
Abstract
Background
The high immune evasion ability of SARS-COV-2 Omicron variant surprised the world and appears to be far stronger than any previous variant. Previous to Omicron it has been difficult to assess and compare immune evasion ability of different variants, including the Beta and Delta variants, because of the relatively small numbers of reinfections and because of the problems in correctly identifying reinfections in the population. This has led to different claims appearing in the literature. Thus we find claims of both high and low immune evasion for the Beta variant. Some findings have suggested that the Beta variant has a higher immune evasion ability than the Delta variant in South Africa, and others that it has a lower ability.
Method
In this brief report, we re-analyse a unique dataset of variant-specific reinfection data and a simple model to correct for the infection attack rates of different variants.
Result
We find that a model with the Delta variant having an equal or higher immune evasion ability than Beta variant is compatible with the data.
Conclusion
We conclude that the immune evasion ability of Beta variant is not stronger than Delta variant, and indeed, the immune evasion abilities of both variants are weak in South Africa.
Similar content being viewed by others

Background
Rates of COVID-19 reinfections, through both immunity evasion and waning immunity, have proven difficult to assess with consistency. Nevertheless, it is crucial to understand the different immune evasion abilities of previous SARS-CoV-2 variants to help us interpret the high immune evasion ability of Omicron and future variants. Shinde et al. and Madhi et al. [1, 2] argued that previous COVID-19 infection provides little protection against reinfection by the Beta (B.1.351) variant in South Africa. Shinde et al. suggested this needs further future study and considered the outcome as preliminary results. Lack of protection was also suggested with model-based estimates of immune evasion at 63.4% for the Beta variant and 24.5% for the Delta (B.1.617.2) variant [3]. In contrast, Chemaitelly [4] demonstrated that previous infection induced strong protection against infection with the Beta variant, as high as 92.3% in Qatar. Similarly, Pulliam et al. [5] could find no evidence of immunity evasion associated with Beta and Delta variants. Because of these differences, the recent detailed household study in South Africa of Cohen et al. [6] provides helpful new details on reinfection rates of Beta and Delta variants, which we seek to re-examine with a more refined analysis.
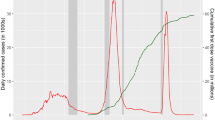
Over the study period July 2020 to August 2021, South Africa experienced three COVID-19 waves caused by the ancestral strain, the Beta variant and the following Delta variant [5, 6]. Cohen et al. found that 749 of 1200 individuals (62.4%) had at least one SARS-CoV-2 infection, and 87 of 749 (11.6%) were reinfected (including probable, possible and confirmed reinfections) [6]. However, Cohen et al. [6] did not compare the different reinfection abilities of the Beta and Delta variants. Based on Fig. 3 of Ref [6], we provide a summary of different reinfection types in Table S1 (first column). The most frequent reinfection is of the Beta-Delta type (43 occurrences), i.e., a person infected with the Beta variant later becomes infected with Delta variant. The second and third most frequent reinfection types are Ancestral-Delta type (20 occurrences) and the Ancestral-Beta type (17 occurrences). The data thus already tends to indicate that Delta leads to more reinfections than Beta, although it is difficult to be sure without a proper analysis. We made an assumption that if a seroconversion occurs in the period a variant dominates, then it is associated with an infection with the variant. This type of variant-specific data is unique to the best of our knowledge.
Method
Following [5], we correct for infection attack rate and susceptible pool size to assess immune evasion of Beta and Delta variants. This is based on the fact that the Delta variant, which arrived later, has a larger pool of previously infected it can reinfect, an effect that needs to be factored out. We denote reported cumulative infections of Ancestral (A), Beta (B), and Delta (D) variants as \({c}_{1}\), \({c}_{2}\), and \({c}_{3}\), respectively, which can be approximated by the reported cumulative infections in three time-intervals, which are bounded by the timings that the Beta variant became dominant and the Delta variant became dominant and by the end of the study, i.e., August 28, 2021 [6]. The Beta variant exceeded 50% of all samples sequenced in South Africa in the week of Oct 26, 2020 and the Delta variant in the week of June 14, 2021 [7].
We let AB represent the number of individuals infected by A and then reinfected by the B strain etc. The naïve relative frequencies of observing AB, BD and AD reinfections are \({c}_{1}{c}_{2}\): \({c}_{2}{c}_{3}\): \({c}_{1}{c}_{3}.\) But note that the relatively longer delay between A infection wave and D infection wave would mean more natural waning of protection for those previously infected with A, and thus a relatively higher frequency of AD reinfections than AB reinfection. Thus, we include a factor to the \({c}_{1}{c}_{3}\) term, i.e., \({c}_{1}{c}_{2}\): \({c}_{2}{c}_{3}\): \({bc}_{1}{c}_{3}\), where \(b\in [1, 2]\) is a reasonable first approximation [8] that we can explore. There are two cases to consider:
-
Case 1: If the immune evasion of Beta is \(\alpha\)-fold (\(\alpha \in [1, 2]\)) of the Delta variant, then the relative frequency becomes \({\alpha c}_{1}{c}_{2}\):\({c}_{2}{c}_{3}\):\({bc}_{1}{c}_{3}\).
-
Case 2: If the immune evasion of Delta is \(\alpha\)-fold (\(\alpha \in [1, 2]\)) of the Beta variant, then the relative frequency becomes \({c}_{1}{c}_{2}\):\(\alpha {c}_{2}{c}_{3}\):\({bc}_{1}{c}_{3}\).
Results
We add the 4 BB reinfections into the 17 AB infections) to obtain 21 reinfections that we term AB, caused by the Beta variant. For AB, BD and AD, the observed frequency is 21, 43, 20, and the total number of reinfections is 84. Other types of reinfections have been ignored due to low number of observed frequencies. Given the total number of reinfections is 84, the theoretical frequencies, the test statistic and p-value (\({\chi }^{2}\)-test, see supplementary SI1) can be calculated for different values of \(\alpha\). In Fig. 1, we show the p-value as function of values of alpha (y-axis) and b (x-axis).

Given the observed frequencies of different types of reinfections from Ref [6], we calculate the p-value under different hypothesized models with different value of \(\alpha ,b\) using the \({\chi }^{2}\)(chi-squared) test (see SI1). The rejection region falls in the region of “stronger Beta immune evasion” scenario
We show two curves of p-value = 0.1 and 0.05. It is very clear that the large rejection region falls in the “stronger Beta” region. A stronger Beta immune escaping (relative to Delta) conclusion is thus not supported by these data (the p-value is less than p = 0.05) On the contrary, a stronger Delta immune escaping (relative to Beta) conclusion is favored by these data. We give more explanation in the supplementary text and Table S1.
After correction for the different infection attack rates of the variants, the Delta variant still has a comparable, if not stronger, immune evasion ability than the Beta. This result conflicts with modelling estimates in Ref. [3], which conclude Beta variants have the stronger immune evasion ability.
Discussion
Our work is interesting in the way we performed a head-to-head comparison between Beta and Delta. Not only were we unable to find evidence to support a stronger immune escaping ability for Beta than Delta, but also we found Delta likely had a stronger immune escaping ability than Beta. Furthermore, if we consider the overall reinfection ratio is 11.6% after three waves of infections [6], the immune escaping ability of both Beta and Delta are weak in this household study. Pulliam et al. [5] found no immune escaping for Beta and Delta in South Africa in a large-scale data analysis. These findings are in line with [4, 9]. All these studies suggested weak immune escaping for Beta and Delta.
The studies that suggested strong immune escaping for Beta and Delta should be viewed as preliminary observations since they were not designed for the purpose of estimating immune evasion [1, 2] and/or have wide confidence intervals [3]). Dhar et al. [10] estimated “a 27.5% reinfection rate during the Delta pandemic wave in Delhi, India” which was cited by [3]. However, it was recently found that the methodology of [10] could suffer overfitting, thus the estimate is questionable [11].
We elaborate our methodology in supplementary SI1 and the data collection and limitation in SI2. In summary, we conclude that our head-to-head comparison study found Delta had a comparable if not stronger immune escaping ability than Beta in South Africa.
Availability of data and materials
Data are in the main text and from Figure 3 of Ref 6.
References
Shinde V, Bhikha S, Hoosain Z, Archary M, Bhorat Q, Fairlie L, Lalloo U, Masilela MS, Moodley D, Hanley S. Efficacy of NVX-CoV2373 Covid-19 vaccine against the B. 1.351 variant. N Engl J Med. 2021;384(20):1899–909.
Madhi SA, Baillie V, Cutland CL, Voysey M, Koen AL, Fairlie L, Padayachee SD, Dheda K, Barnabas SL, Bhorat QE. Efficacy of the ChAdOx1 nCoV-19 Covid-19 vaccine against the B. 1.351 variant. N Engl J Med. 2021;384(20):1885–98.
Yang W, Shaman J. COVID-19 pandemic dynamics in South Africa and epidemiological characteristics of three variants of concern (Beta, Delta, and Omicron). eLife. 2022;11:e78933.
Chemaitelly H, Bertollini R, Abu-Raddad LJ. Efficacy of Natural Immunity against SARS-CoV-2 Reinfection with the Beta Variant. N Engl J Med. 2021;385(27):2585–6.
Pulliam JR, van Schalkwyk C, Govender N, von Gottberg A, Cohen C, Groome MJ, Dushoff J, Mlisana K, Moultrie H: Increased risk of SARS-CoV-2 reinfection associated with emergence of Omicron in South Africa. Science 2022:eabn4947.
Cohen C, Kleynhans J, von Gottberg A, McMorrow ML, Wolter N, Bhiman JN, Moyes J, du Plessis M, Carrim M, Buys A: SARS-CoV-2 incidence, transmission, and reinfection in a rural and an urban setting: results of the PHIRST-C cohort study, South Africa, 2020–21. Lancet Infect Dis. 2022;22(6): 821–34.
CoVariants: SARS-CoV-2 Mutations and Variants of Interest. https://covariants.org
Goldberg Y, Mandel M, Bar-On YM, Bodenheimer O, Freedman LS, Ash N, Alroy-Preis S, Huppert A, Milo R: Protection and Waning of Natural and Hybrid Immunity to SARS-CoV-2. N Engl J Med. 2022;386(23):2201–12.
Hall V, Foulkes S, Insalata F, Kirwan P, Saei A, Atti A, Wellington E, Khawam J, Munro K, Cole M. Protection against SARS-CoV-2 after Covid-19 vaccination and previous infection. N Engl J Med. 2022;386(13):1207–20.
Dhar MS, Marwal R, Vs R, Ponnusamy K, Jolly B, Bhoyar RC, Sardana V, Naushin S, Rophina M, Mellan TA. Genomic characterization and epidemiology of an emerging SARS-CoV-2 variant in Delhi. India Science. 2021;374(6570):995–9.
He D, Lin L, Artzy-Randrup Y, Demirhan H, Cowling BJ, Stone L. Resolving the enigma of Iquitos and Manaus: A modelling analysis of multiple COVID-19 epidemic waves in two Amazonian cities. PNAS. 2023;120 (10):e2211422120.
Acknowledgements
None.
Funding
We were supported by the Collaborative Research Fund (Grant Number HKU C7123-20G) of the Research Grants Council (RGC) of Hong Kong, China. The funding agencies had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; or decision to submit the manuscript for publication.
Author information
Authors and Affiliations
Contributions
DH and LS conceived the study, carried out the analysis and drafted the manuscript. BC and SZ discussed the results and revised the manuscript. All authors read the manuscript and approved it for publishing.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
The data used in this study were collected originally via the public domains, and thus neither ethical approval nor individual consent was applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: Table S1.
Summary of different type ofreinfections from Ref [3].
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
He, D., Chen, B., Zhao, S. et al. The immune evasion ability of Delta variant is comparable to that of Beta variant in South Africa. BMC Public Health 23, 511 (2023). https://doi.org/10.1186/s12889-023-15431-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12889-023-15431-2