
Abstract
Background
Optimal utilization of antenatal care (ANC) services improves positive pregnancy experiences and birth outcomes. However, paucity of evidence exists on which factors should be targeted to increase ANC utilization among women experiencing intimate partner violence (IPV) in Uganda.
Objective
To determine the independent association between IPV exposure and ANC utilization as well as the predictors of ANC utilization informed by Andersen’s Behavioral Model of Healthcare Utilization.
Methods
We analyzed 2016 Uganda Demographic and Health Survey data that included a sample of 1,768 women with children aged 12 to 18 months and responded to both ANC utilization and IPV items. Our outcome was ANC utilization, a count variable assessed as the number of ANC visits in the last 12 months preceding the survey. The key independent variable was exposure to any IPV form defined as self-report of having experienced physical, sexual and/or emotional IPV. Covariates were grouped into predisposing (age, formal education, religion, problem paying treatment costs), enabling (women’s autonomy, mass media exposure), need (unintended pregnancy, parity, history of pregnancy termination), and healthcare system/environmental factors (rural/urban residence, spatial accessibility to health facility). Poisson regression models tested the independent association between IPV and ANC utilization, and the predictors of ANC utilization after controlling for potential confounders.
Results
Mean number of ANC visits (ANC utilization) was 3.71 visits with standard deviation (SD) of ± 1.5 respectively. Overall, 60.8% of our sample reported experiencing any form of IPV. Any IPV exposure was associated with lower number of ANC visits (3.64, SD ± 1.41) when compared to women without IPV exposure (3.82, SD ± 1.64) at p = 0.013. In the adjusted models, any IPV exposure was negatively associated with ANC utilization when compared to women with no IPV exposure after controlling for enabling factors (Coef. -0.03; 95%CI -0.06,-0.01), and healthcare system/environmental factors (Coef. -0.06; 95%CI -0.11,-0.04). Predictors of ANC utilization were higher education (Coef. 0.27; 95%CI 0.15,0.39) compared with no education, high autonomy (Coef. 0.12; 95%CI 0.02,0.23) compared to low autonomy, and partial media exposure (Coef. 0.06; 95%CI 0.01,0.12) compared to low media exposure.
Conclusion
Addressing enabling and healthcare system/environmental factors may increase ANC utilization among Ugandan women experiencing IPV. Prevention and response interventions for IPV should include strategies to increase girls’ higher education completion rates, improve women’s financial autonomy, and mass media exposure to improve ANC utilization in similar populations in Uganda.
Similar content being viewed by others

Background
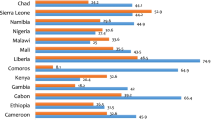
Intimate partner violence (IPV) or behavior that causes physical, sexual or psychological harm perpetrated by an intimate or ex-partner remains a major and pervasive public health problem [1]. Globally, 35% of women are estimated to have ever experienced some form of violence perpetrated by their intimate partner [2]. Sub-Saharan Africa (SSA) has the highest burden of IPV among low and middle- income countries (LMICs), with 45.5% of women experiencing either physical and/or sexual IPV or non-partner sexual violence [3, 4]. In Uganda, 29.9% of women aged 15–49 years and 10.6% of pregnant women report experiencing physical, sexual or emotional violence perpetuated by their intimate male partner within the last 12 months [5]. Comprehensive and multi-institutional approaches to violence prevention may contribute to achievement of Sustainable Development Goal 3 (SDG3) for sustained improvement in women’s and children’s health [6]. IPV is associated with adverse maternal and newborn outcomes among women in SSA [7] that include: preterm births [8, 9], low birth weight (LBW) [10], spontaneous and induced abortion and neonatal mortality [11]. Social problems resulting from IPV include being stigmatized by communities and family [12]. IPV is also associated with negative psychological consequences on IPV survivors such as mental distress [12], depression [13] as well as increasing the risk for HIV acquisition [14].
The World Health Organization (WHO) recommends a minimum of eight focused antenatal care (ANC) visits with the initial visit in the first trimester [15]. According to the most recent Uganda Demographic Health Survey, 60% of women had four or more ANC visits, and 29% had an ANC in their first trimester [16]. Although maternal morbidity and mortality is generally declining in Uganda, it remains high at 375 maternal deaths per 100,000 live births [5, 17, 18]. Evidence shows that attending ANC adequately increases the likelihood of skilled birth attendance [19, 20], and reduces the risk of maternal morbidity and mortality in addition to reducing the risk of adverse birth outcomes such as LBW, stillbirths, neonatal mortality. Positive maternal and child health outcomes (MCH) may be achieved because ANC is a unique opportunity to promote complication readiness and birth preparedness through provision of a range of quality ANC services aimed at recognizing danger signs of pregnancy [21] along the continuum of care [22,23,24,25]. These include routine clinical assessments such as blood pressure measurements, diagnostic evaluations like HIV/STI screening, urine testing, blood group typing, obstetric ultrasound scans for fetal growth monitoring, health education and promotion on breast feeding, and birth planning among others [15]. ANC also includes nutrition advice on iron-folic acid supplementation, deworming, and intermittent preventive treatment for presumptive malaria among others [26]. Studies have shown that low ANC utilization is attributed to inadequate social and financial support, long distances to healthcare facilities [27, 28], unintended pregnancies [29] as well as IPV [24, 25, 30].
Studies consistently show that experiencing IPV lowers ANC clinic attendance in SSA countries [31, 32]. This deterrence from utilizing ANC services limits opportunities to receive the benefits that ANC provides especially being the first point of entry into healthcare systems for pregnant persons for potential detection of IPV among survivors during pregnancy [33]. IPV survivors seek help mostly from family members (57%), followed by their spouse/partner’s family (31%), police (16%); however, most women (71.2%) who experience sexual abuse during pregnancy do not seek any help or tell anyone [5]. Healthcare providers are the least sought after for help following IPV (5%) despite the increased risk of adverse birth outcomes, HIV acquisition, and sero-discordance especially among rural women [34, 35].
Uganda clinical guidelines recommends screening for IPV in primary healthcare settings [33]. This underscores ANC clinics as critical settings to leverage promotion of routine IPV screening by healthcare providers [36, 37] as well as creating opportunities to provide or refer IPV survivors to psychosocial support such as counseling. However, IPV is rarely disclosed or reported by survivors due to fear of retaliatory abuse from partners [38, 39], stigma from society or partners’ family and distrust of healthcare workers [40]. ANC visits provide an opportunity for healthcare workers to build rapport with IPV survivors within a trusting environment and provider-patient relationship fostered to encourage disclosure of spousal abuse [41].
Health worker screening for IPV during ANC supports achievement of the SDG3 target 3.1 to reduce the global maternal mortality [42]. In order to address all forms of gender-based violence (GBV) including IPV, the national policy on elimination of GBV in Uganda [43] prioritizes a multi-sectoral approach using integrated IPV prevention and response efforts. This includes investment in training healthcare providers to gain knowledge and skills to detect IPV, improving health facility infrastructure to allow for more privacy during patient-provider interaction among others. Addressing these policy recommendations may improve detection and disclosure of IPV as well as prompt referrals for existing GBV support services.
Existing literature focuses mainly on individual-level, and socio-cultural determinants of healthcare seeking among women and girls exposed to violence in Uganda [44,45,46,47]. A knowledge gap exists on how the contribution of environmental-, population- and individual-level factors are linked to perpetration of violent behavior by intimate partners and ANC service use by IPV survivors. The Andersen’s behavioral model (ABM) of healthcare utilization is appropriate when evaluating the contribution of enabling, predisposing, and needs factors on choice, access, and/or use of ANC services or facilities. The current paper adopted the ABM of healthcare utilization [48, 49] to examine how ANC utilization is affected by multi-level factors. Previous research in Uganda used the same framework to contextualize predictors of maternal and mental health service use, contraceptive use, and HIV acquisition [50,51,52,53].
For this study, we adopted ABM to identify potential risk/protective factors for ANC utilization from data collected at the national level through the Demographic and Health Survey (DHS) in order to inform response and prevention strategies for violence against women and girls. Therefore, our study objective was to investigate the relationship between IPV and ANC utilization as well as determine the predictors of ANC utilization in Uganda. We hypothesized that the relationship between IPV and ANC utilization would differ among the different groups of ABM factors.
Methods
Study design
We analyzed the 2016 UDHS data for this nationally representative, cross-sectional study among women of reproductive age (15–49 years) in Uganda [54]. This survey was conducted by the Uganda Bureau of Statistics (UBOS) with technical support from USAID-supported MEASURE DHS. The UDHS includes questionnaires for individuals and household members including women, men and biomarker surveys [55]. We analyzed the women’s questionnaire survey data from the 2016 Uganda Demographic Health Survey (UDHS) and the 2014 Uganda Bureau of Statistics (UBOS) health facility data [54, 56].
Data sources
2016 UDHS women’s dataset
The 2016 UDHS dataset is a two-stage stratified cluster survey and the sampling frame includes all census Enumeration Areas (EA) generated by UBOS. In the first stage, 696 accessible EAs were selected, including 162 in urban and 534 in rural areas. In the second stage, a listing of households in each EA was used to select households to be surveyed. Each EA is a geographical area containing an average of 130 households. We used two data files from the 2016 UDHS namely, (i) individual surveys, and (ii) geographic covariate datasets. The survey dataset contains the respondent’s socio-demographic characteristics, and domestic violence items.
2014 UBOS health facility geocode dataset
We extracted geographical coordinates of public health facilities, their HC levels, and geocodes from the 2014 UBOS visualization dashboard [56] into MS Excel. Health facility coordinates identified their location at region, sub-county, and district levels [56]. We exported health facility geocodes into ArcGIS software to compute spatial accessibility as the near point linear distance in meters between EA centroids/clusters and the nearest health facility providing ANC.
Uganda healthcare referral system
The national healthcare system in Uganda is comprised of public and private health sectors [57] providing healthcare services through a decentralized system at national, district and health sub-district levels. In Uganda, ANC services are facility-based and provided at health centers (HC) III, HC IV and hospital levels [58]. At the district level, the healthcare referral system is comprised of village health teams (VHTs), health centers (HC) II, HC III and HC IV [59]. The catchment area for populations served by these HC’s increases from fewer than 500, to 100,000 respectively as described elsewhere [60]. These mainly offer basic prevention, promotion and curative services through outpatient and community outreach. All HCs provide ANC services [57]; however, HC IVs provide additional comprehensive emergency obstetrics and newborn care (CEmONC) services [61].
Study population
Pregnant women with or without exposure to IPV during pregnancy were identified using the IPV and pregnancy status items selected from the Domestic Violence Module [54] that adopted the Revised Conflict Tactics Scale [62]. The total population of women aged 15 to 49 years in the 2016 UDHS individual recode dataset was 18,506. Figure 1 illustrates the flow chart for the criteria followed to create of our study sample of women aged 15–49 years. Our inclusion criteria were women who responded > = 0 to the item asking about the frequency of ANC service use in the last 12 months. These were women aged 15–49 years whose most recent birth was a live birth, and has a child aged 12–18 months. We excluded: (i) participants who “did not know” (n = 44) or had “missing” responses to number of ANC visits item and (ii) participants who did not respond to all of the items assessing sexual, psychological or physical IPV as shown in Fig. 1. Finally, our study population used for analyses was a sub-population of women in the 2016 UDHS dataset who had responses to both IPV (yes/no) and ANC utilization items (n = 1,768).

Derivation of our study population
Study measures
Outcome variable
The dependent variable was utilization of ANC. This was a count variable measured as the number of ANC visits that study participants had during pregnancy in the last 12 months preceding the UDHS survey. Data on ANC visits was collected among individuals at household level as described elsewhere [16].
Key independent variable
Our key independent variable was exposure to at least one form of IPV in the last twelve months (any IPV) preceding this survey interview. This was a composite categorical variable measured as exposure to any: (i) physical, (ii) sexual, and/or (iii) psychological IPV using the revised Conflict Tactics Scale [62]. Similar measures of IPV (any IPV) have been used in previous studies conducted in Uganda [63, 64]. Any IPV form was a categorical variable reported as the proportion of women who reported experiencing at least one of the three IPV forms during pregnancy.
Regarding items measuring physical IPV, respondents were asked whether in the past twelve months, their husband/partner (current or last) ever did the following: “push you, shook or throw something at you”, “slap you”, “fist punch or hit you with something harmful”, “kick or drag you”, “strangle or burn you”, “threaten you with knife/gun or other weapon” and/or “arm twist or hair pulled”. A composite binary variable, physical IPV (No/Yes) namely, was constructed No = Never experienced any physical IPV/Yes = Ever experienced at least one form of physical IPV.
Concerning emotional IPV items, participants were asked whether in the past twelve months, their husband/partner (current or last) ever did the following: “humiliate you”, “threaten you with harm”, and/or “insult or made you feel bad”. These three variables were merged into a binary variable for emotional IPV (No = Never experienced any emotional IPV form/Yes = Ever experienced at least one emotional form of IPV.
In relation to sexual IPV items, participants were asked whether in the past twelve months, their husband/partner (current or last) ever did the following: physically force you into unwanted sex with him? force you into other unwanted sexual acts? and physically forced you to perform sexual acts when you did not want to? A dichotomous composite sexual IPV variable was computed; No = Never experienced any sexual IPV form/Yes = Ever experienced at least one sexual IPV form. Any IPV in the last twelve months was generated as women who reported experiencing either physical, emotional, or sexual violence were coded 1(Yes) while those who reported no to all three types were coded as 0(No).
Covariates
Our study adopted ABM domains [65] in order to explore which group/block of factors that explain the association between exposure to IPV and ANC utilization can be targeted by interventions to prevent violence against women. Therefore, ABM informed selection of predictor variables, which were categorized into four blocks, namely, predisposing, enabling, need and healthcare system/environmental factors. Figure 2 demonstrates our conceptual framework of the adapted Andersen’s behavioral model of healthcare utilization. Predisposing factors refer to factors that influence an individual’s planned or intended healthcare seeking behavior, specifically ANC utilization in the current study. Enabling factors is comprised of factors that may facilitate ANC use or their healthcare seeking behavior. Need factors are composed of an individuals’ perceived or actual health or functional needs. The ABM posits that these groups of factors can collectively influence an individuals’ health seeking behavior, particularly ANC utilization. We grouped our covariates based on these ABM domains described in detail as follows.

Conceptual framework of the adapted Andersen’s behavioral model of healthcare utilization
Predisposing factors. Women’s age was grouped into 15–24, 25–34 and ≥ 35 years of age categories. Education level was categorized into none, primary, secondary and tertiary groups, while religion was categorized into Christian, Muslim, or other groups. We also categorized the item which assessed whether the participant experienced problems getting money for medical treatment (yes/no).
Enabling factors. Women’s autonomy was measured using four items based on prior literature [66, 67], namely whether the respondent: (i) usually decides how to spend respondent’s earnings, (ii) usually make decisions alone about major household purchases, (iii) owns a house alone or jointly, and (iv) owns land alone or jointly. Based on these three items, we generated a composite sum score of women’s autonomy ranging from zero to four, and then categorized the score into three groups: low (none of the items), medium (score 1 to 3), and high (score 4). We generated the mass media exposure variable informed by measurements in prior literature [67, 68]. The three mass media exposure items were: (i) frequency of reading newspapers/magazines, (ii) watching television, and (iii) listening radio. Then, we generated a composite measure ranging from 0 to 3 and categorized into three groups, namely: no exposure (no media exposure), some exposure (one or two media exposures), and full exposure (access to all three mass media items).
Need factors. Items on pregnancy intention assessed whether the respondent wanted their last child (wanted then, wanted later, or wanted no more). We categorized a binary variable as “No” pregnancy wanted later or wanted no more and “Yes” pregnancy wanted then. Parity was a continuous variable defined as the total number of children ever born. ‘Ever terminated pregnancy’ variable assessed whether we the participant has a history of ever terminating a pregnancy (yes/no).
Healthcare system/Environmental factors. Spatial accessibility was categorized as ≥ 5 km (low) or < 5 km (optimal) accessibility based on prior literature [69,70,71,72]. Residence was categorized into two nominal categories (rural and urban).
Data analysis
Descriptive statistics. Data were analyzed using Stata/MPv18.0 and ArcGIS software v16.0 as follows. First, summary statistics were computed for the socio-demographic characteristics and covariates for participants by the mean number of ANC visits. We summarized participant characteristics using frequencies and their respective percentages. Two-sample t-tests, and one-way ANOVA tests were used to assess differences in mean ANC utilization with their corresponding standard deviation (SD) by each participant characteristic with binary, and three or more categories respectively.
Unadjusted Poisson regression analysis. Second, unadjusted Poisson regression models were run for IPV and each covariate against ANC utilization. Figure 3 illustrates the Poisson regression formula highlighting the outcome variable Y as a ANC count (Y/t) with a Poisson distribution with an expected (mean) count of Yi, β0 = intercept, and βj = coefficient of independent variable Xj. Third, interaction terms run were not statistically significant for the relationship between IPV and ANC utilization by rural/urban residence, therefore, stratified analyses were not conducted. Fourth, there was no collinearity between all covariates. Variables with p-values < 0.2 [73] in unadjusted analyses were included in the adjusted models to determine the; (i) independent association of IPV on ANC utilization, and (ii) predictors of ANC utilization.

Poisson regression formula
Adjusted Poisson regression analysis. Fifth, separate adjusted Poisson regression models were run according to blocks of factors from Andersen’s behavioral model of healthcare utilization as follows: the first model controlled for predisposing factors (Model 1) namely, age, formal education, religion, and experiencing problems paying treatment costs. The second model controlled for enabling factors (Model 2) namely, women’s autonomy, and the degree of exposure to mass media. The third model controlled for need factors (Model 3) namely, unintended pregnancy, parity, and history of pregnancy termination. The fourth model, healthcare system/environmental factors controlled for were rural/urban residence, and spatial accessibility. Lastly, an adjusted Poisson regression model was run for the predictors of ANC utilization (Table 3). We included variables that were statistically significant and variables with p < 0.2 in the unadjusted models into the adjusted model. Statistical significance was determined at p < 0.05.
All Poisson regression models were run to generate unadjusted and adjusted coefficients with their 95% confidence intervals by using generalized linear models with link (log) and family (Poisson) commands [74, 75]. Poisson models were run because our outcome variable - ANC utilization in the last 12 months preceding the survey was a count variable [76]. Survey weights were applied to all analyses based on the DHS survey design which accounts for complex survey sampling. Survey commands were run in Stata/MPv18.0 by applying probability/sampling weight (pweight), primary sampling unit (psu) and stratification used in the sample design (strata). pweight were computed using the domestic violence weight as described in the DHS methodology. Strata with a single sampling unit were treated as certainty units.
Ethical considerations
This study was approved by The AIDS Support Organization (TASO) Institutional Review Board (IRB) Ref: TASOREC/083/19-UG-REC-009 and Medical College of Wisconsin (MCW) Ethical Review Committee Ref No: PRO00036397. Permission was obtained from Uganda National Council of Science and Technology (UNCST) Ref: SS 5243. All women who participated in the 2016 UDHS gave informed consent as described elsewhere [54]. Both 2016 UDHS and 2014 UBOS Health facility datasets are publicly available data [56, 77].
Results
In Table 1, the mean ± SD age of respondents was 35.8 ± 4.8 years while the mean ± SD number of ANC visits (ANC utilization) was 3.7 ± 1.5 visits. Overall, 60.8% of respondents reported experiencing at least one form of sexual, physical and/or emotional IPV (any IPV). In addition, women who experienced any IPV had significantly lower mean ± SD number of ANC visits (3.64 ± 1.41) than those without any IPV exposure (3.82 ± 1.64), p = 0.013. ANC utilization was lowest among women: (i) with problems paying treatment costs (3.58 ± 1.41) when compared to those without problems paying treatment costs (3.82 ± 1.60) at p < 0.001, and (ii) who self-reported their pregnancy as being unintended (3.62 ± 1.50) when compared to those with pregnancies self-reported to be intended (3.75 ± 1.50), p < 0.001 (Table 1). Also, the mean ± SD ANC utilization was significantly lower among women in rural settings compared to urban dwellers [3.63 ± 1.45 vs. 3.99 ± 1.71, p < 0.001] and those with low spatial accessibility to the nearest health facility compared to those with optimal spatial accessibility to the nearest health facility [3.58 ± 1.39 vs. 3.76 ± 1.58, p < 0.001] as shown in Table 1.
Table 2 presents the unadjusted and adjusted Poisson regression models for the association between IPV and ANC utilization. In the unadjusted model, IPV exposure was significantly associated with lower ANC utilization (Coef − 0.06; -95%CI -0.11,-0.01, p = 0.028) when compared to no IPV exposure.
Sequential analyses using ABM domains/blocks
Table 2 shows that exposure to IPV was significantly associated with low ANC utilization when compared to those with no IPV exposure after controlling for enabling factors (Coef. -0.02; 95%CI -0.04,-0.01, p = 0.021) in Model 2, and environmental/healthcare system factors in (Coef − 0.06; 95%CI -0.11,-0.04, p = 0.036) (Model 4). Conversely, the association between IPV exposure and ANC utilization was not statistically significant after controlling for predisposing factors (Model 1) and need factors (Model 3).
Adjusting using factors in ABM domains
Model 1
Among the predisposing factors controlled for, women aged 15–24 years were more likely to.
utilize ANC when compared to women aged ≥ 35 years (Coef 0.21; 95%CI 0.03, 0.39, p = 0.024); women with secondary education (Coef 0.11; 95%CI 0.03, 0.20, p = 0.010), and secondary education (Coef 0.33; 95%CI 0.21, 0.44, p < 0.001) were more likely to utilize ANC when compared to those with no formal education (Table 2).
Model 2
After controlling for enabling factors, high autonomy was associated with higher ANC utilization when compared to low autonomy (Coef. 0.12; 95%CI 0.02, 0.23, p = 0.016). In addition, high mass media exposure (Coef. 0.22; 95%CI 0.12, 0.32, p < 0.001) and partial mass media exposure (Coef. 0.08; 95%CI 0.03, 0.13, p = 0.002) were associated with more ANC visits when compared to those with low mass media exposure (Table 2).
Model 3
Regarding need factors, each unit increase in parity (total number of children ever born) was.
significantly associated with lower ANC utilization (Coef. -0.03; 95%CI -0.04, -0.02, p < 0.001) (Table 2).
Model 4
Among healthcare system/environmental factors controlled for in Model 4, low spatial accessibility to nearest health facilities was associated with lower ANC utilization when compared to optimal spatial accessibility to nearest health facilities (Coef. -0.11; 95%CI -0.03, -0.01, p = 0.030) (Table 2).
Table 3 illustrates the predictors of ANC utilization among women of reproductive age (15–49 years) in Uganda. ANC utilization was more likely among women with: higher education compared to those with no education (Coef. 0.27; 95%CI 0.15,0.39), high autonomy compared to those with low autonomy (Coef. 0.12; 95%CI 0.02,0.23), and partial media exposure compared to those with low media exposure (Coef. 0.06; 95%CI 0.01,0.12).
Discussion
To our knowledge, this is one of the first studies to examine the association between IPV and ANC utilization using a nationally representative population of women aged 15 to 49 years in Uganda. Methodologically, we adopted Andersen’s behavioral model of healthcare utilization in order to identify blocks of factors which, when controlled for, affected the relationship between IPV and ANC use. Our study revealed two key findings. First, exposure to any form of IPV was associated with lower ANC visits when compared to women not exposed to IPV after controlling for enabling, and healthcare system/environmental factors respectively. Secondly, the predictors of ANC utilization were attaining higher education, high autonomy levels, and obtaining some (partial) mainstream media exposure. There is a paucity of studies conducted in Uganda that have assessed the relationship between IPV and use of ANC services. However, our findings were in line with previous studies conducted in other SSA countries [30, 78, 79]. For example, women surveyed in Togo who experienced any form of IPV had reduced the number of ANC visits [30], while IPV exposure significantly reduced ANC utilization among women in one province of Mozambique [78]. Similarly, a review representing ten LMICs revealed that experiencing IPV reduced the odds of ANC use [80]. Several potential reasons may explain the association between IPV and ANC utilization.
First, this could be due to low economic autonomy of women experiencing IPV [81] which affects decision making about their finances. This suggests that women who experience IPV may not be able to meet the costs and expenditures needed to obtain ANC. Similarly, as illustrated in our study using the Andersen’s Behavioral Model, high women’s autonomy is an enabling factor that predicted increased ANC utilization. These findings underscore the benefits of promoting economic empowerment like (self)employment [82] guided by theory informed intervention targets. Poverty is another barrier to ANC use especially among women with low-income who may not be able to pay the costs for ANC use. Prior research shows that a woman’s ability to pay for ANC such as their wealth status [83], getting cash payments for their work [84], affects ANC use. This concurred with our study showing that women who had problems paying their treatment costs were less likely to use ANC. Therefore, economic empowerment interventions may increase women’s sources of income and subsequently help women use ANC [85, 86]. Prior research also shows that financial independence may support women in negotiating better treatment within their relationship or leave unsafe circumstances [87]. Conversely, its noteworthy that although empowering women economically is beneficial, it may also increase IPV perpetration because their male partners/spouses may view women’s financial growth as a threat to their control [88].
Secondly, another key factor that potentially explains the negative association between IPV and ANC use could be access to information such as health communication through mainstream media. We revealed that some exposure to mass media increased the likelihood for ANC use. The policy implications of promoting maternal and child health through the media platforms and mobile phone communication are well demonstrated [89,90,91]. We propose to stakeholders, that they should prioritize the inclusion of women’s preferred or appropriate communication channels during provision of ANC to women experiencing IPV.
The second reason that may potentially explain the relationship between IPV and ANC utilization are the psychological and/or mental health effects of IPV. These include perinatal depression, post-traumatic stress disorder among others which may delay IPV survivors’ decision making to seek [92] and late entry [79] into ANC. The risk of subsequent postpartum depression is likely and may be high among women in Uganda [93,94,95].
The fourth reason that could explain the association between IPV and low ANC utilization is unintended pregnancies which tends to occur with perpetration of sexual IPV [96,97,98]. Although our findings showed no association between unintended pregnancy and ANC utilization, prior studies showed that women with sub-optimal ANC visits are more likely to report having an unintended pregnancy [99]. This could be attributed to lack of autonomy in contraceptive decision-making [100] through coercion for pregnancy [101, 102], and contraceptive sabotage by male intimate partners [103, 104] [105]. Our findings call for ANC providers to screen for IPV among pregnant women attending ANC in order to provide or refer IPV survivors for recommended psychosocial and medical management including counseling for family planning according to national policies aimed at the elimination of GBV in Uganda [33, 106].
Finally, another potential reason that may explain the association between IPV and ANC utilization are the healthcare system factors evaluated were rural/urban residence and distance to nearest ANC service providing facility. Prior studies conducted in Uganda [107,108,109,110,111] were in line with our findings showing that shorter distances to the nearest ANC service providing facility were predictors of early or first trimester ANC visits. Related findings were found in other SSA countries which showed that longer distances to the nearest health facilities reduced the number of ANC visits to four or fewer in Ethiopia [112]. Contrary to our findings, prior research conducted in the SSA countries of Ghana [113] and Rwanda [114] found that distance was not associated with optimal ANC utilization. One explanation for this contrary previous finding from the latter countries could be due to implementation of unique national health insurance schemes in Ghana [115, 116], and Rwanda [117, 118] which may address structural barriers to ANC use such as healthcare costs. Regarding the benefits of addressing financial barriers to health service use, prior research from Uganda showed that health insurance increased likelihood for ANC use [119]. The current policy discourse to introduce a national health insurance scheme in Uganda is promising. This may help alleviate barriers to ANC use such as high out-of-pocket payments for ANC use [120].
Future studies should evaluate the impact of IPV on ANC utilization in Uganda using recent data that incorporates current WHO updates to measure eight (8) or more ANC visit cut-offs. Also, future research should assess mediating and moderating effects of predisposing and need factors on the relationship between IPV and ANC utilization. In addition, temporal effects of IPV and ANC utilization should be assessed using longitudinal data in order to draw potential causal inferences. Future research should also use exploratory qualitative methods such as in-depth interviews among women both in communities and health facilities in order to identify underlying factors influencing survivors’ use of ANC as targets for interventions. Policy implications of our findings reveal key targets for policy makers to modify current national policies on elimination of GBV [106] to address/alleviate IPV among pregnant women. Such policy changes should target poverty alleviation, ensure equitable access to ANC, empowerment strategies to improve women’s economic autonomy, ANC education using innovative media and mobile health education platforms to increase ANC utilization.
Study strengths and limitations
Our study has some strengths. First, we applied survey weights to our analysis making our results generalizable to the population of women with or without: (i) IPV exposure and (ii) ANC attendance. Secondly, we measured exposure to any form of IPV using items that assessed the different IPV forms, namely emotional, sexual, and physical forms of violence in the last 12 months. We consider this composite IPV measure a strength because IPV is known to be under-reported especially in the socio-cultural context of some communities in Uganda where violence against women and girls may be condoned. Our study also had some limitations. First, data analyzed from the 2016 UDHS is drawn from a cross-sectional, population-based survey and therefore causal-temporal inferences should not be deduced. Secondly, recall bias may have affected responses to IPV items in the UDHS survey since these questions probed for potential IPV events that occurred over the last twelve months. Finally, social desirability bias may have occurred and experiencing IPV may be under-reported.
Conclusions
Mitigation initiatives and future intervention designs aimed at alleviating IPV should consider addressing enabling and healthcare system/environmental factors to increase ANC utilization among Ugandan women experiencing IPV. Comprehensive strategies to alleviate the impact of IPV should aim at improving higher education completion rates for girls, promote women’s financial autonomy via ongoing poverty eradication efforts, use mass media platforms for health promotion, and improving physical accessibility to health facilities in similar populations in Uganda.
Data Availability
The datasets generated and/or analysed during the current study are available in the DHS Program repository, https://dhsprogram.com/data/available-datasets.cfm for 2016 UDHS data, and the UBOS website accessed via https://ubos.maps.arcgis.com/apps/webappviewer/index.html?id=0fbc1dae45a24f3b89ff61c1f314d375 for the 2014 UBOS health facility geocodes.
References
CDC. Violence Prevention. 2020 October 9, 2020 February 6, 2021]; Available from: https://www.cdc.gov/violenceprevention/intimatepartnerviolence/index.html
WHO. Violence against women. 2018 February 6, 2021]; Available from: https://www.who.int/news-room/fact-sheets/detail/violence-against-women
UN. The Beijing declaration and platform for action turns 20. UN Women; 2015.
Muluneh MD, et al. Gender based violence against women in sub-saharan Africa: a systematic review and meta-analysis of cross-sectional studies. Int J Environ Res Public Health. 2020;17(3):903.
UDHS. Uganda demographic and health survey 2016: key indicators report. UBOS, and Rockville Maryland: Uganda Bureau of Statistics, ICF; 2017.
UN. Sustainable Development Goals. 2020 February 6, 2021]; Available from: https://www.un.org/sustainabledevelopment/health/
Ahinkorah BO. Intimate partner violence against adolescent girls and young women and its association with miscarriages, stillbirths and induced abortions in sub-saharan Africa: evidence from demographic and health surveys. SSM-Population Health. 2021;13:100730.
Laelago T, Belachew T, Tamrat M. Effect of intimate partner violence on birth outcomes. Afr Health Sci. 2017;17(3):681–9.
Sigalla GN, et al. Intimate partner violence during pregnancy and its association with preterm birth and low birth weight in Tanzania: a prospective cohort study. PLoS ONE. 2017;12(2):e0172540.
Musa A, Chojenta C, Loxton D. The association between intimate partner violence and low birth weight and preterm delivery in eastern Ethiopia: findings from a facility-based study. Midwifery. 2021;92:102869.
Shamu S, et al. Intimate partner violence, forced first sex and adverse pregnancy outcomes in a sample of zimbabwean women accessing maternal and child health care. BMC Public Health. 2018;18(1):1–10.
Overstreet NM, et al. The moderating role of centrality on the association between internalized intimate partner violence-related stigma and concealment of physical IPV. J Soc Issues. 2017;73(2):307–21.
Belay S, et al. Intimate partner violence and maternal depression during pregnancy: a community-based cross-sectional study in Ethiopia. PLoS ONE. 2019;14(7):e0220003.
Kiene SM, et al. Depression, alcohol use, and intimate partner violence among outpatients in rural Uganda: vulnerabilities for HIV, STIs and high risk sexual behavior. BMC Infect Dis. 2017;17(1):1–13.
Organization WH. WHO recommendations on antenatal care for a positive pregnancy experience. World Health Organization; 2016.
UDHS. Uganda demographic and health survey 2016, in key indicators report. UBOS, and Rockville Maryland: Uganda Bureau of Statistics, ICF; 2016.
UDHS. Uganda demographic and health survey, in Uganda Bureau of Statistics, Kampala Uganda. Uganda Bureau of Statistics ORC Macro. MEASURE/DHS+; 2011.
UDHS, Uganda Demographic and Health Survey, 2006. 2007, Uganda Bureau of Statistics: Uganda Bureau of Statistics ORC Macro. MEASURE/DHS+.
Sserwanja Q, Mutisya LM, Musaba MW. Exposure to different types of mass media and timing of antenatal care initiation: insights from the 2016 Uganda demographic and Health Survey. Volume 22. BMC women’s health; 2022. pp. 1–8. 1.
Sserwanja Q, et al. Factors associated with health facility utilization during childbirth among 15 to 49-year-old women in Uganda: evidence from the Uganda demographic health survey 2016. BMC Health Serv Res. 2021;21(1):1–13.
Kerber KJ, et al. Continuum of care for maternal, newborn, and child health: from slogan to service delivery. The Lancet. 2007;370(9595):1358–69.
de Graft-Johnson J, et al. The maternal, newborn and child health continuum of care. Opportunities for Africa’s Newborns; 2006. pp. 23–36.
Donovan B, et al. Intimate partner violence during pregnancy and the risk for adverse infant outcomes: a systematic review and meta-analysis. BJOG: An International Journal of Obstetrics & Gynaecology. 2016;123(8):1289–99.
Anguzu R, et al. Facilitators and barriers to routine intimate partner violence screening in antenatal care settings in Uganda. BMC Health Serv Res. 2022;22(1):1–15.
Cassidy LD et al. Healthcare provider experiences interacting with survivors of intimate partner violence: A qualitative study to inform survivor-centered approaches 2023.
Kisuule I, et al. Timing and reasons for coming late for the first antenatal care visit by pregnant women at Mulago hospital, Kampala Uganda. BMC Pregnancy Childbirth. 2013;13:1–7.
Roed MB, et al. Women’s experiences of maternal and newborn health care services and support systems in Buikwe District, Uganda: a qualitative study. PLoS ONE. 2021;16(12):e0261414.
Namusana R, et al. Experiences of seeking Antenatal Care and Delivery among Teenagers in Kibuku District, Uganda. J Res Health. 2022;12(4):239–52.
Basaza RK, Mawerere JN, Namusana R. Experiences of seeking antenatal care and delivery among teenagers at health facilities in Kibuku District, Eastern Uganda 2020.
Ragetlie R, et al. Married women’s experiences of intimate partner violence and utilization of antenatal health care in Togo. Volume 23. Sexual & Reproductive Healthcare; 2020. p. 100482.
Ononokpono DN, Azfredrick EC. Intimate partner violence and the utilization of maternal health care services in Nigeria. Health Care Women Int. 2014;35(7–9):973–89.
Okedo-Alex IN, et al. Determinants of antenatal care utilisation in sub-saharan Africa: a systematic review. BMJ open. 2019;9(10):e031890.
MoH. Uganda Clinical Guidelines 2016, in National guidelines for management of common conditions. Ministry of Health, Uganda; 2016.
Kouyoumdjian FG, et al. Intimate partner violence is associated with incident HIV infection in women in Uganda. Aids. 2013;27(8):1331–8.
Osinde MO, Kaye DK, Kakaire O. Intimate partner violence among women with HIV infection in rural Uganda: critical implications for policy and practice. BMC Womens Health. 2011;11(1):1–7.
Phelan MB. Screening for intimate partner violence in medical settings. Trauma Violence & Abuse. 2007;8(2):199–213.
Hamberger LK, Rhodes K, Brown J. Screening and intervention for intimate partner violence in healthcare settings: creating sustainable system-level programs. J Women’s Health. 2015;24(1):86–91.
Vranda MN, et al. Barriers to disclosure of intimate partner violence among female patients availing services at tertiary care psychiatric hospitals: a qualitative study. J Neurosciences Rural Pract. 2018;9(3):326.
Kaye D. Domestic violence among women seeking post-abortion care. Int J Gynecol Obstet. 2001;75(3):323–5.
McCleary-Sills J, et al. Stigma, shame and women’s limited agency in help-seeking for intimate partner violence. Glob Public Health. 2016;11(1–2):224–35.
Mantler T, et al. Factors influencing rural women’s disclosure of intimate partner violence: a qualitative study. SN Social Sciences. 2021;1(1):1–19.
Nations U. Sustainable development goal 3: ensure healthy lives and promote well-being for all at all ages. New York: UN; 2018.
MoGLSD. The National Policy on elimination of gender based violence 2019, Ministry of Gender, Labour and Social Development.
Kouyoumdjian FG, et al. Risk factors for intimate partner violence in women in the Rakai Community Cohort Study, Uganda, from 2000 to 2009. BMC Public Health. 2013;13:1–9.
Young CR, et al. Prevalence and correlates of physical and sexual intimate partner violence among women living with HIV in Uganda. PLoS ONE. 2018;13(8):e0202992.
Mutumba M, Bhattacharya S, Ssewamala FM. Assessing the social patterning and magnitude of inequalities in sexual violence among young women in Uganda: findings from 2016 demographic and health survey. Glob Public Health. 2022;17(11):2826–40.
Okumu M, et al. Socioeconomic factors and patterns of intimate partner violence among ever-married women in Uganda: pathways and actions for multicomponent violence prevention strategies. J Interpers Violence. 2022;37(17–18):NP16397–420.
Andersen RM. Revisiting the behavioral model and access to medical care: does it matter? J Health Soc Behav, 1995: p. 1–10.
Fletcher JM, Frisvold DE. Higher education and health investments: does more schooling affect preventive health care use? J Hum Capital. 2009;3(2):144–76.
Mbalinda SN et al. Using Andersen’s behavioral model of health care utilization to assess contraceptive use among sexually active perinatally HIV-infected adolescents in Uganda International Journal of Reproductive Medicine, 2020. 2020.
Rutaremwa G, et al. Determinants of maternal health services utilization in Uganda. BMC Health Serv Res. 2015;15:1–8.
Byansi W, et al. Patterns of and factors associated with mental health service utilization among school-going adolescent girls in southwestern Uganda: a latent class analysis. J Adolesc Health. 2023;72(5):S24–S32.
Sileo KM, et al. Determinants of family planning service uptake and use of contraceptives among postpartum women in rural Uganda. Int J Public Health. 2015;60:987–97.
UBOS. Uganda demographic and health survey 2016: key indicators report. UBOS, and Rockville Maryland; 2017.
UDHS. Health Survey Key Indicators Report 2016. Uganda Bureau of Statistics; 2017.
UBOS. Access to Health Facility. 2014 [cited 2023 May 20, 2023]; Available from: https://ubos.maps.arcgis.com/apps/webappviewer/index.html?id=0fbc1dae45a24f3b89ff61c1f314d375.
MoH. Annual Health Sector Performance Report: Financial Year 2015/16. Ministry of Health - Uganda: Kampala, Uganda; 2016.
MoH. Health Sector Strategic Plan III 2010/11-2014/15. Ministry of Health; 2010.
MoH. Uganda Hospital and Health Centre IV Census Survey. Ministry of Health Uganda; 2014.
Sensalire S, et al. Saving mothers, giving life approach for strengthening health systems to reduce maternal and newborn deaths in 7 scale-up districts in northern Uganda. Global Health: Science and Practice. 2019;7(Supplement 1):S168–87.
Mbonye AK, et al. Emergency obstetric care as the priority intervention to reduce maternal mortality in Uganda. Int J Gynecol Obstet. 2007;96(3):220–5.
Straus MA, et al. The revised conflict tactics scales (CTS2) development and preliminary psychometric data. J Fam Issues. 1996;17(3):283–316.
Kwagala B, et al. Empowerment, partner’s behaviours and intimate partner physical violence among married women in Uganda. BMC Public Health. 2013;13(1):1112.
Wandera SO, et al. Partners’ controlling behaviors and intimate partner sexual violence among married women in Uganda. BMC Public Health. 2015;15(1):214.
Andersen R. A behavioral model of families’ use of health services. Behav model families’ use health Serv, 1968(25).
Roy A, et al. Prevalence and correlates of menstrual hygiene practices among young currently married women aged 15–24 years: an analysis from a nationally representative survey of India. Eur J Contracept Reproductive Health Care. 2021;26(1):1–10.
Karjee S, Rahaman M, Biswas PC. Contextualizing the socio-economic and spatial patterns of using menstrual hygienic methods among young women (15–24 years) in India: a cross-sectional study using the nationally representative survey. Clin Epidemiol Global Health. 2023;20:101253.
Rahaman M, et al. Spatial heterogeneity and socio-economic correlates of unmet need for spacing contraception in India: Evidences from National Family Health Survey, 2015-16. Clin Epidemiol Global Health. 2022;15:101012.
Lwasa S. Geospatial analysis and decision support for health services planning in Uganda. Geospat Health. 2007;2(1):29–40.
Zinszer K, et al. Determining health-care facility catchment areas in Uganda using data on malaria-related visits. Bull World Health Organ. 2014;92:178–86.
Ouma P, et al. Methods of measuring spatial accessibility to health care in Uganda, in practicing Health Geography: the african context. Springer; 2021. pp. 77–90.
Karra M, Fink G, Canning D. Distance to Health Facilities, Maternal Health Care Utilization, and Child Mortality, in Low-and Middle-Income Countries. in 2016 Annual Meeting. 2016. PAA.
Hosmer D. Lemeshow S. Applied logistic regression New York, 2000.
Barros AJ, Hirakata VN. Alternatives for logistic regression in cross-sectional studies: an empirical comparison of models that directly estimate the prevalence ratio. BMC Med Res Methodol. 2003;3(1):1–13.
Zou G. A modified poisson regression approach to prospective studies with binary data. Am J Epidemiol. 2004;159(7):702–6.
skove T, et al. Prevalence proportion ratios: estimation and hypothesis testing. Int J Epidemiol. 1998;27(1):91–5.
UBOS. The national population and housing census 2014–main report. Uganda Bureau of Statistics; 2016.
Tura H, Licoze A. Women’s experience of intimate partner violence and uptake of Antenatal Care in Sofala, Mozambique. PLoS ONE. 2019;14(5):e0217407.
Gashaw BT, Magnus JH, Schei B. Intimate partner violence and late entry into antenatal care in Ethiopia. Women Birth. 2019;32(6):e530–7.
Metheny N, Stephenson R. Intimate partner violence and uptake of antenatal care: a scoping review of low-and middle-income country studies. Int Perspect Sex Reproductive Health. 2017;43(4):163–71.
Casabianca MS et al. The Competing Impacts of Self-Employment on Intimate Partner Violence and Women’s Economic Autonomy 2023.
Kwagala B, et al. Empowerment, partner’s behaviours and intimate partner physical violence among married women in Uganda. BMC Public Health. 2013;13(1):1–10.
Edward B. Factors influencing the utilisation of antenatal care content in Uganda. Australasian Med J. 2011;4(9):516.
Idriss-Wheeler D, Yaya S. Exploring antenatal care utilization and intimate partner violence in Benin-are lives at stake? BMC Public Health. 2021;21(1):830.
Sserwanja Q, Nabbuye R, Kawuki J. Dimensions of women empowerment on access to antenatal care in Uganda: a further analysis of the Uganda demographic health survey 2016. Int J Health Plann Manag. 2022;37(3):1736–53.
Kwagala B, et al. Empowerment, intimate partner violence and skilled birth attendance among women in rural Uganda. Reproductive Health. 2016;13(1):1–9.
Becker P, Kafonek K, Manzer JL. Feminist perspectives of intimate partner violence and abuse (IPV/A), Handbook of interpersonal violence and abuse across the lifespan: a project of the National Partnership to end interpersonal violence across the Lifespan (NPEIV). 2021, Springer. 2327–52.
del Eggers I, Steinert JI. The effect of female economic empowerment interventions on the risk of intimate partner violence: a systematic review and meta-analysis. Volume 23. Trauma, Violence, & Abuse; 2022. pp. 810–26. 3.
Aboagye RG, et al. Association between frequency of mass media exposure and maternal health care service utilization among women in sub-saharan Africa: implications for tailored health communication and education. PLoS ONE. 2022;17(9):e0275202.
Asp G, et al. Associations between mass media exposure and birth preparedness among women in southwestern Uganda: a community-based survey. Global Health Action. 2014;7(1):22904.
Sserwanja Q, Mutisya LM, Musaba MW. Mass Media Exposure and Timing of Antenatal Care Initiation among Women in Uganda 2021.
Mahenge B, et al. Intimate partner violence during pregnancy and associated mental health symptoms among pregnant women in T anzania: a cross-sectional study. BJOG: An International Journal of Obstetrics & Gynaecology. 2013;120(8):940–7.
Kakyo TA, et al. Factors associated with depressive symptoms among postpartum mothers in a rural district in Uganda. Midwifery. 2012;28(3):374–9.
Atuhaire C, et al. Prevalence of postpartum depression and associated factors among women in Mbarara and Rwampara districts of south-western Uganda. BMC Pregnancy Childbirth. 2021;21(1):1–12.
Yeboa NK, et al. Prevalence and associated factor of postpartum depression among mothers living with HIV at an urban postnatal clinic in Uganda. Women’s Health. 2023;19:17455057231158471.
Pallitto CC, O’Campo P. The relationship between intimate partner violence and unintended pregnancy: analysis of a national sample from Colombia International family planning perspectives, 2004: p. 165–173.
Merrill KG, et al. The association between violence victimization and subsequent unplanned pregnancy among adolescent girls in Uganda: do primary schools make a difference? PLOS Global Public Health. 2023;3(7):e0001141.
Kaye D, Mirembe F, Bantebya G. Risk factors, nature and severity of domestic violence among women attending antenatal clinic in Mulago Hospital, Kampala, Uganda. Cent Afr J Med. 2002;48(5–6):64–8.
Napyo A et al. Prevalence and predictors for unintended pregnancy among HIV-infected pregnant women in Lira, Northern Uganda: a cross-sectional study. Sci Rep, 2020. 10.
Senderowicz L, Sawadogo N, Langer A. Barriers to contraceptive autonomy in Burkina Faso. Contraception. 2018;98(4):353.
Tusiime S, et al. Prevalence of sexual coercion and its association with unwanted pregnancies among young pregnant females in Kampala, Uganda: a facility based cross-sectional study. BMC Womens Health. 2015;15(1):1–12.
Anguzu R, et al. Knowledge and attitudes towards use of long acting reversible contraceptives among women of reproductive age in Lubaga division, Kampala district, Uganda. BMC Res Notes. 2014;7(1):1–9.
Moore AM, Frohwirth L, Miller E. Male reproductive control of women who have experienced intimate partner violence in the United States. Volume 70. Social science & medicine; 2010. pp. 1737–44. 11.
Sarnak DO, et al. The role of partner influence in contraceptive adoption, discontinuation, and switching in a nationally representative cohort of ugandan women. PLoS ONE. 2021;16(1):e0238662.
Senderowicz L. I was obligated to accept: a qualitative exploration of contraceptive coercion. Soc Sci Med. 2019;239:112531.
MoGLSD. The National Policy on elimination of gender-based violence in Uganda. Ministry of Gender, Labour and Social Development; 2019.
Atuhaire R, et al. Interrelationships between early antenatal care, health facility delivery and early postnatal care among women in Uganda: a structural equation analysis. Global Health Action. 2020;13(1):1830463.
Turyasiima M, et al. Determinants of first antenatal care visit by pregnant women at community based education, research and service sites in Northern Uganda. East Afr Med J. 2014;91(9):317–22.
Uldbjerg CS, et al. Perceived barriers to utilization of antenatal care services in northern Uganda: a qualitative study. Sex Reproductive Healthc. 2020;23:100464.
Kawungezi PC, et al. Attendance and utilization of antenatal care (ANC) services: multi-center study in upcountry areas of Uganda. Open J Prev Med. 2015;5(3):132.
Rogers M. Antenatal Care Services among Pregnant Women in Kampala International University Teaching Hospital Bushenyi-Ishaka Municipality 2023.
Tegegne TK, et al. Antenatal care use in Ethiopia: a spatial and multilevel analysis. BMC Pregnancy Childbirth. 2019;19(1):1–16.
Asundep NN, et al. Determinants of access to antenatal care and birth outcomes in Kumasi, Ghana. J Epidemiol Global Health. 2013;3(4):279–88.
Nathan LM, et al. Decentralizing maternity services to increase skilled attendance at birth and antenatal care utilization in rural Rwanda: a prospective cohort study. Matern Child Health J. 2015;19(9):1949–55.
Kofinti RE, Asmah EE, Ameyaw EK. Comparative study of the effect of National Health Insurance Scheme on use of delivery and antenatal care services between rural and urban women in Ghana. Health Econ Rev. 2022;12(1):13.
Angko W, Wulifan JK, Sumankuuro J. Health insurance coverage, socioeconomic status of women, and antenatal care utilization in Ghana. J Popul Social Stud [JPSS]. 2023;31:62–79.
Dusingizimana T, et al. Predictors for achieving adequate antenatal care visits during pregnancy: a cross-sectional study in rural Northwest Rwanda. BMC Pregnancy Childbirth. 2023;23(1):1–9.
Sserwanja Q, Gatasi G, Musaba MW. Evaluating continuum of maternal and newborn healthcare in Rwanda: evidence from the 2019–2020 Rwanda demographic health survey. BMC Pregnancy Childbirth. 2022;22(1):781.
Medard T, Yawe BL, Oryema JB. Effect of health insurance on utilisation of maternal health care services in Uganda. Afr J Health Sci. 2022;35(5):586–98.
Lindberg C et al. The extent of Universal Health Coverage for maternal Health Services in Eastern Uganda: A Cross Sectional Study. Matern Child Health J, 2022: p. 1–10.
Acknowledgements
None.
Funding
None.
Author information
Authors and Affiliations
Contributions
RA conceptualized this study and drafted the initial manuscript. RA, RJW, JDG, and LDC contributed to the study design. RJW, KMMB, HB, JDG and LDC supervised the implementation of the study. RA, RJW, KMMB, YZ, HB, JDG, and LDC contributed to data analysis and interpretation. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The informed consent was obtained from all women who participated in the 2016 UDHS as described elsewhere [54]. This study’s ethical approval was received from the Medical College of Wisconsin (MCW) Ethical Review Committee (Ref No: PRO00036397), The AIDS Support Organization (TASO) Institutional Review Board (Ref: TASOREC/083/19-UG-REC-009), and Uganda National Council of Science and Technology (Ref: SS 5243) provided the clearance.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Anguzu, R., Walker, R.J., Babikako, H.M. et al. Intimate partner violence and antenatal care utilization predictors in Uganda: an analysis applying Andersen’s behavioral model of healthcare utilization. BMC Public Health 23, 2276 (2023). https://doi.org/10.1186/s12889-023-16827-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12889-023-16827-w