
Abstract
Background
Knee osteoarthritis (KOA) is a common disease based on degenerative pathological changes. Total knee arthroplasty (TKA) is an effective treatment for end-stage of KOA. However, only volume adaptation can be achieved with current knee prostheses, and it is difficult to achieve weight adaptation. This study focused on the weight difference of knee joints and initially explored the impact of this change on knee joint functional recovery and gait changes in patients after surgery.
Methods
From October 2015 to June 2019, patients who underwent primary unilateral TKA were enrolled in this prospective cohort study with the same brand of knee prostheses. General data were collected from patients who met the criteria. The resected bone and soft tissues were collected and weighed precisely during TKA, and multivariate regression analysis was used to determine the factors affecting the weight of the removed knee tissues. We compared the weight of excised tissues and the total weight of the knee prosthesis, and the weight difference was defined as the increased weight of the knee joint (IWKJ). All patients were evaluated by HSS score, gait analysis, and affected side knee X-ray at two weeks, three months, and the last follow-up after the operation. To further determine the influence of IWKJ on postoperative functional recovery, the relationship between IWKJ, HSS score, and gait analysis was analyzed by univariate regression.
Results
In total, 210 patients were eventually included in observation. All patients underwent postoperative follow-up for no less than two years. Multiple regression analysis showed that the course of the disease, body weight, and kellgren-Larencen stage(K-L stage)of the affected knee joint were independent factors affecting the weight of the removed knee tissues and were positively correlated with it. Univariate analysis showed that IWKJ was negatively correlated with HSS score at two weeks and three months after the operation. In addition, the values of spatiotemporal parameters and knee rotation ROM were negatively correlated with IWKJ two weeks after surgery, while outside food load response was positively correlated with IWKJ. Cadence, knee rotation ROM, and Ankle rotation ROM were negatively correlated with IWKJ, while outside food was positively correlated with IWKJ three months after surgery. At the last follow-up, only the hip rotation ROM was positively correlated with IWKJ.
Conclusions
All Patients underwent TKA had varying degrees of increased knee weight. The increased weight was 298.98 ± 63.77 g. Patients' body weight, K-L staging, and disease duration are important factors that cause differences in resected knee tissue. Three months after the operation, the changes in knee joint weight had a negative correlation with the HSS score, which at the same time, it had varying degrees of linearity with gait parameters. However, the influence of weight diminished over time.
Similar content being viewed by others


Background
Knee osteoarthritis (KOA) is a common disease based on degenerative pathological changes. It affects about 10 million adults in the United States [1]. Total knee arthroplasty (TKA) is an effective treatment to relieve pain and improve physical function in patients with severe KOA [2, 3]. Currently, it is estimated that nearly 1.8–2.4‰ patients are treated with TKA in developed countries every year. Moreover, the demand in developed countries for TKA will increase by 26–69% before the middle of the twenty-first century according to previous statistics [4].
With the increasing number of KOA patients, the occurrence of knee joint replacement with medical implants is of great importance for an aging population. Previous studies have shown that there is no significant difference in the effect of the implant design on knee function. However, few reports have focused on the influence of the knee prosthesis weight on postoperative joint functional recovery. A prospective study showed that the weight of knee prosthesis was 3.94 times that of excised tissue. Further analysis showed that this change accounted for about 0.5% of total body weight. They suggest that the increased local weight of the knee may do harm to functional recovery after TKA [5]. Rossi pointed out that patients tend to overestimate the weight of implants and they may refuse to do functional exercises because of their inability to adapt to the increased knee weight in the short term [6]. The weight of implants directly corresponds to the material from which they are made of. However, in many cases, all available materials may not be light. Since most knee prostheses consist of metal materials whose density is obviously higher than that of bone and soft tissue, only volume adaptation, rather than weight adaptation, can be achieved by TKA [7]. The weight of the prosthesis should match the weight of the removed bone and soft tissue, which is in line with the goals of precision medicine. Otherwise, the placement of heavy knee implants may negatively affect postoperative recovery [8]. To the best of our knowledge, the effect of knee weight changes on knee function and gait after TKA has not been reported. Therefore, we conducted such a prospective study to determine whether the change in the knee joint weight affects the recovery of knee function.
Methods
General patient information
Following approval from our institutional review board, patients who underwent unilateral primary TKA for KOA from October 2015 to June 2019 were eligible for enrolment in this prospective trial. Informed consent for participation was obtained from each patient before surgery. All patients involved in the study were required to register their age, sex, body mass index (BMI), course of the disease, visual analogue scale (VAS) score, and some other general information. All patients routinely underwent knee x-rays before surgery to determine the K-L staging of knee osteoarthritis, hip knee ankle (HKA) Angle, and the number of compartments affected [9, 10] (Fig. 1a-b).

X-ray measurement of knee joint as well as weight measurement of excised knee tissue and unused bone cement. a HKA angle measurement before TKA; b HKA angle measurement after TKA; c weight of excised knee tissue; d weight of unused bone cement
Inclusion and exclusion criteria
Inclusion criteria
Patients who met the following criteria were included: (i) initial TKA treatment; (ii) according to the condition, a prosthesis of the observed brand could be used; and (iii) no less than two years of follow-up.
Exclusion criteria
Patients were excluded for the following reasons: (i) lack of follow-up data; (ii) patellar replacement was also performed; (iii) prior knee surgery; (iv) bilateral and simultaneous TKA; (v) use of additional prosthetic components, such as tibial extension rods; (vi) serious basal metabolic disease; and (vii) serious trauma resulting in prosthesis failure or secondary revision surgery.
Operation method
All surgeries were performed by the same senior surgeon under general anaesthesia. Tourniquets.
were not routinely used unless patients were expected to suffer a prolonged operation or had a mild coagulation disorder (tourniquet pressure: 60 kPa). An anterior midline skin incision was made with a medial parapatellar approach. The hyperplastic synovium and part of the infrapatellar fat pad were removed. An intramedullary guide was used for the femur, and an extramedullary guide was used for the tibia. The bone surfaces were cleaned by high-pressure pulsatile lavage after osteotomy was completed. Then, the cement was injected under pressure into the cancellous bone to ensure better cement interdigitation, and a cemented knee joint prosthesis was installed. The patellar replacement was not performed in any patient.
Weight of implanted and removed material
We defined bone and soft tissues removed during the operation as the removed material and the knee prosthesis and bone cement as the implanted material. The removed material and residual polymerized cement were collected using two specimen bags during the operation and then weighed using a precision electronic balance with an accuracy of 0.0001 g (Fig. 1c-d). The manufacturers provided the weight of the specimen bags, prostheses, and one full bottle of cement. The weight of the bone cement in the whole bottle minus the weight of the unused cement was calculated as the weight of the used bone cement. We defined the change of the knee joint weight as the total weight of the implanted material minus the total weight of the removed material.
In order to eliminate the influence of different implants on the postoperative efficacy of patients, all knees received cruciate-retaining (CR) implants (Sigma PFC®, DePuy, America). Otherwise, patients were excluded from this study. The femoral and tibial parts of the prostheses of this brand were made of cobalt-chromium (Co-Cr) alloy, and the spacer was made of highly cross-linked polyethylene.
Multiple regression analysis of the influence on the weight of host removals during TKA surgery
Because the implant's weight is associated with shape, size, and material, it is hard for doctors to choose different weight implants. Therefore, we focused on the factors influencing the weight of removed bone and tissue during TKA surgery. In order to explore possible influencing factors, multiple regression analysis was performed with the weight of the removed bone and tissue as the dependent variable, and age, sex (male = 1, female = 2), BMI, K-L degree, preoperative HKA angle, and other factors as independent variables.
Postoperative treatment
All patients adopted the same nutritional intervention, antibiotic treatment, thrombosis prophylactic, perioperative pain management, and nursing and rehabilitation treatment programs. Immediately after anaesthesia, all patients began to perform isometric contractions of the quadriceps femoris and pumping ankle movements. If the drainage volume was less than 50 ml 24 ~ 48 h after the operation, the drainage tube was removed, and then the dressing was changed every three days. The incision was monitored for signs of infection during dressing changes. All patients were instructed to start walking on the ground with the help of walking aids 48 h after the operation. In addition, all patients began to use a CPM machine to assist with knee functional exercise on the third day after surgery, which lasted for 30 min every day and was converted to independent exercise after one week.
Observation of the curative effect at each time point postoperatively
All patients were evaluated by the Hospital for Special Surgery (HSS) score at two weeks, three months, and the last follow-up postoperatively to evaluate the knee joint recovery after TKA. HSS score is a reliable indicator for evaluating functional recovery after knee joint surgery. It can be used to describe the prognosis of patients in terms of pain, knee movement, and stability. HSS score was calculated by two surgeons who had more than three years of experience in orthopaedic surgery, and the final score was taken as the average of the two. If the results were quite different (differing by more than five points), a senior doctor was responsible for re-evaluation.
In addition, gait analysis data of patients at different postoperative periods were collected to evaluate their walking trajectory and gait changes. At each time point after the operation, patients underwent a gait analysis by an optical motion capture system (Vicon MX, England), which is mainly composed of infrared reflective balls, 10 MX infrared cameras, and information conversion controllers. When the patient moves, the movement tracks of the infrared reflective balls on the patient's body are captured and recorded by the MX cameras (Fig. 2). The motion signals are analyzed by the information converters, and the results are obtained and quantized. According to the clinical trial design, three major outcomes of interest were collected: spatiotemporal parameters, kinematic parameters, and mechanical parameters. There were six observation indexes among the spatiotemporal parameters: walking speed (cm/s), cadence (stride frequency, step/min), step length (cm), single-foot support phase (%), stance phase (%), and swing duration (%). The kinematic parameters included three indexes: hip rotational ROM, knee rotational ROM, and ankle rotational ROM. The plantar reaction force parameter mainly describes the plantar reaction force and includes the reaction on the front side, rear side, inner side, outer side, and the vertical reaction force. The ratio of the maximum reaction force produced by each area to the reaction force on the sole in the static state is the peak reaction force in all directions. To reduce errors, all spatiotemporal parameters were the average values obtained when patients walked for at least three minutes.

Computer simulation of 3D gait model. a Infrared reflective balls were attached to the lower limbs; b A grid plate could be used to calculate the walking distance. c Ten MX infrared cameras recorded the walking path. d Pressure plates were used to collect information on the patient's plantar reaction forces
Univariate regression analysis between IWKJ and HSS score and gait analysis
HSS score and parameters of gait analysis were collected at two weeks, three months, and at the last follow-up after the operation. Pearson's correlation analyses were used to analyze the correlation between the weight of knee joint changes and HSS score and gait analysis.
Sample size calculation
Correlations between the weight of knee joint changes and HSS score and indicators in gait analysis were assessed respectively using Pearson's correlation analyses. We assumed the correlation coefficient was ρ = 0.5, based on α = 0.05, β = 0.1 and a two-tailed test, according to the formula: n = 4 × {(Zα/2 + Zβ) / ln [(1 + ρ) ∕ (1 − ρ)]}2 + 3 [11], and the total sample size should be no less than 165.
Statistical analysis
Statistical analyses were performed using SPSS version 20 (SPSS, Chicago, USA). Quantitative data are presented as the mean and standard deviation (SD). Pearson's correlation analyses were used to analyze the correlation between the weight of knee joint changes and HSS score and gait analysis. Multivariate Linear regression analysis was used to describe the influencing factors on the weight of removed bone and tissue during TKA surgery. Statistical significance was set at p < 0.05.
Results
Preoperative demographic data of patients
A total of 275 patients met the inclusion criteria of this study; 65 patients were excluded for various reasons, and 210 patients were eventually included in the analysis (Fig. 3). All patients were followed up for at least two years. There were 56 males and 154 females, with an average age of 67.16 ± 7.31 years and an average BMI of 25.84 ± 3.75 kg/m2. According to the preoperative knee X-ray, the K-L stages of all patients' knees were III-IV grades. We measured the HKA angle of the patients to determine their deformity condition. 189 cases were of varus deformity and 18 cases were of valgus deformity (Table 1).

Flow diagram of enrolment. A total of 275 patients met the inclusion criteria of this study; 65 patients were excluded for various reasons, and 210 patients were eventually included in the analysis
Changes in knee joint weight after TKA
All patients enrolled in the study received the same brand of prostheses. The average total weight of prosthesis components was 453.71 ± 66.08 g (366.95 g—578.59 g), and the weight of implanted bone cement was 6.83 ± 2.70 g (2.06 g—11.98 g), and the weight of removed knee tissue was 162.70 ± 69.01 g (33.7 g—344.01 g). The increased weight of the knee joint was 298.98 ± 63.77 g (150.50 g—447.35 g). The results of multiple regression analysis showed that the k-L grade of the knee joint, the course of disease, and body weight were independent factors that affected the weight of the removed knee tissue (Fig. 4). Weight of removed knee tissue = -129.8 + 7.979 × course of disease + 38.39 × K-L degree + 1.331 × body weight.

Multiple linear regression analysis of the weight of removed knee tissue
Univariate regression analysis between IWKJ and HSS score after TKA
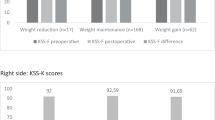
The HSS score was evaluated in all enrolled patients at two weeks, three months, and the final follow-up after TKA. Two weeks after surgery, the patients' HSS scores were 50.47 ± 14.95 and the increased knee weight was negatively correlated with the HSS score (p < 0.001, r = -0.432). Three months after surgery, the patients' HSS scores were 62.66 ± 13.68 and the increased knee weight was also negatively correlated with the HSS score (p = 0.01, r = -0.232). At the last follow-up, the patients' HSS scores were 82.27 ± 19.16, and there was no significant correlation between increased knee weight and HSS score (P = 0.103) (Fig. 5).

HSS score at each time point after TKA. In the early postoperative period, patients with lighter prostheses will get higher HSS scores. In the final investigation, there was no linear regression between the HSS score and IWKJ
Univariate regression analysis between IWKJ and gait analysis data at different time points after TKA
Two weeks after TKA
Two weeks after surgery, all the parameters of spatiotemporal parameters were negatively correlated with IWKJ (Fig. 6). The average stepping speed was 24.98 ± 12.28 cm/s (p < 0.001, r = 0.327); the average walk step per minute was 24.10 ± 9.08 (p = 0.004, r = 0.200), and each step length was 32.49 ± 6.19 cm (p < 0.001, r = 0.351). Among the kinematic parameters, the knee rotation ROM was negatively correlated with IWKJ (p = 0.018, r = -0.163). Among the mechanical parameters, outside foot load response was positively correlated with IWKJ (p = 0.022, r = 0.158). Other gait analysis parameters had no univariate linear relationship with IWKJ (p > 0.05).

Two weeks after TKA, univariate regression analysis was performed between IWKJ and gait analysis. A linear relationship with spatiotemporal parameters; B linear relationship with kinematic parameters; C linear relationship with mechanical parameters
Three months after TKA
Three months postoperatively, some indexes of gait analysis were influenced by IWKJ (Fig. 7). Patients' walking cadence was 71.70 ± 9.23 steps per minute, which was negatively correlated with IWKJ (p = 0.043, r = -0.102). Among the parameters of kinematic, both the knee rotation ROM and ankle rotation ROM were negatively correlated with IWKJ. Besides, there was a positive correlation between vertical foot load response and IWKJ (p = 0.025, r = 0.155). Other gait analysis data had no univariate linear relationship with IWKJ (p > 0.05).

Three months after TKA, univariate regression analysis was performed between IWKJ and gait analysis; A linear relationship with spatiotemporal parameters; B linear relationship with kinematic parameters; C linear relationship with mechanical parameters
At the last follow-up
We observed an interesting phenomenon that results at the last follow-up were completely different from those at two weeks and three months (Fig. 8). There was no clear linear regression relationship between each parameter of spatiotemporal parameters and mechanical parameters and IWKJ. In addition, there was no single factor correlation between the knee rotation ROM and the ankle rotation ROM and weight increase, while there was a positive correlation between the hip rotation ROM and IWKJ (p = 0.010, r = 0.179).

Last follow-up after TKA, univariate regression analysis was performed between IWKJ and gait analysis. A linear relationship with spatiotemporal parameters; B linear relationship with kinematic parameters; C linear relationship with mechanical parameters
Discussion
TKA and weight of knee prosthesis
With the increasing demand for TKA, a full understanding of all parameters related to this surgery is essential [12]. There have been few reports on variation in the weight of the knee joint, an important parameter after TKA. Gibon et al. confirmed that the density of human bone and soft tissues is far less than those of metal prostheses. Therefore, it is inevitable that patients will get an additional weight gain in their knees when they receive implants of similar size instead of their natural knees [7]. The previous study has shown that the weight of knee prosthesis was 3.94 times that of excised tissue, and the increased weight of the knee joint accounted for 0.5% of the total body weight [5]. Although this weight is not important for the whole body, a sharp increase in local knee weight may have significant side effects on the recovery of knee function. In our study, the results showed that the weight of the knee joint increased by 150.08 to 447.35 g, which is basically consistent with the results of previous studies[7, 8]. Our study suggests that patients' body weight, K-L staging, and disease duration are important factors that cause differences in resected knee tissue. KOA condition is often positively correlated with the course of disease, and the higher K-L grade. The narrower the joint space and the more severe subchondral sclerosis in imaging. Therefore, the above two factors can directly reflect the osteophyte hyperplasia of the affected knee joint. In addition, body weight is also closely related to the severity of KOA. Several studies have pointed out that excessive body weight will cause changes in the mechanical load of the knee joint, and intermediate products of fat cell metabolism will destroy the cartilage of the knee joint [13]. Despite these facts, few clinicians pay attention to the problems caused by the increased weight of the knee joint, such as whether it will increase the risk of surgical complications or affect knee joint function. The main purpose of this prospective clinical study is to investigate the effect of knee weight changes on knee function and gait after TKA.
Knee joint weight changes and the HSS score
The HSS score is often used to evaluate KOA severity or knee joint recovery after TKA[14]. It can be used to comprehensively describe a patient's knee joint function from many aspects. Our research shows that postoperative knee function and prosthesis weight were significantly negative correlation in the first three months, and after receiving a long time (more than two years) of functional exercise, the knee joint is gradually less affected by this change. The practical clinical problem is that the first three month is always the golden time for patients to exercise and recover. The poor functional recovery during this period will not only make patients under a certain psychological burden but also have a certain impact on the formation of postoperative joint stiffness and other complications later. Poor functional recovery of the knee joint in the early stage after TKA may be related to the decreased muscle strength around the knee after TKA. Ericsson et al. pointed out that with the progression of the KOA, the quadriceps muscle strength of patients gradually decreased [15]. In addition, a previous study has shown that the strength of the quadriceps muscle and hamstring muscle on the affected side knee joint was significantly lower than that on the healthy side after TKA [16]. At our last follow-up, almost all patients had significantly higher scores than that at two weeks after TKA. We believe that the score improvement is related to the specific content of the grading system. Two weeks after the operation, the patients were in poor physical condition, and most of them needed a walking aid. It was difficult for patients to walk for a long distance, or, up or downstairs, so the functional score at this time would be very low.
Knee joint weight changes and gait analysis
Previous studies have shown a significant difference in gait on the affected side compared to the healthy side in patients after TKA [17]. We wanted to know whether this difference was related to the change in the knee joint weight. In addition, the spatiotemporal parameters of gait analysis can compensate for the deficiency of the HSS score. Meikle's research showed that there was no significant difference in the results of gait analysis in amputees wearing prostheses of different weights, and interestingly, patients were more inclined to choose heavier prostheses [18]. However, our research revealed contrary results: in the early stage after TKA, patients with heavier prostheses showed a slower pace and shorter stride. The main difference between our results and those reported by Ben is that their research objects were patients who had undergone amputation long before the study. The lower limb prosthesis was worn much like an article of clothing, and there was almost no difference in muscle strength between the affected limb and the healthy limb. Our research objects were patients who had recently undergone surgical treatment; at this time, the strength of the quadriceps femoris muscles and hamstring muscles of the affected side was significantly lower than that of the healthy side [19]. The difference in postoperative muscle strength may be an important factor affecting the gait changes of patients.
At the last follow-up, we observed an interesting phenomenon that there was no linear regression relationship between either spatiotemporal parameters or mechanical parameters and IWKJ, while hip joints gained a larger range of motion. We think it might have something to do with the muscles that control hip movement, which become stronger as patients tolerate heavier implants. This finding is consistent with Kim's [20]. In their latest research, a new prosthesis made of titanium (Ti) alloy was used in the clinic, and the weight of the prosthesis was similar to that of the removed material. Due to the limitations of material science and technology, we are now unable to perform TKA with lighter prostheses such as Ti alloy. However, I believe that with more attention paid to the weight parameter of the prosthesis by clinicians and manufacturers, lightweight prostheses will be widely available soon.
Limitations
This study has some limitations. First of all, due to the lack of literature for reference, we defined the bone and soft tissue removed during TKA as the removed material. Obviously, after TKA, it is difficult for the bone to regrow in a short time, but we cannot judge whether soft tissues will return to the preoperative state in a short time given that the post-operative inflammatory state may lead to soft tissue hyperplasia and fibrosis. So the regeneration may be significant. This parameter might worsen the feeling of having a heavy knee after the procedure or might lead to poor outcomes. Although magnetic resonance imaging (MRI) can reflect soft tissue hyperplasia to some extent, most patients did not agree to undergo an MRI examination, so we could not obtain these data. There's another thing I have to point out about tissue weighing, which is that we didn't measure the synovial fluid in our study. When we opened the knee joint, it was very difficult to accurately collect the synovial fluid under certain pressure. We tried to calculate the synovial fluid with an aspirator, but the synovial fluid can easily infiltrate into the tissue or get mixed with the blood. In addition, during the process of expanding the pulp cavity in TKA, a small amount of bone powder cannot be collected. However, we believe that this amount of bone powder is not significant compared to the amount of bone collected. Second, due to the limitation of examination costs, we failed to collect the patients' gait analysis data before surgery, which could have a certain reference value for evaluating the patients' postoperative gait changes. In the following clinical observation, we will focus on this part. Finally, our longest follow-up time was less than six years, so long-term follow-up data to assess the long-term effects of changes in knee weight on knee function is lacking.
Conclusion
All Patients undergoing TKA had varying degrees of increased knee weight. The increased weight was 298.98 ± 63.77 g. Patients' body weight, K-L staging, and disease duration are important factors that cause differences in resected knee tissue. Three months after the operation, the changes in knee joint weight had a negative correlation with the HSS score. Meanwhile, it had varying degrees of linearity with gait parameters. However, the influence of weight diminished over time.
Availability of data and materials
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- KOA:
-
Knee osteoarthritis
- TKA:
-
Total knee arthroplasty
- BMI:
-
Body mass index
- HSS:
-
Hospital for special surgery
- ROM:
-
Range of motion
- MRI:
-
Magnetic resonance imaging
- IWKJ:
-
Increased weight of the knee joint
- K-L grade:
-
Kellgren and Lawrence grade
References
Lawrence RC, Felson DT, Helmick CG, Arnold LM, Choi H, Deyo RA, Gabriel S, Hirsch R, Hochberg MC, Hunder GG, Jordan JM, Katz JN, Kremers HM, Wolfe F, National Arthritis Data Workgroup. Estimates of the prevalence of arthritis and other rheumatic conditions in the United States. Part II. Arthritis Rheum. 2008;58(1):26–35.
Yates AJ Jr, McGrory BJ, Starz TW, Vincent KR, McCardel B, Golightly YM. AAOS appropriate use criteria: optimizing the non-arthroplasty management of osteoarthritis of the knee. J Am Acad Orthop Surg. 2014;22(4):261–7.
Yan JR, Oreskovich S, Oduwole K, Horner N, Khanna V, Adili A. Cement Waste During Primary Total Knee Arthroplasty and its Effect on Cost Savings: An Institutional Analysis. Cureus. 2018;10(11):e3637.
Inacio MCS, Graves SE, Pratt NL, Roughead EE, Nemes S. Increase in Total Joint Arthroplasty Projected from 2014 to 2046 in Australia: A Conservative Local Model With International Implications. Clin Orthop Relat Res. 2017;475(8):2130–7.
Zhu ZY, Zheng X, Guo KJ, Sun ZQ, Zhao FC, Yi LH, Tang JL. Effect of joint weight variance on prognosis of total knee arthroplasty. Orthopedic Journal of China. 2018;26(15):1345–9.
Rossi B, Jayasekera N, Kelly FA, Eyres K. Patients’ Perception of Bone and Tissue Excision, and the Size and Weight of Prostheses at Total Knee Arthroplasty. Surg J (N Y). 2017;3(3):e110–2.
Gibon E, Mouton A, Passeron D, Le Strat V, Graff W, Marmor S. Doctor, what does my knee arthroplasty weigh? J Arthroplasty. 2014;29(11):2091–4.
Sivarasu S, Mathew L. Techniques in the development of a lower weight medical implants and strength validation using finite element methods. J Long Term Eff Med Implants. 2009;19(1):49–54.
Kaneda K, Harato K, Oki S, Yamada Y, Nakamura M, Nagura T, Jinzaki M. Increase in tibial internal rotation due to weight-bearing is a key feature to diagnose early-stage knee osteoarthritis: a study with upright computed tomography. BMC Musculoskelet Disord. 2022;23(1):253.
Diao N, Yu F, Yang B, Ma L, Yin H, Guo A. Association between changes in hip-knee-ankle angle and hindfoot alignment after total knee arthroplasty for varus knee osteoarthritis. BMC Musculoskelet Disord. 2021;22(1):610.
Noordzij M, Dekker FW, Zoccali C, Jager KJ. Sample size calculations. Nephron Clin Pract. 2011;118(4):c319–23.
Liu J, Wilson L, Poeran J, Fiasconaro M, Kim DH, Yang E, Memtsoudis S. Trends in total knee and hip arthroplasty recipients: a retrospective cohort study. Reg Anesth Pain Med. 2019;44(9):854–9.
Schadler P, Lohberger B, Thauerer B, Faschingbauer M, Kullich W, Stradner MH, Husic R, Leithner A, Steinecker-Frohnwieser B. Fatty Acid-Binding Protein 4 (FABP4) Is Associated with Cartilage Thickness in End-Stage Knee Osteoarthritis. Cartilage. 2021;13(2):1165S-1173S.
Zhang Z, Chai W, Zhao G, Zhang Q, Chen Z, Wang X, Wei P, Zhang Y, Jin Z, Qiu Y. Association of HSS score and mechanical alignment after primary TKA of patients suffering from constitutional varus knee that caused by combined deformities: a retrospective study. Sci Rep. 2021;11(1):3130.
Ericsson YB, McGuigan FE, Akesson KE. Knee pain in young adult women- associations with muscle strength, body composition and physical activity. BMC Musculoskelet Disord. 2021;22(1):715.
Moon YW, Kim HJ, Ahn HS, Lee DH. Serial Changes of Quadriceps and Hamstring Muscle Strength Following Total Knee Arthroplasty: A Meta-Analysis. PLoS One. 2016;11(2):e0148193.
Choi JH, Kim BR, Kim SR, Nam KW, Lee SY, Suh MJ. Performance-based physical function correlates with walking speed and distance at 3 months post unilateral total knee arthroplasty. Gait Posture. 2021;87:163–9.
Meikle B, Boulias C, Pauley T, Devlin M. Does increased prosthetic weight affect gait speed and patient preference in dysvascular transfemoral amputees? Arch Phys Med Rehabil. 2003;84(11):1657–61.
Christensen JC, Capin JJ, Hinrichs LA, Aljehani M, Stevens-Lapsley JE, Zeni JA. Gait mechanics are influenced by quadriceps strength, age, and sex after total knee arthroplasty. J Orthop Res. 2021;39(7):1523–32.
Kim JK, Park IW, Ro DH, Mun BS, Han HS, Lee MC. Is a Titanium Implant for Total Knee Arthroplasty Better? A Randomized Controlled Study J Arthroplasty. 2021;36(4):1302–9.
Acknowledgements
Not applicable.
Funding
This study was supported by the National Natural Science Foundation of China (81902244, data collection), the Natural Science Foundation of Jiangsu Province (BK20201154, data analysis), Jiangsu Provincial Medical Youth Talent (QNRC2016801, interpretation of data), and Xuzhou Science and Technology Innovation Project (KC19063, data collection and analysis).
Author information
Authors and Affiliations
Contributions
ZZ and TT carried out the acquisition and interpretation of data, and drafted the manuscript substantially. SP and CH carried out the clinical data collection. ZZ and ZS carried out the radiological measurements, the acquisition and interpretation of data. RR and ZH carried out the statistical analysis. SL, XZ, and KG carried out the design of this study, revised the manuscript critically. All authors gave final approval of the version to be published.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
This study was approved by Xuzhou Medical University Ethics Committee. Written informed consent was obtained from all participants included in the study.
Consent for publication
Not Applicable.
Competing interests
All authors declare that they have no competing interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Zhu, Z., Tang, T., Pan, S. et al. Effect of knee joint weight change on knee function recovery and gait after total knee arthroplasty. BMC Musculoskelet Disord 23, 694 (2022). https://doi.org/10.1186/s12891-022-05647-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12891-022-05647-5