
Abstract
Background
Breastfeeding offers numerous benefits for infants, mothers, and the community, making it the best intervention for reducing infant mortality and morbidity. The World Health Organization (WHO) recommends initiating breastfeeding within one hour after birth and exclusively breastfeeding for the first six months. This study investigated the trend, spatio-temporal variation, and determinants of spatial clustering of early initiation of breastfeeding (EIBF) and exclusive breastfeeding (EBF) in Ethiopia from 2011 to 2019.
Methods
Data from the Ethiopian Demographic and Health Survey (EDHS), which was conducted in 2011, 2016, and 2019, were analyzed utilizing a weighted sample of 10,616 children aged 0–23 years for EIBF and 2,881 children aged 0–5 months for EBF. Spatial autocorrelation analysis was used to measure whether EIBF and EBF were dispersed, clustered, or randomly distributed and Kriging interpolation was employed to predict the outcome variables in the unmeasured areas. Spatial scan statistics were used to identify spatial clusters with a high prevalence of cases. Both global and local regression modeling techniques were employed to examine the spatial relationships between the explanatory variables and the dependent variables.
Results
The trend analysis revealed a notable increase in the prevalence of EIBF from 51.8% in 2011 to 71.9% in 2019. Similarly, the prevalence of EBF increased from 52.7% in 2011 to 58.9% in 2019. Spatial analysis demonstrated significant spatial variation in both EIBF and EBF throughout the country. Cold spots or clusters with a low prevalence of EIBF were observed consistently in the Tigray and Amhara regions, and significant cold spot areas of EBF were observed consistently in the Afar and Somali regions. Multiscale geographically weighted regression analysis revealed significant predictors of spatial variations in EIBF, including the religious affiliation of being a follower of the orthodox religion, parity of 1–2, absence of antenatal care visits, and delivery via cesarean section.
Conclusions
Despite the increase in both EIBF and EBF rates over time in Ethiopia, these rates still fall below the national target. To address this issue, the government should prioritize public health programs aimed at improving maternal healthcare service utilization and maternal education. It is essential to integrate facility-level services with community-level services to achieve optimal breastfeeding practices. Specifically, efforts should be made to promote breastfeeding among mothers who have delivered via cesarean section. Additionally, there should be a focus on encouraging antenatal care service utilization and adapting maternal healthcare services to accommodate the mobile lifestyle of pastoralist communities. These steps will contribute to enhancing breastfeeding practices and achieving better outcomes for maternal and child health.
Similar content being viewed by others
Introduction
Breast milk is the optimal source of nutrition for newborns, as it meets all nutritional needs for the first six months of life. Breastfeeding offers numerous benefits for infants, mothers and the community [1,2,3]. Infants benefit from a decreased incidence and severity of infectious diseases [4,5,6]; improved neurodevelopment [7, 8]; reduced risk of necrotizing enterocolitis [9]; and decreased risks of obesity, cardiovascular risk, diabetes [10] and post neonatal infant mortality [11]. Maternal health benefits include birth spacing [12], a quicker return to pre-pregnancy weight [13], reduced risk of breast cancer, ovarian cancer [14], cardiovascular diseases [15], type 2 diabetes [16] and maternal depression [17]. Breastfeeding plays a significant role in preventing the mortality of more than 820,000 children under 5 years of age and 20,000 deaths from breast cancer each year, contributing to the reduction in under-five and maternal mortality rates [18].
To obtain the benefits of breastfeeding, the WHO and the United Nations Children’s Fund (UNICEF) recommended initiating breastfeeding within one hour after birth and exclusively breastfeeding for the first six months [19]. However, despite efforts to promote early breast feeding initiation [20], only 47% of newborns globally begin breastfeeding within the first hour after birth [21]. In 2012, only 38% of infants under six months of age were exclusively breastfed, which increased to 40% in 2016 [22], and as of 2021, the rate has reached 48% [21]. This indicates that we are approaching the 2025 target for EBF, which is set at 50% [22]. Yet we still fall short of reaching the sustainable development goal (SDG) target for 2030, which is aimed at achieving a 70% EBF rate [23].
Between 2010 and 2018, the global weighted prevalence of early initiation of breastfeeding and exclusive breastfeeding in low- and middle-income countries (LMICs) was 51.9% and 45.7%, respectively [24]. In sub-Saharan Africa (SSA), the overall prevalence of EIBF was 52.8%, with the lowest prevalence observed in Guinea (16.5%) and the overall prevalence of EBF was 41.1%, with the lowest prevalence found in Gabon (6.04%) [25].
Regardless of the progress that has been achieved in Ethiopia, mainly due to different initiatives and programs (such as infant and young child feeding practices, training of health-extension workers and baby-friendly hospital initiatives [26, 27]), only 61.4% of neonates are breastfed within an hour after delivery and just 59.3% of infants are breastfed exclusively [28, 29]. The country is still falling behind in achieving SDG and its national target which is to increase the proportion of EIBF to 92% and that of EBF to 70% [30]. Previously conducted research in Ethiopia have identified factors that are associated with EIBF and EBF, including religion, region, area of residence, household wealth index, marital status, media exposure, maternal education, maternal age, employment status of the mother, antenatal care, place of delivery, mode of delivery, postnatal care, sex of the child and parity [31,32,33,34,35].
Studies have reported significant geographical variation in the prevalence of EIBF and EBF across regions in Ethiopia [35] and one study focused solely on the trends in EIBF and EBF without demonstrating how these trends aligned with geographical variations [34]. To address these limitations, we conducted a comprehensive trends and spatio-temporal analyses of EIBF and EBF from 2011 to 2019. Furthermore, our study incorporated a multiscale geographically weighted regression (MGWR) analysis to overcome the limitations of another prior study [36] that relied on geographically weighted regression (GWR) to investigate the relationships between the EIBF and independent variables. The MGWR model examines the local spatial relationships between clusters of EIBF and EBF and their predictors. This approach improves upon the drawbacks of GWR by adjusting both the space and scale, allowing variables to operate at different scales [37]. Identification of significantly varying predictors across space helps to implement interventions that increase location-specific governmental effort in improving the magnitudes of EIBF and EBF and achieving targets. Hence, the objective of this study was to investigate the trend, spatial variation and spatial determinants of EIBF among children aged 0–23 months and EBF among infants aged 0–5 months in Ethiopia.
Methods and materials
Study setting, design and data
The study was conducted in Ethiopia, which is located in the Horn of Africa. The country is divided into 11 regions and two city administrations, including the two regions which were introduced after the surveys were conducted. Tigray, Afar, Amhara, Oromia, Southern Nations Nationalities and People (SNNP), Benishangul Gumuz, Gambella, Somali, Harari, Sidama, Southwest Ethiopia, Addis Ababa and Dire Dawa [38].
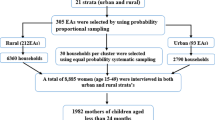
The data used in this study were obtained from three consecutive nationally representative cross-sectional surveys: EDHS 2011 [39], 2016 [40] and 2019 [41]. All the EDHS used a two-stage stratified cluster sampling procedure involving the selection of clusters in the first stage and the selection of households in the second stage. Cluster selection was stratified by place of residence (urban or rural area) and district or woreda, which was further subdivided into kebeles, and each kebele was then subdivided into enumeration areas (EAs). Location data or latitudinal and longitudinal coordinates were included in the selected EAs.
Population
The source populations for this study were all children aged 0–23 months and all children aged 0–5 months in Ethiopia for EIBF and EBF, respectively. We used the Kids record dataset (KR file), and a total weighted sample of 10,616 children aged 0–23 months was included for the EIBF 2011 (4,308), 2016 (4,222) and 2019 (2,086) surveys. A total of 2,881 weighted children aged 0–5 months were analyzed for the EBF 2011 (1179), 2016 (1162) and 2019 (540) surveys after excluding children who did not live with their mother and keeping only the youngest child.
Study variables
The dependent variables for this study were early initiation of breastfeeding (yes/no) and exclusive breastfeeding (yes/no). EIBF was defined as the percentage of children aged 0–23 months who were put to the breast within one hour of birth. EBF was defined as the percentage of infants aged 0–5 months who were fed exclusively breast milk with no other food or drink, not even water [42]. The independent variables considered in the study were residence, household wealth index, marital status, media exposure, maternal education, maternal age, employment status of the mother, antenatal care, place of delivery, mode of delivery, postnatal care, sex of the child and parity. The geographical regions of the participants were categorized into three regions: the larger central region (Tigray, Amhara, Oromia, and SNNP), the small peripheral region (Afar, Somali, Benishangul, and Gambella) and the metropolis region (Harari, Dire Dawa, and Addis Ababa) [43]. Participants were considered to have media exposure if they watched television, listened to the radio or read a newspaper [44].
Data management and analysis
Data extraction, coding and descriptive analysis were conducted using Stata version 17. The data were weighted using sampling weights before any statistical analysis to make them representative. We employed frequency and percentage distributions to report respondent characteristics and trends. The weighted proportions of the dependent and independent variables were extracted by cross tabulating with the cluster number (v001) and exported as a CSV file. The data were subsequently exported to ArcGIS version 10.7 for exploration and visualization of EIBF and EBF in Ethiopia at the regional level during the three survey years. Spatial regression analysis and visualization of significant variables were conducted with Python 3 software.
Spatial autocorrelation
Spatial autocorrelation was employed to examine whether the spatial patterns of EIBF and EBF in Ethiopia were randomly distributed, dispersed or clustered. Global Moran’s I statistics were used to identify the spatial pattern. The range of Moran’s I is from − 1 to 1. A value close to -1 indicates strong dispersion, a value close to 1 indicates strong clustering, and a value close to 0 indicates no spatial autocorrelation or randomness. A statistically significant Moran’s I value reflects the presence of spatial autocorrelation [45, 46].
Hotspot analysis
Hotspot analysis was also conducted to identify areas with statistically significant clustering. The Getis–Ord Gi* statistic was calculated to determine the presence of concentrations that exhibited significantly higher or lower values. It generates an output feature class containing the z score, p value and confidence level bin field (Gi_Bin). The Gi_Bin field categorizes areas of EIBF and EBF into statistically significant hot spots and cold spots at different confidence levels (99%, 95% and 90%). A feature is considered a statistically significant hotspot if it has a high value and is surrounded by other features with high values. On the other hand, a feature is deemed a statistically significant cold spot if it has a low value and is surrounded by other features with low values [47, 48].
Spatial interpolation
A spatial interpolation technique was used to predict the spatial patterns of EIBF and EBF in areas where data were not directly observed from the sampled measurements. The kriging spatial interpolation method was utilized to make predictions about unsampled areas [49].
Spatial scan analysis
Spatial scan statistics was conducted to detect statistically significant spatial clusters with high and low prevalence of EIBF and EBF in Ethiopia. A circular scanning window was used to traverse the study area. The Bernoulli-based model was employed using Kuldorff’s SaTScan version 9.6 software. The case (presence of an outcome variable), control (absence of an outcome variable) and coordinate file (latitude and longitude) were taken to the software to determine the location of the significant clusters. Most likely or primary clusters were identified using p values and likelihood ratio tests. The cluster with the maximum likelihood ratio constitutes the primary cluster [50]. Using the default maximum spatial cluster size of 50% in terms of the total population at risk could hide small core clusters, and a too small maximum size could miss significant clusters in a larger size [51]. Hence, we set the maximum spatial cluster size to 20% of the population at risk to ensure the resulting circles were of a modest size.
Modeling spatial relationships
Using the most recent survey data from the EDHS 2019, we employed spatial regression analysis to identify predictors of the observed spatial patterns of EIBF and EBF in Ethiopia. To examine the spatial relationship between the explanatory variables and the dependent variables, both global and local regression modeling approaches were employed.
Global regression modeling
The ordinary least square (OLS) regression analysis is a global model that was applied as a preliminary test of the correlation between the dependent and independent variables [52]. It assumes a stationary and constant relationship over space, which implies that the relationships do not vary over space [53]. To assess the magnitude of multicollinearity in the model, the variance inflation factor (VIF) was utilized. The OLS model is calculated as follows:
where yi is the dependent variable, β0 is the intercept, xi represents the independent variable, βi is the corresponding coefficient and ε is the error [52].
Local regression modeling
Geographically weighted regression relaxes the assumption of OLS regression by allowing the coefficients to vary spatially. GWR is employed when the Koenker statistics is significant, indicating that the relationships between the outcome and the covariates change from location to location. GWR assumes that the relationships between the outcome and explanatory variables are nonstationary, meaning that they vary spatially. Therefore, the GWR model estimates a local parameter for each location separately. However, it assumes that all the coefficients change at a similar rate across the study area and uses a single constant bandwidth [54]. The GWR model is calculated as follows:
where (ui, vi) represents coordinates; β0 and βk are the intercept and the coefficient of local variable k at location i, respectively; and xik is the kth variable at location i [52].
The multiscale geographically weighted regression model is an extended and advanced version of GWR. This approach allows the relationship between dependent and independent variables to vary spatially and at different spatial scales by using different bandwidths rather than a single constant bandwidth across the study area [53, 55]. The MGWR model is calculated as follows:
The parameters are almost the same as those of GWR, except for the indicated label bw, which represents the different bandwidths of each variable [52].
We assessed the presence of multicollinearity using the variance inflation factor (VIF). The performances of both the local and global models, were compared by the Akaike information criterion (AIC), residual sum of squares (RSS), and adjusted R-squared values [56].
Results
Trends in EIBF and EBF in Ethiopia
We included a total weighted sample of 10,616 children aged 0–23 months and 2,881 children aged 0–5 months in the analysis. The majority of the children were from the larger central regions, while metropolitan areas contained the minority of children in both age groups. Table 1 shows the weighted frequency of participant characteristics in each survey year, with the proportion of EIBF and EBF in parentheses.
The prevalence of early initiation of breastfeeding in Ethiopia increased from 51.8% (95% CI: 50.3%, 53.3%) in 2011 to 73.6% (95% CI: 72.2%, 74.9%) in 2016 and decreased to 71.9% (95% CI: 69.9%, 73.7%) in 2019. Similarly, the prevalence of exclusive breastfeeding increased from 52.7% (95% CI: 49.8%, 55.5%) in 2011 to 57.3% (95% CI: 54.4%, 60.0%) in 2016 to 58.9% (95% CI: 54.7%, 63.0%) in 2019. The small peripheral regions (Afar, Somali, Benushangul and Gambela) had the lowest prevalence of both EIBF and EBF across all survey years, while the larger central regions had the highest prevalence. (Table 1)
Spatial analysis
Spatial variation in EIBF and EBF in Ethiopia
Spatial autocorrelation revealed significant spatial variations in EIBF (Supplementary Fig. 1) and EBF (Supplementary Fig. 2) throughout Ethiopia in all three surveys conducted from 2011 to 2019. The global Moran’s I values revealed a significantly clustered pattern for both outcomes, with a p-value less than 0.05. These findings suggested that the clustering pattern is less likely to be a result of random chance. Rather, both EIBF and EBF exhibited significantly clustered patterns. This finding implies the need to investigate the two outcomes across different regions of the country.
Hotspot analysis of EIBF and EBF in Ethiopia
In the 2011 EDHS, hotspots (high numbers of cases of EIBF surrounded by high numbers of cases) among children younger than 24 months were identified in various regions, including Dire Dawa, Harari, Addis Ababa, parts of eastern and central Oromia, northern Gambela, Sidama and eastern and central SNNP. Conversely, significant cold spot (low numbers of cases of EIBF are surrounded by low cases) areas were observed in central Tigray; central, southern and some parts of northern Amhara; and central, eastern and western Benishangul regions (Fig. 1A). By the 2016 EDHS, hotspots of EIBF were still spotted in Dire Dawa, Harari, parts of eastern and central Oromia, Sidama and northern SNNP. Cold spot areas were detected in the central and eastern Tigray, central and southern Afar, and southern and central Amhara regions (Fig. 1B). Moving to the 2019 EDHS, EIBF hotspots were concentrated in Addis Ababa, some parts of central Oromia, parts of northern SNNP, some parts of northern Gambela and southern and western Benishangul. Cold spots of EIBF were identified in southern parts of the SNNP and certain areas of the central Somali region (Fig. 1C).

Hotspot analysis of EIBF among children aged 0–23 months in 2011 (A), 2016 (B), and 2019 (C) and EBF among children aged 0–5 months in 2011 (D), 2016 (E), and 2019 (F) in Ethiopia
In terms of EBF, in the 2011 EDHS hotspot areas of EBF, where high cases of EBF were surrounded by high cases, were detected in central Tigray, northern and central Amhara, western Benishangul, northern SNNP, Sidama and some parts of central Oromia. On the other hand, cold spots of EBF were identified in northern Gambela, some parts of central and southern Afar, and some parts of the northeastern Oromia region (Fig. 1D). Moving to the 2016 EDHS, hotspots of EBF were identified in eastern and southern Tigray, the western border of Afar with Tigray, northeastern Amhara, a part of southeastern Benishangul and a part of southern Oromia at the border with the Gedeo zone in the SNNP. Cold spot areas were observed in the central and eastern Somali region (Fig. 1E). Finally, in the 2019 EDHS, EBF hotspots were identified in central and northern Amhara, most parts of Benishangul, northern SNNP and the Sidama region. Cold spots were detected in central and eastern Somali, central Afar and southern Afar regions bordering the Amhara region (Fig. 1F).
Spatial interpolation of EIBF and EBF in Ethiopia
We used kriging interpolation to predict geographical variations in EIBF and EBF in unpredicted areas based on the observed data. The resulting predictions were represented using a color scheme in which green indicates predicted areas with lower proportions of EIBF and EBF, while red indicates areas with higher proportions of EIBF and EBF. According to the sampled data from the 2011 EDHS, interpolation predicted the highest prevalence of EIBF in Addis Ababa, Dire Dawa, northern Gambela, Sidama and southern and eastern SNNP (Fig. 2A). Similarly, in the 2016 EDHS, the highest prevalence of EIBF was predicted in Dire Dawa, Harari, parts of eastern, central and southern Oromia, parts of northern Somali and some parts of southern Benishangul based on the sampled data (Fig. 2B). Similarly, for the 2019 EDHS, the predicted highest prevalence of EIBF was concentrated in parts of northwestern Gambella and the southwestern part of the Benishangul borderline with Oromia (Fig. 2C) based on the sampled areas.

Spatial interpolation of EIBF among children aged 0–23 months in 2011 (A), 2016 (B), and 2019 (C) and EBF among children aged 0–5 months in 2011 (D), 2016 (E), and 2019 (F) in Ethiopia
In the 2011 EDHS, the highest prevalence of EBF was predicted based on sampled areas in the northern, central and western parts of Amhara, parts of southwestern Benishangul, northern SNNP, Sidama provinces and parts of northern and southwestern Oromia (Fig. 2D). According to the 2016 EDHS, the highest prevalence of EBF was predicted in various regions, including western, eastern and southern Tigray, northern and northeastern Amhara, central and eastern Benishangul, Addis Ababa, central and southern Oromia, Sidama and some parts of the eastern SNNP and northern Somali (Fig. 2E). Moving to the 2019 EDHS, the sampled data predicted the highest prevalence of EBF in central, western and northeastern Amhara; most parts of Benishangul; parts of central southern and eastern Oromia; some areas in the eastern SNNP bordering Sidama and Oromia; and the Sidama region (Fig. 2F).
Sat-scan analysis
The results of the SaTScan analysis of EIBF and EBF throughout the EDHS survey years are displayed in Fig. 3. The most likely primary and secondary clusters of EIBF and EBF were identified. For EIBF, a total of 129 locations for the primary and secondary clusters were detected in 2011, 103 in 2016 and 39 in 2019. Similarly, for EBF, a total of 30, 84 and 11 primary and secondary clusters were detected in 2011, 2016 and 2019, respectively. (Table 2)

SaTScan analysis of EIBF among children aged 0–23 months 2011 (A), 2016 (B) and EBF among children aged 0–5 months 2016 (C) in Ethiopia
In the EDHS 2011, the primary cluster spatial window of EIBF was found in Dire Dawa and Harari, with a relative risk (RR) of 1.24 and a log likelihood ratio (LLR) of 17.7, at a p-value < 0.001. It revealed children between the ages of 0 and 23 months in the spatial window had a 1.28-fold greater chance of having early initiation of breastfeeding than did those outside the window (Fig. 3A). Based on the 2016 EDHS, the primary or most likely cluster was identified in Eastern Oromia, northern Somali, Harari and Dire Dawa (Fig. 3B), with an RR of 1.29 and an LLR of 27.6, at a p-value < 0.001. This showed that children under the age of 24 months in this spatial window had a 1.3 times greater chance of experiencing EIBF than children outside the window. According to the 2019 EDHS, the spatial window of the primary spatial cluster resulted in an RR of 1.23, an LLR of 6.17 and a p-value of 0.26. This clustering is more likely to occur as a result of chance because the nonsignificant p-value prevents us from ruling out that the cluster was formed by chance. (Table 2)
Considering exclusive breastfeeding, in the 2011 and 2019 EDHS, the spatial window of the primary clusters resulted in RR of 1.30 and 1.37, LLR of 2.97 and 2.68, and p-value of 0.96 and 1.00, respectively. This revealed that clustering was more likely to occur by chance in both survey years, as the nonsignificant p-values failed to rule out that the clusters were formed by chance. The spatial window of the primary cluster in the 2016 EDHS was located in most parts of Tigray and central and northern Amhara, with an RR of 1.42, an LLR of 13.3 and a p-value of 0.0011. The significant p-value ruled out the possibility that the cluster was formed by chance. Therefore, children between the ages of 0 and 5 months are 1.42 times more likely to have EBF than are those outside the window (Fig. 3C) (Table 2).
Spatial regression analysis
We conducted an ordinary least square regression to investigate the assumptions of spatial regression. The model for EIBF yielded statistically significant results, as indicated by the significant Joint F-statistics and Wald statistics. Additionally, the Koenker statistics were also statistically significant, suggesting nonstationarity or heterogeneity in the relationship between the outcome and the explanatory variables across the study areas. Therefore, local models were employed because they assume that the relationship between the independent variables and the dependent variable has spatial heterogeneity (as confirmed by Koenker statistics). We did not observe any multicollinearity issues among the explanatory variables since all the variables had a VIF of less than 7.5. The coefficient estimates displayed a combination of positive and negative values and the most influential variable. Specifically, the proportion of cesarean delivery emerged as the most influential variable, followed by the proportion of no antenatal care visit. The statistically significant variables of the EIBF included the proportion of participants who were Orthodox religion followers, the proportion of participants with a parity of 1–2, the proportion of participants with no antenatal care visit, and the proportion of participants with a cesarean delivery. (Table 3)
On the contrary, the model for EBF did not yield statistically significant results, as indicated by the Joint F-statistics and Wald statistics, which were not significant. Furthermore, the Koenker statistics was not statistically significant suggesting stationarity or homogeneity in the relationship between the outcome and the explanatory variables across the study area. As a result, we were unable to apply local models for EBF. (Table 3)
Model comparison (global and local models)
Due to the presence of spatial non stationarity in the relationship between EIBF and the independent variables, OLS regression was not adequate for accurately describing the underlying relationship. Therefore, we employed a spatially nonstationary local modeling approaches, namely, GWR and MGWR, using the same set of predictors utilized in the global model. The local models exhibited better model performance than did the global model. The adjusted R2 increased from 0.100 (OLS) to 0.258 (GWR) and 0.355 (MGWR). The residual sum of squares, which shows unexplained variations, was high in the OLS model (261.1) but decreased to 194.7 (GWR) to 159.4 (MGWR). Additionally, the AICc decreased from 850.3 in OLS to 826.4 in GWR and 809.8 in MGWR. GWR outperformed OLS, while MGWR outperformed GWR. This is because MGWR allows for covariate-specific bandwidths instead of relying on a single average bandwidth, leading to improved model performance. (Table 4)
The GWR model utilized a single bandwidth of 237, which means that 237 nearest neighbors were considered to inform the construction of parameter estimates at each local regression point. On the other hand, the MGWR computes an optimum bandwidth for each variable. The presence of multiple bandwidths in MGWR allowed the model to account for an optimal number of neighbors to estimate each parameter, which allowed better predictions of the dependent variable. The bandwidths range from 67 to 300. Specifically, the bandwidths for the significant variables were 290 for the proportion of mothers who are orthodox religion followers, 67 for the proportion of mothers with a parity of 1–2, 71 for the proportion of mothers with no antenatal care visit, and 159 for the proportion of mothers with cesarean delivery. (Table 5)
Mapping parameter coefficients
The coefficients of GWR (Fig. 4, left) and MGWR (Fig. 4, right) for EIBF were mapped for the intercept and statistically significant variables. The local intercept is interpreted as the value of the dependent variable that would be expected if every location had exactly the same average value of each independent variable. Based on the mapping of the intercept coefficients, the local intercept in the local models is interpreted as the level of EIBF that would be expected in each region holding all covariates constant. The intercepts in both the GWR and MGWR were not statistically different from zero because they had no statistically nonzero parameter estimates. (Supplementary Fig. 3)

GWR (left) and MGWR (right) parameter estimates for the proportion of being orthodox religion follower, parity of 1–2, no antenatal care visit and cesarean delivery to show local patterns of spatial heterogeneity. Grey dots are not statistically different from zero
The coefficient estimates of being the orthodox religion follower have a negative association with EIBF. Compared to the GWR, this variable displays little spatial heterogeneity in MGWR model as it has a negative association with EIBF all over the country. Regardless of location, the MGWR results support the trend that living in a neighborhood with a higher proportion of orthodox religion is linked with lower EIBF throughout the country. The MGWR also displays the coefficient estimates of the variable para 1–2, which shows a positive association with EIBF in Addis Ababa and parts of central Oromia. This finding implies that mothers who have 1 or 2 children are more likely to have EIBF in Addis Ababa and parts of central Oromia. However, the GWR estimate does not have a nonzero parameter estimate. (Fig. 4)
The MGWR reveals that parameter estimates for no antenatal care visits (absence of ANC) tend to have a negative association with EIBF in pastoralist regions of Ethiopia (central and southern Afar and central, western and southwestern Somali region). This finding indicates that mothers who did not have ANC follow-up tend to have a lower chance of engaging in EIBF in central and southern Afar and central, western and southwestern Somali regions. The GWR estimates also showed spatial heterogeneity. The coefficient estimates of the variable cesarean delivery was manifested to have a negative association with EIBF. The MGWR model showed that mothers who deliver their baby by cesarean delivery tend to have a lower chance of engaging in EIBF in parts of western Tigray, western Amhara, central and southern Afar, eastern Oromia, Harari, Dire Dawa, and most parts of the Somali region. The GWR estimates also showed spatial heterogeneity. (Fig. 4)
Discussion
It is recommended that all newborns start breastfeeding immediately after birth, and exclusive breastfeeding for the first six months of life provides balanced nutrition and prevents child morbidity and mortality. This study examined the overall temporal trend and spatial trend as well as the projection of early initiation and exclusive breastfeeding in Ethiopia. Additionally, spatial modeling was used to explore the spatial predictors of the observed geographical variation based on the EDHS data collected in 2011, 2016 and 2019.
Between 2011 and 2019, the magnitude of the EIBF increased from 51.8% in 2011 to 71.9% in 2019; this value is considered good according to the WHO classification, where EIBF is classified as poor (0–29%), fair (30–49%), good (50–89%) or very good (90–100%) [57]. The magnitude of EBF also increased from 52.7% in 2011 to 58.9% in 2019, which was categorized as good based on the WHO classification. Similarly, previous studies reported that the prevalence of EIBF increased from 47.4% in 2000 to 66.2% in 2011 and that of EBF increased from 54.5% in 2000 to 59.9% in 2016 [31,32,33,34]. Overall, in low- and middle-income countries, 39% of children were breastfed within one hour of birth, with wide variation by region [58]. The prevalence of EIBF in Ethiopia in 2019 was greater than that in lower- and lower-middle-income countries, including Sudan (69%), Ghana (55.1%), the Economic Community of West African States (ECOWAS) (43%), India (41.5%) and Bangladesh (51.2%) [59,60,61,62,63]. The total prevalence of EBF among infants under six months of age in Sub-Saharan Africa was 37% [64], which is lower than the prevalence in Ethiopia. The increase in the prevalence of EIBF and EBF in Ethiopia can be attributed to government efforts, such as the national strategy for infant and young child feeding in the country and the implementation of strategies, including health extension programs [65]. However, despite the improvements in the prevalence of EIBF and EBF in Ethiopia, the country lags far from achieving its targets set by the health sector development program [30].
The national prevalence of EIBF and EBF varies by administrative region across the country. For instance, in 2019, the prevalence of EIBF ranged from 57.3% in the Somali region to 81.4% in the Oromia region. Similarly, the percentage of EBF ranged from 42.2% in Dire Dawa to 82.9% in Benishangul. This variation was confirmed by Moran’s I statistics, which revealed significant geographical variation in EIBF and EBF in the three survey years throughout the country. This findings highlight the role of geography in determining the variation in EIBF and EBF in Ethiopia.
As identified by the hotspot analysis, significant clusters of cold spots of the EIBF, where low numbers of cases of EIBF were surrounded by low numbers of cases, were consistently observed in the three survey years in the Tigray and Amhara regions. This can be explained by the repetitive occurrence of drought in the northern parts of the country, which contributes to poor breastfeeding practices. The political instabilities in these regions might also disturb the implementation of maternal and child health programs [31]. The significant clusters of cold spots in EBF were more or less consistent in the three waves of the EDHS observed in the Afar and Somali regions. This is supported by a study in Ethiopia in which pastoralist regions were less likely to exclusively breastfeed [66]. This is because their mobile lifestyle provides them with a weak healthcare system, which prevents them from understanding the importance of exclusive breastfeeding. Hence, they might initiate cow milk earlier [67].
The spatial scan analysis of EIBF revealed that in the 2011 EDHS, the most likely primary SaTScan clusters were identified in DireDawa and Harari. In 2016, EDHS those clusters were identified in Dire Dawa, Harari, eastern Oromia and the northern Somali region. Children in this spatial window had a better chance of having EIBF than did those outside the window. A previous study [68] indicated that mothers from the Oromia, Harari and Dire Dawa regions were more likely to experience EIBF. Regarding EBF, a significant primary SaTScan cluster was detected only in the 2016 EDHS in the Tigray and Amhara regions. Children in this spatial window had a better chance of EBF than did those outside the window. It has been shown that other regions have lower odds of EBF as compared to the larger central regions (including Tigray and Amhara) [34]. This spatial inequality may be related to most residents of the larger central regions being rural dwellers, and mothers residing in rural areas are more likely to exclusively breastfeed, which can be explained by differences in maternal employment [69, 70].
In this research, the MGWR model overcame the limitations of the OLS and GWR models and resulted in a well-fitted model of EIBF among children aged 0–23 months. The key findings obtained from this study were variables that impact EIBF and vary geographically. The significant predictors obtained were orthodox religion, parity of 1–2, absence of antenatal care visits, and cesarean delivery. Despite the regional location, the MGWR results showed that neighborhoods with a higher proportion of orthodox religion followers had lower rates of EIBF among children younger than 24 months in Ethiopia. This is supported by a similar study in which GWR was utilized in Ethiopia [36]. The parity of 1–2 have more regional and local relationships with EIBF. Parity of 1–2 children has a significant positive relation with EIBF in Addis Ababa and parts of central Oromia. This can be explained by the fact that mothers who are multipara or grand multipara have better prior breastfeeding experience and fewer breastfeeding problems, unlike primiparous women, who usually have delays from delivery to their first breastfeeding attempt. The more experience the mother has, the more likely the infant is to be put to the breast within one hour of delivery [71,72,73].
Having no antenatal care follow-up had a significant negative association with EIBF in central and southern Afar and central, western and southwestern Somali region or pastoralist regions of Ethiopia. This could be due to the counseling and support services provided for newborn feeding practices that mothers obtain when attending ANC visits. ANC is also a means of enhancing mothers’ understanding of the advantages of EIBF by overcoming cultural obstacles related to infant feeding practices [74, 75]. Furthermore, mothers from pastoral regions in Ethiopia utilize health facility services at low levels as they move long distances with their livestock following seasonal movements [76].
Children who were delivered by cesarean section had lower rates of EIBF in parts of the western Tigray, western Amhara, central and southern Afar, eastern Oromia, Harari, Dire Dawa, and most parts of the Somali region. This finding is consistent with a study conducted in Ethiopia utilizing GWR [36]. Several studies have shown that cesarean delivery plays a role in delaying breastfeeding initiation. A possible explanation might be that separating newborns from their mothers after CS leads to insufficient milk production, reduced time spent at the mother’s breast, decreased neonatal interest in breastfeeding and worsening of the wellbeing and psychology of the mother, which might contribute to delays in breastfeeding initiation [77,78,79,80].
Strength and limitations
This study has limitations that must be considered when the results are interpreted. As the DHS data are cross-sectional and only capture a snapshot of information at a particular moment, we were unable to show the cause‒effect relationship between the outcome variable and covariates being examined. Participant responses are also prone to recall bias, as the survey used a 24-h recall method for measuring EBF, but we conducted the analysis on the youngest child who lived with the mother to reduce the effect of bias. Despite these limitations, the study has several strengths. The study is conducted based on weighted, nationally representative data. Appropriate spatial statistical methods were also used to geographically target interventions. GWR and MGWR were conducted on the basis of the latest DHS data from 2019 to identify spatial predictors of EIBF among children under the age of 24 months.
Conclusion
Three consecutive national surveys were used (EDHS 2011, 2016 and 2019), and the trends in EIBF and EBF have shown an increase over time despite still being below the national target. EIBF and EBF varied geographically across regions, and the distributions were nonrandom throughout the three surveys. Therefore, public health programs that improve maternal healthcare service utilization and maternal education should target the cold spot areas of EIBF and EBF in the country. This study utilized a spatial modeling framework to explore the relationship between EIBF and a set of covariates in Ethiopia. Global and local models were applied and compared to explain the spatial heterogeneity, and the MGWR provided the best overall fit. The single-bandwidth assumption of GWR was relaxed by MGWR, in which each covariate had its own bandwidth. The explanatory variables that had a significant influence on the spatial variation in EIBF in Ethiopia were being a follower of the orthodox religion, having a parity of 1–2, not visiting antenatal care, and a cesarean delivery. To address these barriers, the government should integrate facility-level services at the community level to achieve optimal breastfeeding. Mother-to-mother support groups can be utilized to sustain gains in breastfeeding; specifically, multiparous mothers can share their experience with nulliparous and primiparous mothers. To prevent delayed initiation of breastfeeding and early discontinuation of EBF, it is important to address postpartum exhaustion, discomfort, pain and any issues related to cesarean delivery. Strategies and guidance for breastfeeding should be promoted for mothers who experience CS delivery. Antenatal care service utilization must also be encouraged by creating awareness, ensuring service accessibility and availability and improving quality of care. For pastoralist communities, maternal health care services should be suited to their mobile lifestyle, limited access to health care facilities and cultural considerations. The mobile-clinic approach can reach pastoralist communities in different locations by providing health care services directly.
Data availability
The data are available from http://www.dhsprogram.com.
Abbreviations
- AIC:
-
Akaike information criterion
- CS:
-
Cesarean Section
- EAs:
-
Enumeration areas
- EBF:
-
Exclusive Breastfeeding
- EDHS:
-
Ethiopian Demographic and Health Survey
- EIBF:
-
Early Initiation of Breastfeeding
- GWR:
-
Geographically Weighted Regression
- LMICs:
-
low- and middle-income countries
- MGWR:
-
Multiscale Geographically Weighted Regression
- OLS:
-
Ordinary Least Square
- RSS:
-
Residual Sum of Squares
- SDG:
-
Sustainable Development Goal
- SNNP:
-
Southern Nations Nationalities Peoples
- SSA:
-
Sub-Saharan Africa
- WHO:
-
World Health Organization
References
American Academy of Pediatrics. Breastfeeding and the Use of Human Milk. Pediatrics. 2005;115(2):496–506. https://doi.org/10.1542/peds.2004-2491
Brahm P, Valdes V. Benefits of breastfeeding and risks associated with not breastfeeding. Rev Chil Pediatr. 2017;88(1):15–21.
Prentice AM. Breastfeeding in the Modern World. Ann Nutr Metab. 2022;78(Suppl. 2):29–38. https://doi.org/10.1159/000524354
Eidelman AI, Schanler RJ, Johnston M, Landers S, Noble L, Szucs K et al. Breastfeeding and the Use of Human Milk. Pediatrics. 2012;129(3):e827–41. https://doi.org/10.1542/peds.2011-3552
Ip S, Chung M, Raman G, Chew P, Magula N, DeVine D et al. Breastfeeding and maternal and infant health outcomes in developed countries. Evid Rep Technol Assess (Full Rep). 2007;(153):1–186. http://europepmc.org/abstract/MED/17764214
Heinig MJ. Host Defense Benefits of Breastfeeding for the Infant: Effect of Breastfeeding Duration and Exclusivity. Pediatr Clin North Am. 2001;48(1):105–23. https://www.sciencedirect.com/science/article/pii/S0031395505702881
Mortensen EL, Michaelsen KF, Sanders SA, Reinisch JM. The association between duration of breastfeeding and adult intelligence. JAMA. 2002;287(18):2365–71.
Reynolds A. Breastfeeding and brain development. Pediatr Clin North Am. 2001;48(1):159–71.
Herrmann K, Carroll K. An Exclusively Human Milk Diet Reduces Necrotizing Enterocolitis. Breastfeed Med. 2014;9(4):184–90. https://doi.org/10.1089/bfm.2013.0121
Kelishadi R, Farajian S. The protective effects of breastfeeding on chronic non-communicable diseases in adulthood: a review of evidence. Adv Biomed Res. 2014;3:3.
Chen A, Rogan WJ. Breastfeeding and the Risk of Postneonatal Death in the United States. Pediatrics. 2004;113(5):e435–9. https://doi.org/10.1542/peds.113.5.e435
Becker S, Labbok MH. Estimation of births averted due to breast-feeding and rutsteins, increases in levels, of contraception needed to substitute for breast-feeding. J Biosoc Sci. 2003/10/16. 2003;35(4):559–74. https://www.cambridge.org/core/article/estimation-of-births-averted-due-to-breastfeeding-and-increases-in-levels-of-contraception-needed-to-substitute-for-breastfeeding/4D696663F9065A750EFE12094FC9C132
Bobrow KL, Quigley MA, Green J, Reeves GK, Beral V. Collaborators for the MWS. Persistent effects of women’s parity and breastfeeding patterns on their body mass index: results from the Million Women Study. Int J Obes. 2013;37(5):712–7. https://doi.org/10.1038/ijo.2012.76
Chowdhury R, Sinha B, Sankar MJ, Taneja S, Bhandari N, Rollins N et al. Breastfeeding and maternal health outcomes: a systematic review and meta-analysis. Acta Paediatr. 2015;104(S467):96–113. https://doi.org/10.1111/apa.13102
Tschiderer L, Seekircher L, Kunutsor SK, Peters SAE, O’Keeffe LM, Willeit P. Breastfeeding Is Associated With a Reduced Maternal Cardiovascular Risk: Systematic Review and Meta-Analysis Involving Data From 8 Studies and 1 192 700 Parous Women. J Am Heart Assoc. 2022;11(2):e022746. https://doi.org/10.1161/JAHA.121.022746
Aune D, Norat T, Romundstad P, Vatten LJ. Breastfeeding and the maternal risk of type 2 diabetes: A systematic review and dose–response meta-analysis of cohort studies. Nutr Metab Cardiovasc Dis. 2014;24(2):107–15. https://www.sciencedirect.com/science/article/pii/S0939475313002743
Dias CC, Figueiredo B. Breastfeeding and depression: A systematic review of the literature. J Affect Disord. 2015;171:142–54. https://www.sciencedirect.com/science/article/pii/S016503271400576X
Victora CG, Bahl R, Barros AJD, França GVA, Horton S, Krasevec J et al. Breastfeeding in the 21st century: epidemiology, mechanisms, and lifelong effect. Lancet. 2016;387(10017):475–90. https://doi.org/10.1016/S0140-6736(15)01024-7
World Health Organization. Breastfeeding. 2023 [cited 2023 Dec 10]. https://www.who.int/health-topics/breastfeeding#tab=tab_2
Taqi I. Global Breastfeeding Advocacy Initiative. Breastfeed Med. 2014;9(7):355–7. https://doi.org/10.1089/bfm.2014.0084
UNICEF. Infant and young child feeding. 2022. https://data.unicef.org/topic/nutrition/infant-and-young-child-feeding/
WHO, UNICEF. WHO/UNICEF discussion paper. The extension of the 2025 maternal, infant and young child nutrition targets to 2030. 2019. https://data.unicef.org/resources/who-unicef-discussion-paper-nutrition-targets/
World Health Organization. Global breastfeeding scorecard. 2018: Enabling women to breastfeed through better policies and programmes. 2018. https://www.who.int/publications/m/item/global-breastfeeding-scorecard-2018-enabling-women-to-breastfeed-through-better-policies-and-programmes
Zong X, Wu H, Zhao M, Magnussen CG, Xi B. Global prevalence of WHO infant feeding practices in 57 LMICs in 2010–2018 and time trends since 2000 for 44 LMICs. EClinicalMedicine. 2021;37:100971.
Issaka AI, Agho KE, Renzaho AM. Prevalence of key breastfeeding indicators in 29 sub-saharan African countries: a meta-analysis of demographic and health surveys (2010–2015). BMJ Open. 2017;7(10):e014145.
Federal Ministry of Health - FMoH. Guideline for Infant and Young Child Feeding in Emergencies for Ethiopia. 2021. https://www.afro.who.int/sites/default/files/2022-08/Guideline for Infant and Young Child Feeding in Emergencies.pdf.
Martin L. LINKAGES/Ethiopia. 2006. https://pdf.usaid.gov/pdf_docs/Pdaci280.pdf
Alebel A, Dejenu G, Mullu G, Abebe N, Gualu T, Eshetie S. Timely initiation of breastfeeding and its association with birth place in Ethiopia: a systematic review and meta-analysis. Int Breastfeed J. 2017;12(1):44. https://doi.org/10.1186/s13006-017-0133-x
Alebel A, Tesma C, Temesgen B, Ferede A, Kibret GD. Exclusive breastfeeding practice in Ethiopia and its association with antenatal care and institutional delivery: a systematic review and meta-analysis. Int Breastfeed J. 2018;13:31.
Federal Ministry of Health - FMoH. Health Sector Development Program IV 2010/11–2014/15. 2010. https://www.healthynewbornnetwork.org/hnn-content/uploads/HSDP-IV-Final-Draft-October-2010-2.pdf
Amare T, Dellie E, Amare G. Trends of inequalities in early initiation of Breastfeeding in Ethiopia: evidence from Ethiopian demographic and health surveys, 2000–2016. Biomed Res Int. 2022;2022:5533668.
Lucha TA, Mengistu AK. Factors associated with early initiation of breastfeeding among children less than 24 months old: the 2019 Ethiopian mini demographic and health survey. Arch Public Heal. 2022;80(1):164. https://doi.org/10.1186/s13690-022-00920-4
Muluneh MW. Determinants of exclusive breastfeeding practices among mothers in Ethiopia. PLoS One. 2023;18(2):e0281576. https://doi.org/10.1371/journal.pone.0281576
Ahmed KY, Page A, Arora A, Ogbo FA. Trends and determinants of early initiation of breastfeeding and exclusive breastfeeding in Ethiopia from 2000 to 2016. Int Breastfeed J. 2019;14(1):40. https://doi.org/10.1186/s13006-019-0234-9
Woldeamanuel BT. Trends and factors associated to early initiation of breastfeeding, exclusive breastfeeding and duration of breastfeeding in Ethiopia: evidence from the Ethiopia Demographic and Health Survey 2016. Int Breastfeed J. 2020;15(1):3. https://doi.org/10.1186/s13006-019-0248-3
Hailegebreal S, Haile Y, Seboka BT, Enyew EB, Shibiru T, Mekonnen ZA et al. Modeling spatial determinants of initiation of breastfeeding in Ethiopia: A geographically weighted regression analysis. PLoS One. 2022;17(9):e0273793. https://doi.org/10.1371/journal.pone.0273793
Sharma A. Exploratory spatial analysis of food insecurity and diabetes: an application of multiscale geographically weighted regression. Ann GIS.:1–14. https://doi.org/10.1080/19475683.2023.2208199
Ethiopia forms a new regional state. 2021. https://newbusinessethiopia.com/politics/ethiopia-forms-a-new-regional-state/
/Central Statistical Agency, Ethiopia ICF, International. Ethiopia Demographic and Health Survey 2011. Addis Ababa, Ethiopia: Central Statistical Agency/Ethiopia and ICF International; 2012. http://dhsprogram.com/pubs/pdf/FR255/FR255.pdf
CSA/Ethiopia CSA. ICF. Ethiopia Demographic and Health Survey 2016. Addis Ababa, Ethiopia: CSA and ICF; 2017. http://dhsprogram.com/pubs/pdf/FR328/FR328.pdf
ICF. Ethiopia Mini Demographic and Health Survey 2019. Addis Ababa, Ethiopia: EPHI/FMoH/ICF. 2021. https://www.dhsprogram.com/pubs/pdf/FR363/FR363.pdf
WHO/UNICEF. Indicators for assessing infant and young child feeding practices: Definitions and measurement methods. 2021. https://www.who.int/publications/i/item/9789240018389
Abrha S, Shiferaw S, Ahmed KY. Overweight and obesity and its socio-demographic correlates among urban Ethiopian women: evidence from the 2011 EDHS. BMC Public Health. 2016;16(1):636. https://doi.org/10.1186/s12889-016-3315-3
Bitew DA, Asmamaw DB, Belachew TB, Negash WD. Magnitude and determinants of women’s participation in household decision making among married women in Ethiopia, 2022: Based on Ethiopian demographic and health survey data. Heliyon. 2023;9(7):e18218. https://www.sciencedirect.com/science/article/pii/S2405844023054269
Ord JK, Getis A. Local Spatial Autocorrelation Statistics: Distributional Issues and an Application. Geogr Anal. 1995;27(4):286–306. https://doi.org/10.1111/j.1538-4632.1995.tb00912.x
Eboy OV, Dambul R. Viewing preferences of TVRO users in Sabah: identification of distribution patterns using spatial statistics. Geogr Malaysian J Soc Sp. 2011;7(4):30–7.
De Valck J, Broekx S, Liekens I, De Nocker L, Van Orshoven J, Vranken L. Contrasting collective preferences for outdoor recreation and substitutability of nature areas using hot spot mapping. Landsc Urban Plan. 2016;151:64–78.
Hotspot analysis. [cited 2023 Oct 9]. https://pro.arcgis.com/en/pro-app/latest/tool-reference/spatial-statistics/hot-spot-analysis.htm
Bhunia GS, Shit PK, Maiti R. Comparison of GIS-based interpolation methods for spatial distribution of soil organic carbon (SOC). J Saudi Soc Agric Sci. 2018;17(2):114–26.
Kulldorff M. SaTScanTM user guide. Boston; 2006.
Jin C, MacEachren A, Lengerich E. Visual analytics of spatial scan statistic results. PurdueEdu.
Liu L, Yu H, Zhao J, Wu H, Peng Z, Wang R. Multiscale Effects of Multimodal Public Facilities Accessibility on Housing Prices Based on MGWR: a case study of Wuhan, China. Volume 11. ISPRS International Journal of Geo-Information; 2022.
Mansour S, Al Kindi A, Al-Said A, Al-Said A, Atkinson P. Sociodemographic determinants of COVID-19 incidence rates in Oman: Geospatial modelling using multiscale geographically weighted regression (MGWR). Sustain Cities Soc. 2021;65:102627. https://www.sciencedirect.com/science/article/pii/S2210670720308441
Charlton M, Fotheringham AS, Brunsdon C. Geographically weighted regression white paper. Kildare Natl Univ Irel Maynooth. 2009;1–14.
He Y, Seminara PJ, Huang X, Yang D, Fang F, Song C. Geospatial Modeling of Health, Socioeconomic, demographic, and Environmental Factors with COVID-19 incidence rate in Arkansas, US. Volume 12. ISPRS International Journal of Geo-Information; 2023.
Li Z, Fotheringham AS, Oshan TM, Wolf LJ. Measuring Bandwidth Uncertainty in Multiscale Geographically Weighted Regression Using Akaike Weights. Ann Am Assoc Geogr. 2020;110(5):1500–20. https://doi.org/10.1080/24694452.2019.1704680
World Health Organization. Infant and young child feeding: A tool for assessing national practices, policies and programmes. Geneva. 2003. https://www.who.int/publications/i/item/9241562544
Oakley L, Benova L, Macleod D, Lynch CA, Campbell OMR. Early breastfeeding practices: Descriptive analysis of recent Demographic and Health Surveys. Matern Child Nutr. 2018;14(2):e12535. https://doi.org/10.1111/mcn.12535
Abdel-Rahman ME, El-Heneidy A, Benova L, Oakley L. Early feeding practices and associated factors in Sudan: a cross-sectional analysis from multiple Indicator cluster survey. Int Breastfeed J. 2020;15(1):41. https://doi.org/10.1186/s13006-020-00288-7
Duodu PA, Duah HO, Dzomeku VM, Boamah Mensah AB, Aboagye Mensah J, Darkwah E, et al. Consistency of the determinants of early initiation of breastfeeding in Ghana: insights from four demographic and Health Survey datasets. Int Health. 2021;13(1):39–48.
Ezeh OK, Ogbo FA, Stevens GJ, Tannous WK, Uchechukwu OL, Ghimire PR et al. Factors Associated with the Early Initiation of Breastfeeding in Economic Community of West African States (ECOWAS). Vol. 11, Nutrients. 2019.
Senanayake P, O’Connor E, Ogbo FA. National and rural-urban prevalence and determinants of early initiation of breastfeeding in India. BMC Public Health. 2019;19(1):896. https://doi.org/10.1186/s12889-019-7246-7
Sen KK, Mallick TS, Bari W. Gender inequality in early initiation of breastfeeding in Bangladesh: a trend analysis. Int Breastfeed J. 2020;15(1):18. https://doi.org/10.1186/s13006-020-00259-y
Bhattacharjee NV, Schaeffer LE, Marczak LB, Ross JM, Swartz SJ, Albright J et al. Mapping exclusive breastfeeding in Africa between 2000 and 2017. Nat Med. 2019;25(8):1205–12. https://doi.org/10.1038/s41591-019-0525-0
Federal Ministry of Health - FMoH. National Strategy for Infant and Young Child Feeding. 2004.
Tsegaw SA, Ali Dawed Y, Tadesse Amsalu E. Exploring the determinants of exclusive breastfeeding among infants under-six months in Ethiopia using multilevel analysis. PLoS One. 2021;16(1):e0245034. https://doi.org/10.1371/journal.pone.0245034
Belachew AB, Kahsay AB, Abebe YG. Individual and community-level factors associated with introduction of prelacteal feeding in Ethiopia. Arch Public Health. 2016;74:6.
Mengistu GT, Mengistu BK. Early initiation of breast feeding and associated factors among mother-baby dyads with immediate skin-to-skin contact: cross-sectional study based on the 2016 Ethiopian Demographic and Health Survey data. BMJ Open. 2023;13(3):e063258. http://bmjopen.bmj.com/content/13/3/e063258.abstract
Wallenborn JT, Valera CB, Kounnavong S, Sayasone S, Odermatt P, Fink G. Urban-rural gaps in Breastfeeding practices: evidence from Lao people’s Democratic Republic. Int J Public Health. 2021;66:1604062.
Menon P, Garrett J, Slack A. Urbanization and caregiving: a framework for analysis and examples from southern and eastern Africa. Environ Urban. 2011;21.
Hackman NM, Schaefer EW, Beiler JS, Rose CM, Paul IM. Breastfeeding outcome comparison by parity. Breastfeed Med off J Acad Breastfeed Med. 2015;10(3):156–62.
Ekubay M, Berhe A, Yisma E. Initiation of breastfeeding within one hour of birth among mothers with infants younger than or equal to 6 months of age attending public health institutions in Addis Ababa, Ethiopia. Int Breastfeed J. 2018;13:4.
Neves RO, Bernardi JR, da Silva CH, Goldani MZ, Bosa VL. Can parity influence infant feeding in the first six months of life? Cien Saude Colet. 2020;25(11):4593–600.
Ayalew DD, Kassie BA, Hunegnaw MT, Gelaye KA, Belew AK. Determinants of Early Initiation of Breastfeeding in West Belessa District, Northwest Ethiopia. Nutr Metab Insights. 2022;15:11786388211065220. https://doi.org/10.1177/11786388211065221
Mrisho M, Obrist B, Schellenberg JA, Haws RA, Mushi AK, Mshinda H, et al. The use of antenatal and postnatal care: perspectives and experiences of women and health care providers in rural southern Tanzania. BMC Pregnancy Childbirth. 2009;9:10.
Dessie AM, Anley DT, Zemene MA, Aychew EW, Debebe HG, Misganaw NM et al. Health facility delivery service utilization and its associated factors among women in the pastoralist regions of Ethiopia: A systematic review and meta-analysis. Heal Sci Reports. 2023;6(4):e1183. https://doi.org/10.1002/hsr2.1183
Wax JR. Maternal request cesarean versus planned spontaneous vaginal delivery: maternal morbidity and short term outcomes. Semin Perinatol. 2006;30(5):247–52.
Patel RR, Liebling RE, Murphy DJ. Effect of operative delivery in the second stage of labor on breastfeeding success. Birth. 2003;30(4):255–60.
Regan J, Thompson A, DeFranco E. The influence of mode of delivery on breastfeeding initiation in women with a prior cesarean delivery: a population-based study. Breastfeed Med off J Acad Breastfeed Med. 2013;8(2):181–6.
Gedefaw G, Goedert MH, Abebe E, Demis A. Effect of cesarean section on initiation of breast feeding: findings from 2016 Ethiopian demographic and Health Survey. PLoS ONE. 2020;15(12):e0244229.
Acknowledgements
We would like to acknowledge the measure DHS program for providing the dataset to use the EDHS 2011, 2016 and 2019.
Funding
The authors received no funding.
Author information
Authors and Affiliations
Contributions
T.M.T wrote the main manuscript and analyzed the data. TM.T, B.L.S, B.F.K, K.U.M, Y.S.A, Z.A.A, H.A.A, A.H.S, A.A.L, K.G.S, and B.M.F revised, reviewed and finalized the manuscript.
Corresponding author
Ethics declarations
Ethical approval and consent to participate
The research involved secondary data analysis of survey data from the MEASURE DHS program, which was free and publicly available (EDHS 2011, 2016 and 2019); therefore, ethical approval and participant consent were not needed. We obtained permission from the DHS program and access the data for our study from their website http://www.dhsprogram.com.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Tebeje, T.M., Seifu, B.L., Mare, K.U. et al. Geospatial determinants and spatio-temporal variation of early initiation of breastfeeding and exclusive breastfeeding in Ethiopia from 2011 to 2019, a multiscale geographically weighted regression analysis. BMC Public Health 24, 2011 (2024). https://doi.org/10.1186/s12889-024-19552-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12889-024-19552-0