
Abstract
Background
The association between muscle defects and hypertension is well-established. However, the absence of pertinent and uncomplicated clinical indicators presents a challenge. Relative muscle strength (RMS) may offer a viable indicator. This study aimed to explore the association between RMS and hypertension.
Methods
A total of 12,720 individuals aged ≥ 45 years from the 2011 wave of the China Health and Retirement Longitudinal Study (CHARLS) were included. Grip strength was recorded and appendicular skeletal muscle mass (ASM) was estimated using a validated mathematical formula. The RMS was calculated as the ratio of grip strength to ASM. Hypertension was determined based on previous diagnosis, history of hypertension medication use, and current blood pressure. Logistic regression models were employed to investigate the relationship between RMS and hypertension.
Results
The prevalence of hypertension was 41.7% (5,307/12,720 patients). RMS was negatively correlated with hypertension with an OR (95% CI) of 0.68 (0.59–0.79) for males, 0.81 (0.73–0.90) for females, and 0.78 (0.72–0.85) for the entire population after adjusting for related covariates including age, education, marital history, smoking history, drinking history, diabetes, hyperlipidemia, and obesity. The trend test showed a linear association among males, females, or the entire population. Stratified analysis showed a consistent negative correlation between RMS and hypertension.
Conclusions
Higher RMS is an independent protective factor against hypertension and efforts to promote RMS may be beneficial for the prevention and management of hypertension.
Similar content being viewed by others


Background
Hypertension is a risk factor for cardiovascular diseases [1]. Worldwide, the prevalence of hypertension among those reporting a previous diagnosis in 2019 was 59% (55–62) among females and 49% (46–52) among males, with only 47% (43–51) of females and 38% (35–41) of males being treated [2]. Prevention and management of hypertension can reduce the risk of myocardial infarction and stroke, as well as related disability and mortality, thus greatly reducing the economic burden on health care [3]. Despite a better understanding of hypertension and improvements in therapeutic strategies, the incidence of hypertension-related complications of cardiovascular diseases continues to increase [4]. Thus, the risk factors for hypertension need to be explored further.
Muscle quality, as distinguished from muscle quantity or mass, is gaining recognition as a means of elucidating and characterizing intricate intramuscular alterations linked to muscle functionality during the aging process [5]. Evidence increasingly suggests that a decline in muscle quality increases the risk of hypertension. Sarcopenia is an age-related clinical condition caused by the loss of muscle quality. A meta-analysis showed an increased risk of hypertension in subjects with sarcopenia compared with those without (OR = 1.39, 95% CI: 1.15–1.67, p < 0.01) [6]. Myosteatosis, or ectopic adipose infiltration in the skeletal muscle, is one of the manifestations of decreased muscle tissue quality. This increases the degree of local and systemic insulin resistance [7], which in turn, may contribute to hypertension [8]. Advanced myosteatosis measured using abdominal computed tomography (CT) at the L3 level was significantly associated with a higher risk of hypertension even after adjusting for relevant covariates [9]. It should be noted that muscle quality is recognized as a modifiable risk factor, as appropriate strength exercise can improve muscle quality in various populations [10, 11]. Therefore, it is sensible to begin with muscle quality to develop preventive strategies for health problems such as hypertension. However, the diagnostic process of sarcopenia is complex, limiting its clinical applicability. Moreover, the clinician-friendliness of identifying myosteatosis using equipment such as CT and other specific techniques is questionable. Therefore, there is an urgent need to identify clinically accessible indicators of muscle quality.
Relative muscle strength (RMS), defined as muscle power per unit of muscle mass, is comparable to myosteatosis as a metric of muscle quality [5, 12, 13]. RMS is recommended for the characterization of muscle quality in clinical studies. In most studies, upper limb muscle quality is typically calculated as the ratio of grip strength to lean mass in the arms [14, 15]. Lower limb muscle quality is calculated as the ratio of quadriceps strength to lean mass in the legs [15]. Alternatively, muscle quality can be determined through grip strength in relation to appendicular skeletal muscle mass (ASM), that is, the lean mass in both arms and legs [16]. Among the calculated parameters associated with RMS, grip strength is a frequently used indicator of muscle strength in healthcare settings, and ASM is routinely used to diagnose sarcopenia, making grip strength/ASM a more readily accessible measure for clinical use. Several studies have reported an association between RMS and health problems; Park et al. found that RMS was significantly lower in older adults with diabetes than in those without diabetes [17]. Yoon et al. found that the worse the glucose metabolism, the lower the RMS was [18]. In addition, the higher the RMS, the lower the risk of cognitive impairment in men [16]. Among patients undergoing dialysis, a lower RMS is an independent predictor of increased mortality [19]. However, there is currently no research indicating a connection between RMS and hypertension. Therefore, this study aimed to investigate the correlation between RMS and the risk of hypertension using data from the China Health and Retirement Longitudinal Study (CHARLS).
Methods
Study design and participants
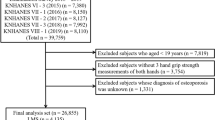
The aim of the CHARLS was to investigate the current state of aging throughout China and facilitate multidisciplinary research on aging using high-quality microdata collected from Chinese households and individuals over 45 years of age. A multistage proportional to size sampling method was used for the baseline survey of the CHARLS in 2011, and three follow-up studies were conducted in 2013, 2015, and 2018 [20, 21, 22]. The CHARLS dataset is available at http://charls.pku.edu.cn/en. The study was approved by the Peking University Biomedical Ethics Committee and informed consent forms were signed by all participants. The data for this study were retrieved from a baseline survey conducted in 2011, which included 17,707 participants. The inclusion criteria were as follows: 1) age ≥ 45 years and 2) complete blood pressure measurement data. Exclusion criteria were as follows: 1) no information on weight or height, 2) no information on drinking or smoking history, and 3) no information on a diagnosis of diabetes or hyperlipidemia (Fig. 1).

Flow chart of the study
Diagnosis of hypertension
Hypertension was diagnosed based on the following conditions: (1) systolic blood pressure ≥ 140 mmHg, (2) diastolic blood pressure ≥ 90 mmHg, (3) self-reported history of hypertension, and (4) self-reported intake of anti-hypertensive drugs [20, 23].
Assessment of RMS
RMS was defined as handgrip strength/ASM. To measure the grip strength (kg) of the dominant and non-dominant hands, the participants were asked to squeeze the dynamometer (TMWL-1000; Yuejian, China) as hard as possible. The maximum value was recorded after testing both hands twice, using a dynamometer at a right angle. A previously reported mathematical formula was used to estimate ASM in the Chinese population [24,25,26,27]: ASM = 0.193 × weight (kg) + 0.107 × height (cm) – 4.157 × sex – 0.037 × age (year) – 2.631. Sex was set to one if male; otherwise, it was set to two.
Potential covariates
Sociodemographic characteristics included age, sex, education (junior high school and below, high school/vocational high school, college and above), and marital status (married/other, including separated, unmarried, divorced, and widowed). Health-related factors included smoking history (no for nonsmoker/yes for former smoker or current smoker), drinking history (no for nondrinker/yes for former drinker or current drinker), diabetes (self-reported diabetes diagnosis history or use of hypoglycemic drugs or fasting glucose ≥ 7 mmol/L or glycosylated hemoglobin ≥ 6.5%), hyperlipidemia (self-reported hyperlipidemia diagnosis history or use of lipid-lowering drugs or blood total cholesterol ≥ 240 mg/dL or low density cholesterol ≥ 160 mg/dL or triglyceride ≥ 200 mg/dL or high density cholesterol < 40 mg/dL), and obesity (BMI ≥ 28 kg/m2).
Statistical analysis
All analyses were performed using the R statistical software package (http://www.R-project.org) and Free Statistics software version 1.8 (http://www.clinicalscientists.cn/freestatistics). Quantitative data with normal distribution were expressed as mean ± standard deviation and median (interquartile, IQR) in cases of skewed distribution. The comparison of groups was conducted using analysis of variance and the Kruskal–Wallis rank-sum test. The qualitative data were summarized in terms of percentages and subsequently compared utilizing the chi-square test. Additionally, logistic regression analysis was conducted to evaluate the association between RMS and hypertension. Regression analyses included unadjusted and adjusted models (adjusted for covariates, including age, education, marital status, smoking history, drinking history, diabetes, hyperlipidemia, and obesity). P < 0.05 was considered statistically significant.
Results
Characteristics of participants
A total of 12,720 individuals were finally included in the analysis: 6081 (47.8%) male and 6639 (52.2%) female. The prevalence of hypertension was 41.7% (5,307/12,720 individuals). The mean RMS was 1.9, with a standard deviation of 0.5. Table 1 shows the characteristics of the participants according to hypertension status. Individuals with hypertension were more likely to be older, obese, and had hyperlipidemia and diabetes, whereas individuals without hypertension had higher grip strength, lower BMI, lower ASM, and higher RMS.
Association between RMS and hypertension
Logistic regression analysis showed that RMS was associated with hypertension with an OR (95% CI) of 0.45 (0.39–0.51) in males, 0.6 (0.54–0.66) in females and 0.54 (0.50–0.58) in the entire population in the unadjusted model. After adjusting for confounders, RMS remained associated with hypertension negatively, with an OR (95% CI) of 0.68 (0.59–0.79) in males, 0.81(0.73–0.90) in females, and 0.78(0.72–0.85) in the entire population (Table 2). The linear association between RMS and hypertension was further explored using a trend test in which participants were grouped according to tertiles of RMS. Results showed that the prevalence of hypertension was significantly lower in those with the highest RMS tertile than in those with the lowest RMS tertile in fully adjusted models among males (OR: 0.74, 95% CI: 0.64–0.84, P for trend < 0.001), females (OR: 0.75, 95% CI: 0.66–0.85, P for trend < 0.001), and the entire population (OR: 0.76, 95% CI: 0.70–0.84, P for trend < 0.001). In addition, subgroup analysis revealed a consistent negative correlation between RMS and hypertension among individuals of different sexes when stratified by age, marital status, smoking history, drinking history, diabetes, hyperlipidemia, and obesity status, with ORs below the reference value. Furthermore, a significant interaction (P for interaction: 0.003) was observed when the analyses of hypertension were stratified by age among females, such that the risk of hypertension by RMS was higher among those in the middle-aged group than among those in the older group (Figs. 2 and 3).

Forest plot for the association between RMS and hypertension in different subgroup of male population. Odd ratios (ORs) were adjusted for age, education, marital status, smoking history, drinking history, diabetes, hyperlipidemia, obesity

Forest plot for the association between RMS and hypertension in different subgroup of female population. Odd ratios (ORs) were adjusted for age, education, marital status, smoking history, drinking history, diabetes, hyperlipidemia, obesity
Discussion
Our findings show that RMS is negatively and linearly correlated with hypertension in both males and females and in the entire population, even after adjusting for covariates. In other words, a higher RMS value reduced the risk of developing hypertension. Stratified analysis further showed that the correlation between RMS and hypertension was robust across subgroups with different ages, marital history, smoking history, diabetes history, hyperlipidemia history, and obesity status.
To the best of our knowledge, few studies have examined the association between RMS and hypertension. However, the relationship between the parameters used to calculate RMS, that is, grip strength, muscle mass, and hypertension, has been reported in several studies. Studies have shown that higher grip strength is independently associated with lower blood pressure and is therefore a protective factor against hypertension [28, 29]. In contrast, another study showed that higher grip strength was associated with higher blood pressure after adjusting for BMI [30]. However, we did not observe any correlation between grip strength and hypertension (Table S1). These inconsistent results may be attributed to significant differences in age and BMI distribution among the populations in these studies. Similarly, there is no consensus regarding the association between muscle mass and hypertension. Julius et al. were the first to report a positive correlation between skeletal muscle mass of the extremities and blood pressure [31]. Vaziri et al. also found a positive correlation between skeletal muscle mass and blood pressure independent of BMI in a younger population [32]. Liu et al. found that the association between muscle mass and incident hypertension followed a J-shaped curve in a community-dwelling population of older Chinese adults [33]. A study by Ye et al. also showed that muscle mass, or height- and weight-corrected muscle mass, were positively associated with blood pressure and hypertension, suggesting that elevated muscle mass may be a risk factor for hypertension [34]. However, Han et al. reported that low muscle mass was correlated with a higher risk of developing hypertension among Korean men, whereas this correlation was not significant in women [35]. We found in this study that muscle mass (ASM) and BMI-corrected muscle mass (ASMI) were positively associated with hypertension in both men and women (Table S1). These discrepancies could be the result of obesity, as obese individuals have higher muscle mass. RMS, which combines grip strength and muscle mass, showed a stable and independent correlation with hypertension. This is likely due to the fact that RMS reflects changes in muscle properties and is not susceptible to factors affecting muscle mass and grip strength, such as BMI, height, and weight. However, it should be noted that while the correlation between RMS and hypertension was maintained among the males after replacing obesity status in the model with BMI, this association disappeared in the female population after making the above substitution (Table S2). This suggests that a higher level of obesity in women than in men has a greater impact on the development of hypertension, thus attenuating the association between RMS and hypertension. Furthermore, within the subgroup analysis focusing on female individuals, the correlation between RMS and hypertension was stronger in the middle-aged cohort (aged 45–59 years). Since the average age of menopause among Chinese women is reported to be 49.3 ± 3.3 years, with a median age of 50 years [36], one possible explanation for this phenomenon could be the fact that some middle-aged women may not have reached menopause, resulting in comparatively elevated levels of estrogen [37]. Estrogen has been shown to offer protection against hypertension [38].
However, the mechanism underlying the association between RMS and hypertension remains unclear. RMS is closely related to myosteatosis [39], which affects muscle strength and reduces RMS [40, 41]. This leads to the accumulation of diacylglycerol and ceramides in muscle cells, thereby inhibiting glucose uptake by the muscles and gluconeogenesis and exacerbating insulin resistance [42,43,44]. Given that insulin resistance is closely associated with the risk of developing hypertension [45,46,47], the correlation between RMS and hypertension may be related to myosteatosis-induced insulin resistance. Previous studies have shown that RMS is closely associated with muscle insulin resistance [48]. Consistent with this, we found that a low RMS was associated with a worse glucolipid metabolic profile (Table S3), which is a parameter associated with insulin resistance. Hyperinsulinemia due to insulin resistance leads to sympathetic excitation, decreased renal vasoconstriction, and increased renal tubular sodium reabsorption, causing an increase in blood pressure [49, 50]. Furthermore, low muscle quality and hypertension share common risk factors such as older age, sedentary lifestyle [51, 52], and obesity [53, 54]. Nevertheless, the cross-sectional results did not elucidate a causal association, which may be an effect of confounding factors and requires further validation.
This study has several strengths. First, the inclusion of a substantial proportion of the population ensures national representation. Second, multiple research groups validated the quality of the data used in this study. Finally, this study represents an initial exploration of the correlation between RMS and hypertension. However, it is important to acknowledge the limitations of this study. First, owing to its cross-sectional nature, the causal relationship between RMS and hypertension could not be confirmed, and requires further investigation through longitudinal studies. Second, despite adjusting for numerous common confounders, certain factors such as genetic predisposition, sodium intake, and physical activity were not considered. Lastly, the study focused solely on a Chinese population; thus, caution must be exercised when generalizing the findings to other populations, particularly given the apparent population differences in muscle quality [55].
Conclusions
Higher RMS is an independent protective factor against hypertension, and measures to increase RMS in middle-aged and older adults may be beneficial for the prevention and management of hypertension. It is notable that RMS may serve as a more accessible and consistent metric than other muscle parameters when assessing the relationship between muscle impairment and hypertension.
Availability of data and materials
The data that support this study are available from the websites of CHARLS (http://charls.pku.edu.cn).
Abbreviations
- CHARLS:
-
China Health and Retirement Longitudinal Study
- RMS:
-
Relative muscle strength
- ASM:
-
Appendicular skeletal muscle mass
- ASMI:
-
Appendicular skeletal muscle mass index
- BMI:
-
Body mass index
- OR:
-
Odds ratio
- IQR:
-
Interquartile
- SD:
-
Standard deviation
References
Montagna S, Pengo MF, Ferretti S, et al. Machine Learning in Hypertension Detection: A Study on World Hypertension Day Data. J Med Syst. 2022;47(1):1.
NCD Risk Factor Collaboration (NCD-RisC). Worldwide trends in hypertension prevalence and progress in treatment and control from 1990 to 2019: a pooled analysis of 1201 population-representative studies with 104 million participants. Lancet. 2021;398(10304):957–80.
Mills KT, Bundy JD, Kelly TN, et al. Global Disparities of Hypertension Prevalence and Control: A Systematic Analysis of Population-Based Studies From 90 Countries. Circulation. 2016;134(6):441–50.
GBD 2019 Risk Factors Collaborators. Global burden of 87 risk factors in 204 countries and territories, 1990–2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet. 2020;396(10258):1223–49.
Fragala MS, Kenny AM, Kuchel GA. Muscle quality in aging: a multi-dimensional approach to muscle functioning with applications for treatment. Sports Med. 2015;45(5):641–58.
Quan Y, Wang C, Wang L, Li G. Geriatric sarcopenia is associated with hypertension: A systematic review and meta-analysis. J Clin Hypertens. 2023;25(9):808–16.
Miljkovic I, Vella CA, Allison M. Computed Tomography-Derived Myosteatosis and Metabolic Disorders. Diabetes Metab J. 2021;45(4):482–91.
Lee M, Park S. Myosteatosis: a potential missing link between hypertension and metabolic disorder in the Asian population. Hypertens Res. 2023;46(6):1603–5.
Jung HN, Cho YK, Kim HS, et al. Association between hypertension and myosteatosis evaluated by abdominal computed tomography. Hypertens Res. 2023;46(4):845–55.
Oh SL, Kim HJ, Woo S, et al. Effects of an integrated health education and elastic band resistance training program on physical function and muscle strength in community-dwelling elderly women: Healthy Aging and Happy Aging II study. Geriatr Gerontol Int. 2017;17(5):825–33.
Radaelli R, Taaffe DR, Newton RU, Galvão DA, Lopez P. Exercise effects on muscle quality in older adults: a systematic review and meta-analysis. Sci Rep. 2021;11(1):21085.
McGregor RA, Cameron-Smith D, Poppitt SD. It is not just muscle mass: a review of muscle quality, composition and metabolism during ageing as determinants of muscle function and mobility in later life. Longev Healthspan. 2014;3(1):9.
Correa-de-Araujo R, Harris-Love MO, Miljkovic I, Fragala MS, Anthony BW, Manini TM. The Need for Standardized Assessment of Muscle Quality in Skeletal Muscle Function Deficit and Other Aging-Related Muscle Dysfunctions: A Symposium Report. Front Physiol. 2017;8:87.
Nogueira Paranhos Amorim D, Nascimento DC, Alves VP, Moraes CF, Coelho Vilaça E, Silva KH. Muscle Quality Is Associated with History of Falls in Octogenarians. J Nutr Health Aging. 2021;25(1):120–5.
Strasser EM, Hofmann M, Franzke B, et al. Strength training increases skeletal muscle quality but not muscle mass in old institutionalized adults: a randomized, multi-arm parallel and controlled intervention study. Eur J Phys Rehabil Med. 2018;54(6):921–33.
Sui SX, Williams LJ, Holloway-Kew KL, Hyde NK, Leach S, Pasco JA. Associations Between Muscle Quality and Cognitive Function in Older Men: Cross-Sectional Data From the Geelong Osteoporosis Study. J Clin Densitom. 2022;25(2):133–40.
Park SW, Goodpaster BH, Strotmeyer ES, de Rekeneire N, Harris TB, Schwartz AV, Tylavsky FA, Newman AB. Decreased muscle strength and quality in older adults with type 2 diabetes: the health, aging, and body composition study. Diabetes. 2006;55(6):1813–8.
Yoon JW, Ha YC, Kim KM, et al. Hyperglycemia Is Associated with Impaired Muscle Quality in Older Men with Diabetes: The Korean Longitudinal Study on Health and Aging. Diabetes Metab J. 2016;40(2):140–6.
Yoda M, Inaba M, Okuno S, et al. Poor muscle quality as a predictor of high mortality independent of diabetes in hemodialysis patients. Biomed Pharmacother. 2012;66(4):266–70.
Ding L, Zhu X, Xiong Z, Yang F, Zhang X. The Association of Age at Diagnosis of Hypertension with Cognitive Decline: the China Health and Retirement Longitudinal Study (CHARLS). J Gen Intern Med. 2023;38(6):1431–8.
Li C, Lumey LH. Impact of disease screening on awareness and management of hypertension and diabetes between 2011 and 2015: results from the China health and retirement longitudinal study. BMC Public Health. 2019;19(1):421.
Wu Y, Tong Y, Wang H, Zhang X, Long Y, Li Q, Ren J, Liu C. Waist-to-height ratio and new-onset hypertension in middle-aged and older adult females from 2011 to 2015: A 4-year follow-up retrospective cohort study from the China Health and Retirement Longitudinal Study. Front Public Health. 2023;11:1122995.
Joint Committee for Guideline Revision. 2018 Chinese guidelines for prevention and treatment of hypertensiona report of the revision committee of Chinese guidelines for prevention and treatment of hypertension. J Geriatr Cardiol. 2019;16(3):182–241.
Wen X, Wang M, Jiang CM, Zhang YM. Anthropometric equation for estimation of appendicular skeletal muscle mass in Chinese adults. Asia Pac J Clin Nutr. 2011;20(4):551–6.
Gao K, Cao LF, Ma WZ, et al. Association between sarcopenia and cardiovascular disease among middle-aged and older adults: Findings from the China health and retirement longitudinal study. EClinicalMedicine. 2022;44:101264.
Hu Y, Peng W, Ren R, Wang Y, Wang G. Sarcopenia and mild cognitive impairment among elderly adults: The first longitudinal evidence from CHARLS. J Cachexia Sarcopenia Muscle. 2022;13(6):2944–52.
Dai S, Wang S, He Y, Dai C, Yu J, Ma X. Association between anemia and sarcopenia among Chinese elderly: A cross-sectional study based on the China health and retirement longitudinal study. Exp Gerontol. 2023;177:112183.
Mainous AG 3rd, Tanner RJ, Anton SD, Jo A. Grip Strength as a Marker of Hypertension and Diabetes in Healthy Weight Adults. Am J Prev Med. 2015;49(6):850–8.
Chon D, Shin J, Kim JH. Consideration of body mass index (BMI) in the association between hand grip strength and hypertension: Korean Longitudinal Study of Ageing (KLoSA). PLoS ONE. 2020;15(10):e0241360.
Dong B, Wang Z, Arnold L, Song Y, Wang HJ, Ma J. The association between blood pressure and grip strength in adolescents: does body mass index matter. Hypertens Res. 2016;39(12):919–25.
Julius S, Majahalme S, Nesbitt S, et al. A “gender blind” relationship of lean body mass and blood pressure in the Tecumseh study. Am J Hypertens. 2002;15(3):258–63.
Vaziri Y, Bulduk S, Shadman Z, et al. Lean Body Mass as a Predictive Value of Hypertension in Young Adults, in Ankara. Turkey Iran J Public Health. 2015;44(12):1643–54.
Liu Y, Sun G, Li Y. A prospective cohort study on the association of lean body mass estimated by mid-upper arm muscle circumference with hypertension risk in Chinese residents. J Clin Hypertens (Greenwich). 2022;24(3):329–38.
Ye S, Zhu C, Wei C, et al. Associations of Body Composition with Blood Pressure and Hypertension. Obesity (Silver Spring). 2018;26(10):1644–50.
Han JM, Lee MY, Lee KB, Kim H, Hyun YY. Low relative skeletal muscle mass predicts incident hypertension in Korean men: a prospective cohort study. J Hypertens. 2020;38(11):2223–9.
Song L, Shen L, Li H, et al. Age at natural menopause and hypertension among middle-aged and older Chinese women. J Hypertens. 2018;36(3):594–600.
Burger HG, Hale GE, Robertson DM, Dennerstein L. A review of hormonal changes during the menopausal transition: focus on findings from the Melbourne Women’s Midlife Health Project. Hum Reprod Update. 2007;13(6):559–65.
Sabbatini AR, Kararigas G. Estrogen-related mechanisms in sex differences of hypertension and target organ damage. Biol Sex Differ. 2020;11(1):31.
Goodpaster BH, Carlson CL, Visser M, et al. Attenuation of skeletal muscle and strength in the elderly: The Health ABC Study. J Appl Physiol (1985). 2001;90(6):2157–65.
Miljkovic I, Zmuda JM. Epidemiology of myosteatosis. Curr Opin Clin Nutr Metab Care. 2010;13(3):260–4.
Koo BK. Assessment of Muscle Quantity, Quality and Function. J Obes Metab Syndr. 2022;31(1):9–16.
Kitessa SM, Abeywardena MY. Lipid-Induced Insulin Resistance in Skeletal Muscle: The Chase for the Culprit Goes from Total Intramuscular Fat to Lipid Intermediates, and Finally to Species of Lipid Intermediates. Nutrients. 2016;8(8):466.
Park M, Kaddai V, Ching J, et al. A Role for Ceramides, but Not Sphingomyelins, as Antagonists of Insulin Signaling and Mitochondrial Metabolism in C2C12 Myotubes. J Biol Chem. 2016;291(46):23978–88.
Bandet CL, Tan-Chen S, Bourron O, Le Stunff H, Hajduch E. Sphingolipid Metabolism: New Insight into Ceramide-Induced Lipotoxicity in Muscle Cells. Int J Mol Sci. 2019;20(3):479.
Tagi VM, Mainieri F, Chiarelli F. Hypertension in Patients with Insulin Resistance: Etiopathogenesis and Management in Children. Int J Mol Sci. 2022;23(10):5814.
Usui I. Hypertension and insulin resistance in adipose tissue. Hypertens Res. 2023;46(6):1478–81.
Manucha W, Ritchie B, Ferder L. Hypertension and insulin resistance: implications of mitochondrial dysfunction. Curr Hypertens Rep. 2015;17(1):504.
Gysel T, Calders P, Cambier D, et al. Association between insulin resistance, lean mass and muscle torque/force in proximal versus distal body parts in healthy young men. J Musculoskelet Neuronal Interact. 2014;14(1):41–9.
Sironi AM, Sicari R, Folli F, Gastaldelli A. Ectopic fat storage, insulin resistance, and hypertension. Curr Pharm Des. 2011;17(28):3074–80.
Soleimani M. Insulin resistance and hypertension: new insights. Kidney Int. 2015;87(3):497–9.
Zhang K, Huang S, Feng D, Lang X, Wang Q, Liu Y. Sedentary Behavioral Studies of Young and Middle-Aged Adults with Hypertension in the Framework of Behavioral Epidemiology: A Scoping Review. Int J Environ Res Public Health. 2022;19(24):16796.
Smith L, Tully M, Jacob L, et al. The Association Between Sedentary Behavior and Sarcopenia Among Adults Aged ≥65 Years in Low- and Middle-Income Countries. Int J Environ Res Public Health. 2020;17(5):1708.
Nurdiantami Y, Watanabe K, Tanaka E, Pradono J, Anme T. Association of general and central obesity with hypertension. Clin Nutr. 2018;37(4):1259–63.
Nordengen AL, Øyri L, Ulven SM, Raastad T, Holven KB, Ottestad I. Comparison of methods to identify individuals with obesity at increased risk of functional impairment among a population of home-dwelling older adults. Br J Nutr. 2022;128(6):1064–71.
Forouhi NG, Jenkinson G, Thomas EL, et al. Relation of triglyceride stores in skeletal muscle cells to central obesity and insulin sensitivity in European and South Asian men. Diabetologia. 1999;42(8):932–5.
Acknowledgements
We thank all the participants for their contribution in the CHARLS.
Funding
Not applicable.
Author information
Authors and Affiliations
Contributions
The research question was formulated by JL, who also designed the study, analyzed the data, and drafted the paper. TZ, LY, and YC contributed to the study design, data analysis, and paper revision. YY provided assistance with research question formulation, data interpretation, and paper quality supervision. The final version of the manuscript was reviewed, feedback was provided, and confirmation was given by all authors.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Ethical approval for CHARLS was granted from the Institutional Review Board(IRB) at Peking University. The IRB approval number for the main household survey, including anthropometrics, is IRB00001052-11015, and the IRB approval number for biomarker collection, was IRB00001052-11014. All participants gave a written informed consent before enrollment in the study. The study methodology was carried out in accordance with approved guidelines.
Consent for publication
Not applicable.
Competing interests
The authors declare no conflict of interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1:
Table S1. Association between ASM, ASMI, grip strength and hypertension in middle-aged and older adults. Table S2. Association between RMS and hypertension in middle-aged and older adults. Table S3. Prevelance of diabetes and hyperlipidemia in different RMS groups.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Luo, Jh., Zhang, Tm., Yang, Ll. et al. Association between relative muscle strength and hypertension in middle-aged and older Chinese adults. BMC Public Health 23, 2087 (2023). https://doi.org/10.1186/s12889-023-17007-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12889-023-17007-6