
Abstract
Background
Hyperlipidemia is a major risk factor for many diseases. Previous studies have shown that diet is closely associated with hyperlipidemia. However, the relationship between cooking methods and hyperlipidemia remains unclear. The objective of this study was to identify the major cooking patterns existing in the Eastern Chinese population and evaluate their association with the prevalence of hyperlipidemia.
Methods
We interviewed 4,710 residents in Eastern China regarding the consumption frequency of each cooking method when they prepare food at home or when eating out and regarding the prevalence of hyperlipidemia. Factor analysis, Chi-square tests, analysis of variance, and binary logistic regression analysis were used to identify the cooking patterns and analyze the characteristics of participants’ categories of cooking patterns and the relationship between different cooking patterns and prevalence of hyperlipidemia.
Results
Three major cooking patterns were identified: Traditional Chinese, Bland (little or no oil is used to process the food), and High-temperature cooking patterns. After controlling for potential confounders, participants in the highest quartile of the Bland cooking pattern had lower odds of hyperlipidemia than those in the lowest quartile. Nevertheless, no significant associations were observed between the Traditional Chinese and High-temperature cooking patterns and the prevalence of hyperlipidemia.
Conclusions
This study confirms the association between cooking patterns and the prevalence of hyperlipidemia and indicates that the Bland cooking pattern is associated with a reduced prevalence of hyperlipidemia.
Similar content being viewed by others

Background
Hyperlipidemia is a major risk factor for cardiovascular disease (CVD), which is the leading cause of morbidity and mortality globally [1]. In addition, recent studies have shown that hyperlipidemia is also a risk factor for bladder cancer [2], breast cancer [3], and enlargement of the prostate [4].
According to the Annual Report on Cardiovascular Health and Diseases in China (2019), total cholesterol (TC), triglycerides (TG), and low-density lipoprotein cholesterol (LDL-C) significantly increased in Chinese adults over the age of 18 between 2002 and 2015, while high-density lipoprotein cholesterol (HDL-C) significantly decreased. Moreover, the overall prevalence of dyslipidemia (defined as the presence of any type of dyslipidemia) in Chinese individuals ≥ 18 years of age was 8.6%, 34.0%, 39.91%, and 40.4% in 2002, 2010, 2011, and 2012, respectively, showing an increasing trend [5].
Diet is closely related to hyperlipidemia [6, 7], and dietary patterns have been significantly associated with hyperlipidemia [8, 9]. Cooking methods modify the organoleptic conditions of foods, making them more palatable and influencing the bioavailability of nutrients, vitamins, and minerals [10]. Some cooking methods such as frying not only increase fat and energy content but also modify food composition. For example, frying food causes water to be replaced by fat, and deep frying results in an increase in trans-fatty acids [11]. Studies have found that frequent consumption of fried foods is associated with a higher risk of hypertension [12], and the social business cooking patterns have shown a relationship with inflammatory and cardio-metabolic health biomarkers [13]. However, the relationship between cooking patterns and hyperlipidemia is unclear.
Over the years, the Chinese people have developed many distinct and unique cooking methods. Data show that there are more than 30 kinds of basic cooking techniques commonly used in China [14]. However, as far as we have been able to determine, no previous study has assessed the association between cooking patterns and the prevalence of hyperlipidemia among the Chinese population.
Eastern China encompasses Jiangsu, Shandong, Anhui, Zhejiang, and Fujian Provinces, as well as the city of Shanghai, and its regional cuisine holds an important position in the culture of Chinese cuisine. Eastern China is home to five of China’s eight major cuisines [15]. Therefore, studies related to cooking performed in Eastern China are useful for guiding decision-making and policymaking nationwide.
The present study identified the major cooking patterns existing in the Eastern Chinese population and evaluated their association with the prevalence of hyperlipidemia.
Materials and methods
Study population
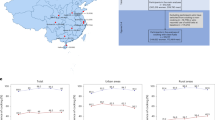
The present cross-sectional study was conducted in Eastern China from March to June 2021. The sample was selected by a stratified cluster random-sampling method. Two cities were randomly selected from each province. In each selected city, two residential areas were randomly selected for sampling. Between180 and240 residents were recruited from each residential area (Fig. 1). Those who agreed to participate completed a face-to-face interview using a standardized questionnaire (see Appendix) conducted by five trained research assistants. Interviews were conducted at the entrance of each residential area in the afternoon at the end of a normal workday. The average interview lasted approximately 15 min per participant. Upon completion of the interview, each participant received a small gift worth approximately 5 Chinese yuan. A total of 4,710 participants completed interviews, for a response rate of 98.1%. Only 90 residents refused to participate or did not complete the interview, citing lack of time or no recent routine physical examination [16].

Flow chart showing the sampling process
Assessment of cooking methods
Based on The Comprehensive Cooking Techniques of China [14] and traditional cooking techniques frequently used by residents of the surveyed provinces and cities in East China [15], we summarized 15 major cooking methods. These consisted of stir-fry and sauté (put a small amount of oil in a pan and cook food quickly over high heat, stirring and turning the pan), boiling (to cook in water or liquids when the temperature is at boiling point), steaming (to cook using vapor), pan-frying (to cook food in a pan with the minimum amount of oil), roasting (to cook in an oven using hot air or radiation, which cooks the food evenly), deep-frying (to cook food in hot oils when the food is totally immersed), stewing (to boil slowly or simmering in a liquid for a long period of time at low heat), marinated in spirits (to soak food in liquor or rice wine for sterilization through pickling), blanching (food is put in boiling water, turned and removed in time, and then sautéed), poaching (to cook the food in boiling water for a short time, remove and pour into a bowl, add fresh clear soup, then season), mixed in soy sauce (to process food into strips or sheets, put into boiling water or hot oil, remove and season), stir-frying and fast-sautéing (to cook small foods in boiling oil or water quickly (about 10 s)), simmer and keep the shape (arrange the raw materials in a neat pattern, add the right amount of stock and condiments and gently heat until mature, keeping the shape), deep-fry first, then season with sauce (fry food materials over high heat until yellow and stiff, then season with sauce), marinated in rice wine (marinate raw materials in rice wine).
Participants were asked to report their adoption and consumption frequency of each cooking method when they prepare food at home or eating out in the previous 12 months (Never eating = 1, Eating occasionally = 2, Sometimes eating = 3, Often eating = 4, and Eating every day = 5).
Identification of cooking patterns
The Kaiser-Meyer-Olkin (KMO) measure of sampling adequacy and Bartlett’s test of sphericity were used to evaluate the adequacy of correlation matrices with the data. Factor analysis (principal component) was used to derive the major cooking patterns. The factors were rotated using orthogonal transformation (varimax rotation) to achieve uncorrelated factors and greater interpretability. The number of factors retained was determined by an eigenvalue ≥ 1. Cooking groups with an absolute factor loading ≥ 0.6 were considered important contributors to this pattern.
The labeling of cooking patterns was based on the interpretation of cooking methods with high factor loading on each pattern. Quartiles based on factor scores were determined for each cooking pattern (Q1 represented a low intake of the food by the cooking pattern; Q4 represented a high intake of the food by the cooking pattern).
Definition of variables
Standing height and body weight were measured without shoes and in light clothes by trained researchers. Body mass index (BMI, kg/m2) was calculated as weight in kilograms divided by height in meters squared. Physical activity and hyperlipidemia were obtained through self-reporting. Participants’ physical activity levels were assessed using the International Physical Activity Questionnaire (IPAQ) [17]. The metabolic equivalent of task (MET) level for each reported activity was calculated based on its duration (hours) per week. Participants were then grouped into one of three categories: Light (< 3 MET), Moderate (3–6 MET), or Vigorous (> 6 MET) [18]. Additionally, their hyperlipidemia diagnosis (yes/no) was recorded based on their most recent doctor visit or a routine physical examination within the past year. Participants reported their gender, age, education level, and total monthly household income.
Statistical analyses
Data were calculated across quartiles for each cooking pattern score and are presented as the mean and standard deviation for continuous variables, or as number and percentage for categorical variables. The Chi-square test was used to assess the differences for categorical variables, while the analysis of variance (ANOVA) was used to describe mean differences for continuous variables. After adjusting for confounders, binary logistic regression analysis was used to estimate the odds ratio (OR) and 95% CI for hyperlipidemia according to quartiles of each cooking pattern score (the first quartile of each pattern was used as the reference group). All statistical analyses were performed using the statistical package SPSS version 21.0, and 2-tailed P-values < 0.05 were considered statistically significant.
Results
The overall prevalence of hyperlipidemia in this population was 3.8%. In males it was 2.4%, and in females it was 1.4%. The participant characteristics with and without hyperlipidemia are shown in Table 1. There were significant differences between participants with and without hyperlipidemia by gender, age, education, income, physical activity, and BMI.
Both the Kaiser-Meyer-Olkin index (0.901) and Bartlett’s test (P < 0.001) indicated that the correlation among the variables was sufficiently strong for a factor analysis. Factor analysis identified three cooking patterns: the Traditional Chinese cooking pattern (high-frequency consumption of food Marinated in spirits, Blanching, Poaching, Mixed in soy sauce, Stir-frying and fast-sautéing, Simmer and keep the shape, Deep-fry first, then season with sauce, and Marinated in rice wine; the Bland cooking pattern (high-frequency consumption of Stir-frying and sautéing, Boiling, Steaming, and Stewing); and the High-temperature cooking pattern (high-frequency consumption of Pan-frying, Roasting, and Deep-frying). These patterns explained 30.0%, 15.2%, and 14.5% of the cooking method consumption variance. The factor loading matrices for the cooking patterns are provided in Table 2.
The characteristics of the study participants by quartiles of cooking pattern scores are shown in Table 3. Participants within the top quartile of the Traditional Chinese pattern were male and younger, with higher education and monthly income, and undertook moderate physical activity; more people had no hyperlipidemia and had higher BMI compared with participants in the lowest quartile. Compared with those in the lowest quartile, participants in the highest quartile of the Bland cooking pattern were female and older, had higher education and monthly income, and undertook light physical activity. Furthermore, we also found that participants in the highest quartile of the High-temperature cooking pattern were male and younger, had lower education and monthly income, undertook moderate physical activity, had no hyperlipidemia, and had lower BMI than those in the lowest quartile.
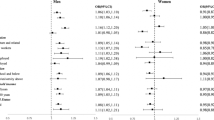
The associations between cooking patterns and the prevalence of hyperlipidemia by logistic regression analysis are presented in Table 4. After adjusting for potential confounding variables, participants in the highest quartile of the Bland cooking pattern had lower odds of hyperlipidemia (OR = 0.59, 95% CI 0.37, 0.94; P < 0·05) than those in the lowest quartile. In addition, no significant associations between Traditional Chinese and High-temperature cooking patterns and the prevalence of hyperlipidemia were observed.
Discussion
In this study of the Eastern Chinese population, the prevalence of hyperlipidemia was low (3.8%), which may be related to the self-report method used in this survey. We identified three major cooking patterns: Traditional Chinese, Bland, and High temperature. The Bland cooking pattern was inversely associated with the prevalence of hyperlipidemia. To the best of our knowledge, the present study is the first to examine the relationship between major cooking patterns and the prevalence of hyperlipidemia in the Chinese population.
This study found that the proportion of male respondents suffering from hyperlipidemia was significantly higher than that of female respondents, and the proportion of respondents in the 46–55 age group suffering from hyperlipidemia was significantly higher compared to other age groups. This was consistent with Annual Report on Cardiovascular Health and Diseases in China (2019) [5]. Our study further found that the proportion of undergraduate college respondents suffering from hyperlipidemia was significantly higher than that of respondents who attained other education levels, and the proportion of respondents with monthly family income (Chinese Yuan) of 5,000–19,999 suffering from hyperlipidemia was significantly higher than that of respondents at other income levels.
In the present study, the traditional Chinese cooking pattern was characterized by a high-frequency consumption of Marinated in spirits, Blanching, Poaching, Mixed in soy sauce, Stir-frying and fast-sautéed, Simmer and keep the shape, Deep-fry first then season with sauce, and Marinated in rice wine. In our data, no significant association was observed between this pattern and the prevalence of hyperlipidemia, and participants with more Traditional Chinese cooking patterns had a lower rate of hyperlipidemia. One possible explanation is that less oil is used as a medium for heating food in the above cooking methods, although previous studies have shown that lipid intake can be a risk factor for hyperlipidemia [6]. Oil is used to heat food for a shorter time in the cooking method of Mixed in soy sauce and Stir-frying and fast-sautéing cooking methods. Additionally, spirits and rice wine are used to treat foods in the method of Marinated in spirits and Marinated in rice wine methods. There have been no reports of hyperlipidemia associated with small amounts of alcohol used during cooking.
The Bland cooking pattern was characterized by a high-frequency consumption of Stir-frying and sautéing, Boiling, Steaming, and Stewing. Steaming, Boiling, and Stewing mainly rely on water vapors or water to transfer heat [19]. In our analyses, we observed an inverse association between the Bland cooking pattern and the prevalence of hyperlipidemia. Our findings align with those of a previous study that reported a significant association of a high consumption of deep-fried foods and a low intake of steamed, boiled, and raw food with hyperlipidemia [8]. Another related study also showed that boiling and sautéing, brining, and light frying tend to have cardio-metabolic benefits [13]. One possible mechanism for this is that steaming increases the concentration of polyphenols and antioxidants [20], and dietary polyphenols can lower LDL-C levels [21]. Additionally, in a comparison of the effects of steaming, oven cooking, and deep fat-frying on the physicochemical and sensory quality of turkey meat patties, steamed patties showed the lowest shrinkage and fat content [22].
The High-temperature cooking pattern is characterized by the frequent use of pan-frying, roasting, and deep-frying techniques. Frying relies on oil to transfer heat, and roasting typically involves cooking on an open flame or baking using coal, firewood, or charcoal during fire roasting [19]. In our study, no significant association was found between the High-temperature cooking pattern and the prevalence of hyperlipidemia. Our findings contrast with previous studies reporting that a low-cholesterol and low-fat (particularly saturated fat) diet is beneficial for managing hyperlipidemia [23]. In addition, the frequent consumption of fried foods has been linked to a higher prevalence of hypertension [12]. However, other studies have shown that dietary cholesterol consumption is not necessarily associated with dyslipidemia or serum lipids [24] and that a high intake of deep-fried foods has no association with components of dyslipidemia [9]. Moreover, some research reports a lack of association between dietary cholesterol intake with dyslipidemia, hypertriglyceridemia, and HDL-hypocholesterolemia [25]. While the cooking method is different from the diet itself, it can still affect the bioavailability of nutrients, vitamins, and minerals in food [10]. Additionally, the absence of data on the categories of food consumed daily by participants leads us to miss important confounders in the relationships between cooking patterns and hyperlipidemia. Therefore, further study should explore this more deeply.
The present study had some limitations. First, because of the cross-sectional design of the study, we could not assess the causal association between cooking patterns and the prevalence of hyperlipidemia. Therefore, further prospective studies are needed to confirm this finding. Second, hyperlipidemia was established by self-report rather than by a clinician-administered structured diagnostic test, and hyperlipidemia may be inaccurately reported by participants. More studies (including clinical trials) are necessary to evaluate the association between cooking patterns and their association with the incidence of hyperlipidemia. Third, the recall method used in the evaluation of cooking methods may lead to some degree of misclassification. Fourth, although various confounders were considered, we could not discount residual confounding. Finally, the study participants were recruited in Eastern China. Therefore, our results may not be generalizable to the entire Chinese population.
Conclusions
We identified three major cooking patterns, namely the Traditional Chinese, Bland, and High-temperature cooking patterns. Our results demonstrate that the Bland cooking pattern is associated with a reduced prevalence of hyperlipidemia. Present findings provide further insight into understanding the associations between cooking patterns and hyperlipidemia. Further longitudinal studies and trials are required to elucidate whether a true causal association exists.
Data availability
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
References
Global Burden of Disease Collaborative Network: Global Burden of Disease Study 2017. (GBD 2017) Results. In. Seattle: United States: Institute for Health Metrics and Evaluation (IHME); 2018.
Shih HJ, Lin KH, Wen YC, Fan YC, Tsai PS, Huang CJ. Increased risk of Bladder cancer in young adult men with hyperlipidemia: a population-based cohort study. Med (Baltim). 2021;100(48):e28125.
Chowdhury FA, Islam MF, Prova MT, Khatun M, Sharmin I, Islam KM, Hassan MK, Khan MAS, Rahman MM. Association of hyperlipidemia with breast cancer in Bangladeshi women. Lipids Health Dis. 2021;20(1):52.
Erbay G, Ceyhun G. Association between hyperlipidemia and prostatic enlargement: a case-control study. Urologia. 2022;89(1):58–63.
Annual Report on Cardiovascular Health and Diseases in China (2019).
Bevilacqua MA, Gimeno SGA, Matsumura LK, Ferreira SRG, Japanese Brazilians Diabet Study G. Hyperlipidemias and dietary patterns: transversal study of Japanese brazilians. Arq Bras Endocrinol Metabol. 2007;51(4):547–58.
Clifton PM. Diet, exercise and weight loss and dyslipidaemia. Pathology. 2019;51(2):222–6.
Lin P, Chang CC, Yuan KC, Yeh HJ, Fang SU, Cheng T, Teng KT, Chao KC, Tang JH, Kao WY et al. Red blood cell aggregation-associated dietary pattern predicts hyperlipidemia and metabolic syndrome. Nutrients 2018;10(8).
Lin LY, Hsu CY, Lee HA, Wang WH, Kurniawan AL, Chao JCJ. Dietary patterns in relation to components of dyslipidemia and fasting plasma glucose in adults with dyslipidemia and elevated fasting plasma glucose in Taiwan. Nutrients 2019, 11(4).
Barzegar F, Kamankesh M, Mohammadi A. Heterocyclic aromatic amines in cooked food: a review on formation, health risk-toxicology and their analytical techniques. Food Chem. 2019;280:240–54.
Boskou G, Salta FN, Chiou A, Troullidou E, Andrikopoulos NK. Content of trans,trans-2,4-decadienal in deep-fried and pan-fried potatoes. Eur J Lipid Sci Technol. 2006;108:109–15.
Sayon-Orea C, Bes-Rastrollo M, Gea A, Zazpe I, Basterra-Gortari FJ, Martinez-Gonzalez MA. Reported fried food consumption and the incidence of hypertension in a mediterranean cohort: the SUN (Seguimiento Universidad De Navarra) project. Br J Nutr. 2014;112(6):984–91.
Moreno-Franco B, Rodriguez-Ayala M, Donat-Vargas C, Sandoval-Insausti H, Rey-Garcia J, Lopez-Garcia E, Banegas JR, Rodriguez-Artalejo F, Guallar-Castillon P. Association of cooking patterns with inflammatory and cardio-metabolic risk biomarkers. Nutrients. 2021;13(2):633.
Chinese Cuisine Association and Japanese Chinese Cuisine Association. Comprehensive of Chinese cooking techniques. Shanghai: Shanghai Lexicographical Publishing House; 2004.
Wang F, Peng J, Ma J, Cui B. Regional differences and changing trends of cooking style preferences: based on survey data in East China. J Researches Diet Sci Cult. 2022;39(02):52–8.
Cui B, Wang LD-L, Wang FR, Peng J, Ma JY, Chen X, Xu MY, Ke J, Tian Y. Correlation between dietary information sources and knowledge of adequate diets in Eastern China. Front Public Health. 2022;10:955766–6.
Craig CL, Marshall AL, Sjöström M, Bauman AE, Booth ML, Ainsworth BE, Pratt M, Ekelund U, Yngve A, Sallis JF, et al. International physical activity questionnaire: 12-country reliability and validity. Med Sci Sports Exerc. 2003;35(8):1381–95.
Ainsworth BE, Haskell WL, Whitt MC, Irwin ML, Swartz AM, Strath SJ, O’brien WL, Bassett DR, Schmitz KH, Emplaincourt PO. Compendium of physical activities: an update of activity codes and MET intensities. Med Sci Sports Exerc. 2000;32(9):498–S516.
Wang Y, Li A, Chen DP. Status and prospects of nutritional cooking. Food Qual Saf. 2019;3(3):137–43.
Dolinsky M, Agostinho C, Ribeiro D, Rocha GD, Barroso SG, Ferreira D, Polinati R, Ciarelli G, Fialho E. Effect of different cooking methods on the polyphenol concentration and antioxidant capacity of selected vegetables. J Culin Sci Technol. 2016;14(1):1–12.
Sun P, Zhao L, Zhang N, Zhou J, Zhang L, Wu W, Ji B, Zhou F. Bioactivity of Dietary polyphenols: the role in LDL-C lowering. Foods 2021, 10(11).
Yadav S, Effect of different cooking methods on quality characteristics of Turkey meat patties. Veterinary Practitioner. 2008;9(2):168–70.
Sum CF, Tan CE, Chew LS. Management of hyperlipidaemia. Singapore Med J. 1995;36(4):410–6.
Pan JQ, Han WQ, Jiang YR, Wu JN, Zhou X. Association of dietary cholesterol and dyslipidemia in Chinese health examinees. J Health Popul Nutr 2022, 41(1).
Huang QM, Jiang HR, Zhang B, Wang HJ, Jia XF, Huang FF, Wang LS, Wang ZH. Threshold-effect association of dietary cholesterol intake with dyslipidemia in Chinese adults: results from the China health and nutrition survey in 2015. Nutrients. 2019;11(12).
Acknowledgements
Not applicable.
Funding
This research was supported by the Open Project Program of Jiangsu Key Laboratory of Zoonosis (No: R2004) and the Chinese Nutrition Society–Nutrition Science Popularization and Communication Research Fund (CNS-SCP2020-122).
Author information
Authors and Affiliations
Contributions
B.C: conceptualization, methodology, investigation, data curation, writing—original draft. W.K.Y: software, investigation, writing—review and editing. L.D.W: software, investigation, writing—review and editing. F.R.W: investigation, writing—review and editing. J.P: investigation, writing—review and editing. J.Y.Ma: investigation, writing—review and editing. X.C: investigation, writing—review and editing. M.Y.X: investigation, writing—review and editing. J.K: investigation, writing—review and editing. Y.T: investigation, writing—review and editing. All authors have read and agreed to the published version of the manuscript. All authors reviewed the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Ethical approval was obtained from the Ethics Committee of the Collaborative Innovation Research Center for Public Health Management at Yangzhou University. The ethical approval reference number is YGWLL-2021-004. The researchers received the informed consent of the subjects involved in this study. All procedures were conducted in accordance with the Declaration of Helsinki.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Supplementary Material 1:
Questionnaire
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Cui, B., Yuan, W.K., Wang, L.DL. et al. Association between cooking patterns and the prevalence of hyperlipidemia in Eastern China. BMC Public Health 24, 75 (2024). https://doi.org/10.1186/s12889-023-17549-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12889-023-17549-9