
Abstract
Background
While it is known that educational inequalities in smoking start during early and middle adolescence, it is unknown how they further develop until adulthood. The aim of this article is to map, in the Portuguese context, how educational inequalities in smoking emerge from pre-adolescence until young adulthood.
Methods
This study used longitudinal data from the EPITeen Cohort, which recruited adolescents enrolled in schools in Porto, Portugal. We included the 1,038 participants followed at ages 13 (2003/2004), 17, 21, and 24 years. We computed the odds ratio (OR) for the prevalence of smoking states (never smoking, experimenter, less-than-daily, daily and former smoker) and the incidence of transitions between these states, as function of age and education, stratified by sex. We also added interaction terms between age and education.
Results
Educational inequalities in daily smoking prevalence, with higher prevalence among those with lower educational level, emerged at 17 years old and persisted until higher ages. They were formed in a cumulative way by the increased risk of experimenting between 13 and 17 years, and increased risk of becoming daily smoker between 17 and 21 years. The incidence of smoking cessation was higher among the higher educated. Inequalities were formed similarly for women and men, but with lower level and showed no significance among women.
Conclusions
These results highlight that actions to prevent smoking should also take in account the potential impact in smoking inequalities, and should focus not only on middle adolescence but also on late adolescence and early adulthood.
Similar content being viewed by others

Introduction
Despite the notable progress in tobacco control, smoking is still an important issue worldwide. Although smoking rates fell 15% globally, from 2007 to 2017, currently, 1.1 billion people smoke, and at least 40% have already attempted to quit [1]. However, the use of tobacco is not uniformly distributed across the population strata.
Socioeconomic inequalities in smoking are often described, with most studies reporting a strong association between education and smoking [2]. Less educated men are more likely to smoke in most countries worldwide, while this gradient is less marked among women [3, 4]. The educational differences have generally been widening in recent decades, mainly due to a larger decline in smoking prevalence among the higher educated [5]. Even now, educational inequalities in smoking contribute substantially to inequalities in mortality [6].
Smoking usually starts before the age of 18, with 15% of smokers starting before 15 years old [7]. Educational differences in smoking are already observed among adolescents, although with differences across considered birth cohorts, sexes, and countries [8]. Smoking is more common among early adolescents (ages 10–14) and late adolescents (ages 15–21) whose parents have lower educational levels [9], and especially among adolescents with lower personal educational levels [10, 11]. Gradients have been found to persist until early adulthood (21–24 years old), with higher prevalence of ever-smoking among the lower educated compared to the higher educated [12].
Although educational inequalities in smoking are found to appear during adolescence, there is still uncertainty regarding the specific ages at which most of these educational inequalities emerge. A precise identification of the most important ages and corresponding smoking transitions is important for targeting interventions addressing those inequalities. For example, interventions focused exclusively on secondary schools might miss opportunities if most of inequalities in smoking are formed at about 17 years or older.
Two studies have described the emergence of educational inequalities across adolescence and early adulthood. One of them, a 10-year longitudinal study in the United States, found evidence that inequalities begin in early adolescence, around 12–14 years old, and widen thereafter [13]. A study among adolescents born in 1970 in Britain found relatively stable inequalities between 16 and 26 years old. These inequalities emerged from persistent inequalities in smoking initiation up to 26 years old, while there were no inequalities in smoking cessation until that age [14]. Beyond those two longitudinal studies, other have investigated the emergence of educational inequalities using retrospective questions about smoking initiation and/or cessation. Those studies suggested that educational differences in smoking emerged during adolescence and widened until early adulthood [8, 15]. Recall bias might be a problem in these studies, since the participants may not remember accurately the timing of events. Longitudinal studies limit the risk of recall bias by instead presenting the questions at the time participants join the study.
The aim of this study is to add to the existing body of literature, using a longitudinal study that allows an accurate assessment of how educational inequalities in smoking evolve from early adolescence until young adulthood. This is of crucial importance since they would be a marker of cumulative socioeconomic disadvantage in health later in live. Given the usual differences on smoking patterns between men and women in Portugal, the analysis is stratified by sex.
Materials and methods
Study design and population
This study uses a sample comprising adolescents from the Epidemiological Health Investigation of Teenagers in Porto, Portugal (EPITeen). The study’s methods are already described elsewhere [16] and summarized here. The information was obtained through self-administered questionnaires. The participants were followed across four waves: 2003/2004, 2007/2008, 2011/2013, and 2014/2015; being on average 13 years old, 17 years old, 21 years old, and 24 years old, at the respective waves. In the first wave, all adolescents born in 1990 and enrolled in public and private schools in Porto were invited to participate (2,786). Of those, 2,159 agreed to participate (77.5%). In the second wave, 1,716 participants (79.5%) were re-evaluated, and a further 783 adolescents were newly included into the cohort as they moved to the schools of Porto. In the third and fourth study waves, 1,764 and 1,094 participants were re-evaluated, respectively. We considered only those who had participated in at least three of the four waves, including the last wave. The final sample was composed of 1,038 individuals. The attrition rate in this study was 39%.
The EPITeen Cohort was approved by the Portuguese Commission for Data Protection, and the Ethics Committees of Hospital S. João and of Instituto de Saúde Pública da Universidade do Porto (ISPUP). Written informed consent was obtained from parents and adolescents in the first and second waves, and from participants in the remaining waves. The study met the guidelines for protection of human subjects concerning their safety and privacy.
Measures
For each wave, we computed smoking prevalence rates. Respondents were classified as never smokers (never experienced cigarette smoking until that wave), ever experimenters (have experimented with smoking at some point, but have not smoked regularly until that wave), less-than-daily smokers (smoked cigarettes at the time of that wave, but less-than-daily), daily smokers (smoked cigarettes daily at the time of that wave), and former smokers (reported smoking daily or less-than-daily in the past wave, but no longer smoked at the time of that wave).
Incidence rates were calculated based on the transition in smoking states between the waves. For each wave we used the data to measure the incidence rates of experimenting (number of new experimenters in that wave as a proportion of the non-smokers in the previous wave), less-than-daily smoking (number of new less-than-daily smokers in the wave as proportion of those who did not smoke, experimented smoking, smoked daily, or had quit smoking in the previous wave), daily smoking (number of new daily smokers in the wave among those who do not smoke, experimented smoke, smoked less-than-daily, or had quit smoking in the previous wave), and former smoking (number of new former smokers in the wave amongst those who smoked daily or less-than-daily in the previous wave). As a result, events between the waves were not considered.
For the participants with no information about smoking status in one of the three first waves, we re-constructed the tobacco history using the age of smoking initiation as reported in the next wave, by taking in consideration both the age of smoking initiation and the smoking status reported in the following waves (more detail in appendix 2). We performed a sensitivity analysis in which we repeated the estimations for original variables without the information given by the age of smoking initiation. There were no noteworthy changes in the results, except that 95% confidence intervals were wider (appendix 3).
We measured acquired education in young adulthood based on the completed level of education of the participant in the last wave. We distinguished between high education (university degree or tertiary education) and low education (otherwise). We considered the highest degree completed for those participants who were still enrolled in school at the time of the last wave(34.8%).
Statistical analysis
We modelled whether the smoking behaviour was associated with educational attainment, in two steps.
We computed the prevalence and incidence of smoking, using generalized estimating equation (GEE) models with a binomial distribution and an identity link, with fixed effects for survey year, and interaction terms for age with education. We stratified the analysis by sex. This method was chosen since we were modelling longitudinal binary outcome variables for never smoker, experimenter, smoke less-than-daily, smoke daily, and former smoker (yes = 1 and no = 1). GEE is a method designed to model longitudinal data across time within the same individual, and it is usually used with non-normal data, such as binary data. It allowed us to make inferences about the population, accounting for the within-subject correlation. To fit a model, we must specify both the family and the link function [17]. We used this method to graph the evolution of the marginal effects for prevalence and incidence rates.
We also computed the prevalence and incidence of smoking, as function of education and age, stratified by sex, using GEE assuming a binomial distribution and a logit link. This method allowed us to compute the odds ratio for longitudinal binary response data [17]. We repeated this procedure, adding interactions for age with education.
All analyses were conducted in Stata version 13.0, using xtgee command.
Results
The number of participants was 1,038, 49.3% of which were men. Most respondents were never smokers at 13 years old: 81.3% among boys and 75.1% among girls (Table 1). This prevalence fell to 19.5% and 29.7% among 24-year-old men and women, respectively. From the 13 years old to the 24 years old, the percentage of daily smokers increased from 0.2 to 32.6% among men, and from 1.0 to 20.5% amongst women. The incidence of experimentation increased between 13 and 21 years old, from 17.2 to 35.5% among men, and from 23.0 to 28.8% among women. The incidence of daily smoking increased greatly between 17 and 21 years old, reaching 22.5% amongst men and 17.3% among women.
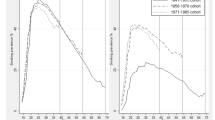
Figure 1 presents the prevalence and incidence of smoking among men. Inequalities in the prevalence of never smoking were present at all ages. There was an increased risk of experimenting between 13 and 17 years old among the lower educated. Regarding daily smoking, inequalities emerged at 17 years old and persisted.

Trends in the prevalence and incidence of smoking among men by education level (EPITeen cohort 2003, 2007, 2011, and 2014)
Legend: Marginal effects for each age given the education category, from the generalized estimation equation
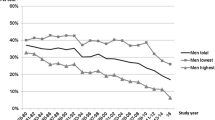
Among women (Fig. 2), inequalities in the prevalence of never smoking were present at all ages. Inequalities in daily smoking prevalence emerged at 17 years old and persisted. The lower educated were more likely to experiment until 17 years old and to be daily smokers at all ages after 17 years old.

Trends in the prevalence and incidence of smoking among women by education level (EPITeen cohort 2003, 2007, 2011, and 2014)
Legend: Marginal effects for each age given the education category, from the generalized estimation equation
Estimates based on regression analyses are presented in Table 2 (prevalence) and Table 3 (incidence). Regarding prevalence, higher educated men were more likely to be never smokers at all ages (Odds Ratio (OR) was 1.63 [1.19; 2.24]); the differences were greatest at 17 years old (OR for the interaction age/education was 1.52 [1.00; 2.30]) (Table 2). The inequalities in daily smoking prevalence existed at all ages among men (OR = 0.62 [0.46; 0.82], being more noticeable at 17 years old (OR for the interaction with 17 years and education was 0.42 [0.21; 0.85]). Among women, the higher educated were more likely to be never smokers at all ages (OR = 1.63 [1.19; 2.24]), and the differences were greatest at 17 years old (OR for the interaction was 1.48 [1.02; 2.14]). The higher educated women were less likely to experiment at 17 years old (OR for the interaction was 0.60 [0.38; 0.95]. Higher educated women were less likely to be daily smokers at all ages (OR = 0.49 [0.35; 0.69]).
The incidence of daily smoking (Table 3) was higher among low educated men at all ages (OR = 0.68 [0.49; 0.93]); and the differences were higher for 13–17 years old (OR for the interaction was 0.22 [0.08; 0.64]). Among women, the differences in smoking incidence according to education were not significant.
Discussion
Key results
This article sought to map how educational inequalities in smoking evolve from pre-adolescence until young adulthood, using a Portuguese longitudinal study. We found that inequalities in daily smoking prevalence emerged at 17 years old and persisted until higher ages. They were formed in a cumulative way by the increased risk of experimenting between 13 and 17 years, and increased risk of becoming daily smoker between 17 and 21 years. Inequalities were formed along similar pathways for women and men, but with lower level and showed no significance among women.
Potential limitations
The use of a longitudinal study design allows us to observe the trends of inequalities from adolescence into early adulthood. However, some potential problems should be considered. First, this design is subject to attrition over time (with a 39% attrition rate), which might result in a selective study population.
Second, the percentage of persons that had at least one missing answer about smoking in at least one survey was 38% (either because they refused to answer or because they were not included in that specific wave). We aimed to overcome this problem by using the age of smoking initiation and the age of trying the first cigarette indicated in the next wave, in order to create a smoking history for participants lacking one response in the first three surveys. The sensitivity analyses (not shown for the sake of brevity) allow us to conclude that the strategy did not significantly affect the results.
Third, around 35% of the participants were still enrolled in education at the time of the last questionnaire (24 years old), and were classified according to the highest completed education instead of the currently attended education. This potential misclassification might result in an underestimation of the differences in smoking between the participants with high versus low education.
Interpretation of results
We may question how smoking in adolescence is linked to education achieved in young adulthood. A possible explanation is unobserved heterogeneity, which means that there are some underlying causes affecting simultaneously the early smoking behaviour and the pathways to educational attainment. For example, people with greater future orientation may be more willing to invest in education and might be more inclined to protect themselves from the health hazards of smoking [18]. Another example is educational and societal aspirations, since they will influence future academic achievement and have been previously associated with smoking in adolescence and adulthood [19]. Also, cognitive functioning influences how information is perceived, while potentially interfering with the perception of smoking hazards [18].
We found a higher incidence of experimentation between 13 and 17 years old by those with lower education. This association might have different explanations. For example, adolescents with negative school experiences might be more prone to relate themselves with deviant groups that are more likely to smoke [20] and they may initiate smoking in order to cope with higher school pressure and demands [21]. In addition, restrictions on sales to minors might be more weakly enforced in the poorest communities. Weak enforcement of sales-related policies in Portugal facilitate adolescents’ access to cigarettes and increased visibility of smoking [22].
The results also showed that young adults with lower academic achievement were more likely to become daily smokers, compared to the ones with higher academic achievement. This might be explained by the fact that the young adults starting a job have their own money, also they are more exposed to smoking co-workers, or their peers, which make them more likely to reinforce their smoking habits [23]. Another explanation is that those attaining highest education levels are more likely tend to quit after experimenting, and avoid becoming addicted [15].
The inequalities in smoking incidence emerged before the age of 18 among men, while among women, the inequalities in smoking emerged and widened across all age ranges, although not significantly. Our results suggest that relevant transitions to adulthood may differ across sex, for example due to cultural norms regarding smoking. In addition, this difference could also reflect that Portuguese women are at an earlier stage of the smoking epidemic, with more marked initiation among low educated women across all ages [24]. It is important to reinforce that the lack of statistical significance in women is not due to a lack of power, since the prevalence of tobacco use is similar in men and women over the waves.
Previous studies have showed that socioeconomic inequalities in adolescent smoking are associated to family background and indicators of their perceived family socioeconomic status [25]. Additionally, evidence suggests that the transmission of smoking behaviour between parents and their children is likely to be consistent across social strata, but parental smoking habits are usually socioeconomically patterned [26]. Therefore, parental smoking influence could potentially contribute to the perpetuation of socioeconomic disparities in smoking. While our objective was not to explore the role of parental smoking and socioeconomic status in their children’s smoking, we acknowledge that these factors may be significant contributors to smoking inequalities among offspring, and future studies could investigate their role.
Conclusions
Inequalities in smoking were formed in a cumulative way, from adolescence to early adulthood, by the increased risk of experimenting between 13 and 17 years, and increased risk of becoming daily smoker between 17 and 21 years, among those with lower educational levels. These results highlight that the initiatives to prevent smoking should also take in account the potential impact in smoking inequalities, and should focus not only on middle adolescence but also on late adolescence and early adulthood. Also, given that most research to date has been focussed on early and middle adolescence, our results stress the need for additional research on inequalities in smoking initiation in late adolescence and early adulthood. Declarations.
Data Availability
The datasets analysed during the current study are not publicly available, since it could compromise research participant privacy, but are available from the corresponding author on reasonable request, and with permission of EPIUnit - Institute of Public Health, University of Porto.
Abbreviations
- ISPUP:
-
Instituto de Saúde Pública da Universidade do Porto
- GEE:
-
Generalized Estimating Equation Models
- OR:
-
Odds Ratio
- 95%CI:
-
95% Confidence Intervals
- NE:
-
Could not be estimated due to small number of participants at risk
References
World Health Organization. WHO report on the global tobacco epidemic, 2019: offer help to quit tobacco use. World Health Organization. 2019. 157 p.
Schaap MM, Kunst AE. Monitoring of socio-economic inequalities in smoking: learning from the experiences of recent scientific studies. Public Health. 2009 Feb;123(2):103–9.
Bosdriesz JR, Mehmedovic S, Witvliet MI, Kunst AE. Socioeconomic inequalities in smoking in low and mid income countries: positive gradients among women? Int J Equity Health. 2014 Feb 6;13(1).
Hu Y, van Lenthe FJ, Platt S, Bosdriesz JR, Lahelma E, Menvielle G et al. The impact of Tobacco Control Policies on Smoking among socioeconomic groups in nine european countries, 1990–2007. Nicotine Tob Res 2016 Aug 16;ntw210.
Bricard D, Jusot F, Beck F, Khlat M, Legleye S. Educational inequalities in smoking over the life cycle: an analysis by cohort and gender. Int J Public Health 2016 Jan 28;61(1):101–9.
Gregoraci G, van Lenthe FJ, Artnik B, Bopp M, Deboosere P, Kovács K et al. Contribution of smoking to socioeconomic inequalities in mortality: a study of 14 European countries, 1990–2004. Tob Control. 2017 May 1;26(3):260 LP – 268.
European Comission. Special Eurobarometer 458: attitudes of Europeans towards tobacco and electronic cigarettes. Luxembourg: Publications Office of the European Union; 2017.
Pampel FC, Legleye S, Goffette C, Piontek D, Kraus L, Khlat M. Cohort changes in educational disparities in smoking: France, Germany and the United States. Soc Sci Med. 2015 Feb;127:41–50.
Hanson MD, Chen E. Socioeconomic status and health behaviors in adolescence: a review of the literature. J Behav Med. 2007 Jun;30(3):263–85.
Kuntz B, Lampert T. Educational differences in smoking among adolescents in Germany: what is the role of parental and adolescent education levels and intergenerational educational mobility? Int J Env Res Public Heal. 2013 Jul;10(7):3015–32.
Paavola M, Vartiainen E, Haukkala A. Smoking from adolescence to adulthood: the effects of parental and own socioeconomic status. Eur J Public Heal. 2004 Dec 1;14(4):417–21.
Huisman M, Kunst AE, Mackenbach JP. Inequalities in the prevalence of smoking in the European Union: comparing education and income. Prev Med. 2005 Jun;40(6):756–64.
Widome R, Wall MM, Laska MN, Eisenberg ME, Neumark-Sztainer D. Adolescence to Young Adulthood: when socioeconomic disparities in Substance Use Emerge. Subst Use Misuse. 2013 Dec;6(14):1522–9.
Andersson MA, Maralani V. Early-life characteristics and educational disparities in smoking. Soc Sci Med. 2015 Nov;1:144:138–47.
Pampel FC, Bricard D, Khlat M, Legleye S. Life course changes in smoking by gender and education: a cohort comparison across France and the United States. Popul Res Policy Rev. 2017 Jun;9(3):309–30.
Ramos E, Barros H. Family and school determinants of overweight in 13-year-old portuguese adolescents. Acta Paediatr 2007 Feb 1;96(2):281–6.
Hanley JA. Statistical analysis of correlated data using generalized estimating equations: an orientation. Am J Epidemiol 2003 Feb 15;157(4):364–75.
Cutler DM, Lleras-Muney A. Education and health: evaluating theories and evidence. Natl Bur Econ Res. 2006 Jul 3;12352.
Brook DW, Brook JS, Zhang C, Whiteman M, Cohen P, Finch SJ. Developmental trajectories of cigarette smoking from adolescence to the early thirties: personality and behavioral risk factors. Nicotine Tob Res 2008 Aug;10(8):1283–91.
Bryant AL, Schulenberg JE, O’Malley PM, Bachman JG, Johnston LD. How academic achievement, attitudes, and behaviors relate to the course of substance use during adolescence: a 6-Year, multiwave national longitudinal study. J Res Adolesc. 2003 Sep;13(3):361–97.
Pampel FC, Mollborn S, Lawrence EM. Life course transitions in early adulthood and SES disparities in tobacco use. Soc Sci Res. 2014 Jan;43:45–59.
Leão T, Kunst AE, Schreuders M, Lindfors P, Kuipers MA, Perelman J. Adolescents’ smoking environment under weak tobacco control: a mixed methods study for Portugal. Drug Alcohol Depend. 2019 Nov;204(107566).
Freedman K, Nelson N, Feldman L. Smoking initiation among young adults in the United States and Canada, 1998–2010: a systematic review. Prev Chronic Dis. 2011 Dec;9:E05.
Nuyts PAW, Kuipers MAG, Willemsen MC, Kunst AE. Trends in age of smoking initiation in the Netherlands: a shift towards older ages? Addiction. 2018 Mar 1;113(3):524–32.
Moor I, Kuipers MAG, Lorant V, Pförtner TK, Kinnunen JM, Rathmann K et al. Inequalities in adolescent self-rated health and smoking in Europe: comparing different indicators of socioeconomic status. J Epidemiol Community Health 2019 Jul 13;73(10):963–70.
Alves J, Perelman J, Soto-Rojas V, Richter M, Rimpelä A, Loureiro I, et al. The role of parental smoking on adolescent smoking and its social patterning: a cross-sectional survey in six european cities. J Public Health (Bangkok). 2017 May;8(2):339–46.
Acknowledgements
Not applicable.
Funding
This study received funding from the Foundation for Science and Technology – FCT (Portuguese Ministry of Science, Technology and Higher Education) Unidade de Investigação em Epidemiologia - Instituto de Saúde Publica da Universidade do Porto (EPIUnit) (UIDB/04750/2020). This study is also part of the SILNE-R project, which received funding from the European Commission (EC), Horizon2020 Program, Call PHC6-2014, under Grant Agreement no. 635056. The publication was funded by Fundação Ciência e Tecnologia, IP national support through CHRC (UIDP/04923/2020). The funding sources had no role in the study design, collection, analysis or interpretation of the data, writing the manuscript, or the decision to submit the paper for publication.
Author information
Authors and Affiliations
Contributions
AJ performed the analysis, and drafted the manuscript. All the authors contributed to the design, to the analysis of the results, provided critical feedback, and revised the manuscript. All authors have approved the final article.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The Epiteen study was approved by the Portuguese Commission for Data Protection, and the Ethics Committees of Hospital S. João and of Instituto de Saúde Pública da Universidade do Porto (ISPUP), where one of the co-authors was affiliated. The study was performed in accordance with relevant guidelines and regulations for protection of human subjects (such as the Declaration of Helsinki).
Written informed consent was obtained from parents in the first and second waves of our study, when the participants were minors. In the remaining waves of the study, informed consent was obtained directly from the participants themselves, since they were over 21 years old.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Alves, J., Perelman, J., Ramos, E. et al. The emergence of socioeconomic inequalities in smoking during adolescence and early adulthood. BMC Public Health 23, 1382 (2023). https://doi.org/10.1186/s12889-023-16182-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12889-023-16182-w