
Abstract
Background
To prevent recurrent ankle sprain, it is important to clarify the pathology of chronic ankle instability (CAI). An association has been reported between CAI and abnormalities of foot posture and ankle alignment. There is no consensus on the types of these abnormalities that occur in individuals with CAI. The objective of this systematic review is to clarify the relevance of abnormality of foot posture and ankle alignment for CAI.
Methods
A systematic computerized literature search was performed of the PubMed, CINAHL, SPORTDiscus, Web of Science, and the Cochrane Register of Clinical Trials databases. The selected studies either compared CAI patients with a control group or CAI ankles with contralateral healthy ankles and specifically reported foot posture and alignment of the ankle in the outcomes. They were written in English and published prior to June 2021. The methodological quality of the included studies was evaluated using a 16-question index. Data were extracted independently by two reviewers, and the certainty of evidence was assessed using GRADE approach.
Results
Sixteen studies including 872 patients of high to low methodological quality were included. These showed there was significant anterior displacement and internal rotation of the talus in CAI ankles (low evidence), but there was no consensus on fibular alignment or foot posture.
Conclusions
This review showed there was significant anterior displacement and internal rotation of the talus in CAI ankles but found no consensus on the characteristics of fibular and foot alignment. Further investigations are required to clarify the characteristic foot and ankle malalignment in CAI to facilitate the development of efficient interventions.
Similar content being viewed by others


Explore related subjects
Find the latest articles, discoveries, and news in related topics.Background
Ankle sprain is one of the most common ankle injuries, with a recurrence rate exceeding 50% [1]. Ankle sprains cause mechanical and functional disorders of the ankle joint, and repeated ankle sprains can result in chronic ankle instability (CAI). The main symptoms of CAI are the ankle “giving way”, perceived ankle instability, and further recurrence of ankle sprain [2]. In addition, CAI associated with repeated ankle sprain leads to an increased risk of future ankle osteoarthritis [1]. Recurrent ankle sprains are associated with dysfunction such as limited range of ankle dorsiflexion, decreased external muscle strength, and static and dynamic postural stability deficit [1]. Furthermore, CAI is associated with a decrease in health-related quality of life [3], so clarifying the pathology of CAI is important for developing interventions that can prevent recurrent ankle sprain.
Individuals with CAI experience repeated ankle sprains caused by various dysfunctions, such as pathologic laxity, neuromuscular inhibition, balance deficit, and muscle weakness, including arthrokinematic restrictions caused by abnormal foot and ankle joint alignment such as talar anterior displacement or cavus foot deformity [4]. Abnormal anterior displacement or internal rotation of talus can affect the talar cartilage strain and contribute to the development of osteoarthritis in the future [5, 6]. Abnormalities of foot posture, such as pes planus, have also been noted to potentially alter lower limb kinematics, including increase rearfoot eversion or tibial internal rotation during running, and may thus increase the risk of medial tibial stress syndrome or patellofemoral pain [7]. Abnormalities associated with CAI thus need to be addressed to mitigate long-term consequences.
Rearfoot varus has been reported as a risk factor for CAI [8], and is considered to contribute to biomechanical changes such as increased ankle inversion and lateral deviation of COP during dynamic tasks [9, 10]. In addition, increased navicular drop [11] and posterior deviation of the fibula [12] have been reported as potential risk factors for ankle sprain, although the results have been inconsistent among individuals with CAI [13,14,15,16]. Furthermore, the anterior talofibular ligament injury contributes to changes in cartilage loading in the ankle joint by altering talar alignment [5, 6]. For these various abnormalities of foot and ankle alignment, conservative interventions such as joint mobilization or taping to address ankle realignment improved the ankle dorsiflexion range of motion or dynamic postural stability of individuals with CAI [17, 18]. In addition, the surgical repair or reconstruction of the lateral ankle ligament was performed to prevent future osteoarthritis of the ankle [19]. Furthermore, insoles are used for abnormalities of foot posture such as pes planus or cavus foot deformity [20, 21]. However, no consensus has been reached on the types of abnormality of foot posture and ankle alignment that occur with CAI. Although understanding these abnormalities could contribute to the development of more efficient conservative treatments, and ligament repair or reconstruction for CAI, no systematic reviews have clarified the relationship between abnormalities of foot and ankle alignment and CAI. The objective of this systematic review was to clarify the relevance of abnormalities of foot posture and ankle alignment for CAI.
Methods
Literature search
This study was conducted and reported according to the PRISMA guidelines for reporting systematic reviews and meta-analysis [22]. A computerized literature search of the PubMed, CINAHL, SPORTDiscus, Web of Science, and the Cochrane Register of Clinical Trials databases was performed on December 6, 2019 and repeated June 15, 2021, and included articles published any time up to that date. The search strategies for each database are shown in Additional file 1: Table A.1-A.4. Articles identified from the search were stored and managed using Endnote X9.
Inclusion and exclusion criteria
The inclusion criteria were as follows: eligible articles had to be full-text reports of a randomized control trial, cohort study, cross-sectional study, case–control study, or case series published in a peer-reviewed journal; the study compared a group of human participants with CAI with a control group or compared a healthy leg with the contralateral leg with CAI; foot posture and static alignment of the ankle were included in the outcome; and the article was written in English. Because this study included the search period before the publication of recommended criteria by the International Ankle Consortium [2], we also included studies that defined CAI based on a history of ankle sprain, perceived ankle instability, or imaging findings, as well as articles that did not specify the coper subjects. Articles were excluded if the numbers of participants in the CAI and control groups were not clearly presented or quantitative data were not reported for both groups.
Literature screening
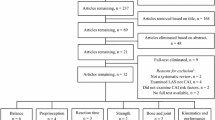
After the initial search, articles duplicated between the databases were removed. The titles and abstracts were assessed for relevance to the aim of the review, and the full-text articles were retrieved for those identified as relevant. These were screened against the inclusion and exclusion criteria, and the reference lists of the articles were cross-checked for additional articles. Two reviewers independently screened all the articles identified in the database search, with any disagreements discussed at a meeting between the two reviewers and resolved by consensus. If no consensus was achieved for a specific item, a third reviewer was involved to achieve a consensus between the two raters (Fig. 1).

PRISMA flow diagram of the study selection process
Data extraction
All alignment outcome measures, measurements of foot posture and static alignment of the ankle were extracted from the included articles by two independent reviewers. Information about participants, study objectives, definitions of CAI, independent and dependent variables, measurement methods, statistical analyses, main findings, and conclusions were also collected.
Quality and certainty assessment
Two independent reviewers assessed the risk of bias, with a third reviewer deciding in cases where consensus was lacking. The included studies were evaluated for quality based on an index (Downs and Blacks criteria checklist) developed for nonrandomized studies [23]. Because the present systematic review did not apply questions relating to methodological design validity associated with an intervention, this study used a 16-question version adapted from the original index by Munn et al. (Additional file 1: Table B.1) [24]. The maximum possible score was 17, and the authors recommended that studies scoring < 60% should be considered of low quality, those scoring 60%—74% of moderate quality, and those scoring > 75% of high quality [24]. The independent critical appraisal and data extraction were completed by two reviewers. Any disagreements were resolved by discussion to reach a consensus. Results of the study bias and quality assessment were considered as a component of the outcome certainty assessment. Two independent reviewers assessed the certainty of evidence as “high”, “moderate”, “low”, or “very low” using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach [25]. As per the GRADE approach, certainty levels for observational studies started at the “low-certainty” evidence classification level and were upgraded or downgraded according to the set criteria.
Results
Study selection and quality
The results of the literature search and review process are presented in Fig. 1. Sixteen papers provided results that were included in the analysis (Table 1) [6, 8, 13,14,15,16, 26,27,28,29,30,31,32,33,34,35]. The methodological quality scores of the included studies ranged from 6 (35.3%) to 13 (76.5%), with a mean score of 9.69 (57.0%) (Table 2). One study was considered to be of high methodological quality, 5 studies were of moderate quality, and 11 studies were of poor quality.
Fibula alignment
Six studies including 239 patients (39.8 patients per study) investigated fibular alignment [13,14,15,16, 28, 35]. Methodological quality was low except for one paper showing moderate quality. Two of these studies recruited patients with CAI who were undergoing lateral ligament reconstruction surgery (only preoperative values were included as results) [13, 16], and the other four studies were based on functional disability, such as recurrent ankle sprains or subjective instability [14, 15, 28, 35]. Two of the papers measured fibular alignment using two-dimensional (2D) analysis in the axial plane based on computed tomography (CT) or magnetic resonance imaging (MRI) images to calculate the axial malleolar index (AMI) [13, 16], three papers used 2D analysis based on sagittal plane radiographs [14, 28, 35], and one study used a three-dimensional (3D) bone model based on CT images [15]. The outcomes measured in these studies were the anterior/posterior and medial/lateral displacement of the fibula.
The two studies involving analysis of the axial plane found the lateral malleolus of the ankle to be significantly posterior in the subjects with CAI [13, 16]. Mean AMI was 11.06–17 degrees in the CAI group and 7.89–9 degrees in the control group [13, 16]. In contrast, of the three analyses using sagittal plane data, one described the lateral malleolus as significantly anterior in the subjects with CAI (mean difference from the control group, 1.8 mm) [14], whereas the others did not detect any significant difference [28, 35]. The 3D analysis did not find a significant difference in anterior/posterior position between the CAI ankles and the contralateral healthy ankles [15]. However, this analysis reported a significant lateral displacement of the fibula (the distal 10 cm of the fibula length) in the CAI ankles compared with the contralateral ankles (Table 1) [15]. The certainty of evidence of fibular anterior/posterior translation could not be determined, because the results were inconsistent. The certainty of evidence for fibular lateral/medial translation was very low (downgraded for bias and imprecision).
Talar positioning
Four studies including 139 patients (34.8 patients per study) investigated alignment of the talus in CAI [6, 16, 32, 34]. The methodological quality of all papers was low. Two studies recruited patients undergoing lateral ligament reconstruction surgery (only preoperative values were included as results) [6, 16], whereas the other two were based on functional disability, such as recurrent ankle sprains or subjective instability [32, 34]. One study measured talus alignment using a 2D analysis in the axial plane based on MRI images [16], two studies used 2D analysis based on sagittal plane radiographs [32, 34], and one study used a 3D-to-2D registration technique [6]. The measured outcomes were anterior/posterior translation and internal/external rotation of the talus.
The four studies reported consistent results. Regardless of the measurement method and whether or not the ankle was weight bearing, the talus of CAI ankles showed significant anterior displacement (0.9–1.0 mm) and internal rotation (3.85–5.7 degrees) compared with healthy ankles (Table 1) [6, 16, 32, 34]. The certainty of evidence of these results was low.
Foot posture
Seven studies including 494 patients (70.6 patients per study) investigated foot posture in CAI [8, 26, 27, 29,30,31, 33]. The methodological quality of one paper was high, with the remaining six showing moderate or low quality. One study recruited patients with CAI who were undergoing lateral ligament reconstruction surgery (only preoperative values were included as results) [31], three of these recruited CAI subjects based on functional disability such as recurrent ankle sprains or subjective instability [8, 30, 33], and the others selected subjects according to scores with the Cumberland Ankle Instability Tool [26, 29] or Identification of Functional Ankle Instability and Foot and Ankle Ability Measure [27]. Two studies measured foot posture using 2D analysis in the frontal/axial plane based on CT images [8, 33], and the other two studies used a 2D analysis of sagittal plane radiographs [30, 31]. In addition, two studies measured from the body surface, applying the Foot Posture Index (FPI-6), [26, 27] and the other two studies calculated arch height index (AHI) or foot mobility magnitude used instrumental measurements (e.g., from a 3D foot scanner) [27, 29]. The measured outcomes were midfoot/rearfoot alignment, including the foot arch height.
The study that used a 2D analysis of sagittal plane radiographs observed mean differences in talocalcaneal, calcaneal, and talometatarsal angles, and tarsal index between the CAI and control groups were 2.0°, 1.5°, 5.4°, and 5.7, respectively [30]. These results suggested a greater frequency of cavus foot deformity in the CAI group than in the control group. In addition, the study using CT images showed mean differences in foot and ankle offset, calcaneal offset, and hindfoot angle between the CAI and control groups of 4.8%, 9.9 mm, and 16.5°, respectively [8]. The authors concluded that hindfoot of CAI ankles was more varus than control ankles. However, the other five studies with image analyses and measurements from the body surface found no significant differences in foot posture between CAI and normal ankles (Table 1) [26, 27, 29, 31, 33]. The certainty of evidence for foot posture could not be determined, because the results were inconsistent.
Discussion
The aim of this systematic review was to clarify the relationships between CAI and abnormalities of foot posture and ankle alignment. The review included 16 studies that examined fibular or talus alignment or foot posture, retrieved through electronic screening. These indicated significant anterior displacement and internal rotation in the talus of CAI ankles compared with healthy ankles. However, there was no consensus regarding fibular alignment and foot posture.
The results for fibular anterior/posterior translation in CAI ankles differed across the six included studies. Differences in the reference bone may have been the main cause of this variation. Some studies referenced to the tibia and others to the talus, making it difficult to compare findings across the studies. The 3D analysis found the fibulas of CAI ankles were in a significantly lateral position compared with those of the contralateral side [15]. The authors' explanation for this was that lateral displacement of the fibula widened the distal tibiofibular joint, affecting the mortise structure and that this was associated with excessive talar rotation [15]. Fibular repositioning tape is used to treat CAI; this has been shown to improve postural stability [36, 37]. The aim of this approach is to correct fibula alignment using a nonrigid and rigid tape applied from the distal aspect of the fibula, wrapped around the posterior aspect of the leg to apply superoposterior mobilization force to the distal fibula, equal to a Grade IV joint mobilization [36, 37]. However, the findings of the present review showed that the fibulas of CAI ankles may not necessarily be displaced anteriorly, so other interventions, including different taping methods, should also be investigated. Meanwhile, the anterior tibiofibular ligament injury may be involved in some patients with lateral ankle sprains, and this ligament dysfunction may contribute to abnormalities of fibular alignment [15]. In addition, the anterior talofibular ligament and the calcaneofibular ligament was connected at the anterior tip of the lateral malleolus, [38, 39] and repair or reconstruction of these ligaments for CAI may contribute to the improvement of fibular alignment. However, the indications for surgery in patients with CAI are determined based on pain and instability, and the degree of fibular deviation to use as a criterion for surgery remains unclear [40]. However, reliable 3D imaging evaluation is important because abnormal alignment is likely to be associated with functional impairment. In addition, we believe that the tibia should be the criterion when evaluating fibular alignment because the results of this review suggest that CAI causes abnormal anterior displacement and internal rotation in the talus.
The studies included in this systematic review consistently showed significant anterior displacement and internal rotation of the talus of CAI ankles. The main cause for this is thought to be damage to a lateral ankle ligament (such as the anterior talofibular ligament) caused by repeated lateral ankle sprains [6]. These abnormalities can cause limited range of motion, pain, and cartilage damage, which may be associated with the development of osteoarthritis in the future [4, 41]. Wainright et al.[19] have reported that surgical repair of the anterior talofibular ligament in CAI decreased anterior translation and internal rotation of the talus, therefore, surgical repair of the lateral ankle ligament appears to be effective in improving talar alignment. In addition, joint mobilization to improve talar posterior gliding is performed as a treatment for CAI, and has been shown to improve the range of ankle dorsiflexion, ankle plantar-flexion angle at initial contact during a single-leg drop landing, and dynamic postural stability as assessed by posteromedial distance in the star excursion balance test [42, 43]. It is thought that increasing talar posterior gliding improves the anterior displacement of the talus in CAI ankles [44]. In contrast, no effective conservative treatment such as taping or semi-rigid brace for increasing internal rotation of the talus has been reported; this needs further study. Furthermore, no conclusions have been reached regarding the most effective technique for improving talar alignment for preventing osteoarthritis [5, 45].
There was no consensus among the seven studies in this review regarding the characteristics of foot posture in individuals with CAI. In the study by Larsen et al. [30], the foot arches of the CAI group were higher than those of the healthy group, and Lintz et al.[8] concluded that CAI ankles was more varus than control ankles. These two studies that used 2D image analysis indicated abnormalities in CAI, but no foot malalignment in CAI was observed in body surface evaluation studies such as AHI, FPI-6, and foot mobility magnitude [26, 27, 29]. This difference may depend on the measurement methods and the criteria of CAI subjects. Although some studies have examined the relationship between foot alignment and ankle sprain, they came to no conclusion [46]. Further studies are needed on the relevance of foot posture abnormalities for CAI using more reliable instrumented measures or 3D image analysis.
In CAI, abnormal alignment of the talus may contribute to abnormal arthrokinematics and cartilage loading pattern of the talocrural joint, so assessment of talar alignment using reliable modality is useful in clinical practice. As no consensus has been reached regarding the abnormalities of fibular alignment in CAI, intervention methods must be considered according to the specific alignment abnormality in each case. The tibia may also represent the optimal reference for reliable assessment of fibular alignment. In addition, no clear relationship was apparent between foot posture and CAI from the findings of this systematic review. However, since abnormalities of foot posture are suspected to be associated with various clinical dysfunctions, accumulation of further results using reliable methods is important.
This systematic review included 16 retrospective cohort, case–control or cross-sectional studies. Although these provided results regarding the relationship between several aspects of foot or ankle alignment and CAI, the quality of almost included studies was not high, so the evidence underpinning the findings of this systematic review is not strong. In addition, differences in CAI selection criteria among the studies may have influenced the results. For example, some studies included patients with mechanical instability of the ankle joint who resisted conservative treatment, while other studies used a history of ankle sprain and perceived instability as inclusion criteria and did not include the presence or absence of mechanical instability. In addition to mechanical impairments (e.g., arthrokinematics restrictions) and perceptual impairments (e.g., perceived instability), neurophysiological problems were also associated with the pathogenesis of CAI [4]. Future studies should therefore refer to the selection criteria of the International Ankle Consortium to consider coper’s subjects as well [2]. Also, because it is likely that ligamentous dysfunction would affect alignment of the foot and ankle, the presence or absence of mechanical instability should be clarified for each subject. Although foot posture is considered to be influenced by biological sex [47], the present study was unable to consider the effects of sex. Finally, the differences in measurement methods among the studies made it difficult to integrate the results through a meta-analysis. The development of a simple, high-precision measurement method for physicians and therapists is needed.
Conclusion
The aim of this systematic review was to clarify the relevance for CAI of foot and ankle alignment. The review identified that there was significant anterior displacement and internal rotation in the talus of CAI ankles compared with healthy ankles, but there was no consensus on the characteristics of fibular and foot alignment. In addition, the quality of the studies that investigated foot and ankle alignment was not high. Future studies are needed to clarify the foot and ankle malalignments characteristic of CAI, as well as related ligament injuries, using unified selection criteria. This should facilitate the development of efficient interventions.
Availability of data and materials
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- CAI:
-
Chronic ankle instability
- 2D:
-
Two-dimensional
- 3D:
-
Three-dimensional
- CT:
-
Computed tomography
- MRI:
-
Magnetic resonance imaging
- FPI:
-
Foot Posture Index
- AHI:
-
Arch height index
- GRADE:
-
Grading of Recommendations Assessment, Development and Evaluation
References
Kobayashi T, Gamada K. Lateral ankle sprain and chronic ankle instability: a critical review. Foot Ankle Spec. 2014;7(4):298–326.
Gribble PA, Delahunt E, Bleakley C, Caulfield B, Docherty C, Fourchet F, Fong DT, Hertel J, Hiller C, Kaminski T, et al. Selection criteria for patients with chronic ankle instability in controlled research: a position statement of the international ankle consortium. Br J Sports Med. 2014;48(13):1014–8.
Houston MN, Hoch JM, Hoch MC. Patient-reported outcome measures in individuals with chronic ankle instability: a systematic review. J Athl Train. 2015;50(10):1019–33.
Hertel J, Corbett RO. An updated model of chronic ankle instability. J Athl Train. 2019;54(6):572–88.
Bischof JE, Spritzer CE, Caputo AM, Easley ME, DeOrio JK, Nunley JA 2nd, DeFrate LE. In vivo cartilage contact strains in patients with lateral ankle instability. J Biomech. 2010;43(13):2561–6.
Caputo AM, Lee JY, Spritzer CE, Easley ME, DeOrio JK, Nunley JA 2nd, DeFrate LE. In vivo kinematics of the tibiotalar joint after lateral ankle instability. Am J Sports Med. 2009;37(11):2241–8.
Hollander K, Zech A, Rahlf AL, Orendurff MS, Stebbins J, Heidt C. The relationship between static and dynamic foot posture and running biomechanics: A systematic review and meta-analysis. Gait Posture. 2019;72:109–22.
Lintz F, Bernasconi A, Baschet L, Fernando C, Mehdi N, Weight Bearing CTISG, de Cesar Netto C. Relationship Between Chronic Lateral Ankle Instability and Hindfoot Varus Using Weight-Bearing Cone Beam Computed Tomography. Foot Ankle Int. 2019;40(10):1175–81.
Delahunt E, Monaghan K, Caulfield B. Changes in lower limb kinematics, kinetics, and muscle activity in subjects with functional instability of the ankle joint during a single leg drop jump. J Orthop Res. 2006;24(10):1991–2000.
Morrison KE, Hudson DJ, Davis IS, Richards JG, Royer TD, Dierks TA, Kaminski TW. Plantar pressure during running in subjects with chronic ankle instability. Foot Ankle Int. 2010;31(11):994–1000.
Saki F, Yalfani A, Fousekis K, Sodejani SH, Ramezani F. Anatomical risk factors of lateral ankle sprain in adolescent athletes: a prospective cohort study. Phys Ther Sport. 2021;48:26–34.
Eren OT, Kucukkaya M, Kabukcuoglu Y, Kuzgun U. The role of a posteriorly positioned fibula in ankle sprain. Am J Sports Med. 2003;31(6):995–8.
Berkowitz MJ, Kim DH. Fibular position in relation to lateral ankle instability. Foot Ankle Int. 2004;25(5):318–21.
Hubbard TJ, Hertel J, Sherbondy P. Fibular position in individuals with self-reported chronic ankle instability. J Orthop Sports Phys Ther. 2006;36(1):3–9.
Kobayashi T, Suzuki E, Yamazaki N, Suzukawa M, Akaike A, Shimizu K, Gamada K. Fibular malalignment in individuals with chronic ankle instability. J Orthop Sports Phys Ther. 2014;44(11):872–8.
Li HY, Zhou RS, Hua YH, Chen SY. MRI identification of the fibular and talus position in patients with mechanical ankle instability. Int J Sports Med. 2017;38(7):546–50.
Jackson BC, Medina RT, Clines SH, Cavallario JM, Hoch MC. The effect of fibular reposition taping on postural control in individuals with chronic ankle instability: a critically appraised topic. J Sport Rehabil. 2019;28(2):205–10.
Terada M, Pietrosimone BG, Gribble PA. Therapeutic interventions for increasing ankle dorsiflexion after ankle sprain: a systematic review. J Athl Train. 2013;48(5):696–709.
Wainright WB, Spritzer CE, Lee JY, Easley ME, DeOrio JK, Nunley JA, DeFrate LE. The effect of modified Brostrom-Gould repair for lateral ankle instability on in vivo tibiotalar kinematics. Am J Sports Med. 2012;40(9):2099–104.
Acak M. The effects of individually designed insoles on pes planus treatment. Sci Rep. 2020;10(1):19715.
Choi JK, Cha EJ, Kim KA, Won Y, Kim JJ. Effects of custom-made insoles on idiopathic pes cavus foot during walking. Biomed Mater Eng. 2015;26(Suppl 1):S705-715.
Page MJ, Moher D, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, Shamseer L, Tetzlaff JM, Akl EA, Brennan SE, et al. PRISMA 2020 explanation and elaboration: updated guidance and exemplars for reporting systematic reviews. BMJ. 2021;372:n160.
Downs SH, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Community Health. 1998;52(6):377–84.
Munn J, Sullivan SJ, Schneiders AG. Evidence of sensorimotor deficits in functional ankle instability: a systematic review with meta-analysis. J Sci Med Sport Sports Med Australia. 2010;13(1):2–12.
Guyatt G, Oxman AD, Sultan S, Brozek J, Glasziou P, Alonso-Coello P, Atkins D, Kunz R, Montori V, Jaeschke R, et al. GRADE guidelines: 11. Making an overall rating of confidence in effect estimates for a single outcome and for all outcomes. J Clin Epidemiol. 2013;66(2):151–7.
Baldwin JN, McKay MJ, Hiller CE, Nightingale EJ, Moloney N, Burns J, Norms Project C. Correlates of perceived ankle instability in healthy individuals aged 8 to 101 years. Arch Phys Med Rehabil. 2017;98(1):72–9.
Fraser JJ, Koldenhoven RM, Jaffri AH, Park JS, Saliba SF, Hart JM, Hertel J. Foot impairments contribute to functional limitation in individuals with ankle sprain and chronic ankle instability. Knee Surg Sports Traumatol Arthrosc. 2020;28(5):1600–10.
Hubbard TJ, Kramer LC, Denegar CR, Hertel J. Contributing factors to chronic ankle instability. Foot Ankle Int. 2007;28(3):343–54.
Kobayashi T, Takabayashi T, Kudo S, Edama M. The prevalence of chronic ankle instability and its relationship to foot arch characteristics in female collegiate athletes. Phys Ther Sport. 2020;46:162–8.
Larsen E, Angermann P. Association of ankle instability and foot deformity. Acta Orthop Scand. 1990;61(2):136–9.
Lee DO, Kim JH, Song SH, Cho HI, Lee J. Is subtle cavus foot a risk factor for chronic ankle instability? Comparison of prevalence of subtle cavus foot between chronic ankle instability and control group on the standing lateral radiograph. Foot Ankle Surg. 2020;26(8):907–10.
Magerkurth O, Frigg A, Hintermann B, Dick W, Valderrabano V. Frontal and lateral characteristics of the osseous configuration in chronic ankle instability. Br J Sports Med. 2010;44(8):568–72.
Van Bergeyk AB, Younger A, Carson B. CT analysis of hindfoot alignment in chronic lateral ankle instability. Foot Ankle Int. 2002;23(1):37–42.
Wikstrom EA, Hubbard TJ. Talar positional fault in persons with chronic ankle instability. Arch Phys Med Rehabil. 2010;91(8):1267–71.
Wikstrom EA, Tillman MD, Chmielewski TL, Cauraugh JH, Naugle KE, Borsa PA. Dynamic postural control but not mechanical stability differs among those with and without chronic ankle instability. Scand J Med Sci Sports. 2010;20(1):e137-144.
Delahunt E, McGrath A, Doran N, Coughlan GF. Effect of taping on actual and perceived dynamic postural stability in persons with chronic ankle instability. Arch Phys Med Rehabil. 2010;91(9):1383–9.
Wheeler TJ, Basnett CR, Hanish MJ, Miriovsky DJ, Danielson EL, Barr JB, Threlkeld AJ, Grindstaff TL. Fibular taping does not influence ankle dorsiflexion range of motion or balance measures in individuals with chronic ankle instability. J Sci Med Sport/Sports Med Australia. 2013;16(6):488–92.
Kobayashi T, Suzuki D, Kondo Y, Tokita R, Katayose M, Matsumura H, Fujimiya M: Morphological characteristics of the lateral ankle ligament complex. Surg Radiol Anat. 2020;42(10):1153–9.
Matsui K, Takao M, Tochigi Y, Ozeki S, Glazebrook M. Anatomy of anterior talofibular ligament and calcaneofibular ligament for minimally invasive surgery: a systematic review. Knee Surg Sports Traumatol Arthrosc. 2017;25(6):1892–902.
Song Y, Li H, Sun C, Zhang J, Gui J, Guo Q, Song W, Duan X, Wang X, Wang X, et al. Clinical guidelines for the surgical management of chronic lateral ankle instability: a consensus reached by systematic review of the available data. Orthop J Sports Med. 2019;7(9):2325967119873852.
Valderrabano V, Hintermann B, Horisberger M, Fung TS. Ligamentous posttraumatic ankle osteoarthritis. Am J Sports Med. 2006;34(4):612–20.
Cruz-Diaz D, Lomas Vega R, Osuna-Perez MC, Hita-Contreras F, Martinez-Amat A. Effects of joint mobilization on chronic ankle instability: a randomized controlled trial. Disabil Rehabil. 2015;37(7):601–10.
Delahunt E, Cusack K, Wilson L, Doherty C. Joint mobilization acutely improves landing kinematics in chronic ankle instability. Med Sci Sports Exerc. 2013;45(3):514–9.
Vicenzino B, Branjerdporn M, Teys P, Jordan K. Initial changes in posterior talar glide and dorsiflexion of the ankle after mobilization with movement in individuals with recurrent ankle sprain. J Orthop Sports Phys Ther. 2006;36(7):464–71.
Michels F, Pereira H, Calder J, Matricali G, Glazebrook M, Guillo S, Karlsson J, Group E-AAI, Acevedo J, Batista J, et al. Searching for consensus in the approach to patients with chronic lateral ankle instability: ask the expert. Knee Surg Sports Traumatol Arthrosc. 2018;26(7):2095–102.
Lopezosa-Reca E, Gijon-Nogueron G, Morales-Asencio JM, Cervera-Marin JA, Luque-Suarez A. Is there any association between foot posture and lower limb-related injuries in professional male basketball players? A cross-sectional study. Clin J Sport Med. 2020;30(1):46–51.
Song J, Choe K, Neary M, Zifchock RA, Cameron KL, Trepa M, Hannan MT, Hillstrom H. Comprehensive biomechanical characterization of feet in USMA cadets: Comparison across race, gender, arch flexibility, and foot types. Gait Posture. 2018;60:175–80.
Acknowledgements
Not applicable.
Funding
This work was supported by the Grants-in-Aid for Scientific Research of Japan Society for the Promotion of Science, Grant Number 19K19916.
Author information
Authors and Affiliations
Contributions
Takumi Kobayashi; design of the work, acquisition, analysis, drafted and revised the work. Yuta Koshino; design of the work, acquisition, analysis, drafted and revised the work. Takahiro Miki; acquisition, analysis.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Kobayashi, T., Koshino, Y. & Miki, T. Abnormalities of foot and ankle alignment in individuals with chronic ankle instability: a systematic review. BMC Musculoskelet Disord 22, 683 (2021). https://doi.org/10.1186/s12891-021-04537-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12891-021-04537-6