
Abstract
Background
Viral hepatitis is highly prevalent among people with HIV (PWH) and can lead to chronic liver complications. Thailand started universal hepatitis B vaccination at birth in 1992 and achieved over 95% coverage in 1999. We explored the prevalence of hepatitis B and C viral infections and the associated factors among PWH from same-day antiretroviral therapy (SDART) service at the Thai Red Cross Anonymous Clinic, Bangkok, Thailand.
Methods
We collected baseline characteristics from PWH enrolled in the SDART service between July 2017 and November 2019. Multivariable logistic regression was performed to determine factors associated with positive hepatitis B surface antigen (HBsAg) and hepatitis C antibody (anti-HCV).
Results
A total of 4011 newly diagnosed PWH who had HBsAg or anti-HCV results at baseline: 2941 men who have sex with men (MSM; 73.3%), 851 heterosexuals (21.2%), 215 transgender women (TGW; 5.4%), and 4 transgender men (0.1%). Median age was 27 years. Overall seroprevalence of HBsAg and anti-HCV were 6.0 and 4.1%, respectively. Subgroup prevalence were 6.2 and 4.7% among MSM, 4.6 and 2.4% among heterosexuals, and 9.3 and 3.7% among TGW, respectively. Factors associated with HBsAg positivity were being MSM, TGW, born before 1992, CD4 count < 200 cells/mm3, and alanine aminotransferase ≥ 62.5 U/L. Factors associated with anti-HCV positivity were being MSM, age > 30 years, alanine aminotransferase ≥ 62.5 U/L, creatinine clearance < 60 ml/min, and syphilis infection.
Conclusions
Around 5–10% of newly diagnosed PWH in Bangkok had hepatitis B viral infection after 25 years of universal vaccination. Anti-HCV positivity was found in 4–5% of PWH who were MSM and TGW. As World Health Organization and Thailand national guidelines already support routine screening of hepatitis B and C viral infections in PWH and populations at increased risk of HIV including MSM and TGW, healthcare providers should reinforce this strategy and provide linkage to appropriate prevention and treatment interventions. Catch-up hepatitis B vaccination should be made available under national health coverage.
Similar content being viewed by others


Background
Hepatitis B virus (HBV) and hepatitis C virus (HCV) infections are prevalent globally. In 2015, chronic HBV infection was estimated to be in 3.5% of the world population [1]. People with HIV (PWH) had a higher estimated prevalence rate of 7.4% [1]. In Thailand, a study estimated that 5.1% of the general population was infected with HBV in 2015 [2]. The proportion of infection was higher at 8.1% among men who have sex with men (MSM) and 8.1% among PWH [2]. A study conducted from 2006 to 2008 reported that 13.8% among MSM living with HIV were coinfected with HBV in Bangkok, Thailand [3]. Similarly, the global hepatitis C prevalence in 2015 was 1.0%, while 6.2% was the reported HCV prevalence among PWH. However, there is a heterogeneity of risk HCV infection among PWH populations: 82.4% in PWH who inject drugs, 6.4% in MSM living with HIV, and only 2.4% in PWH from the general population [1]. A national survey of the Thai general population in 2014 showed that hepatitis C antibody (anti-HCV) seroprevalence was 0.9% [4]. In contrast, a study focused on PWH found that anti-HCV seroprevalence was 7.7% [5], demonstrating that PWH shoulders a disproportionate burden of HCV infection when compared to the general population.
Furthermore, more than 70% of people infected with HCV and less than 6% of people who acquired HBV as an adult could turn into chronic carriers [1, 6]. Twenty per cent of chronic carriers could develop cirrhosis and hepatocellular carcinoma which are life threatening [1]. Having cofactors such as HIV infection and alcohol consumption can also accelerate the development of end-stage liver diseases [1, 6]. HBV and HCV are not only transmitted from mother to child but also sexually transmitted and share routes of transmission, including percutaneous and mucosal exposures [6, 7]. Having unprotected sex, multiple sexual partners, injection drug use, and a history of other sexually transmitted infections are important factors associated with HBV acquisition [6]. HCV is transmitted mainly through unsafe healthcare settings and injection drug use [1]. However, sexual transmission of HCV among PWH and MSM has been observed [6, 8,9,10,11,12]. MSM and transgender women (TGW) are prone to HCV infection due to the high prevalence of needle sharing, either for illicit drugs or cosmetic injections, and mucosal trauma associated with anal intercourse [9, 13,14,15,16].
Unlike HCV infection, HBV infection is a vaccine-preventable disease. Universal hepatitis B vaccination at birth was integrated into Thailand’s Expanded Program on Immunization (EPI) in 1992 and reached over 95% coverage in 1999 [17]. In 2014, a different proportion in HBV infection was seen among persons born before 1992 (4.5%) and persons born after 1992 (0.6%) [17]. Thailand national HIV treatment guidelines recommended baseline screening of newly diagnosed PWH with hepatitis B surface antigen (HBsAg) and anti-HCV, as HBV and HCV coinfections are commonly found and play a critical role in selecting antiretroviral therapy regimens [18].
The Thai Red Cross Anonymous Clinic (TRCAC) is the largest testing center for HIV and sexually transmitted infections in Bangkok, Thailand. Eligible clients who test positive for HIV are included in the same-day antiretroviral therapy (SDART) service [19]. Because this service includes clients of varied populations, namely heterosexuals, MSM, TGW, and transgender men (TGM), this study aims to explore prevalence and the associated risk factors of HBV and HCV seropositivity among PWH in the SDART service.
Methods
This is a cross-sectional descriptive study collecting demographic and laboratory data of clients in the SDART service from 13 July 2017 to 30 November 2019. Included in this study were newly diagnosed PWH at TRCAC who tested for either HBsAg or anti-HCV at baseline. Demographic data included population category, age, birth year, educational level, residential location, and level of income. Persons born in or after 1992 were classified as “born after EPI,” and persons born before 1992 were “born before EPI.” This translates to the age of 25 years for individuals who tested in 2017, 26 in 2018, and 27 in 2019. Baseline laboratory tests included HBsAg, anti-HCV, CD4 count, alanine aminotransferase (ALT), creatinine clearance (CrCl), treponemal test, and nontreponemal test. A severe decrease in CD4 count was defined as a CD4 count of less than 200 cells/mm3 [20]. Regarding ALT, a cutoff of 62.5 U/L calculated from 1.25 times the upper normal limit of the local laboratory was used to indicate a mild increase [20]. Creatinine clearance was calculated with the Cockcroft-Gault equation and categorized as severely decreased if less than 60 ml/min [20]. Syphilis was diagnosed when the treponemal test (enzyme immunoassay, chemiluminescent microparticle immunoassay, rapid immunochromatographic assay, or treponema pallidum hemagglutination assay) and nontreponemal test (either rapid plasma reagin or venereal disease research laboratory) were both positive. Clients who did not initiate antiretroviral therapy at TRCAC might not have all baseline laboratory test results.
Data analysis
Data were analyzed using Stata Version 15.0. Continuous parameters were presented as median with interquartile range (IQR). Categorical parameters were expressed in frequency and percentages. The prevalence of positive HBsAg and anti-HCV were calculated. Univariate and multivariable analyses were performed to determine factors associated with positive HBsAg and anti-HCV. Univariate analysis comparing HBsAg-positive PWH with HBsAg-negative using simple logistic regression model was tested. Factors with p-value less than 0.2 were selected into multivariable analysis. Multivariable analysis with a stepwise multiple logistic regression model including associated factors related to positive HBsAg or anti-HCV was conducted and reported with an adjusted odds ratio (aOR) and a 95% confidence interval (CI). A p-value of less than 0.05 was considered statistically significant.
Results
The total number of PWH who had HBsAg or anti-HCV results at baseline was 4011 out of 6037: 4011 had HBsAg results available, while 3990 had anti-HCV results available. Most of them were MSM (73.3%), followed by heterosexuals (21.2%), TGW (5.4%), TGM (0.1%). Median age was 27 years (IQR 23–34). Sociodemographic and laboratory characteristics are shown in Table 1. Of the included clients, 46.0% were born after EPI, 25.9% had a CD4 count of less than 200 cells/mm3, and 19.3% had syphilis diagnosed at baseline.
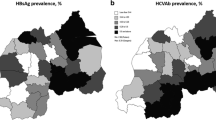
The overall prevalence of positive HBsAg was 6.0%. TGW had a prevalence of 9.3%, followed by MSM, 6.2%. People born after the EPI (1992 or later) had a prevalence of 3.6% as compared to 8.1% in people born before the EPI. Individuals born after the EPI reached more than 95% coverage (1999 or later) had a prevalence of 2.9% as compared to 6.3% in those born before 95% coverage. All nine clients who were born in 1999 or later and had a positive HBsAg were MSM.
The overall anti-HCV seroprevalence was 4.1%. MSM had the highest prevalence among all study population (4.7%). PWH aged over 30 years had a prevalence of 5.2%, while it was 3.5% among those younger than 30 years. Of 3990 who tested for both HBsAg and anti-HCV, 12 (0.3%) were positive for both. Overall and age-stratified prevalence of HBsAg and anti-HCV are shown in Table 2.
Factors found significant at the 95% confidence level from the univariate analysis were carried over to the multivariable analysis as presented in Tables 3 and 4. Factors associated with positive HBsAg were being MSM (adjusted odds ratio [aOR] 1.64, 95% CI 1.13 to 2.40, p = 0.010), being TGW (aOR 2.87, 95% CI 1.60 to 5.17, p < 0.001), being born before 1992 (aOR 2.32, 95% CI 1.69 to 3.16, p < 0.001), CD4 count < 200 cells/mm3 (aOR 1.38, 95% CI 1.03 to 1.86, p = 0.031), and ALT ≥ 62.5 U/L (aOR 2.39, 95% CI 1.66 to 3.43, p < 0.001). Factors associated with positive anti-HCV were being MSM (aOR 2.11, 95% CI 1.26 to 3.55, p = 0.005), age > 30 years (aOR 1.54, 95% CI 1.10 to 2.17, p = 0.012), ALT ≥ 62.5 U/L (aOR 7.74, 95% CI 5.48 to 10.9, p < 0.001), CrCl < 60 ml/min (aOR 5.58, 95% CI 1.95 to 16.0, p = 0.001), and syphilis positive (aOR 1.95, 95% CI 1.36 to 2.78, p < 0.001).
Discussion
Among PWH who were newly diagnosed at the Thai Red Cross Anonymous Clinic, we found 6% prevalence of HBV and 4% prevalence of anti-HCV positivity. Being MSM, TGW, and born before the inclusion of universal hepatitis B vaccination in Thailand’s EPI were statistically associated with HBV infection. Moreover, being MSM and having syphilis increased the chance of being anti-HCV positive.
More than 70% of our clients were MSM, and 5% were TGW. These findings are consistent with the proportions of new HIV infections in Thailand as projected by the AIDS Epidemic Model [21]. We found the HBV prevalence to be highest among TGW (9%), followed by MSM (6%). The anti-HCV seroprevalence was highest among MSM (5%), followed by TGW (4%). These data support the findings from previous studies which demonstrated higher prevalence rates of HBV and HCV among PWH who were MSM and TGW than those who were of heterosexual populations [1, 3, 15, 22,23,24]. The HBV prevalence shown in our clients is quite concerning, as 27% of HBV-infected individuals were born after EPI, indicating that the HBV epidemic is still ongoing. However, among clients infected with HBV, only 4% were born in 1999 or later, which was the year that EPI reached more than 95% coverage. Lower prevalence of HBV in younger generations could be due to both the success of EPI and shorter duration at risk. The overall prevalence of HBV and HCV found in our study were slightly lower than that of the global and Thai reports among PWH [1, 2, 5], possibly because our clients were relatively young with over 60% aged 30 years or less . Apart from viral hepatitis, almost 20% of our clients had syphilis at baseline, illustrating higher burden than what was previously reported in general MSM population by World Health Organization (WHO; 6%) in 2018 [25].
MSM and TGW had 1.6 and 2.9 times the odds of HBV infection compared with heterosexual populations, respectively, which could be explained by sexual practices and routes which are more vulnerable to mechanical trauma [26]. Consistent with the national survey [17], we saw a contrast of HBV prevalence between people who were born before and after EPI (8% vs. 4%). PWH who were born before EPI had 2.3 times higher odds of having HBV infection. Another possible explanation of the association to birth year could be that younger people had less time for exposure to the infection than older people. Nonetheless, the findings from this study shows that HBV infection was not completely eliminated by the EPI. Some newborns might be born to an HBV-infected mother, not complete the full course of the immunization, not respond to HBV vaccination, or be unvaccinated. Regarding PWH who do not have immunity to HBV, it is advised to immunize all PWH regardless of CD4 level [18], even though lower CD4 count is one of the factors affecting the effectiveness of the HBV immunization [27,28,29].
There are many reports of the HCV epidemic among MSM living with HIV in major cities of the world in Europe, Asia-Pacific, and Thailand [8,9,10, 30,31,32,33,34,35,36], and many findings demonstrated an upward trend of HCV infection [9, 30,31,32,33,34,35,36]. For example, a study in Thailand found that HCV incidence increased from 0.7–1.1 per 100 person-years in 2014–2016 to 4.5 per 100 person-years in 2018 [30]. Our findings also indicated similar discovery, as we found that being MSM and having syphilis doubled the risk of having positive anti-HCV in our study. HCV infection is widely known to be associated with recreational drug use [9, 10, 30, 31, 35, 37,38,39,40], as some MSM utilize recreational drugs to enhance their sexual pleasure, the phenomenon known as chemsex [41, 42]. Studies on people who did not use injection drugs found that HCV infection was still associated with recreational drug use and syphilis [33, 35, 43], suggesting that transmission of HCV is associated with sexual intercourse. It has been estimated that the prevalence of drug injection among newly diagnosed Thai PWH in 2020 is 12% [44]. Unfortunately, we did not collect data on substance use and chemsex in our study and could not assess these potential associations. However, as MSM and syphilis were key factors associated with HCV infection among our clients, we hypothesized that HCV acquisition in our HIV-positive MSM clients was likely linked to sexual transmission and possibly in the chemsex context.
There were a few limitations in our study. This study was conducted at one site and two-thirds of our PWH clients lived in Bangkok, suggesting that they may be more educated and had higher income when compared to PWH from other regions in Thailand. Thus, our study sample might not represent the overall population of PWH in Thailand. Additionally, we could not retrieve hepatitis B vaccination history from original medical records, and therefore needed to use PWH clients’ birth year as a surrogate. As previously mentioned, we did not record substance use and chemsex data and thus could not explore their possible associations with HBV and HCV infections in our study. Lastly, we did not perform HCV RNA in anti-HCV-positive clients; therefore, the observed anti-HCV seroprevalence may be higher than the actual infection rate.
WHO aimed to eliminate hepatitis B and C infections by 2030 [45]. To achieve this, a country must target the areas determined to have beneficial impacts as described in Table 5 [45, 46]. In Thailand, HBV vaccination has reached 95% coverage since 1999 [17]. However, Thailand’s diagnosis and treatment coverage of HBV and HCV are far from the target [46]. WHO and Thailand already recommend HBV and HCV infection screening in PWH and those who are at risk of HIV including MSM and transgender people [18, 47, 48]. From the results of this study, continuation of HBV and HCV screening for everyone living with HIV regardless of age would uncover a high proportion of undiagnosed infections and be a chance to bring them to treatment. Providing HIV preexposure prophylaxis to HIV-negative persons at risk of HIV acquisition and following the current WHO and Thailand guidance to test for HIV, HBV, and HCV infections at commencement of the services can be an opportunity to screen, vaccinate (HBV), and if needed, treat these infections to prevent further transmission [49, 50]. In spite of that, catch-up hepatitis B immunization needs to be paid out of pocket for in Thailand. Regarding HCV, some global HCV elimination efforts have now included pangenotypic direct-acting antiretroviral (DAA) therapy for most HCV-infected individuals [51, 52]. In Thailand, costs of HCV genotyping and treatment have been high, but the voluntary licensing of DAA medications is becoming implemented in Thailand [53]. However, the current restriction to only start DAA in individuals with fibrosis METAVIR Stage F2 means that individuals with HCV can continue to transmit the virus to others. Future studies will need to explore strategies to timely and efficiently test and treat HCV, especially among PWH, to contribute to the elimination of HCV.
Conclusions
Thailand’s EPI has successfully reduced HBV infection. However, the infection rate among newly diagnosed PWH remained at around 5–10%. Hepatitis C infection was found in 4–5% of PWH who were MSM and TGW. Healthcare providers should reinforce HBV and HCV screening in PWH, MSM, and TGW and provide linkage to appropriate prevention and treatment interventions. Catch-up hepatitis B vaccination should be made available under national health coverage.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- aOR:
-
Adjusted odds ratio
- CI:
-
Confidence interval
- CrCl:
-
Creatinine clearance
- ALT:
-
Alanine aminotransferase
- Anti-HCV:
-
Hepatitis C antibody
- DAA:
-
Direct-acting antiretroviral
- EPI:
-
Expanded Program on Immunization
- HBsAg:
-
Hepatitis B antigen
- HBV:
-
Hepatitis B virus
- HCV:
-
Hepatitis C virus
- IQR:
-
Interquartile range
- MSM:
-
Men who have sex with men
- PWID:
-
Person who injects drug
- PWH:
-
People with HIV
- SDART:
-
Same-day antiretroviral therapy
- TGW:
-
Transgender women
- TRCAC:
-
Thai Red Cross Anonymous Clinic
- WHO:
-
World Health Organization
References
World Health Organization. Global hepatitis report 2017. Geneva: World Health Organization; 2017. [cited 2021 Mar 09]. Available from: https://apps.who.int/iris/bitstream/handle/10665/255016/9789241565455-eng.pdf
Leroi C, Adam P, Khamduang W, Kawilapat S, Ngo-Giang-Huong N, Ongwandee S, et al. Prevalence of chronic hepatitis B virus infection in Thailand: a systematic review and meta-analysis. Int J Infect Dis. 2016;51:36–43. https://doi.org/10.1016/j.ijid.2016.08.017.
Linkins RW, Chonwattana W, Holtz TH, Wasinrapee P, Chaikummao S, Varangrat A, et al. Hepatitis a and hepatitis B infection prevalence and associated risk factors in men who have sex with men, Bangkok, 2006-2008. J Med Virol. 2013;85(9):1499–505. https://doi.org/10.1002/jmv.23637.
Wasitthankasem R, Posuwan N, Vichaiwattana P, Theamboonlers A, Klinfueng S, Vuthitanachot V, et al. Decreasing hepatitis C virus infection in Thailand in the past decade: evidence from the 2014 National Survey. PLoS One. 2016;11(2):e0149362. https://doi.org/10.1371/journal.pone.0149362 Erratum in: PLoS One 2016 May 18;11(5):e0152451. doi: 10.1371/journal.pone.0152451.
Phuangchoei P, Chotiyaputta W, Chayakulkeeree M. Clinical characteristics of hepatitis B and C virus infections in HIV-infected patients. J Med Assoc Thail. 2015;98(3):226–31.
Workowski KA, Bolan GA. Centers for Disease Control and Prevention (US). Sexually transmitted diseases treatment guidelines, 2015. MMWR Recomm Rep. 2015;64(RR-03):1–137 PubMed PMID: 26042815; PubMed Central PMCID: PMC5885289.
Schillie S, Vellozzi C, Reingold A, Harris A, Haber P, Ward JW, et al. Prevention of hepatitis B virus infection in the United States: recommendations of the advisory committee on immunization practices. MMWR Recomm Rep. 2018;67(1):1–31. https://doi.org/10.15585/mmwr.rr6701a1.
van de Laar T, Pybus O, Bruisten S, Brown D, Nelson M, Bhagani S, et al. Evidence of a large, international network of HCV transmission in HIV-positive men who have sex with men. Gastroenterology. 2009;136(5):1609–17. https://doi.org/10.1053/j.gastro.2009.02.006.
Urbanus AT, van de Laar TJ, Stolte IG, Schinkel J, Heijman T, Coutinho RA, et al. Hepatitis C virus infections among HIV-infected men who have sex with men: an expanding epidemic. AIDS. 2009;23(12):F1–7. https://doi.org/10.1097/QAD.0b013e32832e5631.
Rauch A, Rickenbach M, Weber R, Hirschel B, Tarr PE, Bucher HC, et al. Unsafe sex and increased incidence of hepatitis C virus infection among HIV-infected men who have sex with men: the Swiss HIV cohort study. Clin Infect Dis. 2005;41(3):395–402. https://doi.org/10.1086/431486.
Danta M, Brown D, Bhagani S, Pybus OG, Sabin CA, Nelson M, et al. Recent epidemic of acute hepatitis C virus in HIV-positive men who have sex with men linked to high-risk sexual behaviours. AIDS. 2007;21(8):983–91. https://doi.org/10.1097/QAD.0b013e3281053a0c.
Li H, Marks KM, Talal AH, van Seggelen WO, Akil B, Radix A, et al. Assessing routes of hepatitis C transmission in HIV-infected men who have sex with men using single genome sequencing. PLoS One. 2020;15(7):e0235237. https://doi.org/10.1371/journal.pone.0235237.
Dionne-Odom J, Osborn MK, Radziewicz H, Grakoui A, Workowski K. Acute hepatitis C and HIV coinfection. Lancet Infect Dis. 2009;9(12):775–83. https://doi.org/10.1016/S1473-3099(09)70264-6.
Reback CJ, Fletcher JB. HIV prevalence, substance use, and sexual risk behaviors among transgender women recruited through outreach. AIDS Behav. 2014;18(7):1359–67. https://doi.org/10.1007/s10461-013-0657-z.
Luzzati R, Zatta M, Pavan N, Serafin M, Maurel C, Trombetta C, et al. Prevalence of human immunodeficiency virus, hepatitis B virus, and hepatitis C virus infections among transgender persons referred to an Italian center for total sex reassignment surgery. Sex Transm Dis. 2016;43(7):407–11. https://doi.org/10.1097/OLQ.0000000000000452.
Bastos FI, Bastos LS, Coutinho C, Toledo L, Mota JC, Velasco-de-Castro CA, et al. HIV, HCV, HBV, and syphilis among transgender women from Brazil. Medicine (Baltimore). 2018;97(1 Suppl):S16–24. https://doi.org/10.1097/MD.0000000000009447.
Posuwan N, Wanlapakorn N, Sa-Nguanmoo P, Wasitthankasem R, Vichaiwattana P, Klinfueng S, et al. The success of a universal hepatitis B immunization program as part of Thailand's EPI after 22 years' implementation. PLoS One. 2016;11(3):e0150499. https://doi.org/10.1371/journal.pone.0150499.
Thailand national guidelines on HIV/AIDS treatment and prevention 2017. Nonthaburi: Bureau of AIDS, TB and STIs, Department of Disease Control, Ministry of Public Health (TH); 2017. [cited 2021 Mar 1]. Available from: http://www.thaiaidssociety.org/images/PDF/hiv_thai_guideline_2560.pdf.Thai.
Seekaew P, Teeratakulpisarn N, Surapuchong P, Teeratakulpisarn S, Amatavete S, Jomja P, et al. Same-day ART initiation in HIV/STI testing center in Bangkok, Thailand: initial results from an implementation research [abstract]: Proceedings of the AIDS 2018: 22nd international AIDS conference; 2018. p. 23–7.
U.S. Department of Health and Human Services, National Institutes of Health, National Institute of Allergy and Infectious Diseases, Division of AIDS. Division of AIDS (DAIDS) Table for Grading the Severity of Adult and Pediatric Adverse Events, Corrected Version 2.1. Bethesda (MD): National Institutes of Health (US); 2017. [cited 2021 Mar 1]. Available from: https://rsc.niaid.nih.gov/sites/default/files/daidsgradingcorrectedv21.pdf
Thailand working group on HIV/AIDS projection. AIDS epidemic model projection for HIV/AIDS in Thailand 2021-2030 summary report: AIDS Data Hub; 2015. [cited 2021 Mar 1]. Available from: https://www.aidsdatahub.org/sites/default/files/resource/projection-hiv-aids-thailand-2010-2030.pdf
Cardona-Arias JA, Correa JCC, Higuita-Gutiérrez LF. Prevalence of hepatitis B/C viruses and associated factors in key groups attending a health services institution in Colombia, 2019. PLoS One. 2020;15(9):e0238655. https://doi.org/10.1371/journal.pone.0238655.
Hadikusumo AA, Utsumi T, Amin M, Khairunisa SQ, Istimagfirah A, Wahyuni RM, et al. High rates of hepatitis B virus (HBV), hepatitis C virus (HCV), and human immunodeficiency virus infections and uncommon HBV genotype/subtype and HCV subtype distributions among transgender individuals in Surabaya, Indonesia. Jpn J Infect Dis. 2016;69(6):493–9. https://doi.org/10.7883/yoken.JJID.2015.384.
Grov C, Westmoreland DA, Carrico AW, Nash D. Are we on the precipice of a new epidemic? Risk for hepatitis C among HIV-negative men-, trans women-, and trans men- who have sex with men in the United States. AIDS Care. 2020;32(sup2):74–82. https://doi.org/10.1080/09540121.2020.1739204.
World Health Organization. Men who have sex with men (MSM) with active syphilis (%). Geneva: World Health Organization; 2020. [cited 2021 Mar 7]. Available from: https://www.who.int/data/gho/data/indicators/indicator-details/GHO/men-who-have-sex-with-men-(msm)-with-active-syphilis-(−)
Schreeder MT, Thompson SE, Hadler SC, Berquist KR, Zaidi A, Maynard JE, et al. Hepatitis B in homosexual men: prevalence of infection and factors related to transmission. J Infect Dis. 1982;146(1):7–15. https://doi.org/10.1093/infdis/146.1.7.
Kim HN, Harrington RD, Van Rompaey SE, Kitahata MM. Independent clinical predictors of impaired response to hepatitis B vaccination in HIV-infected persons. Int J STD AIDS. 2008;19(9):600–4. https://doi.org/10.1258/ijsa.2007.007197.
Pasricha N, Datta U, Chawla Y, Singh S, Arora SK, Sud A, et al. Immune responses in patients with HIV infection after vaccination with recombinant hepatitis B virus vaccine. BMC Infect Dis. 2006;6:65. https://doi.org/10.1186/1471-2334-6-65.
Cornejo-Juárez P, Volkow-Fernández P, Escobedo-López K, Vilar-Compte D, Ruiz-Palacios G, Soto-Ramírez LE. Randomized controlled trial of hepatitis B virus vaccine in HIV-1-infected patients comparing two different doses. AIDS Res Ther. 2006;3:9. https://doi.org/10.1186/1742-6405-3-9.
Wansom T, Pinyakorn S, Kolsteeg CJ, Kroon E, Sacdalan CP, Chomchey N, et al. Brief report: group sex and methamphetamine use fuel an explosive epidemic of hepatitis C among HIV-infected men who have sex with men in Bangkok, Thailand. J Acquir Immune Defic Syndr. 2020;84(4):331–5. https://doi.org/10.1097/QAI.0000000000002356.
Ramière C, Charre C, Miailhes P, Bailly F, Radenne S, Uhres AC, et al. Lyon acute hepatitis study group. Patterns of hepatitis C virus transmission in human immunodeficiency virus (HIV)-infected and HIV-negative men who have sex with men. Clin Infect Dis. 2019;69(12):2127–35. https://doi.org/10.1093/cid/ciz160.
Lin AWC, Wong KH, Chan K. More safer sex intervention needed for HIV-positive MSM with higher education level for prevention of sexually transmitted hepatitis C. J Int AIDS Soc. 2014;17(4Suppl 3):19663. https://doi.org/10.7448/IAS.17.4.19663.
Sun HY, Chang SY, Yang ZY, Lu CL, Wu H, Yeh CC, et al. Recent hepatitis C virus infections in HIV-infected patients in Taiwan: incidence and risk factors. J Clin Microbiol. 2012;50(3):781–7. https://doi.org/10.1128/JCM.06014-11.
Sun HY, Uemura H, Wong NS, Chan DP, Wong BC, Lin PH, et al. Molecular epidemiology of acute HCV infection in HIV-positive patients from Hong Kong, Taipei, Tokyo. Liver Int. 2019;39(6):1044–51. https://doi.org/10.1111/liv.14073.
Nishijima T, Shimbo T, Komatsu H, Hamada Y, Gatanaga H, Oka S. Incidence and risk factors for incident hepatitis C infection among men who have sex with men with HIV-1 infection in a large urban HIV clinic in Tokyo. J Acquir Immune Defic Syndr. 2014;65(2):213–7. https://doi.org/10.1097/QAI.0000000000000044.
van der Helm JJ, Prins M, del Amo J, Bucher HC, Chêne G, Dorrucci M, et al. CASCADE collaboration. The hepatitis C epidemic among HIV-positive MSM: incidence estimates from 1990 to 2007. AIDS. 2011;25(8):1083–91. https://doi.org/10.1097/QAD.0b013e3283471cce.
Han WM, Colby DJ, Khlaiphuengsin A, Apornpong T, Kerr SJ, Ubolyam S, et al. Large transmission cluster of acute hepatitis C identified among HIV-positive men who have sex with men in Bangkok, Thailand. Liver Int. 2020;40(9):2104–9. https://doi.org/10.1111/liv.14578.
Centers for Disease Control and Prevention (US). Sexual transmission of hepatitis C virus among HIV-infected men who have sex with men--New York City, 2005–2010. MMWR Morb Mortal Wkly Rep. 2011;60(28):945–50 PMID: 21775948.
Schmidt AJ, Rockstroh JK, Vogel M, An der Heiden M, Baillot A, Krznaric I, et al. Trouble with bleeding: risk factors for acute hepatitis C among HIV-positive gay men from Germany--a case-control study. PLoS One. 2011;6(3):e17781. https://doi.org/10.1371/journal.pone.0017781.
Vanhommerig JW, Lambers FA, Schinkel J, Geskus RB, Arends JE, van de Laar TJ, et al. Risk factors for sexual transmission of hepatitis C virus among human immunodeficiency virus-infected men who have sex with men: a case-control study. Open Forum Infect Dis. 2015;2(3):ofv115. https://doi.org/10.1093/ofid/ofv115.
Piyaraj P, van Griensven F, Holtz TH, Mock PA, Varangrat A, Wimonsate W, et al. The finding of casual sex partners on the internet, methamphetamine use for sexual pleasure, and incidence of HIV infection among men who have sex with men in Bangkok, Thailand: an observational cohort study. Lancet HIV. 2018;5(7):e379–89. https://doi.org/10.1016/S2352-3018(18)30065-1 Erratum in: Lancet HIV 2018 Jul;5(7):e340.
Guadamuz TE, Boonmongkon P. Ice parties among young men who have sex with men in Thailand: pleasures, secrecy and risks. Int J Drug Policy. 2018;55:249–55. https://doi.org/10.1016/j.drugpo.2018.04.005.
Breskin A, Drobnik A, Pathela P, Chan C, Braunstein S, Bornschlegel K, et al. Factors associated with hepatitis C infection among HIV-infected men who have sex with men with no reported injection drug use in new York City, 2000-2010. Sex Transm Dis. 2015;42(7):382–6. https://doi.org/10.1097/OLQ.0000000000000293.
Family Health International; Bureau of AIDS, TB and STIs, Department of Disease Control, Ministry of Public Health (TH). The Asian Epidemic Model (AEM) projections for HIV/AIDS in Thailand: 2005–2025. Nonthaburi: Bureau of AIDS, TB and STIs, Department of Disease Control, Ministry of Public Health (TH); 2008.
World Health Organization. Global health sector strategy on viral hepatitis 2016-2021 towards ending viral hepatitis. Geneva: World health Organization; 2016. [cited 2021 Mar 6]. Available from: https://apps.who.int/iris/bitstream/handle/10665/246177/WHO-HIV-2016.06-eng.pdf
CDA Foundation. Polaris observatory [internet]. Lafayette: CDA Foundation; 2020. [updated 2020 Apr 17; cited 2021 Mar 7]. Available from: https://cdafound.org/polaris/
Thailand practice guideline for management of chronic hepatitis C 2018. Bangkok: Thailand Association for the Study of the Liver; 2018. [cited 2021 Mar 7]. Available from: https://www.thasl.org/files/33.THASL%20Chronic%20hepatitis%20C%20guideline%202018_26-04-2018_r1.pdf.
WHO guidelines on hepatitis B and C testing. Geneva: World Health Organization; 2017. [cited 2021 Mat 7]. Available from: https://www.who.int/hepatitis/publications/HEP17001_WEB11.pdf.
Thailand national guidelines on pre-exposure prophylaxis: HIV-PrEP 2018. Nonthaburi: bureau of AIDS, TB and STIs, Department of Disease Control, Ministry of Public Health (TH); 2018. Thai.
WHO implementation tool for pre-exposure prophylaxis (PrEP) of HIV infection. Module 1: clinical. Geneva: World health Organization; 2017.
Strategic plan for the elimination of hepatitis C virus in Georgia, 2016–2020. Tbilisi: Ministry of Labour, Health and Social Affairs (GE); 2017. [cited 2021 Mar 7]. Available from: https://www.moh.gov.ge/uploads/files/2017/akordeoni/failebi/Georgia_HCV_Elimination_Strategy_2016-2020.pdf.
Viral hepatitis national strategic plan for the United States: a roadmap to elimination (2021–2025). Washington, DC: U.S. Department of Health and Human Services; 2020. [cited 2021 Mar 7]. Available from: https://www.hhs.gov/sites/default/files/Viral-Hepatitis-National-Strategic-Plan-2021-2025.pdf.
Posuwan N, Wanlapakorn N, Sintusek P, Wasitthankasem R, Poovorawan K, Vongpunsawad S, et al. Towards the elimination of viral hepatitis in Thailand by the year 2030. J Virus Erad. 2020;6(3):100003. https://doi.org/10.1016/j.jve.2020.100003.
Acknowledgements
This work was made possible by the generous support of the American people through USAID and PEPFAR. The contents are the responsibility of the LINKAGES project and do not necessarily reflect the views of USAID, PEPFAR, or the United States Government. LINKAGES, a five-year cooperative agreement (AID-OAA-A-14-00045), is led by FHI 360. Additional acknowledgements to the Thai Red Cross Anonymous Clinic and its staff for providing facility and data collection, Oranuch Nampaisan for the precious advice on statistics, and Dr. Nipat Teeratakulpisarn for the contribution to the conceptualization.
Funding
The SDART program and this study was funded by the United States Agency for International Development (USAID) and the U.S. President’s Emergency Plan for AIDS Relief (PEPFAR).
Author information
Authors and Affiliations
Contributions
ST, TC, SA, TP, AA, PP, RR, and NP contributed to the design and concept of the study. ST, TC, SA, and MS contributed the data. JP and SA extracted and prepared the data. ST and JP analyzed the data. ST wrote the manuscript. TC, PS, AA, MA, and NP assisted in interpretation of the data, provided intellectual input, and provided edits. All authors have reviewed and approved the final version.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The Same-Day Antiretroviral Therapy Initiation protocol (NCT04032028) was approved by the Institutional Review Board of the Faculty of Medicine, Chulalongkorn University with Approval Number 158/56. Institutional Review Board of the Faculty of Medicine, Chulalongkorn University has waived the informed consent for the study. All methods were carried out in accordance with relevant guidelines and regulations.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Thitipatarakorn, S., Chinbunchorn, T., Peelay, J. et al. Prevalence and the associated factors of hepatitis B and hepatitis C viral infections among HIV-positive individuals in same-day antiretroviral therapy initiation program in Bangkok, Thailand. BMC Public Health 22, 144 (2022). https://doi.org/10.1186/s12889-021-12429-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12889-021-12429-6