
Abstract
Background
The impact of co-infection with other pathogenic microorganisms after initiation of treatment for Mycobacterium avium complex pulmonary disease (MAC-PD) has not been clearly described. This study sought to clarify the clinical outcomes of co-infection with MAC after antimycobacterial therapy for MAC.
Methods
Co-infection status was defined as the detection of pathogenic microorganisms other than MAC in at least two consecutive sputum cultures 6–24 months after initiation of treatment. Chest computed tomography (CT) findings and culture results were compared between co-infection and MAC alone groups.
Results
The co-infection and MAC alone groups comprised 12 and 36 patients, respectively. The proportion of patients with sputum culture positive for MAC after 24 months of therapy did not differ significantly between the two groups [25% (3/12) vs. 16.7% (6/36); p = 0.671]. The proportion of patients with improved chest CT score after 24 months of starting treatment compared to baseline was significantly lower for the co-infection group than for the MAC alone group [16.7% (2/12) vs. 79.4% (27/34); p < 0.001]. In the co-infection group, median CT score values at 12 and 24 months did not differ from baseline. However, the MAC alone group showed significant improvement at 12 and 24 months compared with baseline.
Conclusions
In the patient group with co-infection of other pathogenic microorganisms after treatment initiation for MAC there was no impact on therapeutic efficacy compared to the MAC alone group. However, therapeutic intervention interfered with improvement in chest CT findings such as nodule formation, bronchiectasis, infiltration, and cavitary lesions.
Similar content being viewed by others

Background
Nontuberculous mycobacterial pulmonary disease (NTM-PD) is increasing in incidence worldwide and has become an important concern [1]. Also, the incidence of NTM-PD in Japan is gradually increasing and exceeded the incidence of mycobacterial pulmonary tuberculosis for the first time in 2014 [2]. The type of NTM differs by region. In Japan, Mycobacterium avium complex (MAC) accounts for about 90% of the total [2]. In a previous study we reported that 12.2% of patients with MAC pulmonary disease (MAC-PD) had co-infections with Haemophilus influenzae (H. influenzae) and Pseudomonas aeruginosa (P. aeruginosa) [3]. According to Fujita et al., 45.1% of patients with MAC-PD had chronic co-infection with other pathogenic microorganisms, and chronic P. aeruginosa co-infection increased after the initiation of treatment for MAC-PD [4]. Kamata et al. reported that chronic co-infection with P. aeruginosa was seen in 7.8% of patients with MAC-PD [5]. However, the impact of co-infection with other pathogenic microorganisms in MAC-PD after initiation of treatment on the therapeutic efficacy against MAC is not clear.
Thus, we investigated the impact of co-infection with other pathogenic microorganisms after initiation of treatment for MAC-PD.
Methods
Study design
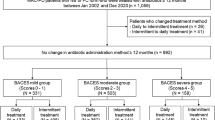
This single-center retrospective cohort study included 48 patients with MAC-PD who had started treatment during the period from November 2014 through February 2019 at Toho University Omori Medical Center. All patients were required to fulfill the American Thoracic Society (ATS) criteria for the diagnosis of NTM [6], and they continued MAC-PD treatment from baseline for at least 12 months (46 patients continued for at least 24 months; 2 patients continued for at least 12 months). Sputum culture for mycobacteria, other bacteria, and fungi was performed at least 3 times during the 6–24 months after treatment initiation for MAC-PD. Patients who had difficulty with sputum collection were excluded.
Definition of co-infection and treatment failure in MAC pulmonary disease
We defined co-infection as the detection of pathogenic microorganisms other than MAC in at least two consecutive sputum cultures 6–24 months after initiation of treatment for MAC-PD. Furthermore, co-infection at baseline was described as ‘base co-infection’. Base co-infection was defined as detection of pathogenic microorganisms other than MAC in at least two separate sputum cultures or at least one bronchoalveolar lavage. The pathogenic microorganisms in ‘co-infection’ are the same pathogens throughout the study, but are different from those in ‘base co-infection’.
Treatment success was defined as sustained negative sputum culture for at least 12 months [7]. Treatment failure was defined as persistent MAC detection in sputum culture after 12 months of treatment.
We compared the clinical characteristics, rate of treatment success, rate of clarithromycin (CAM) resistance, scoring of chest high-resolution CT (HRCT) findings, and subjective symptoms between the co-infection and MAC alone groups. The proportions of patients with improved chest CT and Chronic Obstructive Pulmonary Disease (COPD) assessment testing (CAT) scores at 12 and 24 months after the start of treatment versus baseline were compared between the groups. The CT score and CAT score values at 12 and 24 months were compared with those at baseline for both groups. Univariate and multivariate logistic regression analysis was also performed to identify factors independently associated with co-infection.
Data collection
The following patient data were collected: age, sex, body mass index (BMI), smoking history, serum anti-glycopeptidolipid-core IgA titer, comorbidities, chest and paranasal sinuses CT, and sputum and bronchoscopy culture results. In total, 43 (90%) patients underwent CAT to confirm subjective symptoms at the time of treatment initiation and at 6, 12, 18, and 24 months thereafter [8].
Chest CT score
Chest HRCT score, taken as an index of disease severity, was reviewed as previously described with slight modification as follows [9]. First, on a plain chest radiograph we divided the lungs into 6 zones using 2 horizontal lines at the levels of the carina and inferior pulmonary vein (Fig. 1). These zones are the right and left upper, middle, and lower zones. Next, using HRCT images, we categorized the 4 characteristic lesions in MAC-PD into 4 types namely, cavities, bronchiectasis, nodules (less than 10 mm), and infiltration (an area of opacity greater than 10 mm)]. A score (from 0 to 4) was assigned to each lesion according to the area occupied by the lesion in each zone that is, 0: no area occupied, 1: 1–24% occupied, 2: 25–49% occupied, 3: 50–74% occupied, and 4: 75–100% occupied as shown in Fig. 1. The sum of the scores for each zone comprised the total score. In addition, for the two largest lung cavities overall, changes in cavity wall thickness were reflected by assigning + 2 points for cavity wall thickening by more than 1 mm and — 2 points for thinning (Fig. 2). The thickness of the cavity wall was determined at the thickest segment of the cavity wall with a measuring system using data from Rapideye Core (Canon Inc., Tokyo, Japan) medical imaging information system. This is an integrated healthcare ICT (medical information) and modality (medical equipment) system for electronic medical records. Two respiratory physicians with over 13 years of experience reviewed Chest CT scores independently. Improved Chest CT score was defined as a decrease of even one point.

Scoring for disease severity using characteristic lesions. Representative images showing, A plain chest radiograph showing the lungs divided into six zones at the levels of the carina and inferior pulmonary vein and B the four typical lesions on HRCT described as nodule formation, cavitation, bronchiectasis, and infiltration

Stages of pulmonary lesions in MAC disease by chest CT score. Cavity wall thickness was assigned + 2 points if the thickness increased by more than 1 mm and − 2 points were given for thinning
Statistical analysis
Data are presented as the number of patients and percentages. Age, BMI, chest CT score, and CAT score are expressed as median value (with interquartile range). Associations of categorical and continuous variables between patients in the co-infection and MAC alone groups were tested with the chi-squared or Fisher’s exact test, and the Mann–Whitney U test, respectively. Factors independently associated with co-infection were evaluated with univariate and multivariate logistic regression. Multivariate logistic regression was performed using a stepwise method. A p value of < 0.05 was considered to indicate statistical significance. Statistical analyses were performed with SPSS software version 22 (IBM Corp., Armonk, NY).
Results
Clinical characteristics
In total, 48 patients were included in this study; the co-infection group comprised 12 patients (median age 71.5 years; 2 men, 10 women) and the MAC alone group included 36 patients (median age 71 years; 7 men, 29 women). The characteristics of all 48 patients are shown in Tables 1 and 2. At baseline, there were significant differences between the co-infection and MAC alone groups in scores for chest CT [13 (10.8–14.3) vs. 9 (6.8–11); p = 0.007], bronchiectasis lesions score on chest CT [4 (2.8–5) vs. 2 (1–3.3); p = 0.035], subjective cough symptoms [2 (2–3) vs. 1 (0–2.3); p = 0.015], and sputum [3 (1.5–4) vs. 1 (0–2); p = 0.021]. Both groups showed the same resistance rate to CAM of 8.3% at 24 months after treatment initiation. Overall treatment success rate for MAC was 81.2% (39/48) with no significant differences between the co-infection and MAC alone groups (75% vs. 83.3%; p = 0.671).
Microbiological test results in the co-infection group
Serial changes in microbiological test results in the co-infection group are shown in Table 3. P. aeruginosa was the most common pathogenic microorganism in co-infections after the treatment for MAC and was detected in 7 of 12 (58.3%) patients. Nocardia spp. was detected in 2 of 12 (16.7%) patients, and Methicillin-sensitive Staphylococcus aureus (MSSA), Escherichia coli (E. coli) and Serratia marcescens were detected in 1 (8.3%) patient each. The Geckler classification of sputum examination is shown in Additional file 1: Table S1. The pathogenic microorganism was detected in 10 of the 12 patients in the co-infection group, at least once from examination of high-quality sputum samples (Geckler classification 4 or 5) [10].
Serial changes in Chest CT score
Table 4 shows the clinical course in patients with MAC-PD. The CT score, as a measure of disease severity, was improved in 72.9% and 63% of patients at 12 months and 24 months after treatment initiation. At 24 months after treatment, the proportion of patients with improved chest CT score was significantly lower in the co-infection group than the MAC alone group (16.7% vs. 79.4%; p < 0.001). Figure 3 shows serial changes in chest CT score in the 2 groups. In the co-infection group, mean CT score at 12 and 24 months did not differ compared with the baseline CT score [12(9.3–16.3) and 17(13–21) vs. 13(10.8–14.3); p = 0.757 and p = 0.55]. However, in the MAC alone group, mean CT score at 12 and 24 months was significantly improved compared with the baseline score [5(2–9.3) and 4(2–7.8) vs. 9(6.8–11); p < 0.001 and p < 0.001]. The Chest CT score for all patients is shown in Additional file 2: Table S2.

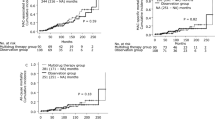
Serial changes in chest CT score. Gray lines indicate change in chest CT score in each patient after initiation of treatment for pulmonary MAC disease. Black lines indicate the median for all patients. A paired t-test was used to compare values at 12 and 24 months with baseline
Serial changes in CAT score
In a comparison of subjective symptoms between the two groups, at 12 and 24 months after initiation of treatment for MAC-PD the proportion of patients with improved CAT scores did not differ significantly between the co-infection and MAC alone groups (70% vs. 54.8% and 40% vs. 48.3%; p = 0.48 and p = 0.726) (Table 4). Figure 4 shows serial changes in CAT score. The co-infection group showed no significant difference in mean CAT score at 12 and 24 months compared with baseline [10.5(3.8–17.5) and 15(3.3–22) vs. 9(6–15); p = 0.576 and p = 0.131]; in the MAC alone group the CAT score at 12 and 24 months did not differ significantly from the baseline score [6(2.5–11) and 5(2–9) vs. 6(4–10.5); p = 0.724 and p = 0.845].

Serial changes in CAT score. Gray lines indicate change in CAT score in each patient after initiation of treatment for MAC pulmonary disease. Black lines indicate the median for all patients. A paired t-test was used to compare values at 12 and 24 months with baseline values
Risk factors for co-infection
Table 5 shows the results of univariate and multivariate logistic regression analysis of independent associations with co-infection. Higher chest CT score (Odds Ratio [OR], 1.27; 95% confidence interval [CI], 1.04–1.55; p = 0.017), higher sputum score (OR, 2.35; 95% CI, 1.28–4.31; p = 0.006), and higher cough score (OR, 2.2; 95% CI, 1.17–4.14; p = 0.014) were independently associated with co-infection in univariate analysis. Higher sputum score (OR, 2.02; 95% CI, 1.08–3.79; p = 0.028) was independently associated with co-infection in multivariate analysis.
Discussion
We demonstrated the impact of co-infection with other pathogenic microorganisms after initiation of treatment for MAC-PD. Although co-infection with other pathogenic microorganisms does not affect therapeutic efficacy against MAC, these organisms may interfere with improvement of chest CT findings. Few studies have investigated the impact of co-infection with other pathogenic microorganisms in MAC-PD [4, 5]. It is important to note that these were cross-sectional studies, and so did not clarify the impact of co-infection on the efficacy of MAC treatment. To our knowledge, this is the first report to investigate the impact of co-infection with other pathogenic microorganisms on clinical course after initiation of treatment for MAC-PD.
This study showed that treatment success rate was 81%, improvement in chest CT score was 63%, and the rate of CAM resistance was 8.3%. These results were consistent with those from previous studies. Earlier reports of macrolide-inclusive daily regimens have shown that the rate of sputum culture conversion was 42–92% [11,12,13,14,15], chest imaging improvement was 68–82% [13, 14], and macrolide resistance was 9–15% [11, 12, 15]. In addition, the rates of MAC culture conversion and CAM resistance did not differ significantly between the co-infection and MAC alone groups. These results suggest that co-infection after the initiation of treatment for MAC-PD did not affect the treatment efficacy.
In the co-infection group, CAM-susceptible bacteria such as MSSA and H. influenzae decreased after MAC treatment while CAM-resistant bacteria such as P. aeruginosa and Nocardia spp. increased after MAC treatment. We speculated that MAC treatment suppressed the proliferation of MAC and other CAM-susceptible bacteria, and this might foster a conversion of the bacteria to CAM-resistant. This result is consistent with previous reports showing that P. aeruginosa was less frequently isolated from positive MAC sputum cultures and more often isolated after MAC sputum conversion [4]. The worse chest CT findings may have been as a result of other pathogenic microorganisms that gained dominance due to weakening of the competing MAC. Also, in the MAC alone group the disappearance of “base co-infection” over time could be because this was contamination. Another possibility is that microorganisms may have been eradicated by treatment with CAM or rifampicin for MAC.
Previous studies showed that NTM-PD including those with cystic fibrosis, had a lower rate of chronic P. aeruginosa infection compared with non-NTM infection [16, 17]. MAC and other pathogenic microorganisms, especially P. aeruginosa, interact with each other and culture results may reflect the dominant pathogenic species at that time. Therefore, we speculate that the negative MAC culture in the co-infection group may not only be due to the effect of MAC treatment but also due to the suppression of MAC culture by other potentially infectious pathogenic microorganisms that became dominant.
In this study, subjective symptoms were more severe in the co-infection group at baseline. Specifically, high sputum score at baseline was an independent risk factor for co-infection. According to Kamata et al., co-infection with P. aeruginosa worsened subjective symptoms in patients with MAC-PD [4]. Previous reports showed that P. aeruginosa colonization was an independent predictor of hospital admission in bronchiectasis [18]. But in our study, the rate of “base co-infection” showed no significant difference between the co-infection and MAC alone groups. We surmised that the presence of trace amounts of other bacteria undetectable by conventional culture in the co-infection group at baseline was the cause of the severe subjective symptoms, and that the bacteria may have become apparently detectable with MAC treatment.
Several risk factors for developing co-infection in patients with MAC-PD have been reported. In the Fujita study, risk factors for co-infection were reported to be COPD and M. intracellulare infection [4]. Their study included 18 of 124 patients who had aspergillus co-infection. In contrast, the Kamata study included 19 patients with P. aeruginosa infection only, and the severity of bronchiectasis, not cavitary lesions, was associated with P. aeruginosa co-infection. The disparity in risk factors for co-infection in these studies may be due to the presence or absence of Aspergillus. Cavitary lesions have been reported to be a risk factor for complications of chronic pulmonary aspergillus infection [19] and M. intracellulare infection was more likely to show fibrocavitary disease than M. avium infection [20]. In addition, the severity of bronchiectasis was significantly associated with the presence of chronic P. aeruginosa infection in patients with non-cystic fibrosis bronchiectasis [21]. In this study, 7 out of 12 patients had P. aeruginosa co-infection and none had Aspergillus co-infection. Also, bronchiectasis score was significantly higher in the co-infection group than the MAC alone group. However, cavitary lesion score and the frequency of concomitant emphysema did not differ between the two groups.
This study revealed considerable discrepancy between radiographic and symptomatic improvement. We considered that CAT score might not reflect the disease status of MAC-PD over time because it does not include other MAC-specific symptoms such as hemoptysis, weight loss, anorexia, and low-grade fever. It is also possible that there was no accurate association due to the small number of cases. Further study is thus needed.
These findings notwithstanding, this study had several limitations that should be mentioned. Firstly, it was a single-center study in a small number of patients. Thus, the findings may not be generalizable to a larger, more diverse population. Secondly, some patients were excluded from this study due to missing sputum examination and chest CT evaluations. These excluded patients might have had infections from a different type of pathogen. Thirdly, the potential presence of indigenous oral bacterial populations cannot be ruled out, and so this may not accurately reflect the status of the lower airway flora because not all patients underwent bronchoscopy. Fourth, since patients were selected based on identified variables (co-infection), there might be some degree of selection bias in the analysis of risk factors for co-infection.
Conclusion
In the patient group with co-infection of other pathogenic microorganisms after treatment initiation for MAC-PD there was no impact on therapeutic efficacy compared to the MAC alone group. However, therapeutic intervention affected improvement in chest CT findings such as nodule formation, bronchiectasis, infiltration, and cavitary lesions.
Availability of data and materials
All data generated or analysed during this study are included in this published article [and its additional files].
Abbreviations
- ATS:
-
American Thoracic Society
- BMI:
-
Body mass index
- COPD:
-
Chronic Obstructive Pulmonary Disease
- CAT:
-
Chronic Obstructive Pulmonary Disease assessment testing
- CAM:
-
Clarithromycin
- CT:
-
Computed tomography
- CI:
-
Confidence interval
- E. coli :
-
Escherichia coli
- H. influenzae :
-
Haemophilus influenzae
- HRCT:
-
High-resolution CT
- MSSA:
-
Methicillin-sensitive Staphylococcus aureus
- MAC:
-
Mycobacterium avium Complex
- MAC-PD:
-
Pulmonary Mycobacterium avium complex disease
- NTM:
-
Nontuberculous mycobacteria
- NTM-PD:
-
Pulmonary nontuberculous mycobacteria disease
- OR:
-
Odds ratio
- P. aeruginosa :
-
Pseudomonas aeruginosa
References
Brode SK, Daley CL, Marras TK. The epidemiologic relationship between tuberculosis and non-tuberculous mycobacterial disease: a systematic review. Int J Tuberc Lung Dis. 2014;18(11):1370–7.
Namkoong H, Kurashima A, Morimoto K, Hoshino Y, Hasegawa N, Ato M, et al. Epidemiology of pulmonary nontuberculous mycobacterial disease. Jpn Emerg Infect Dis. 2016;22(6):1116–7.
Urabe N, Sakamoto S, Sano G, Ito A, Homma S. Characteristics of patients with bronchoscopy-diagnosed pulmonary Mycobacterium avium complex infection. J Infect Chemother. 2018;24(10):822–7.
Fujita K, Ito Y, Hirai T, Kubo T, Togashi K, Ichiyama S, et al. Prevalence and risk factors for chronic co-infection in pulmonary Mycobacterium avium complex disease. BMJ Open Respir Res. 2014;1(1):e000050.
Kamata H, Asakura T, Suzuki S, Namkoong H, Yagi K, Funatsu Y, et al. Impact of chronic Pseudomonas aeruginosa infection on health-related quality of life in Mycobacterium avium complex lung disease. BMC Pulm Med. 2017;17(1):198.
Griffith DE, Aksamit T, Brown-Elliott BA, Catanzaro A, Daley C, Gordin F, et al. An official ATS/IDSA statement: diagnosis, treatment, and prevention of nontuberculous mycobacterial diseases. Am J Respir Crit Care Med. 2007;175(4):367–416.
Van Ingen J, Aksamit T, Andrejak C, Böttger EC, Cambau E, Daley CL, et al. Treatment outcome definitions in nontuberculous mycobacterial pulmonary disease: an NTM-NET consensus statement. Eur Respir J. 2018;51(3):1800170.
Jones PW, Tabberer M, Chen WH. Creating scenarios of the impact of COPD and their relationship to COPD Assessment Test (CAT™) scores. BMC Pulm Med. 2011;11:42.
Morimoto K, Yoshiyama T, Kurashima A, Sasaki Y, Hoshino Y, Yoshimori K, et al. Nutritional indicators are correlated with the radiological severity score in patients with Mycobacterium avium complex pulmonary disease: a cross-sectional study. Intern Med. 2014;53(5):397–401.
Geckler RW, Gremillion DH, McAllister CK, Ellenbogen C. Microscopic and bacteriological comparison of paired sputa and transtracheal aspirates. J Clin Microbiol. 1977;6(4):396–9.
Wallace RJ Jr, Brown BA, Griffith DE, Girard WM, Murphy DT. Clarithromycin regimens for pulmonary Mycobacterium avium complex. The first 50 patients. Am J Respir Crit Care Med. 1996;153(6 Pt 1):1766–72.
Griffith DE, Brown BA, Cegielski P, Murphy DT, Wallace RJ Jr. Early results (at 6 months) with intermittent clarithromycin-including regimens for lung disease due to Mycobacterium avium complex. Clin Infect Dis. 2000;30(2):288–92.
Jeong BH, Jeon K, Park HY, Kim SY, Lee KS, Huh HJ, et al. Intermittent antibiotic therapy for nodular bronchiectatic Mycobacterium avium complex lung disease. Am J Respir Crit Care Med. 2015;191(1):96–103.
Miwa S, Shirai M, Toyoshima M, Shirai T, Yasuda K, Yokomura K, et al. Efficacy of clarithromycin and ethambutol for Mycobacterium avium complex pulmonary disease. A preliminary study. Ann Am Thorac Soc. 2014;11(1):23–9.
Ito Y, Miwa S, Shirai M, Kanai M, Fujita K, Ohba H, et al. Macrolide resistant Mycobacterium avium complex pulmonary disease following clarithromycin and ethambutol combination therapy. Respir Med. 2020;69:106025.
Binder AM, Adjemian J, Olivier KN, Prevots DR. Epidemiology of nontuberculous mycobacterial infections and associated chronic macrolide use among persons with cystic fibrosis. Am J Respir Crit Care Med. 2013;188(7):807–12.
Aksamit TR, O’Donnell AE, Barker A, Olivier KN, Winthrop KL, Daniels MLA, et al. Adult patients with bronchiectasis: a first look at the US bronchiectasis research registry. Chest. 2017;151(5):982–92.
Chalmers JD, Goeminne P, Aliberti S, McDonnell MJ, Lonni S, Davidson J, et al. The bronchiectasis severity index. An international derivation and validation study. Am J Respir Crit Care Med. 2014;189(5):576–85.
Song JW, Koh WJ, Lee KS, Lee JY, Chung MJ, Kim TS, et al. High-resolution CT findings of Mycobacterium avium-intracellulare complex pulmonary disease: correlation with pulmonary function test results. AJR Am J Roentgenol. 2008;191(4):W160.
Koh WJ, Jeong BH, Jeon K, Lee NY, Lee KS, Woo SY, et al. Clinical significance of the differentiation between Mycobacterium avium and Mycobacterium intracellulare in M. avium complex lung disease. Chest. 2012;142(6):1482–8.
Dimakou K, Triantafillidou C, Toumbis M, Tsikritsaki K, Malagari K, Bakakos P. Non CF-bronchiectasis: aetiologic approach, clinical, radiological, microbiological and functional profile in 277 patients. Respir Med. 2016;116:1–7.
Acknowledgements
Not applicable.
Funding
This study received no funding.
Author information
Authors and Affiliations
Contributions
N.U. designed the study, conducted the analysis, and drafted the manuscript; S.S. and K.K. designed the study and participated in editing the manuscript; S.H. confirmed the analyses and revised the article for intellectual content; Y.S. and T.K. conceptualized the study and revised the article for intellectual content; T.M. and N.A. conceptualized the study, and supervised the work; C.K., A.Y., and N.T. participated in editing the manuscript and revised the article for intellectual content. All authors read and critically revised the first as well as the subsequent and final drafts of this manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was conducted in accordance with the amended Declaration of Helsinki and the Ethics Committee of Toho University Omori Medical Center approved the protocol (Approval No. M21218). All methods were carried out in accordance with relevant guidelines and regulations. All patients provided written informed consent to participate in the study.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: Supplementary Table 1.
Detailed sputum culture changes of all patients.
Additional file 2: Supplementary Table 2.
Detailed CT scoring changes of all patients.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visithttp://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Urabe, N., Sakamoto, S., Shimanuki, Y. et al. Impact of chronic co-infection in pulmonary Mycobacterium avium complex disease after treatment initiation. BMC Pulm Med 22, 157 (2022). https://doi.org/10.1186/s12890-022-01947-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12890-022-01947-7