
Abstract
Background
Soil-transmitted helminth (STH) infection control remains a priority in endemic regions where local epidemiological data are needed for sustainable control strategies, particularly regarding population knowledge, attitudes, and practices (KAP). Our work assessed KAP toward STH infection and associated factors among residents of Bata district, Equatorial Guinea.
Methods
A community-based cross-sectional study was conducted among 14 randomly selected communities in the Bata district. Eligible participants were interviewed face-to-face using a standardized questionnaire. Participants aged under 18 years were interviewed in the presence of their parents or legal guardians. For participants aged less than ten, a simplified version of the main questionnaire was developed focusing on children’s practices toward STH and was administered to their parents or legal guardians.
Results
A total of 399 participants were included in the present analysis. Among them, 58% responded to the main questionnaire. The mean (± SD) age of participants aged 10 and over was 37.5 (± 22.2) years, and 60% of them were females, while the mean (± SD) age of those aged less than ten was 5.0 (± 2.5) years. The respondents’ overall knowledge, attitudes, and practices to STH were rated as bad (33%), very good (77%), and good (55%), respectively. Knowledge was significantly associated with education level (p = 0.04) with the knowledge level lower for participants with no formal education than for those with secondary/university education (β = -0.56, 95% CI: -1.00 – -0.12, p = 0.01); Appropriate attitudes level was significantly associated with occupation (p = 0.02) and education levels (p = 0.049) with the appropriate attitude level lower for students than for farmers/fishers (β = -1.24, 95% CI: -2.17—-0.32, p = 0.01) and for primary-level participants than for those with secondary/university education (β = -0.68, 95% CI: -1.23—-0.13, p = 0.02); while appropriate practice level were significantly associated with age (p = 0.01), occupation (p = 0.01), and education (p = 0.02), with the appropriate practices level increasing with age (β = 0.03, 95% CI: 0.005 – 0.05, p = 0.01) and lower in participants with no formal education than in those with secondary/university education (β = -1.19, -2.05 – -0.32, p = 0.007).
Conclusion
The present study revealed a lack of knowledge about STH in the study population, particularly regarding disease causes and transmission ways, highlighting the need for the implementation of integrated health education strategies, both at the community and school levels.
Similar content being viewed by others


Background
Among over 20 diseases classified as Neglected Tropical Diseases (NTDs), soil-transmitted helminth (STH) infections are the most prevalent [1]. The main agents responsible for these infections in human populations are Ascaris lumbricoides, Trichuris trichiura, hookworms (Ancylostoma duodenal and Necator americanus), and Strongyloides stercoralis. Although STH are transmitted mostly in tropical and subtropical regions particularly in areas with poor sanitation, limited access to safe water, and limited economic resources for proper hygiene practices [2]. They constitute a global public health concern. Indeed, there are distributed all over the world, with more than 1.5 billion people infected [3]. In the World Health Organization (WHO) African region, an estimated 350 million individuals are considered at risk for STH infections [4].
STH infections produce a great variety of symptoms that are expressed depending on the parasite infection load. These symptoms include diarrhea, abdominal pain, micronutrient deficiencies, malnutrition, malaise and weakness [5]. Children are the most affected population group, with great impact on their physical growth and cognitive development [6, 7]. In co-endemic areas, STH infections can affect the morbidity of other infectious diseases, such as human immunodeficiency virus [8], malaria [9], and tuberculosis [10]. The morbidity related to STH infection places endemic societies in a state of continuous poverty, making the disease a major public health issue [5, 11].
To attain the WHO 2030 road map for eliminating STHs as a public health problem [12], the WHO proposed periodic community mass deworming for the control of disease morbidity, and the availability of safe water, proper sanitation, hygiene (WASH) and health education for the exposed population to reduce disease transmission [12,13,14]. Community deworming is the most widely implemented intervention worldwide and is considered fundamental in terms of cost and effectiveness [11, 15]. For the control of disease transmission, providing safe water and adequate sanitation aims at reducing environmental fecal contamination, while implementing health education aims at reducing inappropriate attitudes and practices of the population toward the disease. This integrated approach is highly recommended for successful control programs [5, 11]. In 2020, Nath and collaborators [16] reported a significant improvement in the knowledge of the population on STH infections after health education intervention, as well as in STH preventive behaviors and Mass Drug Administration (MDA) involvement attitudes [16], demonstrating that the integration of health education can be a key element to improve STH control in endemic areas. Therefore, for a tailored health education program, the knowledge, attitude, and practice (KAP) of the population toward STH need to be assessed to, for instance, understand the population knowledge gap and misconception of the disease, the risk-full attitudes and practices and their willingness to participate in the implementation of control strategies. KAP surveys are indeed known as basic tools for guiding the proper development of health education strategies [11, 17].
Equatorial Guinea (EG) is a central African country known to be highly endemic for STH [8, 18,19,20]. Indeed, the country is reported among the 20 nations with the highest prevalence of STH before 2003, and among the 12 from 2003 to 2018 [20], indicating the necessity to improve the current situation of STH control in the country. In that vein, if school-aged children and peri-urban areas have previously reported to be at greater risk of STH infections in the most populated district of the country [18], the specific contribution of the population is not yet known. As the country has adhered to the WHO’s recommendations for the control of STH [21], the objective of the present study was to assess for the first time in the country the knowledge, attitudes, and practices of the population toward STH infections, which could contribute to the tailored design of a health education strategy and the optimization of other STH control strategies.
Methods
Study area
The EG, a country located in central Africa, comprises the continental or Rio Muni mainland and the insular Bioko and Annobon islands (Fig. 1). The study was conducted in the district of Bata, one of the 19 districts of the country [22]. Bata city is the capital of Bata district, one of the two main cities in the EG, and it is in the coastal zone of the mainland. It is the largest district in the country, with 25% of the total country population [22]. The survey was conducted in two out of the three municipalities of the Bata district, namely the municipalities of Bata and Rio Campo, where a 60% prevalence of any STH was recently reported [18]. In terms of WASH, 55% of the population have improved water sources; where, 21% are public sources; regarding sanitation; 39.7% have access to improved non-shared facilities, for house floor materials, 54% are cement floors; and 47.4% have a hand washing specific place [23]. The main occupations of the local populations are artisanal fishing, hunting, subsistence agriculture and trading [22].

Map showing the geographical location of Equatorial Guinea (Right panel) and communities at Bata district were the study was conducted (Left panel). The base layer for the country and national border shape was obtained from the ©2018–2022 GADM; an open license database (https://gadm.org/download_country.html). QGIS version 3.22.16 was used to create the map
Study design and study population
The study was a cross-sectional household community KAP survey carried out from October 2020 to January 2021. Volunteers who lived in the selected communities for at least three months before the survey and who were aged one year or older were eligible to participate in the survey.
Sample size consideration
The present survey was conducted concomitantly with a study aiming to determine the prevalence of STH infection in EG, particularly the Bata district, from which the initial sample size was calculated [18]. From the total of 403 participants initially included, 399 were considered in the present analysis as they were able to complete the questionnaires. Of them, 233 (58%) were aged 10 years and above. Considering an expected prevalence of 50% (for a maximum possible sample size) and using the formula of sample size calculation for surveys as described by Charan et al. [24], 233 participants give us a precision of 6.4% in the estimation of the proportion of participants’ appropriate knowledge, adequate attitudes or practices regarding STH infection. In addition, the remaining 166 participants were aged less than 10 and therefore specific questions on their practices towards STH were directed to their parents/guardians.
Sampling and study procedures
The Bata district is divided into three municipalities: Bata, the most populous; Machinda; and Rio Campo. Each municipality is divided into a neighborhood community for the urban zone or into village communities for the peri-urban and rural zones. Participants were selected by applying a three-stage sampling procedure. The first stage consisted of a random selection of two out of the three municipalities (Bata and Rio campo), and the second stage included a probability proportion to the population size in each unit site. In both municipalities, we selected five neighborhoods (representing the urban zone), five peri-urban areas and four villages (representing the rural zone) for a total of 14 communities. The third stage included a convenience selection of households, and where two participants were to be randomly selected and interviewed, based on our eligibility criteria. So, after arriving at a selected household, permission was requested from the person in charge of the household. When permission was granted, the study objectives and participation conditions were explained to the house inhabitants in Spanish and, if needed, in the community local language by a member of the research team originating from the community. Only after that were the volunteers requested to participate. Among those who agreed to participate, eligible volunteers were included in the study after providing informed consent. An identification code was assigned for each participant for confidentiality purposes, and the interviewer administered the questionnaire to the respondent during a face-to-face interview of approximately 15 min. Respondents under 18 years old were interviewed in the presence of their parents or legal guardians. For children aged one to nine years, specific questions on their behavior and practices toward the disease were addressed to their parents or legal guardians.
Data collection
Participant information was collected through a paper case report form that included the study questionnaire.
The standardized study questionnaires
The main study questionnaire (see Supplementary material S1) was designed to collect sociodemographic data and to capture the knowledge, attitudes, and practices of the respondents toward STH infection. The questionnaire aimed to capture knowledge about STH from the perspective of the respondents, appropriate and inappropriate respondents’ attitudes, and practices. In the first section of the questionnaire, sociodemographic questions were asked. In the second section of the questionnaire, open- and close-ended questions about respondents’ knowledge were developed. To ensure a better understanding of the respondents, the term “human intestinal parasite” (“worms”) was used instead of “soil-transmitted helminths”. The third and fourth sections of the questionnaire were designed to collect information on the attitudes and practices of the respondents, respectively. For participants’ attitudes, multiple-choice and open-ended questions were included, while for participant practices, only multiple-choice questions were included. The simplified version of the questionnaire (see Supplementary material S2) developed from the main questionnaire was designed to capture sociodemographic, knowledge, attitude and practices of participants’ (aged 10 to 17) related to STH infection. All questionnaires were built in English and translated into Spanish — the national language — pretested, and the final versions were validated by a research committee created for the purpose.
Statistical analysis
All data collected were digitized using EpiData software version 3.1 and exported to Stata version 13 for analysis. For the respondents’ knowledge assessment, the participants were asked questions with the possibility of providing a maximum of two answers per question. One (1) point was given for each correct answer, while zero (0) points were assigned for each wrong answer, giving a possible total score of six (6) (see Supplementary Table S1). For attitudes and practices assessment, answers to the closed-ended questions were quoted on one (1) mark if correct, while a wrong answer was quoted on zero (0) mark, giving a total possible score of nine (9) and 14, respectively (see Supplementary Table S2 and S3). For knowledge, attitudes, and practices, the mean score for the whole study population was calculated and translated as a percentage. The population level of knowledge, attitudes, and practices was then classified as “bad” if the calculated percentage was less than 50%, “good” if between 50 and 69%, “very good” if between 70 and 89%, and "excellent” if equal to or greater than 90%.
For descriptive statistics, categorical variables were summarized in numbers and proportions, while continuous variables were described as the mean and standard deviation (SD) when normally distributed. The associations between knowledge, attitudes and practices and the sociodemographic characteristics of the respondents were computed using first a simple linear regression model and expressed with the β coefficient and its 95% confidence interval (95% CI). If more than one variable had a p value equal to or less than 0.25, adjusted analysis was performed for all variables included in the final model. A p value less than 0.05 was considered to indicate statistical significance.
Results
Study population characteristics
As presented in Table 1, the mean (± SD) age of the 233 participants (aged from 10 years and above) who responded to the questionnaire was 37.5 (± 22.2) years, with 60% female representation. Most of them (104, 45%) lived in urban areas, while a majority (100, 43%) had a primary education level. Eighty-six (37%) of them were students, and 71 (30%) were farmers/fishermen. For the 166 participants (aged from one year to nine years old) for whom specific questions were directed to their parents or guardians, the mean (± SD) age was 5.0 (± 2.5) years, with 55% male representation. Most of them (72, 43%) lived in urban areas, and more than half (112, 68%) had a primary education, while the remaining 54 (23%) participants had no formal education.
Distribution of background knowledge about STH infection among the study population
In Table 2, we present the background information on STH infection knowledge of the 233 participants who responded to the questionnaire. Of them, 184 (79%) respondents had already heard about human intestinal worms, while 191 (82%) of them considered it a disease. The principal places where they heard about STHs for the first time were at home, representing less than half (82, 35%) of the respondents.
The distribution of knowledge on the causes, symptoms, and prevention of STH infection among the 233 participants who answered the questionnaire is summarized in Table 3. On the question about the cause of STH infection, one out of every three respondents (76; 33%) gave correct answers, while approximately one out of two respondents gave correct answers about disease symptoms (140; 60%) and disease prevention (116; 50%). The remaining participants either never heard about the STH or did not know or provided a wrong answer. Figure 2 provides details on the frequency of the answers given by the responders regarding STH infection. For the cause of disease, the most frequent answers considered correct were “poor feeding" “dirtiness”, and “eat food in bad conditions”; while the most wrong answers provided were “Eat sweet things” and “It is something natural” (see Fig. 2A). For disease symptoms, “abdominal pain” and “vomiting” were the main correct symptoms frequently mentioned, while “swelling body and eyes”, followed by “change in skin color”, were the wrong answers most frequently reported by the study population (see Fig. 2B). With respect to knowledge about disease prevention, “practice hygiene”, “wearing shoes”, and “washing hands before eating and after toilet” were the most frequent preventive measures indicated by the study population, while “medical checkup” was the main wrong answer mentioned as a preventive measure for STH. (See Fig. 2C).

Word cloud map showing the most frequent answers given by the responders to STH infection
Attitudes of respondents toward STH infection
The results of the participants’ attitudes toward the disease are presented in Table 4. For the question of who is considered the most at-risk population to be infected with STH, 164 (70%) of the respondents indicated “anyone”, while 53 (23%) indicated “children”. The best place to seek solutions in case of STH infection, 213 (91%) of the respondents indicated hospitals, while 7 (3%) and 8 (3%) indicated pharmacy and home remedies, respectively. Among those who mentioned home remedies, a 36-year-old female participant who lived in rural areas argued, “When I am sick, I must travel to the main city, that means paying for transportation and then for consultation and medicines. Since I do not have enough money to pay for that, I prefer to take home remedies”. To determine whether pharmaceutical drugs or home remedies are the best, 173 (74%) of the respondents considered pharmaceutical drugs the best, while 16 (7%) considered both or home remedies the best. Assessing the acceptance of drug donation as a community mass drug administration, 129 (55%) respondents indicated “Yes”, while 27 (12%) indicated “No” for diverse reasons. In this regard, a 46-year-old male residing in an urban area stated, “We don´t have to take medicine without medical prescriptions”, while a 51-year-old female residing in a rural area stated, “I will not accept the donation because I’m not sick”.
Practices of respondents regarding STH infection
Table 5 presents the results from the 233 respondents’ practices regarding STH infections. Concerning the question on how often study participants wash their hands with soap; 59 (25%) stated to always do so before cooking, 70 (30%) before eating, and 70 (30%) always do so after eating. Regarding the question of how often they wash fruits and vegetables before eating them, 75 (32%) participants said always, while 11 (5%) never did so. On the practice of walking barefoot, 55 (24%) participants reported never, while 23 (10%) reported always walking barefoot. More than half of the respondents (147; 63%) never treated tap water before drinking. For open defecation, 144 (62%) respondents stated that they sometimes defecated in open places, while 21 (9%) always defecate in open places.
The practices of 166 participants aged one to nine years toward STH infection were investigated. To determine whether they washed their hands with soap before eating or after using the toilet, parents indicated never for 18 (11%) and 20 (16%) of the children, respectively, and sometimes for 131 (79%) and 121 (73%), respectively. For 111 (67%) and 44 (26%) children, parents indicated that they sometimes or always walked barefoot, respectively. For the question on open defecation, 89 (54%) and 50 (30%) parents indicated that they sometimes and never defecated in open places, respectively. To determine whether their child bites his/her nails, 71 (43%) parents indicated sometimes, while 20 (12%) indicated always. Regarding play habits, 86 (52%) and 63 (38%) parents of children indicated that their child sometimes or always played with mud, respectively.
Factors associated with STH knowledge, attitudes, and practices
As presented in Table 6, the mean score for knowledge was 1.99 (33%) out of a possible total of 6, classifying the knowledge level of the population as “bad”. According to the univariate analysis (Table 7), only education was associated with knowledge level (p = 0.04). Compared to participants with a secondary or university education, those with no formal education had a significantly lower knowledge level (β = -0.56, 95% CI: -1.00 – -0.12, p = 0.01), while no difference was observed for those with a primary school education (β = -0.32, 95% CI: -0.71 – 0.06, p = 0.10).
Regarding attitudes toward STH infections, the mean score for appropriate attitudes was 6.97 (77%) out of a possible total of 9, classifying the population-appropriate attitudes toward STH infection as “very good” (Table 6). According to the bivariate analysis (Table 7), occupation (p < 0.001) and education (p < 0.001) were significantly associated with attitudes. After adjusting for occupation and education, an association remained between appropriate attitudes and both variables. Compared to farmers/fishers, students had a lower level of appropriate attitudes (β = -1.24, 95% CI: -2.17 – -0.32, p = 0.009), while no difference was observed with the other modalities of occupation: civil servant (p = 0.86), trader (p = 0.46), and unemployed (p = 0.83). For education, a significantly lower appropriate attitude level was observed among participants with a primary education level than among those with a secondary/university education level (β = -0.68, 95% CI: -1.23—-0.13, p = 0.02), while no difference was observed among participants with no formal education (p = 0.31).
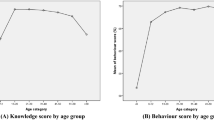
Concerning the practices of the study population toward STH infections, the mean score for appropriate practices was 7.72 (55%) out of a possible total of 14, classifying the practices level of the population as “good” (Table 6). According to the univariate analysis, as presented in Table 7, age (p = 0.006), locality (p = 0.048), occupation (p = 0.002), and education (p = 0.03) were associated with appropriate practices. After adjustment for those variables (Table 8), associations remained for age (p = 0.01), occupation (p = 0.01), and education (p = 0.02). With respect to age, the appropriate practices increase by 0.03 when age increases by one (β = 0.03, 95% CI: 0.005 – 0.05, p value = 0.01). For occupation and compared to farmer/fisherman, traders had a statistically significant lower appropriate practices level (β = 1.81, 95% CI: 0.76 – 2.87, p = 0.001), while no difference was observed for civil servants (p = 0.11), students (p = 0.69), or unemployed individuals (p = 0.50). Compared to participants with a secondary/university education, those with no formal education had a statistically significant lower level of appropriate practices (β = -1.19, 95% CI: -2.05 – -0.32, p = 0.007), while no difference was observed for participants with a primary education level (p = 0.35).
Discussion
The objective of the present survey was to assess the knowledge, attitudes, and practices of inhabitants of Bata districts toward STH infections, which could be helpful for designing health education strategies and optimizing other STH control strategies. Basically, our results indicate a poor level of knowledge but, in contrast, a very good level of appropriate attitudes and good level of appropriate practices of the Bata district population toward STH infections.
Approximately eight out of ten respondents reported having heard about intestinal worm infections, which could indicate that the population is aware of the disease. A similar high proportion of the population aware of the disease was also reported by Oyebamiji and collaborators in southwestern Nigeria with 63% of the study population having heard about intestinal worm infection [25].
In the present survey, the main source of information on STHs was at home for approximately half of the responders, assuming that information was obtained from friends and relatives via word-to-mouth. Our results are different from those reported by a study conducted in Bangladesh, where the main sources of information were schoolteachers and health workers, although in the context of the absence of a health education program [26]. Our findings could explain the poor overall knowledge of STH infections reported by our community. We can therefore assume that our results highlight a lack of health education programs at the study site and probably in the country, which is mainly needed to inform the communities about STH risk factors. Indeed, being informed on the risk factor of STH infection could help the population to apply adequate hygienic habits in order to reduce the risk of infection.
Even though the knowledge level on the causes of STH infections was particularly poor in our study population, we found a good level of knowledge on disease symptoms and prevention, probably because the population experienced these two aspects of the disease. The study site is indeed known to be highly endemic for STH infections [18]. Our results differ from those reported in Western Côte d`Ivoire, where respondents possessed good knowledge of STH causes, transmission and prevention measures but as a consequence of community-based interventions, which can explain the difference observed [27].
Respondents’ knowledge of STHs was associated with education, with participants who did not attend school having a lower knowledge level of STH infections than those who attended at least secondary education. Our results corroborate those reported by Nasr et al. [26] where education level was the most important factor associated with respondents’ knowledge. As we are not aware of health education at schools, we can assume that those with secondary or higher education received more information on proper hygiene in general and probably on general disease prevention measures or are more likely to obtain information themselves through reading for example which can therefore explain the gap in STH knowledge between them and the other population. This could thus highlight the need for the integration of schools and community-based health education strategies in our study areas for the spread of wider prevention information. Indeed, a positive impact of health education and health promotion measures on STH infections in endemic areas has been reported [28].
The study population reported an appropriate attitude toward STH infections. A similar result was reported in Thailand by Narkkul et al. [29] in 2022 but in village health volunteers, where the authors found that a good attitude was associated with training in parasitic control measures for those volunteers [29]. On the one hand, we hypothesize that the good level of appropriate attitudes in our study population is not rooted in STH infection control strategies, as such programs are not implemented in the country, but rather in the general attitude of the population toward adequate hygiene. Indeed, to assess the attitudes of our study population toward STH infections, the questionnaire administered to the responders can also be valid for other infections such as human immunodeficiency virus (HIV), tuberculosis (TB), and malaria, although it was clearly about STH infections.
We found occupation and educational level to be factors associated with respondents’ appropriate attitudes. Compared with other occupations and education levels, primary education level was found to be negatively associated with attitude level. Our result is consistent with that reported by Ba and collaborators among students in Nigeria, where respondent attitudes were more positive for students at high levels than for those at lower levels [30]. Indeed, primary school pupils, particularly school-age children, are classified by the WHO as the most at-risk population for STH infections due to less care and less proper hygiene practices, outdoor play habits, and a lack of WASH at schools and at home [11]. Although we reported a good level of attitude in our population, children and students could therefore be the weakest links for the control of STHs in the country. Regarding the population’s attitudes toward STH infection, we call for a specific emphasis on school-based health education strategies at the early school and primary school levels.
A good level of appropriate practices toward STH infections in our population were found. Indeed, we noticed that practices that favor STH transmission, such as walking barefoot, defecating in open places, and particularly for children, playing with mud, are sometimes or never practiced. Similarly, protective factors, such as washing hands with soap before eating and washing fruits and vegetables before consumption, are mostly or always practiced by the study population. As we hypothesized for the attitudes of our population toward STH infection, a good level of appropriate practices observed in the population could not be specifically rooted in STH infection prevention but rather a general way of life, suggesting that the practices of our population do not play a major role in STH transmission in the country. A recent study conducted in Bata district reported for instance that 96% of the population lacked sewage systems connected to their houses [18]. We can assume that environmental factors could mainly explain the high prevalence of STH infections observed in the country. Tropical climate, sandy soils as it is the case for Bata district, local temperatures, in addition to low proportion of sewage systems and the habit of not processing tap drinking water have been found to increase the risk of STH [22, 23, 31,32,33]. This, however, needs to be properly investigated. We found that age and education level were associated with respondents’ practices. Indeed, a positive association was observed with age and education level, indicating an increase in appropriate practices with increasing age and education level. These results are in agreement with those reported by Le and collaborators in rural areas of Indonesia, where behavior scores presented a positive association with the age and education level of respondents [28]. This result can be explained by adults being more conscious of their hygiene than children are, and people with a high education level are more likely to be in contact with hygienic information and prevention measures. These results could indicate a need to start health education early in life and at low education levels so that children can be aware of appropriate hygiene practices early in life.
Our survey was based on a structured questionnaire with close-ended questions, especially about respondents’ attitudes and practices. We did not include direct observation of the study population. Our finding may therefore be slightly out of keeping with reality. Indeed, in a KAP survey, the inclusion of observation methods is suggested to be able to capture the real reasons behind respondents’ behaviors [34, 35]. Furthermore, our study was conducted in only one out of 19 districts of the whole country, although it is the most populated district, with approximately 25% of the country population. As we must remain cautious about extrapolating our results to the whole country, we think that additional research should be conducted in other districts of the country to obtain a wider understanding of the whole country. Despite the limitations highlighted, the data on our KAP offer relevant information about our population KAP, which could be used for the orientation of control programs focused on population gap knowledge and full risk perception and practices found during the survey.
Conclusions
Despite the good level of appropriate attitudes and practices of the population toward STH we found in our community, the low knowledge level highlights the need for the implementation of integrated health education strategies at both the school and community levels, with great attention given to the early-age stage and primary school children. Such a strategy could contribute to maximizing the effects of any potential control program for STH infection implemented in the country, which is known to be highly endemic for STH infections.
Availability of data and materials
Data sets generated during the current study are available from the corresponding author on reasonable request.
Abbreviations
- CI:
-
Confidence Interval
- EG:
-
Equatorial Guinea
- HIV:
-
Human Immunodeficiency Virus
- KAP:
-
Knowledge, attitudes, and practices
- MDA:
-
Mass Drug Administration
- NTD:
-
Neglected Tropical Disease
- SI:
-
Supplementary information
- SD:
-
Standard deviation
- STH:
-
Soil-Transmitted helminth
- TB:
-
Tuberculosis
- WHO:
-
World Health Organization
- WASH:
-
Water Sanitation and Hygiene
References
Álvarez-Hernández DA, Rivero-Zambrano L, Martínez-Juárez LA, García-Rodríguez-Arana R. Overcoming the global burden of neglected tropical diseases. Ther Adv Infect Dis. 2020;7:1–3.
WHO. Soil-Transmitted Helminthiases: Eliminating soil-transmitted helminthiases as a public health problem in children. Progress report 2001−2010 and strategic plan 2011−2020. Genevea: World Health Organization - Licence: CC BY-NC-SA 3.0 IGO; 2012.
Bethony J, Brooker S, Albonico M, Geiger SM, Loukas A, Diemert D, et al. Soil-transmitted helminth infections: ascariasis, trichuriasis, and hookworm. Lancet. 2006;367:1521–32.
WHO | Regional Office for Africa. Helminthiasis. 2023. Available from: https://www.afro.who.int/health-topics/helminthiasis. Cited 18 Feb 2023.
Ozano K, Dean L, Macpherson E. Discussion paper the gender dimensions of neglected tropical diseases. UNDP-Led Access and Delivery partnership. 2019. Available from: https://adphealth.org/upload/resource/2523_ADP_Discussion_Paper_NTDs_211119_web.pdf.
World Health Organization. Helminth control in school-age children: a guide for managers of control programmes, 2nd ed. 2011; Available from: https://apps.who.int/iris/handle/10665/44671.
Pabalan N, Singian E, Tabangay L, Jarjanazi H, Boivin MJ, Ezeamama AE. Soil-transmitted helminth infection, loss of education and cognitive impairment in school-aged children: a systematic review and meta-analysis. PLoS Negl Trop Dis. 2018. https://doi.org/10.1371/journal.pntd.0005523.
Roka M, Goñi P, Rubio E, Clavel A. Intestinal parasites in HIV-seropositive patients in the continental region of Equatorial Guinea: its relation with socio-demographic, health and immune systems factors. Trans R Soc Trop Med Hyg. 2013;107:502–10.
Dejon-Agobé JC, Zinsou JF, Honkpehedji YJ, Ateba-Ngoa U, Edoa JR, Adegbite BR, et al. Schistosoma haematobium effects on plasmodium falciparum infection modified by soil-transmitted helminths in school-age children living in rural areas of Gabon. PLoS Negl Trop Dis. 2018;12:1–17.
Cadmus SI, Akinseye VO, Taiwo BO, Pinelli EO, van Soolingen D, Rhodes SG. Interactions between helminths and tuberculosis infections: implications for tuberculosis diagnosis and vaccination in Africa. PLoS Negl Trop Dis. 2020;14(6):e0008069.
Montresor A, Crompton DWT, Gyorkos TW, Savioli L, World Health Organization. Helminth control in school-age children: a guide for managers of control programmes. Geneva: World Health Organization; 2002. p. 64.
World Health Organization. Ending the neglect to attain the sustainable development goals: a sustainability framework for action against neglected tropical diseases 2021–2030. Geneva: World Health Organization; 2021. Available from: https://apps.who.int/iris/handle/10665/338886.
WHO. Fifty- fourth, Word Health Assembly. Ninth plenary meeting. 2010. Available from: https://apps.who.int/iris/bitstream/handle/10665/78794/ea54r19.pdf.
WHO. Working to overcome the global impact of neglected tropical diseases: first WHO report on neglected tropical diseases. Geneva: World Health Organization; 2010. p. 1–184
World Health Organization. Guideline: preventive chemotherapy to control soil-transmitted helminth infections in at-risk population groups. Geneva: World Health Organization; 2017. Available from: https://apps.who.int/iris/handle/10665/258983. Cited 21 Oct 2022
Nath TC, Adnan MR, Sultana N, Husna A, Ndossi BA, Kang Y, et al. Integration of health education intervention to improve the compliance to mass drug administration for soil-transmitted helminths infection in Bangladesh: an implementation research. Parasite Epidemiol Control. 2020;1(11):e00165.
Sacolo-Gwebu H, Kabuyaya M, Chimbari M. Knowledge, attitudes and practices on schistosomiasis and soil-transmitted helminths among caregivers in Ingwavuma area in uMkhanyakude district, South Africa. BMC Infect Dis. 2019;22(19):734.
Ribado-Meñe G, Dejon-Agobé JC, Momo-Besahà JC, Ondo-Ndoho Mohamed-Abdulla S, Adegnika Ayôla A. Prevalence, intensity and associated risk factors of soil-transmitted helminth infections among individuals living in Bata district, Equatorial Guinea. PLos Negl Trop Dis. 2023. https://doi.org/10.1371/journal.pntd.0011345.
Afolabi MO, Adebiyi A, Cano J, Sartorius B, Greenwood B, Johnson O, et al. Estimating the burden of malaria and soil-transmitted helminth co-infection in sub-Saharan Africa: a geospatial study. medRxiv; 2022. Available from: https://www.medrxiv.org/content/10.1101/2022.03.14.22272330v1. Cited 28 Aug 2022.
Afolabi MO, Adebiyi A, Cano J, Sartorius B, Greenwood B, Johnson O, et al. Prevalence and distribution pattern of malaria and soil-transmitted helminth co-endemicity in sub-Saharan Africa, 2000–2018: a geospatial analysis. PLoS Negl Trop Dis. 2022;16:e0010321.
Ministerio de Sanidad y Bienestar Social. Plan directeur de lutte contre les Maladies Tropicales Negligees-2018–2022. 2018. Available from: https://espen.afro.who.int/countries/equatorial-guinea.
Instituto Nacional de Estadísticas de Guinea Ecuatorial. Anuario Estadístico de Guinea Ecuatorial 2022. 2022.Available from: https://inege.org/wp-content/uploads/2023/10/Anuario-2022.pdf.
Ministerio de Sanidad y Bienestar Social y Ministerio de Economía, Planificación e Inversiones Públicas. Encuesta demográfica y de salud de Guinea Ecuatorial (EDSGE-I) 2011. Available form: https://dhsprogram.com/pubs/pdf/fr271/fr271.pdf.
Charan J, Biswas T. How to calculate sample size for different study designs in medical research? Indian J Psychol Med. 2013;1(35):121–6.
Oyebamiji DA, Ebisike AN, Egede JO, Hassan AA. Knowledge, attitude and practice with respect to soil contamination by soil-transmitted helminths in Ibadan, Southwestern Nigeria. Parasite Epidemiol Control. 2018;3:e00075.
Nath TC, Padmawati RS, Alam MS, Das S, Murhandarwati EH. Elimination of soil-transmitted helminthiasis infection in Bangladesh: Knowledge, attitudes, and practices regarding mass drug administration. J Glob Health Rep. 2018;2:e2018017.
Acka CA, Raso G, N’Goran EK, Tschannen AB, Bogoch II, Séraphin E, et al. Parasitic worms: knowledge, attitudes, and practices in Western Côte d’Ivoire with implications for integrated control. PLoS Negl Trop Dis. 2010. https://doi.org/10.1371/journal.pntd.0000910.
Lee P, Kurscheid JM, Laksono B, Park MJ, Clements ACA, Lowe C, et al. Model validation for a knowledge and practices survey towards prevention of soil-transmitted helminth infections in rural villages in Indonesia. Sci Rep. 2023;13:1444.
Narkkul U, Na-ek P, Kaewkungwal J, Punsawad C. Knowledge, attitudes, and practices regarding soil-transmitted helminthiasis among village health volunteers in Nakhon Si Thammarat Province, Thailand: a cross-sectional study. Trop Med Infect Dis. 2022;7:33.
Aina BA, Ogunbameru AV. Knowledge, attitude and practice of preventing helminth infections among students of CMUL, Idi Araba. Eur J Pub Health. 2020;30(Suppl 5):166–260.
Ncogo P, Herrador Z, Romay-Barja M, García-Carrasco E, Nseng G, Berzosa P, et al. Malaria prevalence in Bata district, Equatorial Guinea: a cross-sectional study. Malar J. 2015;14:1–10.
Montresor A, Mupfasoni D, Mikhailov A, Mwinzi P, Lucianez A, Jamsheed M, et al. The global progress of soil-transmitted helminthiases control in 2020 and World Health Organization targets for 2030. PLoS Negl Trop Dis. 2020;14:e0008505.
Mackinnon E, Ayah R, Taylor R, Owor M, Ssempebwa J, Olago lD, et al. 21st century research in urban WASH and health in sub-Saharan Africa: methods and outcomes in transition. Int J Environ Health Res. 2019;29:457–78.
Nasr NA, Al-Mekhlafi HM, Ahmed A, Roslan MA, Bulgiba A. Towards an effective control programme of soil-transmitted helminth infections among Orang Asli in rural Malaysia. Part 2: Knowledge, attitude, and practices. Parasites and Vectors. 2013. https://doi.org/10.1186/1756-3305-6-28.
Launiala A. How much can a KAP survey tell us about people’s knowledge, attitudes and practices? Some observations from medical anthropology research on malaria in pregnancy in Malawi. Anthropology Matters. 2009. Available from: https://www.anthropologymatters.com/index.php/anth_matters/article/view/31. Cited 23 Apr 2023
Acknowledgements
The authors gratefully acknowledge the delegates (Delegation of Ministry of Health and Social Welfare in Bata; Government Delegation of the Ministry of Interiors and Local Corporations in Bata – Littoral); community leaders (Bikuy II, Bomudi IV, Bomudi V, IkundeIII, Ekuku II, Adjap Cdo, Bicomo Cdo, Bindung Cdo, Esun Cdo, San Jose de Alum Cdo, Edjabe, Tika, Bongoro Cdo, Nkomakac Cdo); Technical Director of Bata Hospital, our driver and all Bata District populations who were willingly accepted to be part of these studies. We also want to thank Mrs. Heidi Rader for her support on the English revision of the present manuscript and Mr. Ynous Djida for the study map realization. AAA and JCDA are members of the CANTAM (EDCTP-RegNet2015-1045).
Funding
This study was supported by the German Federal Ministry of Economic Cooperation and Development (BMZ) through the KfW (German Development Bank) and managed in Cameroon by the “Organization de Coordination pour la lute contre les Endémies en Afrique Centrale” (OCEAC). Funding allowed for survey development and data collection in the field, not for paper publication. The funders of the study had no role in the review, decision to publish, or preparation of the manuscript.
Author information
Authors and Affiliations
Contributions
GRM: Funding acquisition, conceptualization,work design, investigation, analysis and; interpretation, writing of original draft, and writing - editing of the manuscript. JCDA: Data analysis, reviewing of results and; interpretation, writing-editing of the manuscript. BMAA: Former data analysis, reviewing of results and; interpretation, reviewing and; editing of manuscripts. MFM: Investigation, substantially reviewing, and editing of the manuscripts. JMEE: Investigation, substantially reviewing, and editing of the manuscripts. SA: Conceptualization, work design, investigation, writing of original draft, writing-reviewing & editing of the manuscript, supervision. AAA: Conceptualization, substantial writing reviewing and; editing, supervision. All the authors have read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Ethical approval was granted by the Equatorial Guinea National Ethics Committee (CENGE, Nr Reg-2019–028). Administrative authorizations were obtained from the public health Direction of the Ministry of Health and Social Welfare; Nr Reg- 56–150. The Regional Delegation of the Ministry of Health and Social Welfare in Bata (reference number: 2018) and the Government Delegation of the Ministry of Interiors and Local Corporations in Bata – Littoral (reference number 937) were also included. The study objectives and procedures were explained to the community leaders, sampled household heads, and selected participants. All adult participants provided written consent before they participated in the survey. For illiterate participants, the informed consent to participate was provided by a legal guardian or an appropriate representative and participants were asked to provide a thumb-printed. For participants younger than age of 18, informed consent to participate was obtained from parents or legal guardians, in addition to thumb-printed consent for children aged 10–17 years. Participation was completely voluntary; for confidentiality, an identification number was given to each participant encoded with a given number and participants’ initials.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
12889_2024_19528_MOESM1_ESM.docx
Supplementary Material 1: Supplementary Table S1. Respondents’ knowledge score calculation. Supplementary Table S2. The respondents’ appropriate attitudes score calculation. Supplementary Table S3. Respondents’ appropriate practices score calculation.
12889_2024_19528_MOESM3_ESM.pdf
Supplementary Material 3: Supplementary material S2. Simplify version of the study main questionnaire for children aged 10 to 17 years
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Meñe, G.R., Dejon-Agobé, J.C., Angue, B.M.A. et al. Knowledge, attitudes, and practices related to soil-transmitted helminth infections among residents of Bata district, Equatorial Guinea; a cross-sectional study. BMC Public Health 24, 1962 (2024). https://doi.org/10.1186/s12889-024-19528-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12889-024-19528-0