
Abstract
Background
Parents play a key role in young children’s physical activity and physical literacy development. Little research has explored parent-focused interventions to improve young children’s physical literacy. We examined if a theory-based, feasible physical literacy training workshop (PLAYshop) for parents could improve their physical literacy knowledge and confidence and improve parenting practices related to facilitating the physical literacy development of their preschool-aged child (3-5 years). The secondary objective was to explore implementation facilitators and barriers.
Methods
We conducted a pragmatic controlled trial in two Canadian cities (Edmonton and Victoria) from November 2019 – March 2020. A total of 143/151 parents were eligible and assigned to intervention (n = 71) or control group (n = 72). The PLAYshop included: (i) a 75-min in-person workshop with interactive activities and physical literacy educational messages, (ii) educational materials, (iii) an equipment pack, and (iv) two post-workshop booster emails. Surveys measured parents’ knowledge and confidence at baseline and follow-up. Application of PLAYshop concepts and implementation facilitators and barriers were explored with interviews of parents and workshop leaders. Repeated measures ANOVAs and thematic analyses were completed.
Results
Parents’ knowledge and confidence improved significantly over time; intervention group changes were significantly greater than control group changes (p < 0.001; ɳ2 = .32). Parents applied PLAYshop concepts at-home, including child-led play, making activities fun, and promoting child manipulative and locomotor skills. Time was a key parental implementation barrier. Program implementation issues varied by context (location and participants).
Conclusions
PLAYshop participation changed parents’ physical literacy knowledge and confidence and physical literacy enhancing play with their children. Implementation feasibility was high. The findings from this real-world trial highlight an efficacious and scalable intervention that warrants further testing.
Trial registration
ClinicalTrials.gov: NCT04394312. Registered 19/05/2020.
Similar content being viewed by others


Background
Physical activity in early childhood, the first 5 years of life, is associated with direct health benefits including improved motor and cognitive development as well as psychosocial and cardiometabolic health [1]. Unfortunately, many children internationally fail to meet physical activity guidelines [2]. Concomitantly, evidence suggests that children are lacking some of the foundational elements (i.e., movement competence, motivation, confidence, knowledge and/or understanding) that are necessary to engage in physical activity [3,4,5]. These elements are part of a comprehensive and holistic construct called physical literacy [6].
The understandings of physical literacy vary internationally, however common themes include philosophical underpinnings, core elements (motivation, confidence, physical competence, knowledge and understanding), and a life course perspective [7]. This is reflected in the International Physical Literacy Association (IPLA) definition of physical literacy, informed by Whitehead [8], as “the motivation, confidence, physical competence, knowledge and understanding to value and take responsibility for engagement in physical activities for life” [6]. Physical literacy incorporates many of the critical determinants of behavioral action from established theoretical paradigms (e.g., cognitive and humanistic) in health psychology (see Rhodes et al. [9] for an overview of the most relevant theories), similar to other meta-theoretical frameworks used in implementation science such as the Behaviour Change Wheel [10, 11]). Increasing research supports the targeting of physical literacy to address the childhood physical inactivity crisis. As a result, it is gaining attention from governments and organizations worldwide [12, 13]. Physical literacy is mutually inclusive of physical activity [14, 15], however it is underscored by its integration of various influences on physically active participation, including physical capabilities (e.g., Fundamental Movement Skills [FMS]) as well as affective (e.g., self-esteem and motivation) and cognitive elements (e.g., knowledge and understanding of movement and active play) [7, 15].
Although physical literacy is a life course concept, early childhood represents a significant window of opportunity for its development. First, theories of development [16, 17] and prior studies [18,19,20] suggest that younger children have high confidence in their ability to perform physical movements despite their actual motor competence. Positive self-perceptions are important for the physical activity trajectories of children during this time as they will be more likely to engage in active play pursuits, thus developing their physical capabilities, and affective and cognitive elements of physical literacy that support successive participation [16, 17]. A recent meta-analysis of 12 longitudinal studies found a positive association between FMS and physical activity in early childhood [21]. Actual motor competence and perceptions of motor competence are associated during childhood and thus mutually supportive [22]. Second, basic motor skill movements (e.g., striking, basic throwing, simple kicking, running and jumping) are developed during early childhood [23]. These are essential for learning more complex movements later in life [24], therefore children’s physical capabilities are an important target during this crucial time period. Lastly, physical activity throughout early childhood establishes positive patterns and routines that support participation in physical activity throughout the life course [16, 17, 25, 26].
To date, only a small number of studies have explored programs that promote physical literacy in early childhood. A 2021 systematic review of physical literacy interventions identified only four that targeted children under the age of five; all of which focused exclusively on childcare centers [27]. While these are important settings for intervention, several governing bodies –including the World Health Organization (WHO) [13] and Canada’s Sport for Life [23]– have highlighted the importance of meaningful engagement of parents in supporting young children on their physical literacy journey. Such endorsements are based on a growing body of research that highlights parents’ strong influence on their children’s physical activity-related behaviors [5, 28,29,30]. In a 2020 systematic review of the correlates of parental support for child physical activity [30], it was recommended that future interventions focus on “cognitive-behavioral approaches” of parental support for children’s physical activity as this had the highest evidence of association. Therefore, improving parents’ knowledge, confidence and play practices to encourage and facilitate their child’s physical literacy development offers considerable potential. Although several early childhood physical activity interventions have addressed and/or integrated parents – for example, ‘Healthy Dads Healthy Kids’ [31, 32] and the mother-daughter ‘MADE4Life’ program [33] – physical literacy was not addressed explicitly or comprehensively with little to no focus on parents’ cognitive-behavioral skills.
Drawing on the current evidence base and the noticeable gaps, we developed a brief, multi-strategy, theory-based physical literacy intervention (the PLAYshop) to influence parents' facilitation of their child’s physical literacy development. A recent one-group pretest-posttest study of parents with children aged 3-8 years revealed the feasibility of the PLAYshop [34]. Parents’ self-reported knowledge and confidence had significantly increased (p < 0.05) following participation and 95.6% intended to engage with their child in suggested activities. The majority of parents (81.8%) found the program very to extremely useful and acceptable, and 95% were satisfied or extremely satisfied with both the workshop content and delivery. This small-scale study provided valuable insight, however its methodological limitations, including lack of a control group and small sample size, restricted any conclusions of intervention efficacy. The following paper describes the subsequent controlled trial that was undertaken using more rigorous methods and with a larger sample of parents.
This study aimed to evaluate the preliminary efficacy of a theory-based, feasible and potentially scalable physical literacy intervention for parents of preschool-aged children (aged 3-5 years). The specific objectives are detailed below.
-
1.
The primary objective was twofold: a) To determine if the PLAYshop increases parents’ knowledge and confidence. Based on previous evidence [30, 34, 35] and behavior change theories [10, 36], we hypothesized that parents in the intervention group will have a larger increase in levels of knowledge and confidence in regards to engaging in meaningful play with their preschool child(ren) than parents in the control group. b) To explore whether the PLAYshop improves parenting practices related to facilitating their child’s physical literacy development. We hypothesized that parents will report satisfaction with the implementation and change parenting practices related to physical activity at 2-month follow-up.
-
2.
The secondary objective was to explore implementation facilitators and barriers.
-
3.
The tertiary objective was to examine intervention effects on theoretical mechanisms of change (beliefs, perceived barriers, outcome expectations and perceived availability of resources). No specific hypotheses were developed.
Methods
This study is reported in accordance with the TREND statement for reporting nonrandomized/quasi-experimental evaluations of behavioral and public health interventions [37]. It was retrospectively registered with the clinical trials registry maintained by the National Library of Medicine at the National Institutes of Health (ClinicalTrials.gov identifier NCT04394312).
Study design and setting
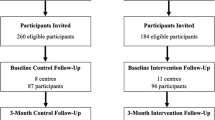
We used a type 1 effectiveness-implementation hybrid research design [38] to explore the preliminary efficacy of the PLAYshop and determine its potential for real world use. A two-arm controlled trial was conducted in the Canadian cities of Edmonton, Alberta (AB) and Victoria, British Columbia (BC) from November 2019 to March 2020. Figure 1 outlines the study procedures used for intervention and control groups. PLAYshop workshops were scheduled in advance at recreation centers and other community sites throughout the 4-month study period. The method used to allocate participants to either intervention or control group differed by region: BC participants were randomly assigned using a computer-generated 1:1 sequence and parents were provided with two choices for intervention workshop times; AB participants were systematically assigned using an alternating sequence as they enrolled and were provided with a list of workshop dates to choose from. Each approach was considered most feasible within that particular jurisdiction to balance groups and prevent wait-times that were anticipated to otherwise impact workshop attendance rates. To facilitate recruitment retention and the ethical treatment of control group participants, the control group in each cohort of recruits was booked in a delayed workshop and completed both pre- and post-test measures concurrent with the intervention participants who received the workshop in between (see Fig. 1).

Study procedures for intervention and control groups
Participants were blinded to group assignment however allocation concealment was not performed for those delivering the intervention due to limited resources (i.e., staff). To ensure intervention fidelity researchers were trained and delivered the PLAYshop using a pre-described program plan for the 75-min with added time points for each key message and related activities (i.e., fidelity checklist). Quantitative data (study objective 1a and 3) and qualitative data (study objective 1b and 2) were collected from participants and workshop leaders. Ethics approval was obtained from the University of Victoria (16-444) and University of Alberta (00093764). Written informed consent was received from participating parents and workshop leaders. All workshops from mid-March 2020 onwards were cancelled due to the COVID-19 pandemic, which halted recruitment and quantitative data collection. Workshops were not scheduled to resume due to public health restrictions and projected pandemic timelines.
Participants and recruitment
Parent participants were recruited during the study period using informational posters placed in community recreation centers, daycare centers, and preschools (AB & BC); Facebook and Twitter posts (AB & BC); posters attached within a local electronic newsletter (AB); and posters emailed to parent playgroups (BC). Eligible parents had to live within a workshop delivery area and have at least one child aged 3-5 years. Parents and siblings outside the age range from the same family were welcome to co-participate, however data were collected from only one parent (self-selection). The initial sample size was set at a total of 100 parents (50 control and 50 intervention), providing an estimated 0.80 power for a medium to large effect size with alpha set at 0.05 for a t-test between two independent means. Workshop leaders (all five; members of the research team) were additionally recruited to address study objective 2.
Intervention
A description of the PLAYshop development including theoretical underpinnings and a detailed logic model has been published elsewhere [34]. Briefly, the PLAYshop aimed to build parents’ knowledge and confidence to assist their child to develop physical literacy and acquire physical activity through play. Bandura’s social cognitive theory [36] broadly informed intervention design. The Behaviour Change Wheel [10, 11] was used to map the factors (capabilities, opportunities, and motivation of behavior [COM-B]) to identified barriers of parents’ target behavior. Potential implementation strategies were identified and assessed in terms of their affordability, practicality, effectiveness, cost-effectiveness, acceptability, side-effects/safety and equity [11], and with consideration of scalability (including adaptation to fit other contexts) from the onset [39, 40]. Table 1 is an extension from the feasibility study [34], describing the selected implementation strategies and the specific behavior change technique(s) used to address factors hypothesized to influence parents’ adoption of target behaviors. Strategy 3 (the provision of material resources) and strategy 4 (follow-up support) were added following the feasibility study to enhance contact time.
The core component of the PLAYshop was a 75-min in-person workshop during which trained leaders provided parents and their child with physical literacy education and experiential learning (strategy 1). The workshop template and content were developed by a member of the research team (PJN) in collaboration with a local BC physical literacy agency (Pacific Institute of Sport Excellence [PISE]) using a combination of the best available evidence and first-hand experience. The active play activities were based on resources and training developed for preschool-aged children by experts in physical education and early years childcare [23, 41, 42] and based on formative qualitative research with childcare providers. Prior to refinement for evaluative research, the PLAYshop underwent an iterative process of feasibility testing for physical literacy content, adult behavior change techniques and delivery format. The resulting template was used to provide structure and maintain fidelity to the core concepts of physical literacy across settings.
The workshop targeted parent’s knowledge, confidence, competence and motivation to engage in purposeful play activities and games that developed their child’s physical literacy. The workshop exposed them and their child to a full range of playful activities (n = 19 + 12 adaptations) to support the development of FMS (8 locomotor, 7 manipulative and 4 balance/stability). Within those, a variety of play or movement forms were also incorporated; for instance, pretend play (e.g., pretending to jump over a river, walk on a log or move like an animal) and movement to music. The workshop was embedded with an emphasis on: a) enhancing confidence and motivation through messages and demonstrations about challenge and adaptations; b) enhancing knowledge and motivation through role modeling, co-activity and following the child’s interest (choice); and c) education about how each activity influenced physical literacy inclusive of all physical literacy domains [6,7,8]. Play and play-based learning [43] – helping parents to create a joyful understanding of movement and play within their children was at the core of the workshop. This has been described more generally as tacit or experiential knowledge [44, 45] or, specific to physical literacy, categorized as comprehension of movement [46]. A play-based approach reflects pre-school children’s developmental stage and recommendations for physical literacy interventions to incorporate opportunities for pre-school children to engage in play [47]. The role of parents was both to facilitate and co-participate in active play rather than engaging in more structured motor skill development and teaching of codified knowledge that occurs in education and sport settings [23]. Other physical literacy concepts were delivered within and between activities through key parent messages which are identified following with their related child-level physical literacy components and domains (PLC/D):
-
Fun, playfulness and play motivates children’s engagement (PLC/D: motivation/affect).
-
Choice is important; follow your child’s interests where possible and let them choose the level of challenge they are comfortable with. (PLC/D: motivation and confidence/affect).
-
Use a variety of activities and create many opportunities and an ‘invitation’ for children to move. (PLC/D: motivation/affect).
-
◦ Manipulative skills are important to ongoing engagement in moderate, vigorous, physical activity and it is possible to do manipulative skills safely indoors with soft materials like balloons, scarves and paper balls and sticks. (PLC/D: FMS/physical).
-
-
Many activities can be played both indoors and outdoors with inexpensive, accessible, simple home-made equipment. (PLC/D: FMS/physical).
-
Avoid equipment or activities that may result in children getting hurt or developing negative associations (e.g., use soft materials such as scarves or balloons to practice catching). (PLC/D: confidence and motivation/affect).
-
Start with small, achievable activities as initial success is important for children’s confidence.(PLC/D: confidence/affect).
-
Modify activities to increase the level of ‘challenge’ where needed. This will facilitate continual development of skills and assist with motivation. (PLC/D: confidence/affect).
-
Be a role model and be playful; children love to play with their parent(s) and this will assist to build the parent-child connection. (PLC/D: motivation/affect).
-
Outdoor play is important; children move more in larger spaces and nature facilitates exploration, challenge and curiosity. (PLC/D: FMS and motivation/physical and affect).
Quantitative data collection
Participants in the intervention group completed paper surveys in-person, immediately before and after their participation in the workshop. Participants in the control group completed online surveys a minimum of seven days apart prior to workshop attendance using a REDCap® [48] personalized link sent via email (Fig. 1). The outcome measures were chosen as indicators of parents’ capability, motivation and opportunity [10] targeted by the PLAYshop.
Parent characteristics
Baseline surveys collected parent characteristics including age, sex, level of education, number of children, and previous training in a similar topic. Additional questions explored parents’ modeling of physically active behaviors using three items from the Activity Support Scale for Multiple Groups (ACTS-MG) [49], and parents’ co-participation with their child using four items from the psychometrically validated physical activity parenting practices (PAPP) item bank [50].
Parents’ knowledge and confidence (study objective 1a)
The primary outcomes of interest were parents’ self-reported knowledge and confidence assessed at baseline and follow-up. Individual scale items focused on key physical literacy constructs derived from Canada’s Sport for Life [23] and PISE physical literacy experts (see Additional file 1). Knowledge was assessed via nine items measured on a 5-point Likert scale (1 = no knowledge to 5 = a lot of knowledge). Confidence was assessed via 11 items measured on a 5-point Likert scale (1 = no confidence to 5 = a lot of confidence). Cronbach alpha (α) tests at baseline and follow-up revealed acceptable values of reliability for knowledge (0.92 and 0.94) and for confidence (0.93 and 0.95) [51].
Mechanisms of change (study objective 3)
Parents’ beliefs, perceived barriers, outcome expectations and perceived availability of resources were assessed at baseline and follow-up using items, in their original format or modified for the parent perspective, from a previous instrument with high measures of internal consistency and test-retest reliability [52]. Each item was measured on a 5-point Likert scale from 1 = strongly disagree to 5 = strongly agree. Parents’ beliefs was assessed via four items (baseline α = 0.89; follow-up α = 0.81), perceived barriers via five items (baseline α = 0.50; follow-up α = 0.58); and outcome expectations via three items (baseline α = 0.86, follow-up α = 0.79). Perceived availability of resources focused on a unique PLAYshop target measured via a single item: Do you feel you have the resources (e.g., information, equipment, space, etc.) you need to promote physical activity and physical literacy for your children?; measured on a 5-point Likert scale from 1 = Yes, I have all of the resources I need to 5 = No, I don’t have the resources I need.
Quantitative data analysis
SPSS Version 21.0 was used to analyze all quantitative data. Descriptive statistics were generated for all outcome measures and one-way ANOVA was used to determine if there were any significant differences between the groups in baseline characteristics. To address study objective 1a and 3, repeated measures ANOVA were used to determine if outcome variables changed over time across groups and if changes differed significantly between intervention and control groups (group-by-time intervention effect). Statistical significance was set a priori at p < 0.05. Effect sizes were reported as partial eta squared (η2) with a small, medium and large effect indicated by values of 0.01, 0.06 and 0.14 [53].
Qualitative data collection
To address study objective 1b (changes in parenting practices) and study objective 2 (implementation facilitators and barriers), an experienced interviewer (MP or MK) conducted 5-10 min semi-structured telephone interviews. Parents from the intervention group were invited to partake in an interview two months following workshop attendance. Open-ended questions focused on their application of workshop learnings at-home, including what activities they had performed and what had made it difficult and/or easy to do so. For the study objective 2, workshop leaders were also interviewed in May 2020 to explore facilitators and barriers of workshop implementation and areas for improvement. All interviews were digitally recorded, transcribed verbatim, de-identified and uploaded into QSR NVivo [54] for thematic analysis.
Qualitative data analysis
Qualitative data were inductively analyzed following the process recommended for multi-disciplinary health research [55]. Two members of the research team independently coded interviews and developed a working analytical framework. Where possible, data were charted into an NVivo [54] matrix to support interpretation of causes, consequences and relationships [56]. The research team discussed and reached negotiated consensus regarding any controversial codes or categorizations, and confirmed the proposed final themes. Concurrent with this process, parent interviews were deductively analyzed to explore the breadth of workshop elements applied at-home (frequencies reported).
Data authenticity was transparently affirmed through data display, exploring deviant cases and establishing trustworthiness of the findings using four quality concepts: credibility, transferability, dependability and confirmability [57]. Credibility and transferability were addressed through a rich and accurate description of the participants, context and setting. Credibility was further established through prolonged engagement of the research team with parents and in the delivery setting. Dependability and confirmability were addressed through the verification of transcript accuracy by interviewees, the use of triangulation across researchers during coding and interpretation, member checks with workshop leaders, and peer debriefing.
Results
Quantitative findings
Figure 2 details the progression of participants through recruitment, group allocation, follow- up and analysis. Of the 151 parents assessed for eligibility, four did not meet our criteria and four declined to participate. The remaining 143 parents were assigned to either the intervention group (n = 71) or control group (n = 72).

PRISMA flow diagram of participants’ progression through recruitment, group allocation, follow-up and analysis
For the control group, 69% (n = 50) of parents provided survey data and 47% (n = 34) proceeded to take part in a workshop (68% of survey respondents). For the intervention group, 55% of parents (n = 39) provided survey data; all of whom participated in a workshop and 33 (46%) of whom participated in the two-month follow-up interview (i.e., complete quantitative and qualitative data). Failure to receive the workshop was the result of disinterest following reading the letter of information (LOI), no-show, or COVID-19 cancellations. Of note, interested families were allocated to a group when sent the LOI because the LOI was different for the intervention group and control group. These families (intervention n = 15; control n = 16) who failed to receive the workshop never consented to participate. A total of 89 (62%) parents provided complete survey data across groups (average age 36.1 years; 93% female; 14% with prior training in physical literacy; 2.01 average children per household). The characteristics of parents at baseline were not significantly different between groups (Table 2).
Parents’ knowledge and confidence (study objective 1a)
Table 3 shows the group-by-time significant intervention effects found for parents’ self-reported knowledge and confidence (p < 0.001) represented by large effect sizes (ɳ2 = .32). Parents’ self-reported knowledge and confidence improved significantly from baseline to follow-up in both the intervention and control group; however, the changes in the intervention group were significantly greater than those in the control group (data not shown).
Mechanisms of change (study objective 3)
Significant group-by-time intervention effects, represented by medium-large effect sizes, were also found for parents’ perceived barriers (p = .031; ɳ2 = .07) and perceived availability of resources (p < 0.001; ɳ2 = .19), but not for beliefs (p = .364; ɳ2 = .01) and outcome expectations (p = .312; ɳ2 = .01) (Table 3). Scores for parents’ perceived barriers, perceived availability of resources, self-reported beliefs, and outcome expectations improved from baseline to follow-up in both the intervention and control group. These changes in the intervention group were significantly greater for all measures with the exception of outcome expectations (data not shown).
Qualitative findings
Thirty-three parents from the intervention group participated in an interview; 26 of whom verified their interview transcript. All five workshop leaders participated in an interview and verified their transcript.
Parenting practices (study objective 1b)
Parents reported a variety of workshop activities performed at-home with their child (see Table 4). The most common was manipulative skill activities, with 26 parents reporting at least one activity that fell within this category, followed by activities related to locomotor skills (n = 13), balance/stability/creativity (n = 11), and multiple-skills at one time (n = 9; for example, an activity that involved both balance and jumping). All interviewed parents stated that they were likely to continue performing physical literacy activities at-home with their child.
Parents also revealed their application of several key workshop messages at-home (see Table 5). For example, several parents cited that they had engaged in activities that were: fun/enjoyable experiences (n = 11), participated in whilst outdoors (n = 9), used minimal or inexpensive equipment (n = 13), child-led (n = 5) and challenging (n = 3). Ten parents mentioned that their child experienced additional benefits (beyond physical literacy skill development) by participating in workshop-related activities.
Implementation barriers and facilitators (study objective 2)
Parent perspectives
Parents experienced numerous facilitators and/or barriers to implementing PLAYshop activities at-home (see Table 6). Themes that arose as facilitators included the simple and inclusive nature of activities, the minimal/inexpensive equipment needed to carry out these activities, and the ability to undertake activities without child enrolment in a special program. Themes that arose as barriers included busy schedules/lack of time, limited indoor space, younger siblings, sustainability difficulties, unfavorable weather, and the short attention span of some children. COVID-19 was mentioned in several interviews as either a facilitator or a barrier. For example, several parents indicated that the increased time spent at-home provided an opportunity to engage in PLAYshop activities (facilitator) whereas some parents felt the disruption to regular schedules made it challenging to facilitate active play opportunities (barrier).
Workshop leader perspectives
Thematic analysis revealed several key facilitators and barriers to workshop implementation (see Table 7). Facilitators related to attributes of the workshop itself (starting with active play, working as a team with other leaders, the presence of strong/adaptable leaders, maintaining the tempo/flow, focusing on equipment that is easy to find and/or make, and providing parents with ‘goody bags’) or the workshop context (champion within the workshop site, engaged parents, children in attendance, and favorable physical spaces). Barriers were primarily related to the workshop context, including parents who were unengaged or felt shy to participate, issues with recruitment and low attendance rates, children’s disruptive or distracting behavior and parents struggling to manage this, unfavorable physical spaces (setting), and parking issues.
Discussion
Leading organizations such as the WHO [13] have suggested that physical activity promoters should engage parents in their child’s physical literacy journey, however, few evidence-based programs were available to assist this. The multi-strategy PLAYshop intervention provides one such option, with high ratings of acceptability and suggested efficacy [34]. The current controlled trial expanded upon a prior feasibility study of the PLAYshop, using a more robust design, in a larger population and within an additional region. Compared to controls, significantly larger improvements for the intervention group were found in parents’ self-reported knowledge, confidence, perceived barriers and perceived availability of resources. Following the workshop, parents also reported engaging in workshop-related activities at-home with their child. Collectively, these findings establish the preliminary efficacy (measured at the parent-level) of the PLAYshop as a promising intervention option for the development of physical literacy in early childhood.
Our positive findings build on those established in the prior feasibility study [34]. However, the current trial explored an improved PLAYshop intervention with two new strategies (material resources and follow-up support) to support parent’s application of workshop learnings at-home. This change appeared to address the ‘lack of follow-up’ previously reported as a significant implementation challenge [34]. No parent expressed difficulty recollecting workshop learnings and/or implementing suggested activities at-home, and workshop leaders reported that the new strategies were indeed a prominent facilitator to implementation. However, several previously identified implementation challenges remained: recruitment issues in the Victoria region, unfavorable workshop spaces and children as a distraction despite the presence of a workshop co-leader. Further action to address these prior to scale-up should be considered and may be informed by investigating cross-regional experiences (e.g., the AB region did not have any issues with recruitment) and trials of similar physical activity interventions with reported success. For example, a recent feasibility trial of a lifestyle intervention for preschool aged children and their fathers [58] used a structured, multi-component, and targeted recruitment campaign that allowed the research team to exceed targets, achieving ≥60% recruitment of the eligible population. Similar to our workshop, the Healthy Dads Healthy Kids intervention also used a co-facilitator for parent-child dyad sessions to assist in the management of group activities [31]. The parent/child interaction varied across workshops and potential need for enhanced child management strategies should be planned for.
Our parent-level results are commensurate with that of previous parent-focused physical activity interventions targeting children’s FMS [32, 33, 58, 59]. However, children’s FMS was one of many targeted behaviors of these interventions, only two of which included FMS, one amidst several physical literacy components, as an outcome measure [58, 59]. Further, these interventions typically emphasized parents’ personal lifestyle behaviors and parent cognitive behavioral approaches was secondary. Evidence suggests that parent’s personal physical activity behaviors are less indicative of their support for children’s physical activity behaviors compared to social cognitive correlates such as their intentions, planning and perceived control [30] as well as encouragement, involvement and facilitation [60]. Theoretically, it was particularly important that parents in the PLAYshop were not only made more aware of how to develop their child’s physical literacy (physical capabilities, affective and cognitive elements), but also had enhanced knowledge and confidence to do so. This aim appeared to be achieved; parents demonstrated increased knowledge and confidence and the types of activities they performed at-home with their child were congruent with the workshop teachings. These are important findings in light of the significant relationship between parental self-efficacy and children’s physical activity [61].
Previous parent-focused physical activity interventions have also been more extensive, time-consuming, and/or resource intensive programming approaches. The PLAYshop offers a brief program focused on activities that can be performed at-home using easily accessible household items and requiring less of parent’s time in the program. Such characteristics are well-suited to address identified barriers of parents influencing preschool-aged children’s physical activity such as cost, opportunity, insufficient time and transportation [61]. However, it should be noted that while the workshop was ‘brief’ (accommodating for the barrier of time) and we supplemented with booster emails, there were still recruitment challenges in one jurisdiction and time remained a barrier to implementation in the home. With competing demands for attention in busy family lives (e.g., parent work commitments, travel, and having more than 1 child [62]) dedicating time for active play, regardless of how simple, remained a challenge. In our study, parents in the intervention group significantly improved in scores for perceived barriers and perceived availability of resources compared to controls. This is consistent with our qualitative findings that parent’s application of workshop learnings was facilitated by the minimal/inexpensive equipment required, simplicity of activities, and ability to perform activities at-home. The PLAYshop may effectively enable parents to overcome barriers and access resources to successfully engage in suggested activities. The potential of the PLAYshop to address multiple barriers may be particularly valuable seeing as the quantity of barriers experienced by parents has been found to be inversely proportional to the physical activity levels of children [61].
We found no significant intervention effect for parents’ beliefs or outcome expectations. This may reflect a ceiling effect: the mean baseline scores were no more than 1.75 below the maximum possible score for both of these measures (20 for beliefs and 15 for outcome expectations). Similarly, a pilot randomized controlled trial of the 8-week Mothers and Daughters Exercising for Life program found no intervention effect for mothers’ beliefs or outcome expectations, with negligible changes from baseline to follow-up [33]. This may be attributable to recruitment bias, at least in our study (see limitations following), however it is likely that the positive outcomes of physical activity are generally known by parents. In a cross-sectional survey of 663 Canadian mothers, 58% ranked physical activity as the first or second most important activity for their child - slightly higher than homework and far higher than other activities (e.g., music/arts = 14%; peer socializing = 13%, and family time = 39%) [63]. Another cross-sectional survey of 483 Canadian parents showed that 79% believed ‘health’ was an important reason to engage with their child in physically active behaviors [64]. Parents’ beliefs and outcome expectations may have less impact driving behavior change compared to other theoretical mechanisms of change, although further research is needed in this regards.
A unique aspect of this study was the workshop timing allowing us to explore the impact of COVID-19 lockdown restrictions during the study. COVID-19 was reported by several parents as either a facilitator (more time spent at-home and increased motivation) or a barrier (disturbed routine and difficulty balancing lifestyle changes) to their application of workshop learnings at-home. These findings complement a cross-sectional study by Moore and colleagues [65] that used an online survey of 1472 Canadian parents to explore the immediate impact of COVID-19 restrictions on movement and play behaviors in Canadian children and youth (5-17 years). The majority of parents reported their child as being ‘a lot less’ active due to COVID-19 restrictions, with significant declines in children’s time spent in physical activity, play and sport. However, several parents also reported adopting new hobbies or accessing new resources. Further analysis showed that parental encouragement, support, and engagement were positively associated with increased physical activity [65]. The PLAYshop successfully improved parent’s knowledge and confidence to engage in play with their child and emphasized the use of accessible household items – this appeared to be of substantial benefit under COVID-19 restrictions.
Limitations
There are several study limitations that warrant acknowledgement. The AB region chose a systematic approach for group assignment to address challenges that were anticipated with the immediate scheduling of both intervention and control workshops in this jurisdiction. Although randomization is considered the gold standard for group allocation in controlled research trials, it is not always practical for public health research [37]. Another limitation was the retrospective registration of the trial after the date of the last workshop which ended unexpectedly due to the COVID-19 pandemic. However, no data was analyzed prior to trial registration. Further limitations include the following: (i) the research team was not blinded to group allocation due to their involvement with intervention delivery and data collection; (ii) fathers were underrepresented (93% of survey respondents were female) with evaluations most often completed by a female partner despite attendance by some fathers; (iii) the use of self-report surveys may be subject to social desirability bias, especially since those in the intervention group were completed with research staff available nearby (however this did provide the opportunity for parents to seek assistance if any survey question was unclear); (iv) the surveys were expert-driven but not sufficiently validated; (v) there was a limited review and feedback from a more diverse range of physical literacy experts (e.g., researchers and/or physical literacy groups in other regions) which may have improved content validity; (vi) the α scores of perceived barriers were in the lower range for reliability however still considered ‘fair’ [51]; (vii) there is a possibility of selection bias due to self-recruitment of participants as parents in this study typically agreed that they enjoyed physical activity and thus may differ significantly from those who did not choose to participate; and finally, (viii) the apriori sample size was based on an estimate, although post-hoc power analysis and the significant small to medium size effects detected indicate that the actual sample size was adequate and allowed us to detect differences between the groups. Our effect sizes were similar to a previous physical activity parenting practices study which reported small to medium effect sizes for measures of parents’ socio-cognitive measures, ranging from a Cohen’s d of 0.24 for support to − 0.45 for self-efficacy [33]. It is possible that the PLAYshop may have attracted parents who were already inclined to engage in active play with their child.
Future directions and recommendations
This trial forms the second in a series of studies to optimize the PLAYshop for dissemination – that is, to develop the most effective and resource-efficient option [66]. Through this process, findings from the current study are used to inform improvements to both the intervention and to research processes, including addressing limitations where possible. For example, resolving insufficient representation of fathers in childhood health and physical activity research has been flagged as a research priority [35, 67]. Future research should incorporate father-specific recruitment strategies and methods to improve their response rates. Similarly, targeting those parents less engaged in physical activity will ensure a more representative evaluation sample. There are also opportunities to improve data collection methods (e.g., validating the surveys would improve the rigor of results) and to increase parent’s exposure to messaging and activity ideas with additional follow-up support strategies (e.g., a smartphone app).
The current trial was conducted largely in a controlled research setting with the research team driving recruitment and workshop delivery. Future research should be conducted in more ‘real-world’ conditions to test the effectiveness of the PLAYshop [68]. This could be achieved by using a train-the-trainer model and/or engaging external delivery partners to extend intervention reach and the delivery context beyond the research team. This would also provide implementation infrastructure support which is considered essential for successful scale-up [40]. Moreover, in light of the recent COVID-19 pandemic it will be important to test other scalable workshop formats (e.g., online/web-based) that are under development and less likely to be impacted by public health restrictions. This will also provide those parents who were unable to receive the workshop in the current study with an opportunity to participate.
The current study is one of very few targeting parents as gatekeepers for physical literacy, and the first of its kind to use a brief and feasible workshop to improve parents’ knowledge and confidence to do so. Therefore, this study provides a valuable contribution to an emerging field of work; however, several key empirical questions remain unaddressed, and should be a future priority in parent-focused physical literacy research. For example, whether parent’s physical literacy parenting practices impact on their child’s physical activity and physical literacy (objectively measured). It is also important to explore the impact of socio-economic status and ethnicity as these factors may significantly influence home life and the opportunities that children are provided by parents to develop physical literacy.
Conclusion
We established that a 75-min, co-facilitated workshop with parent resources and follow-up boosters was effective in improving parents’ physical literacy-related knowledge and confidence. The workshop also appeared to meet other intervention targets – with a positive impact on parents’ perceived barriers, perceived availability of resources, self-reported parenting practices, and participation in suggested activities at-home. This study provides a valuable contribution for an emerging field of work and may be used to inform future research, policy and practice. Its findings are pivotal for optimizing the PLAYshop for future evaluation and scale-up.
Availability of data and materials
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- FMS:
-
Fundamental movement skills
- WHO:
-
World Health Organization
- AB:
-
Alberta
- BC:
-
British Columbia
- PISE:
-
Pacific Institute of Sport Excellence
- ACTS-MG:
-
Activity Support Scale for Multiple Groups
- PAPP:
-
Physical activity parenting practices
References
Carson V, Lee E-Y, Hewitt L, Jennings C, Hunter S, Kuzik N, et al. Systematic review of the relationships between physical activity and health indicators in the early years (0-4 years). BMC Public Health. 2017;17(5):854.
Aubert S, Brazo-Sayavera J, González SA, Janssen I, Manyanga T, Oyeyemi AL, et al. Global prevalence of physical activity for children and adolescents; inconsistencies, research gaps, and recommendations: a narrative review. Int J Behav Nutr Phys Act. 2021;18(1):81.
Active healthy kids Australia (AHKA). 2018 AHKA report card on physical activity for children and Young people (long-form): University of South Australia; 2018.
Tremblay MS, Longmuir PE, Barnes JD, Belanger K, Anderson KD, Bruner B, et al. Physical literacy levels of Canadian children aged 8–12 years: descriptive and normative results from the RBC learn to play–CAPL project. BMC Public Health. 2018;18(2):1036.
ParticipACTION. The 2020 ParticipACTION report card on physical activity for children and youth. Toronto: ParticipACTION; 2020. Available from: https://www.participaction.com/en-ca/resources/children-and-youth-report-card.
International physical literacy association. Physical literacy definition. 2017. Available from: https://www.physical-literacy.org.uk/.
Shearer C, Goss HR, Edwards LC, Keegan RJ, Knowles ZR, Boddy LM, et al. How is physical literacy defined? A contemporary update. J Teach Phys Educ. 2018;37(3):237–45.
Whitehead M. Physical literacy: throughout the lifecourse: Routledge; 2010.
Rhodes RE, McEwan D, Rebar AL. Theories of physical activity behaviour change: a history and synthesis of approaches. J Sport Exerc Psychol. 2019;42:100–9.
Michie S, Johnston M, Francis J, Hardeman W, Eccles M. From theory to intervention: mapping theoretically derived behavioural determinants to behaviour change techniques. Appl Psychol. 2008;57(4):660–80.
Michie S, Atkins L, West R. The behaviour change wheel. 1st ed. Great Britain: Silverback Publishing; 2014.
Tremblay MS, Costas-Bradstreet C, Barnes JD, Bartlett B, Dampier D, Lalonde C, et al. Canada’s physical literacy consensus statement: process and outcome. BMC Public Health. 2018;18(2):1034.
World Health Organization. Global action plan on physical activity 2018–2030: more active people for a healthier world. Geneva: World Health Organization; 2018.
Cairney J, Dudley D, Kwan M, Bulten R, Kriellaars D. Physical literacy, physical activity and health: toward an evidence-informed conceptual model. Sports Med. 2019;49(3):371–83.
Edwards LC, Bryant AS, Keegan RJ, Morgan K, Jones AM. Definitions, foundations and associations of physical literacy: a systematic review. Sports Med. 2017;47(1):113–26.
Harter S. Effectance motivation reconsidered. Toward a developmental model. Hum Dev. 1978;21(1):34–64.
Stodden DF, Goodway JD, Langendorfer SJ, Roberton MA, Rudisill ME, Garcia C, et al. A developmental perspective on the role of motor skill competence in physical activity: an emergent relationship. Quest. 2008;60(2):290–306.
Brian A, Bardid F, Barnett LM, Deconinck FJ, Lenoir M, Goodway JD. Actual and perceived motor competence levels of Belgian and United States preschool children. J Mot Learn Dev. 2018;6(s2):S320–S36.
Lopes V, Barnett L, Rodrigues L. Is there an association among actual motor competence, perceived motor competence, physical activity, and sedentary behavior in preschool children? J Mot Learn Dev. 2016;4(2):129–41.
LeGear M, Greyling L, Sloan E, Bell RI, Williams B-L, Naylor P-J, et al. A window of opportunity? Motor skills and perceptions of competence of children in kindergarten. Int J Behav Nutr Phys Act. 2012;9(1):1–5.
Jones D, Innerd A, Giles EL, Azevedo LB. Association between fundamental motor skills and physical activity in the early years: a systematic review and meta-analysis. J Sport Health Sci. 2020;9(6):542–52.
De Meester A, Barnett LM, Brian A, Bowe SJ, Jimenez-Diaz J, Van Duyse F, et al. The relationship between actual and perceived motor competence in children, adolescents and young adults: a systematic review and meta-analysis. Sports Med. 2020;50(11):2001–49.
Higgs C, Cairney J, Jurbala P, Dudley D, Way R, Mitchell D. Developing physical literacy—Building a new normal for all Canadians. 2019. Available from: https://sportforlife.ca/portfolio-view/developing-physical-literacy-building-a-new-normal-for-all-canadians/.
Gabbard C. Lifelong motor development: Lippincott Williams & Wilkins; 2021.
Craigie AM, Lake AA, Kelly SA, Adamson AJ, Mathers JC. Tracking of obesity-related behaviours from childhood to adulthood: a systematic review. Maturitas. 2011;70(3):266–84.
World Health Organization. Guidelines on physical activity, sedentary behaviour and sleep for children under 5 years of age. Geneva: World Health Organization; 2019.
Carl J, Barratt J, Töpfer C, Cairney J, Pfeifer K. How are physical literacy interventions conceptualized?–a systematic review on intervention design and content. Psychol Sport Exerc. 2021;58:102091.
Brown HE, Atkin AJ, Panter J, Wong G, Chinapaw MJ, Van Sluijs E. Family-based interventions to increase physical activity in children: a systematic review, meta-analysis and realist synthesis. Obes Rev. 2016;17(4):345–60.
Messing S, Rütten A, Abu-Omar K, Ungerer-Röhrich U, Goodwin L, Burlacu I, et al. How can physical activity be promoted among children and adolescents? A systematic review of reviews across settings. Front Public Health. 2019;7:55.
Rhodes RE, Perdew M, Malli S. Correlates of parental support of child and youth physical activity: a systematic review. Int J Behav Med. 2020;27(6):36–46.
Morgan PJ, Lubans DR, Plotnikoff RC, Callister R, Burrows T, Fletcher R, et al. The'Healthy dads, healthy Kids' community effectiveness trial: study protocol of a community-based healthy lifestyle program for fathers and their children. BMC Public Health. 2011;11(1):876.
Morgan PJ, Collins CE, Plotnikoff RC, Callister R, Burrows T, Fletcher R, et al. The ‘healthy dads, healthy kids’ community randomized controlled trial: a community-based healthy lifestyle program for fathers and their children. Prev Med. 2014;61:90–9.
Barnes AT, Plotnikoff RC, Collins CE, Morgan PJ. Feasibility and preliminary efficacy of the MADE4Life program: a pilot randomized controlled trial. J Phys Act Health. 2015;12(10):1378–93.
Lane C, Carson V, Morton K, Reno K, Wright C, Predy M, et al. A real-world feasibility study of the PLAYshop: a brief intervention to facilitate parent engagement in developing their child’s physical literacy. Pilot Feasibility Stud. 2021;7(1):113.
Rhodes RE, Guerrero MD, Vanderloo LM, Barbeau K, Birken CS, Chaput J-P, et al. Development of a consensus statement on the role of the family in the physical activity, sedentary, and sleep behaviours of children and youth. Int J Behav Nutr Phys Act. 2020;17(1):1–31.
Bandura A. Social foundations of thought and action. Englewood Cliffs, NJ: Prentice-Hall Inc; 1986.
Des Jarlais DC, Lyles C, Crepaz N, Group T. Improving the reporting quality of nonrandomized evaluations of behavioral and public health interventions: the TREND statement. Am J Public Health. 2004;94(3):361–6.
Curran GM, Bauer M, Mittman B, Pyne JM, Stetler C. Effectiveness-implementation hybrid designs. Med Care. 2012;50(3):217–26.
World Health Organization & ExpandNet. Beginning with the end in mind: planning pilot projects and other programmatic research for successful scaling up. Geneva: World Health Organization; 2011.
Milat A, Lee K, Conte K, Grunseit A, Wolfenden L, Van Nassau F, et al. Intervention scalability assessment tool: a decision support tool for health policy makers and implementers. Health Res Policy Syst. 2020;18(1):1–17.
Naylor P-J, Temple VA. Enhancing the capacity to facilitate physical activity in home-based child care settings. Health Promot Pract. 2013;14(1):30–7.
Bélanger M, Humbert L, Vatanparast H, Ward S, Muhajarine N, Chow AF, et al. A multilevel intervention to increase physical activity and improve healthy eating and physical literacy among young children (ages 3-5) attending early childcare centres: the healthy start-Départ Santé cluster randomised controlled trial study protocol. BMC Public Health. 2016;16(1):1–10.
Barblett L, Knaus M, Barratt-Pugh C. The pushes and pulls of pedagogy in the early years: competing knowledges and the erosion of play-based learning. Aust J Early Child. 2016;41(4):36–43.
Kothari A, Rudman D, Dobbins M, Rouse M, Sibbald S, Edwards N. The use of tacit and explicit knowledge in public health: a qualitative study. Implement Sci. 2012;7(1):1–12.
Connell N, Klein JH, Powell PL. It's tacit knowledge but not as we know it: redirecting the search for knowledge. J Oper Res Soc. 2003;54(2):140–52.
Shortt CA, Webster CA, Keegan RJ, Egan CA, Brian AS. Operationally conceptualizing physical literacy: results of a Delphi study. J Teach Phys Educ. 2019;38(2):91–104.
Foulkes JD, Foweather L, Fairclough SJ, Knowles Z. “I wasn’t sure what it meant to be honest”—formative research towards a physical literacy intervention for preschoolers. Children. 2020;7(7):76.
Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG. Research electronic data capture (REDCap)—a metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform. 2009;42(2):377–81.
Davison KK, Li K, Baskin ML, Cox T, Affuso O. Measuring parental support for children's physical activity in white and African American parents: the activity support scale for multiple groups (ACTS-MG). Prev Med. 2011;52(1):39–43.
Mâsse LC, O’Connor TM, Lin Y, Carbert NS, Hughes SO, Baranowski T, et al. The physical activity parenting practices (PAPP) item Bank: a psychometrically validated tool for improving the measurement of physical activity parenting practices of parents of 5–12-year-old children. Int J Behav Nutr Phys Act. 2020;17(1):1–17.
Shrout PE. Measurement reliability and agreement in psychiatry. Stat Methods Med Res. 1998;7(3):301–17.
Heitzler CD, Martin SL, Duke J, Huhman M. Correlates of physical activity in a national sample of children aged 9–13 years. Prev Med. 2006;42(4):254–60.
Fritz CO, Morris PE, Richler JJ. Effect size estimates: current use, calculations, and interpretation. J Exp Psychol Gen. 2012;141(1):2.
QSR International Pty Ltd. NVivo (released March 2020), Available from: https://www.qsrinternational.com/nvivo-qualitative-data-analysis-software/home.
Gale NK, Heath G, Cameron E, Rashid S, Redwood S. Using the framework method for the analysis of qualitative data in multi-disciplinary health research. BMC Med Res Methodol. 2013;13(1):117.
Patton MQ. Qualitative Research & Evaluation Methods 3ed. Thousand Oaks, CA: SAGE Publications; 2002.
Lincoln Y, Guba EG. Naturalistic inquiry. Newbury Park, CA: SAGE Publications; 1985.
Morgan PJ, Collins CE, Barnes AT, Pollock ER, Kennedy S-L, Drew RJ, et al. Engaging fathers to improve physical activity and nutrition in themselves and in their preschool-aged children: the “healthy youngsters, healthy dads” feasibility trial. J Phys Act Health. 2021;18(2):175.
Morgan PJ, Young MD, Barnes AT, Eather N, Pollock ER, Lubans DR. Engaging fathers to increase physical activity in girls: the “dads and daughters exercising and empowered”(DADEE) randomized controlled trial. Ann Behav Med. 2018;53(1):39–52.
Sohun R, MacPhail A, MacDonncha C. Physical activity parenting practices in Ireland: a qualitative analysis. Sport Educ Soc. 2021;26(3):281–94.
Smith BJ, Grunseit A, Hardy LL, King L, Wolfenden L, Milat A. Parental influences on child physical activity and screen viewing time: a population based study. BMC Public Health. 2010;10(1):593.
Hamilton K, Hatzis D, Kavanagh DJ, White KM. Exploring parents’ beliefs about their Young Child’s physical activity and screen time Behaviours. J Child Fam Stud. 2015;24(9):2638–52.
Rhodes RE, Berry T, Craig CL, Faulkner G, Latimer-Cheung A, Spence JC, et al. Understanding parental support of child physical activity behavior. Am J Health Behav. 2013;37(4):469–77.
Rhodes RE, Lim C. Promoting parent and child physical activity together: elicitation of potential intervention targets and preferences. Health Educ Behav. 2018;45(1):112–23.
Moore SA, Faulkner G, Rhodes RE, Brussoni M, Chulak-Bozzer T, Ferguson LJ, et al. Impact of the COVID-19 virus outbreak on movement and play behaviours of Canadian children and youth: a national survey. Int J Behav Nutr Phys Act. 2020;17(1):1–11.
Wolfenden L, Bolsewicz K, Grady A, McCrabb S, Kingsland M, Wiggers J, et al. Optimisation: defining and exploring a concept to enhance the impact of public health initiatives. Health Res Policy Syst. 2019;17(1):1–13.
Morgan PJ, Young MD. The influence of fathers on Children’s physical activity and dietary behaviors: insights, recommendations and future directions. Curr Obes Rep. 2017;6(3):324–33.
Milat AJ, Bauman AE, Redman S, Curac N. Public health research outputs from efficacy to dissemination: a bibliometric analysis. BMC Public Health. 2011;11(1):1–9.
Acknowledgements
The authors are grateful for all parents that participated. The authors would also like to thank their community partners that supported recruitment and provided workshop space.
Funding
The study was funded by VC’s University of Alberta Killam Accelerator Research Award. The funding body had no role in the study design, collection, analysis or interpretation of data; or in writing the manuscript.
Author information
Authors and Affiliations
Contributions
First author CL led the development of this manuscript. PJN and PISE representatives conceived and developed the intervention concept. All authors contributed to the research design and trial methodology. PJN, MP, RR, KM, SH and VC advised on, and oversaw, implementation of the intervention. PJN, MP, MK and VC collected and analysed the data. CL, PJN, MP and VC interpreted the data. All authors contributed to and approved the final version of the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This trial received ethics approval from the University of Victoria Research Ethics Board (16-444) and University of Alberta Health Research Ethics Board (00093764). All methods were performed in accordance with relevant guidelines and regulations. Written informed consent were provided from all study participants.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1.
The survey scales used to assess parents’ knowledge and confidence.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Lane, C., Naylor, PJ., Predy, M. et al. Exploring a parent-focused physical literacy intervention for early childhood: a pragmatic controlled trial of the PLAYshop. BMC Public Health 22, 659 (2022). https://doi.org/10.1186/s12889-022-13048-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12889-022-13048-5