
Abstract
Background
Although there are reports on the effectiveness of microendoscopic laminotomy using a spinal endoscope as decompression surgery for lumbar spinal stenosis, predicting the improvement of low back pain (LBP) still poses a challenge, and no clear index has been established. This study aimed to investigate whether microendoscopic laminotomy for lumbar spinal stenosis improves low back pain and determine the preoperative predictors of residual LBP.
Methods
In this single-center retrospective study, we examined 202 consecutive patients who underwent microendoscopic laminotomy for lumbar spinal stenosis with a preoperative visual analog scale (VAS) score for LBP of ≥40 mm. The lumbar spine Japanese Orthopaedic Association (JOA), and VAS scores for LBP, leg pain (LP), and leg numbness (LN) were examined before and at 1 year after surgery. Patients with a 1-year postoperative LBP-VAS of ≥25 mm composed the residual LBP group. The preoperative predictive factors associated with postoperative residual LBP were analyzed.
Results
JOA scores improved from 14.1 preoperatively to 20.2 postoperatively (p < 0.001), LBP-VAS improved from 66.7 to 29.7 mm (p < 0.001), LP-VAS improved from 63.8 to 31.2 mm (p < 0.001), and LN-VAS improved from 63.3 to 34.2 mm (p < 0.001). Ninety-eight patients (48.5%) had a postoperative LBP-VAS of ≥25 mm. Multiple logistic regression analysis revealed that Modic type 1 change (odds ratio [OR], 5.61; 95% confidence interval [CI], 1.68–18.68; p = 0.005), preoperative VAS for LBP ≥ 70 mm (OR, 2.19; 95% CI, 1.17–4.08; p = 0.014), and female sex (OR, 1.98; 95% CI, 1.09–3.89; p = 0.047) were preoperative predictors of residual LBP.
Conclusion
Microendoscopic decompression surgery had an ameliorating effect on LBP in lumbar spinal stenosis. Modic type 1 change, preoperative VAS for LBP, and female sex were predictors of postoperative residual LBP, which may be a useful index for surgical procedure selection.
Similar content being viewed by others


Background
Lumbar spinal stenosis (LSS) is a disease in which the dural tract and nerve roots are compressed because of degeneration of the intervertebral disk and facet joints, causing symptoms such as sciatica, intermittent claudication, and low back pain (LBP) [1, 2]. The number of patients suffering from LSS is expected to increase further in the future due to an aging population. Most patients with LSS initially receive conservative treatment to manage their symptoms. Surgery is an effective treatment option when conservative methodologies fail [2, 3]. Generally, decompression surgery is performed when there is associated lower limb pain and gait disturbance, and fusion surgery is adopted for patients with LBP, spondylolisthesis, lumbar instability, and scoliosis [4, 5].
Microendoscopic laminotomy (MEL) is a minimally invasive surgical procedure that incorporates the use of a spinal endoscope. This procedure, which is derived from the microendoscopic discectomy technique, was developed to treat patients with LSS [6, 7]. The advantages of this procedure include a small incision, excellent visualization, gentle tissue dissection, and bilateral decompression via a unilateral tubular approach. MEL has been reported to be effective for patients with LSS with/without degenerative spondylolisthesis. Additionally, MEL has been shown to provide a good Japanese Orthopedic Association (JOA) score recovery rate, improvement of LSS symptoms, as indicated by the Roland-Morris Disability Questionnaire, and short-form 36 scores at 5-year follow-ups [7].
In the procedure performed to improve lower limb symptoms, patients often report an improvement in LBP. It has been reported that open decompression surgery has an ameliorating effect on LBP [8]. However, it is difficult to predict the improvement of LBP with decompression surgery. The purpose of this study was to investigate whether MEL, a motion-preserving decompression surgery that uses a spinal endoscope, improves LBP with LSS, and to determine the preoperative predictors of residual LBP after surgery.
Methods
This retrospective cohort study was approved by institutional review board of Wakayama Medical University (No. 2945). Written informed consent for involvement in this study was obtained from all patients included. In total, 220 consecutive patients who underwent MEL for LSS between July 2014 and December 2018 were enrolled. Patients who underwent microendoscopic discectomy for lumbar disc herniation were excluded from this study. The LSS diagnoses were made based on the presence of specific clinical symptoms, such as LBP, leg pain, numbness, and intermittent claudication, as well as on the existence of radiological spinal stenosis on magnetic resonance imaging (MRI) that confirmed the neurological symptoms. The inclusion criteria were as follows: (1) patients who underwent MEL for LSS due to failure of conservative treatment, (2) patients who had a preoperative baseline LBP of at least 40 mm on the 100-mm visual analog scale (VAS). Patients were excluded if they had a history of lumbar fusion surgery.
The surgeries were performed using a METRx endoscopic system (Medtronic Sofamor Danek, Memphis, TN) by 11 spine surgeons who were certified as endoscopic spine surgeons by the Japanese Orthopedic Association. To perform the spinal decompression, a small paramedian skin incision of approximately 16 mm in length was made to target the interlaminar space in each decompressed level. The central canal and bilateral lateral recess were decompressed for all the patients through a unilateral tubular approach (Fig. 1). While performing the decompression, the facet joints were preserved using a high-speed drill with a long curved endoscopic bit and curved Kerrison rongeurs, as previously reported [7].

A Microendoscopic laminotomy (MEL) schema. B and C Representative axial computed tomography (CT) images obtained preoperatively (B) and after decompression by MEL (C)
As clinical outcomes, the lumbar spine Japanese Orthopaedic Association (JOA) score and VAS scores for LBP, leg pain, and leg numbness were examined before and at 1 year after surgery. The minimal clinically important difference (MCID) of the VAS value improvement was determined as ≥20 mm [9], and the achievement rate of the MCID for LBP improvement was investigated.
Subsequently, for the purpose of examining preoperative predictors of postoperative residual LBP, patients with a 1-year postoperative LBP-VAS of ≥25 mm or those requiring additional surgery for residual LBP within 1 year after MEL surgery were considered to have postoperative residual LBP. The factors that may be associated with postoperative residual LBP, including age, sex, body mass index (BMI), disease duration, number of decompressed levels, and preoperative clinical scores (VAS scores) were investigated. Preoperative radiological findings, such as spondylolisthesis (Meyerding classification), degenerative scoliosis (Cobb angle ≥20°), spinal instability (anterior translation of the affected motion segment exceeding 10% of the AP vertebral depth or intervertebral rotation exceeding 10° [10]), intervertebral disk degeneration (Pfirrmann classification), endplate disorders (Modic changes [11]), disk space vacuum phenomenon, old vertebral fractures, and sagittal malalignment (sagittal modifiers [12]) were also evaluated. Spondylolisthesis, scoliosis, spinal instability, old vertebral fractures, and sagittal malalignment were measured using plain radiographs, while intervertebral disc degeneration and endplate disorders were evaluated on MRI and disk space vacuum phenomenon was evaluated by computed tomography. Spinal instability, intervertebral disk degeneration, endplate disorders, and disk space vacuum phenomenon were all assessed at the most severe of the surgically treated intervertebral levels. All the measurements were performed by another spine surgeon who was not involved in the surgeries.
Statistical analysis
We performed a univariate analysis to assess whether these factors were related to postoperative residual LBP. The Student’s t-test was used to examine differences in age, BMI, disease period, and VAS scores for LBP, leg pain, and leg numbness between patients with postoperative VAS for LBP ≥ 25 mm as compared to postoperative VAS for LBP < 25 mm. The Chi-square test was used to examine the differences in sex, number of decompressed levels, spondylolisthesis, degenerative scoliosis, spinal instability, disk degeneration, endplate disorder, vacuum phenomenon of disk space, old vertebral fractures, sagittal malalignment, and preoperative VAS scores for LBP between patients with postoperative VAS for LBP ≥ 25 mm and those with postoperative VAS for LBP < 25 mm. The preoperative VAS for LBP was evaluated as 2 values by setting a threshold value through a simple logistic analysis. We performed multiple logistic regression analyses using the residual LBP as the dependent variable, with explanatory variables including factors that showed a p value of < 0.2 in the univariate analysis and factors that have been reported as poor factors for decompression surgery (spondylolisthesis [13, 14], intervertebral instability [15], scoliosis [16], preoperative LBP [4, 5]). The Hosmer-Lemeshow test was performed for the suitability of multiple logistic models.
Statistical analyses were performed using JMP Pro 13 (SAS Institute Japan, Tokyo, Japan) and SPSS Statistics Ver. 28 (SPSS Inc., Chicago, IL). P values < 0.05 were considered statistically significant.
Results
Altogether, 202 patients (males, n = 109; females, n = 93: follow-up rate, 91.8%) who had been observed for > 1 year after surgery were enrolled. Table 1 shows the demographic data of all patients. Patients’ average age at surgery was 72.4 years (range, 51–91 years). The average follow-up period was 29.8 months (range, 12–64 months). All the patients had neurogenic claudication. A total of 134 patients had radicular pain, 119 had bilateral leg numbness, and 51 experienced both symptoms. A total of 170 patients underwent surgery for central stenosis, and the other 32 patients were treated for lateral recess stenosis. In addition, 98 of the patients had spondylolisthesis. There were 105 patients with single-level, 71 with two-level, 23 with three-level, and three with four-level decompression.
Improvement of LBP
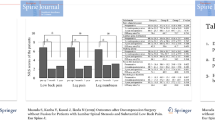
The JOA score improved from 14.1 preoperatively to 20.2 postoperatively (p < 0.001), VAS score for LBP improved from 66.7 mm to 29.7 mm (p < 0.001), VAS score for leg pain improved from 63.8 mm to 31.2 mm (p < 0.001), and VAS score for leg numbness improved from 63.3 mm to 34.2 mm (p < 0.001) (Table 2). Apart from the JOA score and VAS score for leg pain, VAS score for LBP also significantly improved. The MCID for the improvement of VAS score for LBP was achieved in 148 patients (73.3%).
Predictive factors for residual LBP
At 1 year after surgery, 98 patients (including five who underwent salvage with fusion surgery) had a VAS for LBP ≥ 25 mm. Factors that showed a p value of < 0.2 in the univariate analysis were female sex (p = 0.034), BMI (p = 0.141), scoliosis (p = 0.003), Modic type 1 change (p ≤ 0.001), pelvic tilt ≥30° (p = 0.113), and preoperative VAS for LBP ≥ 70 mm (p = 0.001) (Table 3).
Multiple logistic regression analyses showed that Modic type 1 change (odds ratio [OR], 5.61; 95% confidence interval [CI], 1.68–18.68; p = 0.005), preoperative VAS for LBP ≥ 70 mm (OR, 2.19; 95% CI, 1.17–4.08; p = 0.014), and female sex (OR, 1.98; 95% CI, 1.09–3.89; p = 0.047) were predictors of postoperative residual LBP (Table 4). On the other hand, spondylolisthesis, intervertebral instability, and sagittal malalignment were not predictors of LBP residuals.
Discussion
In the selection of a surgical procedure for LSS, it has been reported that decompression alone yields inferior results compared with fusion surgery in patients with LBP [4, 5] or radiological abnormalities, such as spondylolisthesis and intervertebral instability [14,15,16]. For this reason, fusion surgery has been widely accepted as a surgical treatment for LSS with LBP. However, some studies have reported that decompression surgery via the open method performed for improving lower limb pain also has a secondary effect on ameliorating LBP [8, 17]. This suggests that decompression alone may provide satisfactory results in some LSS patients with LBP. In this study, the average VAS score of patients whose VAS score for LBP was ≥40 mm before surgery improved from 66.7 mm before surgery to 29.7 mm after surgery. The MCID for improvement of VAS score was achieved in > 70% of the patients. This result highlights the effect of MEL on LBP improvement. The mechanism by which decompression surgery reduces LBP with LSS includes (1) the direct effects on radicular LBP by decompression of the cauda equina and nerve roots, (2) improvement of LBP associated with leg pain-alleviating posture improvements, (3) denervation around facet joints by a surgical procedure, (4) improvement of physical function or gait disturbance, and (5) psychological effects [8, 18]. However, it is difficult to isolate the exact cause in cases where many factors are involved. The surgical technique used in the present study employed a spinal endoscope for decompression without damaging the facet joints and paravertebral muscles. Therefore, it is difficult to consider the effect of denervation around the facet joint as an improvement mechanism for LBP in the present study. Consequently, it is presumed that these causes are due to nerve decompression or postural changes via MEL; however, further investigation is needed to clarify this mechanism.
As per the preoperative predictive factors, patients were divided according to a postoperative LBP VAS score of 25 mm. We adopted the VAS score of 25 mm, since the pain level less than that value is reported as acceptable pain for degenerative disorders [19]. In the univariate analysis, female sex, BMI, scoliosis, Modic type 1 change, pelvic tilt (≥30°), and preoperative VAS for LBP were identified as predictors of postoperative residual LBP. In the multiple logistic regression analyses, Modic type 1 change of endplate, preoperative VAS for LBP, and female sex remained predictors of postoperative residual LBP. No problem with multicollinearity was noted because all variance inflation factors are < 10. The Hosmer-Lemeshow test was performed for the suitability of the multiple logistic model, and no problems were observed.
Modic type 1 endplate disorder is a change in T1 low intensity and T2 high intensity, which reflects inflammatory findings [11], and its association with LBP has been reported [20]. LBP has been related to histological abnormalities, such as inflammatory cytokines and nerve ingrowth into the vertebral endplates [21, 22], and it is reasonable that decompression alone does not improve the pain. Preoperative VAS for LBP was also associated with residual LBP. In the present study, a model was created by converting the preoperative VAS for LBP into two values with a threshold of 70 mm derived by a simple logistic analysis to make it clinically useful. However, since the area under the receiver operating characteristic curve is 0.62, it should be determined whether or not this threshold is appropriate. Either way, indications for decompression surgery may need to be carefully considered for patients with severe preoperative low back pain. Female sex was also associated with residual LBP. In the postoperative clinical results of LSS, it has been reported that female sex has a negative effect on LBP, lower limb pain, and the Oswestry disability index [4, 23]. The results of this study were consistent with those of previous reports. However, the coexistence of osteoporosis or a decrease of the trunk muscle mass, which was not investigated in the present study, may affect the association between female sex and residual LBP [24, 25]. Moreover, it should be noted that women in the general population are more likely to have LBP [26, 27]. Therefore, we believe that the results of this study do not necessarily indicate the need to limit the indications of decompression surgery for women. On the other hand, the morphological abnormalities such as spondylolisthesis, spinal instability, and sagittal malalignment were not related to postoperative residual LBP in the present study. One factor that contributed to the conflicting results between the present study and previous reports may be that MEL was superior to conventional open decompression in preserving posterior tissues, such as paravertebral muscles and facet joints. This result suggests that there is no need to select fusion surgery just due to these abnormalities in imaging findings, and there are patients in whom satisfactory results can be obtained only by decompression surgery.
There are some limitations in this study. First, this is a retrospective cohort study with a small number of patients. Future prospective studies with a larger patient population are needed. Second, the follow-up period in this study was short. However, since it is intended for LBP, which can be affected by multiple factors, we believe that the evaluation of short-term postoperative results is appropriate for the purpose of clearly evaluating the improving effect of surgery. Third, there is a risk of selection bias, and there is no comparison with fusion surgery. However, this study includes a considerable number of patients with spondylolisthesis or spinal instability, and there have been multiple cases of LBP improvement with decompression surgery alone. These results may provide valuable information for patients undergoing surgery.
Conclusions
Microendoscopic decompression surgery for LSS has an ameliorating effect on LBP. Modic type 1 change of endplate, preoperative VAS for LBP, and female sex are predictors of postoperative residual LBP, which may be a useful index for surgical procedure selection. There is no need to select fusion surgery for these cases due to imaging abnormalities, such as spondylolisthesis, spinal instability, and sagittal malalignment.
Availability of data and materials
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- MEL:
-
Microendoscopic laminotomy
- LSS:
-
Lumbar spinal stenosis
- LBP:
-
Low back pain
- VAS:
-
Visual analogue scale
- JOA:
-
Japanese Orthopaedic Association
- BMI:
-
Body mass index
References
Amundsen T, Weber H, Lilleås F, Nordal HJ, Abdelnoor M, Magnaes B. Lumbar spinal stenosis. Clinical and radiologic features. Spine. 1995;20(10):1178–86.
Katz JN, Harris MB. Lumbar spinal stenosis. N Engl J Med. 2008;358(8):818–25.
Malmivaara A, Slätis P, Heliövaara M, Sainio P, Kinnunen H, Kankare J, et al. Surgical or nonoperative treatment for lumbar spinal stenosis?: a randomized controlled trial. Spine. 2007;32(1):1–8.
Aalto TJ, Malmivaara A, Kovacs F, Herno A, Alen M, Salmi L, et al. Preoperative predictors for postoperative clinical outcome in lumbar spinal stenosis: systematic review. Spine. 2006;31(18):E648–63.
Omidi-Kashani F, Hasankhani EG, Ashjazadeh A. Lumbar spinal stenosis: who should be fused? An updated review. Asian Spine J. 2014;8(4):521.
Minamide A, Yoshida M, Yamada H, Nakagawa Y, Kawai M, Maio K, et al. Endoscope-assisted spinal decompression surgery for lumbar spinal stenosis. J Neurosurg Spine. 2013;19(6):664–71.
Minamide A, Yoshida M, Yamada H, Nakagawa Y, Hashizume H, Iwasaki H, et al. Clinical outcomes after microendoscopic laminotomy for lumbar spinal stenosis: a 5-year follow-up study. Eur Spine J. 2015;24(2):396–403.
Jones ADR, Wafai AM, Easterbrook AL. Improvement in low back pain following spinal decompression: observational study of 119 patients. Eur Spine J. 2014;23(1):135–41.
Hägg O, Fritzell P, Nordwall A. The clinical importance of changes in outcome scores after treatment for chronic low back pain. Eur Spine J. 2003;12(1):12–20.
Hanley EN Jr. The indications for lumbar spinal fusion with and without instrumentation. Spine. 1995;20(24 Suppl):143S–53S.
Modic MT, Steinberg PM, Ross JS, Masaryk TJ, Carter JR. Degenerative disk disease: assessment of changes in vertebral body marrow with MR imaging. Radiology. 1988;166(1):193–9.
Schwab F, Ungar B, Blondel B, Buchowski J, Coe J, Deinlein D, et al. Scoliosis Research Society—Schwab adult spinal deformity classification: a validation study. Spine. 2012;37(12):1077–82.
Martin CR, Gruszczynski AT, Braunsfurth HA, Fallatah SM, O'Neil J, Wai EK. The surgical management of degenerative lumbar spondylolisthesis: a systematic review. Spine. 2007;32(16):1791–8.
Ghogawala Z, Dziura J, Butler WE, Dai F, Terrin N, Magge SN, et al. Laminectomy plus fusion versus laminectomy alone for lumbar spondylolisthesis. N Engl J Med. 2016;374(15):1424–34.
Yone K, Sakou T, Kawauchi Y, Yamaguchi M, Yanase M. Indication of fusion for lumbar spinal stenosis in elderly patients and its significance. Spine. 1996;21(2):242–8.
Ploumis A, Transfledt EE, Denis F. Degenerative lumbar scoliosis associated with spinal stenosis. Spine J. 2007;7(4):428–36.
Crawford CH, Glassman SD, Mummaneni PV, Knightly JJ, Asher AL. Back pain improvement after decompression without fusion or stabilization in patients with lumbar spinal stenosis and clinically significant preoperative back pain. J Neurosurg Spine. 2016;25(5):596–601.
Ikuta K, Masuda K, Tominaga F, Sakuragi T, Kai K, Kitamura T, et al. Clinical and radiological study focused on relief of low back pain after decompression surgery in selected patients with lumbar spinal stenosis associated with grade I degenerative spondylolisthesis. Spine. 2016;41(24):E1434–43.
Mannion AF, Balagué F, Pellisé F, Cedraschi C. Pain measurement in patients with low back pain. Nat Clin Pract Rheumatol. 2007;3(11):610–8.
Toyone T, Takahashi K, Kitahara H, Yamagata M, Murakami M, Moriya H. Vertebral bone-marrow changes in degenerative lumbar disc disease. An MRI study of 74 patients with low back pain. J Bone Joint Surg Br. 1994;76(5):757–64.
Ohtori S, Inoue G, Ito T, Koshi T, Ozawa T, Doya H, et al. Tumor necrosis factor-immunoreactive cells and PGP 9.5-immunoreactive nerve fibers in vertebral endplates of patients with discogenic low back pain and Modic type 1 or type 2 changes on MRI. Spine. 2006;31(9):1026–31.
Rahme R, Moussa R. The modic vertebral endplate and marrow changes: pathologic significance and relation to low back pain and segmental instability of the lumbar spine. Am J Neuroradiol. 2008;29(5):838–42.
Mariconda M, Zanforlino G, Celestino GA, Brancaleone S, Fava R, Milano C. Factors influencing the outcome of degenerative lumbar spinal stenosis. Clin Spine Surg. 2000;13(2):131–7.
Ohtori S, Akazawa T, Murata Y, Kinoshita T, Yamashita M, Nakagawa K, et al. Risedronate decreases bone resorption and improves low back pain in postmenopausal osteoporosis patients without vertebral fractures. J Clin Neurosci. 2010;17(2):209–13.
Sasaki T, Yoshimura N, Hashizume H, Yamada H, Oka H, Matsudaira K, et al. MRI-defined paraspinal muscle morphology in Japanese population: the Wakayama spine study. PLoS One. 2017;12(11):e0187765.
Hoy D, Bain C, Williams G, March L, Brooks P, Blyth F, et al. A systematic review of the global prevalence of low back pain. Arthritis Rheum. 2012;64(6):2028–37.
Teraguchi M, Yoshimura N, Hashizume H, Muraki S, Yamada H, Oka H, et al. The association of combination of disc degeneration, end plate signal change, and Schmorl node with low back pain in a large population study: the Wakayama spine study. Spine J. 2015;15(4):622–8.
Acknowledgements
Not applicable.
Funding
The authors declare that they have no sources of funding for research reported.
Author information
Authors and Affiliations
Contributions
Research conception and design: RT, HY, HH. Data collection: RT, HI, YY, AM, YN, ST, MT, KN, SM, TK, MY. Statistical analysis: RT, HH. Interpretation of data: RT, HY. Drafting the manuscript: RT. Manuscript review: HI, HY. Study supervision: HY. Approval of the final manuscript: all the authors listed above.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study design was approved by the institutional review board of Wakayama Medical University (approval number: 2945). The patients and/or their family members were informed that the patient data would be submitted for publication, and their written consent was obtained.
Consent for publication
Not Applicable.
Competing interests
The authors declare that they have no competing interests and no sources of financial supports.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Taiji, R., Iwasaki, H., Hashizume, H. et al. Improving effect of microendoscopic decompression surgery on low back pain in patients with lumbar spinal stenosis and predictive factors of postoperative residual low back pain: a single-center retrospective study. BMC Musculoskelet Disord 22, 954 (2021). https://doi.org/10.1186/s12891-021-04844-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12891-021-04844-y