
Abstract
Background
Minerals have crucial biological functions in metabolism and are primarily obtained through diet. As a result, various dietary patterns can impact blood mineral levels. The aim of this study was to investigate the correlation between dietary patterns and the concentration of calcium, magnesium, iron, zinc, and copper in the bloodstream.
Methods
Three hundred eighty healthy children (53.7% male) were recruited in a region of Hunan Province in September 2019. We gathered basic information and measured physical proportions, along with completing a food frequency questionnaire (FFQ). Using principal component analysis (PCA), we determined dietary patterns. To analyze mineral levels in the blood, we used flame atomic absorption spectrometry (FAAS). We utilized linear regression models to investigate if certain dietary patterns are related to mineral concentration.
Results
Three dietary patterns were identified: ‘Vegetables/Nuts,’ ‘Snacks/Beverages,’ and ‘Cereal/Beans.’ Children from high-income families (annual average income > 50,000 yuan) prefer the ‘Vegetables/Nuts’ dietary pattern (P = 0.004). In comparison, those from low-income families (annual average income < 20,000 yuan) prefer the ‘Snacks/Beverages’ dietary pattern (P = 0.03). Following adjustment for age, gender, guardian’s identity, education level, and annual household income. We found that an increase in the ‘Vegetables/Nuts’ pattern score (β = 0.153, CI: 0.053 ~ 0.253; P = 0.003) and ‘Snacks/Beverages’ pattern score (β = 0.103, CI: 0.002 ~ 0.204; P = 0.033) were significantly associated blood copper concentration.
Conclusions
Household income was found to be associated with dietary behavior. Furthermore, higher blood copper concentration was significantly correlated with the ‘Vegetables/Nuts’ dietary pattern and ‘Snacks/Beverages’ dietary pattern, but the correlation is extremely low.
Similar content being viewed by others

Background
Essential elements like calcium (Ca), magnesium (Mg), iron (Fe), zinc (Zn), and copper (Cu) play crucial roles in the regulation and maintenance of various physiological functions in the human body despite their low requirements of them [1]. They are critical components of metalloenzymes and are involved in crucial biological processes, such as oxygen transport, free radical scavenging, and hormonal activity [2]. Ca is predominantly accumulated in bone tissue. Getting enough calcium as a child and teenager is crucial for strong bones [3]. Mg is abundant in human cells, plays an important role in 300 + metabolic reactions, and has been shown to be associated with Attention Deficit Hyperactivity Disorder (ADHD) [4,5,6,7]. Fe is a bivalent cation crucial for numerous physiological and cellular processes, and iron deficiency causes diverse health consequences [8]. Zn is the second most abundant metal in humans and is distributed unequally throughout different organs and tissues. In infants and early childhood, zinc supplementation can increase specific growth outcomes [9]. Cu is a crucial cofactor for more than twenty proteins [10]. Research shows that the level of copper in the serum is linked to obesity and various chronic illnesses in children [11, 12].
Dietary pattern analysis is a promising approach to understanding the complex relationship between diet and health [13]. An analysis based on nutrients alone may be confounded by the type of dietary pattern a person follows. They use a dietary pattern approach to overcome these limitations by considering how foods are eaten in combination. Poor diet in early life is a major modifiable risk factor with many health outcomes. Numerous studies have focused on the association between health outcomes and diet [14,15,16]. Research has revealed connections between the dietary patterns of children and adolescents with obesity [17,18,19]. Additionally, some studies have also found links between dietary patterns and cardiometabolic risk and depression [20, 21]. Studies in China examined the consumption of sugar-sweetened beverages and dairy by children and adolescents [22,23,24], but it did not specifically focus on dietary patterns. Recent studies conducted in China have revealed a strong correlation between a child's mineral status and lipid metabolism, and mineral status also has a significant impact on the symptoms of autism. [25, 26]. Meanwhile, Islam MR et al. proposed that alterations of serum mineral was associated with major depressive disorder [27]. Based on this information, we are considering the possibility that various dietary habits may indirectly impact the onset of specific illnesses by affecting the levels of essential minerals in the body.
The background level of minerals in children’s bodies is of great significance for monitoring the environment and evaluating children’s nutritional status [28,29,30,31]. While studies have shown a connection between mineral intake and various diseases [32,33,34,35], research on the correlation between dietary patterns and mineral levels is still lacking. Thus, this study aimed to investigate the correlation between the levels of calcium, magnesium, iron, zinc, and copper with different dietary patterns.
Methods
Study population
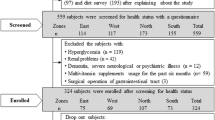
Participants were children enrolled in a cross-sectional study of blood minerals and eating behavior; this study is the first analysis of the recruitment visit, which occurred in Hunan Province, China, in September 2019. This study was approved by the Ethics Committee of Hunan Provincial Center for Disease Control and Prevention. Informed consent for the use of these children’s detection results and personal information in this study was obtained from their parents/legal guardians. Inclusion criteria were that the child was enrolled in local primary schools (either in the first or second year), aged 5 – 7 years, mentally competent, and had no serious medical problems affecting growth or appetite. All questionnaires were interviewer-administered.
Of the full sample of 392 children, 12 were excluded either due to missing or implausible dietary data.
Dietary assessment and identification of dietary pattern
A validated 61-item food frequency questionnaire (FFQ) developed was employed to assess dietary intake. A common unit or portion size for each food was specified, and the participants' parents were asked to recall how often, on average, the child had consumed that item during the previous year. The selected frequency category for each food item was converted to a daily intake.
All data in the questionnaire were input using the software EpiData (version 3.1). According to the nutrient profile, the 61 items of the FFQ were allocated to 13 predefined food groups to identify eating patterns through Principal Component Analysis (PCA) (Table 2). The applicability of the PCA method was evaluated by the Kaiser–Meyer–Olkin coefficient (KMO) and Bartlett’s test of sphericity (BTS). In this study, the KMO value was 0.738, and the BTS test P-value was P < 0.0001, indicating the adequacy of the data for the factor analysis. The factors were rotated by an orthogonal transformation (varimax rotation function in SPSS software). Three dietary patterns were identified using multiple criteria: the diagram of eigenvalues, the scree plot, the interpretability of the factors, and the percentage of variance explained by the factors. The factor score for each pattern was calculated by summing intakes of all food groups weighted by their factor loadings. The food groups with the highest component loadings enabled interpretation of the pattern; groups with component loadings ≥|0.3| are shown in Table 2. To determine how closely each child’s diet aligned with the dietary pattern, scores were calculated by multiplying the component loadings of each food group by the child’s frequency of intake in that food group and the summing. Then scores were categorized into tertiles to differentiate children with lower scores (i.e., tertile 1, lower intake) from higher scores (i.e., tertile 3, higher intake). Finally, each score was converted to Z-scores with a mean of 0 and standard deviation of 1 to facilitate comparisons between 3 dietary patterns.
Elemental analysis
After obtaining consent to participate in the study from each patient, 3 mL of blood was taken from the child to determine the concentration of the following minerals in blood: calcium, magnesium, iron, zinc, and copper. Before element detection, all the blood samples were stored at 0—4℃ for no more than 48 h.
Whole blood concentrations of calcium, iron, copper, magnesium, and zinc were determined by flame atomic absorption spectrometry (FAAS) instrument. Standard curves of these elements were conducted by serial dilution of the stock standard solutions before analyzing the metal on the instrument. Sample digestion was prepared by simply mixing 0.5 mL of blood sample and 4.5 mL of 0.5% Triton X-100 solution containing 1% HNO3 in a digestive tube. Then 0.5 mL sample dilution was added to 2 mL of 0.5% Triton X-100 dilution containing 1% HNO3 for mixing. They were detected immediately on the instrument after homogenizing.
Covariates
Parents or other guardians provided relevant sociodemographic information, including the child’s age, gender, and the identity relationship between the actual guardian and the participants. The guardian relationship is divided into parents and others (others include grandparents, uncles/ aunts, brothers/ sisters). Meanwhile, guardians are required to provide their highest level of education attained and household income from all sources. Guardians' education level was classified into three categories: incomplete high school education, high school diploma, and completion of post-high school education. Similarly, participants' annual per capita household income was divided into three categories: less than 20,000 yuan, 20,000–50000 yuan, and more than 50,000 yuan. We used these categories to gain a better understanding of the group's demographics and to identify any potential correlations with other variables.
Statistical analysis
All analyses were conducted using SPSS software (version 19.0 for Windows). The levels of calcium, magnesium, iron, zinc, and copper elements were analyzed using quantitative variables and assessed for normal distribution using the Kolmogorov–Smirnov test (K-S test). When representing normal distribution, we use mean ± standard deviation, while non-normal distribution is represented by median (IQR). Household income per capita was calculated as the total reported household income divided by the number of family members.
In bivariate analysis, the relationships between dietary patterns and potential confounders were initially explored by comparing the distributions of mean ± standard deviation (SD) of the potential confounders between the lowest and highest tertiles of dietary pattern categories (split at the tertile of dietary pattern scores). They were using dietary pattern scores as the continuous independent variable and minerals level as the continuous dependent variable, linear regression models were used to evaluate the primary study questions about diet and blood minerals. In multivariable models, the child’s gender, guardian’s educational level and income, and kinship to the child were added to each model. These variables were selected as confounders based on the results of the bivariate confounder analysis and prior research [36].
Results
General characteristics of study population
The sample comprised 176 (46.3%) girls and 204 (53.7%) boys. The mean age of the selection was 6.17 years (SD 0.68 years). Other descriptive statistics are shown in Table 1.
Dietary patterns
Using PCA and varimax rotation, three distinct dietary patterns were identified for the overall population, which explained 33.220% of the total variance in food intake. The factor loadings of the food groups contributing to the three dietary patterns are reported in Table 2 (groups with component loadings ≥|0.3| are bolded). Dietary pattern one, named ‘Vegetables/Nuts,’ explained 15.094% of the variance in food intake. High factor loadings on vegetables, homonemeae, nuts, aquatic foods, and fruits characterized this pattern. Pattern two, labeled ‘Snacks/Beverages,’ explained 9.725% of the variance in food intake and was characterized by high loadings on beverages, snacks, poultry, red meat, and nuts. Pattern three explained 8.401% of the variance in food intake and was named ‘Cereals/Beans.’ This pattern had high factor loadings on cereals, beans, fruits, and milk.
Concentrations of calcium, magnesium, iron, zinc, and copper in whole blood
The measurements of blood minerals for selected participants are summarized in Table 3. Based on the results of the K-W test, it appears that the concentration of the five minerals did not follow a normal distribution (P < 0.05). The median (IQR) for calcium, magnesium, iron, zinc, and copper were 69.63 (10.13), 41.09 (7.71), 434.70 (114.53), 4.55 (1.13), and 0.89 (0.19) mg/ L, respectively. The range of five minerals is consistent with previous studies [37, 38].
Correlational analyses
Guardian’s income was associated with all three dietary patterns, such that children with higher scores on the Healthy pattern and lower scores on the Unhealthy pattern were more likely to have parents/legal guardians who have a higher income (Table 4) compared to children with lower scores on the corresponding pattern.
In regression analysis (Table 5), blood copper concentration was related to a 0.14 higher Healthy dietary pattern SD after adjustment for potential confounders (95% Confidence Interval (CI) 0.038 to 0.242, P = 0.004), and copper concentration was also associated with a 0.103 SD higher Unhealthy dietary pattern score (95% CI 0.002 to 0.204, P = 0.045), and neither dietary pattern resulted in a copper concentration exceeding/below the normal range. Concentrations of calcium, iron, magnesium, and zinc were not associated with dietary pattern scores.
Discussion
This is the first study to explore the association between dietary patterns and blood minerals level. In the past 20 years, the nutritional status of children in China has greatly improved, but there are still unhealthy diets and insufficient intake of micronutrients [39]. Dietary patterns directly affect children’s nutritional and health status. Therefore, studying the current situation of dietary patterns and evaluating the association between dietary patterns and micronutrients will provide a practical solution to improve the nutritional intake of children.
This study aimed to identify dietary patterns within school-age children and to explore the correlation with blood minerals (calcium, iron, copper, magnesium, and zinc) concentration. In this sample of school-age children, three dietary patterns were identified – ‘Vegetables/Nuts’ dietary pattern, ‘Snacks/Beverages’ dietary pattern, ‘Cereals/Beans’ dietary pattern. One of the primary findings was that household income was associated with differences in pattern behavior. Children with higher family incomes tend to the ‘Healthy-conscious’ dietary pattern, and middle-income families tend to prefer the traditional ‘Cereals/Beans’ dietary pattern.
Income and food cost are the two most important determinants of dietary convergence in developing nations [40]. While globalization presents a chance for a greater intake of healthy and diverse foods in economies in transition, it also permits an increase in the consumption of inexpensive, energy-dense foods [41]. Several studies described the positive association between household income and ‘Healthy’ dietary patterns [42, 43]. And cross-sectional studies found that the ‘Unhealthy’ dietary pattern was inversely associated with income [44, 45]. The inverse relationship could be due to the high cost of healthy diets. [46,47,48]. A study based on the China Health and Nutrition Survey revealed that an increase in family income boosts protein and fat intake but has a negative correlation with carbohydrate consumption [49]. And individuals with higher salaries tend to consume a wider variety of foods. As expected, a significant positive correlation exists between income and dietary knowledge, as higher-income persons are more health-conscious and have greater access to health information [50,51,52].
Another finding was that blood copper concentration was positively correlated with ‘Healthy-conscious’ dietary pattern scores and ‘Snacks/Beverages’ dietary pattern scores after accounting for confounders, although the regression coefficient is low (P < 0.05, β < 0.3). Copper metabolism is regulated by physiologic demand, but the mechanisms involved have not been elucidated. And copper deficiency does not occur frequently, and it most often occurs in patients with Menkes disease (MD), a genetic disorder of impaired copper homeostasis. Excess copper has also been reported in humans, most often being associated with another rare genetic disorder, Wilson’s disease (WD).
It is well known that none of the five minerals can be synthesized in the human body and can only be consumed through foods. The best dietary sources of copper are shellfish, seeds, nuts, organ meats, and bran cereal. High-loading nuts and homonemeae in the ‘Healthy-conscious’ pattern are rich in copper (> 2.4 μg/g). In addition, about 55%—75% of dietary copper is absorbed, which is considerably higher than other minerals [53]. Therefore, we speculate that elevated blood copper levels are a short-term effect caused by high copper dietary intake. Moreover, mRNA levels for many proteins involved in copper homeostasis in mammals (e.g., CTR1, ATP7A, and ATP7B) do not change in response to dietary copper intake levels, demonstrating a lack of control at the level of gene transcription or transcript stability. Regulation of copper intake and efflux may instead be controlled at a posttranscriptional level, predominantly by protein trafficking, as exemplified by the copper-transporting ATPases moving from the TGN to either the enterocyte BLM (APT7A) or the canalicular membrane of hepatocytes (ATP7B) when copper is in excess [54]. Copper metabolism is best known to be influenced by iron. It has been suggested that iron can interfere with copper utilization, and high iron consumption can interfere with copper absorption in infants and adults [55]. Plant components in vegetables and tea (e.g., polyphenols, phytates) and soft drinks inhibit iron absorption, which may also contribute to an indirect increase in blood copper levels [56].
Therefore, we propose that dietary patterns cannot reflect children’s long-term mineral needs. Firstly, the proportion of mineral elements in the blood is extremely low, making the blood concentration highly susceptible to a short-term diet. Meanwhile, the interaction of mineral elements also makes their concentration unpredictable. In August 2021, the National Health Commission of China issued a notice that trace elements testing of children shall not be carried out as a medical examination item unless the diagnosis and treatment needs. The blood concentration of trace elements in healthy individuals remains relatively stable because they are strictly regulated [57,58,59,60,61,62,63,64]. Evaluating the trace elements status in healthy children through blood concentration still needs further study.
There are several limitations to our study. Firstly, the research may be limited in its ability to generalize conclusions due to a small sample size and narrow age range among participants. Secondly, the research was carried out only in one specific city, which may restrict the generalization of the results to other areas. Thirdly, the study participants were healthy individuals, but low blood levels due to element deficiency are usually accompanied by obvious clinical symptoms. Finally, we cannot exclude the possibility of residual confounding in the analysis due to unmeasured or imprecisely measured factors. It is possible, for example, that dietary intake is only one component of an overall lifestyle that affect the content of blood minerals. Such passive smoking [65, 66] and high-intensity exercise [67, 68] can lead to significant changes in blood minerals.
Mineral homeostasis is a complex and highly regulated process involving acquisition, utilization, storage, and efflux. Although some limitations may apply, blood mineral concentration is still used as the standard for evaluating trace elements status in patients. To comprehensively evaluate minerals status, both laboratory tests and the clinical assessment of trace elements deficit symptoms might be required.
Conclusions
This study demonstrated that dietary patterns had no effect on blood mineral levels and found an association between household income and dietary patterns. Adequate minerals are essential for children’s growth and development. Therefore, the food intake pattern of children should receive greater attention from public health policies, and the complex relationship between dietary patterns and mineral still needs further study.
Availability of data and materials
All data generated or analyzed during this study are included in this published article.
References
Stathopoulou MG, Kanoni S, Papanikolaou G, Antonopoulou S, Nomikos T, Dedoussis G. Mineral intake. Prog Mol Biol Transl Sci. 2012;108:201–36.
Ye J, Du C, Wang L, Li Z, Huang S, Wang H, et al. Relationship of blood levels of Pb with Cu, Zn, Ca, Mg, Fe, and Hb in children aged 0 approximately 6 years from Wuhan. China Biol Trace Elem Res. 2015;164(1):18–24.
Pettifor JM. Nutritional rickets: deficiency of vitamin D, calcium, or both? Am J Clin Nutr. 2004;80(6 Suppl):1725S-S1729.
Glasdam SM, Glasdam S, Peters GH. The Importance of Magnesium in the Human Body: A Systematic Literature Review. Adv Clin Chem. 2016;73:169–93.
Ford ES, Mokdad AH. Dietary magnesium intake in a national sample of US adults. J Nutr. 2003;133(9):2879–82.
Wang LJ, Yang CY, Chou WJ, Lee MJ, Chou MC, Kuo HC, et al. Gut microbiota and dietary patterns in children with attention-deficit/hyperactivity disorder. Eur Child Adolesc Psychiatry. 2020;29(3):287–97.
Huang YH, Zeng BY, Li DJ, Cheng YS, Chen TY, Liang HY, et al. Significantly lower serum and hair magnesium levels in children with attention deficit hyperactivity disorder than controls: A systematic review and meta-analysis. Prog Neuropsychopharmacol Biol Psychiatry. 2019;90:134–41.
Pasricha SR, Tye-Din J, Muckenthaler MU, Swinkels DW. Iron deficiency. Lancet. 2021;397(10270):233–48.
Liu E, Pimpin L, Shulkin M, Kranz S, Duggan CP, Mozaffarian D, et al. Effect of Zinc Supplementation on Growth Outcomes in Children under 5 Years of Age. Nutrients. 2018;10(3):377.
Kirsipuu T, Zadoroznaja A, Smirnova J, Friedemann M, Plitz T, Tougu V, et al. Copper(II)-binding equilibria in human blood. Sci Rep. 2020;10(1):5686.
Gu K, Li X, Xiang W, Jiang X. The Relationship Between Serum Copper and Overweight/Obesity: a Meta-analysis. Biol Trace Elem Res. 2020;194(2):336–47.
Escobedo-Monge MF, Barrado E, Parodi-Roman J, Escobedo-Monge MA, Torres-Hinojal MC, Marugan-Miguelsanz JM. Copper and Copper/Zn Ratio in a Series of Children with Chronic Diseases: A Cross-Sectional Study. Nutrients. 2021;13(10):3578.
Zhao J, Li Z, Gao Q, Zhao H, Chen S, Huang L, et al. A review of statistical methods for dietary pattern analysis. Nutr J. 2021;20(1):37.
Grosso G, Bella F, Godos J, Sciacca S, Del Rio D, Ray S, et al. Possible role of diet in cancer: systematic review and multiple meta-analyses of dietary patterns, lifestyle factors, and cancer risk. Nutr Rev. 2017;75(6):405–19.
Owen L, Corfe B. The role of diet and nutrition on mental health and wellbeing. Proc Nutr Soc. 2017;76(4):425–6.
Requena T, Martinez-Cuesta MC, Pelaez C. Diet and microbiota linked in health and disease. Food Funct. 2018;9(2):688–704.
Liu D, Zhao LY, Yu DM, Ju LH, Zhang J, Wang JZ, et al. Dietary Patterns and Association with Obesity of Children Aged 6(-)17 Years in Medium and Small Cities in China: Findings from the CNHS 2010(-)2012. Nutrients. 2018;11(1):3.
Zhen S, Ma Y, Zhao Z, Yang X, Wen D. Dietary pattern is associated with obesity in Chinese children and adolescents: data from China Health and Nutrition Survey (CHNS). Nutr J. 2018;17(1):68.
Min K, Wang J, Liao W, Astell-Burt T, Feng X, Cai S, et al. Dietary patterns and their associations with overweight/obesity among preschool children in Dongcheng District of Beijing: a cross-sectional study. BMC Public Health. 2021;21(1):223.
Rocha NP, Milagres LC, Longo GZ, Ribeiro AQ, Novaes JF. Association between dietary pattern and cardiometabolic risk in children and adolescents: a systematic review. Jornal de pediatria. 2017;93(3):214–22.
Lassale C, Batty GD, Baghdadli A, Jacka F, Sánchez-Villegas A, Kivimäki M, et al. Healthy dietary indices and risk of depressive outcomes: a systematic review and meta-analysis of observational studies. Mol Psychiatry. 2019;24(7):965–86.
Zhu Z, Cui X, Wei X, Zang J, Feng J, Wang Z, et al. Dietary Sodium Intake Is Positively Associated with Sugar-Sweetened Beverage Consumption in Chinese Children and Adolescents. Nutrients. 2021;13(11):3949.
Duan Y, Pang X, Yang Z, Wang J, Jiang S, Bi Y, et al. Association between Dairy Intake and Linear Growth in Chinese Pre-School Children. Nutrients. 2020;12(9):2576.
Gui ZH, Zhu YN, Cai L, Sun FH, Ma YH, Jing J, et al. Sugar-Sweetened Beverage Consumption and Risks of Obesity and Hypertension in Chinese Children and Adolescents: A National Cross-Sectional Analysis. Nutrients. 2017;9(12):1302.
Guo M, Li L, Zhang Q, Chen L, Dai Y, Liu L, et al. Vitamin and mineral status of children with autism spectrum disorder in Hainan Province of China: associations with symptoms. Nutr Neurosci. 2020;23(10):803–10.
Huang Z, Liu X, Li Z, Cui L, Liu C, Wang W, et al. The Associations of Erythrocyte Fatty Acids with Whole Blood Mineral Elements in Children. Nutrients. 2022;14(3):618.
Islam MR, Islam MR, Shalahuddin Qusar MMA, Islam MS, Kabir MH, Mustafizur Rahman GKM, et al. Alterations of serum macro-minerals and trace elements are associated with major depressive disorder: a case-control study. BMC Psychiatry. 2018;18(1):94.
Li X, Wang C, Wang Y, Zhao X, Li N. Determination of 11 minerals in children using inductively coupled plasma mass spectrometry. BMC Pediatr. 2021;21(1):483.
Nisse C, Tagne-Fotso R, Howsam M, Members of Health Examination Centres of the Nord - Pas-de-Calais region n, Richeval C, Labat L, et al. Blood and urinary levels of metals and metalloids in the general adult population of Northern France: The IMEPOGE study, 2008–2010. Int J Hyg Environ Health. 2017;220(2 Pt B):341–63.
Needham LL, Calafat AM, Barr DB. Uses and issues of biomonitoring. Int J Hyg Environ Health. 2007;210(3–4):229–38.
Baeyens W, Vrijens J, Gao Y, Croes K, Schoeters G, Den Hond E, et al. Trace metals in blood and urine of newborn/mother pairs, adolescents and adults of the Flemish population (2007–2011). Int J Hyg Environ Health. 2014;217(8):878–90.
Swaminath S, Um CY, Prizment AE, Lazovich D, Bostick RM. Combined Mineral Intakes and Risk of Colorectal Cancer in Postmenopausal Women. Cancer Epidemiol Biomarkers Prev. 2019;28(2):392–9.
Wang Z, Wang W, Yang A, Zhao W, Yang J, Wang Z, et al. Lower dietary mineral intake is significantly associated with cervical cancer risk in a population-based cross-sectional study. J Cancer. 2021;12(1):111–23.
Agron E, Mares J, Clemons TE, Swaroop A, Chew EY, Keenan TDL, et al. Dietary Nutrient Intake and Progression to Late Age-Related Macular Degeneration in the Age-Related Eye Disease Studies 1 and 2. Ophthalmology. 2021;128(3):425–42.
Mohammadifard N, Humphries KH, Gotay C, Mena-Sanchez G, Salas-Salvado J, Esmaillzadeh A, et al. Trace minerals intake: Risks and benefits for cardiovascular health. Crit Rev Food Sci Nutr. 2019;59(8):1334–46.
Patrick H, Nicklas TA. A review of family and social determinants of children’s eating patterns and diet quality. J Am Coll Nutr. 2005;24(2):83–92.
Luan F, Liu B, Sun S, Chen Y, Xu Y, Jiang X, et al. Analysis of Eight Nutrient Elements in Whole Blood of Children and Adolescents Using Inductively Coupled Plasma-Mass Spectrometry. Biol Trace Elem Res. 2021;200(7):3078–87.
Zhang H, Man Q, Song P, Li S, Liu X, Wang L, et al. Association of whole blood copper, magnesium and zinc levels with metabolic syndrome components in 6–12-year-old rural Chinese children: 2010–2012 China National Nutrition and Health Survey. Nutr Metab (Lond). 2021;18(1):67.
Qian Z, Xiaoqi H. Nutrition and health status of Children aged 6–17 in China. Report on nutrition and health status of Chinese residents 2010–2013. Beijing: REN MIN WEI SHENG CHU BAN SHE; 2018.
Kennedy G, Nantel G, Shetty P. Globalization of food systems in developing countries: impact on food security and nutrition. FAO Food Nutr Pap. 2004;83:1–300.
Mayen AL, Marques-Vidal P, Paccaud F, Bovet P, Stringhini S. Socioeconomic determinants of dietary patterns in low- and middle-income countries: a systematic review. Am J Clin Nutr. 2014;100(6):1520–31.
Eng CW, Lim SC, Ngongo C, Sham ZH, Kataria I, Chandran A, et al. Dietary practices, food purchasing, and perceptions about healthy food availability and affordability: a cross-sectional study of low-income Malaysian adults. BMC Public Health. 2022;22(1):192.
Rehm CD, Penalvo JL, Afshin A, Mozaffarian D. Dietary Intake Among US Adults, 1999–2012. JAMA. 2016;315(23):2542–53.
Manyanga T, Tremblay MS, Chaput JP, Katzmarzyk PT, Fogelholm M, Hu G, et al. Socioeconomic status and dietary patterns in children from around the world: different associations by levels of country human development? BMC Public Health. 2017;17(1):457.
Wu JC. Parental work characteristics and diet quality among pre-school children in dual-parent households: results from a population-based cohort in Taiwan. Public Health Nutr. 2018;21(6):1147–55.
Darmon N, Drewnowski A. Does social class predict diet quality? Am J Clin Nutr. 2008;87(5):1107–17.
Aggarwal A, Monsivais P, Cook AJ, Drewnowski A. Does diet cost mediate the relation between socioeconomic position and diet quality? Eur J Clin Nutr. 2011;65(9):1059–66.
Lopez CN, Martinez-Gonzalez MA, Sanchez-Villegas A, Alonso A, Pimenta AM, Bes-Rastrollo M. Costs of Mediterranean and western dietary patterns in a Spanish cohort and their relationship with prospective weight change. J Epidemiol Community Health. 2009;63(11):920–7.
Ren Y, Li H, Wang X. Family income and nutrition-related health: Evidence from food consumption in China. Soc Sci Med. 2019;232:58–76.
Clément M. The income-body-size gradient among Chinese urban adults: A semiparametric analysis. China Econ Rev. 2017;44:253–70.
Kennedy G, Ballard T, Dop M. Guidelines for Measuring Household and Individual Dietary Diversity. Rome: FAO; 2011.
Sekabira H, Qaim M. Can mobile phones improve gender equality and nutrition? Panel data evidence from farm households in Uganda. Food Policy. 2017;73:95–103.
Collins JF, Klevay LM. Copper. Adv Nutr. 2011;2(6):520–2.
Doguer C, Ha JH, Collins JF. Intersection of iron and copper metabolism in the mammalian intestine and liver. Compr Physiol. 2018;8(4):1433–61.
Klevay LM. IHD from copper deficiency: a unified theory. Nutr Res Rev. 2016;29(2):172–9.
Zijp IM, Korver O, Tijburg LB. Effect of tea and other dietary factors on iron absorption. Crit Rev Food Sci Nutr. 2000;40(5):371–98.
Maares M, Haase H. A Guide to Human Zinc Absorption: General Overview and Recent Advances of In Vitro Intestinal Models. Nutrients. 2020;12(3):762.
Witkowski M, Hubert J, Mazur A. Methods of assessment of magnesium status in humans: a systematic review. Magnes Res. 2011;24(4):163–80.
Ismail Y, Ismail AA, Ismail AA. The underestimated problem of using serum magnesium measurements to exclude magnesium deficiency in adults; a health warning is needed for “normal” results. Clin Chem Lab Med. 2010;48(3):323–7.
Song Y, Ridker PM, Manson JE, Cook NR, Buring JE, Liu S. Magnesium intake, C-reactive protein, and the prevalence of metabolic syndrome in middle-aged and older U.S. women. Diabetes Care. 2005;28(6):1438–44.
Ross AC, Tarylor CL, Yaktine AL. Institute of Medicine (US) Committee to Review Dietary Reference Intakes for Vitamin D and Calcium. Dietary Reference Intake for Calcium and Vitamin D. Washington: National Academies Press (US); 2011.
Ross AC, Caballero BH, Cousins RJ, Tucker KL, Ziegler TR, Modern Nutrition in Health and Disease: Eleventh Edition. Maryland USA: Wolters Kluwer Health Adis (ESP); 2012.
Gibson RS. Priciples of Nutritional Assessment. New York. 2nd ed. USA: Oxford University Press; 2005.
Ross AC, Caballero B, Cousins RJ, Tucker KL, Modern nutrition in health and disease. Burlington USA: Jones & Bartlett Learning; 2020.
Protano C, Astolfi ML, Canepari S, Vitali M. Urinary levels of trace elements among primary school-aged children from Italy: The contribution of smoking habits of family members. Sci Total Environ. 2016;557–558:378–85.
Serdar MA, Akin BS, Razi C, Akin O, Tokgoz S, Kenar L, et al. The correlation between smoking status of family members and concentrations of toxic trace elements in the hair of children. Biol Trace Elem Res. 2012;148(1):11–7.
Chu A, Holdaway C, Varma T, Petocz P, Samman S. Lower Serum Zinc Concentration Despite Higher Dietary Zinc Intake in Athletes: A Systematic Review and Meta-analysis. Sports Med. 2018;48(2):327–36.
Heffernan SM, Horner K, De Vito G, Conway GE. The Role of Mineral and Trace Element Supplementation in Exercise and Athletic Performance: A Systematic Review. Nutrients. 2019;11(3):696.
Acknowledgements
The authors thank all the participants, researchers, and collaborators for their contribution to physical examinations, biochemical and nutritional evaluation.
Funding
No funding.
Author information
Authors and Affiliations
Contributions
X.C.Y. made an interpretation of data and drafted the work; Z.M.L. and Y.N.W. collected all the samples; Y.J.D., W.F.W., and M.C. conducted the experiments and analyzed the data; Y.M.H. designed and supervised the work. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was conducted according to the guidelines laid down in the Declaration of Helsinki, and all procedures involving research study participants were approved by the [Medical Ethics Committee of Hunan Provincial Center for Disease Control and Prevention]. Written informed consent was obtained from all subjects and their legal guardian(s).
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher'’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Yin, Xc., Wang, Wf., Li, Zm. et al. The relationship between dietary patterns and blood mineral concentration among children in Hunan Province of China. BMC Public Health 23, 1518 (2023). https://doi.org/10.1186/s12889-023-16429-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12889-023-16429-6