
Abstract
Background
Neonatal disorders (ND) are a significant global health issue. This article aimed to track the global trends of neonatal disorders in 204 countries/territories from 1990 to 2019.
Methods
Data was explored from the Global Burden of Disease study 2019. Estimated annual percentage change (EAPC) and age-standardized rate (ASR) were calculated to quantify the trends of neonatal disorders and their specific causes, mainly included neonatal preterm birth (NPB), neonatal encephalopathy due to birth asphyxia and trauma (NE), neonatal sepsis and other neonatal infections (NS), and hemolytic disease and other neonatal jaundice (HD).
Results
In 2019, there were 23,532.23 × 103 incident cases of ND, and caused 1882.44 × 103 death worldwide. During 1990–2019, trends in the overall age-standardized incidence rate (ASIR) of ND was relatively stable, but that of age-standardized death rate (ASDR) declined (EAPC = -1.51, 95% confidence interval [CI]: -1.66 to -1.36). Meanwhile, decreasing trends of ASDR were observed in most regions and countries, particularly Cook Islands and Estonia, in which the respective EAPCs were -9.04 (95%CI: -9.69 to -8.38) and -8.12 (95%CI: -8.46 to -7.77). Among the specific four causes, only the NPB showed decreasing trends in the ASIR globally (EAPC = -0.19, 95%CI: -0.26 to -0.11). Decreasing trends of ASDR caused by ND underlying specific causes were observed in most regions, particularly the HD in Armenia, with the EAPC was -13.08 (95%CI: -14.04 to -12.11).
Conclusions
Decreasing trends of death caused by neonatal disorders were observed worldwide from 1990 to 2019. However, the burden of neonatal disorders is still a considerable challenge, especially in low-resource settings, which need more effective health strategies.
Similar content being viewed by others


Introduction
Neonatal health is a critical global concern, reflecting the national and global progress and challenges of health systems. Over the past decades, significant progress had made in improving neonatal survival [1, 2], with the death decreased by 42.4% since1990, and caused 2.6 million deaths in 2015 [3]. Neonatal disorders ranked the second leading cause of YLLs (accounted for 1.78 million) in 2017, with a decrease of 24.1% since 2007 [4]. Dramatical progress in neonatal diseases was mainly due to socioeconomic factors, including economic growth, international collaboration, improved health systems and service [5,6,7].
However, the considerable disequilibrium of neonatal disorders was found across regions and countries, deeply dependent on the local demographics and socioeconomic status [2, 8, 9]. Neonatal diseases are still the leading public problems in low-resource settings, e.g., serious infections [10], neonatal encephalopathy, and neonatal preterm birth complications [11, 12]. In sub-Saharan Africa, neonatal sepsis caused an estimated 5.3–8.7 million disability-adjusted life-years (DALYs), and an economic burden of over 469 billion US dollars in 2014 [13]. The challenges of maternal malnutrition, poor living conditions, and health resources were still substantial [14,15,16]. Neonatal disorders were a critical part of the UN’s Sustainable Development Goals (SDG) [17], and their epidemiological patterns were essential to health decisions.
The Global Burden of Disease study (GBDs) comprehensively assessed and quantified the burden of diseases and causes globally, which provided an opportunity to track the changing trends of neonatal disorders. Therefore, this article aimed to estimate the trends of neonatal disorders and underlying specific causes from 1990 to 2019.
Methods
Study data
The GBD 2019 comprehensively assessed 369 diseases and injuries and risk factors for 204 countries/territories [18]. The GBD collaborators collect related data sources from censuses, civil registration, and vital statistics, and so on. The data is estimated using a Bayesian meta-regression tool named DisMod-MR model, which is detailly described in previous articles [3, 19]. Data on the incidence and death of neonatal disorders was explored through the Global Health Data Exchange query tool (http://ghdx.healthdata.org/gbd-results-tool). According to the GBD online tools instruction, data was collated by specific causes, and multiple geographic dimensions from 1990 to 2019, without any inclusion/exclusion criteria. The specific causes of neonatal disorders mainly included (1) neonatal preterm birth (NPB), (2) neonatal encephalopathy due to birth asphyxia and trauma (NE), (3) neonatal sepsis and other neonatal infections (NS), and (4) hemolytic disease and other neonatal jaundice (HD). The GBD study provided a comprehensive assessment of neonatal disorders worldwide, including 21 geographic regions (e.g., South Asia, Caribbean, and Central Europe), and 204 countries/territories (e.g. United Kingdom, China, and Greece). By the socio-demographic index (SDI), regions and countries were categorized into 5 levels, including low, low-middle, middle, high-middle, and high.
Statistical analysis
Age-standardization is a necessary and representative step when data involved in multiple population with different age structures or for the same population over time. The age-standardized rate (ASR)/100,000 population was estimated with the following formula:
In the above formula, ai meant the age-specific rate in the ith age group, w meant the number of people (or the weight) in the corresponding ith age group from among the selected reference standard population, and A meant the number of age groups.
Estimated annual percentage change (EAPC) is a well-accepted method of quantifying the trends of ASR, which have been wildly used in public health studies [20, 21]. A regression line was fitted to the natural logarithm of the rates. The EAPC and its 95% confidence interval (CI) were estimated using the linear regression model. The formulas were as following:
Thereinto, y = ln (ASR) and x = calendar year. The trends were determined as follows: 1) An increasing trend was determined if both EAPC and 95% CI were > 0; 2) a decreasing trend was determined if both EAPC and 95% CI were < 0; 3) Others were deemed to be “stable” over time. In order to explore the influential factors of EAPC, the associations between EAPCs and ASDR in 1990, and between EAPCs and HDI in 2019 were calculated using Pearson correlation analysis. Data were analyzed using R 3.6.2 (Lucent Technologies, Jasmine Mountain, USA). A p value of less than 0.05 was considered to be statistically significant.
Results
Trends in incidence and death of neonatal disorders
The incident number of neonatal disorders was 23,532.23 × 103 (95% uncertainty interval (UI): 21,672.53 × 103–25,701.96 × 103) worldwide in 2019, with a decrease of 0.26% since 1990. The overall trend in age-standardized incidence rate (ASIR) was relatively stable during 1990–2019. The decreasing incident trends were observed in low and low-middle SDI areas, particularly the letter (EAPC = -0.35, 95% CI: -0.41 to -0.29). Whereas increasing trends occurred in the high SDI areas, with the EAPC was 0.21 (95%CI: 0.11–0.31). At the regional level, decreasing trends were observed in nine regions, particularly Southeast Asia (EAPC = -0.57, 95%CI: -0.60 to -0.54). Conversely, increasing trends were seen in eight regions, and the most pronounced one occurred in Central Latin America (EAPC = 0.42, 95%CI: 0.33–0.50), followed by High-income Asia Pacific and East Asia (Table 1; Figs. 1A and 2A-B). A negative correlation was found between ASIRs and SDI in 2019 among regions (ρ = -0.69, p < 0.001; Fig. 3A). The ASIR of neonatal disorders in 2019 was heterogeneous among 204 countries/territories, ranging from 107.32/100,000 in Sweden to 612.02/100,000 in Yemen. 1990–2019, the percentages of incident numbers changed from -63.42% in Albania to 178.04% in Qatar. Decreasing trends of ASIR were observed in 115 countries/territories, particularly in Serbia and Paraguay, in which the respective EAPCs were -2.34 (95%CI: -2.58 to -2.10) and -1.52 (95%CI: -1.62 to -1.43). Whereas increasing trends were seen in 77 countries/territories, and the largest ones were Greece (EAPC = 3.35, 95% CI: 3.13–3.56), followed by North Macedonia, and Colombia (Supplementary table 1; Fig. 4A-C).

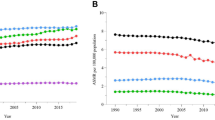
Trends in ASR of neonatal disorders globally, and in SDI areas and geographic regions, 1990–2019. A and (B) were that of incidence and death of neonatal disorders, respectively. ASR, age-standardized rate; EAPC, Estimated annual percentage change; SDI, sociodemographic index

The distribution of incidence and death of neonatal disorders in SDI areas and regions. A was the ASR of incidnece in SDI areas from 1990 to 2019; B was the incident number in geographical regions; C was the ASR of death in SDI areas; D was the death number in geographical regions. ASR, age-standardized rate SDI, sociodemographic index

The associations between ASRs of neonatal disorders and SDI among regions. A and (B) were that of incidence and death, respectively. ASRs were that of from 1990 to 2019, and the abscissa was SDI in 2019. The associations were calculated with Pearson correlation analysis. The symbols were the countries/territories in the corresponding regions. ASR, age-standardized rate; SDI, socio-demographic index

The distribution of ASR, percentage changes, and EAPCs of neonatal disorders incidence, 1990–2019. Countries/territories with an extreme value were annotated. ASR, age-standardized rate; EAPC, estimated annual percentage change
Globally, the death number of neonatal disorders decreased 37.38% between 1990–2019, and it was 1882.44 × 103 (95% UI: 1605.83 × 103–2237.48 × 103) in 2019. The age-standardized death rate (ASDR) decreased by an average 1.51% per year in 1990–2019 (EAPC = -1.51, 95%CI: -1.66 to -1.36). Decreasing trends of neonatal disorders were observed in all SDI areas and geographic regions, particularly Central Europe and East Asia, and their respective EAPCs were -5.10 (95%CI: -5.28 to -4.93) and -5.06 (95%CI: -5.52 to -4.59) (Table 1; Figs. 1B and 2C-D). A negative correlation was found between ASDRs and SDI in 2019 among regions (ρ = -0.89, p < 0.001; Fig. 3B). The ASDR of neonatal disorders in 2019 was heterogeneous among 204 countries/territories, ranging from 1.07/100,000 in Japan to 78.62/100,000 in Pakistan. In the past three decades, the percentage changes in number varied from -95.88% in the Cook Islands to 106.89% in Somalia. The trends of ASDR declined in 197 countries/territories, and the Cook Islands and Estonia had the most pronounced ones, with the respective EAPCs were -9.04 (95%CI: -9.69 to -8.38) and -8.12 (95%CI: -8.46 to -7.77). Conversely, increasing trends were seen in four countries, particularly Dominica (EAPC = 1.27, 95%CI: 1.02–1.53) (Supplementary table 1; Fig. 5A-C).

The distribution of ASR, percent changes, and EAPCs of death caused by neonatal disorders, 1990–2019. Countries/territories with an extreme value were annotated. ASR, age-standardized rate; EAPC, estimated annual percentage change
Trends in incidence and death of neonatal preterm birth (NPB)
During 1990–2019, the overall ASIR of NPB showed a decreasing trend (EAPC = -0.19, 95%CI: -0.26 to -0.11). Meanwhile, decreasing trends were observed in most SDI areas, and the most pronounced one was in the low-middle SDI area (EAPC = -0.66, 95%CI: -0.75 to -0.58). In contrast, only increasing one occurred in high SDI area (EAPC = 0.25, 95%CI: 0.13–0.38). At the regional level, decreasing trends were seen in nine geographic regions, particularly East Asia (EAPC = -0.76, 95%CI: -0.89 to -0.63). On the other hand, increasing trends were seen in nine regions, especially High-income Asia Pacific (EAPC = 0.46, 95%CI: 0.37–0.56) (Supplementary table 2; Fig. 1A, and Supplementary Fig. 1A-B). In 1990–2019, the percentage changes among 204 countries/territories ranged from -67.71% in Albania to 182.10% in Niger. Decreasing trends of ASIR were demonstrated in 104 countries/territories, and the largest ones were seen in Mozambique (EAPC = -1.82, 95%CI: -2.04 to -1.59), followed by Cambodia and Cuba. On the contrary, increasing trends were observed in eighty countries/territories, particularly Greece (EAPC = 3.91, 95%CI: 3.66–4.17) (Supplementary table 3; Supplementary Figs. 5A and 6A).
Globally, decreasing trends in the ASDR of NPB were observed worldwide in 1990–2019, with the EAPC of -2.09 (95%CI: -2.19 to -2.00). Meanwhile, decreasing trends also were seen in SDI areas and most regions, and the most pronounced ones were Eastern Europe and East Asia, and the respective EAPCs were -5.35 (95%CI: -5.69 to -5.02) and -5.32 (95%CI: -5.59 to -5.06) (Supplementary table 4; Fig. 1B, and Supplementary Fig. 1C-D). At the national level, the highest increasing percentage in death number of NPB was observed in Niger (105.52%) between 1990 and 2019. Whereas the largest decreasing one occurred in the Cook Islands (-97.15%). Decreasing trends in the ASDR of NPB were demonstrated in 188 countries/territories, and the largest one was seen in Cook Islands (EAPC = -10.23, 95%CI: -10.98 to -9.48), followed by Saudi Arabia and Czechia. Conversely, increasing trends were seen in 7 countries, especially Guam (EAPC = 1.93, 95%CI: 1.47–2.39) (Supplementary table 5; Supplementary Figs. 7A and 8A).
Trends in incidence and death of neonatal encephalopathy due to birth asphyxia and trauma (NE)
The overall ASIR of NE was relatively stable during 1990–2019. However, decreasing trends of ASIR were observed in most SDI areas and regions, particularly East Asia (EAPC = -3.90, 95%CI: -4.20 to -3.60) (Supplementary table 2; Fig. 1A, and Supplementary Fig. 2A-B). During 1990–2019, the percentage changes of NE were observed from -76.84% in China to 183.47% in Qatar. Decreasing trends were seen in 133 countries/territories, and the largest ones occurred in China (EAPC = -3.96, 95%CI: -4.27 to -3.66), followed by Indonesia and Nicaragua. Whereas increasing trends occurred in fifty-two ones, particularly Dominica (EAPC = 2.40, 95%CI: 2.34–2.47) (Supplementary table 3; Supplementary Figs. 5B and 6B).
Decreasing trend in the ASDR of NE was observed worldwide in 1990–2019 (EAPC = -1.16, 95%CI: -1.38 to -0.94). Meanwhile, decreasing trends were observed in SDI areas and most regions, particularly Central Europe (EAPC = -6.36, 95%CI: -6.56 to -6.15) (Supplementary table 4; Fig. 1B, and Supplementary Fig. 2C-D). Over the past three decades, the percentage changes in the death number of NE varied from -96.49% in Cook Islands to 139.53% in Somalia. Decreasing trends of ASDR were observed in 191 countries/territories, especially the Cook Islands and Hungary, with the EAPCs of -9.60 (95%CI: -10.29 to -8.90) and -9.44 (95%CI: -10.99 to -7.87). However, increasing trends were found in six countries, and the most pronounced one occurred in Dominica (EAPC = 2.05, 95%CI: 1.64–2.46) (Supplementary table 5; Supplementary Figs. 7B and 8B).
Trends in incidence and death of neonatal sepsis and other neonatal infections (NS)
The global trend in the ASIR of NS increased from 1990 to 2019, with the EAPC of 0.46 (95%CI: 0.43–0.48). Meanwhile, increasing trends were seen in SDI areas and most regions, particularly East Asia (EAPC = 2.16, 95%CI: 2.04–2.27). Whereas decreasing trends occurred in ten regions, and the most pronounced ones were in Southern Latin America (EAPCs = -1.71, 95%CI: -1.85 to -1.57) (Supplementary table 2; Fig. 1A, and Supplementary Fig. 3A-B). At the national level, the percentages in the incident number of NS changed from -78.64% in Serbia to 300.45% in North Macedonia during 1990–2019. Decreasing trends in the ASIR were demonstrated in 86 countries/territories, particularly Serbia (EAPC = -4.76, 95%CI: -5.26 to -4.26). On the other hand, increasing trends were seen in 101 countries/territories, and the most pronounced one was North Macedonia (EAPC = 8.41, 95%CI: 7.72–9.10), followed by Bulgaria and Lithuania (Supplementary table 3; Supplementary Figs. 5C and 6C).
The ASDR of NS showed a decreasing trend globally from 1990 to 2019 (EAPC = -0.53, 95%CI: -0.72 to -0.35). Decreasing trends of ASDR were observed in all SDI areas, especially the high SDI area (EAPC = -2.77, 95%CI: -2.98 to -2.55). Decreasing trends were seen in seventeen regions, and the largest ones were seen in Central Europe (EAPC = -4.58, 95%CI: -5.03 to -4.13). However, increasing trends were observed in three regions, including Central Asia, Caribbean, and Southern sub-Saharan Africa (Supplementary table 4; Fig. 1B, and Supplementary Fig. 3C-D). In 1990–2019, the percentages in NS number altered -93.00% in Greece from 227.49% in North Macedonia. Increasing trends were observed in thirty-eight countries/territories, and the largest one was seen in North Macedonia (EAPC = 9.31, 95%CI: 7.81–10.83), followed by Bulgaria and Taiwan. Conversely, decreasing trends were seen in 156 countries/territories, particularly Serbia and Greece, with the respective EAPCs were -8.66 (95%CI: -9.83 to -7.47) and -7.41 (95%CI: -9.32 to -5.46) (Supplementary table 5; Supplementary Figs. 7C and 8C).
Trends in incidence and death of hemolytic disease and other neonatal jaundice (HD)
The ASIR of HD showed an increasing trend over the past 30 years, with the EAPC of 0.13 (95%CI: 0.03–0.23). Meanwhile, increasing trends were also seen in low-middle and middle SDI areas. Whereas decreasing trends occurred in high-middle and high SDI areas, in which the respective EAPCs were -1.23 (95%CI: -1.57 to -0.90) and -1.84 (95%CI: -2.30 to -1.38). Among 21 regions, the most pronounced decreasing trends were observed in Eastern Europe (EAPC = -4.39, 95%CI: -5.17 to -3.61) (Supplementary table 2; Fig. 1A, and Supplementary Fig. 4A-B). During 1990–2019, the percentages altered from -98.22% in Libya to 179.84% in Afghanistan. There were 109 countries/territories had decreasing trends in the ASIR, and the most pronounced one was seen in Latvia (EAPC = -14.43, 95%CI: -16.64 to -12.16), followed by Montenegro and Libya. On the other hand, there were sixty ones had increasing trends, particularly the United Kingdom and Georgia, with the respective EAPCs were 0.71 (95%CI: 0.52–0.90) and 0.69 (95%CI: 0.64–0.75) (Supplementary table 3; Supplementary Figs. 5D and 6D).
Compared with other causes of neonatal disorders, HD had a most pronounced decreasing trend in the ASDR globally from 1990 to 2019 (EAPC = -2.78, 95%CI: -3.00 to -2.57). Meanwhile, decreasing trends of ASDR were observed in all SDI areas and regions, especially Central Europe (EAPC = -7.12, 95%CI: -7.37 to -6.86) (Supplementary table 4; Fig. 1B, and Supplementary Fig. 4C-D). In 1990–2019, the percentages in death number altered from -98.46% in Armenia to 64.24% in Somalia. Decreasing trends in the ASDR were observed in 200 countries/territories, and the largest one was seen in Armenia (EAPC = -13.08, 95%CI: -14.04 to -12.11), followed by the Cook Islands and Nicaragua. Furthermore, the trends were stable in the rest four countries/territories over time, including Azerbaijan, Guatemala, Zimbabwe, and Sri Lanka (Supplementary table 5; Supplementary Figs. 7D and 8D).
Analysis on the influential factors of EAPCs
The ASR in 1990 means the disease reservoir at baseline, and the HDI is a critical index reflecting the level of human development and health resources in regions and countries. At the national level, EAPCs had a negative association with the ASIR in 1990 (ρ = -0.32, p < 0.001, Fig. 6A), and a positive association with the HDI in 2019 (ρ = 0.32, p < 0.001; Fig. 6B). Meanwhile, in terms of death caused by neonatal disorders, EAPCs had a positive association with the ASDR in 1990 (ρ = 0.23, p < 0.001, Fig. 6C), and a negative association with HDI in 2019 (ρ = -0.48, p < 0.001, Fig. 6D).

The association between EAPCs of neonatal disorders and ASR in 1990, and between EAPCs and HDI in 2019. A is the association between EAPCs and ASIR in 1990; B is the association between EAPCs of incidence and HDI in 2019; C is the association between EAPCs and ASDR in 1990; D is the association between EAPCs of death and HDI in 2019. The associations were calculated with Pearson correlation analysis. The size of circle is increased with the numbers in 1990 and 2019, respectively. EAPC, estimated annual percentage change; ASIR, age-standardized incidence rate; ASDR, age-standardized death rate
Discussion
Neonatal health is an important public issue worldwide, which attracted huge funding, domestic policies, and international corporations in recent decades [22,23,24]. EAPC and ASR were used to demonstrate the changing trends of ND, facilitating the horizontally comparison among countries over a long-term interval. The results would be helpful to identify progress and obstacles in disease control, which informed the adjustment and formulation of health strategies. In the present article, the incident trends of neonatal disorders were relatively stable globally from 1990 to 2019, probably being impacted by the population growth, imbalanced allocation of resources, weak health systems, and local socio-economic factors [25,26,27]. The results showed that the burden of ND was significantly associated with the social and economic development status. Low and middle SDI settings undertook the heaviest burden, in where there faced rapid population growth, maternal malnutrition, high prevalence infections, lack of prenatal screening, and limited medical resources [28, 29]. The high morbidity and mortality caused a considerable economic cost, and also exacerbated the social welfare and resource [30], which became a vicious circle subsequently. Among specific causes, neonatal preterm birth had a decreasing incident trend probably related to the improved health systems [31, 32]. Whereas increasing trends were found in NS and HD from 1990 to 2019. The high prevalence of infectious diseases constantly threated the neonates in low- and middle-income countries [26], driving the increasing trends of NS. However, it was reported that the incidence and prevalence of alloimmune hemolytic disease had decreased over the past decades [33]. The difference between ours and the above studies were probably due to disease categories and data sources. Decreasing trends of neonatal disorders commonly occurred in the former Soviet Union countries, probably because of the reconstruction of economy and health systems in recent years, especially in Serbia [34, 35]. Meanwhile, primary healthcare and newborn screening effectively decreased the incidence of neonatal disorders in Paraguay [36, 37]. However, Greece had the largest increasing incident trends of neonatal disorders, in where the economic crisis in 2008 brought about considerable impacts on perinatal outcomes [38, 39]. Adolescent mothers were very common in north Macedonia, who had considerably higher frequencies of perinatal and neonatal disorders [40], and prenatal and maternity care were also influenced by racism and discrimination [41].
Decreasing trends of death caused by neonatal disorders were demonstrated worldwide, and in most regions and countries from 1990 to 2019, indicating that considerable progress in the decline of neonatal mortality during the past decades [42,43,44]. The reasons involved the improvement of mental health care, health infrastructure, and poverty elimination [45, 46]. However, the relatively slow trends occurred in low- and middle-SDI areas were also related to the high non-health government expenditure [47]. Meanwhile, substantial heterogeneity in trends were observed between regions and countries. The Pacific low- and middle-income countries had taken actions to improve to improve the quality of maternal and newborn care over the past decades, including improvements of health infrastructure, considerable financial investment, and training program of healthcare workers [48]. Several island countries launched the Early Essential Newborn Care program (EENC) introduced from the WHO [49]. Meanwhile, the international medical program [50], and the reproductive health study [51] probably promoted trends of neonatal disorders declined pronouncedly in Cook Islands. In Armenia, the reductions in infant mortality were due entirely to a decline in post-neonatal mortality [52]. Studies have linked the pronounced decreasing trends in China to rapid economic growth, rising maternal education, and health policies [5, 53]. In low-resource regions and countries still face increasing challenges of maternal and neonatal disorders for the health systems [54].
Several limitations in this study should be interpreted. First, the GBD estimates depended upon the quality and quantity of data, and the accuracy and reliability of the results were impacted by the potential bias due to misclassification and miscoding. Second, the diagnostic standards and measures of neonatal disorders and specific causes had refined over time, which also affected the estimation of trends. Last but not least, studies on neonatal disorders and specific causes were few in some countries, thus the causes of trends could not be fully discussed in those countries.
Conclusions
Neonatal disorders were a critical issue of the UN’s SDG. This article demonstrated the progress and challenges in the control and management of neonatal disorders using the GBD data. The results showed that global trends of death caused by neonatal disorders and its specific causes declined in most regions and countries from 1990 to 2019. However, the overall trend in the incidence of neonatal disorders declined slowly. The burden of neonatal disorders remained a considerable challenge to the global public health, particularly in low-resource settings. These findings highlighted the progress and challenges in the control and management of neonatal disorders, which would facilitate the adjustment of health strategies to the UN’s SDG at the global, regional, and national levels.
Availability of data and materials
All data were included in this article and its supplementary files. Public link to the database of GBD study is open, and data can be downloaded via the Global Health Data Exchange (GHDx) (http://ghdx.healthdata.org). which is supported by the Institute for Health Metrics and Evaluation (IHME), University of Washington, USA.
Abbreviations
- GBD:
-
Global Burden of Disease
- ND:
-
Neonatal disorders
- NPB:
-
Neonatal preterm birth
- NE:
-
Neonatal encephalopathy due to birth asphyxia and trauma
- NS:
-
Neonatal sepsis and other neonatal infections
- HD:
-
Hemolytic disease and other neonatal jaundice
- UN:
-
United Nations
- SDG:
-
Sustainable Development Goal
- EAPC:
-
Estimated annual percentage change
- GHDx:
-
Global health data exchange
- SDI:
-
Socio-demographic index
- ASR:
-
Age-standardized rate
- CI:
-
Confidence interval
- UI:
-
Uncertainty interval
References
Wang H, Liddell CA, Coates MM, Mooney MD, Levitz CE, Schumacher AE, Apfel H, Iannarone M, Phillips B, Lofgren KT, et al. Global, regional, and national levels of neonatal, infant, and under-5 mortality during 1990–2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet. 2014;384(9947):957–79.
Lozano R, Wang H, Foreman KJ, Rajaratnam JK, Naghavi M, Marcus JR, Dwyer-Lindgren L, Lofgren KT, Phillips D, Atkinson C, et al. Progress towards Millennium Development Goals 4 and 5 on maternal and child mortality: an updated systematic analysis. Lancet. 2011;378(9797):1139–65.
Collaborators GBDCM. Global, regional, national, and selected subnational levels of stillbirths, neonatal, infant, and under-5 mortality, 1980–2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet. 2016;388(10053):1725–74.
Collaborators GBDCoD. Global, regional, and national age-sex-specific mortality for 282 causes of death in 195 countries and territories, 1980–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2018;392(10159):1736–88.
Feng XL, Theodoratou E, Liu L, Chan KY, Hipgrave D, Scherpbier R, Brixi H, Guo S, Chunmei W, Chopra M, et al. Social, economic, political and health system and program determinants of child mortality reduction in China between 1990 and 2006: A systematic analysis. Journal of global health. 2012;2(1):010405.
Verguet S, Jamison DT. Estimates of performance in the rate of decline of under-five mortality for 113 low- and middle-income countries, 1970–2010. Health Policy Plan. 2014;29(2):151–63.
Global Burden of Disease C, Adolescent Health C, Kassebaum N, Kyu HH, Zoeckler L, Olsen HE, Thomas K, Pinho C, Bhutta ZA, Dandona L, et al. Child and Adolescent Health From 1990 to 2015: Findings From the Global Burden of Diseases, Injuries, and Risk Factors 2015 Study. JAMA pediatrics. 2017;171(6):573–92.
Burke M, Heft-Neal S, Bendavid E. Sources of variation in under-5 mortality across sub-Saharan Africa: a spatial analysis. Lancet Glob Health. 2016;4(12):e936–45.
Rajaratnam JK, Marcus JR, Flaxman AD, Wang H, Levin-Rector A, Dwyer L, Costa M, Lopez AD, Murray CJ. Neonatal, postneonatal, childhood, and under-5 mortality for 187 countries, 1970–2010: a systematic analysis of progress towards Millennium Development Goal 4. Lancet. 2010;375(9730):1988–2008.
Mulholland K. Serious infections in young infants in developing countries. Vaccine. 1998;16(14–15):1360–2.
Collaborators GBDCoD. Global, regional, and national age-sex specific mortality for 264 causes of death, 1980–2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet. 2017;390(10100):1151–210.
Deribew A, Tessema GA, Deribe K, Melaku YA, Lakew Y, Amare AT, Abera SF, Mohammed M, Hiruye A, Teklay E, et al. Trends, causes, and risk factors of mortality among children under 5 in Ethiopia, 1990–2013: findings from the Global Burden of Disease Study 2013. Popul Health Metrics. 2016;14:42.
Ranjeva SL, Warf BC, Schiff SJ. Economic burden of neonatal sepsis in sub-Saharan Africa. BMJ global health. 2018;3(1):e000347.
India State-Level Disease Burden Initiative Malnutrition C. The burden of child and maternal malnutrition and trends in its indicators in the states of India: the Global Burden of Disease Study 1990–2017. The Lancet Child & adolescent health. 2019;3(12):855–70.
El Bcheraoui C, Mimche H, Miangotar Y, Krish VS, Ziegeweid F, Krohn KJ, Ekat MH, Nansseu JR, Dimbuene ZT, Olsen HE, et al. Burden of disease in francophone Africa, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet Glob Health. 2020;8(3):e341–51.
Patel AB, Bann CM, Garces AL, Krebs NF, Lokangaka A, Tshefu A, Bose CL, Saleem S, Goldenberg RL, Goudar SS, et al. Development of the Global Network for Women’s and Children’s Health Research’s socioeconomic status index for use in the network’s sites in low and lower middle-income countries. Reprod Health. 2020;17(Suppl 3):193.
GBD Sdg Collaborators. Measuring progress from 1990 to 2017 and projecting attainment to 2030 of the health-related Sustainable Development Goals for 195 countries and territories: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2018;392(10159):2091–138.
GBD Diseases and Injuries Collaborators. Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet. 2020;396(10258):1204–22.
GBD Disease and Injury Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2018;392(10159):1789–858.
Ou ZJ, Yu DF, Liang YH, He WQ, Li YZ, Meng YX, Xiong HS, Zhang MY, He H, Gao YH, et al. Trends in burden of multidrug-resistant tuberculosis in countries, regions, and worldwide from 1990 to 2017: results from the Global Burden of Disease study. Infect Dis Poverty. 2021;10(1):24.
Hankey BF, Ries LA, Kosary CL, Feuer EJ, Merrill RM, Clegg LX, Edwards BK. Partitioning linear trends in age-adjusted rates. Cancer causes & control : CCC. 2000;11(1):31–5.
O’Hare B, Makuta I, Chiwaula L, Bar-Zeev N. Income and child mortality in developing countries: a systematic review and meta-analysis. J R Soc Med. 2013;106(10):408–14.
Jamison DT, Summers LH, Alleyne G, Arrow KJ, Berkley S, Binagwaho A, Bustreo F, Evans D, Feachem RG, Frenk J, et al. Global health 2035: a world converging within a generation. Lancet. 2013;382(9908):1898–955.
Dieleman JL, Templin T, Sadat N, Reidy P, Chapin A, Foreman K, Haakenstad A, Evans T, Murray CJ, Kurowski C. National spending on health by source for 184 countries between 2013 and 2040. Lancet. 2016;387(10037):2521–35.
Black RE, Victora CG, Walker SP, Bhutta ZA, Christian P, de Onis M, Ezzati M, Grantham-McGregor S, Katz J, Martorell R, et al. Maternal and child undernutrition and overweight in low-income and middle-income countries. Lancet. 2013;382(9890):427–51.
Mortality GBD. Causes of Death C: Global, regional, and national age-sex specific all-cause and cause-specific mortality for 240 causes of death, 1990–2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet. 2015;385(9963):117–71.
Collaborators GBDRF, Forouzanfar MH, Alexander L, Anderson HR, Bachman VF, Biryukov S, Brauer M, Burnett R, Casey D, Coates MM, et al. Global, regional, and national comparative risk assessment of 79 behavioural, environmental and occupational, and metabolic risks or clusters of risks in 188 countries, 1990–2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet. 2015;386(10010):2287–323.
GBD Under-5 Mortality Collaborators. Global, regional, and national progress towards sustainable development goal 3.2 for neonatal and child health: all-cause and cause-specific mortality findings from the global burden of disease study 2019. Lancet. 2021;398(10303):870–905.
Hug L, Alexander M, You D, Alkema L. UN Inter-agency Group for Child Mortality Estimation: National, regional, and global levels and trends in neonatal mortality between 1990 and 2017, with scenario-based projections to 2030: a systematic analysis. Lancet Glob Health. 2019;7(6):e710–20.
Alkire BC, Peters AW, Shrime MG. JG M: The Economic Consequences Of Mortality Amenable To High-Quality Health Care In Low- And Middle-Income Countries. Health Aff. 2018;37(6):988–96.
Usman AK, Wolka E, Tadesse Y, Tariku A, Yeshidinber A, Teklu AM, Senturia K, Gezahegn W, Litch JA. And the Every Preemie SEIRCG: Health system readiness to support facilities for care of preterm, low birth weight, and sick newborns in Ethiopia: a qualitative assessment. BMC Health Serv Res. 2019;19(1):860.
Murray CJ, Richards MA, Newton JN, Fenton KA, Anderson HR, Atkinson C, Bennett D, Bernabe E, Blencowe H, Bourne R, et al. UK health performance: findings of the Global Burden of Disease Study 2010. Lancet. 2013;381(9871):997–1020.
Ree IMC, Smits-Wintjens V, van der Bom JG, van Klink JMM, Oepkes D, Lopriore E. Neonatal management and outcome in alloimmune hemolytic disease. Expert Rev Hematol. 2017;10(7):607–16.
Footman K, Roberts B, Mills A, Richardson E, McKee M. Public satisfaction as a measure of health system performance: a study of nine countries in the former Soviet Union. Health Policy. 2013;112(1–2):62–9.
Bjegovic-Mikanovic V, Vasic M, Vukovic D, Jankovic J, Jovic-Vranes A, Santric-Milicevic M, Terzic-Supic Z, Hernandez-Quevedo C. Serbia: Health System Review. Health Syst Transit. 2019;21(3):1–211.
Dullak R, Rodriguez-Riveros MI, Bursztyn I, Cabral-Bejarano MS, Ruoti M, Paredes ME, Wildberger C, Molinas F. Primary Healthcare in Paraguay: overview and prospects. Ciencia & saude coletiva. 2011;16(6):2865–75.
Borrajo GJ. Newborn screening in Latin America at the beginning of the 21st century. J Inherit Metab Dis. 2007;30(4):466–81.
Zilidis C, Chadjichristodoulou C. Economic Crisis Impact and Social Determinants of Perinatal Outcomes and Infant Mortality in Greece. International journal of environmental research and public health. 2020;17(18):6606-18.
Zografaki I, Papamichail D, Panagiotopoulos T. Adverse effect of the financial crisis in Greece on perinatal factors. Eur J Pub Health. 2018;28(6):1116–21.
Rexhepi M, Besimi F, Rufati N, Alili A, Bajrami S, Ismaili H. Hospital-Based Study of Maternal, Perinatal and Neonatal Outcomes in Adolescent Pregnancy Compared to Adult Women Pregnancy. Open access Macedonian journal of medical sciences. 2019;7(5):760–6.
Janevic T, Sripad P, Bradley E, Dimitrievska V. “There’s no kind of respect here” A qualitative study of racism and access to maternal health care among Romani women in the Balkans. International journal for equity in health. 2011;10:53.
Cha S. The impact of the worldwide Millennium Development Goals campaign on maternal and under-five child mortality reduction: “Where did the worldwide campaign work most effectively?” Glob Health Action. 2017;10(1):1267961.
Wang Y, Li X, Zhou M, Luo S, Liang J, Liddell CA, Coates MM, Gao Y, Wang L, He C, et al. Under-5 mortality in 2851 Chinese counties, 1996–2012: a subnational assessment of achieving MDG 4 goals in China. Lancet. 2016;387(10015):273–83.
India State-Level Disease Burden Initiative Child Mortality C. Subnational mapping of under-5 and neonatal mortality trends in India: the Global Burden of Disease Study 2000–17. Lancet. 2020;395(10237):1640–58.
Gakidou E, Cowling K, Lozano R, Murray CJ. Increased educational attainment and its effect on child mortality in 175 countries between 1970 and 2009: a systematic analysis. Lancet. 2010;376(9745):959–74.
Dieleman JL, Schneider MT, Haakenstad A, Singh L, Sadat N, Birger M, Reynolds A, Templin T, Hamavid H, Chapin A, et al. Development assistance for health: past trends, associations, and the future of international financial flows for health. Lancet. 2016;387(10037):2536–44.
Baker P, Hone T, Reeves A, Avendano M, Millett C. Does government expenditure reduce inequalities in infant mortality rates in low- and middle-income countries?: A time-series, ecological analysis of 48 countries from 1993 to 2013. Health Econ Policy Law. 2019;14(2):249–73.
Wilson AN, Spotswood N, Hayman GS, Vogel JP, Narasia J, Elijah A, Morgan C, Morgan A, Beeson J. CSE H: Improving the quality of maternal and newborn care in the Pacific region: A scoping review. The Lancet regional health Western Pacific. 2020;3:100028.
Tosif S, Jatobatu A, Maepioh A, Gray A, Sobel H, Mannava P. T D: Healthcare worker knowledge and skills following coaching in WHO early essential newborn care program in the Solomon Islands: a prospective multi-site cohort study. BMC Pregnancy Childbirth. 2020;20(1):84.
Blattner K, Maoate K, Lloyd T, Iro E, Davidson S, Jacob M. Initial perspectives of New Zealand doctors: developing capacity and a training programme in the Cook Islands. J Prim Health Care. 2017;9(1):16–21.
Ekeroma AJ, Kenealy T, Shulruf B, McCowan LM, Hill A. Building reproductive health research and audit capacity and activity in the Pacific Islands (BRRACAP) study: methods, rationale and baseline results. BMC Med Educ. 2014;14:121.
Hakobyan M, Yepiskoposyan L. Infant mortality decline in Armenia: Why with uneven rates? Econ Hum Biol. 2010;8(1):134–7.
Meng Q, Xu L, Zhang Y, Qian J, Cai M, Xin Y, Gao J, Xu K, Boerma JT, Barber SL. Trends in access to health services and financial protection in China between 2003 and 2011: a cross-sectional study. Lancet. 2012;379(9818):805–14.
Gouda HN, Charlson F, Sorsdahl K, Ahmadzada S, Ferrari AJ, Erskine H, Leung J, Santamauro D, Lund C, Aminde LN, et al. Burden of non-communicable diseases in sub-Saharan Africa, 1990–2017: results from the Global Burden of Disease Study 2017. Lancet Glob Health. 2019;7(10):e1375–87.
Acknowledgements
Thanks to the IHME and the Global Burden of Disease study collaborations.
Funding
Not applicable.
Author information
Authors and Affiliations
Contributions
ZJO: Project administration and drafting. DFY, YHL, YZL: Data analysis and validation. WQH, YHG: Data analysis and visualization. HH, MYZ, FW: Data collection and collation. QC: supervision and drafting and editing. The author(s) read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1:
Figure S1. The distribution of number and ASR of incidence and death of neonatal preterm birth in SDI areas, and geographic regions from1990 to 2019. Figure S2. The distribution of number and ASR of incidence and death of neonatal encephalopathy due to birth asphyxia and trauma in SDI areas, and geographic regions from1990 to 2019. Figure S3. The distribution of number and ASR of incidence and death of neonatal sepsis and other neonatal infections in SDI areas, and geographic regions from1990 to 2019. Figure S4. The distribution of number and ASR of incidence and death of hemolytic disease and other neonatal jaundice in SDI areas, and geographic regions from1990 to 2019. Figure S5. The distribution of percentage changes in number of neonatal disorders incidence in specific causes at the national level. Figure S6. The distribution of EAPCs of neonatal disorders incidence in specific causes at the national level. Figure S7. The distribution of percentage changes in number of death caused by neonatal disorders in specific causes at the national level. Figure S8. The distribution of percentage changes in number of death caused by neonatal disorders in specific causes at the national level. Table S1. the age-standardized rate of incidence and death of neonatal disorders at national level in 2019, and percentage changes in number and the EAPCs from 1990 to 2019. Table S2. The percentage changes in number and the EAPCs of neonatal disorders incidence due to specific causes in global, SDI areas and geographic regions from 1990 to 2019. Table S3. the percentage changes in number and the EAPCs of incidence of neonatal disorders due to etiologies at national level from 1990 to 2019. Table S4. The percentage changes in number and the EAPCs of death caused by neonatal disorders in etiologies in global, SDI areas and geographic regions from 1990 to 2019. Table S5. the percentage changes in number and the EAPCs of death caused by neonatal disorders in etiologies at national level from 1990 to 2019.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Ou, Z., Yu, D., Liang, Y. et al. Global trends in incidence and death of neonatal disorders and its specific causes in 204 countries/territories during 1990–2019. BMC Public Health 22, 360 (2022). https://doi.org/10.1186/s12889-022-12765-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12889-022-12765-1