
Abstract
Background
Various nonpharmaceutical interventions (NPIs) against COVID-19 continue to have an impact on socioeconomic and population behaviour patterns. However, the effect of NPIs on notifiable infectious diseases remains inconclusive due to the variability of the disease spectrum, high-incidence endemic diseases and environmental factors across different geographical regions. Thus, it is of public health interest to explore the influence of NPIs on notifiable infectious diseases in Yinchuan, Northwest China.
Methods
Based on data on notifiable infectious diseases (NIDs), air pollutants, meteorological data, and the number of health institutional personnel in Yinchuan, we first fitted dynamic regression time series models to the incidence of NIDs from 2013 to 2019 and then estimated the incidence for 2020. Then, we compared the projected time series data with the observed incidence of NIDs in 2020. We calculated the relative reduction in NIDs at different emergency response levels in 2020 to identify the impacts of NIPs on NIDs in Yinchuan.
Results
A total of 15,711 cases of NIDs were reported in Yinchuan in 2020, which was 42.59% lower than the average annual number of cases from 2013 to 2019. Natural focal diseases and vector-borne infectious diseases showed an increasing trend, as the observed incidence in 2020 was 46.86% higher than the estimated cases. The observed number of cases changed in respiratory infectious diseases, intestinal infectious diseases and sexually transmitted or bloodborne diseases were 65.27%, 58.45% and 35.01% higher than the expected number, respectively. The NIDs with the highest reductions in each subgroup were hand, foot, and mouth disease (5854 cases), infectious diarrhoea (2157 cases) and scarlet fever (832 cases), respectively. In addition, it was also found that the expected relative reduction in NIDs in 2020 showed a decline across different emergency response levels, as the relative reduction dropped from 65.65% (95% CI: -65.86%, 80.84%) during the level 1 response to 52.72% (95% CI: 20.84%, 66.30%) during the level 3 response.
Conclusions
The widespread implementation of NPIs in 2020 may have had significant inhibitory effects on the incidence of respiratory infectious diseases, intestinal infectious diseases and sexually transmitted or bloodborne diseases. The relative reduction in NIDs during different emergency response levels in 2020 showed a declining trend as the response level changed from level 1 to level 3. These results can serve as essential guidance for policy-makers and stakeholders to take specific actions to control infectious diseases and protect vulnerable populations in the future.
Similar content being viewed by others
Introduction
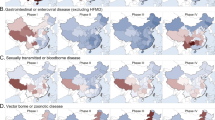
2019 novel coronavirus disease (COVID-19) has had significant and devastating impacts on socioeconomic and human health worldwide [1,2,3]. As of March 6, 2022, over 433 million confirmed cases and over 5.9 million related deaths have been reported worldwide [4]. To address the ongoing COVID-19 pandemic, various nonpharmaceutical interventions (NPIs) measures have been implemented worldwide, including wearing medical masks, maintaining safe social distances, travel restrictions, crowd bans, quarantines, isolation, and increased personal precautions [5, 6]. Several studies have explored the impact of NPIs on airborne respiratory infectious diseases during the COVID-19 pandemic [7,8,9,10,11,12,13]; the recent decrease in other notifiable infectious diseases (NIDs) indicates the cobenefits of NPIs for other NIDs as well. For instance, in Germany [14] and Switzerland [15], with the exception of tick-borne encephalitis, the caseload of all other NIDs has declined. All infectious diseases in China demonstrated a downwards trend after the implementation of NPIs, with the incidences of respiratory, gastrointestinal and enteroviral diseases decreasing more steeply than the incidences of sexually transmitted, bloodborne, vector-borne and zoonotic diseases [5]. In the Taiwan region, the cases of NIDs have also decreased dramatically, with the exception of sexually transmitted diseases [2]. Xiao et al. [1] estimated that the caseload of 39 NIDs during the emergency response in 2020 was 65.6% lower than expected in Guangdong, with the greatest reductions observed for natural focal diseases and vector-borne infectious diseases. This evidence can provide valuable references to inform public health policy on the prevention and control of infectious diseases.
Ningxia Hui Autonomous Region (referred to as “Ningxia”) is located in northwest China and is characterized by a drought-semiarid climate. It is an economically underdeveloped region. Ningxia has become an exemplar in effectively implementing NPIs and was one of the provinces with the lowest incidence rate of COVID-19 in 2020. The daily number of newly confirmed cases of COVID-19 in Ningxia fluctuated at a low level after the first confirmed case was reported in Ningxia on January 22, 2020. As of March 3, 2020, no new confirmed case has been reported, and a total of 75 confirmed cases have been reported. Most studies have focused on areas with a high prevalence of COVID-19 [1, 2]; however, few studies have investigated low-incidence areas. In addition, the impacts of NPIs on notifiable infectious diseases during the COVID-19 pandemic were inconsistent due to the variability of the disease spectrum, high-incidence endemic diseases and environmental factors across different regions [5, 6, 9]. For instance, Ningxia has a high prevalence of brucellosis. Thus, it is of public health interest to explore the influence of NPIs on notifiable infectious diseases in Yinchuan, Northwest China.
Numerous studies have revealed that meteorological and pollution factors are associated with infectious diseases (vector-borne diseases, intestinal infectious diseases, respiratory infectious diseases, etc.) [16, 17]. For instance, the literature has reported that hand, foot and mouth disease is a climate-sensitive disease, and it is positively correlated with temperature, with some day lag [18, 19]. Climate affects the intensity of this disease by impacting the maintenance and replication of the pathogen, host, and vector populations; thus, temperature and precipitation have been shown to have effects in previous studies [20]. Ambient fine particles and temperature may affect the incidence and severity of respiratory infections by affecting vectors and host immune responses [21]. Most vector-borne diseases are sensitive to variations in meteorological factors, especially ambient temperature [22]. Meteorological and pollution factors are the strongest predictors of infectious diseases, including temperature, humidity, ambient fine particles, and ozone. In addition, infectious diseases are also influenced by the development of health infrastructure [23]. Thus, to improve the prediction accuracy of the incidence of infectious diseases in Ningxia, it is essential to incorporate meteorological and pollution factors and the development of health infrastructure into the prediction model of infectious diseases.
Therefore, in this paper, we aimed to assess the impacts of NPIs against the COVID-19 outbreak in 2020 on notifiable infectious diseases by using a dynamic regression model, which takes meteorological and pollution factors and health infrastructure into consideration. We analysed the effect of NPIs against COVID-19 on the changes in NID caseloads in Yinchuan under different geographic features. The results may complement the findings of NPIs in Northwest China and be essential for public health policy-makers and stakeholders to take specific actions to control infectious diseases and protect vulnerable populations in the future.
Materials and methods
Setting and data
This study selected the provincial capital of the Ningxia region, Yinchuan, as the study site. The data for 39 NIDs were obtained from Chinese Notifiable Infectious Disease Surveillance System (CNIDSS) during 2013-2020 and were classified into three categories of infectious diseases (Class A, Class B and Class C) according to the prevalence and risk level. All Class A NIDs and some Class B NIDs with a higher risk should be reported within 2 h, while other Class B NIDs and all C NIDs should be reported within 24 h [24]. The research further divided the NIDs into five groups based on different transmission routes [1]: respiratory infectious diseases; intestinal infectious diseases; sexually transmitted or bloodborne diseases; natural focal diseases and vector-borne infectious diseases and other infectious diseases (see Table S1). Due to the excessively low number of cases of other infectious diseases, we only analysed the top four categories of infectious diseases. Monthly average temperature, monthly average relative humidity, monthly average atmospheric pressure, and monthly average wind speed were collected from the National Meteorological Information Center (http://data.cma.gov). The monthly average pollutant concentrations gathered from the China Meteorological Science data sharing service system (http://hz.hjhj-e.com/home) during the same period included data on carbon monoxide (CO), nitrogen dioxide (NO2), ground-level ozone (O3), particulate matter less than or equal to 10 μm in aerodynamic diameter (PM10), particulate matter less than or equal to 2.5 μm in aerodynamic diameter (PM2.5) and sulfur dioxide (SO2). As the government continues to invest in health infrastructure, more health institutions and personnel can provide services for local residents. Thus, we selected the annual number of health institutional personnel in Yinchuan as a proxy variable to represent the development in health infrastructure (HIP). See Table S2 for details.
NPIs
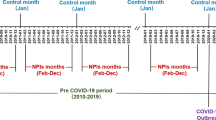
In 2020, in response to the COVID-19 pandemic, the Ningxia government initiated an emergency response to public health emergencies (from level 1 to level 3) according to the contingency plan for public health emergencies outlined in the Ningxia Hui Autonomous Region combined with the prevailing epidemic prevention and control situation [25, 26]. NPIs have been widely implemented worldwide as an important part of the public health response to outbreaks. The time frame of the emergency response levels from level 1 to level 3 for the COVID-19 outbreak in Ningxia [27, 28] is shown in Table S3.
Statistical analysis
The time series model
The autoregressive integrated moving average (ARIMA) model is a time series prediction analysis method that is widely used to predict disease-related data due to its simplicity and practicality [29]. As mentioned above, the development of infectious diseases is influenced by meteorological, pollution factors and health infrastructure. To improve the accuracy of the predicted results, we combined multiple regression analysis with time series analysis to establish the ARIMA model with exogenous variables, namely, the dynamic regression (ARIMAX) model. The ARIMAX model considered infectious diseases as the response series and the indicators of pollutants and meteorological factors as the input series. Assuming that the response series \(\{ {y_t}\} \) and the dependent variable series \(\{ {x_{1t}}\} ,\{ {x_{2t}}\} ,?,\{ {x_{it}}\} \)were smooth, the ARIMAX model was constructed as follows:
where \({y_t}\) is a response variable that denotes the monthly incidence of infectious diseases at time \( t \), \({x_{it}}\) is an independent variable that denotes the corresponding i-th meteorological and pollution factor variables (temperature, relative humidity, atmospheric pressure, wind speed, CO, NO2, O3, PM10, PM2.5 and SO2) or HIP (the same annual data of HIP are used for different months of the same year). \({\varepsilon _t}\)is the regression residual series,\(\mu \) is an average term, \({\Phi _i}\left( B \right)\)and\(\Phi \left( B \right)\)represent the autoregressive coefficient polynomials of the i-th individual variable and the residual series, respectively.\({\Theta _i}\left( B \right)\)and\(\Theta \left( B \right)\)are the moving average coefficient polynomials of the i-th individual variable and the residual series, respectively \({l_i}\) is the delayed order of the i-th individual variable and \({\alpha _t}\)is a zero-mean white noise sequence. In addition, the Akaike information criterion (AIC) value and the mean absolute percentage error (MAPE) are used to determine the best model, which includes the combination of these factors, and to assess the prediction accuracy, respectively (Figure S2 and Figure S3).
The relative reduction of NIDs
We estimated the expected number of cases according to the optimal model (1) and then calculated the actual and expected relative reduction of NIDs with the following formula [1, 5]:
where NAvg and NReal represent the average actual number of NIDs from 2013 to 2019 and the actual number of NIDs in 2020, respectively. Npred represents the predicted number of NIDs during 2020.
A positive ARR or ERR indicates a reduction in NIDs under the effect of NIPs, while a negative value denotes an increase in NIDs under the effect of NPIs. The ARR is the indicator that the crude changes in NIDs are only depicted by comparison with historical data over the same period, and the ERR is the indicator that the changes in NIDs are adjusted by the ARIMAX model with environmental factors and HIP.
In this study, we first employed the ARIMAX model with environmental factors and HIP to predict the expected number of infectious diseases in 2020, and then the relative reduction in historical average years and expected NIDs compared to actual 2020 observations was examined. Next, we further compared the relative reduction in NIDs at different emergency response levels in 2020 to identify the cobenefits of NIPs on NIDs in Yinchuan. Then, we further selected the Baidu index by using the key word “mask” [30] as a proxy of the change in public awareness under the effect of NIPs (more details of the Baidu index and the reason why we selected the word “mask” are given in the Supplement). Taking respiratory infectious disease (influenza) as an example, we entered environmental factors, HIP and public awareness into the ARIMAX model to further explore the effect of NIPs on the relative change in NIDs.
Statistical software
The ARIMAX model was conducted using R (version 4.0.4) with the packages “readxl”, “tsibble”, “TSA”, “tseries”, “fpp3” and “forecast”. A two-sided P value less than 0.05 indicated statistical significance.
Results
The change in NIDs in Yinchuan between 2013 and 2020
Figure 1 depicts the time trends of five different types of NIDs in Yinchuan city from 2013 to 2020: respiratory infectious diseases, intestinal infectious diseases and natural focal diseases and vector-borne infectious diseases exhibited clear seasonality and showed an increasing trend in recent years. Sexually transmitted or bloodborne diseases presented a swinging decline until 2016 and then stabilized. The overarching trend of overall infectious diseases was consistent with that of intestinal infectious diseases, which accounted for the largest proportion of NIDs.

The incidence trend of five categories of notifiable infectious diseases in Yinchuan, China, from 2013 to 2020
As shown in Table 1, a total of 9019 cases of NID were reported in Yinchuan in 2020, which was 42.59% lower than the average annual number of cases from 2013 to 2019. The largest reduction was observed for intestinal infectious diseases (50.62%), followed by respiratory infectious diseases (41.74%) and sexually transmitted or bloodborne diseases (31.74%), and there was an increase in natural focal diseases and vector-borne infectious diseases (-58.92%); the most common disease in each subgroup was hand, foot, and mouth disease (93.21%), scarlet fever (76.52%), hepatitis B (43.74%) and brucellosis (-77.36%), respectively.
As shown in Table 2, the variations between the expected and actual numbers of natural focal diseases and vector-borne infectious diseases presented an increasing trend. The expected relative reduction in cases of natural focal and vector-borne infectious diseases in 2020 was approximately − 46.86% (95% CI: -523.74%, 16.77%), accompanied by 207 additional cases. On the other hand, the other types of NIDs exhibited declining patterns consistent with that of total infectious diseases, i.e., a relative reduction of 50.24% (95% CI: 8.61%,65.81%). Respiratory infectious diseases exhibited the strongest decline, as the actual incidence rate of 65.27% (95% CI: 47.36%, 74.08%) was lower than the expected incidence, which indicates a reduction of 2811 cases. There were also declines in intestinal infectious diseases (58.45%, 95% CI: -35.42%, 75.46%) and sexually transmitted or bloodborne diseases (35.01%, 95% CI: -23.21%, 55.86%), with reductions of 6692 cases and 1140 cases, respectively. The most common NIDs in these subgroups were hand, foot, and mouth disease (5854 cases), infectious diarrhoea (2157 cases) and scarlet fever (832 cases), respectively (more details in Table S4).
The change in NIDs at different emergency response levels in 2020
As shown in Fig. 2, with the activation of the emergency response, all the NIDs showed different degrees of decline but differed after the response of level 2, where the actual number of respiratory infectious diseases, intestinal infectious diseases and sexually transmitted diseases or bloodborne diseases were lower than the historical average from 2013 to 2019. The opposite trend was observed for natural focal diseases and vector-borne infectious diseases. This indicated that the change in the epidemiological characteristics of the above notifiable infectious diseases may be impacts by COVID-19. Thus, NPIs against COVID-19 may have inhibitory effects against respiratory infectious diseases, intestinal infectious diseases and sexually transmitted or bloodborne diseases.

Comparison of the actual number of NIDs for different transmission routes in Yinchuan in 2020 with the synchronous period during 2015–2019
The incidences of respiratory infectious diseases, intestinal infectious diseases and sexually transmitted or bloodborne diseases decreased in general during the whole period of emergency response, but the decreases varied across different emergency response levels. Respiratory infectious diseases had the largest decrease at level 2 (53.90%), followed by level 3 (46.76%) and level 1 (33.09%). Intestinal infectious diseases had the largest decrease at level 1, followed by level 3 and level 2. For sexually transmitted or bloodborne diseases, the rate of decrease fell as the level of emergency response decreased. Compared with the four categories of NIDs above, natural focal diseases and vector-borne infectious diseases showed the opposite trend, with reduction rates ranging from 20.00% (level 1) to -79.60% (level 3) (Table 1; Fig. 3).

Actual relative reduction of notifiable infectious diseases through different transmission routes in Yinchuan during 2013–2020
Table 2 shows the analysis of the reported and expected number of NIDs in Yinchuan in 2020. The findings indicate that the expected relative reduction in 2020 demonstrated a general downwards trend from 65.64% (95% CI: -65.61%, 80.83%) in the primary response to 52.82% (95% CI: 21.06%, 66.36%) in the tertiary response, with variations among the relative reduction in NIDs across different transmission routes. The greatest reductions in intestinal infectious diseases and sexually transmitted or bloodborne diseases were observed during the level 1 response (73.28% and 65.38%, respectively), while the greatest reduction in respiratory infectious diseases was observed during the level 2 response (73.14%). The relative reduction in respiratory infectious diseases, sexually transmitted or bloodborne diseases was lower in the level 3 response than in other response periods (67.06%, 34.63%), while the reduction in intestinal infectious diseases was lowest in the level 2 response period (52.61%). However, natural focal diseases and vector-borne infectious diseases gradually increased from level 1 (21.06%) to level 3 (53.25%) (as also shown in Fig. 4). Especially for brucellosis, we found that the NPIs only had an inhibitory effect on brucellosis in Yinchuan at level 1 (14.39%), and then the inhibitory effect disappeared at levels 2 (-35.69%) and 3 (-63.92%).

Expected relative reduction of notifiable infectious diseases through different transmission routes in Yinchuan at 2020
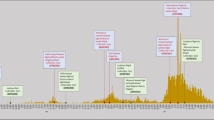
Figure 5 shows a comparison of the actual number of respiratory infectious diseases (e.g., influenza) with fitted values of different predicted models in Yinchuan in 2020. We fitted two models to predict the number of total respiratory infectious diseases and influenza with different covariates (model 1 includes meteorological factors, pollution factors and HIP, and model 2 includes meteorological factors, pollution factors, HIP and public awareness). We observed that the fitted values of model 2 were closer to the actual number of total respiratory infectious diseases and influenza than those of model 1, which further demonstrated that the NPI-induced change in public awareness may be responsible for the reduction in respiratory infectious diseases.

Comparison of the actual number of respiratory infectious diseases (influenza) with fitted values of different predicted models in Yinchuan in 2020. The red line represents the actual observed number, the gray line represents the predicted model with environmental factors, HIP and public awareness, the blue line represents the predicted model with environmental factors and HIP
Discussion
The COVID-19 pandemic has continued to affect socioeconomic [31] and behavioural [32] patterns. To address the pandemic, several NPIs have been implemented in China, and positive results have been observed [33]. However, considering the large territory and population of China, the impacts of NPIs on NIDs are not completely consistent across regions, all of which have different policies as well as meteorological and pollution factors [5]. Therefore, it is worthwhile to explore the impacts of NPIs against COVID-19 implemented in different regions on the prevention and control of other notifiable infectious diseases. This study found that there was a notable reduction in NIDs observed during the COVID-19 pandemic compared to the historical average of NIDs and the predicted caseload of NIDs in 2020, which is consistent with several studies in China [1, 2, 5]. This reduction might be attributed to the positive response of the national public health policy in all regions of the country with various forms of NPIs, such as asking people to wear masks, enhancing health awareness of the population, limitations on gatherings, and strict travel restrictions.
With further analysis of the different transmission routes of NIDs, we found that NPIs for COVID-19 exhibited certain impacts on respiratory infectious diseases, intestinal infectious diseases and sexually transmitted or bloodborne diseases, but the degree of inhibition varied in strength. The impacts on the other NIDs were reflected by the significant reduction in cases, while the impacts on natural focal diseases and vector-borne infectious diseases were not significant. Additional relevant studies [1, 2, 5, 34] suggested that this difference in effects might be attributed to the fact that the degree of impact of NPIs on NIDs has different transmission patterns.
During the COVID-19 pandemic, several respiratory infectious diseases were significantly reduced, and they were mostly transmitted through interpersonal or airborne contact, which is consistent with the transmission route of COVID-19 [35]. Thus, the protective measures of wearing masks and maintaining social distance would suppress the spread of these respiratory diseases when combating COVID-19 [36]. We observed that scarlet fever, influenza, and mumps showed different levels of morbidity at different emergency response levels: a greater decrease at response level 2 than at response level 1 and a smaller decrease at response level 3. This indicated that the NPI in 2020 may have a delayed effect on controlling infectious disease [1]. Additionally, with the lower response levels and socioeconomic restart, the increased mobility of the population may result in a rebound for the general incidence levels, but the number of these diseases was still noticeably lower compared to previous years during the high incidence of respiratory diseases in winter, which is likely due to the postponed school openings [37] and wearing of masks [38], among other measures. One interesting finding was that the NIPs induced change of public awareness may be associated with the reduction of respiratory infectious diseases.
Similar to respiratory infectious diseases, intestinal infectious diseases also showed a dramatic decrease in caseload. During the periods of strict control, massive closures of schools as well as public places reduced the opportunities for person-to-person contact [36, 39], thereby reducing the risk of foodborne infections; additionally, changes in the personal hygiene habits of the population [40] further interrupted the spread of pathogen transmission. We also observed that the incidence of HFMD significantly decreased throughout 2020; the sharpest decline in this disease was observed in the third phase of the emergency response, when most diseases rebounded, which was different from previous studies. As a childhood susceptible disease, HFMD is easily transmitted among children under 5 years of age [41],and the delayed start of kindergarten [42, 43] coincided with missing the peak of the disease epidemic, which might be the reason for the low incidence of HFMD in this region in 2020.
Compared with respiratory infectious diseases or intestinal infectious diseases, the reduction in sexually transmitted or bloodborne diseases increased dramatically in response level 1 and then rebounded more rapidly. Several reasons could be attributed to this: patients interrupted the detection and treatment of diseases with worries about COVID-19 infection [44] and limitations of strict lockdown policies [45]; additionally, the reduction of high-risk sexual behaviour effectively reduced the growth of sexually transmitted diseases such as HIV and hepatitis B [46]. Nevertheless, the rebound of reduction in disease might be the result of progressive recovery of clinical services and sexual activity levels after the gradual control of the epidemic [47].
For natural focal diseases and vector-borne infectious diseases, although the level of exposure to these diseases among the population was sharply reduced, contact with infectious vectors or hosts is the major route of zoonotic disease transmission, and several NPIs (such as wearing masks and hand washing) implemented during the routine phase of the COVID-19 pandemic had limited effects on zoonotic disease prevention and control [48]. We observed significant increase in natural focal diseases and vector-borne infectious diseases (such as brucellosis) after response level 1. There are some reasons for this increase. First, the restrictions on human mobility in level 1 inevitably reduced people’s outdoor activities and hence lowered their exposure to vectors and animal hosts of vector-borne or zoonotic diseases [5]. Second, livestock production in Ningxia is mainly focused on sheep, and the virulence of Brucella in sheep is more potent [49]. Summer and spring are the peak periods of livestock breeding, and contact between the relevant occupational personnel and the abortive products and secretions of diseased animals dramatically enhance the onset of brucellosis [50].
However, this study still had some limitations. First, the congestion of medical resources by COVID-19 and the implementation of strict community control measures might result in underreporting of some notifiable infectious diseases. Second, the data were based on Yinchuan city for the study, and some of the NIDs were merged for analysis due to the low counts. Third, the modelling data were averaged by month, which probably resulted in some biases in the prediction. Finally, the results of this study cannot prove the causal association because of the ecological study design, and the outcomes should be further examined by more rigorous studies in the future (e.g., interrupted time series).
Conclusion
The widespread implementation of NPIs in 2020 impacted the prevention and control of most NIDs, including relatively significant inhibitory effects on the incidence of respiratory infectious diseases, intestinal infectious diseases and sexually transmitted or bloodborne diseases, while the impact on natural focal diseases and vector-borne infectious diseases was limited. The relative reduction in NIDs during different emergency response levels in 2020 showed a declining trend as the response levels changed from level 1 to level 3. These results can serve as guidance for policy-makers and stakeholders to take specific actions to control infectious diseases and protect vulnerable populations in the future.
Data Availability
The datasets used and/or analysed during the current study are available from the corresponding author upon reasonable request.
References
Xiao J, Dai J, et al. Co-benefits of nonpharmaceutical intervention against COVID-19 on infectious diseases in China: a large population-based observational study. Lancet Reg Health West Pac. 2021;17:100282.
Lai CC, Chen SY, et al. The impact of the coronavirus disease 2019 epidemic on notifiable infectious diseases in Taiwan: a database analysis. Travel Med Infect Dis. 2021;40:101997.
Ciravegna L, Michailova S. Why the world economy needs, but will not get, more globalization in the post-COVID-19 decade. J Int Bus Stud. 2022;53(1):172–86.
World Health Organization. COVID-19 Weekly Epidemiological Update.[cited 2022 Mar 8].Available from: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/situation-reports
Geng MJ, Zhang HY, et al. Changes in notifiable infectious disease incidence in China during the COVID-19 pandemic. Nat Commun. 2021;12(1):6923.
Lai S, Ruktanonchai NW, et al. Effect of non-pharmaceutical interventions to contain COVID-19 in China. Nature. 2020;585(7825):410–3.
Chen AP, Chu IY, et al. Differentiating impacts of non-pharmaceutical interventions on non-coronavirus disease-2019 respiratory viral infections: hospital-based retrospective observational study in Taiwan. Influenza Other Respir Viruses. 2021;15(4):478–87.
Huh K, Jung J, et al. Impact of nonpharmaceutical interventions on the incidence of respiratory infections during the Coronavirus Disease 2019 (COVID-19) outbreak in Korea: a Nationwide Surveillance Study. Clin Infect Dis. 2021;72(7):e184–91.
Huang QS, Wood T, et al. Impact of the COVID-19 nonpharmaceutical interventions on influenza and other respiratory viral infections in New Zealand. Nat Commun. 2021;12(1):1001.
Kim DH, Nguyen TM, Kim JH. Infectious respiratory Diseases decreased during the COVID-19 pandemic in South Korea. Int J Environ Res Public Health. 2021;18(11):6008.
Hsieh CC, Lin CH, et al. The Outcome and Implications of Public Precautionary Measures in Taiwan-Declining respiratory disease cases in the COVID-19 pandemic. Int J Environ Res Public Health. 2020;17(13):4877.
Hu CY, Tang YW, et al. Public Health Measures during the COVID-19 pandemic reduce the spread of other respiratory infectious Diseases. Front Public Health. 2021;9:771638.
Kim JH, Roh YH, et al. Respiratory syncytial virus and influenza epidemics disappearance in Korea during the 2020–2021 season of COVID-19. Int J Infect Dis. 2021;110:29–35.
Ullrich A, Schranz M, et al. Impact of the COVID-19 pandemic and associated non-pharmaceutical interventions on other notifiable infectious diseases in Germany: an analysis of national surveillance data during week 1-2016-week 32-2020. Lancet Reg Health Eur. 2021;6:100103.
Steffen R, Lautenschlager S, Fehr J. Travel restrictions and lockdown during the COVID-19 pandemic-impact on notified infectious diseases in Switzerland. J Travel Med. 2020;27(8):taaa180.
Vignal C, Guilloteau E, et al. Review article: epidemiological and animal evidence for the role of air pollution in intestinal diseases. Sci Total Environ. 2021;757:143718.
Ali ST, Wu P, et al. Ambient ozone and influenza transmissibility in Hong Kong. Eur Respir J. 2018;51(5):1800369.
Tian L, Liang F, et al. Spatio-temporal analysis of the relationship between meteorological factors and hand-foot-mouth disease in Beijing, China. BMC Infect Dis. 2018;18(1):158.
Cheng Q, Bai L, et al. Ambient temperature, humidity and hand, foot, and mouth disease: a systematic review and meta-analysis. Sci Total Environ. 2018;625:828–36.
Xu L, Liu Q, et al. Nonlinear effect of climate on plague during the third pandemic in China. Proc Natl Acad Sci. 2011;108(25):10214–9.
Chen G, Zhang W, et al. The impact of ambient fine particles on influenza transmission and the modification effects of temperature in China: a multi-city study. Environ Int. 2017;98:82–8.
Wu X, Lang L, et al. Non-linear effects of mean temperature and relative humidity on dengue incidence in Guangzhou, China. Sci Total Environ. 2018;628–629:766–71.
Smith KF, Goldberg M, et al. Global rise in human infectious disease outbreaks. J R Soc Interface. 2014;11(101):20140950.
National Health Commission of the People’s Republic of China. The information reporting management of public health emergencies and epidemic surveillance of infectious diseases. [cited 2022 Sep 9]. Available from:http://www.nhc.gov.cn/wjw/c100022/202201/31c538d5c99843b5b8beb9591180444e.shtml
The Government of Ningxia Hui Autonomous Region. Emergency plan for public health emergencies in Ningxia Hui Autonomous region. [cited 2022 Sep 9]. Available from: https://www.nx.gov.cn/zwgk/qzfwj/201801/t20180115_668540.html
The Government of the People’s Republic of China. Emergency plan for public emergencies. [cited 2022 Sep 9]. Available from: http://www.gov.cn/banshi/2005-08/01/content_19023.htm
The People’s Government of Ningxia Hui Autonomous Region. Ningxia’s emergency response level has been adjusted from level 2 to level 3 since 17:00 today. [cited 2022 Jan 19]. Available from: http://www.nx.gov.cn/zwxx_11337/wztt/202005/t20200506_2056196.html
The People’s Government of Ningxia Hui Autonomous Region. Ningxia’s first-level response to major public health emergencies has been adjusted to second-level. [cited 2022 Jan 19]. Available from: http://www.nx.gov.cn/zwxx_11337/wztt/202002/t20200228_1974311.html
Box GEPJG, Reinsel GC, Ljung GM. Time series analysis: forecasting and control. John Wiley & Sons; 2015.
Baidu index. [cited 2023 Apr 12]. Available from: https://index.baidu.com/v2/index.html#/
Wei X, Li L, Zhang F. The impact of the COVID-19 pandemic on socio-economic and sustainability. Environ Sci Pollut Res Int. 2021;28(48):68251–60.
McBride E, Arden MA, et al. The impact of COVID-19 on health behaviour, well-being, and long-term physical health. Br J Health Psychol. 2021;26(2):259–70.
Tang JL, Abbasi K. What can the world learn from China’s response to covid-19? BMJ. 2021;375:n2806.
Li H, Ling F, et al. Comparison of 19 major infectious diseases during COVID-19 epidemic and previous years in Zhejiang, implications for prevention measures. BMC Infect Dis. 2022;22(1):296.
Zhang R, Li Y, et al. Identifying airborne transmission as the dominant route for the spread of COVID-19. Proc Natl Acad Sci. 2020;117(26):14857–63.
Chen S, Zhang X, et al. COVID-19 protective measures prevent the spread of respiratory and intestinal infectious diseases but not sexually transmitted and bloodborne diseases. J Infect. 2021;83(1):e37–9.
Ebrahim SH, Ahmed QA, et al. COVID-19 and community mitigation strategies in a pandemic. BMJ. 2020;368:m1066.
Rader B, White LF, et al. Mask-wearing and control of SARS-CoV-2 transmission in the USA: a cross-sectional study. Lancet Digit Health. 2021;3(3):e148–57.
Tanislav C, Kostev K. Fewer non-COVID-19 respiratory tract infections and gastrointestinal infections during the COVID-19 pandemic. J Med Virol. 2022;94(1):298–302.
The Novel Coronavirus Pneumonia Emergency Response Epidemiology T. The epidemiological characteristics of an outbreak of 2019 Novel Coronavirus Diseases (COVID-19)-China, 2020. China CDC Wkly. 2020;2(8):113–22.
Cox B, Levent F. Hand, Foot, and Mouth Disease. JAMA. 2018;320(23):2492.
Zhao Z, Zheng C, et al. Impact of the coronavirus disease 2019 interventions on the incidence of hand, foot, and mouth disease in mainland China. Lancet Reg Health West Pac. 2022;20:100362.
The Government of Yinchuan City. School opening time determined for kindergarten in Yinchuan Chinese Government. [cited 2022 Aug 1]. Available from: http://www.yinchuan.gov.cn/xwzx/mrdt/202008/t20200813_22185701.html
Latini A, Magri F, et al. Is COVID-19 affecting the epidemiology of STIs? The experience of syphilis in Rome. Sex Transm Infect. 2021;97(1):78.
Chow EPF, Hocking JS, et al. Sexually transmitted infection Diagnoses and Access to a sexual Health Service before and after the National Lockdown for COVID-19 in Melbourne, Australia. Open Forum Infect Dis. 2021;8(1):ofaa536.
Yan X, Wang X, et al. The epidemic of sexually transmitted Diseases under the influence of COVID-19 in China. Front Public Health. 2021;9:737817.
Jenness SM, Le Guillou A, et al. Projected HIV and bacterial sexually transmitted infection incidence following COVID-19-Related sexual distancing and clinical service interruption. J Infect Dis. 2021;223(6):1019–28.
Ma C, Guo X, et al. The impact of the COVID-19 pandemic on the incidence and mortality of zoonotic diseases in China. BMJ Glob Health. 2022;7(1):e007109.
Bu Y, Jiang H. Surveillance data of brucellosis in China, 2005–2016. Disease Surveillance. 2018;33(03):188–92.
Abd El-Wahab EW, Hegazy YM, et al. A multifaceted risk model of brucellosis at the human-animal interface in Egypt. Transbound Emerg Dis. 2019;66(6):2383–401.
Acknowledgements
Not applicable.
Funding
This work was supported by the National Natural Science Foundation of China (12061058) and the Ningxia Key Research and Development Project (2021BEG02026).
Author information
Authors and Affiliations
Contributions
Weichen Liu: Formal analysis, Writing original draft. Ruonan Wang: Methodology, writing review & editing. Yan Li: Project administration, resources, review & editing. Shi Zhao: Methodology, Writing-review & editing. Yaogeng Chen: Writing-review & editing. Yu Zhao: Methodology, Supervision, Writing - review & editing. All authors reviewed the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Involvement of humans
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Liu, W., Wang, R., Li, Y. et al. The indirect impacts of nonpharmacological COVID-19 control measures on other infectious diseases in Yinchuan, Northwest China: a time series study. BMC Public Health 23, 1089 (2023). https://doi.org/10.1186/s12889-023-15878-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12889-023-15878-3