
Abstract
Background
In Norrtälje municipality, within Region Stockholm, there is a joint integrated care organisation providing health and social care, which may have facilitated a more coordinated response to the covid-19 pandemic compared to the otherwise decentralised Swedish system. This study compares the risk of covid-19 mortality among persons 70 years and older, in the municipalities of Stockholm, Södertälje, and Norrtälje, while considering area and individual risk factors.
Methods
A population-based study using linked register data to examine covid-19 mortality among those 70 + years (N = 127,575) within the municipalities of interest between the periods March-August 2020 and September 2020-February 2021. The effect of individual and area level variables on covid-19 mortality among inhabitants in 68 catchment areas were examined using multi-level logistic models.
Results
Individual factors associated with covid-19 mortality were sex, older age, primary education, country of birth and poorer health as indicated by the Charlson Co-morbidity Index. The area-level variables associated were high deprivation (OR: 1.56, CI: 1.18–2.08), population density (OR: 1.14, CI: 1.08–1.21), and usual care. Together, this explained 85.7% of the variation between catchment areas in period 1 and most variation was due to individual risk factors in period 2. Little of the residual variation was attributed to differences between catchment areas.
Conclusion
Integrated care in Norrtälje may have facilitated a more coordinated response during period 1, compared to municipalities with usual care. In the future, integrated care should be considered as an approach to better protect and meet the care needs of older people during emergency situations.
Similar content being viewed by others


Introduction
During the coronavirus disease (covid-19) pandemic all age groups were at risk of contracting the virus, however, older age was associated with an increased risk of severe disease, hospitalisation, and mortality [1]. Moreover, variations were observed among older ages that were dependent on health problems and social care needs [2]. The highest mortality rates were observed among older persons receiving home-help services or living in care homes during the first wave of the covid-19 pandemic [3, 4]. In Sweden, 28.4% of deaths in covid-19 were among persons receiving home-help services in their own homes and 50.6% among care homes residents [2]. In Region Stockholm covid-19 mortality varied between municipalities and geographic areas and by time [5].
Other individual factors associated with an increased risk of covid-19 mortality were male sex, country of birth, and lower socio-economic position (SEP) indicated by education and co-morbidities [6,7,8]. Moreover, previous studies identified contextual factors that increased the community spread of the virus, including high population density, urban areas, and socio-economically disadvantaged area [9]. Further, these contextual factors have been associated with an increased risk of covid-19 related hospitalisations and mortality among those 18 years and older in a previous study set in Stockholm [10]. Similarly, a Swedish ecological geospatial study observed contextual factors such as high population density and a greater proportion of migrants, increased the risk of covid-19 related hospitalizations and mortality. In another study, contrarily, areas with a high proportion of persons 65 years and older had a reduced risk of covid-19 related hospitalisations and mortality [9, 10].
In Sweden, there are universal tax-funded health and social care systems, however, the provision is decentralised and fragmented, as the financing and organization of care is separated. The 21 regions are responsible for the provision of medical and health care services, while the 290 municipalities are responsible for providing social care to older people, including both home-help services (domestic and personal care) and the management of care homes. The administrative division between care systems limits the continuity and coordination of care to persons in need under normal circumstances. However, when this division of responsibility is extended to crisis management, such as the covid-19 pandemic, this has had implications for patient safety and quality of care [11, 12]. This division caused problems in the care of older people with covid-19, which was highlighted in a report by the national Corona Commission [13].
During the first wave, measures were introduced to limit the community spread of the virus, and to protect the healthcare system and maintain bed capacity for the inflow of severely ill covid-19 patients. Healthcare workers were prioritized in the allocation of personal protective equipment (PPE) and trained in measures meant to limit the spread of infectious disease. Therefore, at the initial stages the social care system for older persons were not prioritized and PPE was not widely distributed to those working in home-help services or in care homes [2, 4]. There was poor coordination between systems in response to the first wave of the covid-19 pandemic, combined with a limited ability to share information between health and social care systems, which placed vulnerable groups at greater risk of infection and severe outcomes [2].
The municipality Norrtälje, located in the north of Stockholm County at some distance from more central areas, implemented an integrated care (IC) approach in 2006, in contrast to the fragmented organisation of health and social care in the rest of region Stockholm. The IC approach began with pooled health and social care budgets and the formation of a joint board for health and social care which included representatives from the municipality and region. The board purchases services from a jointly owned company, Vårdbolaget Tiohundra which is the main provider of both health and social care in Norrtälje. The implementation and development of IC has been described in detail elsewhere [14, 15]. The IC approach led to organisational changes being introduced to improve the lines of communication and information sharing between health and social care providers [15, 16]. These organisational changes may have been beneficial in coordinating the response to the covid-19 pandemic by health and social care personnel, in terms of sharing of information, resources and coordination of care for risk groups such as those with multiple health problems and social care needs.
This study aimed to compare the risk of covid-19 mortality among persons 70 years and older, in different municipalities Stockholm, Södertälje, and Norrtälje, considering contextual and individual risk factors. The municipalities of Stockholm and Södertälje were selected as comparison, to consider the different municipal responses to the covid-19 pandemic, as both municipalities are examples of the usual decentralised health-and-social care organisation. Stockholm was chosen because it is the largest, centrally located and socio-economically heterogenous municipality. Södertälje was selected because of its similarities to Norrtälje, with a similar population size and socio-economic composition as Norrtälje, except with a larger proportion of inhabitants born outside Sweden.
Methods
A population-based study using register data linked via encrypted serial numbers. The study population was derived from the Total Population Register “Registret över Totalbefolkning’ (RTB), a register which contains information on life events such as births, deaths, and migration [17]. The RTB included all persons 18 years and older living in Stockholm County between 2019 and 2020 N = 1,855,404), of which there was N = 277,417 persons 70 years and older on the 31st of December 2019. The final study population included only those 70 years and older registered as living in the municipalities of Norrtälje, Södertälje and Stockholm (N = 127,575). The study was divided into two periods: period 1 between March 1st and August 31st, 2020, and period 2 between September 1st 2020 and February 28th 2021. Period 1 indicates the first wave and initial response to the covid-19 by the health and social care system, while period 2 is defined by the second wave prior to widespread availability of vaccinations [18]. In period 2, there were (N = 123,622) excluding (n = 3,953) persons who died during period 1.
Outcomes
The Swedish Cause of Death Register was used to distinguish between covid-19 related from other causes of mortality. At the beginning, covid-19-mortality was officially defined as deaths occurring in patients who tested positive for SARS-CoV-2 through an RT-PCR test. However, this definition was later expanded to include covid-19 related deaths without a positive test. The International Classification of Disease (ICD-10) codes used to indicate covid-19 related mortality (U07.1, U07.2, U07.3) based on recommendations by the National Board of Health and Welfare (NBHW) [19].
Individual variables
Individual variables were obtained from RTB; sex was categorised into male or female; age measured using year of birth and categorized into five-year intervals. Country of birth was categorised as born in Sweden or outside of Sweden. The data was linked to the Longitudinal Integrated Database for Social Insurance and Labour Market Studies (LISA), where measures of SEP were obtained. The LISA register is a collection of variables from several different population-based registers which are individually linked [20]. Income was measured using net annual equalised household income in 2019 and was ranked into quintiles with group 1 (lowest) and group 5 (highest), based on the distribution of income in the study population. Education level was categorised according to the Swedish educational system into years of education: primary (< 9 years), secondary (9–12 years) and post-secondary (> 12 years).
Municipal social care use was measured in the Swedish Social Services Register which collects monthly data on individual use of home-help (domestic and/or personal care) services and care home residence [21]. Municipal social care use was categorized into living in own homes without home-help, living in own home with home-help, and care-home resident, during period 1 and/or period 2.
The Charlson Comorbidity Index (CCI) was included as an indicator of health status. The CCI score was measured in the National Patient Register (NPR) using inpatient and outpatient care diagnoses between 2016 and 2018. The CCI assigns scores ranging from 1 to 6 to different morbidities according to the severity of disease. The weighted score was calculated for everyone in the study population and was used to adjust for morbidity in the analysis [22].
Area-level variables
The area-level was delineated by catchment area (“betjäningsområde”) within each municipality, previously used to denote service areas which primary care centres were responsible for. The catchment areas include 7 areas in Norrtälje, 52 areas in Stockholm municipality and 9 areas in Södertälje (see table S1). A variable indicating organisation of care in the municipality was included (IC), where Norrtälje was the reference category which was compared to usual care in Stockholm and Södertälje. Additionally, area variables were calculated based on all inhabitants 18 years and older, including a composite neighbourhood deprivation score (NDS) which was divided into three levels from the least to the most deprived, the NDS was generated to adjust for the socio-economic circumstances of areas in Stockholm County and is described in detail by Bell et al. [10]. Population density was calculated based on the number of inhabitants per square kilometre and was included in the model as a continuous variable.
Analysis
The data had a multi-level structure with level one consisting of individuals residing in the municipalities of interest and were nested within the catchment areas within each municipality [23]. Multivariate logistic regression models used to select the individual-level covariates and goodness of fit was assessed based on plots of the predicted observed values and the pseudo r-squared (see figure S1 and S2).
The multi-level logistic models were specified as follows: model 0 included the random intercept term and provides information on the individual variance in how the probability of covid-19 mortality was distributed across the different catchment areas. Model 1 included the individual covariates selected from the multivariate models, to adjust for the individual composition of the catchment areas. Model 2 included model 1, and a selection of area-level variables (see table S3-S5), this provided information about the association between area-level variables and covid-19 mortality among individuals within the catchment areas. Model 3 expanded upon model 2, to evaluate the specific contextual effects of IC, and the organization of care in the municipality was included as an area-level variable.
Finally, in model 4 the use of municipal social care was included in the fixed effects, considering the potential mediation pathway between the organisation of care (integrated vs. usual) and municipal social care [24]. The variance and the proportional change in the variance (PCV) were estimated to compare each model. Caterpillar plots were used to visually assess and compare the variance between catchment areas across the distribution in period 1 and 2.
The amount of explanatory power attributed to contextual effects was estimated using the variance partition coefficient (VPC), that represents the proportion of variability in covid-19 mortality that is attributable to systematic differences between areas [25]. The VPC was estimated using a simulation method based on a probability scale of a range explanatory variables, from the models described (see table S6) [26].
The regression coefficients were estimated using generalised mixed effects models with a maximum likelihood estimation and a binomial distribution expressed as odds ratios and confidence intervals (R package Lme4).
Results
Among the N = 127,575 inhabitants 70 years and older in the municipalities of Norrtälje, Södertälje and Stockholm there was a total of 1,674 covid-19 related deaths between 1st March 2020 and 28th February 2021, with more covid-19 deaths in period 1 compared to period 2. Age standardized rates of covid-19 mortality stratified by municipality and care groups are shown in Table 1. The covid-19 mortality rate was higher in Södertälje, and Stockholm municipality compared to Norrtälje (3.1 covid-19 deaths per 10,000 persons) in period 1. Home-help users and care home residents had the highest rate of covid-19 mortality in both periods. In period 2, the rate of covid-19 mortality increased in Norrtälje and decreased in the other municipalities compared to period 1.
Table 2 describes the composition of the study population. The age distribution did not vary between the municipalities. In Norrtälje, 47.9% of inhabitants were male compared to 43.7% in Södertälje and 42.5% in Stockholm municipality. Södertälje had the highest proportion of inhabitants born outside of Sweden (34%), compared to 10.5% in Norrtälje. There was a higher proportion of inhabitants in lower income groups and with primary education in Norrtälje and Södertälje, and there were slight differences in morbidity based on the CCI score and risk group diagnosis between the municipalities. In period 1, in Södertälje 14.5% of inhabitants were receiving home-help services compared to 13.8% in Stockholm and 11.3% in Norrtälje. The proportion of care home residents was similar (6.3% and 6.2%) in Norrtälje and Stockholm and 5.7% in Södertälje.
The multivariate logistic models estimating the effect of individual factors on covid-19 mortality for both periods, see table S2. In period 1, men had higher odds than women (OR 1.52, CI:1.38–1.66). Increasing age was strongly associated with increasing odds of covid-19 mortality, as those 75–80 years had (OR 1.96, CI:1.64–2.33) increased risk compared to those 70–74 years, while those 95 + years had a (OR 18.76, CI:15.22–23.13). Those with primary (OR 1.59, CI:1.40–1.79) and secondary (OR 1.41, CI:1.25–1.58) level education had increased odds compared to those with tertiary level education. Individuals born outside of Sweden had higher odds of covid-19 mortality (OR 1.42, CI:1.28–1.58) compared to those born in Sweden. Increased morbidity indicated by CCI score was associated with increased odds of covid-19 mortality (OR 1.24, CI:1.21–1.26). The individual risk factors associated with covid-19 mortality were similar in period 2 with slight differences in effect sizes.
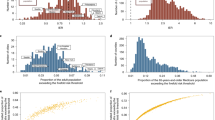
Figure 1 shows area specific effects of covid-19 mortality across the distribution of catchment areas, the variance was 0.3518 in period 1 and 0.1195 in period 2. In period 1, catchment areas within Norrtälje the red dots were lower across the distribution of covid-19 mortality compared to Södertälje and Stockholm, see Fig. 1(A), however, they were more spread across the distribution in period 2, see Fig. 1(B). Table 3 presents the estimates from the multi-level logistic regression models in period 1. the variance in the probability of covid-19 mortality between catchment areas reduced by 39.3% when controlling for individual factors. Model 2 included both individual and area-level factors, high deprivation (OR:2.09, CI: 1.48–2.96) indicated by NDS and population density (OR 1.21, CI 1.13–1.29) were associated with an increased risk of covid-19 mortality, which explained 67.9% of the variance between catchment areas compared to model 0, see Fig. 2 (A). Model 3 expanded on model 2 and included the area level variable organization of care. There was an increased risk of covid-19 mortality in municipalities with usual care (OR:6.01 CI: 3.26–11.08) in Stockholm, and (OR: 3.37, CI:2.10–6.66) Södertälje compared to IC in Norrtälje, this explained 85.9% of the variance in the risk of covid-19 mortality between catchment areas. The effect of municipal social care was considered in model 4, those living in ordinary housing with home-help (OR:5.93, CI4.88-7.21) and care home residents (OR:22.62, CI:18.73–27.33) had increased risk of covid-19 mortality compared to those without home-help in ordinary housing.

Caterpillar plots of the catchment area specific effects (residuals and CIs) on the risk of covid-19 mortality across the distribution of catchment areas based on the random intercept term from model 0, in period 1 (A) and period 2 (B), among inhabitants 70 years and older within the municipalities of Norrtälje (the red dots), Södertälje (blue dots) and Stockholm municipality (back dots)

Caterpillar plot of the catchment area specific effects (residuals and CIs) on the risk of covid-19 mortality after adjusting for individual and area-level factors shown in model 3, Tables 3 and 4 for period 1 (A) and period 2 (B), among inhabitants 70 years and older within the municipalities of Norrtälje (the red dots), Södertälje (blue dots) and Stockholm municipality (black dots)
The VPC reported in Table 3, is based on the following profile (male, 85–89 years, primary education, born outside of Sweden, and an average CCI score) 0.57% of the residual variation is attributable to difference between catchment areas. The VPC decreased slightly when area-level explanatory variables were included 0.52%. Finally, being in a municipality with a usual care the VPC decreased to 0.12% of the residual variation is attributable to differences between catchment areas in period 1.
In period 2, adjusting for individual covariates see Table 4 explained 45.7% of the variation and the addition of area-level factors explained 50.2% of the variation in the distribution of covid-19 mortality across catchment areas. NDS and population density were not significantly associated with risk covid-19 mortality among individuals, and moreover, being in a municipality with usual care was associated with covid-19 mortality in period 2. The addition of area-level variables had a limited effect on the variation of covid-19 mortality between catchment areas in period 2 see Fig. 2(B), and moreover, the VPC estimates show that there was very little residual variation in covid-19 mortality attributable to differences between catchment areas.
Dicussion
The rate of covid-19 mortality among those 70 years and older was lower in Norrtälje compared to the municipalities of Stockholm and Södertälje in period 1, although covid-19 mortality increased in Norrtälje in period 2. Individual risk factors for covid-19 mortality in both periods were male sex, older age, primary education, being born outside of Sweden, and poorer health as indicated by CCI score. Area level risk factors were more important in period 1, as persons in catchment areas with high deprivation, high population density and in municipalities with usual care had an increased risk of covid-19 mortality. Although catchment areas within Norrtälje had lower probability of covid-19 mortality compared to usual care in period 1, the general contextual effects indicate that the relevance of area differences was relatively weak. In period 2, individual risk factors of covid-19 mortality explained more of the variation between catchment areas and the general contextual effects were low, therefore, the area was not as relevant in examining individual differences in covid-19 mortality in period 2.
All persons 70 years and older, irrespective of health status, were identified as a vulnerable group to adverse health outcomes due to covid-19, and recommendations were put in place to protect older people during the covid-19 pandemic [18]. Consistent with previous studies, we observed a strong association between older age and covid-19 mortality [10, 27]. The vulnerability of older people to covid-19 is contributed to by a higher prevalence of multi-morbidity and functional decline [27]. Further, a previous study has shown a positive correlation between CCI score and covid-19 mortality, in which each point increase in CCI score increased the risk of death by 2.5% [28]. The provision of social care is based on needs assessment and those who move into care homes tend to be more frail, have multiple health problems and generally, at greater risk of mortality [29]. Excess mortality due to covid-19 was observed among care home residents compared to individuals living in their own homes during the peak of the covid-19 pandemic [30]. Interventions were introduced to reach vulnerable groups as the Swedish government introduced national restrictions banning visits to care homes on the 1st of April 2020 [18], though some municipalities introduced their own visitation restrictions already in March [13].
The Swedish authorities handling of the covid-19 pandemic was criticised, with concerns about shortages of staff, PPE and testing kits, particularly in municipal social care [13]. In Norrtälje, Tiohundra AB is responsible for the provision and organization of care homes in Norrtälje, which enables more coordination between health-and-social care professionals regarding information sharing which facilitates communication between care professionals [15, 16]. Additionally, the shared funding in Norrtälje supported an effective supply chain for PPE, testing kits and other resources [13]. This aspect of IC could have contributed to the lower covid-19 mortality among municipal social care users in Norrtälje compared to other municipalities in period 1. However, a study found that the proportion of covid-19 infections among care home residents was mostly the same or slightly higher compared to infectious among the care staff in Nordic countries [4]. A systematic review examining the characteristics of care home facilities and staff on risk of infectious disease transmission highlighted that larger facilities in urban areas, with temporary staff or staff residing in highly infectious areas, had an increased risk of transmission in facilities [31]. This might elucidate why covid-19 mortality was higher in the usual care settings indicated by the municipalities of Stockholm and Södertälje as these are more urban and densely populated areas compared to Norrtälje.
Congruent with previous studies, we observed that high population density and neighbourhood deprivation were associated with increased risk of covid-19 mortality [2, 10, 30]. High population density is an indicator of community transmission, as covid-19 was primarily spread through face-to-face interactions, unavoidable in densely populated areas, with more people of working age and including essential workers who were still commuting [32]. As Norrtälje has a lower population density compared to Södertälje and Stockholm municipalities, this must be taken into consideration when interpreting the lower covid-19 mortality among inhabitants 70 years in Norrtälje during period 1. Additionally, older persons born outside of Sweden had an increased risk of covid-19 mortality, which is supported by previous studies [6, 8, 10]. There is a concentration of persons born outside of Sweden in socio-economically disadvantaged neighbourhoods compared to neighbourhoods with a higher concentration of Swedish born [33]. Comparatively, Norrtälje has less inhabitants born outside of Sweden, although with a lower SEP compared to Stockholm municipality. Previous studies have observed that individuals with lower SEP had a higher risk of covid-19 mortality [6, 8]. Further, in other European countries a positive association was found between area-level socio-economic disadvantage and covid-19 mortality [34].
Strengths and limitations
The use of population-based registers to measure individual and area-level risk factors for covid-19 mortality is a strength of this study. Defining area-level based on catchment areas assures an adequate sample size for a multi-level analysis. Distinguishing between the time periods allows for consideration for the differences between the waves of the covid-19 pandemic and the preparedness of the health-and-social care systems to respond [11, 35].
The NBHW reports all cases where the underlying cause of death was covid-19, whether the diagnosis was confirmed via laboratory testing or not [36]. However, discrepancies have been observed between official covid-19 death statistics and the reported underlying and contributing cause-of-death based on a clinical audit in a previous Swedish study [37]. Moreover, this becomes increasingly complicated when ascertaining the underlying cause of death of persons with multiple chronic conditions and limited insight into the process of dying [38]. Using the CCI score to measure morbidity is a strength as the CCI score assesses the number and severity of chronic conditions [22]. Dichotomising country of birth into “Sweden” or “born outside of Sweden” is limitation as it does not consider the diversity of backgrounds or time spent in Sweden.
Additional limitations relate to distinguishing the effect of IC compared to “usual care”. IC systems are often implemented to improve the experience of care for individuals and health-and-social care professionals experience of providing care, along with being compatible with specific needs of the community [39]. The outcome measure of mortality might be considered a crude outcome to assess the experience of care. Moreover, it is difficult to measure whether the provision of care continued as normal during the covid-19 pandemic and what measures were introduced in individual municipalities. The municipalities of Stockholm and Södertälje were considered to have “usual care”. However, to measure what defines usual care is difficult under the unusual circumstances created by the covid-19 pandemic, as ultimately all health-and-social care workers were taking a personal risk to their own health to continue providing good quality care safely while working under extreme pressure [11]. Therefore, it is difficult to ascertain the exact effect of IC, as each municipality has their own funding sources and were the responsible authority who acted as they deemed appropriate during the covid-19 pandemic, though all regions and municipalities must abide by the recommendations introduced nationally [11, 13, 35, 40].
IC might have allowed for better coordination between care providers at the beginning of the covid-19 pandemic systems encountered numerous organisational and logistical challenges. The risk of covid-19 mortality among inhabitants 70 years and older was lower in Norrtälje compared to municipalities with usual care after adjusting for individual and area level risk factors in period (1) However, individual risk factors were more important in period (2) Alternative approaches to organizing care should be considered by policymakers in the future, given that IC approach might help overcome challenges encountered in emergency situations, to better protect and meet the care needs of older people.
Data availability
The data used to perform this study cannot be made available upon request. In accordance with the General Data Protection Regulation, The Swedish law SFS 2018:218, The Swedish Data Protection Act, the Swedish Ethical Review Act, and the Public Access to Information and Secrecy Act, these types of sensitive data can only be made available after legal review, for researchers who meet the criteria for access to this type of sensitive and confidential data. Readers may contact the first author regarding any further details.
Abbreviations
- Covid-19:
-
Coronavirus Disease
- SEP:
-
Socio–economic Position
- PPE:
-
Personal protective equipment
- IC:
-
Integrated care
- RTB:
-
Total population register
- LISA:
-
Longitudinal Integrated Database for Social Insurance and Labour Market Studies
- NBHW:
-
National Board of Health and Welfare
- NPR:
-
National Patient Register
- CCI:
-
Charlson Comorbidity Index
- OR:
-
Odds Ratio
- CI:
-
Confidence Interval
- AIC:
-
Akaike Information Criterion
- VPC:
-
Variance Partition Coefficient
- PCV:
-
Proportional Change in Variance
References
Wu C, Chen X, Cai Y, Xia J, Zhou X, Xu S, et al. Risk factors Associated with Acute respiratory distress syndrome and death in patients with Coronavirus Disease 2019 Pneumonia in Wuhan, China. JAMA Intern Med. 2020;180(7):934–43.
Schön LJP. Mechanisms of coordination between healthcare policy and other public policy sectors to speed up the response to the coronavirus crises: Sweden. CSIC - Instituto de Políticas y Bienes Públicos (IPP); 2021.
Sepulveda ER, Stall NM, Sinha SK. A comparison of COVID-19 Mortality Rates among Long-Term Care residents in 12 OECD Countries. J Am Med Dir Assoc. 2020;21(11):1572–4e3.
Rauhala AS, Fagerström LM, Lindholst AC, Sinervo TS, Bertelsen TM, Bliksvær T, et al. Which factors are associated with COVID-19 infection incidence in care services for older people in nordic countries? A cross-sectional survey. Scand J Public Health. 2022;50(6):787–94.
Bartelink VTP, Walander A, Burström B, Ponce de Leon A. Nederby Öhd J HM, Lager A. Socioekonomiska faktorer och covid-19 i Stockholms län. Stockholm: Region Stockholm, 2020.
Rostila M, Cederström A, Wallace M, Brandén M, Malmberg B, Andersson G. Disparities in Coronavirus Disease 2019 Mortality by Country of Birth in Stockholm, Sweden: A Total-Population-based Cohort Study. Am J Epidemiol. 2021;190(8):1510–8.
Bergman J, Ballin M, Nordström A, Nordström P. Risk factors for COVID-19 diagnosis, hospitalization, and subsequent all-cause mortality in Sweden: a nationwide study. Eur J Epidemiol. 2021;36(3):287–98.
Drefahl S, Wallace M, Mussino E, Aradhya S, Kolk M, Brandén M, et al. A population-based cohort study of socio-demographic risk factors for COVID-19 deaths in Sweden. Nat Commun. 2020;11(1):5097.
Fonseca-Rodríguez O, Gustafsson PE, San Sebastián M, Connolly AF. Spatial clustering and contextual factors associated with hospitalisation and deaths due to COVID-19 in Sweden: a geospatial nationwide ecological study. BMJ Glob Health. 2021;6(7).
Bell M, Hergens MP, Fors S, Tynelius P, de Leon AP, Lager A. Individual and neighborhood risk factors of hospital admission and death during the COVID-19 pandemic: a population-based cohort study. BMC Med. 2023;21(1):1.
Ludvigsson JF. The first eight months of Sweden’s COVID-19 strategy and the key actions and actors that were involved. Acta Paediatr. 2020;109(12):2459–71.
Stein KV, Goodwin N, Miller R. From Crisis to Coordination: challenges and opportunities for Integrated Care posed by the COVID-19 pandemic. Int J Integr Care. 2020;20(3):7.
Sverige Coronakommissionen. Sverige under pandemin: Sjukvård och folkhälsa Volym 22021. 395–807 sidor p.
Doheny M, Agerholm J, Orsini N, Schön P, Burström B. Impact of integrated care on trends in the rate of emergency department visits among older persons in Stockholm County: an interrupted time series analysis. BMJ Open. 2020;10(6):e036182.
Bäck MA, Calltorp J. The Norrtaelje model: a unique model for integrated health and social care in Sweden. Int J Integr Care. 2015;15:e016.
Øvretveit J, Hansson J, Brommels M. An integrated health and social care organisation in Sweden: creation and structure of a unique local public health and social care system. Health Policy. 2010;97(2–3):113–21.
Ludvigsson JF, Almqvist C, Bonamy AK, Ljung R, Michaëlsson K, Neovius M, et al. Registers of the Swedish total population and their use in medical research. Eur J Epidemiol. 2016;31(2):125–36.
Olofsson T, Vilhelmsson A, Dataset. COVID-19 epidemic policy and events timeline (Sweden). Data Brief. 2022;40:107698.
Socialstyrelsen. Koder ur ICD-10-SE och KVÅ vid covid-19. In: Klassifikationsverksamheten, editor. Stockholm2021. p. 1–2.
Ludvigsson JF, Svedberg P, Olén O, Bruze G, Neovius M. The longitudinal integrated database for health insurance and labour market studies (LISA) and its use in medical research. Eur J Epidemiol. 2019;34(4):423–37.
Meyer AC, Sandström G, Modig K. Nationwide data on home care and care home residence: presentation of the Swedish Social Service Register, its content and coverage. Scand J Public Health. 2022;50(7):946–58.
Ludvigsson JF, Appelros P, Askling J, Byberg L, Carrero JJ, Ekström AM, et al. Adaptation of the Charlson Comorbidity Index for Register-Based Research in Sweden. Clin Epidemiol. 2021;13:21–41.
Merlo J, Wagner P, Austin PC, Subramanian SV, Leckie G. General and specific contextual effects in multilevel regression analyses and their paradoxical relationship: a conceptual tutorial. SSM Popul Health. 2018;5:33–7.
Bingenheimer JB, Raudenbush SW. Statistical and substantive inferences in public health: issues in the application of multilevel models. Annu Rev Public Health. 2004;25:53–77.
Austin PC, Merlo J. Intermediate and advanced topics in multilevel logistic regression analysis. Stat Med. 2017;36(20):3257–77.
Jon Rasbash FS, Goldstein WJBH. A user’s guide to MLwiN. United Kingdom: Centre for Multilevel Modelling,University of Bristol; 2012. pp. 127–34.
Ho FK, Petermann-Rocha F, Gray SR, Jani BD, Katikireddi SV, Niedzwiedz CL, et al. Is older age associated with COVID-19 mortality in the absence of other risk factors? General population cohort study of 470,034 participants. PLoS ONE. 2020;15(11):e0241824.
Comoglu S, Kant A. Does the Charlson comorbidity index help predict the risk of death in COVID-19 patients? North Clin Istanb. 2022;9(2):117–21.
P JLaS. Governmental response to the COVID-19 pandemic in long-term care residences for older people preparedness, responses and challenges for the future: Sweden.
Brandén M, Aradhya S, Kolk M, Härkönen J, Drefahl S, Malmberg B, et al. Residential context and COVID-19 mortality among adults aged 70 years and older in Stockholm: a population-based, observational study using individual-level data. Lancet Healthy Longev. 2020;1(2):e80–e8.
Liljas AEM, Morath LP, Burström B, Schön P, Agerholm J. The impact of organisational characteristics of staff and facility on infectious disease outbreaks in care homes: a systematic review. BMC Health Serv Res. 2022;22(1):339.
Cos O, Castillo V, Cantarero D. Facing a second Wave from a Regional View: spatial patterns of COVID-19 as a Key Determinant for Public Health and Geoprevention Plans. Int J Environ Res Public Health. 2020;17:22.
Malmberg B, Clark WAV. Migration and Neighborhood Change in Sweden: the Interaction of ethnic choice and income constraints. Geographical Anal. 2021;53(2):259–82.
McGowan VJ, Bambra C. COVID-19 mortality and deprivation: pandemic, syndemic, and endemic health inequalities. Lancet Public Health. 2022;7(11):e966–e75.
Ludvigsson JF. How Sweden approached the COVID-19 pandemic: Summary and commentary on the National Commission Inquiry. Acta Paediatr. 2023;112(1):19–33.
Socialstyrelsen. Statistik om covid-19. 2021.
Spreco A, Andersson C, Sjödahl R, Timpka T. Concordance between COVID-19 mortality statistics derived from clinical audit and death certificates in Östergötland County, Sweden. Public Health. 2023;221:46–9.
Mieno MN, Tanaka N, Arai T, Kawahara T, Kuchiba A, Ishikawa S, et al. Accuracy of Death certificates and Assessment of factors for misclassification of underlying cause of death. J Epidemiol. 2016;26(4):191–8.
Henderson L, Bain H, Allan E, Kennedy C. Integrated health and social care in the community: a critical integrative review of the experiences and well-being needs of service users and their families. Health Soc Care Community. 2021;29(4):1145–68.
Sverige Coronakommissionen. Sverige under pandemin. 2 volymer (758 sidor) p.
Acknowledgements
A special thank you to our colleagues at the Center of Epidemiology and Community Medicine at Stockholm County Council for guiding in catchment area measures.
Funding
This research was carried out as part of the project “Organisation and response to covid-19 of municipal health and social care services for older people– impact on mortality and health care utilisation in Region Stockholm” funded by the Swedish Research Council (2020–05850); the project “In the wake of covid-19: How can the structure and quality of health and social care for older people with complex care needs in Sweden be improved?” funded by the Swedish Research Council for Health, Working Life, and Welfare (Forte) (2021 − 01830) and the program grant “Inequality dynamics over the life course: family and policy influences” funded by Forte (2016–07206).
Open access funding provided by Karolinska Institute.
Author information
Authors and Affiliations
Contributions
BB, JA, and AL conceived the idea for the project. JA, MD and APDL came up with the study design and analysis approach. MD constructed the dataset used to perform the analysis. MD, APDL and JA performed the statistical analysis and MD drafted the text. BB, JA, and AL commented on the text. All authors read and approved the manuscript.
Corresponding author
Ethics declarations
Ethical approval and consent to Participate
Ethical permission was obtained from the Swedish Ethical Review Authority previously known as Regional Ethics Review Board of Stockholm, Sweden, application reference number Dnr: 2020–04577. The Swedish Ethical Review Authority approved the data linkage between the various registers via encrypted serial numbers, this pseudonymized data is stored securely, and all results are reported on the macro level. Informed consent was not required by the Swedish Ethical Review Authority because this study used large population-based administrative pseudonymized data, in accordance with Swedish law informed consent is not required when using routinely collected administrative data for ethically reviewed research projects undertaken at Swedish universities and colleges. All methods carried out were in accordance with the relevant guidelines and regulations.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Doheny, M., de Leon, A.P., Burström, B. et al. Differences in Covid-19 mortality among persons 70 years and older in an integrated care setting in region Stockholm: a multi-level analysis between March 2020-February 2021. BMC Public Health 24, 462 (2024). https://doi.org/10.1186/s12889-024-17904-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12889-024-17904-4