
Abstract
Background
Family socioeconomic indicators (education, occupation, and household income) are key determinants influencing children’s physical activity (PA). This study aims to systematically review the current research about the association between family socioeconomic indicators and PA among primary school-aged children and to quantify the distribution of reported associations by childs’ and parents’ sex and according to analysis and assessment methods.
Methods
A systematic literature research in multiple scientific databases (MEDLINE via PubMed, Web of Science, ScienceDirect, SPORTDiscus and ERIC) was performed for literature published between 1st January 2010 and 31st March 2022. Only studies reporting statistical associations between an SES indicator of at least one parent (education, occupation, income, or an SES index) and different types and intensities of PA in primary school-aged children (6 to 12 years) were included in the analysis. The distributions of the reported associations were evaluated across and differentiated by sub-group analysis of assessment methods (objectively measured vs. self-reported PA) and analysis methods (univariate vs. multivariate models).
Results
Overall, 93 studies reported in 77 publications were included in this review. Most of the studies were conducted in Europe and used self-reports (questionnaires) to assess PA. Most studies used only a single SES indicator (commonly maternal education), and only two studies calculated an SES index. The majority of the studies focused on moderate-to-vigorous physical activity (MVPA), total physical activity (TPA), and organized physical activity (OPA). Results showed predominantly positive associations between SES indicators and OPA. In contrast, results regarding different intensities of daily PA (TPA, LPA, MPA, MVPA, VPA, LTPA) were heterogeneous, with overwhelmingly no associations.
Conclusion
Overall, the results expand the knowledge about the association between family socioeconomic indicators and children’s PA and disprove the hypothesis of a clear positive association. However, large multicenter studies are lacking using a real SES index as a predictor and analyzing gender-specific multivariate models.
Similar content being viewed by others
Background
There is a large body of evidence demonstrating the relevance of sufficient physical activity (PA) participation for children’s health and development [1,2,3,4]. Despite this knowledge, most children worldwide are insufficiently active [5, 6]. Due to the COVID-19 pandemic and concomitant restrictions on out-of-home activities, this problem has reached a new level [7, 8]. Recent findings show that more than 80% of children and adolescents do not reach the recommendation of 60 min of moderate-to-vigorous PA (MVPA) per day [9] and this trend is increasing [10].
Factors influencing PA are diverse and complex. Among others, key determinants influencing PA relate to socioeconomic factors, especially socioeconomic status (SES) [11], usually consisting of education, occupation and (equivalent household) income of parents [12]. This does not only affect short-term health outcomes of children but also lifetime health behavior, including PA participation during adulthood [13,14,15], which in turn impacts public health in general.
The influence of socioeconomic factors on PA has been investigated in previous systematic reviews for adulthood [16] and for preschool and adolescent age ranges [17]. While results are partially inconsistent, they indicate positive associations for leisure-time PA and a predominantly negative for occupational PA in adults, but no significant associations were identified for children and adolescents. However, there is a lack of systematic evidence syntheses for primary school-aged children (6–12 years). One review examined the relationship between PA and socioeconomic factors during elementary school [18]. However, “payment of fees” (fees parents paid so the child could be active) used as a socioeconomic determinant is only a proxy of socioeconomic status and may not cover non-organized and incidental aspects of PA.
Elementary school age is a sensitive period in terms of PA behavior. With the transition from kindergarten (long periods of free play and time to move) to elementary school (mostly sedentary periods), daily PA decreases significantly [19, 20]. Moreover, the period of youth represents a significant stage of socialization, influencing subsequent behaviors throughout the lifespan, including the formation of a lifelong sufficient PA behavior [21, 22] which is, among other health behaviors, crucial for health outcomes in adulthood [23].
Heterogeneity exists regarding the methodology of available reviews on the associations between PA and socioeconomic status. Often, only one socioeconomic factor is used for analysis (e.g., education). In addition, the PA assessment method has not found sufficient consideration so far. PA assessment in younger age groups (up to 10 years) is not only done mainly by self-report; it also is measured by proxy reports using one or both parents rather than the child itself. This carries the risk of over- or underestimation, aside from other measurement biases such as deliberate changes (e.g., social desirability), item misunderstanding, and misinterpretation [24,25,26].
In comparison, objective measurement tools (e.g., accelerometer, pedometer) directly collect data from the child and are therefore more precise regarding PA frequency, duration, and intensity. Objective PA assessment, however, has several limitations; specific activities, such as swimming, sliding, or cycling) cannot be recorded or only to a limited extent due to technical limitations [27]. In addition, the measured period is usually brief (e.g., one week) and therefore provides less information about habits and regularity of PA, which is of importance concerning seasonal and weather biases [28]. Due to the various advantages and disadvantages of the different PA measurement methods, it is relvant to consider them separately.
There is clear evidence that boys and girls have different PA amounts and habits [29, 30]. Discrepancies between genders for self-report and objective measures concerning the duration and intensity of PA have also been found [31]. In addition, gender-specific differentiation of parents is an issue that needs to be addressed more. While most studies examine the influence of maternal SES indicators as a benchmark for “parental” SES indicators, paternal SES indicators are less often collected and analyzed. This is probably because mothers are seen as playing a greater and more influential role in the responsibility and organization of childcare [32]. Nevertheless, parents’ roles in developing health-related behaviors vary and affect boys and girls in different ways [33, 34]. Gender-specific analyses of parents and children can also provide more insight regarding potential associations [35].
Taken together, for a better understanding of the impact of socioeconomic indicators and their components on children’s activity behavior, more current and gender-specific research is needed [17, 36], especially for elementary school age, where the influence of family social background is higher than in older age groups [12, 37]. Advanced knowledge of these associations can be used to extend and specify explanatory frameworks. This, in turn, can help improve public health strategy construction. Therefore, the purpose of this article was to: (A) Systematically review the current research about the association between family socioeconomic indicators (education, occupation and household income) and PA among primary school-aged children; (B) Quantify the distribution of reported associations of these distinguished family socioeconomic indicators in children’s PA evaluated by child’s and parents sex; (C) Differentiate this distribution according to assessment methods (objective vs. self-report) and analysis method (univariate vs. multivariate models).
Subjects and methods
This review was registered with PROSPERO (CRD42021259102) on 15.07.2021. The methodological approach of the review is based on the guidelines of the German Cochrane Community [38]. This manuscript adheres to the PRISMA statement to equity-focused systematic reviews (PRISMA-E) [39].
Search strategy
Potentially relevant studies from January 2010 until 31st March 2022 were identified by searching five electronic databases (MEDLINE (via PubMed), Web of Science, ScienceDirect, SPORTDiscus, and ERIC). In addition, a hand search was performed using Google Scholar. All databases were searched using combinations of relevant keywords related to exposure and outcome. Database-specific filters about population and language were applied where possible. The specific search strategies for each database are displayed in Table 1.
Eligibility
Inclusion and exclusion criteria are listed below.
-
Population: Children aged between 6 and 12 years.
-
Exposure: Index for socioeconomic status (built out of a combination of the three relevant SES indicators. Indicators considered were income (household level) as well as occupation and education of at least one parent or at least one SES indicator.
-
Outcome: PA in unorganized (e.g., ‘free play’) or organized (e.g., sports clubs) settings. PA intensities (e.g., total physical activity (TPA)), moderate physical activity (MPA), moderate-to-vigorous physical activity (MVPA), vigorous physical activity (VPA), leisure-time physical activity (LTPA), PA domains (e.g., organized physical activity (OPA)), active transport (AT), PA frequencies (e.g., times/week, steps/day) or PA durations (e.g., hours or minutes). Studies using objective (e.g., accelerometer, pedometer) and self-report (questionnaire) assessment methods were included.
-
Study design: Cross-sectional or longitudinal survey studies.
-
There was no restriction as to where studies were conducted.
The following exclusion criteria applied:
-
Patient groups (any form of physical or mental diseases or disabilities, including overweight or obesity).
-
Intervention studies.
-
Qualitative study designs.
-
Excluded SES indicators: neighborhood SES, household and family wealth (e.g., car or house ownership, housing tenure, family affluence scale (FAS)), area-based indicators (e.g., average country’s income, area deprivation), SES scores constructed not using the three included secioeconomic indicators (income, occupation, education).
-
Excluded PA domain (outcome): competitive sport, physical education (PE).
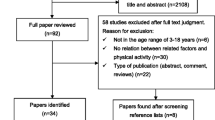
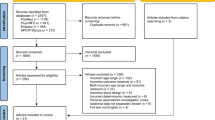
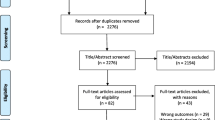
Although some studies technically fulfilled the inclusion criteria, they had to be excluded for the following reasons: thematic context inappropriate (e.g., analysis refers to group differences between ethnicities or countries), the association between exposure and outcome not reported, qualitative deficiencies (missing data e.g., specific age groups) or a combination for several of these reasons (Fig. 1).

Flow chart diagram. *For better comparison with other single-center studies, multi-country studies were separated into single studies according to country
Only articles published in English and peer-reviewed journals were included. Conference abstracts and theses were not considered. In addition, studies were excluded if the risk of bias was considered high (see section risk of bias assessment below).
Due to the amount of data and methodological differences, identified studies for the PA category active transport (AT) will be published separately.
Selection process
Identified citations from the databases were exported into Endnote, and duplicates were removed following the procedure proposed [40]. Title and abstract screening and eligibility assessment of potentially relevant full-texts were done independently by at least two reviewers (AF, AZ, DS, KB). Disagreements were solved by a discussion involving a third reviewer.
Data extraction was done using a pre-piloted Excel spreadsheet by at least two reviewers. The following information was extracted: author, year, country, period of data collection, sample size, age range, gender percentage, response rate, SES indicators, PA outcomes, and measurement methods (Tables 2 and 3). In studies with age groups or age ranges beyond the defined age range of 6–12 years, only data for this age cohort were extracted (as a result, data reported here may be just partial data and may differ from the data of the total sample from the studies).
Classification
The following guidelines were used to classify PA and SES indicators in this study.
Outcome measures
PA was categorized in total physical activity (TPA) if no specific information about duration or intensity was provided and/or if described as ‘total,’ ‘usual,’ ‘daily,’ ‘daily steps,’ ‘daily step counts’, or ‘overall’ PA. PA was also categorized based on intensity in vigorous physical activity (VPA), moderate-to-vigorous physical activity (MVPA), moderate physical activity (MPA) or light physical activity (LPA).
Unorganized physical activity was classified as leisure-time physical activity (LTPA) when described as ‘PA in free time’, ‘play time’, ‘free play’ and/or named ‘total Leisure-time physical activity’.
Extracurricular sports, PA in sports clubs, and PA structured/supervised by a coach, instructor, or other leader were categorized as OPA. Extracurricular sport was classified as OPA only if clearly defined as a guided, structured unit. If not, it is categorized as LTPA.
Socioeconomic indicators
Education (ED) refers to the highest attained level of education (e.g., university education) or the total years of education of one or both parents. Income (IN) refers to the individual income of one (individual level) or both parents (household level). The occupation level (OC) describes the type or amount of employment status of one or both parents. Socioeconomic status (SES) was classified when all three indicators were considered simultaneously in one index.
Risk of bias assessment
Methods of quality assessment were limited by study type. According to the quality assessment used by Beenackers et al. (2012) [16], quality markers: response rate, adjustment, and sample size were conducted to check if quality aspects affect the study results. Following the full-text screening, all remaining studies were re-assessed using these quality markers. The markers were rated as high risk when the response rate was < 50%, associations were not adjusted for at least one variable (e.g., age, gender, etc.) and if a minimum sample size of 500 was not reached to ensure representativeness. Medium risk was classified when the relevant information was unclear, not provided or unspecified, and low risk was classified when all criteria were met. Studies were excluded if two or more quality markers were rated as high risk or if one quality marker was rated as high risk and the other two as medium risk. The risk of bias assessment for the included studies is shown in an additional file (see Additional file 1).
Synthesis of results
Due to high levels of heterogeneity related to population, exposure and outcomes, we refrained from conducting meta-analysis. Studies conducted separately in multiple countries and published as one trial were separated to enhance comparability with other studies. Similar to previous syntheses [16, 40, 41], the results of studies were analyzed on the level of the separate associations instead of just analyzing the complete studies to facilitate understanding of the different associations between various PA domains and various SES indicators.
The associations between the domains of PA behavior and the SES indicators were labeled with ‘+’ when the association was positive and significant. The association was tagged with ‘0’ when no significant association existed. The association was tagged with ‘-’ when a significant negative association was found. A significance level α = 0.05 was considered. In the case of more than two groups, comparisons between them were included based on the applied statistical methods in the original studies.
If available, the adjusted results were used to account for confounding factors. Distributions of reported positive, negative, and null associations were evaluated for each PA outcome by gender and SES indicator (Tables 4, 5, 6, 7 and 8). The same analyses were conducted for both genders, combined as well as separated. Sub-group analyses were performed for self-report versus objective PA assessments and for univariate versus multivariate analyses.
For better comparison with other single-center studies, multi-country studies were separated into single studies according to country (i.e., publications from EuropeaN Energy balance Research to prevent excessive weight Gain among Youth (ENERGY-project), etc.). Respective studies are marked in Tables 2 and 3.
Ethics
Approval by an ethics committee was not required as only published data were used in this systematic review.
Results
The initial yielded a total of 23.935 citations, of which 653 were retrieved as full-text after duplicates removal and title and abstract screening. Finally, 77 reports of 93 studies fulfilled the eligibility criteria and were included. The entire study selection process is displayed in Fig. 1.
The 93 studies reported on 77 publications and 372 unique associations between a SES indicator and PA outcome. The majority of the studies were conducted in Europe (54), followed by North America (14), Asia (14), South America (4), Africa (4), and Australia (3) (Table 2).
The sample size ranged from small studies with 131 participants to multi-country studies with sample sizes of up to 10.190 participants. Most studies reported a response rate between 60% and 80%. 35 publications did not report response rates, and 6 studies reported partial or incomplete information. Most studies (64) used self-reports (questionnaires) to assess PA. The most frequently validated PA questionnaire was the Physical Activity Questionnaire for Older Children (PAQ-C) [42]. Nineteen studies applied objective measurement methodology. The studies predominantly used accelerometers (ActiGraph GT3X, GT3X+, GT1M). Fourteen studies used both methods. Most of the studies were single studies. However, some studies were from more extensive cohort studies, e.g. ISCOLE Study, ENERGY-project, Childhood Obesity Surveillance Initiative (COSI), and Millennium Cohort Study (MCS). Concerning the SES indicators, the most prominent indicator was education, followed by occupation and income. Only 2 studies have calculated an SES index based on education, occupation, and income. Relating PA, most of the studies focused on MVPA and TPA, followed by OPA and LTPA. Only a few studies measured VPA, LPA, and MPA (Table 3).
Education
Results showed a strong association between education and OPA, with nearly all studies demonstrating that higher education led to increased levels of organized PA participation in uni- and multivariate models (Tables 7 and 8). Studies only applied subjective methods of PA measurement. Overall, for education and TPA, most studies showed no association, which was supported by the multivariate study results. A more detailed analysis demonstrated a negative association between objectively measured TPA and maternal education when both genders were combined (2/3 studies) and in gender-separated analysis (n = 1 for boys and girls, respectively). For subjective assessments of TPA, there was a difference between gender-combined and separated studies, with no or negative associations in gender-combined analyses, no association for girls and no or positive associations in boys. Similarly, for MVPA, the vast majority of studies found no associations with education, with very few studies providing gender-separated analyses for paternal (n = 1) and maternal (n = 2) education (Table 4). Trials on maternal education found inconsistent results, with one study each demonstrating no or negative associations for boys and girls when measured objectively, an inconsistency also displayed when genders were combined. Contrarily, for paternal education, a positive association was found in girls; again, MVPA was measured objectively. No association could be identified for boys or when genders were combined. All seven gender-combined studies showed no association when MVPA was measured subjectively, while for maternal (n = 3) and paternal (n = 2) studies, positive and negative associations were found. When measured objectively, nearly all studies did not find associations, with few demonstrating negative ones. Using parental education combined, the results draw a similar picture to maternal education. Multivariate studies were somewhat similar to the results of objectively measured MVPA trials (Tables 5 and 6).
Few studies assessed LPA and MPA, all applying objective measures. Overall, most studies showed no associations between these PA measures and education (Table 4). Due to the lack of studies, no information is available for genders about paternal and maternal education. One of two studies found a negative association between MPA and maternal education when genders were analyzed together. For LPA and parental education mixed, there was no association when genders were combined, while for both genders separated (n = 2 each), inconsistent results with no or negative associations were found. The multivariate results confirmed the negative association for both genders. For VPA, inconsistent results were identified. While most studies showed no associations with education, two trials using objective measurements found positive associations. A Swedish representative sample demonstrated that girls with higher-educated parents were more vigorously active than their less-educated counterparts [43]. Similarly, one of two studies using maternal education as SES indicator found a positive association. While objectively measured, there was no negative association (n = 3), and this was the case in more than one-third of the subjectively reported studies (n = 7/19) for which only three found positive associations.
Few studies investigated the relationship between education and LTPA, and all of them applied subjective PA methods. Just one and two studies on paternal and maternal education respectively separated analyses by gender and found no association (Table 6). Two of three (all multivariate) studies found negative associations for this PA outcome for both paternal and maternal education when genders were combined. When parental education was combined as were genders, heterogeneous results were reported, with some studies showing positive, no, or negative associations. When looking at gender-separated analyses, no positive associations were found (Table 7).
Occupation
For the association of occupation and OPA, only self-report studies were included (Table 6), and all applied multivariate analyses (Table 7). Results demonstrate no effect of maternal (n = 1) and paternal (n = 1) occupation. The same result was found in about one-third of studies combining parental occupation. Here, the majority pointed to a positive relationship. For TPA, no association was found in any study for combined parental, maternal, and paternal occupation. Regarding MVPA, most studies found no association with few reporting a negative relationship between MVPA and occupational status for maternal and paternal occupation. There was no study demonstrating a positive association. For VPA and MPA, only self-report studies were available, showing no associations between parental occupation combined and maternal occupation. No data were reported on paternal occupation (Table 4). For VPA, three out of 18 studies found negative associations for children in Latvia, Albania, and Spain, while the other studies found none. No data were available for LPA. For LTPA, parental occupation combined was positively associated for boys and girls separately, while no such relationship was identified using maternal or paternal occupation. However, for these measures, only one study each was found. When genders were combined, no association was found for parental and maternal occupation. For paternal occupational status, overall one in three or one in two (multivariate analysis) found positive associations (Tables 4 and 7).
Income
Only self-report studies were identified for the association of income and OPA (outcome). Overall, a strong positive association exists between household income and this outcome in studies that combined both genders. Conversly, contrary results were reported for both genders (n = 2 each). With regard to TPA, there appears to be no association with income (Table 6). In multivariate analyses, neither boys’ (n = 2) nor girls’ (n = 2) TPA was affected by the respective household income, measured both objectively and by self-report. Few studies in gender-combined analyses and one study in girls pointed towards a positive association, while one large, representative sample in the US found a negative association. There are inconsistent results for MVPA with regard to household income, with studies mostly split between no and negative associations. Only objective studies (n = 2 for both genders) were available for gender-separated analyses. Multivariate analyses came to the same results (Table 7). For LPA, MPA, and VPA, few available studies overall showed partially positive associations for VPA (n = 1/2), somewhat negative associations for MPA (n = 1/2), and the one study reporting on this outcome found a negative association between income and LPA (Table 4). No study reported results separated for boys and girls. For objectively measured LTPA, no studies could be identified (Table 5). The few studies showed no associations between income and LTPA in gender-separated analyses. In studies reporting both genders combined, inconsistent results between studies were reported, all of which applied multivariate methods.
SES
The few studies investigating the relationships between SES and subjectively measured PA found a positive association for TPA, while no associations could be identified for MVPA and LTPA (Tables 4, 6, 7 and 8).
Discussion
The primary purpose of this study was to systematically review the recent evidence about the associations between family socioeconomic indicators (education, occupation, and household income and their combination (SES)) in different domains (e.g., OPA) or intensities of PA among primary school-aged children and to quantify these associations.
Overall, the analyses showed great heterogeneity in terms of outcomes, measurement of PA and SES variables, and often no clear effects contrary to what has been proclaimed in the literature. A relatively straightforward relationship existed between all individual socioeconomic factors and OPA. Results showed a predominantly positive relationship consistent across all gender variants (maternal, paternal, and parental), indicating that children from mothers and fathers with a higher education, occupation, and income have a higher probability for OPA. This association is likely related, among other things, to monetary conditions. OPA in an institution (e.g., a sports club) costs money, therefore children of higher-income households have fewer financial barriers to participation in OPA than those with a lower household income [44,45,46,47]. Strategies to reduce the gap between higher and lower-income families regarding participation and dropout rates in organized physical activities for their children need to focus on the reduction of financial barriers, e.g., through the use of vouchers [48,49,50].
In addition to the financial requirements, the parents’ educational background is a relevant factor for children’s participation in OPA. Parents with a higher level of education are more likely to deal with topics such as health behavior and to understand the significance of insufficient PA. As a consequence, higher educated parents more often act as role models for their children by being physically active themselves, and they are also more likely to be involved in OPA for their children (e.g., transportation) [51,52,53,54].
In contrast, the results for the different intensities of daily PA (TPA, LPA, MPA, MVPA, VPA, LTPA) are very heterogeneous. Regarding the intensities, an imbalance was shown in terms of the frequencies. Most studies were focused on MVPA. This is probably because the evidence and study situation for the association of MVPA with health benefits is better than for other PA intensities. Existing international recommendations focus on MVPA [55], which in turn causes this intensity being most frequently studied. In addition to MVPA, there are also relatively clear recommendations and evidence for VPA, addressed in many studies as part of the WHO European Childhood Obesity Surveillance Initiative (COSI) [56]. After MVPA and VPA, some studies addressed leisure-time PA. A notable aspect here was the sum of different terminology (e.g., free play, outdoor play, after-school PA, weekend, etc.) for LTPA. Therefore, a clear delimitation from other PA intensities or domains was difficult at some points. Fewest studies were found for TPA, LPA, and MPA. For these PA intensities, however, there is little research and thus no clear recommendations.
Contrarily, the results for associations between parental education and unorganized PA (especially outdoor play) were rather heterogeneous. Most of the PA intensities (TPA, MVPA, VPA) did not show associations or rather negative ones, especially for maternal education and for girls. There were a few outliers with tendencies toward a positive association for boys and for paternal education. Similar findings were reported previously [57, 58]. Possible explanations could include the educational trajectories of children from families with higher levels of education. Higher forms of schooling usually also mean a higher workload with school tasks (e.g., longer school days, more demanding homework) and thus less free time available for PA.
Regarding the occupational status of parents, the majority of studies showed no association and, if anything, a tendency toward a negative association. The same tendency could be found for income. However, studies on the SES index have shown positive or no association. As only two publications of one longitudinal study from Germany were identified for such an index and only associations for a few PA domains were reported, the certainty of this association is very low.
Most studies used parental education, followed by parental occupation, and just a few studies used parental or household income as a marker of SES, likely because information about the level of education is considered less sensitive compared to other information related to SES. Therefore, the response rate is relatively high compared to income. The least of all were studies that used a SES index. This is interesting because most studies reported on the influence of SES or socioeconomic position, mostly measuring only one variable and not having multiple pieces of information to calculate an actual complex index. However, there are differences between the various SES indicators, and with the above-average number of studies that only included education as an SES indicator, a bias in the overall picture of the relationships could potentially arise. To provide a complete picture of the socioeconomic situation, a comprehensive index should be collected [59].
Furthermore, results demonstrate an imbalance in gender-specific data of the individual SES indicators. More studies reported associations between maternal SES indicators, e.g., maternal educational level. This is probably because mothers, compared to fathers, are more responsible for organizational tasks related to the child [32], including filling in questionnaires for their children. Therefore, there is a lack of information on paternal SES indicators, reducing power and certainty into the evidence for latter. These findings differ for income as information on this parameter is usually inquired on a household level, which means that information on both parents’ income is integrated.
Some general aspects are limiting the comparability of identified studies on the one hand, but on the other hand, can also explain the heterogeneity of the results. The location and timing of data collection are essential to consider because of weather and seasonal influences, especially for unstructured PA (e.g., outdoor play) [60,61,62]. This may lead to different results by collecting and analyzing the same parameters. But also different ethnic backgrounds under which the studies took place lead to different results [63, 64] and make international comparability difficult. Also, environmental and structural conditions play a role in the heterogeneity of the results. For example, children from families with similar SES backgrounds but different living situations (urban versus rural) have different PA behaviors [65], e.g., the access for children from rural areas to sports clubs may be limited. Overall, the generalizability of the results on a global level is potentially limited as the majority of the included studies were conducted in Europe.
The heterogeneity of the associations of SES factors, especially in unorganized PA, illustrates the complexity of this context. This was also shown by non-linear and U-shaped associations in some studies. However, fewer studies are analyzing multivariate models for the relationship between SES and its single factors and PA in which various relevant factors (including mediators and moderators) are considered. However, a multivariate approach is better since univariate models do not meet the requirements of the complexity of the topic. Future research in this area should take this into account and adjust for multiple relevant factors.
Strengths and limitations
A strength of this review is the clustering of the identified studies into several smaller subcategories (e.g., objective vs. subjective, univariate vs. multivariate, gender-combined vs. separated) and, by that enabling a more specific insight into this complex topic. We identified several research gaps, such as the need for more information on paternal SES indicators.
Overall, it is important to point out that socioeconomic disparities in health represent a fundamentally complex area of research due to the intricate causal mechanisms involved. The predominance of evidence derived from observational studies introduces the risk of confounding bias, which is defined as a spurious association introduced by an extraneous variable that influences both the socioeconomic exposure and the health outcome [66]. Moreover, due to this complexity, there is also a risk of overadjustment [67]. Considering these factors, the current review describes associations but cannot clearly demonstrate causal relationships.
Furthermore, several other limitations need to be acknowledged. First, PA measures, such as VPA or MVPA, may have been taken during an organized activity in a sports club. Thus, classifying unstructured PA (e.g., free play) or organized PA is complicated or overlapping. This point concerns objective measures more than collecting incidental and planned activities, while self-report measures gather mostly larger chunks of habitual PA information. Second, the possibility of different coding and categorization of the SES indicators may have affected the results. For example, occupational status may have been collected dichotomously (yes or no), according to the number of hours (full-time, part-time, marginal) or according to the actual activity (e.g., craft sector or office) or position (e.g., leading position) and then categorized into high, medium or low. Also, different cut-off values for the SES indicators complicate comparisons between studies (e.g., different thresholds for categorizing the educational level as high, medium, and low). Third, only individual SES indicators were considered in this study. Thus, all studies collecting SES based on the living area (e.g., via Zipcode) were not considered. However, compared to area-based SES measures, SES obtained individually shows greater associations with health outcomes and avoids masking significant heterogeneity amongst populations [68]. In addition, as we focused on few common SES indicators as well as the SES index, it was discovered that children and adolescents, in particular, were unable to provide substantial responses regarding their families’ finances (e.g., paternal occupation) [69]. Consequently, less intrusive and more comprehensible approaches, such as the Family Affluence Scale (FAS), are also used to determine their socioeconomic status. However, this is more prevalent in older children and adolescents. In the age cohort under consideration, it can be assumed that the questionnaires are completed by the parents and that the relevant information can be provided in a valid manner. Nevertheless, the incorporation of additional alternative scales for the assessment of SES (such as the FAS) in future studies could prove beneficial in further elucidating this matter. Lastly, due to the large heterogeneity in the measurement of the SES variables and the study populations (e.g., studies in different regions, at different time points, with different ethnic groups, and with different initial questions), we decided against performing a meta-analysis [70]. Future evidence syntheses may investigate specific factors and attempt to pool results mathematically.
Conclusion
The results of this review showed predominantly positive associations between the individual socioeconomic factors education, occupation and income, and organized PA. In contrast, the results for SES indicators and different intensities of daily PA (TPA, LPA, MPA, MVPA, VPA, LTPA) were very heterogeneous, with overwhelmingly no associations. An uneven distribution was shown with most studies measuring maternal education as a benchmark for family SES. Overall, there is a lack of large multicenter studies using an accurate SES index as a predictor. Future research should focus on larger multicenter studies and analyzing gender-specific multivariate models for the relationship of SES and especially children’s unstructured PA, considering potentially relevant mediators and moderators to cover the complexity of the association.
Data availability
Data will be available upon request of the corresponding author.
Abbreviations
- PA:
-
Physical Activity
- TPA:
-
Total physical activity
- LTPA:
-
Light physcial activity
- MPA:
-
Moderate physical activity
- MVPA:
-
Moderate-to-vigorous physical activity
- VPA:
-
Vigorous physical activity
- LTPA:
-
Leisure-time physical activity
- OPA:
-
Organized physical activity
- AT:
-
Active transport
- SES:
-
Socioeconomic status
- PRISMA:
-
Preferred Reporting Items of Systematic Reviews and Meta-Analysis
References
Poitras VJ, Gray CE, Borghese MM, Carson V, Chaput J-P, Janssen I, et al. Systematic review of the relationships between objectively measured physical activity and health indicators in school-aged children and youth. Appl Physiol Nutr Metab. 2016;41:S197–239. https://doi.org/10.1139/apnm-2015-0663.
Carson V, Ridgers ND, Howard BJ, Winkler EAH, Healy GN, Owen N, et al. Light-intensity physical activity and cardiometabolic biomarkers in US adolescents. PLoS ONE. 2013;8:e71417. https://doi.org/10.1371/journal.pone.0071417.
Biddle SJ, Ciaccioni S, Thomas G, Vergeer I. Physical activity and mental health in children and adolescents: an updated review of reviews and an analysis of causality. Psychol Sport Exerc. 2019;42:146–55. https://doi.org/10.1016/j.psychsport.2018.08.011.
Dale LP, Vanderloo L, Moore S, Faulkner G. Physical activity and depression, anxiety, and self-esteem in children and youth: an umbrella systematic review. Ment Health Phys Act. 2019;16:66–79. https://doi.org/10.1016/j.mhpa.2018.12.001.
Guthold R, Stevens GA, Riley LM, Bull FC. Global trends in insufficient physical activity among adolescents: a pooled analysis of 298 population-based surveys with 1·6 million participants. Lancet Child Adolesc Health. 2020;4:23–35. https://doi.org/10.1016/S2352-4642(19)30323-2.
Aubert S, Barnes JD, Abdeta C, Abi Nader P, Adeniyi AF, Aguilar-Farias N, et al. Global matrix 3.0 physical activity report card grades for children and youth: results and analysis from 49 countries. J Phys Act Health. 2018;15:S251–73. https://doi.org/10.1123/jpah.2018-0472.
Rossi L, Behme N, Breuer C. Physical activity of children and adolescents during the COVID-19 Pandemic-A scoping review. Int J Environ Res Public Health. 2021. https://doi.org/10.3390/ijerph182111440.
Wunsch K, Kienberger K, Niessner C. Changes in physical activity patterns due to the Covid-19 pandemic: a systematic review and Meta-analysis. Int J Environ Res Public Health. 2022. https://doi.org/10.3390/ijerph19042250.
Guerrero MD, Vanderloo LM, Rhodes RE, Faulkner G, Moore SA, Tremblay MS. Canadian children’s and youth’s adherence to the 24-h movement guidelines during the COVID-19 pandemic: a decision tree analysis. J Sport Health Sci. 2020;9:313–21. https://doi.org/10.1016/j.jshs.2020.06.005.
Farooq A, Martin A, Janssen X, Wilson MG, Gibson A-M, Hughes A, Reilly JJ. Longitudinal changes in moderate-to-vigorous-intensity physical activity in children and adolescents: a systematic review and meta-analysis. Obes Rev. 2020;21:e12953. https://doi.org/10.1111/obr.12953.
Poulain T, Vogel M, Sobek C, Hilbert A, Körner A, Kiess W. Associations between Socio-Economic Status and Child Health: findings of a large German cohort study. Int J Environ Res Public Health. 2019. https://doi.org/10.3390/ijerph16050677.
Bradley RH, Corwyn RF. Socioeconomic status and child development. Annu Rev Psychol. 2002;53:371–99. https://doi.org/10.1146/annurev.psych.53.100901.135233.
Elhakeem A, Cooper R, Bann D, Hardy R. Childhood socioeconomic position and adult leisure-time physical activity: a systematic review. Int J Behav Nutr Phys Act. 2015;12:92. https://doi.org/10.1186/s12966-015-0250-0.
Juneau CE, Benmarhnia T, Poulin AA, Côté S, Potvin L. Socioeconomic position during childhood and physical activity during adulthood: a systematic review. Int J Public Health. 2015;60:799–813. https://doi.org/10.1007/s00038-015-0710-y.
Puolakka E, Pahkala K, Laitinen TT, Magnussen CG, Hutri-Kähönen N, Männistö S, et al. Childhood socioeconomic status and lifetime health behaviors: the Young finns Study. Int J Cardiol. 2018;258:289–94. https://doi.org/10.1016/j.ijcard.2018.01.088.
Beenackers MA, Kamphuis CBM, Giskes K, Brug J, Kunst AE, Burdorf A, van Lenthe FJ. Socioeconomic inequalities in occupational, leisure-time, and transport related physical activity among European adults: a systematic review. Int J Behav Nutr Phys Act. 2012;9:116. https://doi.org/10.1186/1479-5868-9-116.
O’Donoghue G, Kennedy A, Puggina A, Aleksovska K, Buck C, Burns C, et al. Socio-economic determinants of physical activity across the life course: a DEterminants of DIet and physical ACtivity (DEDIPAC) umbrella literature review. PLoS ONE. 2018;13:e0190737. https://doi.org/10.1371/journal.pone.0190737.
Edwardson CL, Gorely T. Parental influences on different types and intensities of physical activity in youth: a systematic review. Psychol Sport Exerc. 2010;11:522–35. https://doi.org/10.1016/j.psychsport.2010.05.001.
Reilly JJ. When does it all go wrong? Longitudinal studies of changes in moderate-to-vigorous-intensity physical activity across childhood and adolescence. J Exerc Sci Fit. 2016;14:1–6. https://doi.org/10.1016/j.jesf.2016.05.002.
Arundell L, Fletcher E, Salmon J, Veitch J, Hinkley T. A systematic review of the prevalence of sedentary behavior during the after-school period among children aged 5–18 years. Int J Behav Nutr Phys Act. 2016;13:93. https://doi.org/10.1186/s12966-016-0419-1.
Lenze L. Sport and leisure-time physical activity behavior over the life course: description and explanation of factors and events of individual trajectories. Universität Bern; 2023.
Lenze L, Klostermann C, Schmid J, Lamprecht M, Nagel S. The role of leisure-time physical activity in youth for lifelong activity-a latent profile analysis with retrospective life course data. Ger J Exerc Sport Res. 2024;54:192–200. https://doi.org/10.1007/s12662-023-00884-9.
Kari JT, Tammelin TH, Viinikainen J, Hutri-Kähönen N, Raitakari OT, Pehkonen J. Childhood Physical Activity and Adulthood earnings. Med Sci Sports Exerc. 2016;48:1340–6. https://doi.org/10.1249/MSS.0000000000000895.
Marasso D, Lupo C, Collura S, Rainoldi A, Brustio PR. Subjective versus objective measure of physical activity: a systematic review and Meta-analysis of the Convergent Validity of the physical activity questionnaire for children (PAQ-C). Int J Environ Res Public Health. 2021. https://doi.org/10.3390/ijerph18073413.
Sabia S, van Hees VT, Shipley MJ, Trenell MI, Hagger-Johnson G, Elbaz A, et al. Association between questionnaire- and accelerometer-assessed physical activity: the role of sociodemographic factors. Am J Epidemiol. 2014;179:781–90. https://doi.org/10.1093/aje/kwt330.
Chinapaw MJM, Mokkink LB, van Poppel MNM, van Mechelen W, Terwee CB. Physical activity questionnaires for youth: a systematic review of measurement properties. Sports Med. 2010;40:539–63. https://doi.org/10.2165/11530770-000000000-00000.
Hidding LM, Chinapaw MJM, van Poppel MNM, Mokkink LB, Altenburg TM. An updated systematic review of Childhood Physical Activity questionnaires. Sports Med. 2018;48:2797–842. https://doi.org/10.1007/s40279-018-0987-0.
Schmidt SCE, Anedda B, Burchartz A, Oriwol D, Kolb S, Wäsche H, et al. The physical activity of children and adolescents in Germany 2003–2017: the MoMo-study. PLoS ONE. 2020;15:e0236117. https://doi.org/10.1371/journal.pone.0236117.
Wang L, Wang L. Using theory of Planned Behavior to predict the physical activity of children: probing gender differences. Biomed Res Int. 2015;2015:536904. https://doi.org/10.1155/2015/536904.
Trost SG, Pate RR, Sallis JF, Freedson PS, Taylor WC, Dowda M, Sirard J. Age and gender differences in objectively measured physical activity in youth. Med Sci Sports Exerc. 2002;34:350–5. https://doi.org/10.1097/00005768-200202000-00025.
Sallis JF, McKenzie TL, Elder JP, Hoy PL, Galati T, Berry CC, et al. Sex and ethnic differences in children’s physical activity: discrepancies between self-report and objective measures. Pediatr Exerc Sci. 1998;10:277–84. https://doi.org/10.1123/pes.10.3.277.
Aslam M, Kingdon GG. Parental Education and Child Health—understanding the pathways of Impact in Pakistan. World Dev. 2012;40:2014–32. https://doi.org/10.1016/j.worlddev.2012.05.007.
Beets MW, Cardinal BJ, Alderman BL. Parental social support and the physical activity-related behaviors of youth: a review. Health Educ Behav. 2010;37:621–44. https://doi.org/10.1177/1090198110363884.
Davison KK, Cutting TM, Birch LL. Parents’ activity-related parenting practices predict girls’ physical activity. Med Sci Sports Exerc. 2003;35:1589–95. https://doi.org/10.1249/01.mss.0000084524.19408.0c.
Neshteruk CD, Nezami BT, Nino-Tapias G, Davison KK, Ward DS. The influence of fathers on children’s physical activity: a review of the literature from 2009 to 2015. Prev Med. 2017;102:12–9. https://doi.org/10.1016/j.ypmed.2017.06.027.
Nakabazzi B, Wachira L-JM, Oyeyemi AL, Ssenyonga R, Onywera VO. Prevalence and socio-demographic correlates of accelerometer measured physical activity levels of school-going children in Kampala city, Uganda. PLoS ONE. 2020;15:e0235211. https://doi.org/10.1371/journal.pone.0235211.
Alderman BL, Benham-Deal TB, Jenkins JM. Change in parental influence on children’s physical activity over time. J Phys Act Health. 2010;7:60–7. https://doi.org/10.1123/jpah.7.1.60.
Universitätsklinikum F. Deutsches Cochrane Zentrum. Manual Systematische Literaturrecherche für die Erstellung Von Leitlinien. Universität Freiburg; 2013.
Welch V, Petticrew M, Petkovic J, Moher D, Waters E, White H, Tugwell P. Extending the PRISMA statement to equity-focused systematic reviews (PRISMA-E 2012): explanation and elaboration. J Clin Epidemiol. 2016;70:68–89. https://doi.org/10.1016/j.jclinepi.2015.09.001.
Bramer WM, Giustini D, de Jonge GB, Holland L, Bekhuis T. De-duplication of database search results for systematic reviews in EndNote. J Med Libr Assoc. 2016;104:240–3. https://doi.org/10.3163/1536-5050.104.3.014.
McLaren L. Socioeconomic status and obesity. Epidemiol Rev. 2007;29:29–48. https://doi.org/10.1093/epirev/mxm001.
Crocker PR, Bailey DA, Faulkner RA, Kowalski KC, McGrath R. Measuring general levels of physical activity: preliminary evidence for the physical activity questionnaire for older children. Med Sci Sports Exerc. 1997;29:1344–9. https://doi.org/10.1097/00005768-199710000-00011.
Nyberg G, Kjellenberg K, Fröberg A, Lindroos AK. A national survey showed low levels of physical activity in a representative sample of Swedish adolescents. Acta Paediatr. 2020;109:2342–53. https://doi.org/10.1111/apa.15251.
Andersen PL, Bakken A. Social class differences in youths’ participation in organized sports: what are the mechanisms? Int Rev Sociol Sport. 2019;54:921–37. https://doi.org/10.1177/1012690218764626.
Thibaut E, Eakins J, Vos S, Scheerder J. Time and money expenditure in sports participation: the role of income in consuming the most practiced sports activities in Flanders. Sport Manage Rev. 2017;20:455–67. https://doi.org/10.1016/j.smr.2016.12.002.
Lampinen E-K, Eloranta A-M, Haapala EA, Lindi V, Väistö J, Lintu N, et al. Physical activity, sedentary behaviour, and socioeconomic status among Finnish girls and boys aged 6–8 years. Eur J Sport Sci. 2017;17:462–72. https://doi.org/10.1080/17461391.2017.1294619.
Kirby J, Levin KA, Inchley J. Socio-environmental influences on physical activity among young people: a qualitative study. Health Educ Res. 2013;28:954–69. https://doi.org/10.1093/her/cyt085.
Reece LJ, McInerney C, Blazek K, Foley BC, Schmutz L, Bellew B, Bauman AE. Reducing financial barriers through the implementation of voucher incentives to promote children’s participation in community sport in Australia. BMC Public Health. 2020;20:19. https://doi.org/10.1186/s12889-019-8049-6.
Foley BC, Owen KB, Bauman AE, Bellew W, Reece LJ. Effects of the active kids voucher program on children and adolescents’ physical activity: a natural experiment evaluating a state-wide intervention. BMC Public Health. 2021;21:22. https://doi.org/10.1186/s12889-020-10060-5.
James ML, Christian D, Scott SC, Todd CE, Stratton G, Demmler J, et al. Active children through individual vouchers evaluation: a mixed-method RCT. Am J Prev Med. 2020;58:232–43. https://doi.org/10.1016/j.amepre.2019.10.005.
Seabra A, Mendonça D, Maia J, Welk G, Brustad R, Fonseca AM, Seabra AF. Gender, weight status and socioeconomic differences in psychosocial correlates of physical activity in schoolchildren. J Sci Med Sport. 2013;16:320–6. https://doi.org/10.1016/j.jsams.2012.07.008.
Seabra AC, Seabra AF, Mendonça DM, Brustad R, Maia JA, Fonseca AM, Malina RM. Psychosocial correlates of physical activity in school children aged 8–10 years. Eur J Public Health. 2013;23:794–8. https://doi.org/10.1093/eurpub/cks149.
Ritchie LD, Welk G, Styne D, Gerstein DE, Crawford PB. Family environment and pediatric overweight: what is a parent to do? J Am Diet Assoc. 2005;105:S70–9. https://doi.org/10.1016/j.jada.2005.02.017.
Trost SG, Sallis JF, Pate RR, Freedson PS, Taylor WC, Dowda M. Evaluating a model of parental influence on youth physical activity. Am J Prev Med. 2003;25:277–82. https://doi.org/10.1016/s0749-3797(03)00217-4.
Bull FC, Al-Ansari SS, Biddle S, Borodulin K, Buman MP, Cardon G, et al. World Health Organization 2020 guidelines on physical activity and sedentary behaviour. Br J Sports Med. 2020;54:1451–62. https://doi.org/10.1136/bjsports-2020-102955.
Musić Milanović S, Buoncristiano M, Križan H, Rathmes G, Williams J, Hyska J, et al. Socioeconomic disparities in physical activity, sedentary behavior and sleep patterns among 6- to 9-year-old children from 24 countries in the WHO European region. Obes Rev. 2021;22(Suppl 6):e13209. https://doi.org/10.1111/obr.13209.
Jekauc D, Reimers AK, Wagner MO, Woll A. Prevalence and socio-demographic correlates of the compliance with the physical activity guidelines in children and adolescents in Germany. BMC Public Health. 2012;12:714. https://doi.org/10.1186/1471-2458-12-714.
Boxberger K, Reimers AK. Parental correlates of Outdoor Play in boys and girls aged 0 to 12-A systematic review. Int J Environ Res Public Health. 2019. https://doi.org/10.3390/ijerph16020190.
Lindberg MH, Chen G, Olsen JA, Abelsen B. Combining education and income into a socioeconomic position score for use in studies of health inequalities. BMC Public Health. 2022;22:969. https://doi.org/10.1186/s12889-022-13366-8.
Yildirim M, Schoeni A, Singh AS, Altenburg TM, Brug J, de Bourdeaudhuij I, et al. Daily variations in weather and the relationship with physical activity and sedentary time in European 10- to 12-year-olds: the ENERGY-Project. J Phys Act Health. 2014;11:419–25. https://doi.org/10.1123/jpah.2012-0102.
Atkin AJ, Sharp SJ, Harrison F, Brage S, van Sluijs EMF. Seasonal Variation in Children’s physical activity and sedentary time. Med Sci Sports Exerc. 2016;48:449–56. https://doi.org/10.1249/MSS.0000000000000786.
Rahman S, Maximova K, Carson V, Jhangri GS, Veugelers PJ. Stay in or play out? The influence of weather conditions on physical activity of grade 5 children in Canada. Can J Public Health. 2019;110:169–77. https://doi.org/10.17269/s41997-019-00176-6.
van Dyke ME, Cheung PC, Franks P, Gazmararian JA. Socioeconomic and Racial/Ethnic disparities in physical activity environments in Georgia Elementary schools. Am J Health Promot. 2018;32:453–63. https://doi.org/10.1177/0890117117717016.
Gu X, Zhang T, Chu TLA, Wang J, Zhang X, Nelson L, Brown K. Exploring racial disparities in physical activity and quality of Life through an expectancy-value perspective. J Racial Ethn Health Disparities. 2019;6:973–80. https://doi.org/10.1007/s40615-019-00598-5.
Hansen AY, Umstattd Meyer MR, Lenardson JD, Hartley D. Built environments and active living in rural and remote areas: a review of the literature. Curr Obes Rep. 2015;4:484–93. https://doi.org/10.1007/s13679-015-0180-9.
Meuli L, Dick F. Understanding confounding in Observational studies. Eur J Vasc Endovasc Surg. 2018;55:737. https://doi.org/10.1016/j.ejvs.2018.02.028.
van Zwieten A, Dai J, Blyth FM, Wong G, Khalatbari-Soltani S. Overadjustment bias in systematic reviews and meta-analyses of socio-economic inequalities in health: a meta-research scoping review. Int J Epidemiol. 2023. https://doi.org/10.1093/ije/dyad177.
Pardo-Crespo MR, Narla NP, Williams AR, Beebe TJ, Sloan J, Yawn BP, et al. Comparison of individual-level versus area-level socioeconomic measures in assessing health outcomes of children in Olmsted County, Minnesota. J Epidemiol Community Health. 2013;67:305–10. https://doi.org/10.1136/jech-2012-201742.
Currie CE, Elton RA, Todd J, Platt S. Indicators of socioeconomic status for adolescents: the WHO Health Behaviour in School-aged children Survey. Health Educ Res. 1997;12:385–97. https://doi.org/10.1093/her/12.3.385.
Blettner M, Schlehofer B, Sauerbrei W. Grenzen Von Metaanalysen aus publizierten Daten Bei Epidemiologischen Fragestellungen. [Limitations of meta-analysis from published data in epidemiological research]. Soz Praventivmed. 1997;42:95–104. https://doi.org/10.1007/BF01318138.
Aarts M-J, de Vries SI, van Oers H am, Schuit AJ. Outdoor play among children in relation to neighborhood characteristics: a cross-sectional neighborhood observation study. Int J Behav Nutr Phys Act. 2012;9:98. https://doi.org/10.1186/1479-5868-9-98.
Aarts M-J, Wendel-Vos W, van Oers HAM, van de Goor IAM, Schuit AJ. Environmental determinants of outdoor play in children: a large-scale cross-sectional study. Am J Prev Med. 2010;39:212–9. https://doi.org/10.1016/j.amepre.2010.05.008.
Aggio D, Gardner B, Roberts J, Johnstone J, Stubbs B, Williams G, et al. Correlates of children’s independent outdoor play: cross-sectional analyses from the Millennium Cohort Study. Prev Med Rep. 2017;8:10–4. https://doi.org/10.1016/j.pmedr.2017.07.007.
Aguilar-Farias N, Martino-Fuentealba P, Chandia-Poblete D. Correlates of device-measured physical activity, sedentary behaviour and sleeping in children aged 9–11 years from Chile: ESPACIOS study (Factores asociados con actividad física, conducta sedentaria y sueño medidos con acelerómetros en niños de 9–11 años. Retos. 2019;1–10. https://doi.org/10.47197/retos.v37i37.71142.
Al Yazeedi B, Berry DC, Crandell J, Waly M. Family Influence on children’s Nutrition and physical activity patterns in Oman. J Pediatr Nurs. 2021;56:e42–8. https://doi.org/10.1016/j.pedn.2020.07.012.
Alotaibi T, Almuhanna R, Alhassan J, Alqadhib E, Mortada E, Alwhaibi R. The relationship between Technology Use and physical activity among typically-developing children. Healthc (Basel). 2020. https://doi.org/10.3390/healthcare8040488.
Bagordo F, de Donno A, Grassi T, Guido M, Devoti G, Ceretti E, et al. Lifestyles and socio-cultural factors among children aged 6–8 years from five Italian towns: the MAPEC_LIFE study cohort. BMC Public Health. 2017;17:233. https://doi.org/10.1186/s12889-017-4142-x.
Barr-Anderson DJ, Flynn JI, Dowda M, Taverno Ross SE, Schenkelberg MA, Reid LA, Pate RR. The modifying effects of Race/Ethnicity and socioeconomic status on the Change in Physical Activity from Elementary to Middle School. J Adolesc Health. 2017;61:562–70. https://doi.org/10.1016/j.jadohealth.2017.05.007.
Beckvid Henriksson G, Franzén S, Elinder LS, Nyberg G. Low socio-economic status associated with unhealthy weight in six-year-old Swedish children despite higher levels of physical activity. Acta Paediatr. 2016;105:1204–10. https://doi.org/10.1111/apa.13412.
Brug J, van Stralen MM, Te Velde SJ, Chinapaw MJM, de Bourdeaudhuij I, Lien N, et al. Differences in weight status and energy-balance related behaviors among schoolchildren across Europe: the ENERGY-project. PLoS ONE. 2012;7:e34742. https://doi.org/10.1371/journal.pone.0034742.
Butte NF, Gregorich SE, Tschann JM, Penilla C, Pasch LA, de Groat CL, et al. Longitudinal effects of parental, child and neighborhood factors on moderate-vigorous physical activity and sedentary time in latino children. Int J Behav Nutr Phys Act. 2014;11:108. https://doi.org/10.1186/s12966-014-0108-x.
Cadogan SL, Keane E, Kearney PM. The effects of individual, family and environmental factors on physical activity levels in children: a cross-sectional study. BMC Pediatr. 2014;14:107. https://doi.org/10.1186/1471-2431-14-107.
Cárdenas-Fuentes G, Homs C, Ramírez-Contreras C, Juton C, Casas-Esteve R, Grau M, et al. Prospective Association of Maternal Educational Level with Child’s physical activity, screen time, and Diet Quality. Nutrients. 2021. https://doi.org/10.3390/nu14010160.
Cvetković N, Nikolić D, Pavlović L, Djordjević N, Golubović M, Stamenković S, Veličković M, THE SOCIO-ECONOMIC STATUS OF PARENTS AND THEIR CHILDREN’S SPORTS ENGAGEMENT. / SOCIO-EKONOMSKI STATUS RODITELJA I UCESCE NJIHOVE DECE U SPORTSKIM AKTIVNOSTIMA. Facta Universitatis: Series Physical Education & Sport. 2014.
da Silva IC, van Hees VT, Ramires VV, Knuth AG, Bielemann RM, Ekelund U, et al. Physical activity levels in three Brazilian birth cohorts as assessed with raw triaxial wrist accelerometry. Int J Epidemiol. 2014;43:1959–68. https://doi.org/10.1093/ije/dyu203.
de Moraes Ferrari GL, Matsudo V, Barreira TV, Tudor-Locke C, Katzmarzyk PT, Fisberg M. Correlates of moderate-to-vigorous physical activity in Brazilian children. J Phys Act Health. 2016;13:1132–45. https://doi.org/10.1123/jpah.2015-0666.
Deng WH, Fredriksen PM. Objectively assessed moderate-to-vigorous physical activity levels among primary school children in Norway: the Health oriented Pedagogical Project (HOPP). Scand J Public Health. 2018;46:38–47. https://doi.org/10.1177/1403494818771207.
Ding D, Mielke GI, Silva ICM, Wehrmeister FC, Horta BL, Brage S, et al. Prenatal and birth predictors of objectively measured physical activity and sedentary time in three population-based birth cohorts in Brazil. Sci Rep. 2020;10:786. https://doi.org/10.1038/s41598-019-57070-x.
Dmitruk A, Popławska H, GÓrniak K, Hołub W. The participation of girls and boys from Ages 10 to 18 in Structured sports and extra-curricular activities in the aspect of Social and Economic conditions. Pol J Sport Tourism. 2015;21:240–6. https://doi.org/10.1515/pjst-2015-0005.
Drenowatz C, Eisenmann JC, Pfeiffer KA, Welk G, Heelan K, Gentile D, Walsh D. Influence of socio-economic status on habitual physical activity and sedentary behavior in 8- to 11-year old children. BMC Public Health. 2010;10:214. https://doi.org/10.1186/1471-2458-10-214.
Duncan MJ, Birch S, Al-Nakeeb Y, Nevill AM. Ambulatory physical activity levels of white and south Asian children in Central England. Acta Paediatr. 2012;101:e156–62. https://doi.org/10.1111/j.1651-2227.2011.02566.x.
Engel-Yeger B. Leisure activities preference of Israeli jewish children from secular versus Orthodox families. Scand J Occup Ther. 2012;19:341–9. https://doi.org/10.3109/11038128.2011.600330.
Fakhouri THI, Hughes JP, Brody DJ, Kit BK, Ogden CL. Physical activity and screen-time viewing among elementary school-aged children in the United States from 2009 to 2010. JAMA Pediatr. 2013;167:223–9. https://doi.org/10.1001/2013.jamapediatrics.122.
Fernández-Alvira JM, Te Velde SJ, Singh A, Jiménez-Pavón D, de Bourdeaudhuij I, Bere E, et al. Parental modeling, education and children’s sports and TV time: the ENERGY-project. Prev Med. 2015;70:96–101. https://doi.org/10.1016/j.ypmed.2014.11.021.
Gomes TN, Hedeker D, Dos Santos FK, Souza M, Santos D, Pereira S, et al. Relationship between Sedentariness and Moderate-to-vigorous physical activity in Youth: a Multivariate Multilevel Study. Int J Environ Res Public Health. 2017. https://doi.org/10.3390/ijerph14020148.
Harbec M-J, Goldfield G, Pagani LS. Healthy body, healthy mind: long-term mutual benefits between classroom and sport engagement in children from ages 6 to 12 years. Prev Med Rep. 2021;24:101581. https://doi.org/10.1016/j.pmedr.2021.101581.
Herzig M, Dössegger A, Mäder U, Kriemler S, Wunderlin T, Grize L, et al. Differences in weight status and energy-balance related behaviors among schoolchildren in german-speaking Switzerland compared to seven countries in Europe. Int J Behav Nutr Phys Act. 2012;9:139. https://doi.org/10.1186/1479-5868-9-139.
Huang S-J, Hung W-C, Sharpe PA, Wai JP. Neighborhood environment and physical activity among urban and rural schoolchildren in Taiwan. Health Place. 2010;16:470–6. https://doi.org/10.1016/j.healthplace.2009.12.004.
Huang WY, Wong SH, Salmon J. Correlates of physical activity and screen-based behaviors in Chinese children. J Sci Med Sport. 2013;16:509–14. https://doi.org/10.1016/j.jsams.2012.12.011.
Janssen I, Lévesque L, Xu F. Correlates of physical activity among First Nations children residing in First Nations communities in Canada. Can J Public Health. 2014;105:e412–7. https://doi.org/10.17269/cjph.105.4526.
Jerina T, Volmut T. Social and demographic factors of physical activity in 9–11 years old Slovenian children. Kinesiol (Zagreb Online). 2018;50:68–78. https://doi.org/10.26582/k.50.1.13.
Jiménez-Pavón D, Fernández-Alvira JM, Te Velde SJ, Brug J, Bere E, Jan N, et al. Associations of parental education and parental physical activity (PA) with children’s PA: the ENERGY cross-sectional study. Prev Med. 2012;55:310–4. https://doi.org/10.1016/j.ypmed.2012.07.011.
Kawalec A, Pawlas K. Familial correlates of Leisure Time activities among Polish Early School-Age children: a cross-sectional study. Int J Environ Res Public Health. 2021. https://doi.org/10.3390/ijerph18073704.
Knuth AG, Silva ICM, van Hees VT, Cordeira K, Matijasevich A, Barros AJD, et al. Objectively-measured physical activity in children is influenced by social indicators rather than biological lifecourse factors: evidence from a Brazilian cohort. Prev Med. 2017;97:40–4. https://doi.org/10.1016/j.ypmed.2016.12.051.
Kobel S, Kettner S, Kesztyüs D, Erkelenz N, Drenowatz C, Steinacker JM. Correlates of habitual physical activity and organized sports in German primary school children. Public Health. 2015;129:237–43. https://doi.org/10.1016/j.puhe.2014.12.002.
Lämmle L, Worth A, Bös K. Socio-demographic correlates of physical activity and physical fitness in German children and adolescents. Eur J Public Health. 2012;22:880–4. https://doi.org/10.1093/eurpub/ckr191.
Larouche R, Mire EF, Belanger K, Barreira TV, Chaput J-P, Fogelholm M, et al. Relationships between Outdoor Time, Physical Activity, Sedentary Time, and body Mass Index in children: a 12-Country study. Pediatr Exerc Sci. 2019;31:118–29. https://doi.org/10.1123/pes.2018-0055.
Larouche R, Blanchette S, Faulkner G, Riazi N, Trudeau F, Tremblay MS. Correlates of children’s physical activity: a Canadian Multisite Study. Med Sci Sports Exerc. 2019;51:2482–90. https://doi.org/10.1249/MSS.0000000000002089.
de Lepeleere S, de Bourdeaudhuij I, Cardon G, Verloigne M. Do specific parenting practices and related parental self-efficacy associate with physical activity and screen time among primary schoolchildren? A cross-sectional study in Belgium. BMJ Open. 2015;5:e007209. https://doi.org/10.1136/bmjopen-2014-007209.
Lewis L, Maher C, Katzmarzyk P, Olds T. Individual and school-level socioeconomic gradients in physical activity in Australian schoolchildren. J Sch Health. 2016;86:105–12. https://doi.org/10.1111/josh.12357.
Love R, Adams J, Atkin A, van Sluijs E. Socioeconomic and ethnic differences in children’s vigorous intensity physical activity: a cross-sectional analysis of the UK Millennium Cohort Study. BMJ Open. 2019;9:e027627. https://doi.org/10.1136/bmjopen-2018-027627.
Manyanga T, Barnes JD, Chaput J-P, Katzmarzyk PT, Prista A, Tremblay MS. Prevalence and correlates of adherence to movement guidelines among urban and rural children in Mozambique: a cross-sectional study. Int J Behav Nutr Phys Act. 2019;16:94. https://doi.org/10.1186/s12966-019-0861-y.
Manz K, Krug S, Schienkiewitz A, Finger JD. Determinants of organised sports participation patterns during the transition from childhood to adolescence in Germany: results of a nationwide cohort study. BMC Public Health. 2016;16:939. https://doi.org/10.1186/s12889-016-3615-7.
Matsudo VKR, Ferrari GLM, Araújo TL, Oliveira LC, Mire E, Barreira TV, et al. Socioeconomic status indicators, physical activity, and overweight/obesity in Brazilian children. Revista Paulista De Pediatria (English Edition). 2016;34:162–70. https://doi.org/10.1016/j.rppede.2015.08.018.
McCormack GR, Giles-Corti B, Timperio A, Wood G, Villanueva K. A cross-sectional study of the individual, social, and built environmental correlates of pedometer-based physical activity among elementary school children. Int J Behav Nutr Phys Act. 2011;8:30. https://doi.org/10.1186/1479-5868-8-30.
McMinn AM, Griffin SJ, Jones AP, van Sluijs EMF. Family and home influences on children’s after-school and weekend physical activity. Eur J Public Health. 2013;23:805–10. https://doi.org/10.1093/eurpub/cks160.
McMinn AM, van Sluijs EMF, Nightingale CM, Griffin SJ, Cook DG, Owen CG, et al. Family and home correlates of children’s physical activity in a multi-ethnic population: the cross-sectional child heart and health study in England (CHASE). Int J Behav Nutr Phys Act. 2011;8:11. https://doi.org/10.1186/1479-5868-8-11.
Moraeus L, Lissner L, Yngve A, Poortvliet E, Al-Ansari U, Sjöberg A. Multi-level influences on childhood obesity in Sweden: societal factors, parental determinants and child’s lifestyle. Int J Obes (Lond). 2012;36:969–76. https://doi.org/10.1038/ijo.2012.79.
Moraeus L, Lissner L, Olsson L, Sjöberg A. Age and time effects on children’s lifestyle and overweight in Sweden. BMC Public Health. 2015;15:355. https://doi.org/10.1186/s12889-015-1635-3.
Muthuri SK, Onywera VO, Tremblay MS, Broyles ST, Chaput J-P, Fogelholm M, et al. Relationships between Parental Education and overweight with childhood overweight and physical activity in 9–11 Year Old children: results from a 12-Country study. PLoS ONE. 2016;11:e0147746. https://doi.org/10.1371/journal.pone.0147746.
Muthuri SK, Wachira L-JM, Onywera VO, Tremblay MS. Correlates of objectively measured overweight/obesity and physical activity in Kenyan school children: results from ISCOLE-Kenya. BMC Public Health. 2014;14:436. https://doi.org/10.1186/1471-2458-14-436.
Noonan RJ, Fairclough SJ. Is there a deprivation and maternal education gradient to child obesity and moderate-to-vigorous physical activity? Findings from the Millennium Cohort Study. Pediatr Obes. 2018;13:458–64. https://doi.org/10.1111/ijpo.12287.
Paduano S, Greco A, Borsari L, Salvia C, Tancredi S, Pinca J, et al. Physical and sedentary activities and childhood Overweight/Obesity: a cross-sectional study among First-Year Children of Primary Schools in Modena, Italy. Int J Environ Res Public Health. 2021. https://doi.org/10.3390/ijerph18063221.
Pate RR, Saunders RP, Taverno Ross SE, Dowda M. Patterns of age-related change in physical activity during the transition from elementary to high school. Prev Med Rep. 2022;26:101712. https://doi.org/10.1016/j.pmedr.2022.101712.
Pouliou T, Sera F, Griffiths L, Joshi H, Geraci M, Cortina-Borja M, Law C. Environmental influences on children’s physical activity. J Epidemiol Community Health. 2015;69:77–85. https://doi.org/10.1136/jech-2014-204287.
Rosell M, Carlander A, Cassel S, Henriksson P, J-Son Höök M, Löf M. Generation pep study: a population-based survey on diet and physical activity in 12,000 Swedish children and adolescents. Acta Paediatr. 2021;110:2597–606. https://doi.org/10.1111/apa.15850.
Sanmarchi F, Esposito F, Marini S, Masini A, Scrimaglia S, Capodici A, et al. Children’s and families’ determinants of Health-related behaviors in an Italian primary school sample: the seven days for my Health Project. Int J Environ Res Public Health. 2022. https://doi.org/10.3390/ijerph19010460.
Schmidt SCE, Burchartz A, Kolb S, Niessner C, Oriwol D, Woll A. Influence of socioeconomic variables on physical activity and screen time of children and adolescents during the COVID–19 lockdown in Germany: the MoMo study. Ger J Exerc Sport Res. 2022;52:362–73. https://doi.org/10.1007/s12662-021-00783-x.
Smith NR, Lewis DJ, Fahy A, Eldridge S, Taylor SJC, Moore DG, et al. Individual socio-demographic factors and perceptions of the environment as determinants of inequalities in adolescent physical and psychological health: the olympic regeneration in East London (ORiEL) study. BMC Public Health. 2015;15:150. https://doi.org/10.1186/s12889-015-1459-1.
Tandon P, Grow HM, Couch S, Glanz K, Sallis JF, Frank LD, Saelens BE. Physical and social home environment in relation to children’s overall and home-based physical activity and sedentary time. Prev Med. 2014;66:39–44. https://doi.org/10.1016/j.ypmed.2014.05.019.
Tandon PS, Zhou C, Sallis JF, Cain KL, Frank LD, Saelens BE. Home environment relationships with children’s physical activity, sedentary time, and screen time by socioeconomic status. Int J Behav Nutr Phys Act. 2012;9:88. https://doi.org/10.1186/1479-5868-9-88.
Tercedor P, Segura-Jiménez V, Ávila García M, Huertas-Delgado FJ. Physical activity during school recess: a missed opportunity to be active? Health Educ J. 2019;78:988–99. https://doi.org/10.1177/0017896919859044.
To QG, Gallegos D, Do DV, Tran HT, To KG, Wharton L, Trost SG. Correlates of physical activity in fifth-grade students in Ho Chi Minh City, Vietnam. Sports Med Health Sci. 2020;2:33–7. https://doi.org/10.1016/j.smhs.2020.02.002.
van Stralen MM, Yıldırım M, Wulp A, Te Velde SJ, Verloigne M, Doessegger A, et al. Measured sedentary time and physical activity during the school day of European 10- to 12-year-old children: the ENERGY project. J Sci Med Sport. 2014;17:201–6. https://doi.org/10.1016/j.jsams.2013.04.019.
Vandendriessche JB, Vandorpe BFR, Vaeyens R, Malina RM, Lefevre J, Lenoir M, Philippaerts RM. Variation in sport participation, fitness and motor coordination with socioeconomic status among flemish children. Pediatr Exerc Sci. 2012;24:113–28. https://doi.org/10.1123/pes.24.1.113.
Vandermeerschen H, Vos S, Scheerder J. Who’s joining the club? Participation of socially vulnerable children and adolescents in club-organised sports. Sport Educ Soc. 2015;20:941–58. https://doi.org/10.1080/13573322.2013.856293.
Veitch J, Salmon J, Ball K. Individual, social and physical environmental correlates of children’s active free-play: a cross-sectional study. Int J Behav Nutr Phys Act. 2010;7:11. https://doi.org/10.1186/1479-5868-7-11.
White P, McTeer W. Sociol Sport J. 2012;29:186–209. https://doi.org/10.1123/ssj.29.2.186. Socioeconomic Status and Sport Participation at Different Developmental Stages During Childhood and Youth: Multivariate Analyses Using Canadian National Survey Data.
Wijtzes AI, Jansen W, Bouthoorn SH, Pot N, Hofman A, Jaddoe VWV, Raat H. Social inequalities in young children’s sports participation and outdoor play. Int J Behav Nutr Phys Act. 2014;11:155. https://doi.org/10.1186/s12966-014-0155-3.
Wilk P, Clark AF, Maltby A, Smith C, Tucker P, Gilliland JA. Examining individual, interpersonal, and environmental influences on children’s physical activity levels. SSM Popul Health. 2018;4:76–85. https://doi.org/10.1016/j.ssmph.2017.11.004.
Wilkie HJ, Standage M, Gillison FB, Cumming SP, Katzmarzyk PT. The home electronic media environment and parental safety concerns: relationships with outdoor time after school and over the weekend among 9–11 year old children. BMC Public Health. 2018;18:456. https://doi.org/10.1186/s12889-018-5382-0.
Acknowledgements
Not applicable.
Funding
Open Access funding enabled and organized by Projekt DEAL. Supported by the Open Access Publishing Fund of Leipzig University.
Open Access funding enabled and organized by Projekt DEAL.
Author information
Authors and Affiliations
Contributions
AZ: Conception of the research protocol, literature review, data extraction, data analysis, interpretation and drafting of the manuscript. DS: literature review, data extraction, data analysis, interpretation and drafting of the manuscript. AF: literature review and data extraction. KB: literature review and data extraction. HW: reviewing the manuscript and quality assessment. All authors reviewed the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Ziegeldorf, A., Schoene, D., Fatum, A. et al. Associations of family socioeconomic indicators and physical activity of primary school-aged children: a systematic review. BMC Public Health 24, 2247 (2024). https://doi.org/10.1186/s12889-024-19174-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12889-024-19174-6