
Abstract
Background
A single anthropometric index such as stunting, wasting, or underweight does not show the holistic picture of under-five children's undernutrition status. To alleviate this problem, we adopted a multifaceted single index known as the composite index for anthropometric failure (CIAF). Using this undernutrition index, we investigated the disparities of Ethiopian under-five children's undernutrition status in space and time.
Methods
Data for analysis were extracted from the Ethiopian Demographic and Health Surveys (EDHSs). The space–time dynamics models were formulated to explore the effects of different covariates on undernutrition among children under five in 72 administrative zones in Ethiopia.
Results
The general nested spatial–temporal dynamic model with spatial and temporal lags autoregressive components was found to be the most adequate (AIC = -409.33, R2 = 96.01) model. According to the model results, the increase in the percentage of breastfeeding mothers in the zone decreases the CIAF rates of children in the zone. Similarly, the increase in the percentages of parental education, and mothers’ nutritional status in the zones decreases the CIAF rate in the zone. On the hand, increased percentages of households with unimproved water access, unimproved sanitation facilities, deprivation of women's autonomy, unemployment of women, and lower wealth index contributed to the increased CIAF rate in the zone.
Conclusion
The CIAF risk factors are spatially and temporally correlated across 72 administrative zones in Ethiopia. There exist geographical differences in CIAF among the zones, which are influenced by spatial neighborhoods of the zone and temporal lags within the zone. Hence these findings emphasize the need to take the spatial neighborhood and historical/temporal contexts into account when planning CIAF prevention.
Similar content being viewed by others

Background
In the lowest administrative units like zones and districts, health indicators such as nutrition give information that is needed to improve residents' health and to address local health concerns in susceptible geographic areas [1]. Undernutrition is one of the leading causes of death in children [1,2,3] and it is a major threat to child health. In most of the previous studies, researchers were interested in the relationship between nutrition status and place of residence [4,5,6,7,8]. Moreover, their interest in spatial variability was mainly focused on the macro levels of geography such as countries, states, regions, and cities. But studies of undernutrition at the lower administrative level (zones in our context) have great practical benefits. Besides, those previous studies generally did not account for the potential dependencies of undernutrition on both time and space [4,5,6,7,8,9,10]. In other words, temporally close periods and geographically close areal units tend to have more similar responses than those far apart [11,12,13,14]. Most of the previous studies on the prevalence of undernutrition in Ethiopia have focused on a single conventional anthropometric index of stunting, underweight, or wasting [4, 8, 15,16,17,18,19,20,21], separately proposed by the World Health Organization (WHO) [22]. However, because these traditional indices of undernutrition may overlap, a child may exhibit evidence of having two or more of these traditional measures at the same time, they are insufficient for establishing the overall true burden of undernutrition among children under the age of five [4, 16,17,18, 23,24,25,26,27,28,29]. We, therefore, developed a composite index of anthropometric failure (CIAF) which might overcome these limitations through an aggregation of the common indices of undernutrition measures [15,16,17,18, 30]. Understanding the space–time patterns and the important covariates of undernutrition in terms of the composite index for anthropometric failure (CIAF) in the under-five children in Ethiopia is important for health resource allocation-related issues, which further helps to reduce the child health disparities and inequalities. Additionally, presenting the risk of those indicators at the lower administrative (zonal) level is helpful for a spatially targeted intervention. The space–time dynamic model was used to introduce the time, space, and space–time interaction, and unobserved influencing factors, and thus provide better estimates of the relationships between undernutrition and the risk factors of known covariates [13, 14, 31,32,33]. As far as our knowledge is concerned, there is no study exploring the spatiotemporal patterns of CIAF risk in Ethiopian administrative zones. Hence, we propose a space–time dynamic model for undernutrition to estimate the space–time effects of covariates. Moreover, this study aimed to examine the patterns and identify the influencing covariates of CIAF in the Ethiopian administrative zones over the study period (2000–2016), using the EDHS data with the application of space–time dynamic models.
Methods and statistical analysis
Data for the analysis was drawn from 72 administrative zones in Ethiopia. Ethiopia is located in East Africa (Fig. 1), with a total land area of 1.1 million km2. The country has 11 national regions and 72 administrative divisions (zones).

Locations of the 72 administrative divisions (zones) of Ethiopia: a Regions; b administrative zones of the study area (Source: Authors)
The country has undertaken several economic development programs across regions and zones for eradicating undernutrition, poverty, hunger, illiteracy, and infant and maternal mortality, among others. Despite all these efforts by the concerned bodies, there are economic or poverty disparities and inequalities between the different administrative zones of Ethiopia [34]. We used the secondary Ethiopian Demographic and Health Survey (EDHS). There are several EDHS datasets and for this study, we used birth history records. A total of 30,791 children consisting of 8,765 from 2016, 9,611 from 2011, 3,850 from 2005, and 8,565 from the 2000 EDHS respectively were plausible for analysis.
Variables of the study
In this study, the zones are the spatial unit of analysis [13]. The outcome variable in this study was the proportion of CIAF for the zones [34]. Most of the previous studies on the prevalence of undernutrition in Ethiopia have focused on a single conventional anthropometric index of stunting, underweight, or wasting [4,5,6,7,8, 12, 19,20,21], separately proposed by the World Health Organization (WHO) [10]. However, these conventional indices of undernutrition may overlap so that the same child could show signs of having two or more of the indicators simultaneously; insufficient for determining the overall real burden of undernutrition situations among under-five children [5,6,7, 11,12,13,14,15,16,17,18]. The CIAF is computed by grouping those children whose height and weight were above the age-specific norm (above -2 z-scores) and those children whose height and weight for their age are below the norm and those who are experiencing one or more forms of anthropometric failure as express as B-wasting only, C-wasting and underweight, D- wasting, stunting and underweight, E- stunting and underweight, F-stunting only and Y- underweight only. The CIAF is then calculated by aggregating these six (B-Y) categories [16, 18, 27,28,29]. The choice of the covariates is guided by existing literature to study the determinants of child undernutrition in developing countries [4, 8, 10, 35]. In this paper, these explanatory variables considered in this study are also measured at the zone level. The zone-specific information on children, and households, such as the availability of improved drinking water, the percentage of literate mothers, the proportion of working mothers, and the percentage of households having access to drainage and sanitation facilities in the zones, was modeled with CIAF. The variables have been classified into the following categories: child, maternal, household, and geographic variables (Table 1).
Different studies [1,2,3,4,5] showed that children from “arid” geographic areas were associated with undernutrition. In Ethiopia, we wanted to see the impacts of the change of geographical covariates on undernutrition [3,4,5]. This is because of frequent and severe shortfalls in precipitation, and continuous rises in temperature, which may result in food insecurity, droughts, and undernutrition. Furthermore, more than three-quarters of Ethiopians depend on subsistence and rain-fed farming, livestock production that is historically linked to low crop production, and less diversified and commercial foods. Therefore we have extracted the geospatial covariates from the GPS dataset of the demographic and health survey data and this is joined with the DHS row dataset. Finally, we successfully modeled the CIAF at the zonal level by using both the EDHS and geospatial covariates.
Statistical methodology
The classical linear models estimated by ordinary least squares methods cannot take into account the fact that data collected based upon spatial and time specifications is not independent of its spatial location across different periods. If the spatial and temporal effects are neglected in the model, the estimated values will be biased [4,5,6,7,8,9,10,11, 36,37,38,39,40]. Observations available across space (N spaces) and time (T time points), a range of different model specifications need to be considered to allow different combinations of the two cases.
Let \({{\varvec{y}}}_{t}\) denote an NT \(\times\) 1 column vector of observations on the dependent variable with spatial units (i = 1,2,..., N) and temporal units (t = 1,2,..., T), X be an NT \(\times\) k matrix of observations on the covariates, and the spatial weight matrix W, which is constant over time, is the N \(\times\) N positive matrix describing the spatial arrangement of the n units whose diagonal elements are set to be zero. Each entry \({w}_{ij}\in {\varvec{W}}\) represents the spatial weight matrix associated with units i and j [38,39,40,41,42]. The elements of \({w}_{ij}\) is (i, j), which is the neighborhood matrix of the row standardized matrix with a dimension of 72 \(\times\) 72. Hence, the non-zero elements of the matrix indicate whether the two locations are neighbours. This weighted matrix is commonly expressed as:
The existence of spatial autocorrelation in the dataset is checked by using Moran’s I. The Moran’s I is used to associate weight (wij) to each of the pairs [261–265], which quantifies the spatial pattern. The test is given as follows,
where n is the number of investigated points, xi,xj the observed value of two points of interest, \(\mu\) the expected value of x, and wij the elements of the spatial weight matrix. In Moran’s I ranges [-1, 1] the value of 1 signifies that clusters with high values of the variable of interest are close to clusters with similar high values, while -1 indicates that high values are near to low values.
In this paper, the four basic spatial time dynamics models (spatial Durbin model, spatial autoregressive model, spatial error model, and general nested model with space–time), were adopted [14, 42, 43]. Let the WX be the interaction effects among the covariates with the spatial components, and the Wu the interaction effects among the error terms of different observations, \({[{\varvec{W}}{{\varvec{y}}}_{t}]}_{i}\) is the ith element of the spatial lag vector in the same period. The \({[{\varvec{W}}{{\varvec{y}}}_{t-1}]}_{i}\) is the ith element of the spatial lag vector of observations on the response variable in the previous time. When the response variable is related to the same locations as well as the neighboring locations in another period, the model is called a space–time recursive model. The \({y}_{it-1}\) is the observations on the dependent variable in the previous period. Moreover, let \(\rho\) be the spatial dependence parameter, \(\theta\) the spatio-temporal diffusion parameter, and \(\phi\) the autoregressive time dependence parameter [4,5,6,7,8,9,10,11, 36,37,38,39,40] (Fig. 2).

The space–time dynamic models. GNS: General Nesting Spatial model; SDM: Spatial Durbin Model; SAR: Spatial Autoregressive model; SEM: Spatial Error Model.
When the response variable is related to the same locations as well as the neighboring locations in another period, the model is called the space–time recursive model. The \({y}_{it-1}\) is the observations on the dependent variable in the previous period. The standard assumptions that \({\varepsilon }_{ij}\sim N(0, {\sigma }^{2})\) and \(E\left({\varepsilon }_{it}{\varepsilon }_{js}\right)=0\) for \(i\ne j\) or \(t\ne s\) apply in any case [12, 14, 36, 42, 43].
Results
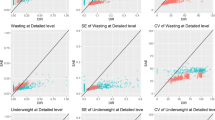
Table 2 summarizes the different measures of undernutrition status in Ethiopian children aged 0–59 months in the years 2000, 2005, 2011, and 2016. In the 2000 EDHS, 61.38% of children had one or more kinds of undernutrition (CIAF). According to established measures of undernutrition, 38.3%of children in the 2016 EDHS were stunted, 10% were wasting, and 23.3% were underweight. Moreover, around 46.49% of the children had at least one form of traditional undernutrition measures (Groups B-Y). For 2016 EDHS, the highest prevalence of undernutrition was found to be in Group F (19.47%) followed by Group E(15.76%), while Group Y was observed to be the lowest with respect to undernutrition (1.16%).
From time to time, except for stunting only, the prevalence of all anthropometric measures was declined. Moreover, the CIAF was higher than the other measures, which indicated the real burden of the child's under-nutrition status in the country. Moreover, compared with 2000 EDHS, children in the years 2005, 2011, and 2016 were associated with lower the values of CIAF by 12.4%, 23%, and 29.7% respectively (Table 2).
The data for 72 Ethiopian administrative zones were considered for four consecutive EDHS (2000, 005, 2011, and 2016) for each wave. The data of CIAF and the risk factors from the 72 administrative zones of the country were aggregated to provide zone-level summaries over time. The observed value of CIAF varied with time, and Fig. 3 shows the temporal variations in the CIAF from 2000–2016 (the higher value occurs in 2000).

Observed prevalence of CIAF at zone-level among children under five years old in Ethiopia by survey years
The observed prevalence with a 95% confidence interval which is adjusted by survey weight is shown in Fig. 3 for the 72 Ethiopian administrative zones. The observed value of CIAF generally decreased in 2016 which also showed less heterogeneity between zones, while it varied among zones in 2000, 2005, and 2011, with several zones showing high prevalence (> 50%). The zones with very high observed proportion (> 50%) included Dawuro, Wag Hemira, and Dege Habur in 2000; Amaro Special Woreda, West Wellega, and Konta special Woreda in 2005; and Yem Special Woreda, Liben, and West Wellega in 2011 (Fig. 3).
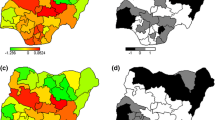
The spatial and temporal patterns of CIAF have been pictorially presented in Fig. 4. Overall, there is a great variation in the time trends across zones, suggesting inequalities and disparities in the rates of change in CIAF within the country over time. The diagram shows that all zones had the steepest improvement in CIAF over the study period. Moreover, the map suggests the existence of both spatial and temporal dependence structures in the CIAF relative risks. As can be seen from Fig. 4, by 2000 the CIAF was high in almost all zones of the country. On the other hand, the results of 2016 showed low relative risks of CIAF with less heterogeneity between zones.

The estimated relative CIAF risk in Ethiopian administrative zones from 2000 to 2016
The units of analysis were the zones, hence the results are entirely dependent on the aggregated zonal level data. The average proportion of the CIAF rate of the 72 Ethiopian zonal communities was 52%. The average percentage of mothers’ illiteracy in 72 Ethiopian zones was 73%, the average percentage of the community in the zones with no improved water and no improved toilets was 38.44% and 59.80% respectively. The coefficients of variation for urban–rural settlements, evi, dietary diversity score, wealth index, and working mothers, were high; showing wide variations among zones in Ethiopia. Significant autocorrelation was observed for both the CIAF and most of the independent covariates, indicating that CIAF and the covariates were highly spatially correlated (Table 3).
The estimated parameters of the models were given in Table 4. Different space–time dynamic models for the period between 2000–2016 were fitted, by considering both the time, space, and their interactions as well to determine the relationships between the CIAF and different levels of covariates. The result reports the estimates of the parameters with a 95% confidence interval.
The results show different spatio-temporal dynamic models of neighborhood contexts and CIAF of under-five children in Ethiopia. According to the AIC (AIC = -409.33), the lowest statistic and the higher R2 adjusted values indicated is the more appropriate statistical model, which suggests that using the general nesting space–time dynamic model is superior to other models in characterizing the undernutrition (CIAF) status of the under-five children in the 72 administrative zones in Ethiopia, as shown by the smallest values. The significant and positive temporal dependence (\(\gamma\)) indicated that past undernutrition tends to produce future sustained undernutrition status. Both the previous year and same place effects (\(\varphi\)) and the corresponding spatial parameter (\(\lambda\)) are statistically significant for the undernutrition status of the under-five children. All the covariates were standardized before the model was fitted so that the interpretation of the odds (relative risks) is expressed based on a one-standard deviation (SD) increase in the standardized covariates. The chosen dynamic model revealed significant child, household, and geographical covariates.
The coefficients from the spatial-time dynamic model indicated that zones with a higher percentage of breastfeeding are negatively associated with lower CIAF (Spatial GNS lag: B = -0.45, p < 0.001). The zones with higher percentages of a child without comorbidity are negatively associated with higher CIAF status (Spatial GNS lag: B = -0.53, p < 0.001). Moreover, zones with a higher illiteracy rate of mothers are also positively associated with higher CIAF percentages (Spatial GNS lag: B = 0.43, p < 0.001). Moreover, the regression coefficients of breastfeeding rate, minimum and above dietary diversity score rate, presence of comorbidity rate, and wealth index rate, were negative. This indicated that the variables were associated with a decrease in the incidence of undernutrition in terms of CIAF. However, the regression coefficients of the rate of women’s illiteracy, women’s low autonomy, and having no access to improved water and sanitation were positive, indicating that these factors were associated with an increase in the risk of under-five children undernutrition in the Ethiopian administrative zones (Table 4).
Discussion
Childhood undernutrition is a major public health concern in Ethiopia [4, 10, 34, 44, 45]. Undernutrition (CIAF) in Ethiopia decreased from 61.38% to 46.49% for under-five children respectively, between 2000 and 2016. Various space–time dynamics models have been used for reducing spatial autocorrelation in model residuals. Our findings identified variations in the undernutrition of children under five among the 72 administrative zones in Ethiopia over the periods from 2000 to 2016. Four spatial–temporal dynamic models were used to evaluate the relationships between the CIAF and its covariates. In the modeling process, we sought to select the best model by considering the evaluation criteria of the models such as R2 and AIC. The result showed that when the spatial weight and spatial lag weight matrix were added in the GNS model, the adjusted R2 was maximized and AIC was minimized. This result is reasonable because neighboring zones may have effects on each other through sharing similar dietary and living habits, and environmental conditions, and the like. Both the observed and model-based estimated relative risks showed a decrease of CIAF risk from 2000 to 2016 in most of the Ethiopian administrative zones which is similar to what has been reported in different countries [46,47,48, 3,4,5] . Even though overall decreasing temporal trend of CIAF in Ethiopia is encouraging, the local trends have shown apparent heterogeneity. This is due to the fact that different administrative zones have their own cultural practices towards nutrition and even the local administrators have different commitments to the implementation of rules and regulation to minimize the undernutrition. The significant socio-economic covariates were in line with studies previously conducted in different countries [4,5,6,7,8,9,10, 44, 45, 49]. Particularly, our studies revealed that the risk of having CIAF decreased with an increase in the proportion of mothers’ education, which is in line with the results of previous works [4, 5, 10, 39, 50]. This might be due to the fact that educated mothers could feed their children better, as they have more knowledge, attitude, and practices (KAP) on nutrition-rich foods and the importance of a hygienic living environment [51]. The household wealth index is also found to be strongly associated with CIAF and children from the lowest (poorest) households are considerably disadvantaged concerning the CIAF than those from rich households. This is expected since poor households have no economic power to access and afford the required nutrition-rich foods and to access healthcare services, unlike their rich counterparts. In line with our findings, the role of household wealth status in undernutrition has also been well-documented in the extant literature [4, 16, 52,53,54, 3,4,5]. Even though the CIAF risk decreased from time to time, it is still high with increased trends in several zones in Ethiopia, which should be given priority when intervention and planning are made. Besides these, the decision-makers of those zones (showing increasing/no progress of CIAF) should pay more attention to the potential causes of CIAF, and the most important control mechanisms should be undertaken. In this study, potentially, we explored a vast number of risk factors for CIAF, but other influencing unobserved or unknown heterogeneous factors in space and time dimensions may be missed.
Conclusions
The data used in this study are obtained from four waves of Ethiopian DHS. Ethiopia is located in East Africa and divided into 11 regions and 72 administrative zones. Our findings identified variations in the undernutrition of children under five among the 72 administrative zones in Ethiopia over the periods from 2000 to 2016. In this study, four space–time dynamic spatiotemporal models were used to model the relationships between the CIAF and covariates among the administrative zones in Ethiopia. This study provides meaningful information from a spatial analysis of the effects of the neighborhood contexts on the CIAF in Ethiopian 72 zones. Our empirical results revealed that the general nesting space–time dynamic model is more suitable for characterizing the dependent nature of undernutrition (CIAF) in the administrative zones over time. In summary, there exist geographical differences in CIAF in Ethiopian administrative zones, which are influenced by various neighborhood contexts. Higher breastfeeding rate, a lower percentage of comorbidity, a higher percentage of minimum and above dietary diversity, a higher percentage of literacy, and a higher percentage of BMI of women, were positively associated with higher values of CIAF. However, a higher percentage of unimproved water and a higher percentage of unimproved sanitation facilities, a low percentage of women's autonomy, a higher percentage of the employment status of women, a higher percentage of wealth index, and higher values of precipitation were positively associated with higher proportions of CIAF. There is a need to reassess the policies aimed at reducing the child malnutrition status in Ethiopia’s administrative zones.
Availability of data and materials
The dataset used for the current study is available at the DHS program repository and the shapefile of the map of Ethiopia was accessed as an open-source without restriction from open Africa 2016 https://dhsprogram.com/data/available-datasets.cfm.
References
Organization, W.H., The state of food security and nutrition in the world 2018: building climate resilience for food security and nutrition. 2018: Food & Agriculture Org.
Kumar S, Kumar N, Vivekadhish S. Millennium development goals (MDGS) to sustainable development goals (SDGS): Addressing unfinished agenda and strengthening sustainable development and partnership. Indian journal of community medicine: official publication of Indian Association of Preventive & Social Medicine. 2016;41(1):1.
Hák T, Janoušková S, Moldan B. Sustainable Development Goals: A need for relevant indicators. Ecol Ind. 2016;60:565–73.
Fenta HM, et al. Determinants of stunting among under-five years children in Ethiopia from the 2016 Ethiopia demographic and Health Survey: Application of ordinal logistic regression model using complex sampling designs. Clinical Epidemiology and Global Health. 2020;8(2):404–13.
Degarege D, Degarege A, Animut A. Undernutrition and associated risk factors among school age children in Addis Ababa. Ethiopia BMC Public Health. 2015;15(1):1–9.
Amugsi DA, Mittelmark MB, Oduro A. Association between maternal and child dietary diversity: an analysis of the Ghana demographic and health survey. PLoS ONE. 2015;10(8): e0136748.
Aheto JMK, et al. Childhood Malnutrition and Its Determinants among Under-Five Children in G hana. Paediatr Perinat Epidemiol. 2015;29(6):552–61.
Habyarimana F, Zewotir T, Ramroop S. A proportional odds model with complex sampling design to identify key determinants of malnutrition of children under five years in Rwanda. Mediterr J Soc Sci. 2014;5(23):1642–1642.
Ahmed MM, et al. Prevalence of undernutrition and risk factors of severe undernutrition among children admitted to Bugando Medical Centre in Mwanza. Tanzania BMC Nutrition. 2016;2(1):1–6.
Takele K, Zewotir T, Ndanguza D. Understanding correlates of child stunting in Ethiopia using generalized linear mixed models. BMC Public Health. 2019;19(1):1–8.
Tobler WR. A computer movie simulating urban growth in the Detroit region. Econ Geogr. 1970;46(sup1):234–40.
Sarmiento-Barbieri, I. An introduction to Spatial Econometrics in R. in University of Illinois. Available online:http://www. econ. uiuc. edu/~{} lab/workshop/Spatial_in_R. html (accessed on 7 August 2018). 2016.
Puig, F., B. García‐Mora, and C. Santamaría, The influence of geographical concentration and structural characteristics on the survival chance of textile firms. J Fashion Market Manag Int J. 2013.
Banerjee, S., B.P. Carlin, and A.E. Gelfand, Hierarchical modeling and analysis for spatial data. 2014: CRC press.
Al-Sadeeq AH, Bukair AZ, Al-Saqladi AWM. Assessment of undernutrition usingyears in rural Yemen. East Mediterr Health J. 2018;24(12):1119–26.
Nandy S, Svedberg P. The Composite Index of Anthropometric Failure (CIAF): An alternative indicator for malnutrition in young children. In: Handbook of anthropometry. Springer; 2012. p. 127–37.
Svedberg, P., Poverty and undernutrition: theory, measurement, and policy. 2000: Clarendon press.
Rasheed W, Jeyakumar A. Magnitude and severity of anthropometric failure among children under two years using Composite Index of Anthropometric Failure (CIAF) and WHO standards. Int J Pediatr Adolesc Med. 2018;5(1):24.
Kassie GW, Workie DL. Exploring the association of anthropometric indicators for under-five children in Ethiopia. BMC Public Health. 2019;19(1):1–6.
Amugsi DA, et al. Influence of childcare practices on nutritional status of Ghanaian children: a regression analysis of the Ghana Demographic and Health Surveys. BMJ Open. 2014;4(11): e005340.
Fotso J-C. Urban–rural differentials in child malnutrition: trends and socioeconomic correlates in sub-Saharan Africa. Health Place. 2007;13(1):205–23.
De Onis M, et al. Worldwide implementation of the WHO child growth standards. Public Health Nutr. 2012;15(9):1603–10.
Endris N, Asefa H, Dube L. Prevalence of malnutrition and associated factors among children in rural Ethiopia. BioMed research international. 2017;2017:6587853.
Khamis AG, et al. The burden and correlates of childhood undernutrition in Tanzania according to composite index of anthropometric failure. BMC Nutrition. 2020;6(1):1–13.
Nandy S, Miranda JJ. Overlooking undernutrition? Using a composite index of anthropometric failure to assess how underweight misses and misleads the assessment of undernutrition in young children. Soc Sci Med. 2008;66(9):1963–6.
Nandy S, et al. Poverty, child undernutrition and morbidity: new evidence from India. Bull World Health Organ. 2005;83:210–6.
Shit S, et al. Assessment of nutritional status by composite index for anthropometric failure: a study among slum children in Bankura, West Bengal. Indian J Public Health. 2012;56(4):305.
Mandal G, Bose K. Assessment of overall prevalence of undernutrition using composite index of anthropometric failure (CIAF) among preschool children of West Bengal, India. 2009.
Sen J, Mondal N. Socio-economic and demographic factors affecting the Composite Index of Anthropometric Failure (CIAF). Ann Hum Biol. 2012;39(2):129–36.
Biswas S, Giri SP, Bose K. Assessment of nutritional status by composite index of anthropometric failure (CIAF): a study among preschool children of Sagar Block, South 24 Parganas District, West Bengal. India AnthropologicAl review. 2018;81(3):269–77.
Lawson, A.B., Bayesian disease mapping: hierarchical modeling in spatial epidemiology. 2018: CRC press.
Gilks, W.R., M arkov Chain M onte C arlo. Encyclopedia of biostatistics, 2005. 4.
Breslow NE, Clayton DG. Approximate inference in generalized linear mixed models. J Am Stat Assoc. 1993;88(421):9–25.
Fenta HM, Zewotir T, Muluneh EK. Disparities in childhood composite index of anthropometric failure prevalence and determinants across Ethiopian administrative zones. PLoS ONE. 2021;16(9): e0256726.
Kassie GW, Workie DL. Determinants of under-nutrition among children under five years of age in Ethiopia. BMC Public Health. 2020;20(1):1–11.
Anselin, L., Spatial econometrics: methods and models. Vol. 4. 2013: Springer Science & Business Media.
Hao Y, Liu YM. The influential factors of urban PM2. 5 concentrations in China: a spatial econometric analysis. Journal of Cleaner Production. 2016;112:1443–53.
Duncan EW, White NM, Mengersen K. Spatial smoothing in Bayesian models: a comparison of weights matrix specifications and their impact on inference. Int J Health Geogr. 2017;16(1):1–16.
Getis A, Aldstadt J. Constructing the spatial weights matrix using a local statistic. Geogr Anal. 2004;36(2):90–104.
Fischer, M.M. and J. Wang, Spatial data analysis: models, methods and techniques. 2011: Springer Science & Business Media.
Besag J, York J, Mollié A. Bayesian image restoration, with two applications in spatial statistics. Ann Inst Stat Math. 1991;43(1):1–20.
LeSage JP, Pace RK. Spatial econometric models. In: Handbook of applied spatial analysis. Springer; 2010. p. 355–76.
Cameron, A.C. and P.K. Trivedi, Microeconometrics: methods and applications. 2005: Cambridge university press.
Akombi BJ, et al. Child malnutrition in sub-Saharan Africa: A meta-analysis of demographic and health surveys (2006–2016). PLoS ONE. 2017;12(5): e0177338.
Chirande L, et al. Determinants of stunting and severe stunting among under-fives in Tanzania: evidence from the 2010 cross-sectional household survey. BMC Pediatr. 2015;15(1):1–13.
Spray AL, et al. Spatial analysis of undernutrition of children in leogane Commune. Haiti Food and nutrition bulletin. 2013;34(4):444–61.
Simler, K.R., Nutrition mapping in Tanzania: an exploratory analysis. IFPRI Food Consumption and Nutrition Division Discussion Paper, 2006(204).
Khan J, Mohanty SK. Spatial heterogeneity and correlates of child malnutrition in districts of India. BMC Public Health. 2018;18(1):1–13.
Kejo D, et al. Prevalence and predictors of undernutrition among underfive children in Arusha District. Tanzania Food science & nutrition. 2018;6(8):2264–72.
Knorr-Held L. Bayesian modelling of inseparable space-time variation in disease risk. Stat Med. 2000;19(17–18):2555–67.
Wamani H, et al. Boys are more stunted than girls in sub-Saharan Africa: a meta-analysis of 16 demographic and health surveys. BMC Pediatr. 2007;7(1):17.
Griffiths P, et al. A tale of two continents: a multilevel comparison of the determinants of child nutritional status from selected African and Indian regions. Health Place. 2004;10(2):183–99.
Rahman MS, et al. Association of low-birth weight with malnutrition in children under five years in Bangladesh: do mother’s education, socio-economic status, and birth interval matter? PLoS ONE. 2016;11(6): e0157814.
Svefors P, et al. Stunted at 10 years. Linear growth trajectories and stunting from birth to pre-adolescence in a rural Bangladeshi cohort. PloS one. 2016;11(3):e0149700.
Acknowledgements
The datasets used in this study were obtained from the DHS program thanks to the authorization received to download the dataset on the website.
Funding
Not applicable.
Author information
Authors and Affiliations
Contributions
HMF was involved in this study from data management, data analysis, drafting, and revising the final manuscript. TZ and EKM contributed to the conception, design, and interpretation of data, as well as to manuscript reviews and revisions. All authors have read and approved the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
We used the demographic and health survey dataset. This is a secondary dataset and no need for ethical clearance. https://dhsprogram.com/data/available-datasets.cfm.
Consent for publication
Not applicable.
Competing interests
We, the authors, declare that we have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Fenta, H.M., Zewotir, T. & Muluneh, E.K. Space–time dynamics regression models to assess variations of composite index for anthropometric failure across the administrative zones in Ethiopia. BMC Public Health 22, 1550 (2022). https://doi.org/10.1186/s12889-022-13939-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12889-022-13939-7