
Abstract
Background
Does preschool height predict adult stature in undernourished settings? The extent to which preschool length or height forecasts young adult stature is unclear in chronically undernourished populations.
Methods
In 2006-8, we assessed height in a cohort of 2074 young adults, aged 16–23 years, in rural Nepal who, as preschoolers (≤ 4 year), were measured at baseline and again 16 months later during a vitamin A supplementation trial in 1989-91. We assessed by linear regression the ability of preschool length (L, measured < 24 mo) or height (Ht, 24–59 mo), at each year of age to predict 16–23 year old height, adjusted for month of young adult age, interval duration (in months), caste, preschool weight-for-height z-score and, in young women, time since menarche, marriage status and pregnancy history.
Results
Young women were a mean of 0.81, 1.11, 0.82, 0.24, 0.44 cm taller (all p < 0.01) and young men, 0.84, 1.18, 0.74, 0.64 and 0.48 cm taller (all p < 0.001) per cm of attained L/Ht at each successive preschool year of age and, overall, were 2.04 and 2.40 cm taller for each unit increase in preschool L/Ht z-score (L/HAZ) (both p < 0.001). Coefficients were generally larger for 16-month follow-up measurements. The percent of young adult height attained by children with normal L/HAZ (>-1) increased from 38–40% mid-infancy to ∼ 69–74% by 6 years of age. By 3–6 years of age heights of stunted children (L/HAZ<-2) were consistently ∼ 4–7% lower in their young adult height versus normal statured children. There was no effect of preschool vitamin A receipt.
Conclusions
Shorter young children become shorter adults but predictive effects can vary by sex, age assessed, and may be influenced by year or season of measurement.
Similar content being viewed by others

Background
Adult height represents accumulated linear growth from fetal life through infancy, childhood and adolescence [1,2,3]. Although velocities uniformly decrease with age until pubescence, within supportive environs of routine dietary adequacy and generally good health, children are expected to reach around 70% of their final height by age 7 and about 80% by age 10 years [4]. Approximately 15% of adult height is attained during adolescence, most of which occurs during puberty (ages 10 to ∼ 14 years) [5,6,7,8]. For example, in British and Denmark cohort studies, adult height was strongly predicted from child height at age 7 for both sexes, [1, 4] emphasizing the importance of adequate linear growth in childhood toward establishing final adult height.
In less supportive environs, where early childhood nutritional status is often characterized in terms of wasting and stunting, it is of interest to quantify, if possible, the extent to which attained preschool growth anticipates adult stature. In an early 21st century longitudinal study in India, the association between preschool height and adult height strengthened with increasing age, reaching a correlation coefficient of 0.7 by age five and continued increasing after puberty [9]. Expressing achieved linear growth as length for age z-scores (LAZ), the Cohorts Study, which has followed growth of 4659 children from infancy into adulthood in Brazil, Guatemala, India, the Philippines, and South Africa, has reported a mean increment of 0.45 height-for-age z-score (HAZ) at ages 15 to 32 years per z-score increment at 12 months of age [10]. In Pelotas, Brazil Cohorts Study investigators reported that heights of young women were, on average, 0.8 cm taller at 19 years per cm of attained height at four years of age [11]. Panels of synthetic cohorts have been created in 21 low-middle income countries (LMICs) by matching distributions of preschool child and adult height aligned by chronological years of birth from repeated Demographic and Health Surveys (DHS) conducted over a period of three decades. Based on these aligned cross-sectional datasets, Karra and Fink have estimated that each unit increase in HAZ under 5 years of age is associated with an estimated increase in adult height of 2.92 cm and 1.88 cm in men and women, respectively [12].
In this paper, we contribute predictive relationships between preschool length (< 24 months) and height (24–59 months) and late adolescent/young adultFootnote 1 height in a population-based cohort of individuals who, as preschoolers, participated in a vitamin A supplementation trial from 1989 to 1991. Study participants lived in the rural District of Sarlahi, lying along the southern plains (Terai) of Nepal [13], a setting where moderate undernutrition remains a chronic public health concern [14]. We report estimates adjusted only for study design factors and, in addition, adjusted for nutritional and socioeconomic status and, for young women, age at menarche, marital status and pregnancy history (that may affect adolescent growth), and to a limited extent season and year of measurement. The influence of cluster-randomized supplement allocation during the original placebo-controlled vitamin A trial was also examined.
Methods
This secondary data analysis was based on longitudinal records of a subset 2074 children, within a growth sub-study cohort of 4765 children ≤ 60 months of age, who were enrolled from September to December 1989 into a large cluster-randomized, placebo-controlled vitamin A supplementation trial (total n = 28,630) that involved home visits with supplement provision every 4 months [13]. The trial was stopped following completion of a 16-month assessment (in January-April 1991) due to an observed 30% reduction in child mortality. The entire trial cohort was revisited to receive a vital, health and nutritional assessment ∼ 16 years later. This analysis was restricted to children who were assessed at either the trial’s baseline or 16-month visit, and had complete data at young adult follow-up.
Original trial
The design of the original trial and its findings on the efficacy of vitamin A supplementation in reducing child mortality and xerophthalmia and improving growth have been previously reported [13, 15,16,17,18]. Among 261 subdistrict wards (clusters) that were mapped, addressed and randomized for the trial, 40 were randomly sampled, stratified by allocation and geographic area, for all resident, enrolled children at baseline to receive an ocular exam and be measured for anthropometry. At both baseline (Sep – Dec 1989, pre-harvest) and 16-month visits (Jan – Apr 1991, post-harvest), children were weighed either naked or lightly clothed on hanging Salter spring scales (West Bromwich, England), with values recorded to the nearest 0.1 kg after the pointer was stable for ≥ 2 s. Recumbent length (L, for children aged < 24 months) and standing height (Ht, for children ≥ 24 months) were measured and recorded independently 3 times to the nearest 0.1 cm on wooden boards with footplate, sliding head block and attached steel tape to the nearest 0.1 cm (Weigh and Measure LLC, Olney, MD, USA), with the median taken as actual. Height-for-age (HAZ) or length-for-age (LAZ), weight-for-height (WHZ) and weight-for-age (WAZ) z-scores were derived from the WHO reference population [19]. Mid-upper arm circumference and tricipital and subscapular skinfold measurements and 1-week morbidity histories were also measured at each visit. Household socioeconomic characteristics, including caste membership (Brahmin, Chhetri, Vaishya, Shudra, and non-Hindu), were assessed shortly after the baseline visit. The trial was approved by the Nepal Medical Research Council (Kathmandu, Nepal) and the Johns Hopkins Joint Committee on Clinical Investigation (Baltimore, MD, USA).
Follow-up study
Households of children who completed the 1989-91 trial were initially revisited by field teams in 2006-8 to record vital status, confirm identity and residency, obtain informed consent for a follow-up assessment, and be scheduled for a home-based assessment. Children in households that had permanently moved from the district were followed for vital status, if possible, but excluded from assessment protocols.
Cohort follow-up procedures and findings related to multiple health outcomes have been reported [20,21,22,23]. Briefly, data were collected on household socioeconomic variables, adolescent/young adult participant health and marital status, and for females, recalled age (in years) at menarche, marriage status and if married, pregnancy history. Anthropometry was conducted by trained, original trial field staff who measured participant height with shoes removed on a locally constructed stadiometer, recorded the median of 3 measurements to the nearest 0.1 cm, and weight without shoes and light clothing recorded from a Seca digital scale (Seca, Chino, CA, USA) to the nearest 0.1 kg. Body mass index (BMI) was calculated as weight in kg/height in m². Caste was assumed to be unchanged from the original trial. As month and year of birth had been recorded with assistance of event calendars during the trial, ages were considered accurately known, ranging from 16 to 23 years, converted to age in months which was used to further refine age-adjusted size measures. All follow-up assessments by staff were conducted blinded to supplement allocation, and preschool nutritional, health and household socioeconomic status data from the original trial. The follow-up study was approved by the Nepal Health Research Council (Kathmandu, Nepal) and the Institutional Review Board at Johns Hopkins Bloomberg School of Public Health (Baltimore, MD, USA).
Statistical analysis
Anthropometric data at baseline (Sept-Dec 1989), derived from preschoolers in a highly compliant, random selection of wards throughout the rural study area of ∼ 250 sq km, when paired to 2006-8 follow-up data, was considered the primary dataset for assessing preschool child growth: follow-up statural associations. Sixteen-month follow-up data collected from Jan-April 1991 in the same cohort of children provided further opportunity to examine the same relationships involving a different season and year of initial assessment. Age-sex specific anthropometric z-scores for length-for-age (LAZ), height-for-age (HAZ), weight-for-height (WHZ) and weight-for-age (WAZ) were derived from the WHO Multicenter Growth Reference Study [19].
Sex-specific, linear regression models for each preschool year of age were employed to quantify the associated effect size of preschool length or height on young adult height. As the 2006-8 follow-up study was conducted over a period of ∼ 1.5 years, without attempting to match visits to month or sequence of preschool assessment, all models are adjusted for late adolescent/young adult age in months to account for this source of variation in age.
For the baseline-derived analysis, children at exactly 60 months of age (n = 26) were dropped to remain consistent with ages being < 5 years. An initial linear regression (Model 1) was introduced to adjust for late adolescent/young adult age and interval duration between preschool assessment and the 2006-8 follow-up. Multivariable regression analysis (Model 2) further included preschool WHZ and caste as covariates, and for females, marriage status, pregnancy history and time since menarche. Preschool WHZ has been included to adjust coefficients for initial wasting status and as a proxy for other associated anthropometric measures (i.e. mid-upper arm circumference and skinfolds). Caste, acting as a strong indicator of socio-economic status, has been added as a covariate to broadly adjust for social, economic, local environmental risk factors [24,25,26,27]. As age at marriage and pregnancy may be associated with sexual maturation, age at menarche [28], growth and development [29, 30], and as pregnancy can have a suppressing effect on late adolescent growth [31], these factors have also been included in the models. As history of menarche was obtained by year of age, and as age of menarche follows a sigmoidal curve [32], we assigned mid-year ages for girls who reported menarche at 14 (i.e., 174 mo) and 13 (162 mo) years, progressively shifting the assigned age to older months for girls reporting menarche at 12, 11 and 10 years, and toward younger months for girls reporting menarche at ages 15, 16 and older years. To aggregate effect sizes across all preschool ages, we repeated analyses replacing preschool L or Ht measurements in cm with L/HAZ as the independent variable, accounting for age.
Identical growth interval analyses were carried out using measurements taken at the 16-month trial visit, which encompassed the winter post-harvest season of 1991, in contrast to the initial assessments taken during the post-monsoon, preharvest season of 1989. Using this interval also excluded infancy with aging of the cohort and generated estimates for each 1-year stratum from 1 to 6 years of age. Children with complete data at 16-month visit and follow-up during late adolescence to young adulthood were included in this second evaluation. Since 16-month follow-up is closer by this amount of time to the young adult measurement, an interval duration covariate was further introduced to both Model 1 and Model 2 to account for this potential source of variation due to design. The potential influence of vitamin A vs. placebo supplementation during the original trial was examined by including ward allocation as a covariate in preschool-to-late adolescent/young adult height models.
We further estimate the percentage of young adult height attained at each years of age at the baseline and 16-month visit, stratified by sex and L/HAZ [i.e., > -1 z (normal length or height), -2 to -1 z (mildly stunted) and < -2 z (moderately to severely stunted)] to maximize use of available age-specific data and enable comparison with data from better nourished societies.
Complete data during the original trial baseline or 16-month visit, and at the young adult follow-up were required for inclusion in this analysis. Given this requirement, we examined the potential for bias by comparing preschool household socioeconomic variables assessed during the original trial between participants included in this analysis and those excluded due to incomplete data or reportedly being alive but unreachable at follow-up. Significance of distributional differences was compared by the Chi-squared test. Household characteristics of children who had died between the end of trial and time of young adult follow-up are also presented.
All analyses were conducted using Stata, version 17.0, software.
Results
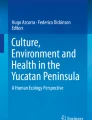
Initially, 4765 children aged 0–60 months were included into this analytical substudy, of whom 4651 were alive at the end of the original trial, among whom 442 were missing anthropometry at baseline and excluded. By the time of either the census or follow-up assessment ∼ 16 years later, an additional 155 children had been identified as deceased and 1138 had moved or refused and were considered lost. At follow-up, 816 were reported to be resident but not measured after ≥ 2 repeat visits, leaving 2100, or 50% of 4214 surviving and measured children who exited the original trial (Fig. 1). Sex was available for 858 girls and 1216 boys, representing the number of participants in this analysis. With respect to assessed household socio-economic characteristics at the time of the original survey, surviving individuals included and excluded from the analytical cohort were comparable (Table 1), providing no evidence of selection bias based on factors in early childhood.

Flowchart of Participants as Preschoolers (< 60 months) at Baseline (in 1989), and as Censused (in 2006) and Followed-up as Late Adolescents and Young Adults (in 2006–2008), Nepal Nutrition Intervention Project-Sarlahi, Nepal
Table 2 summarizes preschool and young adult growth characteristics of the cohort. At baseline preschool heights increased with age, with boys being a mean of 1.1 to 2.8 cm taller than girls in each age group. Among young adult females stratified by their preschool ages during the trial, mean heights are consistently at ∼ 151 cm, while males within the same original strata were, on average, 11–12 cm taller.
Young adult height was positively associated with preschool length/height. In linear regression, Model 1, which adjusts for the preschool-to-adult time interval and young adult age, the beta-coefficient (b) revealed a height at 16 to 23 years that was 0.86 –0.84 cm and 1.09–1.19 cm higher per cm of attained length during infancy and 2nd year of life, respectively, and a b = 0.84 and 0.75 cm at age 2 yrs, for females and males, respectively. A strong association generally remained at 3 and 4 years of age for boys (Δ = 0.68 and 0.50 cm), but was weaker for girls (Δ = 0.33 and 0.29 cm, respectively). In Model 2 (Table 2), increments were further adjusted for potential effects of several variables summarized in Supplemental Table 1 (See Supplemental Table 1, Additional File 1), including preschool WHZ and household caste, for young women, marital status, time since menarche and pregnancy history. None of these adjustments, however, notably changed slope coefficients of young adult height on preschool length or height from Model 1 for either sex, suggesting a lack of confounding among model covariates.
Applying the same analyses with data from 16-month visits instead of baseline, 1999 children (See Supplemental Fig. 1, Additional File 1) were stratified by the cohort’s 16-month end-of-trial ages of 1, 2, 3, 4, 5, and 6 years. Qualitatively similar but stronger associations were observed, reflected by Model 2 regression beta-coefficients of 1.06, 1.00, 1.16, 0.49, 0.50, and 0.46 cm/cm among young women (all p < 0.001), and 1.06, 1.09, 0.89, 0.74, 0.66, and 0.61 cm/cm among young men (all p < 0.001), respectively (See Supplemental Table 2, Additional File 1). None of the above same covariates added into Model 2 notably changed the results.
Expressing attained preschool L/Ht as height-for-age z-scores (L/HAZ), Table 3 allowed a sex specific effect size to be estimated for all ages combined, adjusted for the same covariates in Models 1 and 2. For each unit increase in LAZ or HAZ, females and males were an additional 2.04 and 2.40 cm taller at 16–23 years of age. The effect size was stronger for the 16-month follow-up than baseline assessment, revealing young adult height increments of 2.95 and 3.39 cm per L/HAZ score for females and males, respectively (See Supplemental Table 3, Additional File 1). Modeled young adult height distributions by caste, marriage, and pregnancy factors are summarized in Supplemental Table 4.
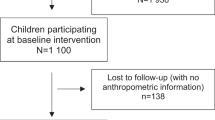
Figure 2 and Supplemental Fig. 2 present the percentage of height at 16–23 years of age that was attained at each early childhood year of age, stratified by L/HAZ and sex. Children (female|male) of normal height (L/HAZ>-1) achieved 39|38, 50|47, 55|53, 63|59, and 67|62 percents of their young adult height at each year of age from infancy (0) through 4 yrs of age (See Supplemental Table 5, Additional File 1). Data from 16-month visit complement height attained by children aged 5 and 6 yrs, at which girls with normal height gained 72% and 74%, and boys, 66% and 69% of their young adult height, respectively. For both sexes by ages 3–6 years, children in the mid-range of L/HAZ (-1 to -2 Z) had attained ∼ 1–3% less, and stunted children (L/HAZ <-2) ∼ 4–7% less of their young adult height than children of normal height.

Percent of Height at 16–23 Years of Age Attained by Year of Early Childhood Age at Baseline, by Sex and Preschool Length/Height for Age Z-score in a Population Cohort in the Terai of Nepal
There was no cohort effect due to vitamin A versus placebo supplement receipt during the original trial.
Discussion
In this chronically undernourished rural South Asian setting, height attained by late adolescence through young adulthood was positively associated with preschool length below two years or height at older ages, with regression coefficients derived from baseline measurements of the original trial ranging from 0.24 to 1.11 and 0.48 to 1.18 cm increases in young adult height per preschool cm in girls and boys, respectively. Effect sizes, determined from measurements taken 16 months later in the same cohort but in a different season (winter, post-harvest vs. post-monsoon, pre-harvest) of the following year, were comparable, ranging from 0.46 to 1.16 and 0.61 to 1.09 cm in young adult height per cm, respectfully. Linear growth appeared to most efficiently translate to young adulthood height in the 1st three years of life, during which most coefficients exceeded 1 cm of young adult height per cm of length or height. Coefficients derived from ages four to six years were generally lower, 0.44 to 0.50 and 0.48 to 0.74 cm per cm in girls and boys, respectively (Table 2 & Supplemental Table 2).
We also examined associations of early childhood length or height for age z-scores for each sex, allowing all early child ages to be combined, finding late adolescent and young adult stature to increase by 2.04 and 2.40 cm per standardized normal deviate in length or height for age in girls and boys, respectively. Caste, as a strong proxy for socioeconomic status [24,25,26,27], preschool weight for height z-score, time since menarche, after which growth slows in girls [28], marriage status, the age at which can be influenced by maturation and growth of girls [29, 30], and history of pregnancy which may slow maternal growth [31], exerted no influence on this relationship.
Our longitudinal cohort findings support those from a synthetic panel cohort study derived from 21 cross-sectional Demographic Health Surveys in low- and middle-income countries [12]. This study found that among children under five years, there was an estimated increase of 2.01 cm (2.92 cm and 1.88 cm for male and female, respectively) in adult height for each additional z-score increase in preschool height-for-age. Given that the average adult male and female height was approximately 164 cm and 151 cm in our study, the increments per HAZ represented 1.8% and 1.2% of final adult height. The synthetic cohorts for each country were assumed to have maintained residence in their same locales without loss to follow-up. Similarly, our study tracked the same children over time, excluding children who migrated out of the study area or had incomplete data.
In a third descriptive approach we took, we revealed that about 40% of late adolescent/young adult height was achieved, on average, by mid-infancy, and that by mid-year in their 2nd year of life, children had gained almost half of their young adult height. This display revealed that girls and boys, whose heights were in a normal range (L/HAZ > -1) at six years of age had reached 74% and 69%, respectively, of their young adult height, while children who were stunted at six-years of age (L/HAZ < -2) had achieved less, 68% and 64%, respectively, of their young adult height. Interestingly, this latter finding raises a hypothesis that children who were stunted at six years may have accelerated their school-aged linear growth, relative to children of normal height, to reach their final young adult height. Our findings in children with normal height at six years are similar to a previous report in Denmark where, by age 7 years, girls and boys had reached 73% and 69%, respectively, of their adult height [4]. This comparison suggests that relative attainment of adult height by school entrant age is comparable among normally growing children across different habitats, and that distributions of young adult height may be approximated by age six years.
In the present study, while ranges of age-specific regression coefficients were comparable, more coefficients reflecting young adult height as a function of preschool length or height were larger based on measurements in the same age strata taken sixteen months later. Adjusting for the shorter early childhood to young adult interval length did not affect this observation, suggesting possible unmeasured influences that vary by season or year. The later early childhood measurements were taken in January-April 1991, covering the dry, cool post-rice harvest winter months when vegetables are also more available compared to the timing of the initial measurements, taken from September through December 1989, representing a post-monsoon, pre-harvest, and generally “lean” period of the year (Table 2 and Supplemental Table 2).
Children who had died during the ∼ 16 year interval from end of trial to young adulthood were from poorer families (Table 1). Otherwise, potential biases of excluding children with incomplete data, including young adults known to have been alive but unreachable for measurement, appear to have be minimal based on comparability of baseline factors assessed during the original trial.
Conclusion
Our findings add evidence to the literature that attained early childhood stature can be informative in predicting young adult height in a rural, chronically undernourished setting in South Asia. Associations revealed were robust to adjustments for other factors that were themselves variably associated with adult height, such as preschool wasting, socioeconomic status and, in girls, timing of menarche and pregnancy history. In such settings, preschooler anthropometric surveys reveal not only current nutritional status but offer predictive information about young adult size.
Data availability
No datasets were generated or analysed during the current study.
Notes
Late adolescent (16–18 years) and young adult (19–23 years) participants are referred to as “young adults” in this paper.
Abbreviations
- L:
-
Recumbent length
- Ht:
-
Standing height
- HAZ:
-
Height-for-age z-score
- LAZ:
-
Length-for-age z-score
- WHZ:
-
Weight-for-height z-score
- WAZ:
-
Weight-for-age z-score
References
Tanner JM. Growth and maturation during adolescence. Nutr Rev. 1981;39(2):43–55. https://doi.org/10.1111/j.1753-4887.1981.tb06734.x.
Tanner JM. A history of the study of human growth. Cambridge University Press; 1981.
Bogin B. Patterns of human growth. 3rd ed. Cambridge: Cambridge University Press; 2020. https://doi.org/10.1017/9781108379977.
Pedersen DC, Meyle KD, Ängquist L, et al. Changes and correlations in height from 7 to 69 years of age across the birth years of 1930 to 1989. Am J Hum Biol. 2020;32(4):e23378. https://doi.org/10.1002/ajhb.23378.
Christian P, Smith ER. Adolescent undernutrition: global burden, physiology, and nutritional risks. Ann Nutr Metab. 2018;72(4):316–28. https://doi.org/10.1159/000488865.
Spear BA. Adolescent growth and development. J Am Diet Assoc. 2002;102(3 Suppl):S23–9. https://doi.org/10.1016/s0002-8223(02)90418-9.
Talwar I, Sharma K, Kapur S. Growth trends in body, fat, circumferential and physiological traits during adolescence among Rajput females of Theog, Shimla District (Himachal Pradesh), India. Ann Hum Biol. 2010;37(4):536–53. https://doi.org/10.3109/03014460903448040.
Adams AM, Khan A, Roy AS, et al. Growth dynamics among adolescent girls in Bangladesh: evidence from nationally representative data spanning 2011–2014. PLoS ONE. 2021;16(7):e0255273. https://doi.org/10.1371/journal.pone.0255273. Published 2021 Jul 29.
Sachdev HS, Fall CH, Osmond C, et al. Anthropometric indicators of body composition in young adults: relation to size at birth and serial measurements of body mass index in childhood in the New Delhi birth cohort. Am J Clin Nutr. 2005;82(2):456–66. https://doi.org/10.1093/ajcn.82.2.456.
Stein AD, Wang M, Martorell R, et al. Growth patterns in early childhood and final attained stature: data from five birth cohorts from low- and middle-income countries. Am J Hum Biol. 2010;22(3):353–9. https://doi.org/10.1002/ajhb.20998.
Gigante DP, Horta BL, Lima RC, Barros FC, Victora CG. Early life factors are determinants of female height at age 19 years in a population-based birth cohort (Pelotas, Brazil). J Nutr. 2006;136(2):473–8. https://doi.org/10.1093/jn/136.2.473.
Karra M, Fink G. Long run height and education implications of early life growth faltering: a synthetic panel analysis of 425 birth cohorts in 21 low- and middle-income countries. BMC Public Health. 2019;19(1):876. https://doi.org/10.1186/s12889-019-7203-5. Published 2019 Jul 4.
West KP Jr, Pokhrel RP, Katz J, et al. Efficacy of vitamin A in reducing preschool child mortality in Nepal. Lancet. 1991;338(8759):67–71. https://doi.org/10.1016/0140-6736(91)90070-6.
Angela KC, Thorne-Lyman AL, Manohar S, et al. Preschool Child Nutritional Status in Nepal in 2016: a National Profile and 40-Year comparative Trend. Food Nutr Bull. 2020;41(2):152–66. https://doi.org/10.1177/0379572120916343.
West KP, LeClerq SC, Shrestha SR, et al. Effects of vitamin A on growth of vitamin A-deficient children: field studies in Nepal. J Nutr. 1997;127(10):1957–65. https://doi.org/10.1093/jn/127.10.1957.
Pradhan EK, Katz J, LeClerq SC, West KP Jr. Data management for large community trials in Nepal. Control Clin Trials. 1994;15(3):220–34. https://doi.org/10.1016/0197-2456(94)90059-0.
Khatry SK, West KP Jr, Katz J, et al. Epidemiology of xerophthalmia in Nepal. A pattern of household poverty, childhood illness, and mortality. The Sarlahi Study Group. Arch Ophthalmol. 1995;113(4):425–9. https://doi.org/10.1001/archopht.1995.01100040039024.
Katz J, West KP Jr, Khatry SK, et al. Impact of vitamin A supplementation on prevalence and incidence of xerophthalmia in Nepal. Invest Ophthalmol Vis Sci. 1995;36(13):2577–83.
de Onis M, World Health Organization. Dept. of Nutrition for Health, Development. WHO child growth standards. Geneva: World Health Organization; 2006.
Schmitz J, Pillion JP, LeClerq SC, et al. Prevalence of hearing loss and ear morbidity among adolescents and young adults in rural southern Nepal. Int J Audiol. 2010;49(5):388–94. https://doi.org/10.3109/14992020903555708.
Schmitz J, West KP Jr, Khatry SK, et al. Vitamin a supplementation in preschool children and risk of hearing loss as adolescents and young adults in rural Nepal: randomised trial cohort follow-up study. BMJ. 2012;344:d7962. https://doi.org/10.1136/bmj.d7962. Published 2012 Jan 10.
Stewart CP, Christian P, Wu LS, LeClerq SC, Khatry SK, West KP Jr. Prevalence and risk factors of elevated blood pressure, overweight, and dyslipidemia in adolescent and young adults in rural Nepal. Metab Syndr Relat Disord. 2013;11(5):319–28. https://doi.org/10.1089/met.2013.0016.
Emmett SD, Schmitz J, Pillion J, et al. Hearing loss is associated with decreased nonverbal intelligence in rural Nepal. Otol Neurotol. 2015;36(1):86–92. https://doi.org/10.1097/MAO.0000000000000619.
Duc LT. Household wealth and gender gap widening in height: evidence from adolescents in Ethiopia, India, Peru, and Vietnam. Econ Hum Biol. 2019;34:208–15. https://doi.org/10.1016/j.ehb.2019.05.008.
Subramanian SV, Özaltin E, Finlay JE. Height of nations: a socioeconomic analysis of cohort differences and patterns among women in 54 low- to middle-income countries. PLoS ONE. 2011;6(4):e18962. https://doi.org/10.1371/journal.pone.0018962. Published 2011 Apr 20.
Silventoinen K. Determinants of variation in adult body height. J Biosoc Sci. 2003;35(2):263–85. https://doi.org/10.1017/s0021932003002633.
Bishai D, Samir Kumar KC, Waters H, et al. The impact of vitamin A supplementation on mortality inequalities among children in Nepal. Health Policy Plann. 2005;20(1):60–6. https://doi.org/10.1093/heapol/czi007.
Riley AP, Huffman SL, Chowdhury AK. Age at menarche and postmenarcheal growth in rural Bangladeshi females. Ann Hum Biol. 1989;16(4):347–59. https://doi.org/10.1080/03014468900000472.
Riley AP. Determinants of adolescent fertility and its consequences for maternal health, with special reference to rural Bangladesh. Ann N Y Acad Sci. 1994;709:86–100. https://doi.org/10.1111/j.1749-6632.1994.tb30390.x.
Rah JH, Shamim AA, Arju UT, Labrique AB, Rashid M, Christian P. Age of onset, nutritional determinants, and seasonal variations in menarche in rural Bangladesh. J Health Popul Nutr. 2009;27(6):802–7. https://doi.org/10.3329/jhpn.v27i6.4332.
Rah JH, Christian P, Shamim AA, Arju UT, Labrique AB, Rashid M. Pregnancy and lactation hinder growth and nutritional status of adolescent girls in rural Bangladesh. J Nutr. 2008;138(8):1505–11. https://doi.org/10.1093/jn/138.8.1505.
Hur J, Schulze KJ, Thorne-Lyman AL, et al. Characterization of pubertal development of girls in rural Bangladesh. PLoS ONE. 2021;16(4). https://doi.org/10.1371/journal.pone.0247762.
Acknowledgements
Authors wish to acknowledge contributions of Noornath Acharya (deceased), Dev Narayan Mandal, Luke Mullany, Kerry Schulze, Tirta Raj Shakiya, Shadara Ram Shrestha (deceased), James Tielsch and the field research, data management and logistics teams of the Nepal Nutrition Intervention Project – Sarlahi (NNIPS), the Sushil Kedia Seva Mandir, Hariaun, Nepal and the Nepal Netra Jyoti Sangh (NNJS) in Tripureswar, Kathmandu for providing a base of operations for the NNIPS Project for over three decades.
Funding
Funding for the trial was provided under Cooperative Agreement DAN 0045-A-5094 between the Office of Nutrition, US Agency for International Development, Washington DC and the Center for Human Nutrition, Department of International Health, Johns Hopkins Bloomberg School of Public Health, Baltimore MD, USA. The follow up study was supported through grant GH614 between the Bill & Melinda Gates Foundation and Center for Human Nutrition at Johns Hopkins Bloomberg School of Public Health. Support for JC was provided through the George G. Graham Professorship Endowment, Department of International Health, Johns Hopkins Bloomberg School of Public Health, Baltimore, MD, USA.
Author information
Authors and Affiliations
Contributions
JC analyzed all data and wrote the paper; RKA was co-investigator for the trial and follow-up study and approved the paper; LS-FW curated and guided analysis of data for both studies and guided data analysis; SKK directed field research for both studies and approved the paper; PC was co-investigator of the follow-up study and edited the paper; SCL co-directed field work for both studies and approved the paper; JK was co-investigator for both studies and edited the paper; KWJr was PI of both studies, conceived the question and edited the paper.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The original trial was approved by the Nepal Medical Research Council (Kathmandu, Nepal) and the Johns Hopkins Joint Committee on Clinical Investigation (Baltimore, MD, USA). The follow-up study was approved by the Nepal Health Research Council (Kathmandu, Nepal) and the Institutional Review Board at Johns Hopkins Bloomberg School of Public Health (Baltimore, MD, USA). During the original trial from 1989 to 91 parental/guardian verbal informed consent was obtained, with language separately reviewed and approved by the Nepal Medical Research Council in Kathmandu, Nepal and the Joint Committee on Clinical Investigation at the Johns Hopkins School of Medicine in Baltimore, MD, USA. At the time of the 2006-8 follow up study, verbal informed consent was obtained for interviews and physical measurements and tests from parents of unmarried teenagers < 18 years, from whom assent was also obtained. If the adolescent < 18 years of age was married and living with spouse, we were approved to consider the participants “emancipated minors” and obtained informed consent directly from them, as obtained also for all participants 18 years and older. All consent and assent procedures were independently reviewed and approved by the Nepal Health Research Council in Kathmandu, Nepal and the Johns Hopkins Bloomberg School of Public Health Institutional Review Board (IRB) in Baltimore, MD, USA
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Chen, J., Adhikari, R.K., Wu, L.SF. et al. Early childhood height is a determinant of young adult stature in rural Nepal. BMC Public Health 24, 2046 (2024). https://doi.org/10.1186/s12889-024-19469-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12889-024-19469-8