
Abstract
Objective
Benzene, ethylbenzene, meta/para-xylene, and ortho-xylene, collectively referred to as benzene, ethylbenzene, and xylene (BEX), constitute the main components of volatile organic aromatic compounds (VOACs) and can have adverse effects on human health. The relationship between exposure to BEX and hearing loss (HL) in the adult U.S. population was aimed to be assessed.
Methods
Cross-sectional data from the National Health and Nutrition Examination Survey (NHANES) for the years 2003–2004, 2011–2012, and 2015–2016 were analyzed. This dataset included complete demographic characteristics, pure-tone audiometry measurements, and volatile organic compound detection data from the NHANES database. A weighted multivariate logistic regression model was employed to investigate the associations between blood BEX concentrations HL, low-frequency hearing loss (SFHL), and high-frequency hearing loss (HFHL).
Results
2174 participants were included, with weighted prevalence rates of HL, SFHL, and HFHL being 46.81%, 25.23%, and 45.86%, respectively. Exposure to benzene, ethylbenzene, meta/para-xylene, and ortho-xylene, and cumulative BEX concentrations increased the risk of hearing loss (odds ratios [ORs] were 1.36, 1.22, 1.42, 1.23, and 1.31, respectively; all P < 0.05). In the analysis with SFHL as the outcome, ethylbenzene, m-/p-xylene, o-xylene, benzene, and overall BEX increased the risk (OR 1.26, 1.21, 1.28, 1.20, and 1.25, respectively; all P < 0.05). For HFHL, exposure to ethylbenzene, m-/p-xylene, o-xylene, benzene, and overall BEX increased the risk (OR 1.36, 1.22, 1.42, 1.22, and 1.31, respectively; all P < 0.05).
Conclusion
Our study indicated that a positive correlation between individual or cumulative exposure to benzene, ethylbenzene, meta/para-xylene, and ortho-xylene and the risk of HL, SFHL, and HFHL. Further research is imperative to acquire a more comprehensive understanding of the mechanisms by which organic compounds, notably BEX, in causing hearing loss and to validate these findings in longitudinal environmental studies.
Similar content being viewed by others


Introduction
According to the 2021 World Health Organization’s World Hearing Report, nearly one-quarter of the global population will experience varying degrees of hearing loss by 2025, resulting in an estimated economic loss of 980 billion USD [1]. This financial burden is accompanied by increased risks of conditions like Alzheimer’s disease and dementia in individuals with age-related hearing loss [2, 3]. Additionally, individuals with hearing loss often face communication difficulties that lead to linguistic degradation, reduced social engagement, social isolation, emotional detachment, and depression [4, 5]. Among the factors contributing to hearing loss, ototoxic mechanisms have been a central focus, with clinical research primarily centered around the adverse effects of platinum-based drugs and aminoglycosides [6, 7]. Some pioneers have investigated the effects of trace heavy metals (such as lead and cadmium), ingested and accumulated by humans, on hearing loss, revealing the stress-induced damage and toxic effects of these metals on cochlear hair cells [8,9,10]. However relationship between accumulated environmental pollutants in human blood and hearing loss has not yet been thoroughly researched.
Benzene, ethylbenzene, meta/para-xylene (m-/p-xylene), and ortho-xylene (o-xylene) (collectively referred to as Benzene, Ethylbenzene, and Xylene or BEX) are aromatic compounds containing benzene rings that exhibit strong volatility at room temperature, making them prominent pollutants within the group of volatile organic aromatic compounds (VOACs). BEX originates from various sources, primarily including gas emissions resulting from the combustion of petroleum products, chemical solvents, paints, and other building materials. BEX is recognized as a carcinogen by the International Agency for Research on Cancer, and prolonged exposure to BEX has been demonstrated to disrupt reproductive function, induce asthma, and lead to leukemia [11,12,13]. Accumulation of BEX in the human body can occur through inhalation, ingestion of contaminated water sources, and subsequent dissolution in the bloodstream, thereby spreading to various organs and tissues. This has raised public concerns regarding the potential life and health threats posed by BEX. In recent years, BEX has been implicated in the discovery of additional potential health issues. For instance, benzene poisoning has been linked to immune suppression and splenic damage through the B-cell receptor signaling pathway [14]. Partha et al. demonstrated through epidemiological research that BEX exposure contributes to premature birth in pregnant women [15].
Observational studies also have found a positive correlation between the occupational workers’ urinary biomarkers of toluene, such as hippuric acid and ortho-cresol, and toxicity to the auditory system [16, 17]. Wenzhen Li et al. pointed out that the concentration of polycyclic aromatic hydrocarbons (PAHs) in urine is related to various frequencies of hearing loss across different age groups [18]. However, most solvents have a short biological half-life, and varying degrees of metabolism, and a small amount of the solvent is excreted in the urine in metabolized forms [19]. Therefore, using organic solvents in urine as biomarkers for hearing loss has certain limitations. Considering this limitation, the focus of this study has shifted towards a comprehensive exploration of the relationship between blood BEX concentrations and hearing loss in the general population. Through this research, we hope to provide a more comprehensive understanding of the association between environmental factors and auditory health.
Methods
Study population
Given that the National Health and Nutrition Examination Survey (NHANES)working group collected auditory data from adults in the following three cycles: 2003–2004, 2011–2012, and 2015–2016, our study incorporates the aforementioned three cycles for investigation. We excluded participants aged < 20 years (n = 13,529) and participants aged > 60 years (n = 5250). In this study, we initially recruited participants for the measurement of benzene, ethylbenzene, o-xylene, and m/p-xylene, resulting in the exclusion of participants with missing data for these four volatile organic compound concentrations (VOACs) (n = 948). Participants with missing data for family income-poverty ratio (n = 189), lack of marital status (n = 2), self-reported cerumen or collapsing external ear canals (n = 612), wearing hearing aids (n = 17), and suffering from Parkinson’s (n = 13) were further excluded.
According to previous studies [20], NHANES recorded objective indicators of Eustachian Tube Dysfunction (ETD), specifically the middle ear pressures in participants’ left and right ears (measured in daPa units). Based on the standard tympanogram classifications by Linden11 and Jerger1, we defined peak middle ear pressures below 99 daPa as type C, middle ear pressures with compliance values of 0.2 as type B, and all other middle ear pressures as type A. If a participant had tympanometric type B or C in either or both ears, they were categorized as abnormal and excluded from the analysis (n = 264).
To exclude the possibility of drug-induced hearing loss, we extracted information on participants’ prescription medication use from the Prescription Medication Section (DSQ) of NHANES. Upon matching, the types of medications taken by participants were primarily focused on treating conditions such as diabetes, hypertension, infections, and hyperlipidemia, among others. As detailed information regarding participants’ medication, including dosage, duration, administration method, and brand was unavailable, we relied on clinical drug experience and existing literature evidence to primarily define participants taking the following 11 drugs (acetaminophen [21], hydrocodone [22], ciprofloxacin [23], phenytoin [24], levofloxacin [25], rifampin [26], minocycline [27], aspirin [28], metronidazole [29], nitroglycerin [30], and bumetanide [31]) as a high-risk group for drug-induced hearing loss and subsequently excluded them from the study (n = 46).
Ultimately, a total of 2174 participants were included for analysis (Fig. 1). The NHANES study protocol was approved by the Institutional Review Board of the National Center for Health Statistics. All participants provided informed consent.

Flow chart of the patients included in the study
Blood aromatic volatile organic compounds determination
Participants arrived at a central location consisting of Mobile Examination Centers (MEC), where blood samples were collected. Analysis of the blood samples was performed using automated methods employing capillary gas chromatography (GC) and mass spectrometry (MS) combined with selected ion monitoring (SIM) detection and isotope dilution techniques. This analytical method was established to quantify VOACs in the blood of non-occupationally exposed individuals within this range, making it suitable for identifying cases with these levels of exposure over a sustained or recent period of low-level exposure.
Audiometric measures and hearing loss
All sections of the audiometry exam were conducted by trained examiners on participants in a dedicated sound-isolating room at the MEC. Hearing threshold testing was performed on both ears of participants at seven frequencies: 500, 1000, 2000, 3000, 4000, 6000, and 8000 Hz. Hearing loss was characterized by pure-tone averages surpassing 25 dB in both ears among adults. Individuals were classified as having hearing loss if their hearing thresholds exceeded 25 dB in either ear across any of the examined frequencies. (500, 1000, 2000, 3000, 4000, 6000, and 8000 Hz) [32, 33].
Moreover, the research delved into the examination of two distinct categories of auditory impairment, encompassing Speech Frequency Hearing Loss (SFHL) and High-Frequency Hearing Loss (HFHL), which do not exhibit a mutually exclusive relationship. The assessments for SFHL were conducted at frequencies of 500, 1000, 2000, and 4000 Hz, while the evaluations for HFHL were performed at 3000, 4000, 6000, and 8000 Hz [34, 35].
Ascertainment of covariates
Demographic particulars, encompassing age, sex, racial/ethnic background, and marital status, were garnered through a universally recognized questionnaire. Height, gauged in meters, and weight, measured in kilograms, were acquired following a stipulated protocol, subsequently utilized in the computation of body mass index (BMI), denoted in kilograms per square meter. Then the participants could be further separated into three subgroups, normal weight (BMI < 25 kg/m2), overweight (25 kg/m2 ≤ BMI < 30 kg/m2), and obese (BMI ≥ 30 kg/m2) [36]. Education level was categorized as below high school, high school or higher, and college or higher. Smoking status was classified as non-smoking (less than 100 lifetime cigarettes) and smoking (more than 100-lifetime cigarettes) [10]. Drinking status were categorized into two groups: those who consumed alcohol (a minimum of 12 beverages annually) and those who abstained from alcohol [37]. Hypertension was defined as self-reported physician diagnosis or current use of antihypertensive medication. Diabetes was defined as self-reported physician diagnosis or current use of antihyperglycemic medication. Ascertaining household income levels was accomplished through the utilization of the self-reported family income-poverty ratio (PIR), which was subsequently categorized into three distinct groups (0–1.3, 1.3–3.5, and > 3.5) [38]. The participant selection process was conducted in the aforementioned order.
In the NHANES cycles of 2003–2004, the questionnaire design related to hearing tests differs from the surveys conducted in 2011–2012 and 2015–2016. In the absence of questions regarding occupational noise exposure in the hearing questionnaire of the 2003–2004 cycle, according to the NHANES guidance manual, information on occupational noise exposure was obtained from the Occupation Section of the SP Household Questionnaire (OCQ). Therefore, in our study, occupational noise exposure is defined as “currently exposed to loud noise at work for an average of ≥ 4 hours/day” or “presence of noisy work conditions: ever exposed, 3 months or more.” Firearm noise exposure is defined as “presence of firearm noise exposure outside of work.” Recreational noise exposure is defined as “presence of other types of noise exposure, such as loud music, outside of work” [39].
For participants in the 2011–2012 and 2015–2016 cycles, occupational noise exposure is defined as “ever exposed to noisy work conditions for 4 hours or longer, several days a week.” Firearm noise exposure is defined as “use of firearms for any reason.” Recreational noise exposure is defined as “exposure to very loud noise or music for 10 hours or longer per week outside of work” [40].
Statistical analysis
NHANES formulates survey-specific weighting factors to accommodate intricate survey structure, non-participation, and post-stratification, thereby guaranteeing that the derived estimations accurately portray the demographic composition of the non-institutionalized civilian populace in the United States. Regarding the measurement of volatile organic compounds in blood, BEX’s data are weighted using the corresponding subsample weight (WTSVOC2Y) for each cycle. NHANES data is collected in cycles of two years each, and since our data spans three cycles, the weight for each cycle is calculated as 2/6 * WTSVOC2Y to account for the proportional representation of each cycle. The statistical analysis was performed according to the guidelines provided in the NHANES data documentation [41].
Due to the skewed distribution of blood VOACs data, we performed a logarithmic transformation of BEX for our analysis. When describing the baseline characteristics of the study population, the data are presented as weighted means ± standard errors (SD) for continuous measurements, and as unweighted counts along with weighted percentages for categorical measurements. For continuous variables, statistical significance was assessed using Student’s t test. Similarly, for categorical variables, P-values were determined through the utilization of chi-square tests.
Weighted logistic regression, we addressed the intricacies of the survey design elements within the statistical analysis. To comprehend the potential confounding influences of diverse covariates, we systematically introduced adjustments across two successive models. Model 1 adjusted for age (continuous years), BMI, sex, race (non-Hispanic white, non-Hispanic black, Mexican American, etc.). Model 2 adjusted for variables in Model 1 plus education level (below high school, high school or equivalent, college or higher), marital status (married, separated including widowed and divorced groups, unmarried), smoking status (no, yes), drinking status (no, yes), hypertension (no, yes), diabetes (no, yes), and PIR levels (0–1.3, 1.3–3.5, and > 3.5).
In order to assess the robustness of the identified associations, we conducted three sensitivity analyses. Firstly, in the latest edition (2021) of “The World Report on Hearing” by the WHO), new recommendations for hearing classification have been proposed, introducing updated criteria for grading hearing loss [42]. Accordingly, we have reclassified participants into three levels based on the average hearing threshold (PTA): normal (< 20 dB), mild (20–35 dB), and moderate to severe (> 35 dB). Subsequently, we employed weighted ordered logistic regression analysis to investigate the relationship between BEX and varying degrees of hearing loss. Secondly, to mitigate the impact of age, participants aged > 40 were excluded, and a weighted logistic regression analysis was subsequently conducted. Lastly, given that one of the significant sources of VOCs is cigarette smoke, and previous studies have identified environmental tobacco smoke (ETS) exposure as a risk factor for hearing loss [43], we extracted biochemical test results for ‘serum cotinine’ from NHANES. Serum cotinine serves as a biomarker to quantify tobacco smoke exposure, and individuals with serum cotinine > 0.015 ng/mL are considered acutely exposed to ETS [44]. This variable was included as a control in the model for weighted logistic regression analysis.
As part of our analysis, we conducted subgroup analyses based on gender (male and female), age (20–40 years and 40–60 years), BMI categories (< 25, 25-29.9, and ≥ 30 kg/m2), smoking status (no and yes), diabetes (no and yes), hypertension (no and yes), education levels (below high school, high school or higher, and college or higher), and PIR (0–1.3, 1.3–3.5, and > 3.5) were subjects of investigation. Furthermore, potential effect variations were explored by introducing a product term for each stratifying variable and BEX into the primary model, followed by evaluation through a Wald test.
The dose-response relationship between VOACs and the occurrence of hearing loss was examined using Restricted Cubic Splines with three knots positioned at the 1th, 50th, and 90th percentiles. Advanced statistical analyses were carried out utilizing STATA version 17.0 and R version 4.3.1. Significance was determined when the two-tailed P-value fell below 0.05.
Results
Basic characteristics
Over the span of three NHANES cycles, encompassing the years 2003–2004, 2011–2012, and 2015–2016, a cumulative participant cohort of 29,849 individuals was included. After eliminating individuals below the age of 20 and those surpassing 60 years, lack of blood organics measurement information and hearing measurement information, cerumen embolism and collapse of the external auditory canal, lack of marriage information, and insufficient household income, 2174 participants were finally included in the analysis. The participants exhibited an average age of 39.20 years. Among the participants, there were a total of 995 instances of hearing loss, with 513 cases categorized as SFHL and 973 cases as HFHL. Additionally, 491 participants demonstrated the concurrent occurrence of two distinct types of hearing loss. The sample included in this study is representative of a weighted population of 77,433,612 noninstitutionalized U.S. adults.
Table 1 presents the characteristics of participants based on the presence or absence of hearing loss, SFHL, and HFHL. In our study population, the weighted prevalence of hearing loss was 46.81%, low-frequency hearing loss was 25.23%, and high-frequency hearing loss was 45.86%. Apart from race, alcohol drinking history, exposure to recreational noise, exposure to firearm noise, and PIR, no significant differences were observed among the groups in terms of these characteristics. However, statistically significant differences were noted in other baseline characteristics. Compared to participants without hearing loss, those with higher age, BMI, male, education level of High school or equivalent, marital status, history of smoking, alcohol consumption, hypertension, exposure to work noise, and diabetes had a higher prevalence of hearing loss. These associations remained consistent for both low-frequency and high-frequency hearing loss. Detailed characteristics of the study population are provided in Supplementary Tables 1–2.
Associations between BEX and HL
To investigate potential associations between hearing loss and blood BEX levels, we conducted weighted logistic regression analyses (Table 2). In the analysis with hearing loss as the outcome, exposure to ethylbenzene, m-/p-xylene, o-xylene, benzene, and overall BEX increased the risk of occurrence (OR 1.36, 1.22, 1.42, 1.23, and 1.31, respectively; all P < 0.05). In the analysis with SFHL as the outcome, ethylbenzene, m-/p-xylene, o-xylene, benzene, and overall BEX increased the risk (OR 1.26, 1.21, 1.28, 1.20, and 1.25, respectively; all P < 0.05). For HFHL, exposure to ethylbenzene, m-/p-xylene, o-xylene, benzene, and overall BEX increased the risk (OR 1.36, 1.22, 1.42, 1.22, and 1.31, respectively; all P < 0.05).
Table 3 presents the results of the multivariate weighted ordered logistic regression between BEX and different degrees of hearing loss. The results indicate a positive correlation between the severity of hearing loss and the concentration of BEX and its components. Interestingly, such a relationship was observed only in HL and HFHL; in SFHL, there was no association between the severity of hearing loss and the concentration of BEX and its components. Supplementary Tables 3–4 summarize the results of the second and third sensitivity analyses, revealing that the impact of BEX and its components on hearing loss remains robust.
Subgroup analyses
Figure 2 illustrates a subgroup analysis of BEX based on gender, age, BMI, smoking status, diabetes, hypertension, education level, and PIR. No significant differences were observed among the various components. Additionally, Supplementary Figs. 1–4 present subgroup analysis results for Ethylbenzene, M-/P-Xylene, O-Xylene, and Benzene, respectively. No significant differences were found among the components in these subanalyses. Refer to the supplementary figures for detailed results.

Association between log-transformed creatinine-corrected BEX and hearing loss in subgroups. Models were adjusted for age (20–40 and 40–60 years), sex (male and female), BMI categories (< 25, 25-29.9, and ≥ 30 kg/m2), education levels (less than high school, high school, and college or above), race/ethnicity (Mexican American, Other Hispanic, Non-Hispanic White Non-Hispanic Black, Other Race - Including Multi-Racial), marital status (married, widowed, divorced, separated, never married, living with partner), PIR (< 1.3, 1.3–3.5, > 3.5), smoking status (no and yes), drinking status(no and yes), diabetes (no and yes), hypertension (no and yes), work noise (no and yes), recreational noise (no and yes), firearm noise(no and yes), and year cycle (2003–2004, 2011–2012, and 2015–2016). P values for interaction were estimated by adding a product term of each stratifying variable and BEX in the main model and assessing it via a Wald test. Abbreviations: BMI, body mass index; CI, confidence interval; OR, odds ratio; PIR, family income-poverty ratio
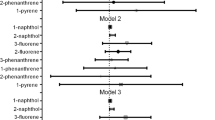
The cubic spline of the association between log-transformed volume-based BEX and risk of hearing loss
In accordance with the fully adjusted model, we employed a constrained cubic spline method to investigate the dose-response relationship between the concentrations of BEX and its components and the incidence of hearing loss (refer to Fig. 3). The outcomes illuminate a linear correlation between the logarithmic concentration of BEX and the susceptibility to hearing loss (P-linear-value < 0.05). Furthermore, upon stratification by distinct age groups, genders, and BMI categories, the dose-response relationship suggests a comparatively higher risk among individuals of older age, female gender, and those with normal weight. Notably, no evidence of a nonlinear correlation was observed between the logarithmically transformed concentrations of ethylbenzene, ortho-xylene, meta/para-xylene, benzene, and hearing loss (P-linear-value < 0.05; Supplementary Figs. 5–8).

The cubic spline of the association between log-transformed volume-based BEX and risk of hearing loss. (A) BEX and HL; (B) BEX and HL stratified by age; (C) BEX and HL stratified by sex; (D) BEX and HL stratified by BMI. Models were adjusted for age (continuous, years), sex (male and female), BMI (continuous, kg/m2), education levels (less than high school, high school and college or higher), race/ethnicity (Mexican American, Other Hispanic, Non-Hispanic White Non-Hispanic Black, Other Race - Including Multi-Racial), marital status (married, widowed, divorced, separated, never married, living with partner), PIR (< 1.3, 1.3–3.5, > 3.5), smoking status (no and yes), drinking status(no and yes), diabetes (no and yes), hypertension (no and yes), work noise(no and yes), recreational noise(no and yes), firearm noise(no and yes), and year cycle (2003–2004, 2011–2012, and 2015–2016). Knots = 3. Abbreviations: BMI, body mass index; PIR, family income-poverty ratio
Discussion
In this study targeting US adults, we observed a positive correlation between concentrations of volatile organic compounds, including benzene, ethylbenzene, o-xylene, and m/p-xylene, in blood samples from diverse populations and various types of hearing loss in American adults, including overall hearing loss, low-frequency hearing loss, and high-frequency hearing loss.
Currently, effective treatments for hearing loss remain limited, emphasizing the significance of primary prevention to mitigate and reduce risk factors. Multiple studies, conducted through both animal experimentation and epidemiological research, have explored the potential correlation between BEX exposure and hearing loss. In rat animal models, exposure to ethylbenzene induces apoptosis in cochlear precursor cells, inhibits cell proliferation, and alters mitochondrial membrane potential, affecting hearing. Additionally, combined exposure to toluene and ethylbenzene leads to enhanced outer hair cell death, resulting in auditory function loss [45, 46]. Previous investigations have explored the occupational risks of toluene, ethylbenzene, xylene, and styrene (TEXS) exposure concerning hearing loss among petrochemical workers [47]. Other studies have found an association between organic solvents (benzene, toluene, and xylene) and the incidence of high-frequency hearing loss [48]. However, each of these studies has certain limitations. Some are confined to occupational cohorts, others focus solely on individual component impacts, while some solely concentrate on the overall effects of TEXS. This study further reveals that exposure to BEX in the bloodstream is associated with an elevated risk of hearing loss, impacting both speech frequency and high-frequency auditory function.
The organ of the Corti, situated within the cochlea, serves as the central hub for encoding electrical signals in the auditory system. The Organ of Corti’s is quite a complex one. During sound-induced hearing, vibrations from the stapes are propagated by the traveling wave phenomenon to the different spectral components’ tonotopic locations along the basilar membrane (BM). The traveling wave derives from the interaction between the basilar membrane elastic structure and the fluid differential pressure developed between the scala vestibuli and the scala Tympani. The true mechano-electrical transduction happens at the level of the inner hair cells (IHC), in which the signal is conveyed to the spiral ganglion. The outer hair cells (OHC) are responsible for the amplification of the mechanical vibration of the basilar membrane at low stimulus levels. The somato-elasticity of the OHC provides an electromechanical stage of amplification. The transmembrane potential of the OHC is triggered by the hair bundle displacement against the tectorial membrane. This mechanism provides a mechano-electrical piezoelectric stage. Due to this complexity in the sound transduction the interplay among hair cells, both inner hair cells and outer hair cells, vascular structures, and the spiral ganglion neurons is indispensable to formulate hypotheses about the BEX–cochlea interaction in inducing hearing loss. Notably, exposure to ethylbenzene in mice was observed to hinder the Wnt/β-catenin signaling pathway, leading to mitochondrial abnormalities in cochlear progenitor cells, resulting in excessive apoptosis and contributing indirectly to hearing loss [49]. Moreover, ethylbenzene exposure has been linked to altered neurotransmitter profiles and hearing loss [50]. The α9/α10 nicotinic acetylcholine receptors, predominantly expressed in the mammalian cochlea, mediate synaptic transmission between hair cells and spiral ganglion neurons [51]. At low concentrations, both ethylbenzene and m-xylene (10 µM) inhibit the opening of α9/α10 nAChR ion channels, affecting synaptic signal transmission and resulting in auditory impairment [52]. A study exploring the toxicity of aromatic solvents on the organ of Corti revealed that ethylbenzene exhibited more pronounced cytotoxicity than o-xylene, inducing damage to both outer hair cells and first-row inner hair cells [53].
Not all components of BEX have been thoroughly studied for their impact on hearing loss. Studies investigating the effects of benzene and the three isomers of xylene on hearing loss in rats have found that only m-/p-xylene has ototoxic effects on hair cells [54, 55]. However, our research indicates that both benzene and ortho/meta-xylene have an impact on human hearing loss. Literature review reveals that ortho/meta-xylene can induce ear edema, oxidative stress, and inflammation, while also causing constriction or damage to vascular endothelium, and para-xylene can reduce potassium ion concentration in lymph fluid [56, 57]. These factors could potentially hinder blood supply to the cochlea or lymphatic reflux, ultimately leading to dysfunction of the cochlear organ. Although there is no explicit experimental evidence of the ototoxic effects of benzene, prolonged exposure to low doses of benzene can activate cellular oxidative stress, which may contribute to hearing loss [58]. Furthermore, the animal models used for studying ortho/meta-xylene and benzene may have species-specific variations. Further research is necessary to elucidate the specific mechanisms underlying hearing loss associated with the isomers of benzene and xylene.
It is noteworthy that the restricted cubic spline plots reveal a higher risk in the 40–60 age group compared to the 20–40 age group. This contradicts the results of subgroup analysis, and some factors contributing to this discrepancy can be partly explained by the design of our study and the relatively small sample size. Age and other demographic factors (gender, race/ethnicity, educational level) are important influencing factors contributing to hearing impairment [59]. Therefore, potential factor could be the ongoing increase in the contribution of exposure to other environmental risk factors, such as cadmium, lead, and other heavy metals, which may continuously augment the impact of BEX that we have been investigating on hearing loss [10]. Furthermore, there exists the possibility of heterogeneity introduced by our definition of hearing loss (> 25dB) in the 20–60 age group. However, this definition of hearing loss (> 25dB) still applies in numerous age-related studies of hearing loss, particularly in the speech frequency range [59,60,61]. To better address this heterogeneity, we conducted sensitivity analyses. Our results remained robust even after excluding individuals over the age of 40, redefining hearing loss, and controlling for serum exposure to cotinine. In conclusion, future studies necessitate more samples, longer follow-up periods, and foundational experiments to explore the relationship between age, BEX, and hearing loss.
Additionally, individuals with obesity exhibit a lower risk from BEX compared to those with normal weight, while females are more susceptible than males. These two phenomena might be attributed to Insulin-like Growth Factor 1 (IGF-1). Studies suggest that IGF-1, acting as a neurotrophic factor, can enhance the antioxidant response of cochlear hair cells via the IGF1R/AKT pathway, thus protecting auditory cells from oxidative stress and cell apoptosis [62]. For obese patients, the secretion of IGF-1 is complex and subject to controversy. Some studies suggest that free IGF-1 increases during obesity and promotes the expression of IGFR (Insulin-like Growth Factor Receptor). However, obese individuals with metabolic disturbances and associated complications tend to have lower levels of free IGF-1 than the absolute levels would suggest [63, 64]. This phenomenon might be related to the RCS (restricted cubic spline) curve we derived, indicating that higher levels of IGF-1 and IGFR could result in a lower risk of hearing loss induced by BEX in obese individuals compared to normal-weight individuals. However, overweight patients might experience a partial failure of protective factors due to a more disrupted endocrine system, leading to a risk lying between that of normal-weight individuals and obese patients. This speculation is based on our analysis of the research results. As it is a cross-sectional study, further experiments may be necessary to ascertain whether obesity can indeed prevent hearing loss. Abdel Halim Harrath and colleagues’ research indicates that exposure to benzene and ethylbenzene can significantly decrease the levels of IGF-1 in female rats, while also increasing the secretion of estrogen and progesterone [13]. Therefore, the difference in risk between men and women may not be limited solely to IGF-1, but also associated with sex hormones. Estrogen and progesterone are primarily secreted by the ovaries in female individuals, and in addition to their role in reproductive system maintenance, they also exert protective effects on the auditory system. Estrogen receptors are widely distributed in the cochlea and vascular endothelium, promoting vascular growth and safeguarding against hearing loss [65, 66]. Nevertheless, studies by Kassotis and colleagues have reported antagonistic activity of BEX on estrogen receptors [67]. Prolonged combined stimulation of estrogen and progesterone in females can elevate hearing thresholds, leading to negative impacts on hearing [68]. Additionally, expression of aquaporin 5, a water channel protein in the cochlea, can be influenced by uterine estrogen, promoting the movement of cellular fluid to interstitial tissue, thus causing water and sodium retention effects that could result in cochlear vascular microcirculation or lymphatic congestion, ultimately affecting hearing [69]. Therefore, we hypothesize that BEX may contribute to the disruption of the female endocrine system. Although compensatory increases in estrogen may occur, the negative effects resulting from estrogen imbalance far outweigh its protective benefits.
Our study possesses several strengths: benzene, ethylbenzene, m-/p-xylene, and o-xylene, as major components of volatile organic compounds in human blood, are positively associated with hearing loss in the adult population of the United States. Consistent conclusions were also observed for both low-frequency and high-frequency hearing loss. Future research should delve deeper into the mechanisms of organic compounds, especially BEX, in causing hearing loss, to validate these findings longitudinally within the environmental context. Nevertheless, our study has inherent limitations. First, its cross-sectional nature restricts the ability to infer causality between exposure and outcomes. Additionally, the measurement of volatile organic compounds in the blood is temporary and may not represent long-term BEX exposure levels. Lastly, our study focuses on BEX exposure and does not account for the potential effects of other hazardous substances.
Conclusions
Our study indicated a positive correlation between individual or cumulative exposure to benzene, ethylbenzene, meta/para-xylene, and ortho-xylene and the risk of HL, SFHL, and HFHL. Further research is imperative to acquire a more comprehensive understanding of the mechanisms by which organic compounds, notably BEX, cause hearing loss and to validate these findings in longitudinal environmental studies.
Data availability
Data described in the manuscript are publicly and freely available without restriction at: https://www.cdc.gov/nchs/nhanes/index.htm.
References
World report on. hearing [Licence: CCBY-NC-SA 3.0 IGO].
Omura JD, McGuire LC, Patel R, Baumgart M, Lamb R, Jeffers EM, Olivari BS, Croft JB, Thomas CW, Hacker K. Modifiable risk factors for Alzheimer Disease and related dementias among adults aged ≥ 45 years - United States, 2019. MMWR Morbidity Mortal Wkly Rep. 2022;71(20):680–5.
Huang AR, Jiang K, Lin FR, Deal JA, Reed NS. Hearing loss and dementia prevalence in older adults in the US. JAMA. 2023;329(2):171–3.
LeClair KL, Saunders JE. Meeting the educational needs of children with hearing loss. Bull World Health Organ. 2019;97(10):722–4.
Cao X, Liu Q, Liu J, Yang B, Zhou J. The impact of hearing loss on cognitive impairment: the mediating role of depressive symptoms and the moderating role of social relationships. Front Public Health. 2023;11:1149769.
Cheng C, Ma J, Lu X, Zhang P, Wang X, Guo L, Li P, Wei Y, Li GL, Gao X, et al. P2X7 receptor is required for the ototoxicity caused by aminoglycoside in developing cochlear hair cells. Neurobiol Dis. 2023;183:106176.
Sanchez VA, Shuey MM, Dinh PC Jr., Monahan PO, Fosså SD, Sesso HD, Dolan ME, Einhorn LH, Vaughn DJ, Martin NE, et al. Patient-reported functional impairment due to hearing loss and Tinnitus after cisplatin-based chemotherapy. J Clin Oncol. 2023;41(12):2211–26.
Schmid C, Alampi I, Briggs J, Tarcza K, Stawicki TM. Mechanotransduction activity facilitates hair cell toxicity caused by the Heavy Metal Cadmium. Front Cell Neurosci. 2020;14:37.
Schaal N, Slagley J, Zreiqat M, Paschold H. Effects of combined exposure to metals, solvents, and noise on permanent threshold shifts. Am J Ind Med. 2017;60(3):227–38.
Liang M, Guo X, Ding X, Song Q, Wang H, Li N, Su W, Liang Q, Sun Y. Combined effects of multiple metals on hearing loss: a bayesian kernel machine regression approach. Ecotoxicol Environ Saf. 2022;247:114279.
Lawrence KG, Niehoff NM, Keil AP, Braxton Jackson W 2nd, Christenbury K, Stewart PA, Stenzel MR, Huynh TB, Groth CP, Ramachandran G, et al. Associations between airborne crude oil chemicals and symptom-based asthma. Environ Int. 2022;167:107433.
Wang J, Chen Y, Guo X, Zhang W, Ren J, Gao A. LncRNA OBFC2A modulated benzene metabolites-induced autophagy and apoptosis by interacting with LAMP2. Food Chem Toxicology: Int J Published Br Industrial Biol Res Association. 2023;178:113889.
Harrath AH, Alrezaki A, Jalouli M, Aldawood N, Aldahmash W, Mansour L, Alwasel S. Ethylbenzene exposure disrupts ovarian function in Wistar rats via altering folliculogenesis and steroidogenesis-related markers and activating autophagy and apoptosis. Ecotoxicol Environ Saf. 2022;229:113081.
Qiao Y, Hu H, Zhao Y, Jin M, Yang D, Yin J, Wu P, Liu W, Li J. Benzene induces spleen injury through the B cell receptor signaling pathway. Ecotoxicol Environ Saf. 2023;257:114924.
Partha DB, Cassidy-Bushrow AE, Huang Y. Global preterm births attributable to BTEX (benzene, toluene, ethylbenzene, and xylene) exposure. Sci Total Environ. 2022;838(Pt 4):156390.
Morata TC, Fiorini AC, Fischer FM, Colacioppo S, Wallingford KM, Krieg EF, Dunn DE, Gozzoli L, Padrão MA, Cesar CL. Toluene-induced hearing loss among rotogravure printing workers. Scand J Work Environ Health. 1997;23(4):289–98.
Morata TC, Johnson AC, Nylen P, Svensson EB, Cheng J, Krieg EF, Lindblad AC, Ernstgård L, Franks J. Audiometric findings in workers exposed to low levels of styrene and noise. J Occup Environ Med. 2002;44(9):806–14.
Li W, Chen D, Ruan W, Peng Y, Lu Z, Wang D. Association of polycyclic aromatic hydrocarbons exposure, systemic inflammation with hearing loss among adults and adolescents. Environ Pollut. 2022;296:118772.
Aylward LL, Hays SM, Smolders R, Koch HM, Cocker J, Jones K, Warren N, Levy L, Bevan R. Sources of variability in biomarker concentrations. J Toxicol Environ Health B Crit Rev. 2014;17(1):45–61.
Juszczak H, Aubin-Pouliot A, Sharon JD, Loftus PA. Sinonasal risk factors for eustachian tube dysfunction: cross-sectional findings from NHANES 2011–2012. Int Forum Allergy Rhinol. 2019;9(5):466–72.
Yorgason JG, Kalinec GM, Luxford WM, Warren FM, Kalinec F. Acetaminophen ototoxicity after acetaminophen/hydrocodone abuse: evidence from two parallel in vitro mouse models. Otolaryngol Head Neck Surg. 2010;142(6):814–9. 819 e811-812.
Ho T, Vrabec JT, Burton AW. Hydrocodone use and sensorineural hearing loss. Pain Physician. 2007;10(3):467–72.
Dirain CO, Antonelli PJ. Cytotoxicity of tetracyclines in human tympanic membrane fibroblasts. Otol Neurotol. 2023;44(5):520–4.
Hamed SA. The auditory and vestibular toxicities induced by antiepileptic drugs. Expert Opin Drug Saf. 2017;16(11):1281–94.
Baluku JB, Bongomin F. Treatment outcomes of pregnant women with drug-resistant tuberculosis in Uganda: a retrospective review of 18 cases. Int J Infect Dis. 2021;105:230–3.
Goodall RL, Meredith SK, Nunn AJ, Bayissa A, Bhatnagar AK, Bronson G, Chiang CY, Conradie F, Gurumurthy M, Kirenga B, et al. Evaluation of two short standardised regimens for the treatment of rifampicin-resistant tuberculosis (STREAM stage 2): an open-label, multicentre, randomised, non-inferiority trial. Lancet. 2022;400(10366):1858–68.
Reese S, Grundfast K. Minocycline-induced hyperpigmentation of tympanic membrane, sclera, teeth, and pinna. Laryngoscope. 2015;125(11):2601–3.
Langworthy B, Wu Y, Wang M. An overview of propensity score matching methods for clustered data. Stat Methods Med Res. 2023;32(4):641–55.
Rotman A, Michael P, Tykocinski M, O’Leary SJ. Sudden sensorineural hearing loss secondary to metronidazole ototoxicity. Med J Aust. 2015;203(6):253–253e251.
Qi R, Zhang J, Diao T, Yu L. The auditory function in migraine model rats induced by postauricular nitroglycerin injection. Front Neurol. 2023;14:1259982.
Rybak LP. Ototoxicity of loop diuretics. Otolaryngol Clin North Am. 1993;26(5):829–44.
Ikeda N, Murray CJ, Salomon JA. Tracking population health based on self-reported impairments: Trends in the prevalence of hearing loss in US adults, 1976–2006. Am J Epidemiol. 2009;170(1):80–7.
Choi YH, Hu H, Mukherjee B, Miller J, Park SK. Environmental cadmium and lead exposures and hearing loss in U.S. adults: the National Health and Nutrition Examination Survey, 1999 to 2004. Environ Health Perspect. 2012;120(11):1544–50.
Schade DS, Lorenzi GM, Braffett BH, Gao X, Bainbridge KE, Barnie A, Cruickshanks KJ, Dalton D, Diminick L, Gubitosi-Klug R, et al. Hearing impairment and type 1 diabetes in the Diabetes Control and Complications Trial/Epidemiology of Diabetes Interventions and complications (DCCT/EDIC) Cohort. Diabetes Care. 2018;41(12):2495–501.
Bainbridge KE, Hoffman HJ, Cowie CC. Risk factors for hearing impairment among U.S. adults with diabetes: National Health and Nutrition Examination Survey 1999–2004. Diabetes Care. 2011;34(7):1540–5.
Rossing P, Caramori ML, Chan JCN, Heerspink HJL, Hurst C, Khunti K, Liew A, Michos ED, Navaneethan SD, Olowu WA, et al. Executive summary of the KDIGO 2022 Clinical Practice Guideline for Diabetes Management in chronic kidney disease: an update based on rapidly emerging new evidence. Kidney Int. 2022;102(5):990–9.
Zou P, Li M, Chen W, Ji J, Xue F, Wang Z, Xu L, Cheng Y. Association between trace metals exposure and hearing loss. Front Public Health. 2022;10:973832.
Bao W, Liu B, Simonsen DW, Lehmler HJ. Association between exposure to pyrethroid insecticides and risk of all-cause and cause-specific mortality in the General US Adult Population. JAMA Intern Med. 2020;180(3):367–74.
Lin FR, Maas P, Chien W, Carey JP, Ferrucci L, Thorpe R. Association of skin color, race/ethnicity, and hearing loss among adults in the USA. J Assoc Res Otolaryngol. 2012;13(1):109–17.
Wu S, Zhu S, Mo F, Yuan X, Zheng Q, Bai Y, Yang W, Chen Q. Association of coffee consumption with the prevalence of hearing loss in US adults, NHANES 2003–2006. Public Health Nutr. 2023;26(11):2322–32.
Statistics NCfH: NHANES survey methods and analytic guidelines. Availabe online: https://www.ncdcgov/nchs/nhanes/analyticguidelinesaspx#sample-design (accessed on 8 December 2022) 2018.
World Health O. World report on hearing. Geneva: World Health Organization; 2021.
Goderie TPM, Stam M, Lissenberg-Witte BI, Merkus P, Lemke U, Smits C, Kramer SE. 10-Year Follow-Up results of the Netherlands Longitudinal Study on hearing: Trends of Longitudinal Change in Speech Recognition in noise. Ear Hear. 2020;41(3):491–9.
Wang Z, Shi H, Peng L, Zhou Y, Wang Y, Jiang F. Gender differences in the association between biomarkers of environmental smoke exposure and developmental disorders in children and adolescents. Environ Sci Pollut Res Int. 2022;29(56):84629–39.
Fechter LD, Gearhart C, Fulton S, Campbell J, Fisher J, Na K, Cocker D, Nelson-Miller A, Moon P, Pouyatos B. Promotion of noise-induced cochlear injury by toluene and ethylbenzene in the rat. Toxicol Sci. 2007;98(2):542–51.
Sun L, Zhang M, Xu P, Fan L, Cui B, Zeng Q, Gu Q. [Effects of ethylbenzene on cell injury and mitochondrial membrane potential of CPCs]. Zhonghua Lao Dong Wei Sheng Zhi Ye Bing Za Zhi. 2018;36(2):146–9.
Zhang Y, Liu Y, Li Z, Liu X, Chen Q, Qin J, Liao Q, Du R, Deng Q, Xiao Y, et al. Effects of coexposure to noise and mixture of toluene, ethylbenzene, xylene, and styrene (TEXS) on hearing loss in petrochemical workers of southern China. Environ Sci Pollut Res Int. 2023;30(11):31620–30.
Staudt AM, Whitworth KW, Chien LC, Whitehead LW, Gimeno Ruiz de Porras D. Association of organic solvents and occupational noise on hearing loss and tinnitus among adults in the U.S., 1999–2004. Int Arch Occup Environ Health. 2019;92(3):403–13.
Zhang M, Qu T, Liu S, Yu F, Fan L, Lin D, Zhang Q, Song F, Zhang M, Cui B, et al. Ethylbenzene induces hearing loss by triggering mitochondrial impairments and excess apoptosis in cochlear progenitor cells via suppressing the Wnt/β-catenin signaling. Ecotoxicol Environ Saf. 2023;254:114721.
Zhang M, Wang Y, Wang Q, Yang D, Zhang J, Wang F, Gu Q. Ethylbenzene-induced hearing loss, neurobehavioral function, and neurotransmitter alterations in petrochemical workers. J Occup Environ Med. 2013;55(9):1001–6.
Matta JA, Gu S, Davini WB, Bredt DS. Nicotinic acetylcholine receptor redux: Discovery of accessories opens therapeutic vistas. Science 2021, 373(6556).
van Kleef RG, Vijverberg HP, Westerink RH. Selective inhibition of human heteromeric alpha9alpha10 nicotinic acetylcholine receptors at a low agonist concentration by low concentrations of ototoxic organic solvents. Toxicol Vitro. 2008;22(6):1568–72.
Gagnaire F, Langlais C. Relative ototoxicity of 21 aromatic solvents. Arch Toxicol. 2005;79(6):346–54.
Gagnaire F, Marignac B, Blachère V, Grossmann S, Langlais C. The role of toxicokinetics in xylene-induced ototoxicity in the rat and guinea pig. Toxicology. 2007;231(2–3):147–58.
Liu Y, Rao D, Fechter LD. Correspondence between middle frequency auditory loss in vivo and outer hair cell shortening in vitro. Hear Res. 1997;112(1–2):134–40.
Soliman SM, Teaima MH, Rashwan KO, Ali BM, Jasti BR, El-Nabarawi MA, Abd El-Halim SM. The deleterious effect of xylene-induced ear edema in rats: protective role of dexketoprofen trometamol transdermal invasomes via inhibiting the oxidative stress/NF-κB/COX-2 pathway. Int J Pharm. 2023;631:122525.
Tallandier V, Chalansonnet M, Merlen L, Boucard S, Thomas A, Campo P, Pouyatos B. An in vitro model to assess the peripheral vestibulotoxicity of aromatic solvents. Neurotoxicology. 2021;84:105–13.
Fenga C, Gangemi S, Giambò F, Tsitsimpikou C, Golokhvast K, Tsatsakis A, Costa C. Low-dose occupational exposure to benzene and signal transduction pathways involved in the regulation of cellular response to oxidative stress. Life Sci. 2016;147:67–70.
Hoffman HJ, Dobie RA, Losonczy KG, Themann CL, Flamme GA. Declining prevalence of hearing loss in US adults aged 20 to 69 years. JAMA Otolaryngol Head Neck Surg. 2017;143(3):274–85.
Golub JS, Brickman AM, Ciarleglio AJ, Schupf N, Luchsinger JA. Association of Subclinical hearing loss with cognitive performance. JAMA Otolaryngol Head Neck Surg. 2020;146(1):57–67.
Golub JS, Brickman AM, Ciarleglio AJ, Schupf N, Luchsinger JA. Audiometric age-related hearing loss and cognition in the Hispanic Community Health Study. J Gerontol Biol Sci Med Sci. 2020;75(3):552–60.
García-Mato Á, Cervantes B, Rodríguez-de la Rosa L, Varela-Nieto I. IGF-1 controls metabolic homeostasis and survival in HEI-OC1 Auditory cells through AKT and mTOR Signaling. Antioxid (Basel) 2023, 12(2).
Kubo H, Sawada S, Satoh M, Asai Y, Kodama S, Sato T, Tomiyama S, Seike J, Takahashi K, Kaneko K, et al. Insulin-like growth factor-1 levels are associated with high comorbidity of metabolic disorders in obese subjects; a Japanese single-center, retrospective-study. Sci Rep. 2022;12(1):20130.
Amin MN, Hussain MS, Sarwar MS, Rahman Moghal MM, Das A, Hossain MZ, Chowdhury JA, Millat MS, Islam MS. How the association between obesity and inflammation may lead to insulin resistance and cancer. Diabetes Metab Syndr. 2019;13(2):1213–24.
Feng ZY, Huang TL, Li XR, Chen L, Deng S, Xu SR, Ma KT, Li L, Si JQ. 17β-Estradiol promotes angiogenesis of stria vascular in cochlea of C57BL/6J mice. Eur J Pharmacol. 2021;913:174642.
Chen J, Nathans J. Estrogen-related receptor beta/NR3B2 controls epithelial cell fate and endolymph production by the stria vascularis. Dev Cell. 2007;13(3):325–37.
Kassotis CD, Klemp KC, Vu DC, Lin CH, Meng CX, Besch-Williford CL, Pinatti L, Zoeller RT, Drobnis EZ, Balise VD, et al. Endocrine-disrupting activity of Hydraulic Fracturing Chemicals and adverse health outcomes after prenatal exposure in male mice. Endocrinology. 2015;156(12):4458–73.
Williamson TT, Ding B, Zhu X, Frisina RD. Hormone replacement therapy attenuates hearing loss: mechanisms involving estrogen and the IGF-1 pathway. Aging Cell. 2019;18(3):e12939.
Kobayashi M, Takahashi E, Miyagawa S, Watanabe H, Iguchi T. Chromatin immunoprecipitation-mediated target identification proved aquaporin 5 is regulated directly by estrogen in the uterus. Genes Cells. 2006;11(10):1133–43.
Funding
This study was supported by the Chengdu High-level Key Clinical Specialty Construction Project.
Author information
Authors and Affiliations
Contributions
SW and YL conceived the study. SW, JL conducted the analyses and drafted the manuscript. SW, JL, FZ, RMZ, WTJ, NWW, JHZ, and YJL revised the manuscript for intellectual content. All authors contributed to and approved the final manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
All human studies have been approved by NCHS Ethics Review Board (ERB) and have therefore been performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments. The NCHS ERB protocol numbers for the National Health and Nutrition Examination Survey were Protocol #98 − 12, and Continuation of Protocol #2011-17.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Wang, S., Luo, J., Zhang, F. et al. Association between blood volatile organic aromatic compound concentrations and hearing loss in US adults. BMC Public Health 24, 623 (2024). https://doi.org/10.1186/s12889-024-18065-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12889-024-18065-0