
Abstract
Background
Gender-based violence is a tool that primarily functions to maintain gendered power hierarchies. Manifestations of gender-based violence, sexual assault and street harassment have been shown to have significant effects on mental wellbeing in the global North, however there is little research centering the experiences and consequences of gendered harassment in the Africa region.
Methods
We analyzed a cross-sectional random sample of 372 women attending a major university in Eswatini in 2017 to measure the prevalence of street harassment among female university students and assess the relationship between experiences of sexual assault, sexualized street harassment, and mental health outcomes in this population.
Results
We found that in the previous 12 months, women reported experiencing high levels of sexual assault (20%), street harassment (90%), and depression (38%). Lifetime sexual assault, past 12 months sexual assault, and street harassment were all significantly associated with symptoms of depression. We created a structural model to test hypothesized causal pathways between street harassment, previous experiences of sexual assault, and symptoms of depression, with social support as a potential mediator. We found that a history of sexual violence significantly mediated the association between street harassment and depression, and that social support mediated a large proportion of the association between both forms of gender-based violence and depression.
Conclusion
Sexualized street harassment is associated with increased depressive symptomology for nearly all women, however the effects are especially pronounced for women who have previous experiences of sexual violence. Sexualized street harassment functions as a tool to maintain gendered power hierarchies by reminding women of ongoing threat of sexual violence even in public spaces. Social support and solidarity among women is a potentially important source of resiliency against the physical and mental harms of all forms of gender based violence.
Similar content being viewed by others

Background
Gender-based violence encompasses a spectrum of behaviors which all function to reinforce gendered power hierarchies. Sexual assault, harassment, and street-based verbal harassment all fall within this spectrum [1]. The public nature of street harassment reinforces gendered power structures by providing perpetrators the opportunity to perform sexually aggressive behaviors congruent with toxic hegemonic masculinity while simultaneously reinforcing women’s status as sexual objects who are vulnerable to control by sexual violence and potentially unsafe in public spaces [2, 3]. Experiencing street harassment has been associated with increased depression, anxiety, inability to sleep, disempowerment, humiliation and fear of public spaces [4,5,6,7,8,9].
A growing body of literature is emerging on gender-based violence among university women both on and off campus [10,11,12,13,14]. Social movements such as #MeToo have increased awareness of the prevalence of gender-based violence across many contexts, with women across the globe coming forward to speak openly about their experiences. Likewise, in many high income countries we have seen improved reporting mechanisms become available for students who fall victim to sexual assault or sexual harassment, and university policies that have been reconstructed with a lower tolerance for instances of sexual violence [15] However, much work is still needed to curb the high rates of behaviors across the spectrum of sexual violence for women attending university, particularly in settings such as Southern Africa where rates of sexual violence remain high [16,17,18].
Sexual harassment is both a manifestation of sexual violence and a tacit threat of future sexual assault, and as such, can have serious effects on women’s willingness to participate in public spaces. When this form of gender-based violence manifests in secondary and higher educational settings, the potential for adverse downstream consequences are serious. Sexual harassment in academic settings can negatively affect academic performance, which in turn reduces women’s future workforce participation, compromising future individual earnings as well as social benefits [19, 20]. Women may feel unsafe or unwelcome as they travel to school [21], engage in coursework [22], or pursue mentorship or higher level training [19, 20, 23].
Previous studies have established that a history of sexual assault corresponds with higher risk of depression, anxiety and post-traumatic stress disorder [24,25,26]. As with sexual harassment, a history of sexual assault can also compromise academic attendance and performance, as well as subsequent relationships [27]. Sexual assault before the age of 18 years has been linked to increased levels of heavy alcohol use, suicide ideation and suicide attempts [28, 29].
Efforts to operationalize and measure the prevalence of street harassment are relatively new, however existing reports suggest that street harassment is extremely prevalent [9, 30, 31]. Data on street harassment from low and middle income countries (LMICs) are less robust: a 2021 systematic review and meta-analysis of sexual harassment in LMICs found that sexual harassment was both extremely common and associated with higher rates of anxiety and depression [9]. Relatively few of these studies focused on harassment in public, however. We know of no studies assessing the prevalence and statistical associations between poor mental health and street harassment in southern Africa.
While each woman’s experience of sexual violence and its aftermath is unique, the relationships between gender based violence (including harassment) and poor mental health outcomes are influenced by factors at individual, relational, and structural levels [32, 33]. A robust body of evidence demonstrates that social support plays a particularly important role in mediating the association between sexual violence and adverse mental health outcomes [34], although there is less research exploring how social support might potentially influence the link between sexual or street harassment and mental health.
The goal of the present study was to assess the effects of sexual assault and street harassment on mental health among female university students in Eswatini. We further hypothesized that a woman’s perceived access to social support would significantly mediate the relationship between threatened or actual sexual assault. In other words, we hypothesized that [1] knowing (or believing) that one’s friends would provide support in the event of sexual violence would likely buffer the association between threatened violence and negative mental health outcomes, and [2] perceived likelihood of social support would similarly mediate the association between actual sexual violence and negative mental health outcomes.
Methods
Study setting, sample and design
Eswatini is a small Kingdom in Southern Africa with a population close to 1.1 million [35]. In Eswatini, one third of girls have experienced sexual abuse by the age of 18 years and close to half of women experience gender-based violence in their lifetime [36]. The current study is part of a larger project to measure the prevalence and correlates of campus sexual assault at the University of Eswatini (UNESWA) [37]. UNESWA enrolls approximately 7,500 students, most of whom are undergraduates. The main campus, Kwaluseni, enrolls approximately 4500 students, 30% of whom live on campus with the remainder in peri-urban areas nearby. Women make up 58% of the total student population but are 15% more likely to drop out before their 4th year than men. The majority of students are Swazi citizens. However, the university enrolls students from throughout the region including South Africa, Botswana, and Zimbabwe, and the language of instruction is English. Women were eligible to participate if they spoke English, were enrolled full time, and were at least 18 years old. Selected participants were contacted via email, text, and phone calls inviting them to visit the on-campus student health clinic to complete the consent process. Participants were randomly selected from the University Register’s list of all full-time female students enrolled at the primary UNESWA campus. After indicating that they understood the risks and benefits of the study by providing written informed consent, participants were asked to complete a behavioral survey using a tablet with computer-assisted self-interview (CASI) software. Participants completed the survey in a private office, with a trained research assistant nearby to provide assistance and answer questions. Data collection occurred from February – November 2018.
Ethics
The study was reviewed and approved by UNESWA Research Ethics Board and the University of California, San Diego Institutional Review Board (IRB). Data collection procedures followed the World Health Organization’s Recommendations for Intervention Research on Violence Against Women. All participants were offered a 25 Emalangeni (approximately $2 USD) honorarium to thank them for their time and expertise. A research assistant who was trained in trauma informed counselling was always available while participants completed the survey, and all participants were given a card with a phone number for free-of-charge tele-counselling services when they left the study site. The study team made pro-active efforts to reduce vicarious trauma in frontline staff, including engaging in regular debriefing sessions and ensuring that a local, no-cost third party counselor was available to all staff members.
Measures
Our primary outcome was depressive symptomology, assessed using the 10-item Center for Epidemiological Studies Depression Scale (CES-D-10). The CES-D-10 asks participants to report on their experiences and symptoms in the previous seven days and has been validated in the southern African context [38]. The scale ranges from possible scores of 0–30, and previous validation work in the region suggests that participants are likely experiencing depression if they score 12 or above [38].
Our primary predictors of interest were women’s self-reported experiences of [1] sexual assault and [2] street harassment. We measured sexual assault using the sexual experiences survey short form (SES-SF) [39], a behavioral scale that asks participants to report on their experiences of completed and attempted sexual assault in their lifetime and past 12-months. Women were categorized as having experienced sexual assault if they reported non-consensual penetration by means of threats, coercion, physical violence, or being incapacitated. Concrete behavioral scales such as the SES-SF are the best practice for sexual violence research because criminal justice definitions widely vary across jurisdictions and subjective labels of an experience have been shown to significantly lower reported prevalence [39]. Street harassment was measured by asking women “how often do you experience unwanted comments from men in public” with the options of “never”, “less than once a month”, “once a month”, a few times a week”, and “every day”.
Social support was assessed using three survey items, each with a 4-point Likert response: “If I were sexually assaulted by a [stranger / acquaintance / boyfriend or person I have spent time alone with] I have friends who would support me.” Women could respond “definitely yes,” “probably yes,” “probably no,” and “definitely no.”
Analyses
We conducted univariate descriptive analyses for our primary outcome (CES-D-10 scale) and hypothesized predictors (lifetime penetrative sexual assault, street harassment, perceived social support), followed by bivariate analysis of variance (ANOVA) tests to assess the difference in mean CES-D-10 scores across predictors.
We then used STATA 16.0 software [40] to build two confirmatory factor analysis (CFA) measurement models assessing [1] the validity of the CES-D-10 as a latent construct in the population of interest, and [2] the three social support items as a coherent construct of perceived social support following a sexual assault. Indicators that loaded with a value below 0.50 in these CFA models were removed, and measurement error covariances were added based on theoretical considerations and after considering modification indices suggested by the estat mindices command. Estat mindices uses Lagrange multiplier tests to suggest additional covariances or path coefficeints that would significantly improve model fit [41]. With each modification to the CFA measurement model, we used chi-square tests to assess whether the nested model had a statistically significant improved fit to the data compared to the previous iteration at p < 0.05 [42]. After finalizing the measurement models we constructed a full structural equation model to test the hypotheses that previous experiences of sexual assault and perceived social support significantly mediated the association between experiences of sexualized street harassment and depression.
We used a full-information maximum likelihood (FIML) estimation strategy (mlmv estimation command) for both the measurement and full structural equation models to account for the presence of ordinal indicators in the depression and social support latent variables. Overall model goodness of fit for measurement and the full structural model was assessed across multiple fit indices, per Kline’s recommendation: Model chi-square, RMSEA and RMSEA 90% confidence interval, and the Bentler Comparative Fit Index (CFI) [42]. Direct, indirect, and total effects were examined using Stata’s teffects command.
Results
Three-hundred and seventy-two women participated in the survey (response rate of 49.5%). Mean participant age was 23.3. years, (range 18–45, standard deviation: 3.7). Three hundred and eighteen participants completed all 10 CES-D-10 items, with a median score of 9.5 (range: 0–30, SD: 5.6). The CES-D 10-item scale had reasonable internal consistency, with a Chronbach alpha of 0.81. There were no significant differences in outcomes of interest between participants who did (n = 318) and did not (n = 54) complete all CES-D-10 items (analyses not shown). 31% of participants (n = 97) who completed all CESD-10 items reported experiencing penetrative sexual assault in their lifetime and the vast majority (90%) reported experiencing unwanted sexual comments from men in public in the previous year. The majority of study participants felt that they had a friend who would ‘definitely’ support them if they were assaulted by a stranger (62%), acquaintance (60%), or boyfriend (54%).
There were statistically significant associations between all hypothesized predictors and reported depressive symptomology. The median CES-D score for women who reported ever experiencing penetrative sexual assault was 12.0 compared to 9.5 for women who never experienced penetrative assault (p < 0.01). There was also a significant dose response relationship between the frequency of unwanted sexual comments from men in public and CES-D scores, ranging from a median CES-D score of 8.1 for women who reported ‘never’ receiving comments, to 14.0 for women who reported receiving comments ‘every day’ (p < 0.001). There were similar linear associations between depressive symptoms and perceived social support in the instance of assault from a stranger, acquaintance, and boyfriend or boy with whom the respondent had spent time alone (all p < 0.001) (Table 1).
While the overall CES-D scale had reasonable internal consistency, item-score analyses suggested that two items (“everything I did was an effort” and “I felt hopeful about the future”) had item-rest correlations at or below the threshold of reliability (0.29 and 0.35, respectively) [43]. To address this, we constructed measurement models assessing how well all 10 CES-D items fit our data as a single latent construct. Two of the ten indicators (“everything I did was an effort” and “I felt hopeful about the future.”) had a factor loading below 0.50. After removing these two indicators, the more parsimonious model fit the data approximately as well as the 10-item model (chi-square = 40.0, df = 20 vs. chi-square = 103.6, df = 35), and so we chose to measure the latent depression construct using the more parsimonious 8 item model. We further modified the model to correlate error measurements between “I was bothered by things that don’t usually bother me” and “I had trouble keeping my mind on things I was doing,” as well as “I felt depressed” and “I had trouble sleeping” and then “I felt lonely” and “I could not get going.” (Fig. 1a). The final CFA measurement model fit the data well, with all factor coefficients greater than 0.50 (p < 0.05), chi-square = 18.6 (df = 17, p = 0.60) RMSEA = 0.02, and CFI = 0.998. The social support measurement model was just-identified, with 0 degrees of freedom. All 3 social support indicators loaded at 0.80 or above, with p < 0.001 (Fig. 1b).

a Measurement model of depression as a latent construct. b Measurement model for social support as a latent construct
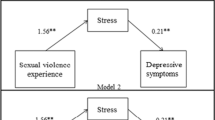
The fully specified structural model fit the data well, with chi-square = 74.4, (df = 58, p = 0.07), RMSEA = 0.03 (90% CI: 0.00–0.05), and CFI = 0.99 (Fig. 2). Confidence that a friend would support her in the case of sexual assault had the largest direct effect on the probability of experiencing depression. For each standard deviation increase in perceived social support, CES-D score decreased by 0.27 standard deviations (standardized b = -0.27, 95% CI: -0.37 -- -0.17). Experience of lifetime penetrative sexual assault was associated with a 0.11 standard deviation increase in CES-D score (standardized b = 0.11, 95% CI: 0.01–0.22) and one standard deviation increase in the reported frequency of sexualized street harassment was associated with a 0.19 standard deviation increase in the probability of depression, (standardized b = 0.19, 95% CI: 0.09–0.30). Women who reported experiencing street harassment were significantly more likely to also report a lifetime experience of penetrative sexual assault (standardized b = 0.13, 95% CI: 0.03–0.23), and were less certain that a friend would support them after an experience of assault (standardized b = 0.28, 95% CI: 0.18–0.38) (Table 2).

Structural equation model with standardized path coefficients
Decomposed direct and indirect standardized effects of each covariate are shown in Table 3. When we examined indirect effects, we found that the perceived social environment played a significant mediating role in the association between sexual assault and CES-D score. 39% of the association between lifetime experience of sexual assault and CES-D score in the previous two weeks was mediated by perceived social support, while 22% of the association between experiencing sexualized street harassment and CES-D score was mediated by having a lifetime experience of sexual assault.
Discussion
Depression, sexual assault, and frequent sexual harassment were pervasive in this sample of Swazi female undergraduates. Using a cut-point score of 12 on the CES-D scale, Over 38% of study participants reported symptoms consistent with depression in the previous week, with the prevalence significantly higher amongst those who had experienced sexual assault in their lifetime, and amongst those who reported higher rates of street-based sexual harassment. Close to 90% of women reported experiencing unwanted sexual comments in public, with nearly 30% experiencing this harassment on a weekly basis. This prevalence is comparable with data reported from the United States which used a similar measure of street harassment [44]. Our findings suggest that the social environment in which women live, work, and attain their education can have a significant effect on the mental health impact of sexual assault. A primary function of sexualized street harassment is to reinforce patriarchal dominance via an ever-present threat of sexualized male violence and humiliation [3, 4, 8, 32, 34, 45, 46]. This experience of harassment is likely to be especially salient for women who have previous experiences of sexual assault. In contrast, a supportive social environment may serve as a key aspect of resilience, significantly mediating the pathway between sexual violence and depressive symptoms.
Social support has been shown to mitigate the adverse mental health consequences of sexual harassment and assault in other settings [47, 48], underscoring its potential as a strategy for collective resistance against sexual violence as a tool of gendered power and control [49]. Notably, while approximately 90% of women reported that they had friends who would ‘definitely’ or ‘probably’ support them if they disclosed assault by stranger or an acquaintance, the number was slightly lower in the case of assault by a boyfriend (85%). While this difference was not statistically significant, marital rape was only outlawed in the Kingdom of Eswatini in 2019, and university women have previously reported the difficulty associated with disclosing assaults committed by an intimate partner [50]. This is consistent with the ways in which Connell has articulated cathexis, or the role of emotional and affective relationships in maintain gendered power structures (46). While a pre-existing romantic, sexual, or otherwise social relationship obviously does not negate the possibility of sexual assault (and is indeed the most common setting for sexual violence), it may dampen women’s access to social support and willingness to disclose an event.
Women who were more certain that their friends would support them in the event of a sexual assault reported lower levels depressive symptoms in the previous two weeks. It is important to note that this association is a correlation within a cross-sectional study and cannot be interpreted as causal. Low levels of social support have been found to be predictive of repeat sexual assault in some university populations [51], suggesting that women with lower levels of social support may be more vulnerable to additional experiences of gender-based violence. Moreover, the association between sexual violence and perceived sexual support may be a result of lived experience – it is possible that women who have not been sexually assaulted may be more optimistic about the likelihood that their friends will support them, while women who have been assaulted may be more likely to report that they did not, in fact, receive social support when it was needed, or may fear friends’ reaction if they do disclose.
The findings of this study should be interpreted within the study’s limitations. Our response rate, at 49.5%, was low for a demographic survey, although it is quite high for a campus sexual assault survey [52]. Survey data are self-reported, and therefore vulnerable to both recall and social desirability bias. However, both of these biases were mitigated to the extent possible by asking about current or past year experiences, and by using self-administered surveys in a private office [53]. Moreover, because this was a secondary analysis of data collected for a separate primary outcome, social support was measured according to women’s perceptions of what might happen, rather than whether they had actually received support from friends and family. Our model tested the hypothesized role of social support as a buffer for the mental health impacts of gendered violence. This hypothesis is consistent with the literature; however it is important to acknowledge that social support, violence, and mental health are complex phenomena that do not exist outside of other social determinants such as food security, adverse childhood experiences, and other social-structural determinants [54,55,56,57]. It is our hope that this study can act as the beginning of a conversation rather than the final word.
To our knowledge, this is the first documentation of the association between verbal sexual street harassment and adverse mental health amongst young women in the southern African context and is in line with findings elsewhere as well as social movements such as #MeToo [4, 5, 44, 45, 58,59,60,61]. The ubiquity of street harassment faced by women is a reminder that women often lack the autonomy and normative right to safely occupy public spaces. Research on male perpetrators of street harassment indicates that they harass in order to control women, and that they are more likely to harass when they feel they have less power than women [3]. Our data lends additional credence to the notion that sexualized street harassment exists as part of a spectrum of sexual violence, the function of which is primarily to reinforce gendered social control. Bystander interventions could play an important role in addressing the social norms surrounding street harassment. Unfortunately, to date very few (if any) interventions exist which specifically aim to prevent perpetrators from engaging in street harassment, or to support women and/or gender non-conforming individuals to engage in resistance strategies when they experience harassment [1]. More focused intervention and support strategies have the potential to meaningfully improve women’s safety, bodily integrity, and mental health.
Data availability
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
References
Fileborn B, O’Neill T. From Ghettoization to a Field of Its Own: A Comprehensive Review of Street Harassment Research. Trauma, Violence, & Abuse.0(0):15248380211021608.
Wamoyi J, Ranganathan M, Mugunga S, Stockl H. It gives you a feeling of pride when you touch her: the role of masculinity in sexual harassment of adolescent schoolgirls in Tanzania. Journal of Interpersonal Violence.
DelGreco M, Ebesu Hubbard AS, Denes A. Communicating by catcalling: power dynamics and communicative motivations in street harassment. Violence against Women. 2021;27(9):1402–26.
DelGreco M, Christensen J. Effects of street harassment on anxiety, depression, and sleep quality of college women. Sex Roles. 2020;82(7):473–81.
Davidson MM, Butchko MS, Robbins K, Sherd LW, Gervais SJ. The mediating role of perceived safety on street harassment and anxiety. Psychol Violence. 2016;6(4):553.
Rosenbaum MS, Edwards KL, Malla B, Adhikary JR, Ramírez GC. Street harassment is marketplace discrimination: the impact of street harassment on young female consumers’ marketplace experiences. J Retailing Consumer Serv. 2020;57:102220.
Bharucha J, Khatri R. The sexual street harassment battle: perceptions of women in urban India. J Adult Prot. 2018.
Ahmad NM, Ahmad MM, Masood R. Socio-psychological implications of public harassment for women in the capital city of Islamabad. Indian J Gend Stud. 2020;27(1):77–100.
Ranganathan M, Wamoyi J, Pearson I, Stöckl H. Measurement and prevalence of sexual harassment in low- and middle-income countries: a systematic review and meta-analysis. BMJ Open. 2021;11(6):e047473–e.
Mamaru A, Getachew K, Mohammed Y. Prevalence of physical, verbal and nonverbal sexual harassments and their association with psychological distress among Jimma University female students: a cross-sectional study. Ethiop J Health Sci. 2015;25(1):29–38.
Sivertsen B, Nielsen MB, Madsen IEH, Knapstad M, Lønning KJ, Hysing M. Sexual harassment and assault among university students in Norway: a cross-sectional prevalence study. BMJ Open. 2019;9(6):e026993–e.
Klein LB, Martin SL. Sexual Harassment of College and University students: a systematic review. Trauma Violence Abuse. 2019:1524838019881731.
Mahlangu P, Machisa M, Sikweyiya Y, Nunze N, Dartnall E, Pillay M et al. Preliminary evidence of promise of a sexual violence risk reduction intervention for female students in South African tertiary education institutions. Glob Public Health. 2021.
Machisa M, Chirwa ED, Mahlangu P, Sikweyiya Y, Nunze N, Dartnall E et al. Factorsassociatedwithfemalestudents’pastyearexperienceofsexualviolenceinSouthAfricanpublichighereducationsettings:a cross-sectionalstudy. PLoS ONE. 2021;16(12).
Klein LL, Graham LM, Treves-Kagan S, Deck PG, DeLong SM, Martin SL. Leveraging data to strengthen campus sexual assault policies. J Interpers Violence. 2018;33(21):3298–314.
Beyene AS, Chojenta C, Roba HS, Melka AS, Loxton D. Gender-based violence among female youths in educational institutions of Sub-saharan Africa: a systematic review and meta-analysis. Syst Rev. 2019;8(1):59.
Ajayi AI, Mudefi E, Owolabi EO. Prevalence and correlates of sexual violence among adolescent girls and young women: findings from a cross-sectional study in a South African university. BMC Womens Health. 2021;21(1):299.
Mathur S, Okal J, Musheke M, Pilgrim N, Kishor Patel S, Bhattacharya R, et al. High rates of sexual violence by both intimate and non-intimate partners experienced by adolescent girls and young women in Kenya and Zambia: findings around violence and other negative health outcomes. PLoS ONE. 2018;13(9):e0203929–e.
Hay K, McDougal L, Percival V, Henry S, Klugman J, Wurie H, et al. Disrupting gender norms in health systems: making the case for change. Lancet. 2019;393(10190):2535–49.
Liani ML, Nyamongo IK, Pulford J, Tolhurst R. Institutional-level drivers of gender-inequitable scientific career progression in sub-saharan Africa. Health Res Policy Syst. 2021;19(1).
Eagle G, Kwele K. You just come to School, if you made it, its grace: young black women’s experiences of violence in Utilizing Public Minibus Taxi Transport in Johannesburg, South Africa. J Interpers Violence. 2021;36(15–16):Np8034–55.
Mayeza E, Bhana D, Mulqueeny D. Normalising violence? Girls and sexuality in a South African high school. J Gend Stud. 2022;31(2):165–77.
Fisher M, Nyabaro V, Mendum R, Osiru M. Making it to the PhD: gender and student performance in sub-saharan Africa. PLoS ONE. 2020;15(12).
Hossain M, Pearson RJ, McAlpine A, Bacchus LJ, Spangaro J, Muthuri S, et al. Gender-based violence and its association with mental health among Somali women in a Kenyan refugee camp: a latent class analysis. J Epidemiol Commun Health. 2021;75(4):327–34.
McClain TS, Kammer-Kerwick M, Wood L, Temple JR, Busch-Armendariz N. Sexual harassment among medical students: prevalence, prediction, and correlated outcomes. Workplace Health Saf. 2021;69(6):257–67.
Vallières F, Gilmore B, Nolan A, Maguire P, Bondjers K, McBride O et al. Sexual violence and its associated psychosocial effects in Ireland. J Interpers Violence. 2020:0886260520978193.
Rothman K, Georgia Salivar E, Roddy MK, Hatch SG, Doss BD. Sexual assault among women in college: Immediate and long-term associations with mental health, psychosocial functioning, and romantic relationships. J Interpers Violence. 2019:0886260519870158.
Tsai MH, Chen YH, Chen CD, Hsiao CY, Chien CH. Deliberate self-harm by Taiwanese adolescents. Acta Paediatr. 2011;100(11):e223–6.
Masters NT, Stappenbeck CA, Kaysen D, Kajumulo KF, Davis KC, George WH, et al. A person-centered approach to examining heterogeneity and subgroups among survivors of sexual assault. J Abnorm Psychol. 2015;124(3):685–96.
Kearl H, Johns N, Raj A. Measuring# MeToo: a national study on sexual harassment and assault. UC San Diego Center on Gender Equity and Health; 2019.
Kearl H. Stop global street harassment: growing activism around the world: growing activism around the world. ABC-CLIO; 2015.
Campbell R, Dworkin E, Cabral G, An ecological model of, the impact of sexual assault on women’s mental health. Trauma Violence Abuse. 2009;10(3):225–46.
Vandemark LM, Mueller M. Mental health after sexual violence: the role of behavioral and demographic risk factors. Nurs Res. 2008;57(3):175–81.
Grose RG, Roof KA, Semenza DC, Leroux X, Yount KM. Mental health, empowerment, and violence against young women in lower-income countries: a review of reviews. Aggress Violent Beh. 2019;46:25–36.
Central Statistical Office, Kingdom of Eswatini. The 2017 Population and Housing Census volume 3. Eswatini: Central Statistical Office; 2019.
Anderson M, Bamrah S, Blanton C, Breiding M, Dahlberg LL, Mercy JA et al. A National study on violence against children and young women in Swaziland. 2007.
Fielding-Miller R, Shabalala F, Masuku S, Raj A. Epidemiology of campus sexual assault among University women in Eswatini. J Interpers Violence. 2019:0886260519888208.
Baron EC, Davies T, Lund C. Validation of the 10-item centre for Epidemiological Studies Depression Scale (CES-D-10) in Zulu, Xhosa and Afrikaans populations in South Africa. BMC Psychiatry. 2017;17(1):6.
Koss MP, Oros CJ. Sexual experiences Survey: a research instrument investigating sexual aggression and victimization. J Consult Clin Psychol. 1982;50(3):455.
StataCorp. Stata statistical software: release 16. College Station. TX: StataCorp LLC; 2019.
Sorbom D. Model modification. Psychometrika. 1989;54(3):371–84.
Kline RB. Structural equation modeling. New York: Guilford; 1998.
Zijlmans EAO, Tijmstra J, van der Ark LA, Sijtsma K. Item-score reliability in Empirical-Data sets and its relationship with other Item Indices. Educ Psychol Meas. 2018;78(6):998–1020.
Raj A, Johns N, Jose R. Racial/Ethnic disparities in sexual harassment in the United States, 2018. J Interpers Violence. 2019:886260519842171.
Akinbode GA, Ayodeji F. Sexual harassment: experiences, prevalence and psychopathology in some selected higher institutions in Lagos, South-West Nigeria. Afr J Psychol Stud Social Issues. 2018;21(3):112–36.
Connell R. Gender and power: Society, the person and sexual politics. Wiley; 2013.
Ullman SE, Relyea M. Social Support, Coping, and posttraumatic stress symptoms in female sexual assault survivors: a longitudinal analysis. J Trauma Stress. 2016;29(6):500–6.
Dworkin ER, Ojalehto H, Bedard-Gilligan MA, Cadigan JM, Kaysen D. Social support predicts reductions in PTSD symptoms when substances are not used to cope: a longitudinal study of sexual assault survivors. J Affect Disord. 2018;229:135–40.
Dworkin ER, Ullman SE, Stappenbeck C, Brill CD, Kaysen D. Proximal relationships between social support and PTSD symptom severity: a daily diary study of sexual assault survivors. Depress Anxiety. 2018;35(1):43–9.
Fielding-Miller R, Shabalala F, Masuku S, Raj A. Epidemiology of campus sexual assault among University women in Eswatini. J Interpers Violence. 2021;36(21–22):NP11238–63.
Hawn SE, Lind MJ, Conley A, Overstreet CM, Kendler KS, Dick DM, et al. Effects of social support on the association between precollege sexual assault and college-onset victimization. J Am Coll Health. 2018;66(6):467–75.
Cantor D, Fisher B, Chibnall SH, Townsend R, Lee H, Thomas G et al. Report on the AAU campus climate survey on sexual assault and sexual misconduct. 2015.
Phillips AE, Gomez GB, Boily MC, Garnett GP. A systematic review and meta-analysis of quantitative interviewing tools to investigate self-reported HIV and STI associated behaviours in low- and middle-income countries. Int J Epidemiol. 2010;39(6):1541–55.
Fielding-Miller R, Mnisi Z, Adams D, Baral S, Kennedy C. There is hunger in my community: a qualitative study of food security as a cyclical force in sex work in Swaziland. BMC Public Health. 2014;14(1):79.
Fielding-Miller R, Dunkle KL, Murdock D. Not everyone can afford an apple a day: stigma and food insecurity in rural South African young adults. Afr J AIDS Res. 2015;14(4):361–9.
Hatcher AM, Page S, Van Aletta L, Pearson I, Fielding-Miller R, Mazars C, et al. Systematic review of food insecurity and violence against women and girls: mixed methods findings from low- and middle-income settings. PLOS Global Public Health. 2022;2(9):e0000479.
Bloom BE, Wagman JA, Dunkle K, Fielding-Miller R. Exploring intimate partner violence among pregnant Eswatini women seeking antenatal care: how agency and food security impact violence-related outcomes. Glob Public Health. 2022;17(12):3465–75.
Dhillon M, Bakaya S. Street harassment:a qualitative study of the experiences of Young women in Delhi. SAGE Open. 2014;4(3):2158244014543786.
Jaffe S. The collective power of# MeToo. Dissent. 2018;65(2):80–7.
Johns NE, Raj A, Lee DS, Kearl H. Measuring #MeToo in California: a statewide assessment of sexual harassment and assault. Sacramento, CA, USA: California Coalition Against Sexual Assault (CALCASA); 2019.
Wånggren L. Our stories matter: storytelling and social justice in the hollaback! Movement. Gend Educ. 2016;28(3):401–15.
Acknowledgements
The study team wishes to thank the women who shared their time and stories with us to make this research happen. We are indebted to their generosity of spirit. We thank the staff and administration of the University of Eswatini for their willingness to support this work and desire to build an evidence-based response to sexual violence on campus. RFM wishes to thank her research assistant, Ms. Esther Krohne, who made vital contributions to survey programming and in-person training activities.
Funding
Funding was provided by a Sexual Violence Research Initiative (SVRI) and World Bank Development Marketplace Research Grant. Additional support was provided by the National Institutes of Mental Health (K01MH112436, PI: Fielding-Miller).
Author information
Authors and Affiliations
Contributions
RFM: Conceptualization, methodology, formal analysis, data curation, writing (original draft), supervision, funding acquisition; LM and EF: Writing (review and editing); SM: Conceptualization, project administration, writing (reviewing and editing); FS: Conceptualization, methodology, resources, writing (reviewing and editing), supervision, funding acquisition.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
All research was performed in accordance with the Declaration of Helsinki. The study was reviewed and approved by UNESWA Research Ethics Board and the University of California, San Diego Institutional Review Board (IRB) (Federalwide Assurance 00004495; protocol 181603). Data collection procedures followed the World Health Organization’s Recommendations for Intervention Research on Violence Against Women. All participants provided informed written consent previous to completing a survey. A research assistant who was trained in trauma informed counselling was always available while participants completed the survey. The study team made pro-active efforts to reduce vicarious trauma in frontline staff, including engaging in regular debriefing sessions and ensuring that a local, no-cost third party counselor was available to all staff members.
Consent for publication
NA.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Fielding-Miller, R., McDougal, L., Frost, E. et al. Association between sexual violence and depression is mediated by perceived social support among female university students in the kingdom of Eswatini. BMC Public Health 24, 2526 (2024). https://doi.org/10.1186/s12889-024-20040-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12889-024-20040-8