Sci Rep. 2019;9(1):1–10.
Shiri R, Coggon D, Falah-Hassani K. Exercise for the prevention of low back pain: systematic review and meta-analysis of controlled trials. Am J Epidemiol. 2018;187(5):1093–101.
Owen PJ, Miller CT, Mundell NL, Verswijveren SJ, Tagliaferri SD, Brisby H, Bowe SJ, Belavy DL. Which specific modes of exercise training are most effective for treating low back pain? Network meta-analysis. Br J Sports Med. 2020;54(21):1279–87.
Gordon R, Bloxham S: A systematic review of the effects of exercise and physical activity on non-specific chronic low back pain. In: Healthcare: 2016: MDPI; 2016: 22.
Muto S, Muto T, Seo A, Yoshida T, Taoda K, Watanabe M. Prevalence of and risk factors for low back pain among staffs in schools for physically and mentally handicapped children. Ind Health. 2006;44(1):123–7.
Ozguler A, Leclerc A, Landre M-F, Pietri-Taleb F, Niedhammer I. Individual and occupational determinants of low back pain according to various definitions of low back pain. J Epidemiol Community Health. 2000;54(3):215–20.
Choi WJ, Kang YJ, Kim JY, Han SH. Symptom prevalence of musculoskeletal disorders and the effects of prior acute injury among aging male steelworkers. J Occup Health. 2009;51(3):273–82.
Gerbaudo L, Violante B. Relationship between musculoskeletal disorders and work-related awkward postures among a group of health care workers in a hospital. Med Lav. 2008;99(1):29–39.
Jia N, Zhang M, Zhang H, Ling R, Liu Y, Li G, Yin Y, Shao H, Zhang H, Qiu B, et al. Prevalence and risk factors analysis for low back pain among occupational groups in key industries of China. BMC Public Health. 2022;22(1):1493.
Al-Salameen AH, Abugad HA, Al-Otaibi ST. Low back pain among workers in a paint Factory. Saudi J Med Med Sci. 2019;7(1):33–9.
Kahere M, Ginindza T. The prevalence and risk factors of chronic low back pain among adults in KwaZulu-Natal, South Africa: an observational cross-sectional hospital-based study. BMC Musculoskelet Disord. 2021;22(1):955.
Miranda H, Viikari-Juntura E, Punnett L, Riihimäki H. Occupational loading, health behavior and sleep disturbance as predictors of low-back pain. Scand J Work Environ Health. 2008;34(6):411–9.
Abdul-Samad NI AH, Moin S, Mohd Tamrin SB, Hahim Z. : Prevalence of low back pain and its risk factors among school teachers. Am J Applied Sci. 2010, 7(5):634.
Jegnie M, Afework M. Prevalence of self-reported work-related lower back pain and its associated factors in Ethiopia: a systematic review and meta-analysis. J Environ Public Health. 2021;2021:6633271.
Acknowledgements
Not applicable.
Funding
This study did not receive any funding.
Author information
Authors and Affiliations
Contributions
AHT was involved in the conceptual development, data abstraction, selection, reviewing of articles, and report writing. GA and FMA were involved in the data analysis and writing of the manuscript. THM and AGJ were involved in guiding the work and manuscript writing. All the authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
All authors declare that they have no conflict of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Tesfaye, A.H., Abere, G., Mekonnen, T.H. et al. A systematic review and meta-analysis of low back pain and its associated factors among school teachers in Africa. BMC Musculoskelet Disord 24, 499 (2023). https://doi.org/10.1186/s12891-023-06633-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12891-023-06633-1