
Abstract
Background
The COVID-19 pandemic has been linked to chronic pulmonary complications all over the world. Respiratory complications such as chronic cough, dyspnea, increased respiratory rate, and oxygen support demand are prevalent in recovered COVID-19 patients. These problems are long-term and have a negative impact on one’s quality of life. Patients must be evaluated for potential complications, and risk factors must be found. Some reports around the world explain the factors that contribute to the development of these complications. However, to the best of our understanding, no reports of post-COVID-19 complications have been reported from Ethiopia.
Methods
Facility based cross-sectional study was done among 405 participants selected by simple random sampling technique. Structured questionnaire which includes participants’ demographic, clinical and 3rd month visit characteristics was collected by Open Data Kit and exported to SPSS version 25.0 for analysis. Percentage with frequency and median with Interquartile range was used in descriptive statistics. The association between variables was analyzed with bivariate and multi variable logistic regression. A statistical significance was declared at p-value < 0.05, with 95% confidence interval.
Results
The median (Interquartile range) age of participants was 57.0 (43.0, 65.0) years, 63.2% were males. The prevalence of post-COVID-19 pulmonary complication in recovered COVID-19 patients was 14.1% (95% CI: 10.8%, 17.8%). After adjusting for possible confounders on multivariate analysis, older age [AOR = 0.227, 95% CI (0.08–0.66)] and consolidation [AOR = 0.497, 95% CI (0.258–0.957)] were shown to have significant association with post COVID-19 pulmonary complications.
Conclusion
The prevalence of post COVID-19 pulmonary complication was observed to be lower than other reports globally. Older age and the presence of consolidation on lung imaging were associated with those complications. Clinicians are recommended to consider assessing the lasting effects of the pandemic, beyond immediate care, and should also investigate the COVID-19 history in patients presenting with respiratory issues.
Similar content being viewed by others


Background
The COVID-19 pandemic is observed to have long-lasting impacts on the respiratory system, which is primarily affected in the acute phase of infection. In recovering patients, it is common to observe a cough, shortness of breath, decreased respiratory functions, a need for oxygen support, and radiologic evidence of chronic lung inflammation [1,2,3,4].
The care and follow-up of infected patients should continue after the acute phase, as an important proportion of patients continue to have persistent symptoms and complications, as can be learned from the previous coronavirus-originating epidemics [5,6,7]. Given that this pandemic impacted a considerably higher number of patients, the post-acute phase of the pandemic presents a significant challenge, as is demonstrated in a number of reports from around the world [8,9,10,11].
Post COVID-19 pulmonary complications have been reported around the globe. Multiple reports from US, Italy and other countries suggest that the prevalence of these symptoms is high, some reporting as high as 87.4% [12,13,14]. Fatigue, shortness of breath, decreased activity and other psychological effects are seen in these patients. Additional diagnosis and even death were reported during follow-ups of recovered patients in some reports, which were attributed to the less anticipated post-acute infection complications of the virus [4, 14]. The Egypt study done on female survivors, with a result of 77.4% prevalence of post-COVID-19 symptoms is the only one from our continent [15]. Female gender, Intensive Care Unit admission, presence of comorbidities and treatments given during the acute phase are some of the factors outlined in the reports [9, 10, 16,17,18]. To the best of our knowledge, there are no reports done in Ethiopia so far.It will be essential to describe the prevalence and factors linked with these complications in order to reduce the morbidity and mortality caused by the post-acute phase of the pandemic. There is a research gap in this topic from low income countries like Ethiopia and this study aims to provide some evidence.
Methods
Study design and setting
Facility based cross sectional study design was conducted to assess the prevalence and associated factors of post COVID-19 pulmonary complications among recovered COVID-19 patients in Eka Kotebe General Hospital, which is the largest treatment centre in the country. The hospital had post-COVID follow up clinic which is run by general practitioners, consultant internists and a pulmonologist. The data was taken from the medical records of patients who, between January 2021 and January 2022, had their third month follow-up appointment after being admitted with confirmed COVID-19 and were discharged as recovered.
Sampling procedure and eligibility criteria
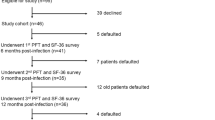
The sample size was calculated by using single population formula with the assumptions of: 95%CI, 5% margin of error, with 40.2% expected proportion [10]. 10% was added accounting for chart loss, which gives a total of 405. All patients whose age was greater than 18 years were included in the study. In the months of January 2021 and January 2022, 1573 people went to the post-COVID-19 Out Patient Department at Eka Kotebe General Hospital. 763 of these individuals underwent visits during the third month of follow-up. Using the Microsoft Excel application, a simple random sampling process was carried out.
Data collection and quality assurance
The data was collected by using pretested structured checklist which is adopted from reviewing different related literatures [10, 14, 17, 19]. The checklist had 4 major sections. These were socio-demographic, acute phase and 3rd month clinical condition with comorbidities, treatment given and imaging & lab profiles. The data included the dates of onset of symptoms, admission status and date of discharge. Patients’ admission clinical status and their 3rd month follow-up data was collected from their chart. Trained general practitioners collected the data by an electronic data collection tool ODK (Kobo tool box). Questionnaires were pre-tested.
Operational definitions
Presence of 2 or more of persistent cough, persistent shortness of breath, increased respiratory rate (> 22 breaths per minute) and requirement of oxygen support (SpO2 < 90% on room air) was used to define post-COVID-19 pulmonary complication during 3rd month visit [8, 13, 19]. The definition and classification of COVID-19 and discharge criteria was primarily based on the national COVID-19 clinical management guideline [20]. Severe COVID-19; defined by any of oxygen saturation < 90%, increased respiratory rate (respiratory rate > 30) and signs of respiratory distress. Critical COVID-19 was defined by the criteria for acute respiratory distress syndrome (ARDS), sepsis, septic shock that will require the provision of life sustaining therapies. Time based recovery: Declaring recovery considering days after the day of lab confirmed diagnosis of COVID-19. Symptom based recovery: Declaring recovery considering days after being asymptomatic (fever and/or cough) in a patient with lab confirmed diagnosis of COVID-19 with moderate, severe or critical illness. If cough is the only symptom judgment should be left for clinician decision. Test based recovery: Declaring recovery considering two negative lab tests done 24 h apart in a patient with lab confirmed diagnosis of COVID-19.
Statistical analysis
Data was collected using ODK software and, transported to and analyzed using SPSS software version 25.0. Categorical variables were presented as frequency and percentages (%), and continuous variables were described using the median and interquartile range, after checking for skewness. The association of independent variables with the outcome variable was investigated using binary logistic regression analysis. The variables that showed an association with the outcome variable at the bi-variable analysis with p value < 0.25 were entered into the final multivariable analysis to control for potential confounders. Adjusted odds ratio (AOR) along with 95% confidence interval was estimated to assess the strength of association and a P value < 0.05 was considered to declare the statistical significance in the multivariable analysis. Assumptions like model fitness was checked to be satisfied using Hosmer and lemeshow p-value (which should not be significant, i.e. p – value > 0.05).
Results
Socio-demographic characteristics of the participants
A total of 405 study participants were involved, 256 (63.2%) were males. The median (IQR) age of the participants was 57.0 (43.0, 65.0) years (Table 1).
Admission status of participants
Majority of the participants were symptomatic during admission. Cough (86.9%), easy fatigability (69.4%), loss of appetite (54.8%), and fever (53.1%) were the most common symptoms presentation at admission. Shortness of breath and headache were also recorded in 46.2% and 34.6% of participants respectively (Table 1).
Comorbidities and imaging findings
56.5% of participants had at least one comorbidity. Diabetes Mellitus and hypertension were the most common comorbid illnesses during the time of admission, being present in 35.3% and 30.4% of participants respectively.
Chest imaging (X-ray or CT- Scan) was done for 322 (79.5%) participants. The most common findings were ground glass opacities (GGO) and consolidation. Consolidation was found in 159 (39.3%) of participants, while GGO was present in 274 (67.7%). Infiltration and effusion were also found in 69 (17.0%) and 7 (1.7%) participants respectively (Table 2).
Laboratory parameters
The median (IQR) hemoglobin level was 14.6 g/dl (13.3, 15.8) and the WBC count was 7530 (5340, 10,840) cells per microliter. More than half (51.4%) of participants had a low lymphocyte count (ALC) of less than 1000 per microliter. The median (IQR) lymphocyte count was 973 (656, 1437) cells per microliter. The median (IQR) creatinine and BUN level were 0.91 (0.74, 1.12) mg/dl and 14.0 (10.0, 21.0) mg/dl respectively (Table 3).
Clinical course of participants during admission
Among the 405 participants, 327 (80.7%) had severe COVID-19 diagnosis during their hospital stay. Twenty eight (6.9%) had critical COVID-19, 29 (7.2%) had moderate COVID-19 and 21 (5.2%) had mild COVID-19. Majority (87.7%) were admitted to the medical ward while 8.9% of participants admitted to ICU/HDU. The remaining 14 (3.5%) participants were admitted to other wards like the labor ward or psychiatry ward.
Participants received different levels of oxygen support during their stay. Forty seven (11.6%) participants were maintaining their oxygen saturation with room air, without any support, 70.4% of them were supported with 1-5 L per minute of oxygen, 47 (11.6%) participants were given 6-15 L per minute while 5.2% (n = 21) were put on non-invasive ventilation (NIV) support. Only 5 (1.2%) of participants were put on a mechanical ventilator (MV). Steroid was given to 92.1% (n = 373) of participants and 86 (21.2%) participants received antiviral treatment for COVID-19.
The median (IQR) length of stay was 11 [8, 15] days, with a range of 45 days (3–48). When discharged, symptom-based discharge criteria was used for 214 (52.8%) participants. 176 (43.5%) and 15 (3.7%) participants were discharged according to time-based and test-based criteria respectively (Table 4).
Prevalence of post-covid-19 pulmonary complication
The median (IQR) number of days elapsed from the date of discharge to the visit day was 88 (78, 93) days. During this visit, 72 (17.8%) participants had respiratory complaints. 57(14.1%) had shortness of breath and 31(7.7%) had a cough. Among these symptomatic patients, 16 (4%) participants complained of both cough and shortness of breath, while 56 (13.8%) of them had only one respiratory complaint.
The respiratory rate of participants during the 3rd month visit ranged from 10 to 38 breaths per minute, with a mean number of 22.29 (SD = 2.87), and participants with a respiratory rate of more than 22 breaths per minute were 42.2% (n = 171) of all participants. Oxygen saturation measured at room air during the visit also ranged from 72 − 99%, with a mean measure of 95.54% (SD = 2.74). 23 (5.7%) participants had an oxygen saturation level of less than 90% (Table 5).
When we take these four pulmonary complications (presence of cough, presence of shortness of breath, increased respiratory rate, and lower oxygen saturation level), 135 (33.3%) of participants had one or more of these complications. Two of the complications were present in 7.7% (n = 31) of participants, while 19 (4.7%) had three complications. 1.7% (n = 7) of participants had all the above four complications. The proportion of participants with 2 or more pulmonary complications which is used to define the prevalence of post COVID-19 pulmonary complications is 14.1% (n = 57) with 95% CI: 10.8%, 17.8%.
3rd month visit status of participants
New onset comorbid illnesses, which were not diagnosed during admission were also reported during this period, the most common being DM and hypertension. They were reported in 11.6% (n = 47) and 9.4% (n = 38) of participants respectively. Cardiac disease was found in 10 (2.5%) and CKD was diagnosed in 8(2.0%). GGO was found in 19 (4.7%) and consolidation was seen in 3(0.7%) of participants (Table 5).
The median (IQR) WBC count during 3rd month visit was 6530 (5010, 8290) cells per microliter. Participants with lymphocyte count less than 1000 cells per microliter were 7.9% (n = 32). The median (IQR) lymphocyte count was 1776 (1294, 2343) cells per microliter (Table 3).
Associated factors of post-COVID-19 pulmonary Complications
In bivariate analysis, p value of < 0.25 was used to determine association between the dependent and independent variables. From demographic characteristics, older age showed significant association with post-COVID-19 pulmonary complications.
From factors in admission status of participants, ALC < 1000 cells per microliter, consolidation, GGO, and infiltration in chest imaging showed significant association with developing pulmonary complications.
When we take variables related with clinical course of participants during admission, COVID severity, admission place, maximum oxygen support level and steroid use were the variables that showed significant association in bivariate analysis.
After adjusting for possible confounders on multivariate analysis, age and consolidation have significant association with the dependent variable at 95% CI (p < 0.05).
Participants whose age is less than 40 years are 77.3% less likely to develop post-COVID-19 pulmonary complications than those aged greater than 60 years [AOR = 0.23, 95% CI (0.08–0.66)]. There is also a 59.9% reduced odds of developing complications in participants aged from 41 to 60 years [AOR = 0.401, 95% CI (0.21–0.79)]. Participants whose chest imaging did not show consolidation were 50.3% less likely to develop pulmonary complications after discharge than their counterparts [AOR = 0.497, 95% CI (0.258–0.957) (Table 6).
Discussion
In this study, the prevalence of post-COVID-19 pulmonary complications was assessed on a median of 88 days after hospital discharge, which is close to the 3 month (90 days) cut point used to define long- COVID-19 in most literatures. These literatures showed a higher prevalence of post COVID-19 complications, up to 39% prevalence report [8, 9, 19, 21]. In our study, cough was present in 7.7% of participants. This was comparable to the Egypt study, which reported 8.7% cough prevalence in recovered patients at 2 month visit post recovery [15]. According to the multicenter study done in Spain, at 11.2 months 2.5% cough prevalence was reported. This low prevalence might be due to the much longer visit day after discharge, compared to this study [18]. A higher prevalence of cough (43%) was also reported in the US study that evaluated patients at 16 days after testing date [22].
Shortness of breath on the day of visit was observed in 14.1% participants, which was close to the Egypt study that reported 17.4% [15]. It is much lower than the study in US, which reported a 29% prevalence, while it is higher than the Spain study that reported a 6.5% prevalence [18, 22].
Compared to majority of reports, this study has a lower prevalence rate of pulmonary complications. A meta-analysis on long COVID by A.V.Raveendran et al. reported around 35% prevalence of residual symptoms at 3 months follow up [8]. A 32% prevalence of 2 complications was also reported in one study [13]. In another study a 40.2% prevalence was reported [10].
New onset comorbidities, which were not recorded during admission, were observed in participants during the visit, DM and hypertension being the commonest ones with 11.6% and 9.4% prevalence. Cardiac illnesses were observed in 2.5% participants. This is comparable to other studies which reported new onset comorbid illnesses after COVID infection. A systematic review and meta-analysis on new onset diabetes reported 19.7% new-onset DM and 25.23% hyperglycemia prevalence [23]. In another Turkey study, 12% new onset hypertension was reported during post-COVID-19 period [24].
Regarding the factors associated with development of pulmonary complications, age greater than 60 years was observed to be at more risk than those lower than that age. There was a 77.3% less chance of pulmonary complications in participants whose age is less than 40 years and 59.8% reduced odd of developing complications in participants aged from 41 to 60 years. This finding was similar to some studies globally, which reported older age as a risk factor for pulmonary complications [9, 10, 22, 25]. In one study with more than 4000 COVID-19 survivors, symptoms lasting more than 28 days were significantly associated with age, rising from 9.9% in the individuals aged 18–49 years to 21.9% in those aged ≥ 70 years [25]. Others also found that, persistent symptoms were common in older age group [9, 10]. In the US study, participants whose age is \(\ge 50\) years were 2.29 times more associated with post COVID-19 symptoms [22]. A cross sectional study in Japan also reported an increased risk of long term COVID-19 complications in older age population [26]. This can be due to decreased pulmonary function associated with age increment.
Among the admission status of participants, presence of consolidation was the one factor that showed significant association with post-COVID-19 pulmonary complication, participants with no consolidation in their chest imaging being protected by 50.3%. Extensive chest imaging finding were observed to be associated with pulmonary complications in other studies too [27]. Patients with finding of consolidation and subsequent effect on the lung parenchyma were associated with lasting effects of COVID-19 in this study. Other factors, like number of symptoms, comorbidities and laboratory parameters didn’t show a significant association in this study.
Conclusion
The prevalence of post-COVID-19 pulmonary complication in recovered COVID-19 individuals is lower than reported elsewhere. Age > 60 years and consolidation in chest imaging have a significant association with pulmonary complications. Clinicians must evaluate the long-term impact of the pandemic, in addition to acute management, and look for a history of COVID-19 infection in patients with pulmonary complaints.
Data Availability
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- ALC:
-
Absolute Lymphocyte Count
- BUN:
-
Blood Urea Nitrogen
- CI:
-
Confidence Interval
- CKD:
-
Chronic Kidney Disease
- COVID-19:
-
Coronavirus Disease 2019
- DM:
-
Diabetes Mellitus
- GGO:
-
Ground Glass Opacities
- HDU:
-
High Dependency Unit
- ICU:
-
Intensive Care Unit
- IRB:
-
Institutional Review Board
- MERS-CoV:
-
Middle East Respiratory Syndrome; Coronavirus
- MV:
-
Mechanical Ventilator
- NIV:
-
Non-Invasive Ventilation
- OR:
-
Odds Ratio
- SARS-CoV:
-
Severe Acute Respiratory Syndrome; Coronavirus
- WBC:
-
White Blood Cell
References
Lutchmansingh DD, Knauert MP, Antin-Ozerkis DE, Chupp G, Cohn L, Dela Cruz CS, et al. A clinic blueprint for Post-coronavirus Disease 2019 RECOVERY: learning from the past, looking to the future. Chest. 2021;159(3):949–58.
Lombardi F, Calabrese A, Iovene B, Pierandrei C, Lerede M, Varone F, et al. Residual respiratory impairment after COVID-19 Pneumonia. BMC Pulm Med. 2021;21(1):241.
Tale S, Ghosh S, Meitei SP, Kolli M, Garbhapu AK, Pudi S. Post-COVID-19 Pneumonia pulmonary fibrosis. QJM: Monthly Journal of the Association of Physicians. 2020;113(11):837–8.
Ahmed OF, Kakamad FH, Hama Amin BJ, Abdullah BA, Hassan MN, Salih RQ et al. Post COVID-19 pulmonary complications; a single center experience. Annals of medicine and surgery (2012). 2021;72:103052.
Lam MH, Wing YK, Yu MW, Leung CM, Ma RC, Kong AP, et al. Mental morbidities and chronic fatigue in severe acute respiratory syndrome survivors: long-term follow-up. Arch Intern Med. 2009;169(22):2142–7.
Ahmed H, Patel K, Greenwood DC, Halpin S, Lewthwaite P, Salawu A, et al. Long-term clinical outcomes in survivors of severe acute respiratory syndrome and Middle East respiratory syndrome coronavirus outbreaks after hospitalisation or ICU admission: a systematic review and meta-analysis. J Rehabil Med. 2020;52(5):jrm00063.
Hui DS, Joynt GM, Wong KT, Gomersall CD, Li TS, Antonio G, et al. Impact of severe acute respiratory syndrome (SARS) on pulmonary function, functional capacity and quality of life in a cohort of survivors. Thorax. 2005;60(5):401–9.
Raveendran AV, Jayadevan R, Sashidharan S, Long COVID. An overview. Diabetes & Metabolic Syndrome. 2021;15(3):869–75.
Yong SJ. Long COVID or post-COVID-19 syndrome: putative pathophysiology, risk factors, and treatments. Infectious Diseases. (London England). 2021;53(10):737–54.
Peghin M, Palese A, Venturini M, De Martino M, Gerussi V, Graziano E, et al. Post-COVID-19 symptoms 6 months after acute Infection among hospitalized and non-hospitalized patients. Clin Microbiol Infection: Official Publication Eur Soc Clin Microbiol Infect Dis. 2021;27(10):1507–13.
Pavli A, Theodoridou M, Maltezou HC, Post -COVID, Syndrome. Incidence, clinical spectrum, and challenges for primary Healthcare professionals. Arch Med Res. 2021;52(6):575–81.
Nalbandian A, Sehgal K, Gupta A, Madhavan MV, McGroder C, Stevens JS, et al. Post-acute COVID-19 syndrome. Nat Med. 2021;27(4):601–15.
Carfì A, Bernabei R, Landi F. Persistent symptoms in patients after Acute COVID-19. JAMA. 2020;324(6):603–5.
Huang C, Huang L, Wang Y, Li X, Ren L, Gu X, et al. 6-month consequences of COVID-19 in patients discharged from hospital: a cohort study. Lancet (London England). 2021;397(10270):220–32.
Aly M, Saber HG. Long COVID and Chronic Fatigue Syndrome: a survey of elderly female survivors in Egypt. Int J Clin Pract. 2021;75(12):e14886.
Sarfraz Z, Sarfraz A, Barrios A, Garimella R, Dominari A, Kc M, et al. Cardio-pulmonary sequelae in recovered COVID-19 patients: considerations for primary care. J Prim care Community Health. 2021;12:21501327211023726.
Kayaaslan B, Eser F, Kalem AK, Kaya G, Kaplan B, Kacar D, et al. Post-COVID syndrome: a single-center questionnaire study on 1007 participants recovered from COVID-19. J Med Virol. 2021;93(12):6566–74.
Fernández-de-Las-Peñas C, Guijarro C, Plaza-Canteli S, Hernández-Barrera V, Torres-Macho J. Prevalence of Post-COVID-19 Cough One Year after SARS-CoV-2 Infection: a Multicenter Study. Lung. 2021;199(3):249–53.
Aiyegbusi OL, Hughes SE, Turner G, Rivera SC, McMullan C, Chandan JS, et al. Symptoms, Complications and management of long COVID: a review. J R Soc Med. 2021;114(9):428–42.
Fmoh E. National Comprehensive Covid19 Management Handbook. 2020.
Tirelli U, Taibi R, Chirumbolo S. Post COVID syndrome: a new challenge for medicine. Eur Rev Med Pharmacol Sci. 2021;25(12):4422–5.
Tenforde MW, Kim SS, Lindsell CJ, Billig Rose E, Shapiro NI, Files DC, et al. Symptom Duration and Risk factors for delayed return to Usual Health among outpatients with COVID-19 in a Multistate Health Care Systems Network - United States, March-June 2020. MMWR Morbidity and Mortality Weekly Report. 2020;69(30):993–8.
Shrestha DB, Budhathoki P, Raut S, Adhikari S, Ghimire P, Thapaliya S, et al. New-onset Diabetes in COVID-19 and clinical outcomes: a systematic review and meta-analysis. World J Virol. 2021;10(5):275–87.
Akpek M, Does. COVID-19 cause. Hypertension? Angiol. 2022;73(7):682–7.
Sudre CH, Murray B, Varsavsky T, Graham MS, Penfold RS, Bowyer RC, et al. Attributes and predictors of long COVID. Nat Med. 2021;27(4):626–31.
Sugiyama A, et al. Long COVID occurrence in COVID-19 survivors. Sci Rep. 2022;12(1):6039.
Alarcón-Rodríguez J, Fernández-Velilla M, Ureña-Vacas A, Martín-Pinacho JJ, Rigual-Bobillo JA, Jaureguízar-Oriol A, et al. Radiological management and follow-up of post-COVID-19 patients. Radiologia. 2021;63(3):258–69.
Acknowledgements
We would like to acknowledge Eka Kotebe General Hospital frontline health care workers who gave their service during this pandemic.
Funding
No funding.
Author information
Authors and Affiliations
Contributions
Conceptualization: ABS, SST; Methodology: ABS, SST, DKH; Investigation: ABS, MMM, TDM, AGD, AGD, AMA; Data curation: ABS, TND, BKG; Formal analysis: ABS, TND, TGH, BKG; Interpretation of data: ABS, TND; Original draft preparation: ABS, DKH; Review and editing: All authors; Supervision: ABS, TGH; Submission: ABS, DKH. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Ethical approval was obtained from Eka Kotebe General Hospital IRB with a reference number EK/SA-326/4/26. The need for informed consent for the use of deidentifed medical records was waived by the Eka Kotebe General Hospital ethics committee. Documentation to support the approval and waiver for informed consent can be provided upon reasonable request. The data used in this study were anonymized before use. The study was conducted in accordance with the Declaration of Helsinki.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Seyoum, A.B., Tegegnework, S.S., Mengistu, M.M. et al. Post-COVID-19 pulmonary complications among recovered COVID-19 patients: a cross-sectional study from Addis Ababa, Ethiopia. BMC Pulm Med 23, 409 (2023). https://doi.org/10.1186/s12890-023-02731-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12890-023-02731-x