
Abstract
Background
Studies in Africa have examined the association between helmet use and injury prevention, however, there has been no systematic review to synthesize the literature within an African context nor has there been any meta-analysis examining the effect of helmet use on injury prevention.
Methods
The review was performed in accordance with the Joanna Briggs Institute for Systematic Reviews. Articles were searched using several databases (e.g. CINAHL, OVID Medline) and select gray literature (e.g. TRID) sources. Articles were included if they were quantitative studies published in English between 2000 and 2019 and examined the association between motorcycle helmet use with head injuries, hospitalizations, and deaths in low- and lower-middle income countries in Africa with comprehensive motorcycle helmet laws. A meta-analysis was performed using pooled effect sizes assessing the impact of helmet use on reducing head injuries.
Results
After screening 491 articles, eight studies met the inclusion criteria. Helmet use ranged from 0 to 43%. The mean age of being involved in a crash was 30 years with males being two times more likely to be involved in motorcycle crashes than females. Drivers (riders) were more likely to be involved in a crash, followed by passengers and then pedestrians. Helmet use reduced injury severity and provided an 88% reduction in serious head injuries (OR 0.118, 95% CI: 0.014–0.968, p = 0.049).
Conclusions
In our study, helmet usage significantly reduced the likelihood of fatal head injuries. African countries with no helmet laws should consider adopting helmet use policies to reduce severe head related injuries from motorcycle crashes.
Similar content being viewed by others
Introduction
Road traffic crashes (RTC) account for a considerable portion of the global public health burden [1] resulting in approximately 1.35 million fatalities and 20 to 50 million injuries annually [2]. RTCs are the 8th leading cause of death in the world and the leading cause of death among those between 5 and 29 years of age [2]. According to the Global Health Burden report, there has been a positive trend over the last 20 years in the reduction of RTCs in high-income countries, yet there is an opposite trend in low- and middle-income countries [3]. In fact, the RTC fatality rates in low-income countries are three times higher compared to high-income countries [4]. The highest RTC fatality rates are reported in Africa with 26.6 deaths per 100,000 people, substantially higher than the 8.3 death per 100,000 people in high-income countries [2, 5]. Consequently, the United Nations (UN) Sustainable Development Goals and the UN Decade of Action on Road Safety are targeting improvements in road safety initiatives in Africa to reduce the number of RTC by 50% in the coming years [5, 6].
Throughout most of Africa, motorcycles are used as both public and private modes of transportation [7, 8]. For example, motorcycles have become increasingly popular over the last decade, due to their ability to navigate through poor road conditions and congested traffic compared to other larger motor vehicles [7, 9]. However, this trend has also resulted in an increase in mortality and morbidity rates [9]. Together, RTCs for motorcyclists, cyclists, and pedestrians account for more than 50% of head-related deaths [2]. Even after controlling for distance travelled, fatalities among motorcyclists and their passengers are approximately 35 times higher than other motor vehicle types [7, 10]. A possible reason for the elevated fatality rate is the lack of protective equipment and shielding [11, 12], such as low helmet use, as evidenced in low and middle-income countries [13, 14].
Studies show the importance of wearing helmets in preventing motorcycle crash (MC) injuries and deaths [2, 15,16,17,18,19,20]. For example, a Cochrane review found helmet use reduced the risk of head injuries and deaths by 69 and 42%, respectively [14]. Additionally, ecological studies demonstrate motorcycle helmet laws are associated with a decline in morbidity and mortality rates [14, 20, 21]. Although studies have examined the association between helmet use and injury prevention in Africa [19, 22,23,24,25,26], there has been no systematic review to synthesize the literature within an African context nor has there been any study examining the effect of helmet use on injury prevention. Understanding the effectiveness of helmet use on road crashes is a priority area for Safer Africa, an organization funded by Horizon 2020 to improve road safety in Africa [27]. Thus, the objective of this study is to examine the literature on the effectiveness of motorcycle helmet use in reducing the severity of crash related injuries, hospitalizations and mortalities in low to lower-middle income countries in Africa with comprehensive motorcycle helmet laws.
Methods
Search strategy
This systematic review was conducted in accordance with the Joanna Briggs Institute (JBI) for Systematic Reviews [28]. A search for published peer-reviewed articles and conference proceedings was performed using the following databases: CINAHL, Public Health Database, Medline OVID, and Web of Science. In addition, a gray literature search was conducted using Transport Research International Documentation (TRID), which combines more than 1.3 million articles from the Transportation Research Board’s Transportation Research Information Services and the OECD’s Joint Transport Research Centre’s International Transport Research Documentation Database. Additionally, we searched for articles using Google Scholar and by manually screening the reference list of eligible articles from the search.
The search terms were developed by two reviewers in consultation with the University of Saskatchewan librarian. The search strategy only included the terms motorcycles, helmets and Africa in order to broaden the scope and find more relevant articles. The strategy was developed in Medline and terms were entered in combination using “AND’ and “OR” operators. Terms were then tailored to the other databases used (see Additional file 1: Appendix I).
Inclusion and exclusion criteria
The search was limited to low- and lower-middle income countries in Africa, more specifically Ghana, Guinea-Bissau, Kenya, Madagascar, Morocco, Nigeria, Swaziland (Eswatini), and Zimbabwe. The selected countries were identified according to the Countries with Helmet Laws Meeting Best Practice 2017 from the WHO Global Status Report on Road Safety 2018 and the Helmet Laws, Enforcement and Wearing Rates by Country/Area 2015, and cross-referenced with the World Bank [29]. Countries were selected if they had a comprehensive motorcycle helmet law, defined as a requirement of both drivers and passengers of motorized two-wheelers to wear helmets on all roads, regardless of the engine type [30]. Given this definition, selected countries were required to have the following:
-
National motorcycle helmet law
-
Applies to drivers and adult passengers
-
Applies to all roads
-
Applies to all engines
-
Helmet fastening required, and standard referred to and/or specified
Peer-reviewed studies and conference proceedings published in English between 2000 and 2019 were included. The date range was determined based on the implementation date of motorcycle helmet regulations, policies, or procedures in the selected countries, which mainly came into effect from the year 2000 onwards. All quantitative study types were included if they measured the impact of helmet use on injuries, hospitalizations, and mortality rates. Motorcycle riders were considered both riders (drivers) and passengers.
Studies were excluded if they were:
-
Not in English
-
Intervention or Modelling studies
-
Qualitative or Evaluation studies (e.g. cost benefit analysis)
-
High-income countries or were not the selected countries
-
Did not measure the targeted outcomes- hospitalizations, injuries or mortalities
-
Did not report on helmet use
Reviewers did not find published articles on motorcycle helmet use in some of the pre-defined countries (i.e. Guinea-Bissau, Madagascar, Morocco, Swaziland, and Zimbabwe). A search was recreated in each database using the same strategy (as detailed above) replacing “Africa” with the individual country name. No additional studies were found.
Study screening and selection
Following the search, articles were entered into a Microsoft™ Excel sheet; duplicates were removed. Two independent reviewers undertook the screening process which consisted of three phases: title, abstract, and full-text review. In instances where it was unclear whether a study met the inclusion criteria in the title and abstract screening phases, a full-text review was conducted to ensure all relevant studies were captured. There was a 98.7% agreement between the reviewers during the title review stage and 100% agreement during the abstract and full-text review stages. All disagreements were resolved through consensus in the first stage.
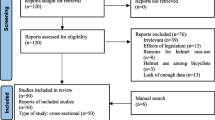
The study selection process followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA), illustrated in Fig. 1. The literature search identified a total of 491 results, of which 485 studies were found via database searches, and six studies through grey literature searches; 181 duplicate studies were omitted. Three hundred ten records were screened for title review, resulting in the exclusion of 291 studies: 62 did not examine helmet use or report on injuries; 49 were policy evaluations/description; 51 were intervention or programming-based studies; 17 reported on helmet features (e.g. material); 56 were based in the selected countries; 3 were not published in English; and 53 were for other reasons (e.g. training manual, travel advisory notices; usage of helmets in occupational groups). Full texts were obtained and screened against the inclusion criteria for the remaining 19 records, resulting in the exclusion of eight studies (5 were not specific to helmet use; 2 were removed because they were based on projections/modelling; and one study reported on equipment quality).

PRISMA Flow Diagram of Study Selection
Data extraction
Data were extracted from the included articles using a pinch table (Table 1). Information on the title, author(s), date, and location; study population (i.e. sample size, age, gender, socioeconomic status); study design (inclusion/exclusion criteria), independent variables (including instrument); outcome variable; and results were collected.
Data synthesis
Critical appraisal
The JBI Critical Appraisal checklists were used to assess the validity, methodological quality and bias in each study. The nine-question Checklist for Prevalence Studies [35] was used to assess six studies classified as descriptive by reviewers as they characterized the prevalence of the exposure (i.e. helmet or non-helmet use) and outcome (i.e. injuries and/or death). The eight-question Checklist for Analytical Cross-Sectional Studies [36] was used for the other five studies categorized as analytical as they examined the relationship between the exposure and outcome. Two reviewers independently conducted the critical appraisals for each study with an 88% consensus. Disagreements were resolved by the inclusion of a third reviewer. Three studies were excluded from the review from being classified as being of low methodological quality. In this review, low methodological quality referred to failing more than half of the criteria (50%). Eight studies met the criteria and were considered as being of moderate quality.
As shown in Table 2, three of the six descriptive studies met the criteria for inclusion [31,32,33]. One article met seven out of the nine criteria [31] while the other two studies met five of the nine criteria [32, 33].
As shown in Table 3, all five analytical studies passed the methodological appraisal review [22, 23, 25, 32, 34]. One study met seven out of the eight criteria [22]. Three studies met six out of the eight criteria [23, 25, 34]. Inclusion criteria were clearly defined in all studies, and the exposures were measured in a valid and reliable way. Only one study mentioned and adjusted for confounders [22].
Preliminary assessment and Meta-analysis
A preliminary assessment was conducted to determine whether a meta-analysis was appropriate and which studies would be eligible to be included. The PICO (population, intervention, comparator, outcome) method was utilized and documented in Table 4. A meta-analysis was performed on three studies measuring head injuries as an outcome, examining helmet use as the intervention. Effect size was reported as an odds ratio (OR), with a 95% confidence interval (CI) and corresponding p-value. A random effects model was applied due to the distribution of true effect sizes amongst the three studies. Heterogeneity was analyzed using I squared (I2). Funnel plot and Egger test were the indicators used to assess publication bias. All analyses including sensitivity analysis were performed using the Comprehensive Meta-Analysis V3 software.
Results
Design and setting
All eight studies were cross-sectional and used convenience sampling. Seven of the eight studies were conducted prospectively; one was retrospective. Five studies were conducted in Kenya and three in Nigeria. Motorcycle crashes were the variable of interest for six studies while two studies looked at RTCs including motorcycle-related crashes. Participants were recruited from hospitals in seven studies; five recruited victims involved in motorcycle crashes and two studies examined victims of road related traffic crashes. The settings included the Crash and Emergency department in five studies, one maxillofacial unit, and one referral trauma and pediatric surgical center. One study collected data from participants who were previously involved in MCCs using a structured questionnaire in eleven rural and urban sites in Kenya. Three studies were conducted over a one-year period, three took place in less than a year, and two were conducted for more than a year.
Population characteristics
The sample sizes varied between 107 and 384 patients. MCCs accounted for 18 to 53% of all crashes among the studies. Among all studies, the study population consisted of more males than females, with approximately a 2:1 ratio in three of the studies; 3:1 in two studies; and more than 3:1 in three studies. The mean age for nearly all the studies was about 30 years old, however, some age and gender differences emerged. One study found the peak age of sustaining motorcycle related injuries for males was 20–29 years compared to the 10–19 age bracket for females [32]. Another study found that the average age of male drivers who suffered injuries was 25–31 years, followed by 18–24, with the opposite being observed for females [33]. However, one study reported no difference between male and female MCC injury victims [23]. More than half of the studies classified participants based on road type user, in which three differentiated between riders, passengers, and pedestrians; one study assessed riders and passengers; and one of the RTC studies distinguished between two-wheeled vehicle occupants and pedestrians. The road user most injured were riders, followed by passengers and pedestrians, respectively, across all studies. In the four studies that assessed education level, primary school (41–65%) was the highest level attained by the participants, followed by secondary level (32–40%), then college/tertiary level (2.6–15%).
Helmet use
Six studies reported helmet use at the time of a crash ranged from 0 to 43%. Only one study reported that none of the crash victims wore a helmet at the time of a crash [32]. Two studies compared helmet use between road users [24, 34]. Helmet use ranged from 9 to 50% for riders and 9–20% for passengers. One study found that people on 2-occupant motorcycles were more than seven times more likely to wear helmets compared to more than 2-occupants riders [34].
Time and day of crash
Three studies compared time and day of crash. One study found that 51% of the crashes occurred during the afternoon hours (7 am-11:59 am), followed by the 36.7% in the morning (7 am-11:59 am), 10.3% in the evening (6 pm-11:59 pm) and 2.1% in the early morning (12 am-6:59 am), however, time of crash was not significantly associated with head injuries [23]. Similarly, another study found that 32% of crashes occurred during the day, 22% in the morning, 29% at sunset and 17% at night (hours of day undefined) [32]. Individuals involved in crashes during the night were five times more likely to suffer injuries compared to daytime crashes (Unadjusted OR 5.3, 95% CI 1.7–16.2, p = 0.00) [33].
About 65% of motorcycle crashes occurred during the day (versus night) [24] and almost three-quarters (71.8%) of head-related motorcycle crashes occurred on weekdays (Monday to Friday) compared to the week-end [23]. The highest proportion of crashes occurred on Friday’s (16.1%) and Mondays (15.8%) respectively, although there was no association between head injuries and the days of the week the crash occurred [22].
Setting of crash
The studies examining crash settings were varied [22, 24, 32] One study reported that 93.9% all the crashes occurred on the highway and 0.3% occurred on rural roads [22] whereas another study reported that 70.4% took place on smaller roads in residential areas and the suburbs compared to the 29.6% that occurred on main city roads [24]. In another study, 36.6% of the injuries occurred on paved non-highway roads, 31.7% on dirt roads, 22.0% on the highway, 8.9% on gravel and 0.8% in the parking lot [33].
Mechanism of crash
Three studies assessed mechanism of crash. Motorcycle-vehicle collisions accounted for 45.6% of the crashes, followed by 23.4% of motorcycle-motorcycle collisions, 18.5% of motorcycle-animal collisions, 9.9% motorcycle-bicycle, along with motorcycle-lone and motorcycle tree/pole collisions, each representing 0.5% of the crashes [22]. In a later study by the same first author, 48.3% of collisions were motorcycle-vehicle, followed by 22.6% motorcycles-motorcycle crashes, 17% motorcycles-pedestrians, 9.4% motorcycle-bicycle, 1.5% motorcycle-animal, and 0.6% motorcycle-poles/trees crashes [23]. Similarly, another study reported the nature of the collisions were motorcycle to vehicle (19.6%), tied with head-on collision with other objects (19.6%), rear collisions (10.3%), falls (25.2%), collision with motorcycle (10.3%) and others (15.0%) [32].
Injury type
Head and neck injuries ranged from 40 to 60.6% [22, 31], followed by lower extremities injuries that ranged from of 39.9% [22] to 48.5% [31]. There was a significant reduction in head injuries in those wearing helmets in three studies. Head injuries in those wearing helmets ranged from 1.6 to 37.7% compared to 62.3 to 85.6% in riders not wearing helmets [22, 23, 33]. Extremities were the main site of injury in two studies, followed by head or neck injuries [24, 34]. Injury types varied in the three studies with one study reporting skin lacerations and abrasions being the primary injury type for all road traffic crash victims including motorcycle crashes [25]. One study reported minor injuries made up 38% of injury types followed by bruises (36%) [33]. A study analyzing maxillofacial injuries found moderate laceration as the main type of soft tissue injury and the mandible as the leading type of fracture [32]. The proportion of injuries were significantly reduced in riders using helmets although these studies did not specify the exact nature of the injuries. For example, one study found that 28 and 35.6% of helmet users were injured compared to 72 and 89.5%, respectively [21, 33].
Two studies examined injuries sustained by road users. One study reported that 50% of riders suffered head injuries compared to 35% of passengers and 22% of pedestrians [22]. Riders (49%) also sustained other injuries (not specified) compared to 35% of passengers and 16% of pedestrians [22]. Being a rider was significantly associated with sustaining a head injury (χ2 = 80.658, p < 0.00) [23]. The other study observed that more passengers suffered head injuries (69.5%) and injuries to the extremities (68.7%) compared to 30.5% of riders that sustained head injuries and 31.3% suffered injuries to the extremities [34]. Alternatively, riders sustained more chest (62.5%) and external (53.7%) injuries compared to chest (37.5%) and external injuries (46.3%) of passengers [28]. However, an equal percent of riders and passengers sustained facial (50%) and abdominal (50%) injuries [34].
Injury severity based on type of road user
Many studies used instruments to measure patterns of morbidity and mortality. The Glasgow Comma Scale (GCS) was used to measure head injury and severity in four studies [22,23,24, 31]; and the Abbreviated Injury Scale (AIS) was used in one study [24]. In three studies, the Injury Severity Score (ISS) was used to measure severity [24, 31, 34]; and one study used the Trauma and Injury Severity Score (TRISS) to measure the probability of survival [24]. Questionnaires, interviews or a combination of the two were used in six studies [22, 23, 31,32,33,34]. Information from patient files, admission register books, or medical charts were collected in 6 studies [22, 23, 25, 32,33,34]. Other instruments utilized included clinical examination [22, 23] and radiological data [22, 23], as well as information from the police and healthcare professionals [31].
Two articles explored the relationship between type of road users and injury severity. One study reported that 69.5% of road users suffered moderate injuries, 16.1% severe injuries and 14.2% minor injuries [22]. More riders (29.3%) suffered severe injuries compared to passengers (6.2%) and pedestrians (3.4%) [22]. Alternatively, passengers sustained more moderate injuries (88.2%) compared to riders (63.5%) and pedestrians (42.4%) [22]. More pedestrians (54.2%) sustained minor injuries compared to riders (7.7%) and passengers (5.6%) [22]. The relationship between injury severity and road user was found to be statistically significant (χ2 = 129.94, p < 0.001) [22]. Another study reported that 100% of the riders suffered moderate injuries while 90.4% of passengers sustained moderate injuries and 9.6% suffered severe injuries [34].
Mortality
The relationship between helmet use and mortality was examined in two studies. One study examined predictors of mortality at 2 weeks after a motorcycle crash, in which 2.8% of those who used helmets died compared to 14.3% of non-helmet users [24]. Injury severity was predictive of mortality within 2 weeks of admission [24]. In another study, none of the 21 patients that wore a helmet at the time of crash died compared to 10.5% that did not wear a helmet [25].
Meta-analysis
Head injury
Figure 2 displays the random effects meta-analysis results. Three studies measuring effects of helmet use on head injuries, compared to non-helmet use, were included in the meta-analysis. Overall, the pooled results were statistically significant and indicated that helmet use provides an 88% reduction in sustaining head injuries (OR = 0.118, 95% CI: 0.014 to 0.968). In two of the individual studies, there was a statistically significant protective association between helmet use and head injury [22, 24]. In one study, there was no protective effect of using helmets and sustaining a head injury [23].

Random effects meta-analysis comparing helmet use vs non-helmet use. Reference point was non-helmet use (OR = 1.0)
Substantial heterogeneity (I2 = 94.256) was noted among effect sizes which may be attributed to confounders as only one study adjusted for them [22] with the other two not identifying confounders or failing to report them in their study [23, 24]. Egger’s regression test was significant for publication bias (p = 0.049).
Discussion
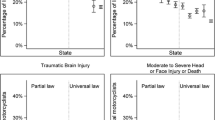
The findings indicate a low prevalence of motorcycle helmet use ranging from 0 to 43%. Helmet use ranged from 28 to 43% in Kenya [22,23,24] and 0–35.6% in Nigeria [25, 32, 34]. This is consistent with prior findings in other low- and lower-middle income countries in Africa; however, they are different from non-African low- and low-middle income countries. For instance, in a cross-sectional observational study in Ghana, the prevalence of helmet use was 45.8% in riders and 3.7% in passengers [26]. In India, helmet use was observed to be 89% in Calicut city but only 23% in rural areas [39]. Greater use of helmets in urban centres was credited to stringent and consistent enforcement strategies that were not found in the rural areas [39]. Helmet use in an Ethiopian study was predicted by having a valid license, having greater driving experience, driving greater distances, being exposed to accidents and having an accident risk perception [40]. However, a comprehensive helmet law was not a motivator to wearing a helmet which may explain why only 12.4% of riders wore a helmet [40]. In high income countries such as the USA, 99% of motorcyclists wear helmets in states that have helmet laws compared to 71% that do not. Moreover, 89% of motorcyclists in states with helmet laws were compliant with helmet safety regulations where only 56% were compliant in states without helmet laws [41]. Considering the trend of low helmet use in our study, and in low-middle income countries [26, 39, 40, 42], efforts are needed to examine underlying factors such as lack of enforcement strategies, or uninformed knowledge, attitudes, and practices of riders.
The findings that helmet use reduced injuries was supported by the meta-analysis. Our meta-analysis found that wearing a helmet at the time of the crash was protective against head injuries. Our study also found that helmet use reduced mortality consistent with prior studies in developed [15,16,17,18,19,20] and developing countries [14, 42, 43]. For example, studies from Kenya found a risk reduction of head injuries by 69% and mortality by 42% from using helmets [14, 43] and another study in Vietnam found the implementation of helmet laws in Cu Chi city resulted in a 65% decrease in head injuries and a 31% reduction in the number of deaths from motor vehicle crashes [42]. It is clear that helmet use not only reduces the likelihood of significant injuries but also saves the health care system in treatment and rehabilitation costs [44].
Our study also found that riders were more likely to be involved in MCCs (range 45–68%) compared to passengers (range 17–39%), which is consistent with other African studies not included in this review. For example, in Benin-City, Nigeria, 60.8% of riders were involved in MCCs compared to 39.2% of passengers [37]. Our review also found that approximately 15% of crashes occur in pedestrians. This could be because there is no designated sidewalk for pedestrians (resulting in them walking along the road) and poor street lighting, increasing the risk of being struck by a motor vehicle [23]. Future research should consider differences between riders, passengers and pedestrians on several criteria, including age distribution, education level, rate of helmet use, head injury sustained, other types of injuries sustained, injury severity, and mortality. Additionally, there may be differences in helmet practices for those that use motorcycles for employment vs personal use. For example, a study in Cameroon found that commercial motorcycle riders were 4x less likely to wear any protective gear (including helmets) compared to riders who used motorcycles for personal use [45]. Distinctions between the category of road users can reveal trends or patterns that may be useful in tailoring interventions.
Our review shows that males were at least two times as likely to be admitted to a hospital following a motor vehicle crash. Other findings have demonstrated that males are also more likely to be involved in MCCs and RTCs, which reflects that males are typically more likely to engage in risk taking behaviors including speeding [7, 46]. Among all the studies in this review, primary school was more often the highest level of education obtained which may contribute to difficulty navigating road signs or understanding the rules of the road. Additionally, our review found a trend that crashes occur in the daytime and during the week (compared to the week-end). It is possible that motorcycle crashes during the day are related to employment, however, none of the included studies captured the reasons why crashes occurred or the circumstances that led up to the crash. Understanding the factors associated with crashes can result in infrastructure changes to reduce crash risk, especially in areas where traffic is dense.
Limitations and opportunities for further research
This review also found several methodological gaps that can be improved upon in future research. First, the studies identified for the systematic review and meta-analysis were all cross-sectional which only examined the association between exposure and outcome variables at one point in time [47], precluding the ability to determine causality [48,49,50]. Additionally, only one of the three studies included in the meta-analysis adjusted for confounding factors which could explain the high heterogeneity observed. There may also have been differences in standards of helmets, or the type of helmets used (i.e. full-face or half face) since these were not defined or captured in the studies. The use of non-standard helmets that are often used in low- and middle-income countries may negate the positive benefits of having a comprehensive helmet law [51]. Given the price of a standard helmet is 2-3x greater than that of non-standard helmets [50], future studies should assess the types of helmets used (i.e. full-face versus half-face; standard versus novelty helmets) and examine practices such as proper fastening of the helmet to garner a more in-depth understanding of this issue. There is also a need to determine how many riders and/or passengers use helmets. According to the African Road Safety Action Plan, fewer than 18% of African countries provide information on rates of helmet use [52].
All studies employed convenience sampling which does not capture a true representation of the general population [53]. While most studies recruited participants from hospitals, studies did not include those who did not present at the hospital due to minor injuries or those pronounced dead at scene [54]. Consequently, it is possible the true effects of helmet use on reducing injuries is understated [55]. Other limitations included the lack of published helmet use studies from African countries with comprehensive helmet policies, specifically Guinea-Bissau, Madagascar, Morocco, Swaziland, and Zimbabwe. Capturing data from these countries would reaffirm the trend surrounding helmet use in Africa. Data from Africa are generally underreported and there are many inconsistencies between data that is collected, due to lack of road traffic data collection systems [56,57,58].
Research has demonstrated the impact of motorcycle helmet legislation in improving helmet uptake, however, governance alone is insufficient [43, 59,60,61,62,63,64]. While the reviewed studies did not provide details on how helmet laws were enforced or advertised, it is clear that helmet uptake is important in order to reduce the number of RTC injuries and fatalities. An examination of enforcement strategies, stigma, and advertising campaigns is warranted in African settings, including differences between urban and rural contexts. Lessons learned from developed countries in implementing helmet laws have potential to be applied and tailored for African settings.
Conclusion
The outcomes of this systematic review support the assumption that helmet use protects against head injuries, according to the current literature addressing the case of African riders. Therefore, low- and middle-income countries in Africa should highly consider implementing comprehensive motorcycle helmet laws. Further research efforts are crucial in these countries due to the high prevalence of crashes resulting in head injuries. Evidence-based data and collaborative efforts between stakeholders are required to inform the development of helmet policies to improve road safety in low and lower-middle income countries.
Availability of data and materials
The search strategy including the databases used and the key terms are available upon request from the corresponding author.
Abbreviations
- RTC:
-
Road Traffic Crashes
- MCC:
-
Motorcycle accident
- JBI:
-
Joanna Briggs Institute
- OR:
-
Odds ratio
- CI:
-
Confidence interval
- I2 :
-
I-squared
- GCS:
-
Glasgow Comma Scale
- AIS:
-
Abbreviated Injury Scale
- ISS:
-
Injury Severity Score
- TRISS:
-
Trauma and Injury Severity Score
References
Population Reference Bureau, Worley H. Road Traffic Accidents Increase Dramatically Worldwide; 2006. [cited 30 Nov 2020]. Available from: https://www.prb.org/roadtrafficaccidentsincreasedramaticallyworldwide/
World Health Organization. Global status report on road safety; 2018. [cited 3 May 2020]. Available from: https://www.who.int/violence_injury_prevention/road_safety_status/2018/en/
Haagsma J, Graetz N, Bolliger I, Naghavi M, Higashi H, Mullany E, et al. The global burden of injury: incidence, mortality, disability-adjusted life years and time trends from the global burden of disease study 2013. Injury Prevention. 2016;22(1):3–18.
Centers for Disease Control and Prevention. Road Traffic Injuries and Deaths-A Global Problem | Features; 2019. [cited 30 Nov 2020]. Available from: https://www.cdc.gov/features/globalroadsafety/index.html
Ralaidovy A, Bachani A, Lauer J, Lai T, Chisholm D. Cost-effectiveness of strategies to prevent road traffic injuries in eastern sub-Saharan Africa and Southeast Asia: new results from WHO-CHOICE. Cost Eff Resourc Alloc. 2018;16(59). https://doi.org/10.1186/s12962-018-0161-4.
United Nations. Sustainable Development Goals; n.d. [cited 30 Nov 2020]. Available from: https://sustainabledevelopment.un.org/?menu=1300
Faduyile F, Emiogun F, Soyemi S, Oyewole O, Okeke U, Williams O. Pattern of injuries in fatal motorcycle accidents seen in Lagos state university teaching hospital: an autopsy-based study. Open Access Maced J Med Sci. 2017;5(2):112–6.
Nwadiaro H, Ekwe K, Akpayak I, Shitta H. Motorcycle injuries in north-central Nigeria. Niger J Clin Pract. 2011;14(2):186.
Arosanyin G, Olowosulu A, Oyeyemi G. An examination of some safety issues among commercial motorcyclists in Nigeria: a case study. Int J Inj Control Saf Promot. 2013;20(2):103–10.
Tumwesigye N, Atuyambe L, Kobusingye O. Factors Associated with Injuries among Commercial Motorcyclists: Evidence from a matched case control study in Kampala City, Uganda: E0148511. PLoS One 2016;11(2):E0148511.
Cavalcanti AL, Lucena BM, Rodrigues IS, Silva AL, Lima TT, Xavier AF. Motorcycle accidents: morbidity and associated factors in a city of northeast of Brazil. Tanzania J Health Res. 2013;15(4):209–15.
Albalate D, Fernàndez-Villadangos L. Motorcycle injury severity in Barcelona: the role of vehicle type and congestion. Traffic Inj Prev. 2010;11(6):623–31.
Zaccaro H, Carbone E, Dsouza N, Xu M, Byrne M, Kraemer J. Assessing the reliability and validity of direct observation and traffic camera streams to measure helmet and motorcycle use. Inj Prev. 2015;21(6):415–7.
Liu BC, Ivers R, Norton R, Boufous S, Blows S, Lo SK. Helmets for preventing injury in motorcycle riders. Cochrane Database Syst Rev. 2009;23(3). https://doi.org/10.1002/14651858.CD004333.pub3.
Rice TM, Troszak L, Ouellet JV, Erhardt T, Smith GS, Tsai B. Motorcycle helmet use and the risk of head, neck and fatal injury. Accid Anal Prev. 2016;91:200–7.
Khor D, Inaba K, Aiolfi A, Delapena S, Benjamin E, Matsushima K, et al. The impact of helmet use on outcomes after a motorcycle crash. Injury. 2017;48(5):1093–7.
Kim S, Ro YS, Shin SD, Song KJ, Hong KJ, Jeong J. Preventive effects of motorcycle helmets on intracranial injury and mortality from severe road traffic injuries. Am J Emerg Med. 2018;36(2):p173–8.
Wiznia DH, Kim CY, Dai F, Goel A, Leslie MP. The effect of helmets on motorcycle outcomes in a level 1 trauma center in Connecticut. Traff Inj Prev. 2016;17(6):633–7.
Solagberu BA, Ofoegbu CKP, Nasir AA, Ogundipe OK, Adekanye AO, Abdur-Rahman LO. Motorcycle injuries in a developing country and the vulnerability of riders, passengers and pedestrians. Inj Prev. 2006;12(4):266–8.
Branas CC, Knudson MM. Helmet laws and motorcycle rider death rates. Accid Anal Prev. 2001;33(5):641–8.
Sosin DM, Sacks JJ, Holmgreen P. Head injury-associated deaths from motorcycle crashes. J Am Med Assoc. 1990;264:2395–9.
Sisimwo P, Mwaniki P, Bii C. Crash characteristics and injury patterns among commercial motorcycle users attending Kitale level IV district hospital, Kenya. Pan African Med J. 2014;19:296.
Sisimwo P, Onchiri G. Epidemiology of head injuries and helmet use among motorcycle crash injury: a quantitative analysis from a local hospital in Western Kenya. Pan Afr Med J. 2018;31:70.
Saidi H, Mutisto B. Motorcycle injuries at a tertiary referral hospital in Kenya: injury patterns and outcome. Eur J Trauma Emerg Surg. 2013;39(5):481–5.
Osifo O, Osagie T, Iribhogbe P. Pediatric road traffic accident deaths presenting to a Nigerian referral center. Prehosp Disaster Med. 2012;27(2):136–41.
Akaateba M, Amoh-Gyimah R, Yakubu I. A cross-sectional observational study of helmet use among motorcyclists in Wa, Ghana. Accid Anal Prev. 2014;64:18–22.
Safer Africa. African-European dialogue platform on road safety; 2020. Available from: http://www.saferafrica.eu/en/
Aromataris E. In: Munn Z, editor. JBI Manual for Evidence Synthesis. JBI; 2020. Available from: https://synthesismanual.jbi.global. https://doi.org/10.46658/JBIMES-20-01.
World Bank. Countries and Economies; 2019. [cited 30 Nov 2020] Available from: https://data.worldbank.org/country
United Nations. UN Regulation No. 22 sets Safety Requirements for Helmets; 2016. Available from:. https://doi.org/10.18356/7be0c920-en.
Mogaka EO, Ng’ang’a Z, Oundo J, Omolo J, Luman E. Factors associated with severity of road traffic injuries, Thika, Kenya. Pan-Afri Med J. 2011;8:20. https://doi.org/10.4314/pamj.v8i1.71076.
Oginni F, Ugboko V, Ogundipe O, Adegbehingbe B. Motorcycle-related maxillofacial injuries among Nigerian intracity road users. J Oral Maxillofac Surg. 2006;64(1):56–62.
Matheka D, Omar F, Kipsaina C, Witte J. Road traffic injuries in Kenya: a survey of commercial motorcycle drivers. Pan Afr Med J. 2015;21:17.
Oluwadiya K, Ojo O, Adegbehingbe O, Mock C, Popoola O. Vulnerability of motorcycle riders and co-riders to injuries in multi-occupant crashes. Int J Inj Control Saf Promot. 2014;23(2):189–96.
Joanna Briggs Institute. Checklist for Analytical Cross Sectional Studies Critical Appraisal Checklist for Analytical Cross Sectional Studies 2; 2017a. [cited 30 Nov 2020]. Available from: https://joannabriggs.org/sites/default/files/2019-05/JBI_Critical_Appraisal-Checklist_for_Analytical_Cross_Sectional_Studies2017_0.pdf
Joanna Briggs Institute. Checklist for Prevalence Studies; 2017b. [cited 30 Nov 2020]. Available from: https://joannabriggs.org/sites/default/files/2019-05/JBI_Critical_Appraisal-Checklist_for_Prevalence_Studies2017_0.pdf
Nzegwu M, Aligbe J, Banjo A, Akhiwui W, Nzegwu C. Patterns of morbidity and mortality amongst motorcycle riders and their passengers in Benin-City Nigeria: one-year review. Ann Afr Med. 2008;7(2):82–5.
Osoro ME, Nganga Z, Oundo J, Omolo J, Luman E. Factors associated with road traffic injuries, Thika, Kenya. Pan Afr Med J. 2011;8(20):1–8.
Karuppanagounder K, Vijayan AV. Motorcycle helmet use in Calicut, India: user behaviors, attitudes, and perceptions. Traff Inj Prev. 2016;17(3):292–6.
Bedru D, Teshome F, Kebede Y, Birhanu Z. Helmet wearing behavior where people often ride motorcycle in Ethiopia: a cross-sectional study. PLoS One. 2022;17(1):e0262683. https://doi.org/10.1371/journal.pone.0262683.
National Center for Statistics and Analysis. (2020). Motorcycle Helmet Use in 2019 – Overall Results. (Traffic Safety Facts Research Note. Report No. DOT HS 812 936). National Highway Traffic Safety Administration.
Ha NT, Ederer D, Vo V, Pham AV, Mounts A, Nolen LD, et al. Changes in motorcycle-related injuries and deaths after mandatory motorcycle helmet law in a district of Vietnam. Traff Inj Prev. 2018;19(1):75–80. https://doi.org/10.1080/15389588.2017.1322203.
Bachani A, Hung Y, Mogere S, Akunga D, Nyamari J, Hyder A. Helmet wearing in Kenya: prevalence, knowledge, attitude, practice and implications. Public Health. 2017;144:S23–31.
McSwain NE, Belles A. Motorcycle helmets - medical costs and the law. J Trauma. 1990;30(10):1189–97.
Tanyitiku BS, Tindong M, Agbor V, Haman M, Fondong A, Ditah C, et al. Determinants of helmet and protective wear utilization among motorcycle drivers and passengers in Bamenda, Cameroon: a hospital-based, cross-sectional study. East Central Afr J Surg. 2020. https://doi.org/10.4314/ecajs.v25i3.5.
Akinpelu O, Oladele A, Amusa Y, Ogundipe O, Adeolu A, Komolafe E, et al. Review of Road Traffic Accident Admissions in a Nigerian Tertiary Hospital. East Central Afr J Surg. 2007;12(1):63–7.
Carlson M, Morrison R. Study design, precision, and validity in observational studies. J Palliat Med. 2009;12(1):77–82.
Levin K. Study design III: cross-sectional studies. Evidence-Based Dentistry. 2006;7(1):24–5.
Pandis N. Cross-sectional studies. Am J Orthod Dentofac Orthop. 2014;146(1):127–9.
Setia MS. Methodology series module 3: cross-sectional studies. Indian J Dermatol. 2016;61(3):261–4. https://doi.org/10.4103/0019-5154.182410.
Ackaah W, Afukaar F, Agyemang W, Anh TT, Hejar AR, Abdul G, et al. The use of non-standard motorcycle helmets in low- and middle-income countries: a multicenter study. Injury Prevention. 2013;19(3):158–63.
Thomas P, Welsh R, Mavromatis S, Folla F, Laiou A, Yannis G. Survey results: road safety data, data collection systems and definitions. Report prepared for safer Africa, 2018. Retrieved from: http://www.saferafrica.eu/media/1868/sa-ntua-wp4-d41.pdf.
Hedt B, Pagano M. Health indicators: eliminating bias from convenience sampling estimators. Stat Med. 2011;30(5):560–8.
Oluwadiya K, Kolawole I, Adegbehingbe O, Olasinde A, Agodirin O, Uwaezuoke S. Motorcycle crash characteristics in Nigeria: implication for control. Accid Anal Prev. 2009;41(2):294–8.
La Torre G, Bertazzoni G, Zotta D, Van Beeck E, Ricciardi G. Epidemiology of accidents among users of two-wheeled motor vehicles. A surveillance study in two Italian cities. Eur J Public Health. 2002;12(2):99–103.
McSween-Cadieux E, Dagenais C, Ridde V. A deliberative dialogue as a knowledge translation strategy on road traffic injuries in Burkina Faso: a mixed-method evaluation. Health Res Policy Syst. 2018;16(1):113.
Bonnet E, Nikiéma A, Traoré Z, Sidbega S, Ridde V. Technological solutions for an effective health surveillance system for road traffic crashes in Burkina Faso. Glob Health Action. 2017;10:1295698.
Adeloye D, Thompson JY, Akanbi MA, Azuh D, Samuel V, Omoregbe N, et al. The burden of road traffic crashes, injuries and deaths in Africa: a systematic review and meta-analysis. Bull World Health Organ. 2016;94(7):510–521A. https://doi.org/10.2471/BLT.15.163121.
Chiu WT, Kuo CY, Hung CC, Chen M. The effect of the Taiwan motorcycle helmet use law on head injuries. Am J Public Health. 2000;90(5):793–6. https://doi.org/10.2105/ajph.90.5.793.
La Torre G, Van Beeck E, Bertazzoni G, Ricciardi W. Head injury resulting from scooter accidents in Rome: differences before and after implementing a universal helmet law. Eur J Pub Health. 2007;17(6):607–11.
Mayrose J. The effects of mandatory motorcycle helmet law on helmet use and injurypatterns among motorcyclist fatalities. J Saf Res. 2008;39(4):429–32. https://doi.org/10.1016/jsr.2008.07.001.
Passmore J, Tu N, Luong M, Chinh N, Nam N. Impact of mandatory motorcycle helmet wearing legislation on head injuries in Viet Nam: results of a preliminary analysis. Traff Inj Prev. 2010;11(2):202–6.
Servadei F, Begliomini C, Gardini E, Giustini M, Taggi F, Kraus J. Effect of Italy's\motorcycle helmet law on traumatic brain injuries. Inj Prev. 2003;9(3):257–60.
World Health Organization (2015a). Global status report on road safety 2015. [cited 30 Nov 2020]. Available from: https://www.who.int/violence_injury_prevention/road_safety_status/2015/GSRRS2015_Summary_EN_final.pdf
Acknowledgements
The authors would like to thank Vicky Duncan, University of Saskatchewan Librarian, Liaison to Dentistry, Public Health, and Community Health & Epidemiology for assisting with the search strategy for this study. We would also like to thank Hayelom Gebrekirstos Menegesha, BSc, MSc, MPH for providing advice regarding the meta-analysis.
Funding
Not applicable.
Author information
Authors and Affiliations
Contributions
NA Responsible for searching the literature, selecting articles, data extraction and writing of reports, as well as a first draft of the manuscript. She also reviewed the near final version of the manuscript. TP Responsible for being the secondary reviewer (searching the literature, article selection). She also reviewed the near final version of the manuscript. PP Conceptualized and developed the study, oversaw the methodology, review of the findings, and data interpretation, as well revising the near final manuscript draft. AC Conceptualized and developed the study, oversaw the methodology, review of the findings, and data interpretation, as well as writing the manuscript (and all revisions). All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
REB approval was not required to undertake this systematic literature review.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: Appendix I.
Search Strategy.
Rights and permissions
This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Abdi, N., Robertson, T., Petrucka, P. et al. Do motorcycle helmets reduce road traffic injuries, hospitalizations and mortalities in low and lower-middle income countries in Africa? A systematic review and meta-analysis. BMC Public Health 22, 824 (2022). https://doi.org/10.1186/s12889-022-13138-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12889-022-13138-4