
Abstract
Background
Despite the high occurrence of floods in Iran, its psychological consequences have been less discussed. The present paper addresses the prevalence of Post-traumatic Stress Disorder (PTSD) and its determinants among the affected adults by the huge flood of 2019.
Methods
An analytical cross-sectional study was conducted through household face-to-face surveys in August and September 2019. Individuals who were affected by floods and were at least 16 years old were randomly selected from three provinces in Iran: Lorestan and Khuzestan in the west and southwest, and Golestan in the northeast. The questionnaire of demographic and flood related variables in addition to the Impact of Event Scale-Revised (IES-R) were utilized to collect the data. We applied a complex sample analysis to describe the prevalence of PTSD and logistic regression analyses to find its determinants.
Results
Out of the 2,305 individuals approached for surveys, 1,671 (72.5%) adults affected by the floods participated in the study. The majority of participants were housewives, married, had either no formal education or primary education, and resided in rural areas. The prevalence of PTSD in the participants was 24.8% (CI 95%: 20.7–28.8%) and was significantly higher in Lorestan province (39.7%, P < 0.001). Determinants of PTSD, were unemployment (adjusted odds ratio [AOR] = 3.53, CI 95%: 1.38-9.00), primary (AOR = 2.44, CI 95%: 1.10–5.41) or high school (AOR = 2.35, CI 95%: 1.25–4.40) education (vs. university), a history of mental disorders (AOR = 2.36, CI 95%: 1.22–4.58), high damage to assets (AOR = 2.29, CI 95%: 1.40–3.75), limited access to health care services after the flood (AOR = 1.95, CI 95%: 1.20–3.19), not receiving compensation for flood damage (AOR = 1.94, CI 95%: 1.01–3.83), high wealth index (AOR = 1.90, CI 95%: 1.23–2.93), and flooded house with a height of more than one meter (AOR = 1.66, CI 95%: 1.02–2.76).
Conclusion
Results show a notable prevalence of PTSD, especially in Lorestan province, among adults affected by floods. Determinants of PTSD include unemployment, lower education, psychiatric history, extensive property damage, limited post-flood healthcare access, lack of compensation, and increased flood exposure. We recommend adopting an inclusive screening approach for high-risk groups and developing appropriate therapeutic and supportive interventions.
Similar content being viewed by others


Introduction
Some Studies have demonstrated that over the past five decades, coinciding with the escalation of global warming, floods have emerged as the most prevalent natural disaster [1, 2]. In Iran, more than 80% of the cities are exposed to floods and the incidence of floods has been increasing in recent decades [3, 4]. The flood damage is very extensive and is economically, socially and healthily significant [1, 5].
In 2019, Iran experienced a huge flood due to heavy rains occurring from March to April, primarily impacting the northeastern, western, and southwestern regions [6]. The flood affected thirty-one provinces, 3,800 towns and villages, and 140 rivers. It resulted in the destruction of 65,000 houses, damage to 159 main roads, 700 bridges, and a disruption to the Health System Response [7, 8].
Floods can cause a wide range of health impacts, including immediate or short-term physical, infectious, chemical, family, and residential consequences [9]. They can also lead to reduced access to medical and mental health services, as well as disruptions in mental health [10]. According to the studies, among the psychological consequences of floods, post-traumatic stress and depressive disorders were the most frequent [11, 12].
Studies indicate that the psychological consequences of flooding are more prominent in the first months [11], but these problems are not limited to the immediate aftermath of flooding and can continue to be significant in the following months and even years. For example, in Australia, Matthews et al. [13] examined the mental health status of the flooded population in a cross-sectional study six months after the Northern New South Wales flood. At this point in time, more than a fifth of the population was still distressed about the flood. As another example, we can mention the high frequency of Post-traumatic Stress Disorder (PTSD) and depression in the flooded agricultural population in Korea, even 18 months after the flood [14]. A study on the victims of the spring 2019 floods in Iran revealed that six months after the event, the prevalence of psychological distress and depression was 33.6% and 23.0%, respectively [15]. In the study on PTSD after the flood in Iran, research conducted in Mazandaran Province [16] three months after the 2012 flood reported a PTSD prevalence of 64%, while a recent study in Lorestan province [17] reported it to be 12.8% one year after the 2019 flood.
Despite the high frequency of floods and the extensive material damage they cause in Iran, there are few references, and a substantial gap still exists in understanding the psychological consequences of floods in the Iranian context. After the huge and extensive flooding in Iran in 2019, there arose a necessity to run projects to answer the questions on the flood’s consequences. In line with the President’s decision to establish a “Special Commission for National Report on Floods” with the aim of providing scientific, credible and accurate answers to the various aspects of the floods, the Mental Health Committee was formed as a subset of the Social, Cultural and Media working group. The committee’s studies used a combined approach of qualitative and quantitative research methods, including interviews, group discussions, observations, and a wide-ranging household study, to comprehensively explore the mental health in flood-affected provinces. The present paper addresses the prevalence of PTSD and its determinants among adults affected by the huge flood in 2019, as part of a larger study [15].
Methods
Study design and sampling
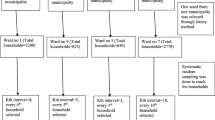
An analytical cross-sectional study was conducted through household face-to-face surveys in August and September 2019, using three-stage random sampling. The present report focuses on the prevalence of PTSD and its determinants among the flooded adults, as part of a larger study [15]. The individuals affected by the flood, aged at least 16 years, were randomly selected from three heavily affected provinces: Lorestan [including Pol Dokhtar and Mamulan], Khuzestan [including Dasht-e-Azadegan, west Ahvaz and Hamidiyeh] in the west and southwest, and Golestan [including Aq Qala and Gomishan] in the northeast of Iran. The study utilized a three-stage random sampling method (detailed in another paper [15]), with 210 clusters, each comprising 8 adult participants. In the first stage, 70 clusters were selected in each of three provinces based on the ratio of flood victims in cities and villages. This involved identifying affected areas on a map and randomly choosing blocks. In the second stage, households were selected within each block by choosing one plaque randomly and including eight households every second plaque. In the third stage, one adult from each household was randomly chosen based on the proximity of their birthdate to the survey day.
Criteria for study exclusion
Individuals who were absent from home until the end of data collection, lacked an understanding of the Persian language, were aged less than 16 years, or had physical or cognitive impairments preventing participation in the surveys were excluded from the study.
Data collection and quality assurance
The data collectors included 18 mental health experts, with 6 assigned to each province to complete the questionnaires on behalf of participants after conducting the surveys. They held a bachelor’s or master’s degree in psychology or related disciplines and underwent a 16-hour hands-on workshop to learn how to implement the protocol and collect data using reliable and widely accepted standardized questionnaires. An observer was assigned for each province to ensure the accurate selection of the sample and to review the completed forms for precision and accuracy.
Instruments
1) A questionnaire of demographic variables
including age, gender, marital and employment status, education, being urban or rural (as the place of residence), and the ownership of assets (in detail in another paper [15]), was administered. Additionally, participants self-reported their past history of mental disorders diagnosed by a psychiatrist.
2) A questionnaire of flood related variables
including height of incoming flood to the house, percentage of flood damage to property, compensation for flood damage, access to health care services after the flood (limited or not limited), and temporary stay in the camp after the flood.
3) Impact of event scale-revised (IES-R)
The IES-R is a 22-item scale in which respondents indicate their experiences over the past seven days using a response scale ranging from “never” (zero) to “very high” (four) [18]. This is composed of eight items related to avoidance symptoms, another eight items on intrusion and six items about hyperarousal symptoms. The range of scores from zero to 88 can be obtained from this scale, so that the higher the score, the more unfavorable the situation. Any individual with a score of 33 or more on the IES-R was defined as a case of PTSD; with a sensitivity of 91% and a specificity of 82% [19]. Panaghi and colleagues have reported acceptable validity and reliability of the Persian version of the scale [20].
Ethical considerations
Participants provided written informed consent, acknowledging the voluntary nature of their participation and the option to withdraw without consequences. The consent process covered confidentiality and the anonymized publication of results. The project received approval from the ethics committee of the Iran University of Medical Sciences (#IR.IUMS.REC.1398.718), adhering to the principles of the Declaration of Helsinki.
Statistical analysis
We analyzed the data using STATA version 11 (Stata Corporation, College Station, TX, USA). Continuous variables were represented by the mean and standard deviation or weighted standard error, whereas categorical variables were described using frequency and percentage. Principal component analysis was employed to estimate wealth index and level of damage to assets, considering ownership of assets and the percentage of flood damage to them, respectively [21]. In order to account for the multistage sampling method and non-response adjustment in the analysis, the “svyset” command was employed, introducing the provinces and clusters into the dataset. Sampling weights were computed to adjust each respondent’s representation to encompass other individuals within the study provinces. The post-stratification weights were determined by comparing the proportion of individuals within each stratum from the National Census 2016 to the corresponding proportion observed in the sample. These weights were calculated considering various factors such as age groups (divided into 5 categories), gender, and the 6 counties within the study provinces, resulting in the generation of 60 post-stratification weights. The final weights were determined by multiplying the inverse probability of unit selection into the sample with the post-stratification weights. Statistical tests, including Chi-square, t-test, one-way analysis of variance with Tukey post hoc, and logistic regression analysis, were employed to examine the associations between variables. In the logistic regression analysis, the Hosmer-Lemeshow method was used for modeling [22]. Variables that exhibited a p-value below 0.2 in the univariable models were included in the multiple model. Odds ratios, along with their corresponding 95% confidence intervals, were reported to assess the association between the variables and the outcomes. To ensure model validity, potential multicollinearity and interactions were assessed. The fitness of the models was evaluated using the Hosmer-Lemeshow goodness-of-fit test, specifically designed for complex survey data [23]. A p < 0.05 was used to determine statistical significance.
Results
Out of 2,305 people who were approached for surveys, 1,671 (72.5%) flood-affected adults from Golestan (560 of 786), Lorestan (558 of 780) and Khuzestan (553 of 739) provinces participated in the study, and their data were analyzed. The non-response group had a slightly higher mean age (38.9 vs. 36.8 years old) and included a higher percentage of men (81.4% vs. 19.2%). The mean age of participants was 36.8 ± 12.1 years and the minimum and maximum ages were 16 and 85 years, respectively. The majority of participants were housewives, married, illiterate or with primary education, and from rural areas. In regard to flood-related characteristics, 31.5% of participants reported that they temporarily lived in the camps after the flood and for 27%, the height of the flood entering the house was more than one meter. More than 42% of the participants suffered high damage to their assets by the flood and in 74% of the cases, the damage was not compensated. Table 1 shows the demographic and flood-related characteristics of the participants by province.
The prevalence of PTSD in the participants was 24.8% (CI 95%: 20.7–28.8%). PTSD was more prevalent in female (28.0%, CI 95%: 24.3–31.6%) than male participants (21.6%, CI 95%: 15.0-28.2%), but the difference was not statistically significant (P = 0.094). Table 2 shows the prevalence of PTSD in the studied provinces. The prevalence of PTSD was significantly higher in flood victims of Lorestan province (39.7%, P < 0.001). The distribution of IES-R score in the flooded provinces can be found in Fig. 1, which shows higher scores in Lorestan province. The highest prevalence of PTSD was observed in participants with a history of mental disorders (42%), followed by people who were exposed to the flood with a height of more than one meter and suffered high damage to their assets (40.7 and 37.8% respectively).
Determinants of PTSD, based on a multiple logistic regression model, were unemployment (adjusted odds ratio (AOR) = 3.53, CI 95%: 1.38-9.00), primary (AOR = 2.44, CI 95%: 1.10–5.41), or high school (AOR = 2.35, CI 95%: 1.25–4.40) education (vs. university), a history of mental disorders (AOR = 2.36, CI 95%: 1.22–4.58), high damage to assets (AOR = 2.29, CI 95%: 1.40–3.75), limited access to health care services after the flood (AOR = 1.95, CI 95%: 1.20–3.19), not receiving compensation for flood damage (AOR = 1.94, CI 95%: 1.01–3.83), high wealth index (AOR = 1.90, CI 95%: 1.23–2.93), and flooded house with a height of more than one meter (AOR = 1.66, CI 95%: 1.02–2.76) (Tables 3 and 4).

Violin plot for the distribution of IES-R scores in the flooded provinces
Discussion
The prevalence of post-traumatic stress disorder (PTSD) approximately 5 to 6 months after the massive flood of 2019 in Iran was estimated to be around 25%, with the highest prevalence observed in Lorestan province at 40%. This prevalence is near the average prevalence of PTSD in studies of various countries (29.5%), as reported by a systematic review and meta-analysis conducted by Golitaleb et al. in 2022 [24]. According to this review, the sole study concerning floods in Iran between 2015 and 2021 was the investigation conducted by Seyedin et al. [16]. This study examined the impact of the 2012 flood in Behshahr and Neka (Mazandaran province) with a random sample of 400 individuals, three months after the flood, using the PTSS-10 questionnaire and estimated the PTSD prevalence as 64%. A recently published study by Bastami et al. [17] reported a prevalence of PTSD one year after the 2019 flood in Lorestan province as 12.8%, using the Post-Traumatic Stress Disorder Checklist. The prevalence of PTSD has been reported in various populations in Iran, including the general population (2.1%) [25], earthquake victims (51.9% in Bam) [26], veterans, combatants, and freed soldiers (27.8%), and health system workers during the COVID era (14.6%) [27].
The high prevalence of PTSD among 2019 flood victims in Iran, particularly in Lorestan province, can be attributed to several factors. Firstly, the country has a pre-existing high prevalence of psychiatric disorders (23.6%), creating a baseline susceptibility [25]. Recent studies also indicate a rising trend in mental disorders, contributing to an increased burden [28]. Urban settings experience a growing frequency of stress, potentially amplifying vulnerability to PTSD [29, 30]. Economic issues and social factors further exacerbate mental health challenges [31, 32], highlighting the need for comprehensive strategies to address the impact of natural disasters on mental well-being in Iran.
The prevalence of PTSD in the present study was higher in women (28%), but there was no significant difference between two genders. Similarly, in a study on Malaysian flood victims, the higher prevalence of PTSD in women was not significant [33]. In the 2012 flood study in Mazandaran province [16], the PTSD score was significantly higher in men, but in the majority of studies, the female gender was significantly associated with PTSD [17, 34]. Differences in the characteristics and severity of floods, time interval, the demographic composition and context of the studied populations, and the methodologies employed contribute to these variations.
The highest prevalence of PTSD was seen in Lorestan province. Given that the intensity of the flood in Lorestan province was more than the other two provinces, this finding is consistent with the results that show a direct relationship between the intensity of the flood and the prevalence of PTSD [10, 35]. In the present study, the height of the water inundation was measured as one of the indicators of flood severity and it was correlated with the diagnosis of PTSD. The latter finding is consistent with the study of Waite et al. [10]. Several studies have emphasized that flood victims become more vulnerable when confronted with increasingly intense floods [34,35,36].
According to the present study, unemployment and low education were found to be associated with PTSD. The association of PTSD with low education is consistent with the findings of the assessment of Chinese flood victims in 2000 [37]. Higher education levels may enhance individuals’ knowledge, coping skills, and access to resources, potentially reducing the risk of developing PTSD [38, 39]. A study of PTSD in rural areas of Australia six months after river flooding revealed that socioeconomically marginalized people are more likely to be flooded and forced to leave their homes, and the risk of mental health and PTSD are also higher for cases of house, occupation, or farm inundation [13]. A study of Chinese flood victims also demonstrated that low level of social support is related to PTSD, 17 years after the flood [40] and people with weak social support are less likely to recover from this disorder after 13–14 years [41].
Considering the association between unemployment and PTSD, it is important to explore the possible causal relationship between the two variables. On one hand, the experience of flood trauma and subsequent job loss may contribute to the development of PTSD [42]. On the other hand, it is also plausible to consider that individuals may already have PTSD as a result of various factors following a disaster, which in turn could lead to unemployment [43]. Given the cross-sectional nature of the study and the potential for reverse causality, caution should be exercised when interpreting the observed relationships between unemployment and PTSD.
One of the consequences of the flood was the reduction of access to healthcare services, and this factor had a significant correlation with PTSD. A study by Waite et al. [10] also found in England that impaired access to health and social care, as well as education and work, was associated with PTSD.
In contrast to previous studies [34], the present study found a higher prevalence of PTSD among individuals with a high wealth index. This unexpected finding may be attributed to the fact that individuals who had greater assets prior to the flood may have experienced greater difficulties in coping with the aftermath of the disaster. The loss of their assets without the prospect of compensation could contribute to their heightened distress and lack of hope for recovery.
The results indicated that individuals with a history of mental disorders are more susceptible to developing PTSD following a traumatic event such as a flood. This finding underscores the importance of considering mental health history when prioritizing services and conducting PTSD screening for flood victims [34].
Apart from the obvious need to address the socio-economic situation of flood victims and plan to prevent future incidents, it is recommended to screen high-risk and vulnerable groups based on the factors obtained from the present study and prioritize resources for managing the mental health of this population. Considering the prolongation of PTSD after the huge flood, periodic screening of the affected population and the preparation of appropriate therapeutic and supportive interventions are recommended.
Limitations
One limitation is the lack of use of a diagnostic interview, which is often considered the gold standard for PTSD diagnosis. However, in studies with large sample sizes, it is usually neither cost-effective nor feasible to use this method. Nevertheless, the use of self-report questionnaires is inherently more biased than the diagnostic interview. We addressed this concern by employing a standardized and validated questionnaire, clarifying the study goals, and ensuring the participants about the confidentiality of the findings.
The study acknowledges a potential source of error in the data collection process attributed to the practices of 18 data collectors. To address this issue, they received training based on an executive protocol. Despite these efforts, the study recognizes the inherent subjectivity in questioning as a limitation.
The flood and the destruction of some houses caused the displacement of a number of people and their withdrawal from the sampling process. Paying attention to the fact that the prevalence of PTSD in this group of people is usually higher, it can lead to an underestimation of this disorder. When generalizing the results, it is essential to take into account the study setting and the characteristics of the participants.
Conclusion
In conclusion, our study highlights a concerning prevalence of PTSD, particularly in Lorestan province, among adults affected by severe flooding in Iran. Independent determinants of PTSD include unemployment, lower education, a psychiatric history, extensive property damage, limited post-flood healthcare access, lack of compensation, and greater flood exposure. We recommend adopting an inclusive screening approach for high-risk groups based on identified factors, prioritizing resources for mental health management, and developing appropriate therapeutic and supportive interventions.
Data availability
The data that support the findings of this study are available from the corresponding author, upon reasonable request.
Abbreviations
- PTSD:
-
Post-traumatic Stress Disorder
- IES-R:
-
Impact of Event Scale-Revised
- CI:
-
Confidence Interval
- AOR:
-
Adjusted Odds Ratio
- COR:
-
Crude Odds Ratio
References
Shaikh Baikloo Islam B. Evidence and consequences of the flood in Iran from prehistory to the present. Water Soil Manage Model. 2021;1(1):24–40. https://doi.org/10.22098/mmws.2021.1173.
Alifu H, Hirabayashi Y, Imada Y, Shiogama H. Enhancement of river flooding due to global warming. Sci Rep. 2022;12(1):20687. https://doi.org/10.1038/s41598-022-25182-6.
Moayeri M, Entezari M. Floods and review floods in province of Esfahan. J Stud Hum Settl Plann. 2008;3(6):110–24. https://jshsp.rasht.iau.ir/article_522468.html?lang=en.
Modarres R, Sarhadi A, Burn DH. Changes of extreme drought and flood events in Iran. Global Planet Change. 2016;144:67–81. https://doi.org/10.1016/j.gloplacha.2016.07.008.
Seddighi H, Seddighi S. How much the Iranian government spent on disasters in the last 100 years? A critical policy analysis. Cost Eff Resour Alloc. 2020;18(1):46. https://doi.org/10.1186/s12962-020-00242-8.
Aminyavari S, Saghafian B, Sharifi E. Assessment of precipitation estimation from the NWP models and satellite products for the spring 2019 severe floods in Iran. Remote Sens. 2019;11(23):2741. https://doi.org/10.3390/rs11232741.
Shokri A, Sabzevari S, Hashemi SA. Impacts of flood on health of Iranian population: infectious diseases with an emphasis on parasitic infections. Parasite Epidemiol Control. 2020;9:e00144. https://doi.org/10.1016/j.parepi.2020.e00144.
Khankeh H, Kolivand P, Ahmadi S, Farzinnia B, Bazyar J. Health System Response and Management: lessons learned from Iran’s 2019 floods. Health Emerg Disasters Q. 2020;5(4):227–36. https://doi.org/10.32598/hdq.5.4.355.1.
Sharifi L, Bokaie S. Priorities in prevention and control of flood hazards in Iran 2019 massive flood. Iran J Microbiol. 2019;11(2):80–4. https://doi.org/10.18502/ijm.v11i2.1065.
Waite TD, Chaintarli K, Beck CR, Bone A, Amlôt R, Kovats S, Reacher M, Armstrong B, Leonardi G, Rubin GJ, et al. The English national cohort study of flooding and health: cross-sectional analysis of mental health outcomes at year one. BMC Public Health. 2017;17(1):129. https://doi.org/10.1186/s12889-016-4000-2.
Asim M, Mekkodathil A, Sathian B, Elayedath R, N RK, Simkhada P, van Teijlingen E. Post-traumatic stress disorder among the flood affected population in Indian subcontinent. Nepal J Epidemiol. 2019;9(1):755–8. https://doi.org/10.3126/nje.v9i1.24003.
Nöthling J, Gibbs A, Washington L, Gigaba SG, Willan S, Abrahams N, Jewkes R. Change in emotional distress, anxiety, depression and PTSD from pre- to post-flood exposure in women residing in low-income settings in South Africa. Arch Womens Ment Health. 2023. https://doi.org/10.1007/s00737-023-01384-3.
Matthews V, Longman J, Berry HL, Passey M, Bennett-Levy J, Morgan GG, Pit S, Rolfe M, Bailie RS. Differential mental health impact six months after extensive river flooding in rural Australia: a cross-sectional analysis through an equity lens. Front Public Health. 2019;7:367. https://doi.org/10.3389/fpubh.2019.00367.
Heo JH, Kim MH, Koh SB, Noh S, Park JH, Ahn JS, Park KC, Shin J, Min S. A prospective study on changes in health status following flood disaster. Psychiatry Investig. 2008;5(3):186–92. https://doi.org/10.4306/pi.2008.5.3.186.
Tiyuri A, Rasoulian M, Hajebi A, Naserbakht M, Shabani A, Hakim Shooshtari M, Rezapour A, Motevalian SA. Psychological impact of the Spring 2019 flood among adult population of Iran. Int J Soc Psychiatry. 2023;69(8):1916–27. https://doi.org/10.1177/00207640231180824.
Seyedin H, HabibiSaravi R, sayfouri N, Hoseini Djenab V, Ghasemi Hamedani F. Psychological sequels of flood on residents of southeast Caspian region. Nat Hazards. 2017;88(2):965–75. https://doi.org/10.1007/s11069-017-2926-z.
Bastami F, Mohammadi R, Piri ZA, Valipour E, Ahmadi P, Almasian M, Nouraei Motlagh S. Prevalence of post-traumatic stress disorder and its relationship with coping strategies among flood victims: evidence from Iran. 2024, 15:100704. https://doi.org/10.1016/j.jadr.2023.100704. https://www.sciencedirect.com/science/article/pii/S266691532300241X.
Weiss DS, Marmar CR. The impact of event Scale—revised. Assessing psychological trauma and PTSD. edn. New York, NY, US: The Guilford Press; 1997. pp. 399–411.
Creamer M, Bell R, Failla S. Psychometric properties of the impact of event scale - revised. Behav Res Ther. 2003;41(12):1489–96. https://doi.org/10.1016/j.brat.2003.07.010.
Panaghi L, Hakim Shooshtari M, Atari Mogadam J. Persian version validation in impact of event scale-revised. Tehran Univ Med J. 2006;64(3):52–60. http://tumj.tums.ac.ir/article-1-974-en.html.
Filmer D, Pritchett LH. Estimating wealth effects without expenditure data–or tears: an application to educational enrollments in states of India. Demography. 2001;38(1):115–32. https://doi.org/10.1353/dem.2001.0003.
Hosmer DW, Lemeshow S, Sturdivant RX. Applied logistic regression. Wiley; 2013. https://books.google.ru/books?id=64JYAwAAQBAJ.
Archer KJ, Lemeshow S. Goodness-of-fit test for a logistic regression model fitted using survey sample data. Stata J. 2006;6(1):97–105. https://doi.org/10.1177/1536867x0600600106.
Golitaleb M, Mazaheri E, Bonyadi M, Sahebi A. Prevalence of post-traumatic stress disorder after flood: a systematic review and meta-analysis. Front Psychiatry. 2022;13:890671. https://doi.org/10.3389/fpsyt.2022.890671.
Sharifi V, Amin-Esmaeili M, Hajebi A, Motevalian A, Radgoodarzi R, Hefazi M, Rahimi-Movaghar A. Twelve-month prevalence and correlates of psychiatric disorders in Iran: the Iranian Mental Health Survey, 2011. Arch Iran Med. 2015;18(2):76–84. http://journalaim.com/Article/778.
Farhoudian A, Sharifi V, Rahimi Movaghar A, Radgoudarzi R, Mohammadi M, Younesian M, Yasami M. The prevalence of posttraumatic stress disorder and its symptoms among bam earthquake survivors. Adv Cogn Sci. 2006;8(3):58–70. https://icssjournal.ir/article-1-211-en.html
Keyhani A, Rahnejat AM, Dabaghi P, Taghva A, Ebrahimi MR, Nezami Asl A. Prevalence of post-traumatic stress disorder among the healthcare workers involved with Covid-19 treatment and its effective factors in military hospitals of Iran. Iran J War Public Health. 2023;15(1):61–6. https://doi.org/10.58209/ijwph.15.1.61.
Taheri Mirghaed M, Abolghasem Gorji H, Panahi S. Prevalence of psychiatric disorders in Iran: a systematic review and meta-analysis. Int J Prev Med. 2020;11:21. https://doi.org/10.4103/ijpvm.IJPVM_510_18.
Tavangar F, Ghaedamini Harouni G, Noorbala AA, Nosrati Nejad F, Mohammadi Gharehghani MA, Rafiey H. Inequality in the experience of stressful psychological events: evidence from a regional survey in Tehran. Med J Islam Repub Iran. 2022;36:22. https://doi.org/10.47176/mjiri.36.22.
Tavangar F, Ghaedamini Harouni G, Nosrati Nejad F, Noorbala A, Rafiey H. Stressful events distribution in regions of Tehran based on geographic information system. Zanko J Med Sci. 2021;22(73):26–35. http://zanko.muk.ac.ir/article-1-577-en.html.
Mohamadnejad N, Faraji Dizaji S. The poverty and mental health association in Iran. Iran Econ Rev. 2019;23(3):533–59. https://doi.org/10.22059/ier.2019.71778.
Dini Torkamani A. An explanation for falling of social capital in Iran. Soc Welf. 2007;6(23):147–72. http://refahj.uswr.ac.ir/article-1-1966-en.html.
San SO, Amin RBM, Abd Aziz AB, Aung MMT. Prevalence and perceived severity of post-traumatic stress disorder among flood victims in Kuala Terengganu, Malaysia. Malays J Public Health Med. 2016;16(2):30–40. http://wprim.whocc.org.cn/admin/article/articleDetail?WPRIMID=626815&articleId=626815.
Chique C, Hynds P, Nyhan MM, Lambert S, Boudou M, O’Dwyer J. Psychological impairment and extreme weather event (EWE) exposure, 1980–2020: a global pooled analysis integrating mental health and well-being metrics. Int J Hyg Environ Health. 2021;238:113840. https://doi.org/10.1016/j.ijheh.2021.113840.
Huang P, Tan H, Liu A, Feng S, Chen M. Prediction of posttraumatic stress disorder among adults in flood district. BMC Public Health. 2010;10:207. https://doi.org/10.1186/1471-2458-10-207.
Chen L, Liu A. The incidence of posttraumatic stress disorder after floods: a meta-analysis. Disaster Med Public Health Prep. 2015;9(3):329–33. https://doi.org/10.1017/dmp.2015.17.
Mulchandani R, Armstrong B, Beck CR, Waite TD, Amlôt R, Kovats S, Leonardi G, Rubin GJ, Oliver I. The English National Cohort Study of Flooding & Health: psychological morbidity at three years of follow up. BMC Public Health. 2020;20(1):321. https://doi.org/10.1186/s12889-020-8424-3.
Li L, Reinhardt JD, Van Dyke C, Wang H, Liu M, Yamamoto A, Chen Q, Hu X. Prevalence and risk factors of post-traumatic stress disorder among elderly survivors six months after the 2008 Wenchuan earthquake in China. BMC Psychiatry. 2020;20(1):78. https://doi.org/10.1186/s12888-020-2474-z.
Tang B, Deng Q, Glik D, Dong J, Zhang L. A meta-analysis of risk factors for post-traumatic stress disorder (PTSD) in adults and children after earthquakes. Int J Environ Res Public Health. 2017;14(12). https://doi.org/10.3390/ijerph14121537.
Dai W, Kaminga AC, Tan H, Wang J, Lai Z, Wu X, Liu A. Long-term psychological outcomes of flood survivors of hard-hit areas of the 1998 Dongting Lake flood in China: prevalence and risk factors. PLoS ONE. 2017;12(2):e0171557. https://doi.org/10.1371/journal.pone.0171557.
Dai W, Wang J, Kaminga AC, Chen L, Tan H, Lai Z, Deng J, Liu A. Predictors of recovery from post-traumatic stress disorder after the dongting lake flood in China: a 13–14 year follow-up study. BMC Psychiatry. 2016;16(1):382. https://doi.org/10.1186/s12888-016-1097-x.
Peek-Asa C, Ramirez M, Young T, Cao Y. Flood-related work disruption and poor health outcomes among university students. Prehosp Disaster Med. 2012;27(6):503–8. https://doi.org/10.1017/s1049023x1200129x.
Serrano C, Leiva-Bianchi M, Ahumada F, Araque-Pinilla F. What is the association between post-traumatic stress disorder and unemployment after a disaster? Int J Occup Med Environ Health. 2021;34(6):755–66. https://doi.org/10.13075/ijomeh.1896.01557.
Acknowledgements
The authors appreciate the help of Dr. Hadi Khaniki, Dr. Seyyed Hossein Serajzadeh, Dr. Abbas Ghanbari-Baghestan, Dr. Mohammad Fazeli, Dr. Reza Davasaz Irani, Dr. Noushin Ahmadpourian and Dr. Mousaalreza Shabihi in conducting the project. The authors are also grateful to the interviewers and all study participants.
Funding
This research was commissioned and funded by the Special Commission for National Report on Floods and was a part of the Ph.D. dissertation of the corresponding author, supported by Iran University of Medical Sciences (No. 17255).
Author information
Authors and Affiliations
Contributions
SA.M and A.T designed the study. All authors collaborated in developing the study protocol, monitoring the study, and data collection in the provinces. M.R was head of the mental health committee and principal investigator. SA.M and A.T analyzed the data. All authors collaborated in interpreting the data. A.S and A.T wrote the draft of the manuscript. All authors critically reviewed the manuscript for important intellectual content and provided their consent for publication.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Written informed consent was obtained to fulfill ethical considerations. The project, approved by the ethics committee of Iran University of Medical Sciences (#IR.IUMS.REC.1398.718), adhered to the principles of the Declaration of Helsinki throughout the study.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Shabani, A., Rasoulian, M., Naserbakht, M. et al. Prevalence and determinants of post-traumatic stress disorder five months after the 2019 huge flooding in Iran. BMC Public Health 24, 346 (2024). https://doi.org/10.1186/s12889-024-17861-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12889-024-17861-y