
Abstract
Background
Physical activity (PA), sedentary behaviour (SB) and diet play an important role in the physical and mental health of young people. Understanding how these behaviours cluster, and the impact of clusters on health is important for the development of public health interventions. This review examines the prevalence of clusters of PA, sedentary time, and dietary behaviours, and how clusters relate to physical and mental health indicators among children, adolescents and young adults.
Methods
Electronic (PubMed, Web of Science and Scopus) and manual searches were conducted for articles that were (i) observational studies including children, adolescents and/or young adults aged 5–24 years, (ii) examined the 'patterning', ‘clustering’, or ‘co-existence’ of each of PA, dietary behaviour and SB, and (iii) published in English up to and including July 2022. In addition to information on clustering, data on physical and mental health outcomes were extracted where reported. Included studies were assessed using the Cochrane risk of bias for observational studies. A narrative synthesis was conducted due to high heterogeneity. This review was registered with PROSPERO (CRD42021230976).
Results
Forty-nine cross-sectional studies and four prospective cohort studies from eighteen countries reporting data from 778,415 individual participants were included. A broad range of clusters (n = 172) were found (healthy, unhealthy, and mixed). Mixed clusters were common (n = 98), and clusters of high diet quality, low PA and high SB were more prevalent in girls, while mixed clusters of high PA, high SB and low diet quality were more prevalent in boys. Unhealthy clusters comprising low moderate to vigorous PA, low consumption of fruits and vegetables, and high screen time were prevalent, particularly in those from lower socioeconomic status families. Compared to those with healthy behavioural clusters, those with unhealthy and mixed clusters had a higher adiposity, higher risk of cardiovascular disease, poorer mental health scores, and lower cardiorespiratory fitness.
Conclusions
PA, SB and diet cluster in healthy, unhealthy and mixed patterns in young people that differ across sociodemographic characteristics. Unhealthy clusters are associated with poorer health outcomes. Intervention strategies targeting un-clustering multiple unhealthy behaviours should be developed and evaluated for their impact on health outcomes.
Similar content being viewed by others
Background
Overweight and obesity, and their associated comorbidities, are increasing globally [1]. In the UK, the prevalence of obesity in adults has tripled over the last 20 years and continues to rise albeit at slower rates [2]. A similar pattern is seen in children (aged 10–11 years) in the UK, with obesity levels increasing from 21.0% in 2019–20 to 25.5% in 2020–21 [3]. Living with overweight or obesity is associated with long term health conditions including cardiovascular disease, diabetes, depression and premature mortality [4]. Furthermore, obesity is challenging to manage, and intervention strategies targeted at younger age groups should be a priority [5]. Modifiable health behaviours, including physical inactivity, sedentary behaviours (SB), and unhealthy dietary habits, have all been linked independently to increased risk of obesity in children, adolescents, and young adults [6,7,8].
Physical activity (PA), SBs, and dietary habits are developed early in life and have been shown to track through childhood [9,10,11,12,13,14,15] into adulthood [16]. Evidence suggests that poor lifestyle behaviours are likely to co-occur or ‘cluster’ within groups of individuals [14, 15, 17, 18], and that clustering of unhealthy behaviours increases significantly with age [19]. A recent study found that the prevalence of clustering of unhealthy behaviours increased from 29.0% in children aged 2–5 years to 73.9% among older adolescents aged 16–19 years [19]. Moreover, the most common health behaviour combinations at both time points were high screen time and unhealthy diet (the prevalence increased from 14.4% at ages 2–5 years to 45.3% for ages 16–19 years) [19].
It has been found that the clustering of unhealthy behaviours has synergistic effects on health outcomes, meaning that a combination of health behaviours is more harmful to health than the sum of the effects of each individual health behaviour; this, in turn, will increase the risk of chronic illnesses and premature mortality [20]. For example, clustering of multiple unhealthy behaviours (i.e., SB, lack of PA, and poor dietary habits) has been shown to be associated with poor mental and physical health outcomes such as increased likelihood of developing depression [21,22,23], anxiety, psychological distress, and weight gain [24]. Furthermore, Nelson et al. found that 51% of boys and 43% of girls had three or more behavioural risk factors that were associated with obesity, including low PA, high screen time, low consumption of fruits and vegetables (FV), and high consumption of soft drinks and snacks [25]. Conversely, clustering of beneficial health-related behaviours (being physically active, a non-smoker, moderate drinker and consuming five or more servings of FV a day) has been shown to be associated with improved mental health, improved self-reported physical health, and healthier body weight in adults [26].
Previous systematic reviews have focused on individual health behaviours (i.e. diet, PA, or SB), examined specific health outcomes or combinations of health behaviours (for example, Leech et al. focused only on weight related outcomes), and/or have focused on a narrow age group [27,28,29,30,31,32,33,34,35,36], which limits their ability to address the impact of simultaneous health behaviours on the health of young people more generally. Previous reviews have also combined or synthesised health behaviours under general/broad categories (i.e., total PA, SB or diet) rather than specifying the exact behaviour (such as moderate to vigorous physical activity (MVPA) or FV consumption), which reduces the accuracy of defining specific clusters and trends [37, 38]. Furthermore, many previous reviews have included studies in which additional health behaviours (e.g., smoking, alcohol use) have been included in the creation of clusters that also include PA, SB and dietary behaviours. Being able to disentangle these behaviours from PA, SB and diet is important for our understanding of how PA, SB and diet cluster as lifestyle behaviours, and the impact of clusters of these specific behaviours on health is important for the development of public health interventions. Despite this, clustering of these specific behaviours and their associations with both physical and mental health have not been synthesised in previous systematic reviews. Therefore, it is valuable and timely to investigate the prevalence of clustering patterns of PA, SB, and diet and their associations with physical and mental health indicators in children, adolescents, and young adults. Thus, the aim of this systematic review is to synthesize evidence from longitudinal, cross-sectional and cohort studies on the prevalence of PA, SB, and dietary behaviours clusters by age, sex, and socioeconomic status and their associations with physical and mental health in children, adolescents, and young adults.
Methods
This review was conducted in July 2022 following the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) [39], and was registered with the International Prospective Register of Systematic Reviews (PROSPERO) (CRD42021230976).
Search strategy
The search strategy was developed using the Population Exposure Context Outcome (PECO) concepts, and searches were built around each concept: Population (children, adolescents and young adults), Exposure (clusters of dietary habits, PA and SB), and health Outcomes (physical and mental). Scoping searches were conducted to refine the search strategy and checked by an information specialist and the review team, ensuring that relevant studies were identified with the search syntax. Comprehensive lists of keywords were used to ensure a broad and comprehensive search (please see Additional file 1 for the full search strategy). PubMed (Medline), Web of Science and Scopus electronic databases were searched for articles up to and including July 2022. Electronic searches were supplemented by examination of the bibliographies of included studies and relevant reviews, as well as consultation with subject experts.
Inclusion and exclusion criteria
For studies to be included they were required to: (1) be an observational study including school-aged children and/or adolescents (ages 5–19 years) and/or young adults (ages 19–24 years) as participants; (2) include an examination of the 'patterning', ‘clustering’, or ‘co-existence’ of at least one domain each of PA, dietary behaviour and SB; and (3) be published in English up to and including 24th July 2022. Studies that included all three behaviours but did not attempt to identify clusters of these three behaviours or examine an interaction or association between these behaviours were excluded. Similarly, studies that included PA, SB and dietary variables in addition to other health behaviours (e.g., alcohol consumption, sleep) were excluded if data on the three behaviours of interest could not be extracted. In addition, randomised controlled trials or any intervention studies where behaviours had been manipulated were excluded.
Identification of relevant studies
Covidence review management software (www.covidence.org) was used for the screening and selection of records retrieved from the database and manual searches, including the removal of duplicates. Screening by title and abstract was conducted initially. A full text copy of all articles meeting the initial screening was obtained for examination. All screening was conducted by two independent reviewers, with a third reviewer assessing a random sample of 10% of the excluded studies at both title/abstract and full text stages. Any disagreements, at any stage, were resolved via consulting a third reviewer.
Data extraction
A data extraction form was developed in Excel for the purpose of this review and was used to collate the data. The data extraction form was piloted by two reviewers on a proportion of the included studies to assess its suitability. After consultation with the review team, it was modified accordingly. The following data was extracted from each paper: (1) general information (study ID, title, author/s, date, study location (country), study aim, study type); (2) participant characteristics (participant selection and sample size, etc.); and (3) type of study, duration of study, methods and measures of health behaviours, analytical methods for clustering and statistical analyses. In addition to information on prevalence of clustering, data on any reported physical and mental health outcomes were extracted. Data extraction was performed by one reviewer and 50% of articles were checked for completeness, accuracy and consistency by a second independent reviewer. Any disagreements were resolved via discussion between the reviewers and lessons learned applied to the remaining studies.
Risk of bias assessment
A risk of bias assessment was carried out for each of the included studies, as described in the Cochrane Handbook [40] and elsewhere [41].As this is a review of observational studies, the risk of bias assessment assessed each study against the following domains: (1) selection bias, (2) performance bias, (3) detection bias, (4) attrition bias, (5) selective reporting bias, and (6) other factors that may increase the risk of bias. Risk of bias assessments were completed independently by two reviewers, and discrepancies (n = 2) were resolved through discussion and the judgement of a third author. Each study was classified as either a low risk of bias, high risk of bias, or an unclear risk.
Synthesis of results
Each included article had to include all three health behaviours of interest. For synthesis, we report the cluster names and descriptions exactly as they are reported in the original manuscripts. Results were synthesised narratively because a meta-analysis was not feasible due to the considerable heterogeneity in terms of methodological, statistical, and clinical aspects.
Results
Search results
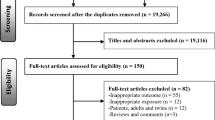
A full summary of the search results is presented in the PRISMA flowchart diagram (Fig. 1). A total of 21,282 records were identified during the electronic database searches. After duplicates were removed, a total of 17,115 records remained. Of those, 16,814 records were deemed ineligible during the titles and abstracts screening process, 301 full-text articles were retained for further review, and 53 studies met the inclusion criteria.

PRISMA flow diagram for the identification, screening, eligibility and inclusion of studies
Study characteristics
Characteristics of the 53 included studies are summarised in Additional file 2. Studies were conducted across eighteen countries; the majority were from the US (n = 9) [19, 42,43,44,45,46,47,48,49], Brazil (n = 9) [50,51,52,53,54,55,56,57,58] and Australia (n = 5) [25, 59,60,61,62], and seven provided data from more than one country [63,64,65,66,67,68,69]. Studies were published between 2007 [46] and 2022 [57, 58], with the majority (87%) published within the last decade. Forty-nine studies employed a cross-sectional design and four used a longitudinal design [59, 70,71,72] with follow-up durations ranging between two [70, 71] and six [72] years post baseline. Most studies included adolescents (n = 31) [25, 42, 44, 46,47,48, 50,51,52,53,54,55,56,57,58, 63, 64, 66, 68, 72,73,74,75,76,77,78,79,80,81,82,83], thirteen included children (n = 13) [43, 49, 61, 62, 65, 67, 69, 70, 84,85,86,87,88], seven included both children and adolescents (n = 7) [19, 45, 59, 60, 71, 89, 90], one included adolescents and young adults (n = 1) [91], and only one study included young adults only (n = 1) [92]. Participants’ ages ranged from five [19, 49, 59,60,61, 70, 89] to 25 [92] years, with sample sizes ranging from 189 [78] to 304,779 [68], representing a total of 778,415 children, adolescents, and young adults. Forty-nine studies provided data on the prevalence of clusters of PA, SB and diet [19, 25, 42, 44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68, 71, 72, 74,75,76,77,78,79,80,81,82,83,84,85,86,87,88,89,90,91,92]. Twenty studies examined the associations between clusters and physical health outcomes (adiposity or cardiometabolic health) [43, 44, 51, 55, 56, 58, 59, 63,64,65, 67, 69,70,71,72,73,74,75, 89, 90], and one study examined associations with mental health outcomes [74].
Risk of bias and quality assessment
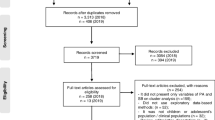
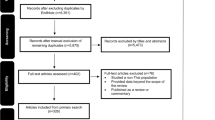
Risk of bias was conducted for all included studies. For both study types, between 5 and 30% had a high-risk judgment across all domains, while low-risk judgment varied between ~ 50–90%. Some of the domains had an unclear judgment due to lack of information (~ 5–55%) (Figs. 2 and 3).

Overview of prevalence study quality and risk of bias [low, high, and unclear] assessment (n = 49)

Overview of health outcomes study quality and risk of bias [low, high, and unclear] assessment (n = 20)
Overview of measures
The included studies employed a variety of methods to assess behaviours. PA and SB were measured using accelerometers in nine [44, 46, 49, 59,60,61, 71, 84, 87] and four [44, 59, 60, 71] studies, respectively, and were either self-reported or parent-reported in the other studies. For dietary data collection, questionnaires (e.g., a set of questions in a survey pack) were the most prevalent instrument used (n = 28) [45, 48, 50,51,52,53,54, 56,57,58, 61, 62, 68, 69, 71, 73, 74, 79,80,81,82,83, 85, 86, 88,89,90, 92], followed by food frequency questionnaires (FFQ) (n = 16) [25, 42, 43, 59, 60, 64, 65, 67, 70, 72, 75,76,77,78, 87, 91], 24-h dietary recall (n = 8) [19, 44, 46, 49, 55, 63, 64, 66], a diet diary (n = 1) [84], and multiple-pass recall methods (n = 1) [47].
PA was presented using varied units including daily MVPA [25, 44, 59, 60, 63, 64, 71, 87], daily PA [68, 82, 89], moderate physical activity (MPA) [44], vigorous physical activity (VPA) [44, 65],weekly MVPA [19, 43, 50, 55, 66, 74, 78, 83, 88], days per week of PA [19, 42, 51, 54, 57, 79, 80, 92], MPA [91], and VPA [48], meeting PA recommendations [46, 47, 49, 61, 62, 76, 81, 84], weekly [53, 56, 67, 70, 88, 90] or daily [45, 86] sport participation and playing outside, weekly sports at a club [69, 70, 72, 77], frequency and duration of weekly leisure time [52, 72, 75, 77], days per week of active commuting [52, 70, 81], days per week of physical education [48], and other PA/sport at school [48, 52, 70, 75, 81] and non-school [48, 73, 81], activity preferences [85], and PA score [58]. For SB, the most common outcomes measured were daily screen time (n = 20) [19, 25, 43, 45, 50, 51, 54,55,56, 58, 63, 65, 66, 71, 75, 86,87,88,89,90], followed by meeting screen time recommendations (n = 8) [46, 47, 49, 61, 62, 76, 81, 84] and daily sedentary time (n = 10) [44, 53, 57, 59, 60, 71, 79, 80, 82, 83]. Other studies used daily [52, 59, 64, 73, 93] or weekly [69] TV viewing, daily [42, 44, 48, 81, 92] or weekly [70] TV viewing and computer use, daily electronic media use [72, 77], and daily non screen SB (e.g. sitting and homework) [52, 63, 68, 91]. Finally, two studies used weekly screen time [74, 78], and only one used weekly sedentary time [67] and activity preference (e.g. computer use, TV viewing, reading, and tinkering) [85].
The most prevalent dietary outcomes used were daily [25, 42, 45, 51, 59, 60, 64, 68, 78,79,80, 82, 83, 87, 90, 91] and weekly [50, 51, 56,57,58, 65, 67, 69, 73, 74, 78] FV consumption, diet quality index [19, 43, 44, 63, 66, 71, 72, 77, 88], meeting dietary recommendations (i.e., FV, sugar-sweetened beverages (SSB), fat, energy dense food/drink, discretionary food, having breakfast, milk/yogurt intake, and total dietary fat and non-milk extrinsic sugar) [46, 47, 49, 61, 62, 76, 81, 84], daily [45, 64, 86, 90] and weekly [67, 69, 87] intake of SSB, daily [42, 51, 83, 90] and weekly [25, 51, 56,57,58, 65, 74, 81] intake of sweetened soft drinks, daily [59, 93] and weekly [58] energy dense food/drink consumption, daily [42, 45, 86, 90] and weekly [25, 56, 57, 73, 74, 81] intake of snacks, daily [42, 48, 54, 55, 75, 78, 90] and weekly [52, 53, 58, 70, 73, 75, 78, 92] consumption of diverse foods (e.g. fibre, dairy, chips, etc.), meal frequency [89], breakfast intake [45, 81, 90] or skipping [89], and daily [83, 90] and weekly [19, 81] fast-food intake. Weekly eating at restaurants [45] and food preferences [85] were each used once. All methods used to assess PA, diet, and SB are shown in Additional file 2, along with the measures of these behaviours.
Cluster analysis methods
The included studies used various methods for clustering analysis (Additional file 2). To determine the number of meaningful clusters into which to assign participants most studies combined the Ward and k-means methods [51, 64,65,66,67, 69, 71, 77, 78, 86, 88], while one study used a combination of hierarchical method and k-means cluster analysis [63], one applied the Ward method exclusively [61], and two used a k-means non-hierarchical method [52, 74]. Latent class analysis [42, 44, 45, 56, 83, 87, 90, 91], latent profile analysis [48], K-means [73, 75] and k-medians [59, 60], principal component [70, 85], and two-step [53, 57, 58, 81, 92] cluster analyses were also used to identify subgroups of participants with similar patterns. In addition, some studies used the observed-over-expected ratio (O/E) [25, 50, 54, 68, 79, 80, 82, 84] or other descriptive analyses [19, 43, 46, 47, 49, 55, 62, 72, 76, 89] to determine the prevalence of health-related behaviour patterns observed.
Clusters of behaviours identified
The 53 studies reviewed presented 172 unique clusters of health-related behaviours of interest, broadly classified as healthy (n = 28), unhealthy (n = 46), and mixed (n = 98) clusters (Additional file 3). A healthy cluster was typically characterised by good diet quality, high PA, and low SB, while an unhealthy cluster was characterised by poor diet quality, low PA and high SB. The majority fell into the mixed cluster, which included one or more healthy behaviours coexisting with one or more unhealthy behaviours (e.g. high PA, high FV, and high SB). In the healthy lifestyle clusters, only two clusters (high MVPA high FV low SSB low screen time [47, 49] and high MVPA low energy dense food/drink low SB low TV [59, 93]) were reported in two studies, while the unhealthy lifestyle cluster low MVPA low FV high screen time was reported in three studies [25, 50, 81]. Nineteen mixed lifestyle clusters were common in two studies each. Among the included studies, the health-related behaviours of interest (diet/PA/SB) were represented by a minimum of one (e.g. high PA high FV low SB) and a maximum of 13 distinct clusters.
Prevalence of clusters of health behaviours
The prevalence of clusters of health behaviours are described in Table 1. Twenty-four healthy clusters showed a prevalence of between 0–30%, eighteen clusters between 30–60% and only one cluster between 60–100%. Mixed clusters didn’t follow a particular structure, but rather they were classified as mixed because of presence of one or more healthy behaviour coexisting with one or more unhealthy behaviour (e.g. high PA, high FV, and high SB). For the mixed clusters, ninety-six showed a prevalence between 0–30%, thirty-seven clusters between 30–60% and six clusters between 60–100%. Fifty-five unhealthy clusters showed a prevalence of between 0–30%, twenty-one clusters between 30–60% and seven clusters between 60–100%.
Twenty-two studies stratified clusters of health behaviours by sex [25, 42, 44, 46, 50,51,52, 55, 56, 63, 64, 66,67,68,69, 72, 76, 79, 80, 83, 89, 90], ten studies by age group [19, 45, 57, 59, 60, 63, 69, 71, 72, 89], three by region [64, 65, 82], and one study by maturity status [58]. Overall, more females were found in the unhealthy clusters [25, 44, 46, 53,54,55, 57, 59, 60, 68, 71, 77, 80, 83, 89, 92] or mixed clusters comprising a combination of high diet quality, low PA, and/or high SB [44, 45, 48, 51,52,53, 58, 63, 66, 74, 77, 81, 85, 88]. Males tended to be found in healthy [45, 58, 59, 62, 71, 77] or mixed clusters characterised by a combinations of high PA, high SB, and/or low diet quality [48, 51, 53, 56, 63, 66, 69, 70, 74, 77, 81, 86, 88, 92]. With regard to differences in age groups, most studies found that younger individuals (i.e. children, younger adolescents) tended to belong to healthier clusters [45, 51, 59, 63, 64, 75, 85], while older participants (i.e. older adolescents, young adults) were likelier to be in unhealthy [42, 45, 46, 59, 60, 63, 64, 66, 75, 88, 89] or mixed clusters characterised by lower PA [44, 46, 53, 74, 89].
Twenty-two studies assessed differences in socioeconomic status among clusters of health behaviours of interest [25, 42, 47, 48, 51,52,53,54, 57, 60, 62, 64, 66, 67, 71, 75, 77, 78, 81, 86, 89, 90]. The data suggest that young people from low socioeconomic status exhibit unhealthier lifestyle patterns compared to those from families with higher socioeconomic status [25, 51, 53, 60, 67, 70, 71, 77, 78, 81, 86, 89].
Markers of adiposity
Sixteen studies examined associations between clusters of health behaviours and markers of adiposity (Table 2) [51, 55, 56, 59, 63,64,65, 67, 70,71,72,73,74,75, 89, 90]. Three examined those associations in children [65, 67, 70], nine in adolescents [51, 55, 56, 63, 64, 72,73,74,75], and four in both children and adolescents [59, 71, 89, 90]. The majority included body mass index (BMI) as the main anthropometric marker, whether continuous [59, 65, 67, 70, 73, 89] or in categories (e.g. normal weight, overweight, obese) [51, 55, 56, 59, 64, 65, 70, 72, 74, 75, 89, 90], except one study that used body fat percentage [63, 71], and one study that used body fat percentage with fat-free mass percentage, and waist circumference [63]. Some studies measured additional adiposity indicators in addition to BMI, such as waist-to-height ratio (WHtR) [75, 89], waist circumference [55, 64, 67], skinfolds [67], and body fat percentage using bio-electrical impedance [64]. Sixteen studies examined the association of behavioural clusters and adiposity; twelve cross-sectional [51, 55, 56, 63,64,65, 67, 73,74,75, 89, 90] and four longitudinal [59, 70,71,72]. Of the studies that examined BMI, continuous or in categories (overweight/obesity), a total of nine studies [51, 55, 64, 65, 67, 70, 74, 75, 89] found an association between clusters with mixed (low PA and/or high SB) and unhealthy behaviour clusters and increased probability of overweight/obesity, one found an unexpected inverse association [73], and two found no association [56, 59].
Three longitudinal studies [59, 70, 72] examined associations between clusters and BMI and concluded that high TV viewing, high energy-dense food/drink consumption [59] and high SB and unhealthy snacks [70], resulted in a higher likelihood of being classified as overweight/obese [59] and increased BMI [70]. One study found that unhealthy clusters characterised by high media use (i.e., watching TV, using a computer, and playing console games) and low PA and diet quality resulted in the greatest difference in weight status and was related to change from normal weight to overweight over time [72].
One study investigating the clustering of health behaviours across groups of countries (North and East Europe, South Europe/Mediterranean Countries, and West-Central Asia) found that unhealthy and mixed clusters were positively associated with a greater risk of being overweight or obese compared to healthy clusters [65]. Another study conducted in eight European countries (Italy, Estonia, Cyprus, Belgium, Sweden, Hungary, Germany and Spain) found that increased time in sedentary activities and low PA was associated with higher BMI, but only in boys [67].
All studies that examined mixed and unhealthy clusters showed positive associations with waist circumference [55, 64, 67, 75, 89]. Although the findings of these studies varied; for example, one found an association only among boys [67] and another found that the risk of central obesity was over double among those in an unhealthy cluster (high fast foods, sweetened beverages, energy drinks and sweets, and breakfast or school meal skipped and had screen time more 10 h/day) compared to those in a healthy cluster (high FV, dairy products and fish, consumed daily breakfast or school meal, had VPA and low screen time) [75]. Another study showed that young people in the healthy cluster (low screen time and SB, high MVPA, and average to high levels of adherence to Mediterranean diet) had considerably lower body fat at baseline and two years later, with body fat percentage at baseline being a positive predictor of body fact percentage two years later for all groups [71]. However, no significant differences by cluster were noted in body composition [63] or skin folds [67].
Cardiometabolic outcomes
Five studies examined associations between clusters of health behaviours and cardiometabolic markers, including aerobic fitness (Table 3) [43, 44, 58, 63, 69]. One study found that girls and boys in the healthy cluster (high diet quality and MVPA and low screen use) had higher aerobic fitness levels [63], whereas boys in the unhealthy cluster —high screen time and low diet quality—had the lowest aerobic capacity compared to other clusters [63]. In another study, there were no associations between clusters and cardiorespiratory fitness (VO2 max) in girls, but boys in the healthy cluster (high diet score and MVPA and screen time) had the highest VO2 max [44]. Furthermore, another study found that clusters with low SSB consumption and/or low levels of screen time were associated with a healthier cardiovascular disease (CVD) profile than being physically active or eating a diet high in FV [69]. However, clusters of self-reported diet, screen-time and PA were not related to CVD risk in children in one study [43]. One study examined the association with metabolic risk in adolescents according to maturity status and found that early-maturing adolescents in the cluster with a greater number of healthy behaviours but less PA had a greater metabolic risk score [58].
Mental health outcomes
Mental health outcomes were examined in one study which showed that children in the healthy cluster had better self-regulation, motivation, communication with parents, and liking school compared to those in a mixed clusters [74]. Furthermore, those in a mixed cluster characterised by high PA and high SB and poor diet had better relationships with classmates than their peers in a mixed cluster characterised by low PA and low FV and moderate TV.
Discussion
The aim of this systematic review was to synthesize evidence on the prevalence of clusters of PA, SB, and dietary behaviours and to examine their associations with physical and mental health outcomes in children, adolescents, and young adults aged 5–24 years. Health behaviour patterns by age, sex, and socioeconomic status were also examined. The health behaviour clusters in this review were classified as healthy, unhealthy or mixed (the co-occurrence of both healthy and unhealthy behaviours). Overall, the majority of participants examined fell into the mixed clusters, which is in line with previous reviews’ findings [38, 93, 94], and supports the need for multicomponent interventions addressing several unhealthy behaviours simultaneously. It is also noteworthy that high PA and high SB most frequently clustered together, refuting the displacement hypothesis that assumes that time spent on one activity cannot be spent on another (i.e., SB displaces PA) [95]. Supportive of our findings, a previous review examined the association between SB and PA in young people and concluded that these behaviours do not directly displace one another and should be seen as different constructs [96].
Almost a quarter of clusters identified in the present review were classified as ‘unhealthy’. Clusters characterised by high SB and low PA were commonly reported across the studies. Previous reviews have shown similarly high numbers of unhealthy clusters. For example, Leech et al. found that eight of eighteen studies identified unhealthy clusters [93]. The present review also showed the coexistence of unhealthy food intake (e.g., snacks, sweets, soft drinks, junk food, SSB) with high SB (i.e., TV, media use, and/or computer use). These clusters were found in a previous review that found that SB, particularly high TV viewing, was associated with greater intake of discretionary foods and less FV consumption in children age 5–11 years [97]. The mechanisms of the observed associations between SB and diet have been examined previously and may be explained by the stimulating influence of commercials/advertisements for intake of foods high in fat, sugar and salt (HFSS) [98], that sedentary activities encourage passive snacking or overeating [99], and that watching TV while eating may disrupt habituation to food cues [100]. Not surprisingly, children were more likely to be overweight or obese in clusters with both high levels of SB and high consumption of unhealthy foods or poor diet quality. These results are in agreement with a review conducted by Leech et al. (2014), who showed that TV viewing in combination with energy-dense food and drink consumption were associated with overweight and obesity among Australian children [93]. Based on these findings, prevention programs should identify strategies aimed at uncoupling the combination of unhealthy dietary habits in front of screens.
Healthy clusters characterised by high MVPA, low screen time and overall high diet quality (e.g., high FV, low SSB, etc.), followed by high PA, low screen time and overall high diet quality were most prevalent. These findings are similar to the healthy clusters identified in Leech et al.’s (2014) review that observed these clusters in children and adolescents [93]. Another important finding in the present review that extends the findings of previous reviews was that children and adolescents with these healthy clusters had lower BMI and higher fitness compared to those in mixed and unhealthy clusters. On the other hand, more active adolescents with unfavourable diet quality showed lower fitness than those with similar activity levels but favourable diet quality [63]. It is important to note that PA might be protective of increases in adiposity and might increase fitness level when combined with a healthy diet and/or low screen time. This finding is informative for future interventions that should combine strategies for increasing PA and healthy diets while simultaneously including strategies to lower screen time. In addition, a notable finding was that only one study examined mental health outcomes of clusters. This study found that healthy clusters (high PA and FV, low sweets and soft drinks, and lowest SB) were associated with better mental health outcomes compared to mixed and unhealthy clusters. It is worth noting that in this one study PA appeared to be associated with better mental health outcomes on its own, as clusters with high PA and high SB were more strongly associated with mental health outcomes than clusters with low PA and high SB. Further research is needed to examine a range of mental health outcomes of clusters of lifestyle behaviours.
This review found that both unhealthy clusters and mixed clusters that include either high SB, low PA, and/or high SSB, alongside healthy behaviours, were associated with higher adiposity in young people. This was contrary to findings from a previous systematic review [38], which concluded that only unhealthy clusters were associated with higher adiposity levels. It is worth highlighting that in the present review only a particular combination of health behaviours within mixed clusters (i.e., those that include either high SB, low PA and/or high SSB alongside healthy behaviours) were associated with unfavourable weight status. Previous research has suggested that the combination of healthy and unhealthy behaviours negate each other’s health effects [94]. These findings suggest that, to decrease obesity risk, future research should focus on understanding in who and why, where and when such behaviours cluster together with a view to informing future multicomponent/multi-behaviour interventions to uncouple unhealthy behaviours.
In this review, clusters characterised by high SB, particularly screen time, were found to increase the risk of adiposity, irrespective of being combined with other healthy or unhealthy behaviours. As a result, it is likely that excessive screen time may reduce the beneficial effects of PA and a healthy diet on the risk of obesity. These results match those cited in Leech et al.’s (2014) review, which found a positive association between overweight and high SB [93]. The current review also found that clusters with higher screen time had greater risk of individual and clustered cardiovascular risk scores, which were predominantly seen in older boys, worse fitness levels, and greater psychosocial risks, mostly in girls. In line with this, a recent systematic review that examined the relationship between SB and health indicators in young people aged 5–17 years found that an increase in SB, expressed as total hours of screen time, was associated with an increase in cardiovascular risk markers in children and adolescents [101]. Despite PA having previously being linked with clustered metabolic risk in children [102], this review suggested that SB, expressed as screen time, has a greater role in the cardiovascular risk profile than PA. This is alarming, given the growing body of evidence to suggest that SB is independently and positively related to poor health outcomes [103]. Future public health plans need to target a reduction in screen time among young people and could be considered within multicomponent/complex interventions.
Young people’s gender, age, and socioeconomic status have consistently been shown to be associated with health behaviour cluster scores, underlining the need for tailoring prevention and intervention efforts for groups at risk. In the current review, girls tended to be in unhealthy clusters or mixed clusters mostly defined by better diet quality, but lower PA compared to boys. However, boys were almost equally distributed between unhealthy and healthy clusters or mixed clusters with high PA, unhealthy diets and/or high SB. These results can be explained by sex differences in dietary habits as hypothesized in a previous study [104], in addition to unbalanced patterns of PA [105]. Moreover, younger people (for example, children and young adolescents) and those from higher socioeconomic status were found in healthy clusters or mixed clusters with higher PA, in contrast with older people (for example, older adolescents and young adults) and those from lower socioeconomic status who were found in unhealthy clusters or mixed clusters with lower PA. These findings were consistent with previous reviews [93, 94]. A longitudinal study concluded that children’s behaviours tended to shift to unhealthier clusters with aging [59], which is in line with other longitudinal studies that show an age-related increase in SB and decrease in PA [106]. At present many monitoring efforts, such as the National Child Measurement Programme [107] in the UK, policy and interventions target children and young adolescents [108]. Given the results of this intervention there is a need to also focus efforts on older adolescents. Furthermore, the findings that socioeconomic status were negatively associated with adiposity and positively associated with health, provides further evidence for the need to devote more resources to policies and programmes targeting lower socioeconomic families.
Strengths and limitations
To the best of our knowledge, this was the first study to systematically review clusters of PA, SB, and diet in children, adolescents, and young adults and the associations with physical and mental health outcomes. This information will be valuable for designing intervention strategies to improve the health of young people. Limitations that must be considered when interpreting these results include that a meta-analysis was not possible due to heterogeneity in the measures and analyses used in the studies included. The majority of studies were of a cross-sectional nature, which did not allow us to draw causal relationships. Also, data on many behaviours were obtained via self-report tools (such as questionnaires), which are subject to measurement errors due to social desirability or recall bias [109].
Conclusion
This review synthesised the evidence on the prevalence of clustering of PA, SB, and diet in 5- to 24-year-olds and examined physical and mental health outcomes associated with the clusters. Clusters of health behaviours appeared to differ across socio-demographic groups and were broadly grouped into healthy, unhealthy, and mixed lifestyle clusters, emphasising the complexity and diversity across the populations examined. Mixed clusters were the most prevalent, and both mixed and unhealthy clusters were related to poor health in young people. The complex nature of these findings’ stresses the need for more research examining, in more detail, the sociodemographic factors that influence different clusters of behaviours and how these influence health. More studies that include young adults are needed.
Availability of data and materials
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- SB:
-
Sedentary behaviour
- PA:
-
Physical activity
- FV:
-
Fruits and vegetables
- MVPA:
-
Moderate to vigorous physical activity
- PRISMA:
-
Preferred reporting items for systematic reviews and meta-analysis
- PROSPERO:
-
International prospective register of systematic reviews
- PECO:
-
Population exposure context outcome
- MPA:
-
Moderate physical activity
- VPA:
-
Vigorous physical activity
- SSB:
-
Sugar-sweetened beverages
- O/E:
-
Observed-over-expected ratio
- BMI:
-
Body mass index
- WHtR:
-
Waist-to-height ratio
- CVD:
-
Cardiovascular disease
- HFSS:
-
High in fat, sugar and salt
References
Malik VS, Willet WC, Hu FB. Nearly a decade on — trends, risk factors and policy implications in global obesity. Nat Rev Endocrinol. 2020;16(11):615–6.
Statistics on Obesity, Physical Activity and Diet, England, 2020. https://digital.nhs.uk/data-and-information/publications/statistical/statistics-on-obesity-physical-activity-and-diet/england-2020. Accessed 28 Nov 2021.
National Child Measurement Programme, England 2020/21 School Year. https://digital.nhs.uk/data-and-information/publications/statistical/national-child-measurement-programme/2020-21-school-year. Accessed 28 Nov 2021.
Reilly JJ, Kelly J. Long-term impact of overweight and obesity in childhood and adolescence on morbidity and premature mortality in adulthood: systematic review. Int J Obes. 2011;35(7):891–8.
Summerbell CD, Waters E, Edmunds L, Kelly SA, Brown T, Campbell KJ. Interventions for preventing obesity in children. Cochrane Database Syst Rev. 2005. https://doi.org/10.1002/14651858.cd001871.pub2.
Healy GN, Wijndaele K, Dunstan DW, Shaw JE, Salmon JO, Zimmet PZ, et al. Objectively measured sedentary time, physical activity, and metabolic risk the australian diabetes, obesity and lifestyle study (AusDiab). Diabetes Care. 2008;31(2):369–71.
Newby PK. Are dietary intakes and eating behaviors related to childhood obesity? a comprehensive review of the evidence. Journal of Law, Medicine & Ethics. 2007;35(1):35–60.
Kipping RR, Jago R, Lawlor DA. Obesity in children. Part 1: Epidemiology, measurement, risk factors, and screening. BMJ. 2008;337(7675):922–7.
Khaw K-T, Wareham N, Bingham S, Welch A, Luben R, Day N. Combined impact of health behaviours and mortality in men and women: The EPIC-norfolk prospective population study. PLoS Med. 2008;5(1): e12.
Maffeis C. Aetiology of overweight and obesity in children and adolescents. Eur J Pediatr. 2000;159(S1):S35–44.
Lobstein T, Baur L, Uauy R. Obesity in children and young people: a crisis in public health. Obes Rev. 2004;5(1):4–104.
Global Health Risks. http://www.who.int/healthinfo/global_burden_disease/GlobalHealthRisks_report_full.pdf. Accessed 5 Dec 2021.
Lioret S, Campbell KJ, McNaughton SA, Cameron AJ, Salmon J, Abbott G, et al. Lifestyle patterns begin in early childhood, persist and are socioeconomically patterned, confirming the importance of early life interventions. Nutrients. 2020;12(3):724.
Pearson N, Biddle SJH, Griffiths P, Johnston JP, Haycraft E. Clustering and correlates of screen-time and eating behaviours among young children. BMC Public Health. 2018;18(1):1–9.
Pearson N, Griffiths P, Biddle SJ, Johnston JP, McGeorge S, Haycraft E. Clustering and correlates of screen-time and eating behaviours among young adolescents. BMC Public Health. 2017;17(1):533.
Mikkilä V, Räsänen L, Raitakari OT, Pietinen P, Viikari J. Consistent dietary patterns identified from childhood to adulthood: The Cardiovascular Risk in Young Finns Study. Br J Nutr. 2005;93(6):923–31.
Poortinga W. The prevalence and clustering of four major lifestyle risk factors in an English adult population. Prev Med (Baltim). 2007;44(2):124–8.
Pearson N, Sherar LB, Hamer M. Prevalence and correlates of meeting sleep, screen-time, and physical activity guidelines among adolescents in the United Kingdom. JAMA Pediatr. 2019;173(10):993–4.
Mayne SL, Virudachalam S, Fiks AG. Clustering of unhealthy behaviors in a nationally representative sample of U.S. children and adolescents. Prev Med (Baltim). 2020;130:105892.
Kaczynski A. Smoking and physical activity: a systematic review. Am J Health Behav. 2008;32(1):93–110.
Ye YL, Wang PG, Qu GC, Yuan S, Phongsavan P, He QQ, et al. Associations between multiple health risk behaviors and mental health among Chinese college students. Psychol Health Med. 2016;21(3):377–85.
Dodd LJ, Al-Nakeeb Y, Nevill A, Forshaw MJ. Lifestyle risk factors of students: a cluster analytical approach. Prev Med (Baltim). 2010;51(1):73–7.
Kwan MY, Arbour-Nicitopoulos KP, Duku E, Faulkner G. Patterns of multiple health risk–behaviours in university students and their association with mental health: application of latent class analysis. Health Promot Chronic Dis Prev Can. 2016;36(8):163–70.
Nelson MC, Gordon-Larsen P, Adair LS, Popkin BM. Adolescent physical activity and sedentary behavior: Patterning and long-term maintenance. Am J Prev Med. 2005;28(3):259–66.
Hardy LL, Grunseit A, Khambalia A, Bell C, Wolfenden L, Milat AJ. Co-occurrence of obesogenic risk factors among adolescents. J Adolesc Health. 2012;51(3):265–71.
Harrington J, Perry IJ, Lutomski J, Fitzgerald AP, Shiely F, McGee H, et al. Living longer and feeling better: healthy lifestyle, self-rated health, obesity and depression in Ireland. Eur J Public Health. 2010;20(1):91–5.
Liberali R, Kupek E, de Assis MAA. Dietary patterns and childhood obesity risk: a systematic review. Child Obes. 2020;16(2):70–85.
Hoare E, Milton K, Foster C, Allender S. The associations between sedentary behaviour and mental health among adolescents: a systematic review. Int J Behav Nutr Phys Act. 2016;13(1):108.
Wu XY, Zhuang LH, Li W, Guo HW, Zhang JH, Zhao YK, et al. The influence of diet quality and dietary behavior on health-related quality of life in the general population of children and adolescents: a systematic review and meta-analysis. Qual Life Res. 2019;28(8):1989–2015.
Wu XY, Han LH, Zhang JH, Luo S, Hu JW, Sun K. The influence of physical activity, sedentary behavior on health-related quality of life among the general population of children and adolescents: a systematic review. PLoS ONE. 2017;12(11): e0187668.
Rodriguez-Ayllon M, Cadenas-Sánchez C, Estévez-López F, Muñoz NE, Mora-Gonzalez J, Migueles JH, et al. Role of physical activity and sedentary behavior in the mental health of preschoolers, children and adolescents: a systematic review and meta-analysis. Sports Med. 2019;49(9):1383–410.
Biddle SJH, Asare M. Physical activity and mental health in children and adolescents: a review of reviews. Br J Sports Med. 2011;45(11):886–95.
Głąbska D, Guzek D, Groele B, Gutkowska K. Fruit and vegetables intake in adolescents and mental health: a systematic review. Rocz Panstw Zakl Hig. 2020;71(1):15–25.
Głąbska D, Guzek D, Groele B, Gutkowska K. Fruit and vegetable intake and mental health in adults: a systematic review. Nutrients. 2020;12(1):115.
Stiglic N, Viner RM. Effects of screentime on the health and well-being of children and adolescents: a systematic review of reviews. BMJ Open. 2019;9(1): e023191.
Jao NC, Robinson LD, Kelly PJ, Ciecierski CC, Hitsman B. Unhealthy behavior clustering and mental health status in United States college students. J Am Coll Health. 2019;67(8):790–800.
de Mello GT, Lopes MVV, Minatto G, da Costa RM, Matias TS, Guerra PH, et al. Clustering of physical activity, diet and sedentary behavior among youth from low-, middle-, and high-income countries: a scoping review. Int J Environ Res Public Health. 2021;18(20):10924.
D’Souza NJ, Kuswara K, Zheng M, Leech R, Downing KL, Lioret S, et al. A systematic review of lifestyle patterns and their association with adiposity in children aged 5–12 years. Obes Rev. 2020;21(8): e13029.
Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, The PRISMA, et al. statement: an updated guideline for reporting systematic reviews. BMJ. 2020;2021:372. https://doi.org/10.1136/BMJ.N71.
Higgins JP, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, et al. Cochrane Handbook for Systematic Reviews of Interventions version 6.3. 2022.
Dutil C, Walsh JJ, Featherstone RB, Gunnell KE, Tremblay MS, Gruber R, et al. Influence of sleep on developing brain functions and structures in children and adolescents: a systematic review. Sleep Med Rev. 2018;42:184–201.
Iannotti RJ, Wang J. Patterns of physical activity, sedentary behavior, and diet in U.S. adolescents. J Adolesc Health. 2013;53(2):280–6.
Drenowatz C, Carlson JJ, Pfeiffer KA, Eisenmann JC. Joint association of physical activity/screen time and diet on CVD risk factors in 10-year-old children. Front Med. 2012;6(4):428–35.
Hartz J, Yingling L, Ayers C, Adu-Brimpong J, Rivers J, Ahuja C, et al. Clustering of health behaviors and cardiorespiratory fitness among U.S. adolescents. J Adolesc Health. 2018;62(5):583–90.
Schmiege SJ, Gance-Cleveland B, Gilbert L, Aldrich H, Gilbert KC, Barton A. Identifying patterns of obesity risk behavior to improve pediatric primary care. J Spec Pediatr Nurs. 2016;21(1):18–28.
Sanchez A, Norman GJ, Sallis JF, Calfas KJ, Cella J, Patrick K. Patterns and correlates of physical activity and nutrition behaviors in adolescents. Am J Prev Med. 2007;32(2):124–30.
Foltz JL, Cook SR, Szilagyi PG, Auinger P, Stewart PA, Bucher S, et al. US adolescent nutrition, exercise, and screen time baseline levels prior to national recommendations. Clin Pediatr (Phila). 2011;50(5):424–33.
Berlin KS, Kamody RC, Thurston IB, Banks GG, Rybak TM, Ferry RJ. Physical activity, sedentary behaviors, and nutritional risk profiles and relations to body mass index, obesity, and overweight in eighth grade. Behav Med. 2017;43(1):31–9.
Kunin-Batson AS, Seburg EM, Crain AL, Jaka MM, Langer SL, Levy RL, et al. Household factors, family behavior patterns, and adherence to dietary and physical activity guidelines among children at risk for obesity. J Nutr Educ Behav. 2015;47(3):206–15.
Silva KS, Barbosa Filho VC, del Duca GF, de Anselmo Peres MA, Mota J, Lopes A da S, et al. Gender differences in the clustering patterns of risk behaviours associated with non-communicable diseases in Brazilian adolescents. Prev Med (Baltim). 2014;65:77–81.
de Souza Dantas M, Dos Santos MC, Lopes LAF, Guedes DP, Guedes MRA, Oesterreich SA. Clustering of excess body weight-related behaviors in a sample of Brazilian adolescents. Nutrients. 2018;10(10):1505.
Maia EG, Mendes LL, Pimenta AM, Levy RB, Claro RM. Cluster of risk and protective factors for obesity among Brazilian adolescents. Int J Public Health. 2018;63(4):481–90.
Matias TS, Silva KS, Da SJA, De MGT, Salmon J. Clustering of diet, physical activity and sedentary behavior among Brazilian adolescents in the national school - Based health survey (PeNSE 2015). BMC Public Health. 2018;18(1):1283.
Nunes HEG, Gonçalves ECDA, Vieira JAJ, Silva DAS. Clustering of risk factors for non-communicable diseases among adolescents from southern Brazil. PLoS ONE. 2016;11(7): e0159037.
Cureau FV, Sparrenberger K, Bloch KV, Ekelund U, Schaan BD. Associations of multiple unhealthy lifestyle behaviors with overweight/obesity and abdominal obesity among Brazilian adolescents: a country-wide survey. Nutr Metab Cardiovasc Dis. 2018;28(7):765–74.
de Mello GT, Silva KS, Matias TS, de Assis MAA, Borgatto AF. Obesogenic clusters associated with weight status in brazilian adolescents of the movimente school-base intervention. Int J Environ Res Public Health. 2021;18(19):10350.
de Mello GT, Silva KS, da Costa RM, de Sousa ACFC, Benedet J, Del Duca GF, et al. How physical activity, diet, and sedentary behavior cluster according to age in adolescents? Sport Sci Health. 2022;18(2):499–507.
Magalhães KCS, Matias TS, Araujo RH, Werneck AO, Ferrari G, Luz LGO, et al. Clusters of obesogenic behaviors and metabolic risk according to somatic maturity status among adolescents. Am J Hum Biol. 2022;34(9): e23778.
Leech RM, McNaughton SA, Timperio A. Clustering of diet, physical activity and sedentary behaviour among Australian children: cross-sectional and longitudinal associations with overweight and obesity. Int J Obes. 2015;39(7):1079–85.
Leech RM, McNaughton SA, Timperio A. Clustering of children’s obesity-related behaviours: Associations with sociodemographic indicators. Eur J Clin Nutr. 2014;68(5):623–8.
Cameron AJ, Crawford DA, Salmon J, Campbell K, McNaughton SA, Mishra GD, et al. Clustering of obesity-related risk behaviors in children and their mothers. Ann Epidemiol. 2011;21(2):95–102.
Bell L, Ullah S, Olds T, Magarey A, Leslie E, Jones M, et al. Prevalence and socio-economic distribution of eating, physical activity and sedentary behaviour among South Australian children in urban and rural communities: baseline findings from the OPAL evaluation. Public Health. 2016;140:196–205.
Cuenca-García M, Huybrechts I, Ruiz JR, Ortega FB, Ottevaere C, González-Gross M, et al. Clustering of multiple lifestyle behaviors and health-related fitness in European adolescents. J Nutr Educ Behav. 2013;45(6):549–57.
Moreira NF, da Veiga GV, Santaliestra-Pasías AM, Androutsos O, Cuenca-García M, de Oliveira ASD, et al. Clustering of multiple energy balance related behaviors is associated with body fat composition indicators in adolescents: Results from the HELENA and ELANA studies. Appetite. 2018;120:505–13.
Bel-Serrat S, Ojeda-Rodríguez A, Heinen MM, Buoncristiano M, Abdrakhmanova S, Duleva V, et al. Clustering of multiple energy balance-related behaviors in school children and its association with overweight and obesity—WHO european childhood obesity surveillance initiative (COSI 2015–2017). Nutrients. 2019;11(3):511.
Ottevaere C, Huybrechts I, Benser J, De Bourdeaudhuij I, Cuenca-Garcia M, Dallongeville J, et al. Clustering patterns of physical activity, sedentary and dietary behavior among European adolescents: The HELENA study. BMC Public Health. 2011;11:328.
Santaliestra-Pasias AM, Mouratidou T, Reisch L, Pigeot I, Ahrens W, Mårild S, et al. Clustering of lifestyle behaviours and relation to body composition in European children. the IDEFICS study. Eur J Clin Nutr. 2015;69(7):811–6.
Uddin R, Lee EY, Khan SR, Tremblay MS, Khan A. Clustering of lifestyle risk factors for non-communicable diseases in 304,779 adolescents from 89 countries: a global perspective. Prev Med (Baltim). 2020;131: 105955.
Bel-Serrat S, Mouratidou T, Santaliestra-Pasías AM, Iacoviello L, Kourides YA, Marild S, et al. Clustering of multiple lifestyle behaviours and its association to cardiovascular risk factors in children: The IDEFICS study. Eur J Clin Nutr. 2013;67(8):848–54.
Gubbels JS, Kremers SPJ, Goldbohm RA, Stafleu A, Thijs C. Energy balance-related behavioural patterns in 5-year-old children and the longitudinal association with weight status development in early childhood. Public Health Nutr. 2012;15(8):1402–10.
Sánchez-Oliva D, Grao-Cruces A, Carbonell-Baeza A, Cabanas-Sánchez V, Veiga OL, Castro-Piñero J. Lifestyle clusters in school-aged youth and longitudinal associations with fatness: The UP&DOWN Study. J Pediatr. 2018;203:317-324.e1.
Spengler S, Mess F, Schmocker E, Woll A. Longitudinal associations of health-related behavior patterns in adolescence with change of weight status and self-rated health over a period of 6 years: Results of the MoMo longitudinal study. BMC Pediatr. 2014;14:242.
van der Sluis ME, Lien N, Twisk JWR, Steenhuis IHM, Bere E, Klepp KI, et al. Longitudinal associations of energy balance-related behaviours and cross-sectional associations of clusters and body mass index in Norwegian adolescents. Public Health Nutr. 2010;13(10 A):1716–21.
Veloso SM, Matos MG, Carvalho M, Diniz JA. Psychosocial factors of different health behaviour patterns in adolescents: association with overweight and weight control behaviours. J Obes. 2012;2012: 852672.
Wadolowska L, Hamulka J, Kowalkowska J, Kostecka M, Wadolowska K, Biezanowska-Kopec R, et al. Prudent-active and fast-food-sedentary dietary-lifestyle patterns: The association with adiposity, nutrition knowledge and sociodemographic factors in Polish teenagers—The ABC of healthy eating project. Nutrients. 2018;10(12):1988.
Iaccarino Idelson P, Scalfi L, Vaino N, Mobilia S, Montagnese C, Franzese A, et al. Healthy behaviours and abdominal adiposity in adolescents from southern Italy. Public Health Nutr. 2014;17(2):353–60.
Spengler S, Mess F, Mewes N, Mensink GBM, Woll A. A cluster-analytic approach towards multidimensional health-related behaviors in adolescents: The MoMo-Study. BMC Public Health. 2012;12:1128.
Niermann CYN, Spengler S, Gubbels JS. Physical activity, screen time, and dietary intake in families: a cluster-analysis with mother-father-child triads. Front Public Health. 2018;6:276.
Teh CH, Teh MW, Lim KH, Kee CC, Sumarni MG, Heng PP, et al. Clustering of lifestyle risk behaviours and its determinants among school-going adolescents in a middle-income country: a cross-sectional study. BMC Public Health. 2019;19(1):1177.
Khan A, Uddin R, Islam SMS. Clustering patterns of behavioural risk factors for cardiovascular diseases in Bangladeshi adolescents: a population-based study. Health Policy Technol. 2019;8(4):386–92.
Mandic S, Bengoechea EG, Coppell KJ, Spence JC. Clustering of (Un)Healthy behaviors in adolescents from Dunedin. New Zealand Am J Health Behav. 2017;41(3):266–75.
Kerkadi A, Al Mannai H, Saad D, Yakti FAZ, Attieh G, Bawadi H. Clustering of lifestyle risk factors among algerian adolescents: comparison between urban and rural areas: Gshs data. Int J Environ Res Public Health. 2021;18(13):7072.
Long KQ, Ngoc-Anh HT, Phuong NH, Tuyet-Hanh TT, Park K, Takeuchi M, et al. Clustering lifestyle risk behaviors among Vietnamese adolescents and roles of school: a Bayesian multilevel analysis of global school-based student health survey 2019. Lancet Reg Health West Pac. 2021;15: 100225.
Elsenburg LK, Corpeleijn E, van Sluijs EMF, Atkin AJ. Clustering and correlates of multiple health behaviours in 9–10 year old children. PLoS ONE. 2014;9(6): e99498.
Rodenburg G, Oenema A, Pasma M, Kremers SPJ, van de Mheen D. Clustering of food and activity preferences in primary school children. Appetite. 2013;60(1):123–32.
Yang-Huang J, van Grieken A, Wang L, Jansen W, Raat H. Clustering of sedentary behaviours, physical activity, and energy-dense food intake in six-year-old children: Associations with family socioeconomic status. Nutrients. 2020;12(6):1722.
Pereira S, Katzmarzyk PT, Gomes TN, Borges A, Santos D, Souza M, et al. Profiling physical activity, diet, screen and sleep habits in Portuguese children. Nutrients. 2015;7(6):4345–62.
López-Gil JF, Brazo-Sayavera J, García-Hermoso A, de Camargo EM, Yuste Lucas JL. Clustering patterns of physical fitness, physical activity, sedentary, and dietary behavior among school children. Child Obes. 2020;16(8):564–70.
Schröder H, Bawaked RA, Ribas-Barba L, Izquierdo-Pulido M, Roman-Viñas B, Fíto M, et al. Cumulative effect of obesogenic behaviours on adiposity in spanish children and adolescents. Obes Facts. 2018;10(6):584–96.
Khoshhali M, Heidari-Beni M, Qorbani M, Heshmat R, Motlagh ME, Ziaodini H, et al. Assoziation der Häufung von ungesunden Lebensgewohnheiten mit dem wahrgenommenen und tatsächlichen Gewichtsstatus von Kindern und Jugendlichen. Aktuel Ernahrungsmed. 2021;46(2):87–94.
Watts P, Buck D, Netuveli G, Renton A. Clustering of lifestyle risk behaviours among residents of forty deprived neighbourhoods in London: Lessons for targeting public health interventions. Journal of Public Health (United Kingdom). 2015;38(2):308–15.
Al-Nakeeb Y, Lyons M, Dodd LJ, Al-Nuaim A. An investigation into the lifestyle, health habits and risk factors of young adults. Int J Environ Res Public Health. 2015;12(4):4380–94.
Leech RM, Mcnaughton SA, Timperio A. The clustering of diet, physical activity and sedentary behavior in children and adolescents: a review. Int J Behav Nutr Phys Act. 2014;11(1):1–9.
Gubbels JS, van Assema P, Kremers SPJ. Physical activity, sedentary behavior, and dietary patterns among children. Curr Nutr Rep. 2013;2(2):105–12.
Mutz DC, Roberts DF, van Vuuren DP. Reconsidering the displacement hypothesis: television’s influence on children’s time use. Communic Res. 1993;20(1):51–75.
Pearson N, Braithwaite RE, Biddle SJH, van Sluijs EMF, Atkin AJ. Associations between sedentary behaviour and physical activity in children and adolescents: a meta-analysis. Obes Rev. 2014;15(8):666–75.
Hobbs M, Pearson N, Foster PJ, Biddle SJH. Sedentary behaviour and diet across the lifespan: an updated systematic review. Br J Sports Med. 2015;49(18):1179–88.
Halford JCG, Boyland EJ, Hughes G, Oliveira LP, Dovey TM. Beyond-brand effect of television (TV) food advertisements/commercials on caloric intake and food choice of 5-7-year-old children. Appetite. 2007;49(1):263–7.
Coon KA, Goldberg J, Rogers BL, Tucker KL. Relationships between use of television during meals and children’s food consumption patterns. Pediatrics. 2001;107(1): e7.
Temple JL, Giacomelli AM, Kent KM, Roemmich JN, Epstein LH. Television watching increases motivated responding for food and energy intake in children. Am J Clin Nutr. 2007;85(2):355–61.
Tremblay MS, LeBlanc AG, Kho ME, Saunders TJ, Larouche R, Colley RC, et al. Systematic review of sedentary behaviour and health indicators in school-aged children and youth. Int J Behav Nutr Phys Act. 2011;8(1):1–22.
Brage S, Wedderkopp N, Ekelund U, Franks PW, Wareham NJ, Andersen LB, et al. Features of the metabolic syndrome are associated with objectively measured physical activity and fitness in Danish children: the European Youth Heart Study (EYHS). Diabetes Care. 2004;27(9):2141–8.
Park JH, Moon JH, Kim HJ, Kong MH, Oh YH. Sedentary lifestyle: overview of updated evidence of potential health risks. Korean J Fam Med. 2020;41(6):365–73.
Vereecken CA, Inchley J, Subramanian SV, Hublet A, Maes L. The relative influence of individual and contextual socio-economic status on consumption of fruit and soft drinks among adolescents in Europe. Eur J Public Health. 2005;15(3):224–32.
Sallis JF, Prochaska JJ, Taylor WC. A review of correlates of physical activity of children and adolescents. Med Sci Sports Exerc. 2000;32(5):963–75.
Zhang P, Lee JE, Stodden DF, Gao Z. Longitudinal trajectories of children’s physical activity and sedentary behaviors on weekdays and weekends. J Phys Act Health. 2019;16(12):1123–8.
The Health and Social Care Information Centre. National Child Measurement Programme: England, 2021/22 Year. https://digital.nhs.uk/data-and-information/publications/statistical/national-child-measurement-programme. Accessed 5 Jul 2023.
Kipping RR, Howe LD, Jago R, Campbell R, Wells S, Chittleborough CR, et al. Effect of intervention aimed at increasing physical activity, reducing sedentary behaviour, and increasing fruit and vegetable consumption in children: active for Life Year 5 (AFLY5) school based cluster randomised controlled trial. BMJ. 2014;348:g3256.
Althubaiti A. Information bias in health research: Definition, pitfalls, and adjustment methods. J Multidiscip Healthc. 2016;9:211–7.
Acknowledgements
We would like to thank Justine Anthony and Amber Guest at Loughborough University, UK for helping with electronic searches, and Henrietta Graham for helping with risk of bias assessment.
Funding
None.
Author information
Authors and Affiliations
Contributions
NA, NP, and LS designed the protocol. NA screened all electronic searches, extracted data, assessed risk of bias and drafted the manuscript. NP screened electronic searches and resolve any conflicts. LS screened electronic searches. NP, LS, and PG discussed the draft paper with NA and provided written comments and edits. All authors critically revised the final manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Alosaimi, N., Sherar, L.B., Griffiths, P. et al. Clustering of diet, physical activity and sedentary behaviour and related physical and mental health outcomes: a systematic review. BMC Public Health 23, 1572 (2023). https://doi.org/10.1186/s12889-023-16372-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12889-023-16372-6