
Abstract
Objective
The aim of this study was to explore the associations between different body mass index (BMI) levels and different lung function impairment (LFI) in Chinese people aged over 40 years.
Methods
We used a multi-stage stratified cluster random sampling method to investigate 3000 residents aged over 40 years from 5 areas in Hubei province of China in 2019-20. The data on questionnaire, physical measurements, and spirometry of the participants were collected. The associations of different BMI levels with different LFI were analyzed using multivariate logistic regressions after complex weighting. The spirometry data were analyzed using one-factor analysis of variance (ANOVA), and post-hoc was performed using the least significance difference (LSD)-t test.
Results
A total of 2860 subjects were included. The prevalence (95%CI) of obstructive lung disease (OLD), restrictive lung disease (RLD), mixed lung disease (MLD), chronic obstructive pulmonary disease (COPD), COPD mild, and COPD moderate/severe/very severe were 24.1% (95% CI: 22.2–26.2), 11.6% (95% CI: 10.3–12.9), 4.0% (95% CI: 3.3–4.8), 12.6% (95% CI: 11.0-14.1), 7.2% (95% CI: 6.0-8.4), and 5.3% (95% CI: 4.3–6.4) respectively. After multivariate adjustment, the risk of OLD, COPD, and COPD mild decreased with the increment of BMI levels (both P for trend < 0.05). When compared to the normal weight group, the overweight group and obese group were at lower risk of experiencing OLD than normal group, the ORs were 0.77 (95% CI: 0.59–0.99) and 0.59 (95% CI: 0.40–0.86) respectively. The obese group was at lower risk for people with COPD mild (OR: 0.42, 95%CI: 0.21–0.85). Participants in underweight group were more likely to experience COPD and COPD moderate/severe/very severe, the ORs were 2.82 (95% CI: 1.07–7.39) and 3.89 (95% CI: 1.28–11.87) respectively.
Conclusion
Higher BMI levels were associated with an decreased risk of OLD and COPD. Obesity had a protective effect on lung function in OLD patients and COPD patients. However, there was no significant difference in RLD and MLD prevalence between different BMI groups.
Similar content being viewed by others


Introduction
Lung function is a long-term predictor for overall survival rates and could be used as a tool in individual lung health assessment as well as general health assessment [1,2,3]. Lung function impairment (LFI) is a sign of early respiratory injury and a syndrome of progressive lung function decline. There are several lung diseases accompanied by LFI, such as obstructive lung disease (OLD), restrictive lung disease (RLD), mixed lung disease (MLD), chronic obstructive pulmonary disease (COPD), etc. It has been well documented that impaired lung function is associated with various adverse clinical outcomes such as all-cause mortality, stroke, heart failure, coronary heart disease, and cognitive impairment [1, 4,5,6,7,8,9,10]. The underlying causal mechanisms, such as chronic systemic inflammation, hypoxia, and right ventricular dysfunction have been considered to account for these associations [11,12,13].
Apart from the unremitting health problems for individuals, LFI has also become a major public health threat that deserves more attention. As the main and representative disease of LFI, COPD has caused significant morbidity and mortality with excessive health resource consumption and health expenditures, making it one of the major contributors for the rising burden of un-communicable chronic diseases in China [14, 15]. The prevalence and disease burden of COPD in China have received considerable attention. In a large, nationally representative sample of adults over 40 years, the prevalence of COPD was reported as high as 13.7% [16]. Meanwhile, the COPD prevalence at the provincial level in China have been published elsewhere [17,18,19,20]. However, the population-based studies on the prevalence of other lung diseases such as OLD, RLD, and MLD in China are very limited. Specifically, the studies focusing on the prevalence and spirometry parameters of different lung diseases by different subgroups have been lacking.
Many factors influence the lung function values such as age, sex, height, weight, ethnicity, etc., among which body mass index (BMI) plays an very important role. The relationship of BMI with lung function and COPD has been previously described in many studies, but the results were inconsistent. A number of studies revealed that low BMI and being underweight were linked to a reduced FEV1 and higher risk of COPD than normal body composition [21,22,23]. A positive association between BMI and lung function, measured using forced vital capacity (FVC) and forced expiratory volume in 1s (FEV1), has been demonstrated in a study of 22,743 participants [24]. However, the exact correlation between obesity and COPD remains controversial. There were studies indicating that overweight and obesity were protective factors for COPD [25,26,27], while a large cross-sectional population-based study considered them as risk factors for COPD [28]. Moreover, it has also been reported that there was no statistical significance between overweight or obesity and COPD [29,30,31]. Some findings suggested that poor exercise ability and muscle function in underweight people and oxidative stress as well as inflammation in obese people may be the factors contributing to the pathogenesis of LFI [23, 32, 33].
Despite the increasing number of studies exploring the associations between BMI and COPD, there is a lack of studies on the association between different BMI categories and lung function in patients with different lung diseases. There are also few epidemiological studies on the prevalence of OLD, RLD, MLD in China. In this study, we tried to provide an up-to-date estimate of the prevalence of COPD as well as other lung diseases (OLD, RLD, and MLD) in Hubei province of mid-China using data from a survey done in 2019-20, which was a part of a nationally cross-sectional study following a strict quality assurance and control programme to ensure data validity and reliability. Also, we aimed to examine the associations between different BMI categories and different LFIs as well as the effect of BMI on spirometric parameters.
Methods
Study population and design
This study was a part of nationwide cross-sectional study of China using the integrated national disease surveillance point (DSP) system from the Chinese Center for Disease Control and Prevention [16, 34, 35]. We conducted multi-center surveys using a complex, multistage, and probability sampling strategy from five DSPs in Hubei province of China from December 2019 to December 2020. Hubei province, located in the central part of China and the middle reaches of Yangtze River, has an area of 185,900 square kilometers and a population of nearly 60 million. In the first stage, three sub-districts/townships were randomly chosen in each DSP. Secondly, two neighboring communities/villages were randomly selected within each sub-districts/township. Thirdly, one group of villagers with more than 150 households was randomly chosen within each community/village. Finally, 100 households within each group of villagers were randomly selected. From each household, one family member aged over 40 years old was randomly selected using a Kish grid sampling approach [16]. Residents with cognitive/literal/mental disorders, pregnancy, cancers, or paraplegia were excluded. A representative sample of adults aged 40 years or older in Hubei Province in 2019-20 was enrolled. All participants provided written informed consent. The overall response rate defined according to the American Association for Public Opinion research was 99.8% in this study (Table S1) [36].
Procedures
All participants were invited to an face-to-face interview by trained staff to obtain information on demographic characteristics, medical history, influencing factors of respiratory disease, and respiratory symptoms. Specifically, influencing factors of respiratory disease included smoking status and family history of lung diseases. Physical examination includes measurements of height, weight, waistline, blood pressure, and heart rate. Body weight was measured in light clothing to the nearest 0.1 kg with a calibrated balance beam scale. Height without shoes on was measured to the nearest 0.5 cm using a vertical ruler. Body mass index (BMI) was computed as the ratio of body weight (kg) to height squared (m2). Body weight status was defined as BMI based on World Health Organization guidelines. BMI status was classified as “low (< 18.5 kg/m2 ),” “normal (18.5–23.9 kg/m2),” “overweight (24.0–27.9 kg/m2 )” or “obese (≥ 28.0 kg/m2)” [37].
Spirometry was conducted based on the recommendations by the American Thoracic Society using calibrated spirometers (MasterScreen Pneumo, Jaeger, Germany) [16, 38]. Prebronchodilator and post-bronchodilator (15 min after administration of 400 µg salbutamol) forced expiratory volume in 1s (FEV1), and forced vital capacity (FVC) were measured. The detailed information on these procedures (including definition of other COPD-specific risk factors, full details of the spirometry method used, and a quality grade method for spirometry results) is described in the nationwide prevalence study [16]. Lung function parameters, including the forced vital capacity (FVC), the forced expiratory volume in the first second (FEV1), and the ratio of FEV1/FVC, were collected before and after using bronchodilator. The predicted values of FEV1 for normal lung function and the lower limited normal (LLN) of FEV1 from a nationwide study of reference values for spirometry in the Chinese population aged 4–80 years old [39]. The prediction equations include age, sex, height, and weight. All results were graded as A, B, C, D, and F based on acceptable operation and repeatability of FVC and FEV1. Grades of A, B, and C were regarded as acceptable for analyses. The severity of airflow limitation was measured by the absolute FEV1, the predicted FEV1, and by the ratio of absolute FEV1/the predicted percentage of FEV1 (FEV1%).
Definitions
We defined different lung function impairments based on the collected FEV1 (L), FVC (L), the predicted FEV1 (%), the predicted FVC (%), FEV1/FVC ratio (%), and the predicted FEV1/FVC ratio (%). COPD was defined by a post-bronchodilator FEV1/FVC < 70% as per the recommendation of the 2018 Global Initiative for Chronic Obstructive Lung Disease (GOLD) [40]. The four GOLD severity grades are defned as GOLD stage I(mild, corresponding to FEV1 ≥ 80% predicted), GOLD stage II(moderate, FEV1 ≥ 50% to <80% predicted), GOLD stage III (severe, FEV1 ≥ 30% to <50% predicted), and GOLD stage IV (very severe disease, FEV1 < 30% predicted). For other respiratory impairments. According to the guidelines for pulmonary function tests (PFTs) published by Chinese Thoracic Society [41], obstructive lung disease (OLD), restrictive lung disease (RLD), and mixed lung disease (MLD) were defined. (1) OLD: FEV1/FVC < 92% of predicted value; FEV1 < 80% predicted, and FVC > 80% predicted; meet any one of the above two requirements. (2) RLD: FVC < 80% predicted. (3) MLD: simultaneously meeting the above (1)+(2) criteria.
Statistical analysis
Statistical analyses were performed with SAS version 9.4 software (SAS Institute, Cary, NC). Categorical variables were expressed as number (n) or percentage (%) and continuous variables as mean ± standard deviation (SD). We used Rao-Scott χ2 test for categorical variables for comparison. We calculated p values for trend using Cochran-Armitage trend test for proportions. The association between BMI and different lung function impairments was evaluated using multivariable logistic regression after complex weighting, and odds ratios (ORs) for different lung function impairments were calculated after adjustment for age, residence, gender, education level, occupation, smoking status, family history of lung diseases. All hypothesis testing was judged at the 0.05 significance level (two-sided). The spirometry parameters (means and SD) were analyzed by univariate analysis of variance (ANOVA) using the Proc GLM procedures of SAS, and least-significant-difference (LSD) pairwise comparisons was used to analyze differences in spirometry parameters among different BMI categories.
Results
Characteristics of study subjects
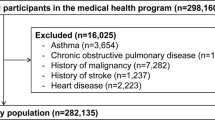
Between December 2019 and December 2020, a total of 3000 subjects were contacted to take part in the survey, of whom 2993 (99.8%) were interviewed. 133 individuals were not eligible for spirometry. 2860 participants completed pre-bronchodilator spirometry examination, among which 2830 participants completed post-bronchodilator examinations. Subjects with unacceptable post-bronchodilator test results were excluded. In total, 2782 participants took part in the interview and had acceptable post-bronchodilator spirometry examinations (Fig. 1). Table 1 presents the demographic characteristics and exposures of 2860 study participants. The proportion of the age group of 50–59 years was the highest (42.8%). Participants from rural areas (68.1%) were more than those from urban areas (31.9%). For exposures of study participants, 1204 (39.9%) participants had smoking status, of whom 940 (30.9%) were current smokers, 264 (8.9%) were former smokers, 593 (22.8%) had family history of lung diseases.

Flowchat on selection of participants in the study
Prevalence of COPD and other lung function impairment
Among 2860 participants who had pre-bronchodilator results, the prevalence of OLD, RLD, and MLD were 24.1% (95% CI: 22.2–26.2), 11.6% (95% CI: 10.3–12.9), and 4.0% (95% CI: 3.3–4.8) respectively. Among 2830 participants who had both pre-bronchodilator and post-bronchodilator results, the prevalence of COPD, COPD mild, and COPD moderate/severe/very severe was 12.6% (95% CI: 11.0-14.1), 7.2% (95% CI: 6.0-8.4), and 5.3% (95% CI: 4.3–6.4) respectively. The age-specific prevalence of OLD, RLD, MLD, COPD, COPD mild, and COPD moderate/severe/very severe rose significantly with increasing age (P < 0.05) and were significantly different between urban and rural residence (P < 0.001). Univariate analysis demonstrated that lower education level (primary school or lower) was correlated significantly with higher COPD and COPD mild prevalence in this population. The prevalence of those above differed significantly between men and women (P < 0.001) except for RLD (P > 0.05). Regarding smoking status, the prevalence of OLD, MLD, COPD, COPD mild, and COPD moderate/severe/very severe were significantly higher in current smokers and former smokers than never smokers, while the prevalence of RLD was not significantly different. Subjects with family history of lung diseases had significantly higher prevalence in OLD and COPD than those without (P < 0.05).
Associations between different BMI and lung function impairment
When BMI was used as a qualitative variable, the trend analysis showed that lower BMI was positively correlated with higher prevalence of OLD, COPD, and COPD mild (P < 0.05). For people diagnosed with COPD moderate/severe/very severe, the prevalence was the highest in underweight group (16.1%) compared to other BMI groups, but the p value for trend was not significant (Table 2). However, there was no significant difference in RLD and MLD prevalence between different BMI groups (P > 0.05). Table 3 displayed associations of different BMI categories with lung function impairment. When the normal weight group was designated as the reference level after using adjusted logistic analysis, the overweight group and obese group were at lower risk of experiencing OLD than normal group, the ORs were 0.77 (95% CI: 0.59–0.99) and 0.59 (95% CI: 0.40–0.86) respectively. However, the overweight group was at higher risk of experiencing RLD (OR: 1.40, 95%CI: 1.04–1.87). Compared to normal group, participants in underweight group were more likely to experience COPD and COPD moderate/severe/very severe, the ORs were 2.82 (95% CI: 1.07–7.39) and 3.89 (95% CI: 1.28–11.87) respectively. The obese group was at lower risk for people with COPD mild (OR: 0.42, 95%CI: 0.21–0.85). The negative dose response relationships between different BMI groups and the risk of OLD, COPD, and COPD mild were statistically significant (P value for trend < 0.05).
The effect of BMI on lung function in lung function impairments
To investigate the effect of BMI on lung function of different lung function impairment categories, we compared the spirometry parameters using ANOVA analysis. As shown in Table 4, there were statistically significant differences of lung function measurements for different BMI categories in people with OLD, COPD, COPD mild, and COPD moderate/severe/very severe. For people with OLD, the mean value of FEV1/FVC ratio and FEV1/FVC%predicted increased significantly from underweight to obese group (P < 0.05). For people with RLD, the mean value of FEV1/FVC ratio and FEV1/FVC%predicted in overweight and obese group were significantly higher when compared to the normal group (P < 0.05). For people with MLD, there was no significant difference in spirometry parameters between different BMI categories (P > 0.05). For people with COPD, significant differences were observed in the mean value of FEV1, FEV1%predicted, FEV1/FVC ratio and FEV1/FVC%predicted between different BMI groups. Specifically, the FEV1 and FEV1%predicted in underweight group were significantly lower than normal group, while the FEV1 in underweight group was also significantly lower than overweight group and obese group (P < 0.05). For people with COPD moderate/severe/very severe, the FEV1/FVC ratio and FEV1/FVC%predicted in overweight group and obese group were significantly higher than those in normal group (P < 0.05).
Discussion
This population-based and spirometry-based study followed a stringent quality-control method which is the first survey of COPD and other lung diseases in Hubei province of mid-China. As a part of the nationwide survey, the study allows us to make a comparison between COPD prevalence at provincial level and national estimation in China. As a province located in the central part of China, the prevalence of COPD of Hubei province (12.6%) in our study was higher than the prevalence of central China (10.2%) reported in the national survey, but was lower than the national prevalence (13.6%) [16]. Compared to other regions of China, the prevalence was lower than Kashi region, northwestern China (17.01%), but was higher than Anhui province (9.8%), Hainan province (5.07%), Jiangsu province (11.8%), and Shenzhen municipality (5.92%) among adults aged over 40 years [17, 19, 20, 42, 43]. A Global Burden of Disease Study of COPD in Hubei province showed that although the mortality of COPD in Hubei has been reduced, the absolute number of COPD cases is increasing [44]. Therefore, sustained attention to COPD control and ongoing surveillance are of great importance. As for other lung diseases, very little is currently known about the prevalence of OLD, RLD, and MLD in China as well as other countries. To the best of our knowledge, this is the first to report the prevalence of OLD (24.1%), RLD (11.6%), and MLD (4.0%) among the sampled people in China. A population-based Korea National Health and Nutrition Examination Survey (KNHANES) reported that the RLD was detected in 11.3% and OLD was detected in 13.2% among 16,151 subjects aged over 40 years [45, 46]. A national spirometric surveillance data in the United States showed that 13.5% of participants had OLD and 6.5% had RLD [47]. Both OLD, RLD, and COPD impose a significant burden on individuals through progressive symptoms, acute pulmonary exacerbations, worsening quality of life, and premature death [48].
The higher smoking exposure in men than women may explain the reason why the prevalence of OLD, MLD, and COPD were significantly higher in men than women [49]. It is well known that smoking habits are important determinants in reduced lung function and developed COPD [50]. The higher prevalence rates of OLD, RLD, MLD, and COPD in rural areas than those in urban areas can also be explained by the fact that cigarette smoking is more prevalent in rural areas [51]. Therefore, smoking may be the primary cause behind the observed disparities between different regions and different gender. Nevertheless, there was no significant disparity in RLD prevalence between male and female as well as with different smoking status. A community-based, cross-sectional study conducted in Taiwan showed that smoking was independently associated with obstructive or mixed types of lung impairment, but not for restrictive type [52]. Another longitudinal study revealed that individuals with the obstructive-only and mixed patterns, but not the restrictive-only pattern, had a significanly higher prevalence of adult smoking compared with the reference pattern. A Italian mulicentric study also proved that smoking was associated with obstructive ventilatory pattern, but not with restrictive ventilatory capacity [53]. It was reported that smoking would harm the airways with less than 2 mm internal diameter, so it results in airway obstruction [54]. The restrictive-only pattern might characterize individuals with poor lung development in childhood, but was found to have true lung restriction by middle age [55].
The effect of body mass index on the lung function have received considerable attention. It is widely demonstrated that being underweight or losing weight increased the risk of COPD exacerbation which leads to reduced lung function and increased risk of mortality [21,22,23,24, 27]. In our study, we found that underweight patients had higher prevalence of OLD and COPD than other BMI groups. Being underweight was shown to be a risk factor for COPD as well as COPD moderate/severe/very severe. This result is consistent with that of a cross-sectional study of 13,023 participants in low- and middle-income countries, which showed that individuals with lower BMI were more likely to have COPD and had lower lung function compared to those in higher BMI [21]. Although the exact cause of unplanned weight loss with a reduced BMI in COPD has not been clearly understood, the underweight patients might have malnutrition, low muscularity and weak resistance against respiratory infection [56]. Also, Rawal and Yadav (2015) concluded that several factors such as a raised resting energy expenditure, inflammation, hypoxia and medication use may contribute to the increasing risk of COPD [57]. On the other hand, the causal relationship between underweight and COPD can also work in the opposite direction. COPD can lead to weight loss and poor nutritional status over a prolonged period of time through appetite loss, diminished general physical activity, a depressive tendency, dyspnea while eating, enhanced energy expenditure due to increased work of breathing, and increased production of inflammatory cytokines [58]. A recent study has estimated that 25–40% of COPD patients are underweight while 35% of patients have severely low fat-free mass index [57]. Therefore, low body weight have been recognized as unfavorable prognostic factors in patients with COPD, especially in those with COPD moderate/severe/very severe level.
Another finding in our study was that the negative dose-response relationship between BMI levels and risk of OLD was significant among participants. Compared to participants with normal BMI, those who were overweight and obese have decreased risk for OLD. Also, participants with obesity had decreased risk for COPD mild. A meta-analysis of thirty articles with 1,578,449 participants concluded that overweight and obesity might reduce the risk of COPD while underweight might increase the risk of COPD [59]. A cross-sectional study of 32,033 subjects also showed that slight obesity was a protective factor for lung function in people at risk of COPD, but being severely obese were associated with reduced lung function [60]. The reduced risk of OLD and COPD in overweight or obese participants might be explained by several mechanisms. Firstly, patients with OLD or COPD need high respiratory muscle mass to deal with increased airway. resistance and airflow obstruction [61]. Secondly, obese COPD patients has the protective effect of higher fat-free mass (FFM), which is a substitute for skeletal muscle mass [62]. Moreover, obese COPD patients have smaller expiratory reserve volume and end-expiratory lung volume [63]. Although being overweight or obesity seemed to have protective effect on the prevalence of OLD and COPD, the mechanisms underlying the “obesity paradox” require further studies and elucidation. On the other hand, being overweight increased the risk of RLD. These findings in our study can be confirmed by a longitudinal study, which showed that adult obesity was significantly more prevalence in individuals with the restrictive-only pattern and less prevalent in the obstructive-only pattern, but was not associated with the mixed pattern [55]. Another longitudinal population-based study from Vienna also revealed that restrictive lung function was strongly modified by high fat mass, central obesity, and adiposity [64]. It has been implied that BMI increase may mostly relate to the development of a restrictive rather than obstructive lung function pattern [65].
We conducted further analysis about spirometry parameters to explore the effect of BMI on lung function for different lung diseases. Spirometry is considered as a tool in various clinical scenarios, including the diagnosis of lung diseases, the monitoring of disease progression, and the assessment of its severity. The data obtained via spirometry can be used in order to detect abnormalities in individuals, among which FVC, FEV1, and the ratio of FEV1 to FVC are commonly used to assess lung functions. In our study, FEV1 and FVC of patients with OLD and COPD from underweight groups were the lowest compared to other BMI groups. The same finding was found in two studies that low BMI was associated with a lower FEV1 and FVC [66, 67]. Our study extended the findings to show that low BMI is associated with decreased lung function represented by parameters such as FEV1, predicted FEV1(%), FVC, and predicted FVC(%) in people with OLD and COPD, but not in people with RLD and MLD. The association between overweight/obesity and spirometry parameters remains controversial. A positive and negative association between overweight/obesity and FEV1/FVC have been both reported before [21, 24, 32, 60, 63]. In our study, significant higher FEV1/FVC was found in overweight/obesity than normal BMI group in people with OLD and COPD moderate/severe/very severe. For people with RLD, the FEV1/FVC and FEV1/FVC%predicted of overweight and obesity group were significantly higher than those of normal BMI group. Study by Jing Zhu also found that increased BMI had a protective effect on lung function in COPD GOLD 3–4 grade, which was consistent with our result [68]. Since nutritional status plays a significant role in the lung function in later stage COPD patients, the prognostic value of BMI was particularly convincing in patients with severe COPD [69].
Our study does have a major strength in our ability to use spirometry measurements for identifying different lung function impairment. Of note, there were some limitations to our study. First, it was a cross-sectional study, so we cannot evaluate any temporal relationships and establish any causality. Second, the different reference equations and diagnostic criteria may lead to overdiagnosis or underdiagnosis of lung function impairment. Third, although the sampled size was not small, the relatively smaller sample size in several subgroups could limit the estimated precision. Moreover, we cannot eliminate the possibility that we misclassified people with different lung diseases.
Conclusion
Our results in this study indicated that lower BMI was positively correlated with higher prevalence of OLD and COPD. Obesity had a protective effect on lung function in OLD patients and COPD patients. However, there was no significant difference in RLD and MLD prevalence between different BMI groups. Future longitudinal studies are needed to clarify the direction of the association between BMI and lung function.
Data availability
The data analyzed in the current study are not publicly available but may be made available from the corresponding authors on reasonable request.
References
Schünemann HJ, Dorn J, Grant BJ, Winkelstein W Jr, Trevisan M. Pulmonary function is a long-term predictor of mortality in the general population: 29-year follow-up of the Buffalo Health Study. Chest. 2000;118(3):656–64. https://doi.org/10.1378/chest.118.3.656.
Shah CH, Reed RM, Liang Y, Zafari Z. Association between lung function and future risks of diabetes, asthma, myocardial infarction, hypertension and all-cause mortality. ERJ Open Res. 2021;7(3):00178–2021. https://doi.org/10.1183/23120541.00178-2021.
Sarycheva T, Capkova N, Pająk A, Malyutina S, Tamosiunas A, Bobák M, Pikhart H. All-cause and cardiovascular mortality in relation to lung function in the full range of distribution across four eastern European cohorts. Sci Rep. 2022;12(1):12959. https://doi.org/10.1038/s41598-022-17261-5.
McAllister DA, Newby DE. Association between impaired lung function and Cardiovascular Disease. Cause, Effect, or force of circumstance? Am J Respir Crit Care Med. 2016;194(1):3–5. https://doi.org/10.1164/rccm.201601-0167ED.
Yang K, Wu Y, Chen D, Liu S, Chen R. The Impact of Lung Function on Extra-Pulmonary Diseases and All-Cause Mortality in US Adult Population with and without COPD. Clin Epidemiol. 2020;12:997–1005. https://doi.org/10.2147/CLEP.S270599.eCollection 2020.
Baughman P, Marott JL, Lange P, Martin CJ, Shankar A, Petsonk EL, Hnizdo E. Combined effect of lung function level and decline increases morbidity and mortality risks. Eur J Epidemiol. 2012;27(12):933–43. https://doi.org/10.1007/s10654-012-9750-2. Epub 2012 Dec 14.
Sin DD, Wu L, Man SF. The relationship between reduced lung function and cardiovascular mortality: a population-based study and a systematic review of the literature. Chest. 2005;127(6):1952–9. https://doi.org/10.1378/chest.127.6.1952.
Agarwal SK, Heiss G, Barr RG, et al. Airflow obstruction, lung function, and risk of incident heart failure: the atherosclerosis risk in communities (ARIC) study. Eur J Heart Fail. 2012;14(4):414–22. https://doi.org/10.1093/eurjhf/hfs016. Epub 2012 Feb 25.
Hozawa A, Billings JL, Shahar E, Ohira T, Rosamond WD, Folsom AR. Lung function and ischemic stroke incidence: the atherosclerosis risk in communities study. Chest. 2006;130(6):1642–9. https://doi.org/10.1378/chest.130.6.1642.
Pathan SS, Gottesman RF, Mosley TH, Knopman DS, Sharrett AR, Alonso A. Association of lung function with cognitive decline and dementia: the atherosclerosis risk in communities (ARIC) Study. Eur J Neurol. 2011;18(6):888–98. https://doi.org/10.1093/aje/kwad140. Epub ahead of print.
Peers C, Dallas ML, Boycott HE, Scragg JL, Pearson HA, Boyle JP. Hypoxia and neurodegeneration. Ann N Y Acad Sci. 2009;1177:169–77. https://doi.org/10.1111/j.1749-6632.2009.05026.x.
Haddad F, Hunt SA, Rosenthal DN, Murphy DJ. Right ventricular function in cardiovascular disease, part I: anatomy, physiology, aging, and functional assessment of the right ventricle. Circulation. 2008;117(11):1436–48. https://doi.org/10.1161/CIRCULATIONAHA.107.653576.
Lu Y, Feng L, Feng L, Nyunt MS, Yap KB, Ng TP. Systemic inflammation, depression and obstructive pulmonary function: a population-based study. Respir Res. 2013;14:53. https://doi.org/10.1186/1465-9921-14-53. PMID: 23676005.
GBD Chronic Respiratory Disease Collaborators. Prevalence and attributable health burden of chronic respiratory diseases, 1990–2017: a systematic analysis for the global burden of Disease Study 2017. Lancet Respir Med. 2020;8(6):585–96. https://doi.org/10.1016/S2213-2600(20)30105-3.
Zhu B, Wang Y, Ming J, Chen W, Zhang L. Disease burden of COPD in China: a systematic review. Int J Chron Obstruct Pulmon Dis. 2018;13:1353–64. https://doi.org/10.2147/COPD.S161555.
Fang L, Gao P, Bao H, Tang X, Wang B, Feng Y, et al. Chronic obstructive pulmonary disease in China: a nationwide prevalence study. Lancet Respir Med. 2018;6:421–30. https://doi.org/10.1016/S2213-2600(18)30103-6.
Li L, Zhong X, Zheng A, JianKun C, Budukadeer AA, Aini P, Tuerxun M, Yasen M, Ma T, Ren J, Semaiti R, Xie C, Li F, Rexiati M, Tang L, Abudurexiti G, Zheng D, Li JQ. Prevalence and risk factors of Chronic Obstructive Pulmonary Disease in Kashi Region, Northwestern China. Int J Chron Obstruct Pulmon Dis. 2021;16:655–63. https://doi.org/10.2147/COPD.S289620.
Wang R, Xu J, Wang Y. A population-based survey of the prevalence and risk factors of chronic obstructive pulmonary disease in Shanxi Province, China. Rev Clin Esp (Barc). 2022;222(4):218–28. https://doi.org/10.1016/j.rceng.2021.04.011.
Zha Z, Leng R, Xu W, Bao H, Chen Y, Fang L, Liu Z, Ye D. Prevalence and risk factors of chronic obstructive pulmonary disease in Anhui Province, China: a population-based survey. BMC Pulm Med. 2019;19(1):102. https://doi.org/10.1186/s12890-019-0864-0.
Zhang DD, Liu JN, Ye Q, Chen Z, Wu L, Peng XQ, Lu G, Zhou JY, Tao R, Ding Z, Xu F, Zhou L. Association between socioeconomic status and chronic obstructive pulmonary disease in Jiangsu Province, China: a population-based study. Chin Med J (Engl). 2021;134(13):1552–60. https://doi.org/10.1097/CM9.0000000000001609.
Grigsby MR, Siddharthan T, Pollard SL, Chowdhury M, Rubinstein A, Miranda JJ, Bernabe-Ortiz A, Alam D, Kirenga B, Jones R, van Gemert F, Checkley W. Low body Mass Index is Associated with higher odds of COPD and lower lung function in low- and Middle-Income Countries. COPD. 2019;16(1):58–65. https://doi.org/10.1080/15412555.2019.1589443.
Keogh E, Mark Williams E. Managing malnutrition in COPD: a review. Respir Med. 2021;176:106248. https://doi.org/10.1016/j.rmed.2020.106248.
Jones RL, Nzekwu M-MU. The effects of body mass index on lung volumes. Chest. 2006;130:827–33.
Svartengren M, Cai GH, Malinovschi A, et al. The impact of body mass index, central obesity and physical activity on lung function: results of the EpiHealth study. ERJ Open Res. 2020;6(4):00214–2020. https://doi.org/10.1183/23120541.00214-2020.
Kanervisto M, Vasankari T, Laitinen T, et al. Low socioeconomic status is associated with chronic obstructive airway diseases. Respir Med. 2011;105(8):1140–6. https://doi.org/10.1016/j.rmed.2011.03.008.
Li H, Xu B, Zheng W. The prevalence of obesity in middle-aged and old men and its relationship with chronic diseases. Chin J Epidemiol. 2010;31(4):370–4.
Fu C, Yang H. Association between appendicular lean mass and chronic obstructive pulmonary disease: epidemiological cross-sectional study and bidirectional mendelian randomization analysis. Front Nutr. 2023;10:1159949. https://doi.org/10.3389/fnut.2023.1159949.
Fuller-Thomson E, Howden KEN, Fuller-Thomson LR, et al. A strong graded relationship between level of obesity and COPD: findings from a national population-based study of lifelong non-smokers. J Obes. 2018;2018:1–9. https://doi.org/10.1155/2018/6149263.
Daldoul H, Denguezli M, Jithoo A, et al. Prevalence of COPD and tobacco smoking in Tunisia–results from the BOLD study. Int J Environ Res Public Health. 2013;10(12):7257–71. https://doi.org/10.3390/ijerph10127257.
Park H, Jung SY, Lee K, et al. Prevalence of chronic obstructive lung disease in Korea using data from the fifth Korea national health and nutrition examination survey. Korean J Fam Med. 2015;36(3):128–34. https://doi.org/10.4082/kjfm.2015.36.3.128.
Zhou Y, Wang C, Yao W, et al. COPD in Chinese nonsmokers. Eur Respir J. 2009;33(3):509–18. https://doi.org/10.1183/09031936.00084408.
Molani Gol R, Rafraf M. Association between abdominal obesity and pulmonary function in apparently healthy adults: a systematic review. Obes Res Clin Pract. 2021;15(5):415–24. https://doi.org/10.1016/j.orcp.2021.06.011.
Vermeeren MA, Creutzberg EC, Schols AM, Postma DS, Pieters WR, Roldaan AC, Wouters EF, COSMIC Study Group. Prevalence of nutritional depletion in a large out-patient population of patients with COPD. Respir Med. 2006;100(8):1349–55. https://doi.org/10.1016/j.rmed.2005.11.023.
Liu S, Wu X, Lopez AD, Wang L, Cai Y, Page A, et al. An integrated national mortality surveillance system for death registration and mortality surveillance, China. Bull World Health Organ. 2016;94:46–57. https://doi.org/10.2471/BLT.15.153148. Epub 2015 Oct 28.
Wang L, Gao P, Zhang M, Huang Z, Zhang D, Deng Q, et al. Prevalence and ethnic pattern of diabetes and prediabetes in China in 2013. JAMA. 2017;317:2515–23. https://doi.org/10.1001/jama.2017.7596.
American Association for Public Opinion Research (AAPOR). Standard definitions: final dispositions of case codes and outcome rates for surveys. https://www.aapor.org/AAPOR_Main/media/publications/Standard-Definitions20169theditionfinal.pdf. Accessed 20 Apr 2023.
World Health Organization. Global database on body Mass Index: BMI classification. Geneva: WHO; 2009.
Graham BL, Steenbruggen I, Miller MR, Barjaktarevic IZ, Cooper BG, Hall GL, Hallstrand TS, Kaminsky DA, McCarthy K, McCormack MC, Oropez CE, Rosenfeld M, Stanojevic S, Swanney MP, Thompson BR. Standardization of Spirometry 2019 Update. An official American Thoracic Society and European Respiratory Society Technical Statement. Am J Respir Crit Care Med. 2019;200(8):e70–e88. https://doi.org/10.1164/rccm.201908-1590ST.
Jian W, Gao Y, Hao C, et al. Reference values for spirometry in Chinese aged 4–80 years. J Thorac Dis. 2017;9:4538–49. https://doi.org/10.21037/jtd.2017.10.110.
Global Initiative for Chronic Obstructive Lung Disease (GOLD). Global Strategy for Prevention, Diagnosis and Management of COPD (2018 Report). (Accessed 20 September 2018). https://goldcopd.org/archived-reports/2018.
Group SPFT. Guidelines for pulmonary function tests. Chin J Tubere Respir Dis. 2014;7487–91. https://doi.org/10.3760/cma.j.issn.1001-0939.2014.07.002).
Ji LC, Yin JF, Lu CR, Guan HY, Tan WG, Wang LW, Jiang Q. Control of chronic obstructive pulmonary disease in urban populations: findings from a cross-sectional prevalence survey in Shenzhen, China. Environ Sci Pollut Res Int. 2022;29(8):11843–53. https://doi.org/10.1007/s11356-021-16553-z.
Ding Y, Yang D, He P, Yao J, Sun P, Li Q, Xie P, Lin D, Sun D, Niu H, Tian Z. Prevalence and risk factors of chronic obstructive pulmonary diseases in a Hlai community in Hainan Island of China. Clin Respir J. 2018;12(1):126–33. https://doi.org/10.1111/crj.12497.
Tang YM, Liu XN, Zhang QJ, Pan JJ, He TJ, Li Q, Yu CH, Zhang L. Chronic obstructive pulmonary disease deaths, disability-adjusted life years, and risk factors in Hubei province of Mid-china, 1990–2015: the global burden of Disease Study 2015. Public Health. 2018;161:12–9. https://doi.org/10.1016/j.puhe.2018.02.016.
Lee JY, Hwang YI, Park YB, Park JY, Kim KU, Oh YM, Yoon HK, Yoon HI, Sheen SS, Lee SY, Lee CH, Lee HB, Lim SC, Jung SS, Oh K, Kim Y, Chun C, Yoo KH. Prevalence of spirometrically-defined restrictive ventilatory defect in Korea: the Fourth-2, 3, and Fifth Korean National Health and Nutrition Examination Survey, 2008–2012. J Korean Med Sci. 2015;30(6):725–32. https://doi.org/10.3346/jkms.2015.30.6.725.
Park HJ, Leem AY, Lee SH, Song JH, Park MS, Kim YS, Kim SK, Chang J, Chung KS. Comorbidities in obstructive lung disease in Korea: data from the fourth and fifth Korean National Health and Nutrition Examination Survey. Int J Chron Obstruct Pulmon Dis. 2015;10:1571–82. https://doi.org/10.2147/COPD.S85767.
Ford ES, Mannino DM, Wheaton AG, Giles WH, Presley-Cantrell L, Croft JB. Trends in the prevalence of obstructive and restrictive lung function among adults in the United States: findings from the National Health and Nutrition Examination surveys from 1988–1994 to 2007–2010. Chest. 2013;143(5):1395–406. https://doi.org/10.1378/chest.12-1135.
Vogelmeier CF, Criner GJ, Martinez FJ, Anzueto A, Barnes PJ, Bourbeau J, et al. Global strategy for the diagnosis, management and prevention of chronic obstructive lung disease 2017 report. Respirology. 2017;22(3):575–601.
Postma DS, Bush A, van den Berge M. Risk factors and early origins of chronic obstructive pulmonary disease. Lancet. 2015;385(9971):899–909.
Anthonisen NR, Connett JE, Murray RP. Smoking and lung function of Lung Health Study participants after 11 years. Am J Respir Crit Care Med. 2002;166:675–9.
Correia M, Magalhães R, Silva MR, Matos I, Silva MC. Stroke types in rural and urban northern Portugal: incidence and 7-year survival in a community-based study. Cerebrovasc Dis Extra. 2013;3(1):137–49. https://doi.org/10.1159/000354851.
Lin YC, Huang TJ, Yeh MH, Lin MS, Chen MY. Lung function impairment and cardiometabolic risks among rural adults: implication for an aging society. BMC Public Health. 2021;21(1):960. https://doi.org/10.1186/s12889-021-10990-8.
Scarlata S, Pedone C, Fimognari FL, Bellia V, Forastiere F, Incalzi RA. Restrictive pulmonary dysfunction at spirometry and mortality in the elderly. Respir Med. 2008;102(9):1349–54. https://doi.org/10.1016/j.rmed.2008.02.021.
McDonough JE, Yuan R, Suzuki M, et al. Small-airway obstruction and emphysema in chronic obstructive pulmonary disease. N Engl J Med. 2011;365:1567–75.
Dharmage SC, Bui DS, Walters EH, Lowe AJ, Thompson B, Bowatte G, Thomas P, Garcia-Aymerich J, Jarvis D, Hamilton GS, Johns DP, Frith P, Senaratna CV, Idrose NS, Wood-Baker RR, Hopper J, Gurrin L, Erbas B, Washko GR, Faner R, Agusti A, Abramson MJ, Lodge CJ, Perret JL. Lifetime spirometry patterns of obstruction and restriction, and their risk factors and outcomes: a prospective cohort study. Lancet Respir Med. 2023;11(3):273–82. https://doi.org/10.1016/S2213-2600(22)00364-2.
Dobner J, Kaser S. Body mass index and the risk of infection - from underweight to obesity. Clin Microbiol Infect. 2018;24(1):24–8. https://doi.org/10.1016/j.cmi.2017.02.013.
Rawal G, Yadav S. Nutrition in chronic obstructive pulmonary disease: a review. J Trans Int Med. 2015;3:151–4.
Itoh M, Tsuji T, Nemoto K, Nakamura H, Aoshiba K. Undernutrition in patients with COPD and its treatment. Nutrients. 2013;5(4):1316–35. https://doi.org/10.3390/nu5041316.
Zhang X, Chen H, Gu K, Chen J, Jiang X. Association of Body Mass Index with Risk of Chronic Obstructive Pulmonary Disease: a systematic review and Meta-analysis. COPD. 2021;18(1):101–13. https://doi.org/10.1080/15412555.2021.1884213.
Tang X, Lei J, Li W, Peng Y, Wang C, Huang K, Yang T. The relationship between BMI and lung function in populations with different characteristics: a cross-sectional study based on the enjoying breathing program in China. Int J Chron Obstruct Pulmon Dis. 2022;17:2677–92. https://doi.org/10.2147/COPD.S378247.
Gea J, Pascual S, Casadevall C, et al. Muscle dysfunction in chronic obstructive pulmonary disease: update on causes and biological findings. J Thorac Dis. 2015;7(10):E418–38. https://doi.org/10.3978/j.issn.2072-1439.2015.08.04.
Park CH, Yi Y, Do JG, et al. Relationship between skeletal muscle mass and lung function in Korean adults without clinically apparent lung disease. Med (Baltim). 2018;97(37):e12281.
Guenette JA, Jensen D, O’donnell DE. Respiratory function and the obesity paradox. Curr Opin Clin Nutr Metab Care. 2010;13(6):618–24. https://doi.org/10.1097/MCO.0b013e32833e3453.
Schiffers C, Ofenheimer A, Breyer MK, Mraz T, Lamprecht B, Burghuber OC, Hartl S, Wouters EFM, Breyer-Kohansal R. Prevalence of restrictive lung function in children and adults in the general population. Respir Med. 2023 Apr-May;210:107156. https://doi.org/10.1016/j.rmed.2023.107156.
Bermúdez Barón N, Kankaanranta H, Hedman L, Andersson M, Stridsman C, Lindberg A, Rönmark E, Backman H. Body mass index increase: a risk factor for forced expiratory volume in 1 s decline for overweight and obese adults with asthma. ERJ Open Res. 2022;8(4):00110–2022. https://doi.org/10.1183/23120541.00110-2022.
Wang S, Sun X, Hsia TC, Lin X, Li M. The effects of body mass index on spirometry tests among adults in Xi’an, China. Medicine. 2017;96(15):e6596. https://doi.org/10.1097/MD.0000000000006596.
Do JG, Park CH, Lee YT, Yoon KJ. Association between underweight and pulmonary function in 282,135 healthy adults: a cross-sectional study in Korean population. Sci Rep. 2019;9(1):14308. https://doi.org/10.1038/s41598-019-50488-3.
Zhu J, Zhao Z, Wu B, Shi Z, Nie Q, Fu Z, Zeng Z, Hu W, Dong M, Xiong M, Hu K. Effect of body Mass Index on lung function in Chinese patients with chronic obstructive Pulmonary Disease: a Multicenter cross-sectional study. Int J Chron Obstruct Pulmon Dis. 2020;15:2477–86. https://doi.org/10.2147/COPD.S265676.
Landbo C, Prescott E, Lange P, Vestbo J, Almdal TP. Prognostic value of nutritional status in chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 1999;160(6):1856–61. https://doi.org/10.1164/ajrccm.160.6.9902115.
Funding
This work was supported by Hubei Provincial Natural Science Foundation of China (grant 2023AFB519) and the Health Commission of Hubei Province Scientific Research Project (Grant no. WJ2019M250).
Author information
Authors and Affiliations
Contributions
YT developed the study concept and design, collected and analyzed the data, interpreted the results and drafted the article. YT, LZ, SZ and MS contributed to data collection. MC and FP provided technical support for this study. SZ and FP take responsibility for the integrity of the data and the accuracy of the data analysis. MS and YT acquired study funding. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
This study was approved by the Ethics Review Committee of the National Center for Chronic and Non-communicable Disease Control and Prevention, Chinese Center for Disease Control and Prevention (No. 201901). Each participant provided the written informed consent before the survey.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Supplementary Material 1:
Table S1. American Association for Public Opinion Research outcome rate calculator (Panel of in-person household surveys)
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Tang, Y., Zhang, L., Zhu, S. et al. Associations between different body mass index and lung function impairment in Chinese people aged over 40 years: a multicenter cross-sectional study. BMC Pulm Med 24, 30 (2024). https://doi.org/10.1186/s12890-024-02844-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12890-024-02844-x