
Abstract
Background
A significant proportion of the global burden of disability and premature mortality has caused by hypertension. It seems that the relationship between obesity and hypertension is not only associated with excessive body fat mass (FM) but also with body adipose distribution patterns. The present study investigated the association between regional fat distribution using dual-energy X-ray absorptiometry and hypertension in older adults.
Methods
This cross-sectional study was performed using the data from Bushehr Elderly Health Program (BEH) on a total of 2419 participants aged 60 and over. Hypertension was defined as SBP of at least 140 mmHg and/or DBP of at least 90 mmHg. SBP between 120 and 139 mmHg and/or a DBP between 80 and 89 mmHg were considered prehypertension. Participants underwent body composition measurement by dual-energy x-ray absorptiometry to analyze FM, fat-free mass (FFM) in trunk and extremities composition.
Results
The results showed that 460 (19.02%) of participants had prehypertension, and 1,818 (75.15% ) had hypertension. The odds of having prehypertension (OR: 1.06, 95%CI: 1.01–1.12) and hypertension (OR: 1.08, 95%CI: 1.03–1.13) increased with a rise in total body FM percentage. Moreover, people with a higher FM to FFM ratio had increased odds of being prehypertensive (OR: 9.93, 95%CI: 1.28–76.99) and hypertensive (OR: 16.15, 95%CI: 2.47-105.52). Having a higher android to gynoid FM ratio was related to increased odds of being prehypertensive and hypertensive.
Conclusions
This study showed that a higher body FM, particularly in the android region, is associated with higher odds of having hypertension in older adults.
Similar content being viewed by others


Background
Non-communicable diseases (NCDs) are the notable cause of mortality, increasing over the recent two decades. Four major NCDs, including cancers, diabetes, chronic respiratory diseases, and cardiovascular diseases (CVDs), were responsible for 70% of the 56.4 million deaths worldwide in 2015, according to World Health Organization (WHO) [1]. A significant proportion of the global burden of cardiovascular disease, disability, and premature mortality has caused by hypertension. More than one billion people suffer from hypertension, of which 75% live in low- and middle-income countries [2]. In 2019, high systolic blood pressure was accountable for about 30.6% of mortalities in Iran [3].
Although high blood pressure can be controlled by many demonstrated and effectual pharmacological treatments and lifestyle modifications (such as salt intake, smoking, alcoholic drinks, sleep duration, obesity, and abdominal obesity), it remains highly prevalent [4]. Adipose tissue is an endocrine organ and active tissue for energy homeostasis which synthesizes and secrets hormones such as leptin and adiponectin and inflammatory mediators like TNF-alpha and Interluekin-6. Adipose tissue dysfunction can be caused by obesity, which is recognized by dysregulation in secreting many vasoactive adipokines and anti-inflammatory cytokines, changing secretory profiles, mitochondrial dysfunction, and tissue inflammation [5, 6]. It seems that the relationship between obesity and hypertension is not only associated with excessive body fat but also with body adipose distribution patterns [7].
Although body mass index (BMI) is the most typical obesity indicator to predict the risk of CVDs, it suffers from the inability to determine tissue type (muscle or adipose tissue) or regions of body mass distribution [8, 9]. Since body composition assessment plays a crucial role in studying human metabolism and physiology, it is preferable to use segmental measurements that can indicate the effect of obesity more accurately [10]. A study by Yano et al. showed that excessive fat accumulation in the visceral area, but not subcutaneous adipose tissue, was related to higher mean blood pressure in the short- and long-term and decreased long-term blood pressure variability [11]. In addition, another study demonstrated that trunk fat mass was the predominant contributor to a higher SBP and DBP, while leg fat mass had the opposite relationship with BP [12]. Dual-energy X-ray absorptiometry (DXA) scan is a gold standard that is able to differentiate between fat tissues and measure body fat distribution accurately and objectively [13, 14].
There is a lack of understanding regarding the precise relationship between regional fat distribution, prehypertension, and hypertension risk in older adults. This gap is especially significant considering that conventional measures such as body mass index (BMI) do not provide sufficient precision for this specific age group. To address this, the study aims to investigate the relationship between regional fat distribution (using DXA), and hypertension in the older adult population of southern Iran based on the Bushehr Elderly Health (BEH) program. By examining specific patterns of fat accumulation, the research aims to provide insights for targeted interventions and preventive strategies.
Methods
Design study and participants
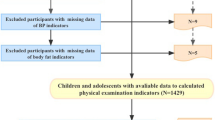
This cross-sectional study was performed using the data from Bushehr Elderly Health Program (BEH), a prospective demographic cohort study conducted in Bushehr, Southern Iran. Detailed protocols have been reported previously, including the study design and methodology for the BEH program [15, 16]. In summary, the first phase of the BEH program commenced in March 2013 to investigate the prevalence of cardiovascular risk factors and their relationship with adverse cardiovascular events in the older adult population. A total of 3000 participants aged 60 and over were recruited by stratified random sampling method. Subjects were selected if they lived in Bushehr for at least one year before the recruitment with no plan to leave in the following two years, had adequate physical and mental ability to cooperate in the study, and signed written consent. The second stage of the first phase of the study was completed in 2015–2018. The participation rate in the second phase was 81%. Finally, all the 2419 individuals with completed databanks were included in this study (Fig. 1).

Flow chart of enrolment in the Bushehr Elderly Health (BEH) program
The database included demographic status, general health, mental and functional health, lifestyle, and history of drug use, which was collected using valid forms and questionnaires. The Ethics Research Committee of Bushehr University of medical sciences (IR.BPUMS.REC.1401.173) and the Endocrinology and Metabolism Research Institute of Tehran University of Medical Sciences approved the study protocol.
Blood pressure
As our primary outcome, systolic blood pressure (SBP) and diastolic blood pressure (DBP) were measured twice using a standard mercury sphygmomanometer in the right arm after 15 min of rest in a sitting position with a time interval of 10 min. The average of the two measurements was taken as the participant’s blood pressure. Individuals were classified according to SBP and DBP levels into normal blood pressure, prehypertension, and hypertension. Hypertension was defined as SBP of at least 140 mmHg and/or DBP of at least 90 mmHg or taking antihypertensive medications. SBP between 120 and 139 mmHg and/or a DBP between 80 and 89 mmHg were considered prehypertension [7].
Laboratory evaluations
After 8–10 h of fasting, 25 ml of venous blood samples were collected by a trained nurse and stored in coded containers for further testing. Laboratory tests included fasting blood sugar (FBS) (mmol/L) and blood lipid profile (total cholesterol, HDL-c, LDL-c, and triglycerides) (mmol/L). All the processes were executed by professional personnel and advanced tools. Laboratory FBS and blood lipid profile testing were measured by enzymatic colorimetric method using a Pars Azmun kit (Pars Azmun, Karaj, Iran).
Anthropometric and clinical assessments
Anthropometric indexes were quantified under the standard protocol by wearing light clothing and removing shoes. A fixed stadiometer and a digital scale were used to measure height and weight. A flexible, constant tension tape was used to determine neck, waist and hip circumferences at the level of the umbilicus and the widest part over the buttocks, respectively. Body mass index (BMI) was calculated by dividing the weight (kg) by height squared (m2). Participants underwent body composition measurement by dual-energy x-ray absorptiometry (DXA, Discovery WI, Hologic Bedford, Virginia, USA) to analyze fat mass, muscle mass, and head, trunk, and extremities composition.
Android and gynoid regions
The Android region height was considered equal to 20% of the distance from the pelvis horizontal line to the neckline. The lower boundary of the Android region coincided with the pelvic horizontal line, and the lateral boundaries of the Android region coincided with the arm lines. The Gynoid region height was considered equal to twice the height of the Android region. The upper limit of the Gynoid region was below the pelvic horizontal line by 1.5 times the Android region’s height, and the Gynoid region’s lateral boundaries coincided with the arm lines [17].
Other covariates
Socio-demographic information, such as age, gender, marital status, physical activity, income levels, education, occupation, smoking history, medical history, and drug use, were collected through interviews. The average physical activity level, encompassing sports, work, and leisure time, was determined by assessing the metabolic equivalent of tasks over a 24-hour period using the International Physical Activity Questionnaire (IPAQ). The widely adopted self-report tool is designed to measure the physical activity levels of individuals and has been validated within the Iranian population [15, 18, 19]. The level of physical activity was categorized into three classes: no activity and sedentary: ≤1.39; low active: 1.4–1.59; active: ≥1.6 (MET/24 h) [20, 21].
Data analysis
Categorical variables of general characteristics were presented as frequencies and percentages, whereas continuous variables were expressed as mean values and standard deviation (SD). Differences between the groups were evaluated using a one-way ANOVA for continuous and Chi-square for categorical variables. The odds ratio and 95% confidence interval were calculated through multinomial logistic regression analyses to determine the association of prehypertension and hypertension with anthropometric and body composition indices.
Relevant confounders were selected based on an extensive literature search. Firstly, their clinical and pathophysiological association with the desired outcome and exposures was assessed using univariate regression models. Then, statistically significant covariates, which have clinical implications, were included in the multivariable logistic regression models. Analytical models were set as model crude; model 1: adjusted for age; model 2: adjusted for age and gender; model 3: adjusted for age, gender, marital, education, job, physical activity, smoking, income, kidney stone, diabetes, BMI, TG, TC, LDL, HDL. All analyses were done in Stata MP (version 17). P-value < 0.05 was taken as statistically significant for all analyses.
Results
The general characteristics of the participants are shown in Table 1. This study included 2,419 participants, 460 (19.02%) of whom had prehypertension, and 1,818 (75.15%) had hypertension. The mean age in people with hypertension was significantly higher (69·65 ± 6·53 years vs. 68·45 ± 5·58 years) than the mean age in the group with normal blood pressure. While the prevalence of prehypertension was higher in men than in women (21.6% vs. 16.6%), the proportion of women with hypertension was higher than in men (76.7% vs. 73.5%). 68.7% of people with hypertension had a history of smoking (50.6% past smokers, 18.1% current smokers). The prevalence of hypertension was lower in those still employed than in those who were retired or unemployed (66.6% vs. 74.4% and 76.7%, respectively). Also, being physically sedentary or not active and having diabetes was related to a higher prevalence of hypertension. No statistical differences were observed in the prevalence of prehypertension and hypertension regarding having diseases such as stroke, chronic renal failure, thyroid diseases, or lung disease. There was also a group of individuals that they were not consuming any antihypertensive medicine although 22% and 71% of them were suffering from prehypertension and hypertension, respectively, as untreated individuals (Table 1).
According to Table 1, normotensive people had significantly lower mean weight, BMI, NC, WC, HC, and WHR in comparison with prehypertensive and hypertensive groups. In addition, DXA analysis showed that mean Lean Body Mass (LBM), Appendicular Skeletal Muscle (ASM), total fat percentage, and FM to LBM ratio were lower in the group with normal blood pressure.
In the examination of the laboratory data, it was seen that while TC, HDL, and LDL were statistically lower in participants with hypertension, TG and FBS were higher (Table 1).
According to Table 2, the hypertension group had the highest mean Fat Mass Percentage (FMP) and Fat Mass (FM) to Fat-Free Mass (FFM) ratio in the limbs and trunk regions and the total body. Also, the trunk-to-limbs FM ratio and Android-to-Gynoid FM ratio in the HTN group were higher than the normal and pre-HTN group (p < 0.001).
Table 3 represents the relationship of adiposity indexes with prehypertension and hypertension among the older adults in this study. The odds of having prehypertension (OR: 1.06, 95%CI: 1.01–1.12; p = 0.009) and hypertension (OR: 1.08, 95%CI: 1.03–1.13; p = 0.001) increased with a rise in total body FM percentage in comparison with the normal group. Moreover, people with a higher FM to FFM ratio had increased odds of being prehypertensive (OR: 9.93, 95%CI:1.28–76.99; p = 0.028) and hypertensive (OR: 16.15, 95%CI: 2.47-105.52; p = 0.004). With a rise in the FM to FFM ratio in limbs, the risk of being prehypertensive (OR: 6.74, 95%CI: 1.39–32.73; p = 0.018) and hypertensive (OR: 7.69, 95%CI: 1.80-32.84; p = 0.006) increased; however, in the trunk area, the FM to FFM ratio was only associated with higher odds of hypertension (OR: 7.73, 95%CI: 1.60-37.32; p = 0.011).
Regarding the relationship of fat distribution, having a higher android to gynoid FM ratio was related to increased odds of being prehypertensive and hypertensive in the crude model. In addition, the crude model’s FM ratio of the trunk to the limbs had a positive relationship with a higher odds of having prehypertension and hypertension. However, after considering confounders in the full model, the change was only significant for the association of Android-to-gynoid FM ratio and having hypertension (OR: 5.12, 95%CI: 1.45–18.08; p = 0.011).
Discussion
Hypertension has been one of the significant public health issues in the last century, especially in older adults. The current study aimed to evaluate the association between body composition, emphasizing body fat distribution and hypertension in older adults. The result showed that body fat in the whole body and the regions of the trunk and limbs is closely related to being prehypertensive and hypertensive. In addition, the older adults with a higher Android to Gynoid fat mass ratio had an increased odds of developing hypertension in the Bushehr Elderly Health (BEH) program study.
The mean of age in the group with hypertension was higher than the group of normal blood pressure. Our results showed that 68.7% of hypertensive people were currently using smoke or used to consume it in the past. The previous studies indicated that life-course-adjusted smoking consumption was a major contributor to the increased risk of incidence of hypertension [22]. In addition, a sedentary lifestyle was also more prevalent in hypertensive individuals in our study. As a modifiable factor, physical activity has been shown to be a related intervention to prevent hypertension. It has been reported that people with active work styles tend to have lower blood pressure [23].
Our descriptive data indicated that individuals with higher education or employment appeared to have a lower prevalence of hypertension compared to those with no education or who were unemployed. However, it is important to note that the observed differences do not reach statistical significance for education levels. Although education’s impact on hypertension is reported to be limited in high-income countries, a meta-analysis has revealed that lower educational levels are associated with higher hypertension prevalence/incidence [24]. Being unemployed has also been identified as a factor for a 1.65-fold increase in the risk of hypertension [25].
Fat mass percentage and fat mass to free-fat mass ratio
In this study, older adults with higher fat mass percentage and fat mass to fat-free mass ratio were more susceptible to prehypertension and hypertension. Our results showed that with each percent increase in fat mass percentage in the whole body, the odds of having prehypertension and hypertension increase by 6% and 8%, respectively. Moreover, the fat to fat-free mass ratio in the whole body was related to a 9.9-fold and 16.1-fold higher odds of having prehypertension and hypertension per unit increase, respectively. The association trend for regional fat distribution (namely limbs and trunk) and hypertension also was the same as the whole body.
Consistent with our results, Previous studies have stated that higher body fat was related to the increased prevalence of cardiometabolic diseases [26,27,28]. In addition, the odds of being metabolically abnormal were nearly tripled in people with elevated body fat compared to people with lower body fat [26]. Takase et al. also reported that a higher fat mass index was related to the increased prevalence of hypertension, which could be because of increased insulin resistance, raised sympathetic tone, and renin-angiotensin-aldosterone system abnormalities [29]. The study of Saito et al. assessed the higher body fat percentage variability related to a higher incidence of hypertension. They reported that hypertrophy of adipocytes is associated with inflammatory cytokines dysregulation, which could indicate the potential mechanism of body fat percentage fluctuation effect on cardiovascular risk [30]. Also, a lower basal metabolic rate can be related to a lower muscle mass. Muscle loss can enhance inflammation and oxidative pathways, leading to diabetes, material stiffness, and hypertension. Previous studies reported a higher lean body mass in the upper limbs and torso is a protective factor against metabolic diseases [10] and sarcopenic obesity, characterized by the presence of low muscle mass and strength combined with high levels of adiposity, is linked to elevated cardiovascular risk factors and a higher mortality risk among older adults [31, 32]. However, a study by Ye et al. showed an opposite results. They stated that after accounting for various potential confounding factors such as body fat mass and fat distribution, arm lean body mass (LBM) could emerge as a risk factor for increased blood pressure (BP) and hypertension [33]. Moreover, the relationship between various adiposity indexes (such as body mass index, waist circumference, and waist-to-height ratio) with hypertension has been revealed, and central adiposity indicators seem to be more associated with the risk of hypertension [34].
Android to gynoid fat mass ratio
In this study, the fat mass ratio in the area of android to gynoid was positively associated with a rise in the prevalence of hypertension in older adults. We observed a 5.1-fold increase in the odds of hypertension per unit increase in the android-to-gynoid fat mass ratio in the fully adjusted model. Our research results are consistent with those previously reported in the existing literature [33, 35].
DXA analysis is a superior method to accurately determine body fat’s amount and distribution to the traditional methods such as skinfold or waist circumference [17, 36]. Gynoid refers to a relative excess of fat in the hips and thighs, while the android type illustrates excess upper-body fat [37]. The association of the android-to-gynoid ratio with metabolic and cardiovascular diseases has been reported, which can be explained by the crucial role of insulin in metabolism. The underlying linkage between diabetes, cardiovascular diseases, and obesity can be insulin resistance [17]. Accumulated fat in upper-body regions (such as visceral and epicardial adipose tissue) is a source of various proinflammatory cytokines like TNF-a and Interleukin-6. Conversely, higher gluteofemoral adipose tissue (GAT) mass plays a protective role in metabolic and cardiovascular diseases. GAT is related to lower cholesterol, glucose, and insulin levels, decreased vascular calcification, and arterial stiffness [5]. Yan et al. found that the accumulated trunk fat and decreased leg fat can be associated with increased blood pressure [36]. In addition, the study by Toss et al. showed peripheral obesity was associated with a higher level of adiponectin and lower insulin resistance in comparison with central obesity [38].
The potential mechanisms linking adiposity and metabolic health
Adipose tissue is considered a metabolically active organ that constitutes 20% of the weight of a normal healthy person. Since adipose tissue plays a part in homeostasis, its prolonged disturbance can cause severe health issues [39]. The expanding ability of adipose tissue is one of the major factors in causing metabolic dysregulation. Adipose tissue has limited hyperplasia, so by reaching their limitation, the cells will hypertrophy. This process, which is regulated by genetics and environmental factors, leads to the excessive release of free fatty acids in blood circulation, followed by low-grade inflammation, atherogenesis, cardiovascular diseases, hypertension, insulin resistance, and dyslipidemia [5, 39]. Synthesizing and releasing diverse cytokines and hormones, including tumor necrosis factor-a, interleukin-6, C-reactive protein, leptin, adiponectin, and non-esterified fatty acids, is one of the significant factions of adipose organ. Low-grade inflammation, endothelial dysfunction, metabolic dysregulation, and free fatty acid circulation due to the excessive accumulation of fat mass can contribute to causing hypertension [2].
This study has some strengths and limitations. The present investigation has received significant advantages from a relatively substantial sample size obtained using a stratified random sampling approach. This sampling method has augmented the ability of the study to generalize its outcomes to the population of older adults residing in Bushehr, Iran.
On the other hand, the present study is characterized by a cross-sectional design, which precludes the establishment of causal relationships between variables. Specifically, the inability to measure changes in the exposure and outcome variables over time limits the capacity to discern the direction of causality or determine any temporal relationship between them. Furthermore, the lack of complete dietary intake records for study participants presents a potential limitation, as it hinders the identification of nutritional confounders that may influence the outcomes of interest.
Conclusion
To summarize, hypertension is a significant health concern closely linked to body composition and fat mass distribution throughout the body. According to this study, older adults with a higher body fat mass are more likely to develop hypertension. The research indicates that the likelihood of increased blood pressure is not only related to overall body fat but also to the accumulation of fat in specific regions such as the trunk, limbs, and android area. Consequently, when managing blood pressure in older adults, it is necessary to consider regional body fat in addition to total body fat. Hence utilizing an accurate indicator can be more beneficial in addressing the risk of hypertension, as the gynoid-to-android FM ratio was associated with a higher risk of hypertension while the relationship between the trunk-to-limb FM was insignificant. Furthermore, the importance of the location of fat accumulation should be highlighted in health care screenings and in developing health policies.
Data Availability
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Abbreviations
- BEH:
-
Bushehr elderly health
- AHA:
-
American Heart Association
- MMS:
-
Measurements of Metabolic Syndrome
- SBP:
-
Systolic blood pressure
- DBP:
-
Diastolic blood pressure
- BMI:
-
Body mass index
- MAP:
-
Mean arterial pressure
- LVH:
-
Left ventricular hypertrophy
- WHR:
-
Waist to hip ratio
- HTN:
-
Hypertension
- HDL:
-
High-density lipoproteins
- LDL:
-
Low-density lipoproteins
- TG:
-
Triglycerides
- TC:
-
Total cholesterol
- Hgb:
-
Hemoglobin
- RBC:
-
Red blood cells
- HbA1c:
-
Hemoglobin A1c
- NC:
-
Neck circumferences
- WC:
-
Waist circumferences
- HC:
-
Hip circumferences
- WHR:
-
Waist to hip ratio
- FM:
-
Fat mass
- FFM:
-
Fat-free mass
- LBM:
-
Lean body mass
- ASM:
-
Appendicular skeletal muscle
- FBG:
-
Fasting blood glucose
- GAT:
-
Gluteofemoral adipose tissue
- DXA:
-
Dual-energy X-ray absorptiometry
References
Rai SS, Syurina EV, Peters RMH, Putri AI, Zweekhorst MBM. Non-communicable diseases-related stigma: a mixed-methods systematic review. Int J Environ Res Public Health. 2020;17(18):6657.
Li M, Lin J, Liang S, Huang S, Wen Z, Mo Z. Predicted Fat Mass, lean body Mass, and risk of Hypertension: results from a Chinese male cohort study. Obes Facts. 2022;15(5):638–47.
Azadnajafabad S, Mohammadi E, Aminorroaya A, Fattahi N, Rezaei S, Haghshenas R, et al. Non-communicable Diseases’ risk factors in Iran; a review of the present status and action plans. Journal of Diabetes & Metabolic Disorders; 2021.
Hu L, Hu G, Huang X, Zhou W, You C, Li J, et al. Different adiposity indices and their associations with Hypertension among Chinese population from Jiangxi Province. BMC Cardiovasc Disord. 2020;20(1):115.
Saxton SN, Clark BJ, Withers SB, Eringa EC, Heagerty AM. Mechanistic links between obesity, Diabetes, and blood pressure: role of Perivascular Adipose tissue. Physiol Rev. 2019;99(4):1701–63.
Naguib YM, Samaka RM, Rizk MS, Ameen O, Motawea SM. Countering adipose tissue dysfunction could underlie the superiority of telmisartan in the treatment of obesity-related Hypertension. Cardiovasc Diabetol. 2021;20(1):70.
Wang Z, Zeng X, Chen Z, Wang X, Zhang L, Zhu M, et al. Association of visceral and total body fat with Hypertension and prehypertension in a middle-aged Chinese population. J Hypertens. 2015;33(8):1555–62.
Bohn B, Müller MJ, Simic-Schleicher G, Kiess W, Siegfried W, Oelert M, et al. BMI or BIA: is body Mass Index or Body Fat Mass a Better Predictor of Cardiovascular risk in overweight or obese children and adolescents? A German/Austrian/Swiss Multicenter APV Analysis of 3,327 children and adolescents. Obes Facts. 2015;8(2):156–65.
Jaspers NEM, Dorresteijn JAN, van der Graaf Y, Westerink J, Kappelle LJ, Nathoe HM, et al. Relation between adiposity and vascular events, malignancy and mortality in patients with stable Cerebrovascular Disease. Int J Obes (Lond). 2017;41(12):1775–81.
Qi Q, Sun K, Rong Y, Li Z, Wu Y, Zhang D, et al. Body composition of the upper limb associated with Hypertension, hypercholesterolemia, and Diabetes. Front Endocrinol (Lausanne). 2022;13:985031.
Yano Y, Vongpatanasin W, Ayers C, Turer A, Chandra A, Carnethon MR, et al. Regional Fat distribution and blood pressure level and variability. Hypertension. 2016;68(3):576–83.
Zhao S, Tang J, Zhao Y, Xu C, Xu Y, Yu S et al. The impact of body composition and fat distribution on blood pressure in young and middle-aged adults. Front Nutr. 2022;9.
George C, Goedecke JH, Crowther NJ, Jaff NG, Kengne AP, Norris SA, et al. The Role of Body Fat and Fat Distribution in Hypertension Risk in Urban Black South African women. PLoS ONE. 2016;11(5):e0154894.
Cichosz SL, Rasmussen NH, Vestergaard P, Hejlesen O. Is predicted body-composition and relative fat mass an alternative to body-mass index and waist circumference for Disease risk estimation? Diabetes & Metabolic Syndrome: Clinical Research & Reviews. 2022;16(9):102590.
Shafiee G, Ostovar A, Heshmat R, Darabi H, Sharifi F, Raeisi A, et al. Bushehr Elderly Health (BEH) programme: study protocol and design of musculoskeletal system and cognitive function (stage II). BMJ Open. 2017;7(8):e013606.
Ostovar A, Nabipour I, Larijani B, Heshmat R, Darabi H, Vahdat K, et al. Bushehr Elderly Health (BEH) Programme, phase I (cardiovascular system). BMJ Open. 2015;5(12):e009597.
Samsell L, Regier M, Walton C, Cottrell L. Importance of android/gynoid fat ratio in predicting metabolic and Cardiovascular Disease risk in normal weight as well as overweight and obese children. J Obes. 2014;2014:846578.
Aadahl M, Jørgensen T. Validation of a new self-report instrument for measuring physical activity. Med Sci Sports Exerc. 2003;35(7):1196–202.
Moghaddam MB, Aghdam FB, Jafarabadi MA, Allahverdipour H, Nikookheslat SD, Safarpour S. The Iranian version of International Physical Activity Questionnaire (IPAQ) in Iran: content and construct validity, factor structure, internal consistency and stability. World Appl Sci J. 2012;18(8):1073–80.
Ohkawara K, Ishikawa-Takata K, Park JH, Tabata I, Tanaka S. How much locomotive activity is needed for an active physical activity level: analysis of total step counts. BMC Res Notes. 2011;4(1):512.
Ma G, Luan D, Li Y, Liu A, Hu X, Cui Z, et al. Physical activity level and its association with metabolic syndrome among an employed population in China. Obes Rev. 2008;9(Suppl 1):113–8.
Gao K, Shi X, Wang W. The life-course impact of Smoking on Hypertension, Myocardial Infarction and Respiratory Diseases. Sci Rep. 2017;7(1):4330.
Twinamasiko B, Lukenge E, Nabawanga S, Nansalire W, Kobusingye L, Ruzaaza G, et al. Sedentary lifestyle and Hypertension in a Periurban Area of Mbarara, South Western Uganda: a Population Based Cross Sectional Survey. Int J Hypertens. 2018;2018:8253948.
Nakagomi A, Yasufuku Y, Ueno T, Kondo K. Social determinants of Hypertension in high-income countries: a narrative literature review and future directions. Hypertens Res. 2022;45(10):1575–81.
Roba HS, Beyene AS, Mengesha MM, Ayele BH. Prevalence of Hypertension and Associated factors in dire Dawa City, Eastern Ethiopia: A Community-based cross-sectional study. Int J Hypertens. 2019;2019:9878437.
Shea JL, King MT, Yi Y, Gulliver W, Sun G. Body fat percentage is associated with cardiometabolic dysregulation in BMI-defined normal weight subjects. Nutr Metab Cardiovasc Dis. 2012;22(9):741–7.
Yang Y, Xie M, Yuan S, Zeng Y, Dong Y, Wang Z, et al. Sex differences in the associations between adiposity distribution and cardiometabolic risk factors in overweight or obese individuals: a cross-sectional study. BMC Public Health. 2021;21(1):1232.
Zeng H, Lin C, Wang S, Zheng Y, Gao X. Genetically predicted body composition in relation to cardiometabolic traits: a mendelian randomization study. Eur J Epidemiol. 2021;36(11):1157–68.
Takase M, Nakamura T, Tsuchiya N, Kogure M, Itabashi F, Narita A, et al. Association between the combined fat mass and fat-free mass index and Hypertension: the Tohoku Medical Megabank Community-based Cohort Study. Clin Exp Hypertens. 2021;43(7):610–21.
Saito Y, Takahashi O, Arioka H, Kobayashi D. Associations between body fat variability and later onset of Cardiovascular Disease risk factors. PLoS ONE. 2017;12(4):e0175057.
Atkins JL, Wannamathee SG. Sarcopenic obesity in ageing: cardiovascular outcomes and mortality. Br J Nutr. 2020;124(10):1102–13.
Atkins JL, Whincup PH, Morris RW, Lennon LT, Papacosta O, Wannamethee SG. Sarcopenic obesity and risk of Cardiovascular Disease and mortality: a population-based cohort study of older men. J Am Geriatr Soc. 2014;62(2):253–60.
Ye S, Zhu C, Wei C, Yang M, Zheng W, Gan D, et al. Associations of body composition with blood pressure and Hypertension. Obesity. 2018;26(10):1644–50.
Liu T, Wang Y, Gao N, Zhou J, Wang Y, Fu C, et al. Central Adiposity indicators maintain a stronger Association with the risk of Hypertension: a prospective cohort study in Southwest China. Int J Public Health. 2022;67:1605305.
Wiklund P, Toss F, Weinehall L, Hallmans Gr, Franks PW, Nordström A, et al. Abdominal and Gynoid Fat Mass Are Associated with Cardiovascular Risk factors in men and women. J Clin Endocrinol Metabolism. 2008;93(11):4360–6.
Yan S, Zhao X, Shen X, Yang L, Yuan X, Huang L, et al. Abnormal regional body fat distribution also exists in non-obese subjects with High Blood Pressure. Clin Exp Hypertens. 2013;35(7):528–33.
Kouda K, Nakamura H, Fujita Y, Ohara K, Iki M. Increased ratio of trunk to appendicular fat and increased blood pressure: study of a general population of Hamamatsu children. Circ J. 2012;76(12):2848–54.
Toss F, Wiklund P, Franks PW, Eriksson M, Gustafson Y, Hallmans G, et al. Abdominal and gynoid adiposity and the risk of Stroke. Int J Obes (Lond). 2011;35(11):1427–32.
Dhawan D, Sharma S. Abdominal obesity, Adipokines and non-communicable Diseases. J Steroid Biochem Mol Biol. 2020;203:105737.
Acknowledgements
The authors would like to express their appreciation to all medical research center employees at Bushehr University of Medical Sciences (BPUMS) and Tehran University of Medical Sciences (TUMS) for their dedication and collaboration. The authors would also like to convey their heartfelt appreciation to the Persian Gulf Martyrs Hospital’s Clinical Research Development Center and the Persian Gulf Tropical Medicine Research Center. We would like to thank all participants for their participation in the study.
Funding
The Persian Gulf Biomedical Sciences Research Institute, affiliated with Bushehr (Port) University of Medical Sciences (BPUMS), and the Endocrinology and Metabolism Research Institute, affiliated with Tehran University of Medical Sciences, both contributed to funding for the BEH Program. This study project was designed and carried out with the help of researchers from both research institutions.
Author information
Authors and Affiliations
Contributions
Mohamad Mehdi Khaleghi has the first authorship, and Ali Jamshidi is the co-first author. Study concept and design (IN, AF, BL); acquisition of subjects and/or data analysis and interpretation (MKH, SA, HE, AF); preparation of the manuscript (AJ, MKH, AF, HE, HM, ZJ). All authors have read and approved the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval and consent to participate
Ethics approval and consent to participate The Ethics Committee of Bushehr University of Medical Sciences granted ethical permission for this study (Ethical Code: IR.BPUMS.REC.1401.173) in compliance with the Helsinki Declaration and national guidelines for research ethics. The interviewers diligently apprised all participants of the study’s procedures and methodologies, subsequently procuring written informed consent from each individual. In instances where a participant was unable to execute the consent due to specific circumstances, either legal guardianship facilitated the authorization process and provided the informed consent; or the individual was excluded from participation in the study. Participation remained voluntary, with each contributor retaining the privilege to withdraw their agreement at any juncture without encountering consequences, or opt not to continue with the study.
Consent for publication
The BEH program protocols have confirmed that the human research participants provided written informed consent for the usage of their data for further and secondary analysis. If a participant was unable to give their consent due to specific circumstances, either their legal guardian facilitated the authorization process and provided informed consent, or the individual was excluded from the study. The participants were assured that any use of their data would be non-identifiable, and neither the authors nor the readers would have access to any identifiable personal information. Moreover, any data that could potentially identify individuals would never be published anywhere.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Khaleghi, M.M., Jamshidi, A., Afrashteh, S. et al. The association of body composition and fat distribution with hypertension in community-dwelling older adults: the Bushehr Elderly Health (BEH) program. BMC Public Health 23, 2001 (2023). https://doi.org/10.1186/s12889-023-16950-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12889-023-16950-8