
Abstract
Background
The ongoing Covid-19 pandemic not only threatens physical health, but also affects the mental health of people. Yet, health consequences of the pandemic do not affect all members of society equally. We therefore assessed the mental health burden of individuals who are at increased risk of severe illness from Covid-19 compared to individuals who are at low risk of severe illness during the first lockdown (March, 2020) in Germany. Furthermore, we investigated variables mediating the effect of being an individual at increased risk of serve illness on depression.
Methods
Adult German residents (n = 2.369) provided responses to a cross-sectional online survey about risk factors for of severe illness from Covid-19 and various aspects of mental health during the first lockdown in Germany. For data collection, standardized and validated self-report measures were used and for data analysis Mann-Whitney U-tests as well as regression and mediation analyses were performed.
Results
The results clearly show that the mental health burden is higher among individuals at increased risk of severe illness from Covid-19 compared to individuals at low risk of severe illness from Covid-19. Moreover, our findings indicate that the association between Covid-19 risk status and depressive symptoms is mediated by concerns about mental health, anxiety and loneliness in a causal effect chain.
Conclusions
Individuals at increased risk of severe illness from Covid-19 have an increased need for psychosocial support during times of lockdown. Future public health policies should pay special attention to these individuals and support them by targeted offers. More research, however, is needed on possible long-term consequences of social distancing on mental health.
Similar content being viewed by others

Introduction
The most recently discovered coronavirus, known as severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), has spread globally within a few months after its first identification in December 2019 [1]. The World Health Organization (WHO) declared the Covid-19 disease caused by the virus as a pandemic on March 11th 2020. In Germany, the first case of Covid-19 was confirmed on January 27th 2020 [2]. First infection clusters emerged in the federal states North Rhine-Westphalia and Bavaria throughout February 2020 [3]. Subsequently, Covid-19 cases increased rapidly, culminating in about 6016 new cases on March 16th 2020 [4]. As of June 2020, by the end of the so-called “first wave”, 183,594 persons had been diagnosed with a SARS-CoV-2 infection in Germany and the number of deaths registered in this group amounted to 8555 [5]. The cumulative rate of officially recognized Covid-19-associated hospitalizations in Germany is 10% [6].
Older people above the age of 50-60 and people with underlying medical conditions, such as heart conditions, chronic obstructive pulmonary disease (COPD), or obesity are at increased risk of severe illness from Covid-19 [7, 8]. On March 22nd 2020, the German government imposed a first lockdown to reduce infection rates and thus protect these vulnerable groups and maintain the proper functioning of the health care system. This lockdown included the closing of schools, stores, restaurants, bars, clubs, social venues and prohibited any form of mass gatherings. In addition, citizens were urged to minimized personal social contact and keep a minimum distance of 1.5 m from one another [9]. It lasted until May 4th 2020 and associated regulations were gradually eased by June 15th 2020 (see Fig. 1).

First Covid-19 lockdown in Germany. Sources: Own elaboration based on data from RKI [4]
These governmental actions aim at a reduction of social contacts. Social distancing however may be associated with a substantial mental health burden and there is evidence for an association between social isolation and (mental) health problems [10, 11]. This is also supported by recent studies showing that the Covid-19 pandemic and related regulations are associated with increases in anxiety, depression and psychological distress [12,13,14]. The increase in mental health problems may in turn also favor dysfunctional coping and emotion regulation strategies such as substance use [15]. Even though these mental health impacts of the Covid-19 pandemic may be more significant for those who are prone to psychological problems [16], previous studies have not taken into account the mental health of individuals at increased risk of severe illness from Covid-19 due to their age or underlying medical conditions [7, 8]. Individuals at risk of severe illness from Covid-19 may be more worried about their own health and therefore avoid social contacts to reduce the risk of a Covid-19 infection. Previous studies demonstrated a relationship between concern of COVID pandemic and feelings of loneliness [17, 18]. This may increase feelings of loneliness, which in turn may result in mental health problems such as depression [19].
Hence, the primary aim of the present study is the investigation of the mental health burden of individuals who are at increased risk of severe illness from Covid-19 (high risk group for Covid-19, HRGC) compared to individuals who are at low risk of severe illness (low risk group for Covid-19, LRGC). The central hypothesis is that individuals of the HRGC are more anxious and experience more depressive symptoms due to the pandemic than individuals of the LRGC. Based on associations between anxiety, depression, and substance use, we moreover expect that HRCG individuals report enhanced substance use. Furthermore, the second aim of the current study is to investigate whether the hypothesized increase in depressive symptoms in the HRGC group is mediated by concerns about own mental health, anxiety, stress and loneliness.
Methods
Study design and data collection
Cross-sectional data were collected via an online survey from June 1st 2020 until July 17th 2020. The survey was developed in LimeSurvey (LimeSurvey GmbH, Hamburg). The weblink of the survey was included in an advert that was promoted on the websites and social media platforms of several German social service organisations and associations (German AIDS Service Organisations, German Society for Social Psychiatry, German Federation of Telephone Emergency Services, German Federation for Social Work in the Healthcare System, German Society for Social Work in Addiction Aid).
To be able to participate in the study, participants had to be at least 18 years and have sufficient knowledge of the German language. Participants did not get any compensation for participating in the survey. In total, 3154 people were reached through the online survey. For this study, a subset of participants (n = 2.369) has been analysed for the comparison of the mental health burden of HRGC and LRGC participants.
Measures
The survey started with comprehensive participant information and consent forms. This introductory part was followed by 132 items on sociodemographic variables, participants’ mental health status, their perceptions of the Covid-19 pandemic and the governmental actions designed to encounter the pandemic.
Mental health
All items on mental health were part of standardized and validated self-report measures. Subscales of the German version of the Patient Health Questionnaire (PHQ-D) [20] were used to assess levels of depression (PHQ-9) (Kromke et al. 2006), anxiety (General Anxiety Disorder-7, GAD-7) [21] and somatisation (Patient Health Questionnaire-15, PHQ-15) [22]. The PHQ-9 scale assesses severity of depressive symptoms with a maximum score of 27. GAD-7 measures symptoms of anxiety with a maximum of 21. A score of 10 or above on each of the two scales points to an at least moderate major depressive episode and moderate levels of clinical anxiety [21, 23]. The items of the PHQ-15 scale include the most prevalent DSM-IV somatization disorder somatic symptoms. The total PHQ-15 scale has a maximum score of 30 and a score of 10 and above represent a moderate level of somatization [22]. The internal reliability of the PHQ-9 was with a Cronbach’s α of 0.90 similar to other studies (0.86-0.89) [23]. The internal consistency of the GAD-7 was with a Cronbach’s α = 0.91 similar to another study (0.89) [21] and of PHQ-15 with a Cronbach’s α = 0.81 equal to another study (0.82) [22].
Suicidality
Suicidality was assessed by the first item of the German version of the Suicide Behaviours Questionnaire – Revised (SBQ-R) which is acknowledged as a reliable instrument to measure suicidal risk (“Have you ever thought about or tried to take your own life?” = never (1); I had only a fleeting thought about it (2); I had at least 1 intention to kill myself, but I did not try (3); I had at least 1 intention to kill myself and I really wanted to die (3); I tried to kill myself, but I did not want to die (4); I tried to kill myself, and I really wanted to die (5)). A score of 3 and higher represents an increased risk of suicide [24, 25]. This item was complemented by a question on suicidal ideation during the first lockdown in Germany (“How often have you thought about killing yourself during the lockdown?”).
Loneliness
Emotional and social loneliness were surveyed by the 11-item De Jong Gierveld Loneliness Scale with a maximum score ranges from 0 to 22 [26]. The internal consistency of the Loneliness-Scale was with a Cronbach’s α = 0.77.
Social support
The level of social support was assessed with the help of the Oslo 3 Social Support Scale (OSSS-3). The score ranges from 3 to 14. A score of 12 and above represent a strong social support. The internal consistency of the OSSS-3 was with a Cronbach’s α = 0.66 simliar to another study (0.64) [27, 28].
Drug use
Moreover, the use of alcohol, nicotine and a range of illegal substances during the last 12 months as well as changes in substance use during the lockdown were assessed by asking the participants which substances they used in the last 12 months, respectively during the first lockdown.
To differentiate between HRGC and LRGC participants, risk factors for an increased risk of severe illness from Covid-19 were assessed by the criteria of the Robert Koch Institute [29] which include smoking, obesity, cardiovascular diseases, chronic lung diseases, diabetes mellitus, cancer, and a compromised immune system. If at least one of these criteria was met, participants were included in the HRGC group.
Statistical analysis
We used a subset of the dataset and included all participants who gave information about their Covid-19 risk profile (n = 2.369). The analyses presented here compare two groups: (i) individuals at increased risk of severe illness from Covid-19 (n = 1.136; HRGC group) and (ii) Individuals at low risk of severe illness from Covid-19 (n = 1.233; LRGC group). Data analysis was conducted using IBM SPSS Statistics 25.0 (IBM corp., Armonk, USA). Significance level of p < 0.05 was considered in all analyses.
For group comparisons Mann-Whitney U-tests were performed for ordinal and non-normally distributed data. Cohen’s d is reported as the estimated effect size for statistically significant results. The distribution of categorical variables was assessed by Chi-square tests. Spearman’s correlation coefficients were used to determine correlations between ordinal variables and non-normally distributed continuous variables. Pearson’s correlation was used for normally distributed continuous variables. Linear regression analysis was used to explore predictors for depressive symptoms. Additionally, mediation analysis using PROCESS macro [30] for SPSS 25 (IBM corp., Armonk, USA) was run to explore whether concerns about one’s own health, anxiety and feelings of loneliness mediated depressive symptoms. Multiple mediator models were performed to estimate indirect effects [31]. All analyses were based on 5000 bootstrapped samples. An indirect effect was considered significant when the 95% bias-corrected confidence interval did not include zero [30].
Results
Sample characteristics
Of the 3154 persons who commenced the survey, 2.369 participants completed questions on Covid-19 risk factors (75.11%). 47% (n = 1291) of those participants were classified into the HRGC. Data of non-completers were included on a pairwise basis, resulting in a different number of responses per analysis (for details on the sociodemographic characteristics of the HRGC and the LRGC, see Table 1).
Mental health measures
In total, 30.9% of the participants of both groups reported symptoms of a moderate depression on the PHQ-9 scale (score of 10 or higher). The median PHQ-9 score was significantly higher in the HRGC than in the LRGC group. 35.6% of the HRGC participants and 26.6% of the LRGC participants had a PHQ-9 score of 10 or higher and, therefore, exhibited moderate depressive symptoms. Compared to the LRGC, the median GAD-7 score of the HRGC was also significantly higher. Here, 29.6% of the HRGC participants and 21.4% of the LRGC participants showed at least moderate levels of generalized anxiety disorders (GAD-7 score ≥ 10). A similar pattern applies to somatic symptoms. The median PHQ-15 score was again significantly higher in the HRGC than in the LRGC group. 15,6% of the HRGC participants and 7.6% of the LRGC participants exhibited at least moderate somatic symptoms (PHQ-15 score ≥ 10). In total, 14.4% of the participants showed an elevated risk for suicide (SBQ-R Item 1 ≥ 3). Again, an elevated risk for suicide was significantly higher in the HRGC than in the LRGC (19.5% vs. 9.7%) group. The same results can be found for the median suicidal ideation during the lockdown (see Table 2).
Substance use during lockdown
There were no significant differences between the HRGC and the LRGC group for alcohol use during the lockdown. In contrast, the use of nicotine and THC during the lockdown differed significantly between the two groups. 20.1% of the HRGC reported an increased use of nicotine during the lockdown compared to 6.1% of the LRGC participants. An increased use of THC during the lockdown was reported by 6.7% of the HRGC individuals compared to 2.1% of the LRGC participants (see Table 3).
Loneliness, social support and professional assistance
Loneliness was significantly higher in the HRGC group compared to the LRGC (7.3% vs. 3.8%). The level of perceived social support did not differ significantly between both groups (see Table 4).
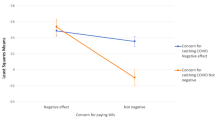
Feelings of stress associated with social distancing did not differ significantly between both groups. HRGC individuals, however, were significantly more likely to perceive government actions to encounter Covid-19 as legitimate and meaningful than LRGC participants. Generally, HRGC individuals were significantly more concerned about the pandemic than LRGC participants. Here, HRGC individuals were significantly more worried about their own health, the health of their friends, the health system in Germany, their financial situation as well as the German economic and political system than LRGC participants (see Table 4).
Factors contributing to depressive symptoms during the lockdown
Bivariate correlations showed a significant positive association between depression, anxiety, loneliness and the perceived stress level due to social distancing (see Table 5).
Linear regression was used to identify predictors of depressive symptoms during the lockdown. Being male (β = −.025, p = .044), younger age (β = −.041, p = .001), being a HRGC individual (β = .052, p < .001), loneliness (β = .238, p < .001), lower worries about the own health (β = −.030, p = .020) as well as anxiety (β = .681, p < .001) were significantly associated with depressive symptoms during the lockdown. Perceived stress due to social distancing did not significantly predict depression (β = .014, p = 314). The overall regression was statistically significant (R2 = .732, F(7-1867) = 730,778, p < .001) (see Table 6).
Mediation analysis using PROCESS macro for SPSS 25 (IBM corp., Armonk, USA) was run to explore variables mediating the effect of being a HRGC individual on depression. All mediation analyses were controlled for age and gender as covariates.
First, a parallel mediation model was run to test whether the effect of being a HRGC individual (X) on depression (Y) was mediated by concerns about own health (M1), by feelings of loneliness (M2), by stress due to social distancing (M3) or by anxiety (M4). The results of the mediation analysis (total effect: 2.02, 95% CI: 1.48-2.56; direct effect: .573, 95% CI: .278-.868) demonstrated that the indirect effects were only significant for concerns about own health (M1: CI:-.142--.009;) feelings of loneliness (M2: 95% CI:.195-.475;) and anxiety (M4: 95% CI: .815 -1.55), but not for stress due to social distancing (M3: 95% CI: −.012-.031).
Based on this mediation model, a serial multiple mediation model was run. Here, mediators are linked together in a causal effect chain, with mediators allowing to influence each other (M1 (concerns about own health) → M2 (anxiety) → M3 (loneliness)). The mediation model showed that the association between Covid-19 risk group and depression was mediated by this serial mediation chain (total effect: 2.04, 95% CI: 1.49-2.57; direct effect: 95% CI: .289-.879; indirect effect: 95% CI: .055-.113) with concerns about own health being linked to anxiety and this in turn being associated with feelings of loneliness (see Fig. 2).

Serial multiple mediator model. Notes: Significant indirect effect of X on Y through M1, M2 and M3 in serial (total effect: 2.04, 95% CI: 1.49-2.57; direct effect: 95% CI: .289-.879; indirect effect: 95% CI: .055-.113). Unstandardized beta coefficients are presented. For the direct effect unstandardized coefficients (before and after the mediators (in parentheses) were added to the model) are presented. Mediation analyses was controlled for gender and age. *p < .05** p < .01, *** p < .001
Discussion
According to estimations of the RKI, 52% of all persons living in Germany aged 15 or older belong to a group at risk for severe illness from Covid-19 [32]. The proportion of individuals at increased risk for severe illness from Covid-19 (HRGC) in this study was 47% and thus remarkably higher. The primary aim of this study was to investigate differences in mental health problems (such as depression, anxiety, psychosomatic symptoms and substance use) during the Covid-19 pandemic in HRGC individuals compared to LRCG individuals. In addition, we discuss the relation of these findings in regard to the general German population. We found that 35.9% of the HRGC individuals reported moderate depressive symptoms compared to 26.6% of the LRGC individuals. The proportion of persons with at least moderate depressive symptoms in the HRGC group is remarkably higher than in the LRGC group and four times as high as in the German general population [33]. Regarding the overall rate of depression during the time of the first lockdown in Germany, rates were estimated to have increased to 14.3% (PHQ-2 score ≥ 3) in the general population [12]. Yet, more than twice as many individuals in the HRCG group reported depressive symptoms. Moreover, 29.6% of the HRGC individuals exhibited clinically relevant symptoms of a generalized anxiety disorder in the presented study, while this applies to only 21.4% of the LRGC group. Again, this rate is considerably higher than in the general German population, where the prevalence is estimated at 5,9% [34]. Several studies confirm an increase of generalized anxiety disorders during the first period of the pandemic. A German study [12] reported at least moderate symptoms of generalized anxiety disorders (GAD-7 score ≥ 10) in 16.8% of the participants, which is still a substantially lower rate than in our HRGC group. In terms of somatic symptoms 15.6% of the HRGC individuals and 7.6% of the LRGC individuals showed clinically relevant somatic symptoms in this study, compared to only 9.3% in the German general population [22]. In addition, 19.5% of the HRGC individuals and 9.7% of the LRGC individuals reported an elevated risk for suicide. Hence, the proportion of individuals with and increased risk for suicide is three times higher in the HRGC group than in the German general population [24].
Based on previous studies [19, 35] pointing to the importance of feelings of loneliness for depression, the second aim of the current study was to investigate the association of concerns about own health, anxiety, perceived loneliness, and stress due to lockdown measures with depressive symptoms. Using mediator models, we demonstrated that the direct effect of being an HRGC individual on depression was mediated by concerns about own health, anxiety and feelings of loneliness. In a serial mediation model, an indirect causal effect chain was observed showing that being an HRCG individual was related to concerns about own health, which was associated with increased feelings of anxiety and loneliness and loneliness in turn was related to higher rates of depression. These findings show that HRGC individuals appear to be more worried about their own health during the pandemic than LRGC individuals. We assume that HRGC individuals have avoided social contacts to protect themselves from Covid-19 infections. This increase in social isolation may have resulted in the observed higher rates of loneliness in HRCG individuals, which were associated with depressive symptoms. This is in line with a study by Mayerl et al. [36] showing that COVID-19-related social restrictions were associated with feelings of loneliness and predicted depressive symptoms 10 months later. Quadt et al. [37], proposed a model that perceived loneliness may initiate a cascade of complex body-brain interactions responsible for severe mental and physical health problems.
The results clearly show that the mental health burden is higher among persons at increased risk of severe illness from Covid-19 compared to persons at low risk of severe illness from Covid-19. HRGC individuals are more worried about their own health and report more loneliness, anxiety and depressive symptoms. One factor that may counteract feelings of loneliness and low social connectedness is social support. Therefore, social support during lockdown periods is of utmost importance for individuals prone to mental health problems. Consequently, people at increased risk of severe illness from Covid-19 should not only be protected from a Covid infection but should also receive psychosocial support to decrease feelings of loneliness and increase feelings of social connectedness (e.g. chat-based hotlines, online communication platforms) in order to minimize negative consequences for their mental health during periods of lockdown. This is also in line with a recent study showing that greater social connectedness is associated with reduced stress and fatigue during Covid-19 related lockdown [38]. These findings underline the importance of maintaining social connections also during Covid-19 restrictions to reduce depressive symptoms in pandemic situations.
This study has several limitations. Firstly, it needs to be pointed out that cross-sectional data were collected via an online survey tool, which was mainly promoted by German social service organisations. This recruitment process is likely to have caused a selection bias within the sample by primarily reaching individuals in need for advice from those organisations. Hence, the data collected is not representative of the German general population. Accordingly, representative cross-sectional samples and longitudinal data are desirable in future research. Secondly, the outcome instruments used in the survey were not entirely adapted to the time period of interest, i. e. the first lockdown in Germany. Therefore, it remains unclear whether the mental health burdens reported here changed due to the lockdown. Third, we have not measured social withdrawal directly, but only assume that concerns about own health resulted in reduced social contacts, which may explain the association with perceived loneliness.
Conclusions
This study demonstrates that the mental health burden of the Covid-19 pandemic is high. This is especially true for individuals who are at increased risk of severe illness from Covid-19. These individuals have a particular need for psychosocial support during times of lockdown. Therefore, they should be specifically supported by corresponding offers (e.g. by phone, in chats or online). Moreover, government officials should take into account the mental health consequences of measures aiming at social distancing. More research, however, is needed on possible long-term consequences of social distancing on mental health.
Availability of data and materials
The datasets generated and/or analyzed during the current study are not publicly available due to reasons of sensitivity but are available from the corresponding author Daniel Deimel on reasonable request.
Abbreviations
- COVID-19:
-
Coronavirus SARS-COV2 disease 2019
- SARS-CoV-2:
-
Severe acute respiratory syndrome coronavirus 2
- WHO:
-
World Health Organization
- RKI:
-
Robert Koch Institut
- HRGC:
-
Individuals at increased risk of severe illness from Covid-19
- LRGC:
-
Individuals at low risk of severe illness from Covid-19
- PHQ:
-
Patient Health Questionnaire
- GAD:
-
Generalized Anxiety Disorder
- SBQ-R:
-
Suicide Behaviours Questionnaire – Revised
- OSSS-3:
-
Oslo Social Support Scale – 3
References
WHO. Coronavirus disease 2019 (COVID-19) situation report–34. Geneva; 2019. https://apps.who.int/iris/handle/10665/331220
WHO (2020). WHO announces COVID-19 outbreak a pandemic 2020. http://www.euro.who.int/en/health-topics/health-emergencies/coronavirus-covid-19/news/news/2020/3/who-announces-covid-19-outbreak-a-pandemic.
Bundesministerium für Gesundheit (BMG). Coronavirus SARS-CoV-2: Chronik der bisherigen Maßnahmen. https://www.bundesgesundheitsministerium.de/coronavirus/chronik-coronavirus.html. 16 March 2021.
Robert-Koch Institut (2021a). Tabelle mit Nowcasting-Zahlen zur R-Schätzung. https://www.rki.de/DE/Content/InfAZ/N/Neuartiges_Coronavirus/Projekte_RKI/Nowcasting_Zahlen_csv.html 09 March 2021.
Johns Hopkins University (2021). COVID-19 Dashboard by the Center for Systems Science and Engineering (CSSE) at Johns Hopkins University (JHU). https://gisanddata.maps.arcgis.com/apps/opsdashboard/index.html#/bda7594740fd40299423467b48e9ecf6. 16 March 2021.
Robert-Koch Institut (2021b). Epidemiologischer Steckbrief zu SARS-CoV-2und COVID-19. https://www.rki.de/DE/Content/InfAZ/N/Neuartiges_Coronavirus/Steckbrief.html;jsessionid=B555BAF75F6201541A60FFEEFDB4EEEB.internet102?nn=13490888. 16 March 2021.
Jordan RE, Adab P, Cheng KK. Covid-19: risk factors for severe disease and death. BMJ. 2020;368:m1198. https://doi.org/10.1136/bmj.m1198.
Gao YD, Ding M, Dong X, Zhang JJ, Kursat Azkur A, Azkur D, et al. Risk factors for severe and critically ill COVID-19 patients: A review. Allergy. 2021;76(2):428–55. https://doi.org/10.1111/all.14657.
Bundesregierung (2020). Erweiterung der beschlossenen Leitlinien zur Beschränkung sozialer Kontakte. Besprechung der Bundeskanzlerin mit den Regierungschefinnen und Regierungschefs der Länder vom 22.03.2020. https://www.bundesregierung.de/breg-de/themen/coronavirus/besprechung-der-bundeskanzlerin-mit-den-regierungschefinnen-und-regierungschefs-der-laender-vom-22-03-2020-1733248. 09 March 2021.
Cacioppo JT, Hawkley LC, Norman GJ, Berntson GG. Social isolation. Ann N Y Acad Sci. 2011;1231(1):17–22.
Matthews T, Danese A, Wertz J, Odgers CL, Ambler A, Moffitt TE, et al. Social isolation, loneliness and depression in young adulthood: a behavioural genetic analysis. Soc Psychiatry Psychiatr Epidemiol. 2016;51(3):339–48.
Bäuerle A, Teufel M, Musche V, Weismüller B, Kohler H, Hetkamp M, et al. Increased generalized anxiety, depression and distress during the COVID-19 pandemic: a cross-sectional study in Germany. J Public Health. 2020;42(4):672–8. https://doi.org/10.1093/pubmed/fdaa106.
Gualano MR, Lo Moro G, Voglino G, Bert F, Siliquini R. Effects of Covid-19 Lockdown on Mental Health and Sleep Disturbances in Italy. Int J Environ Res Public Health. 2020;17(13):4779. https://doi.org/10.3390/ijerph17134779.
Salari N, Hosseinian-Far A, Jalali R, Vaisi-Raygani A, Rasoulpoor S, Mohammadi M, et al. Prevalence of stress, anxiety, depression among the general population during the COVID-19 pandemic: a systematic review and meta-analysis. Glob Health. 2020;16(1):57. https://doi.org/10.1186/s12992-020-00589-w.
Horigian VE, Schmidt RD, Feaster DJ. Loneliness, Mental Health, and Substance Use among US Young Adults during COVID-19. J Psychoactive Drugs. 2021;53(1):1–9.
Cullen W, Gulati G, Kelly BD. Mental health in the COVID-19 pandemic. QJM. 2020;113(5):311–2. https://doi.org/10.1093/qjmed/hcaa110.
Savage RD, Wu W, Li J, Lawson A, Bronskill SE, Chamberlain SA, et al. Loneliness among older adults in the community during COVID-19: a cross-sectional survey in Canada. BMJ Open. 2021;11(4):e044517. https://doi.org/10.1136/bmjopen-2020-044517.
Groarke JM, Berry E, Graham-Wisener L, McKenna-Plumley PE, McGlinchey E, Armour C. Loneliness in the UK during the COVID-19 pandemic: Cross-sectional results from the COVID-19 Psychological Wellbeing Study. PLoS One. 2020;15(9):e0239698. https://doi.org/10.1371/journal.pone.0239698.
Erzen E, Çikrikci Ö. The effect of loneliness on depression: a meta-analysis. Int J Soc Psychiatry. 2018;64(5):427–35. https://doi.org/10.1177/0020764018776349.
Gräfe K, Zipfel S, Herzog W, Löwe B. Screening psychischer Störungen mit dem "Gesundheitsfragebogen für Patienten (PHQ-D)". Diagnostica. 2004;50(4):171–81. https://doi.org/10.1026/0012-1924.50.4.171.
Löwe B, Decker O, Müller S, Brähler E, Schellberg D, Herzog W, et al. Validation and standardization of the Generalized Anxiety Disorder Screener (GAD-7) in the general population. Med Care. 2008;46(3):266–74. https://doi.org/10.1097/MLR.0b013e318160d093.
Kocalevent RD, Hinz A, Brähler E. Standardization of a screening instrument (PHQ-15) for somatization syndromes in the general population. BMC Psychiatry. 2013;13:91. https://doi.org/10.1186/1471-244X-13-91.
Kroenke K, Spitzer RL, Williams JBW. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med. 2001;16:606–13. https://doi.org/10.1046/j.1525-1497.2001.016009606.x.
Glaesmer H, Kapusta ND, Teismann T, Wagner B, Hallensleben N, Spangenberg L, et al. Psychometrische Eigenschaften der deutschen Version des suicide behaviors questionnaire revised (SBQ-R). Psychother Psycho Med Psychol. 2018;68:346–52. https://doi.org/10.1055/s-0043-118335.
Osman A, Bagge CL, Gutierrez PM, Konick LC, Kopper BA, Barrios FX. The suicidal behaviors questionnaire-revised (SBQ-R): validation with clinical and nonclinical samples. Assessment. 2001;8:443–54. https://doi.org/10.1177/107319110100800409.
de Jong-Gierveld, J., & van Tilburg, T. G. (1999). Manual of the Loneliness Scale. Methoden en technieken.
Kilpeläinen K, Aromaa A, the ECHIM project (Hrsg), editors. Europe- an Health Indicators: Development and Initial Implementation. Final report of the ECHIM project. Helsinki: National Public Health Institute; 2008.
Kocalevent RD, Berg L, Beutel ME, et al. Social support in the general population: standardization of the Oslo social support scale (OSSS-3). BMC Psychol. 2018;6:31. https://doi.org/10.1186/s40359-018-0249-9.
Robert Koch Institut (2020). Epidemiologischer Steckbrief zu SARS-CoV-2 und COVID-19. https://www.rki.de/DE/Content/InfAZ/N/Neuartiges_Coronavirus/Steckbrief.html;jsessionid=C915BAA6301122643053EA2059614DC6.internet112?nn=13490888#doc13776792bodyText15
Hayes AF. Introduction to mediation, moderation, and conditional process analysis: a regression-Based approach. New York: The Guilford Press; 2013.
Hayes AF, Rockwood NJ. Regression-based statistical mediation and moderation analysis in clinical research: Observations, recommendations, and implementation. Behav Res Ther. 2016; https://doi.org/10.1016/j.brat.2016.11.001.
Rommel A, von der Lippe E, Treskova-Schwarzbach M, Scholz S. Bevölkerung mit einem erhöhten Risiko für schwere COVID-19-Verläufe in Deutschland. Auswertungen der Studie GEDA 2019/2020-EHIS. J Health Monitor. 2021;6(S2):2–15. https://doi.org/10.25646/7858.2.
Busch M, Maske U, Ryl L, et al. Prävalenz von depressiver Symptomatik und diagnostizierter Depression bei Erwachsenen in Deutschland. Bundesgesundheitsblatt. 2013;56:733–9. https://doi.org/10.1007/s00103-013-1688-3.
Hinz A, Klein AM, Brähler E, Glaesmer H, Luck T, Riedel-Heller SG, et al. Psychometric evaluation of the generalized anxiety disorder screener GAD-7, based on a large German general population sample. J Affect Disord. 2017;210:338–44. https://doi.org/10.1016/j.jad.2016.12.012.
Loades ME, Chatburn E, Higson-Sweeney N, Reynolds S, Shafran R, Brigden A, et al. Rapid Systematic Review: The Impact of Social Isolation and Loneliness on the Mental Health of Children and Adolescents in the Context of COVID-19. J Am Acad Child Adolesc Psychiatry. 2020;59(11):1218–1239.e3. https://doi.org/10.1016/j.jaac.2020.05.009.
Mayerl H, Stolz E, Freidl W. Longitudinal effects of COVID-19-related loneliness on symptoms of mental distress among older adults in Austria. Public Health. 2021;200:56–8. https://doi.org/10.1016/j.puhe.2021.09.009.
Quadt L, Esposito G, Critchley HD, Garfinkel SN. Brain-body interactions underlying the association of loneliness with mental and physical health. Neurosci Biobehav Rev. 2020;116:283–300. https://doi.org/10.1016/j.neubiorev.2020.06.015.
Nitschke JP, Forbes P, Ali N, Cutler J, Apps M, Lockwood PL, et al. Resilience during uncertainty? Greater social connectedness during COVID-19 lockdown is associated with reduced distress and fatigue. Br J Health Psychol. 2021;26(2):553–69. https://doi.org/10.1111/bjhp.12485.
Acknowledgements
Not applicable.
Authors’information
Not applicable.
Funding
Open Access funding enabled and organized by Projekt DEAL. The study was realised through funds from Catholic University of Applied Science NRW, Germany.
Author information
Authors and Affiliations
Contributions
DD: Conceptualization study design, questionnaire and study organization, data analysis, drafted the manuscript; CF: data analysis, data interpretation; TK: statistical consulting; NG and JD: data interpretation; finalization and translation of the article. The authors critically revised and approved the final draft of the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The studies involving human participants were reviewed and approved by Ethics Committee of the Catholic University NRW, Department Aachen, approval nr. AZ 2020-I (25.05.2020). The minimum age for participation in the survey was set at 18 years, whereby on the basis of the German guidelines, All participants gave electronic informed consent for the participation and for illiterates from their Legal representative. The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional committees on human experimentation and the Helsinki Declaration of 1975, as revised in 2008. Participation in the study was anonymous.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests nor conflicts of interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Deimel, D., Köhler, T., Dyba, J. et al. Mental health of Covid-19 risk groups during the first Covid-19 lockdown in Germany: a cross-sectional study. BMC Public Health 22, 1187 (2022). https://doi.org/10.1186/s12889-022-13593-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12889-022-13593-z