
Abstract
Background
Web-based stress management interventions (SMI) fit increasingly digital lifestyles, reduce barriers of uptake and are easily scalable. SMIs might lower levels of stress in employees and thereby contribute to the prevention of depressive symptomatology. Different guidance formats can impact the efficacy of SMIs, with higher intensity assumed to result in larger effects. However, head-to-head comparisons of guidance formats are rare. This is the first trial to examine the impact of adherence-focused guidance compared to self-help on the efficacy of an occupational SMI compared to a wait list control condition. Additionally, it will be investigated if the SMI enfolds its impact on preventing depressive symptomatology by different pathways through reducing health impairing and increasing promoting factors.
Methods
A three-armed randomised controlled trial (RCT) on an occupational SMI was conducted. 404 employees with elevated levels of perceived stress (PSS-10 ≥ 22) were randomly assigned to: adherence-focused guidance (AFG), self-help (SH) or a wait list control group (WLC). The primary outcome was perceived stress (PSS-10). Secondary outcomes included health- and work-related measures. A parallel mediation analysis with stress and resilience as mediators for the effect on depression (CES-D) was carried out. Data collection took place at baseline (T1), after 7 weeks (T2) and 6 months (T3).
Results
The SMI was effective for all groups on the primary and secondary outcomes. For stress, analyses of covariance (ANCOVA) revealed significant group effects at T2 (F2,400 = 36.08, P < .001) and T3 (F2,400 = 37.04, P < .001) with large effect sizes for AFG (T2: d = 0.83; T3: d = 0.85) and SH (T2: d = 0.88; T3: d = 0.91) compared to WLC. No significant group differences were found for the efficacy between AFG and SH on the outcomes. Adherence in terms of completed modules was significantly higher for AFG compared to SH. The SMI’s impact on depression was mediated by perceived stress: a1b1 = − 0.77, 95% CI [− 1.26, − 0.34] and resilience: a2b2 = − 0.62, 95% CI [− 1.05, − 0.26].
Conclusions
The SMI was effective for reducing stress and improving other health- and work-related outcomes, irrespective of the guidance format. Results did not demonstrate superiority of adherence-focused guidance for the efficacy but for adherence in terms of completed modules. Among other reasons, better communication strategies about offered guidance and awareness-raising measures are discussed. Results from mediation analysis suggest that preventive SMIs should be designed to reach two goals: reducing the risk factor of stress and simultaneously increasing health promoting factors such as resilience.
Trial registration
German Clinical Trial Registration (DRKS) DRKS00005687, 6/6/2014.
Similar content being viewed by others

Background
Work-related stress is associated with increased risk for development and maintenance of adverse physical [1,2,3] and mental health consequences [4]. Experiencing stressors at work is associated with an elevated risk of sickness absence due to a diagnosed mental disorder [5] and can precede depressive symptoms over time, thereby increasing the risk for subsequent depression [6, 7]. As one of the three leading causes, unipolar depression largely contributes to the burden of disease and is predicted to be number one by 2030 [8]. The World Health Organization (WHO) therefore calls for prevention to effectively reduce this tremendous burden [9].
This in turn leads to substantial socio-economic harms. These can be divided into direct costs due to growing use of health care services and indirect costs resulting from productivity loss caused by work loss days, presenteeism, employee turnover and work impairment [10, 11]. Notably, indirect costs account for most of the total stress-related cost with 70–90% [10]. As a national example, work stress, depression and anxiety predominantly caused for 44% of ill health cases and 57% of lost working days in Great Britain in 2017/2018 [12].
Ongoing digitisation and rapidly developing technology altered the labour market profoundly with a transformation towards the Fourth Industrial Revolution. As a result, employees can experience severe stress due to unfavourable changes of workplace cultures, employee turnover or job insecurity [3, 13, 14]. The other side of the coin is the potential of using digital facilities to deliver web-based interventions which have been shown to be effective in reducing stress [15] and improving mental health in those affected by serious disorders such as depression [16, 17]. Not least, the COVID-19 pandemic has highlighted the need for the implementation of e-health interventions into routine health care and overcoming barriers to effectively do so [18].
From a public health point of view, Internet Interventions generally may offer many advantages compared to face-to-face approaches. They fit increasingly digital lifestyles, are easily scalable and reduce barriers of uptake [19]. Furthermore, health economic evaluations showed that a guided version of the utilised SMI from prior studies was cost-effective [20, 21].
Reaching a greater proportion of affected individuals that otherwise may remain untreated hence seems more feasible [22]. Substantial benefits of this delivery mode are the portability and time-spatial independent accessibility [23] allowing users to review contents at their own pace. The anonymity of the Internet might circumvent fears of possible stigmatisation or self-disclosure in traditional therapy settings that for such reasons may be rejected by many subjects in need [24, 25]. Supporting evidence stems from studies showing that the web-only delivery mode can be as effective as face-to-face settings [26,27,28].
Web-based occupational stress management interventions (SMI) seem to be a promising approach against this background. Studies have demonstrated treatment effects on various health outcomes within the occupational context [29] with maintaining reductions of stress for up to 6 months [15, 30]. Meta-analytic evidence showed that exposure to work-related stressors could precede the onset of depressive symptoms [31] and clinical depression [6]. There are three well investigated and prominent theories and models to explain these associations, namely the demand-control model, effort-reward imbalance model and organisational injustice framework [32]. There is evidence that each of these theoretical approaches is valid and correctly predicts that stressors at work are linked to a moderately elevated risk of the onset of depression [32]. Against this background, effects of SMI on depression were also investigated and found to be positive at post-intervention and at 6-month follow-up, although larger for the former [15, 30, 33, 34]. Notably, these studies are characterised by moderate to high heterogeneity [15, 30].
A fundamental aspect varying along these studies that seems to be crucial in affecting the efficacy of SMI, is the impact of human guidance [35]. The intensity of guidance can differ regarding the format and scope of provided human support. On the one side, intensive guidance is expert driven, requiring a high invest of resources. It can for example be content-focused with personalised written feedback on completed exercises or modules [15]. On the other side and opposed to this format, a self-help format requires only few resources and provides no professional support [36]. This format can easily be scaled to maximum, is cost-effective and needed to sufficiently treat subjects who otherwise would not receive any professional service at all [20, 37]. Adherence-focused guidance is an attempt to find a good compromise between those two intensities in guidance. This guidance format was established in earlier studies and consists of adherence monitoring and feedback on demand [35, 38]. Therefore, adherence-focused guidance is client driven, requiring an active role and initiative of a participant when in need of support. Providing guidance by human support is expected to be conducive to the efficacy of Internet Interventions [15, 39, 40]. The support provided usually is of a technical or clinical kind or focusses on the correct usage of the intervention [41]. According to the Supportive Accountability Model [42], human support enhances adherence to e-health interventions. Social presence or performance monitoring by an e-coach that is perceived as benevolent and trustworthy are for example integral factors to foster accountability. Studies demonstrated declining clinical outcomes with decreasing coaching time spent on each participant, with an increasing likelihood of study dropout at the same time [38, 43, 44]. Further findings indicate that guidance also seems to impact user satisfaction and acceptance that both in turn affect adherence [45,46,47]. Previous trials suggested the use of adherence-focused guidance [48] and showed that it was effective for Internet Interventions targeting stress management [49] or subthreshold depression [50]. Investigating different guidance formats is particularly important since little or no adherence and low uptake rates are major issues of Internet Interventions [45, 51]. Until now, there is no evidence on the comparison of adherence-focused guidance to self-administered formats for SMI unguided interventions, although empirical validations of the effects of varying guidance formats are highly necessary for large-scale dissemination into routine health care. Against this background, this study aims at comparing the effectiveness for adherence-focused guidance which combines adherence-monitoring and human support, with a self-help mode.
While guidance is crucial for an evidence-based design of SMI, the underlying mechanisms of how such interventions come into effect have not been fully captured yet. Despite an increasing number of studies, the process by which SMI result in effects on depression is unclear. A theoretical framework that can be applied to address this gap is the job-demands-resources (JD-R) model that was developed to explain the genesis of job strain [52, 53]. According to this model, any occupational characteristics can be classified into one of the two underlying clusters: job demands or job resources. These two clusters initiate two diverging processes. Job demands that no longer can be met instigate a health impairment process, whereas the availability of sufficient job resources launches a motivational process. This model can be used for this study to examine the global issue of stress in a more detailed manner. In particular, to elucidate how the SMI can affect depressive symptoms. Based on the JD-R model and earlier research on the relationships between stress and health outcomes, the SMI may work through two different paths. One of these paths can be assumed to be health impairing with work stress often being precedent to depression. Hence, positive effects on depression might be preceded by an efficacious stress reduction. Opposed to this, available resources can promote resilience that can buffer such deleterious effects and prevent pathogenesis [54, 55]. Taken together, positive effects of SMI on depression might be the result of either one of these paths acting individually or a dual pathway working simultaneously.
This is the first investigation of the comparable efficacy of different guidance formats within a single, homogenous study on SMI yet. Therefore, this three-armed randomised controlled trial has three aims. First, to assess the comparative efficacy of adherence-focused guidance, self-help and a wait list control group, assuming each of the intervention groups will be superior to the waitlist control group and adherence-focused guidance will be superior to self-help. Second, to reveal further insights into utilisation rates and acceptability of the various guidance formats. And third, to investigate mediating paths of how this SMI affects depression, considering perceived stress and resilience as potential mediators.
Methods
Study design and hypotheses
A three-armed randomised controlled trial (RCT) was conducted in compliance with the study protocol [35] and the Declaration of Helsinki and Good Clinical Practice (GCP). Subjects were randomised into three groups: (1) adherence-focused guidance (AFG), (2) self-help (SH) and (3) a wait list control condition (WLC). Accordingly, both AFG and SH received the same SMI, but guidance was different. Each group had full access to treatment as usual (TAU).
Based on data from an earlier pilot evaluation we expected a mean effect for the AFG condition compared to WLC of at least d = 0.70. Evidence available at the time of planning the study showed that meta-analytic data for cognitive-behavioural occupational SMI indicated an effect size of d = 0.68 [56] and that unguided Internet Interventions consistently seem to produce lower effect sizes compared to guided trainings [39]. Against this background, this study aimed to be able to detect a between group effect size of d = 0.30. To detect this effect with a power (1-ß) of 80% and α = .05 in multiple Bonferroni-adjusted tests (H1: AFG superior to WLC at post-intervention, H2: SH superior to WLC at post-intervention, H3: AFG superior to SH at post-intervention), a required sample size of 408 participants was calculated with PASS12 (NCSS).
After screening for eligibility (T0) and allocation, assessments were conducted at baseline (T1), 7 weeks post-intervention (T2) and at 6-month follow-up (T3) using a secured online-based self-report system (AES, 256-bit encrypted). Primary and secondary outcomes were used as dependent variables and treatment condition as the independent variable with respective baseline scores as covariates; for a description of the sample, baseline characteristics were assessed that are listed in the section Other measures. The University of Marburg ethics committee approved of this study (No. 2014-5 K). All participants gave informed consent. The trial was registered in the German Clinical Trials Register (DRKS00005687).
Inclusion and exclusion criteria
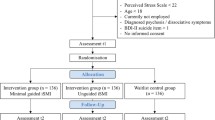
Inclusion criteria required (1) participants being adults (aged ≥18), (2) current employment, (3) Internet access, (4) sufficient German reading and writing skills, (5) willingness to give informed consent and (6) scores ≥22 on the Perceived Stress Scale (PSS-10) [57]. The PSS-10 cut-off allows for the selection of subjects with elevated stress levels, as identified by one standard deviation (SD = 6.2) above the mean (M = 15.3) in a large sample of working people [58]. Exclusion criteria were previous or current diagnosis of psychosis or dissociative symptoms, or a notable suicidal ideation indicated by a score > 1 on the ninth item (“I feel I would be better off dead”) of the Beck Depression Inventory (BDI) [59].
Recruitment and randomisation
Between January and May 2014, nationwide recruitment took place trough newsletters, press releases and the support of a large German health insurance company that advertised the study in their member journal and regional offices (n = 918). Participation was not limited to the health company’s insurants. Interested subjects signed up on the website (www.geton-training.de) by providing their e-mail address. After screening for eligibility, giving written informed consent and completing the baseline assessment, participants were randomly allocated to the three different intervention arms. A third independent party performed individual randomisation at a ratio of 1:1:1 and a block size of three using an automated computer-based random integer generator (DatInf® RandList). Thereafter, participants were not blinded to conditions and either received immediate access to the SMI or 6 months later if allocated to the WLC.
Intervention
Based on Lazarus’ transactional model of stress [60], the intervention was developed for employees and focusses on problem solving [61, 62] and emotion regulation skills [63, 64]. It comprises seven core modules for psychoeducation (module 1), problem solving (modules 2–3), emotion regulation (modules 4–6), planning future (module 7) and an optional booster session offered four weeks after training completion (module 8). Table 1 supplies a more detailed description of the contents. Within modules 2–6, participants could autonomously choose to adapt their intervention for additional modules covering time management, rumination and worrying, psychological detachment from work, sleep hygiene, rhythm and regularity of sleeping habits, nutrition and exercise, organising work breaks, and social support. In that way, the intervention was tailored to the subjects’ individual needs depending on responses that they opted for. Subjects were advised to complete at least one and at maximum two modules per week. It took 45 to 60 min to complete a module, resulting in a total intervention period of approximately four to seven weeks. The interactive lessons incorporated units of various media formats, such as texts, audios and videos. Additionally, subjects could make use of an inbuilt read-out function. Further key elements were exercises, the encouragement to keep a daily stress diary and homework assignments, as the intervention aimed to assist participants in fostering newly acquired stress management techniques in their everyday life. Furthermore, participants were able to decide if they wanted to receive automatic motivational text messages and short exercises (e.g., for relaxation) to their mobile phones and if their frequency should be rather low (one text message alternately) or intense (two to three text messages daily). The responsive web application could be accessed through mobile phones and (tablet) computers. A more comprehensive description of the intervention can be found in the study protocol [35].
Adherence-focused guidance (AFG)
Previous studies established AFG as guidance format which comprises (1) adherence monitoring and (2) feedback on demand by e-coaches [38]. Every subject was assigned to an e-coach in a one-to-one ratio throughout the intervention. The e-coaches were trained psychologists that followed guidelines for the feedback process based on the standardised manual for the intervention. Adherence was monitored by frequently checking for duly module completion and sending reminders if subjects did not finish at least one module within a week. In other studies, reminders (personal and automatic) ameliorated adherence to self-guided health promotion and health behaviour interventions [65,66,67]. Participants received personalised and written feedback on demand only upon request via the internal platform messaging system within 48 h. Contact to an e-coach could be established by clicking on the respective button. The provided feedback was expected to enhance adherence and therefore impact the comparative efficacy in favour of this study condition [42, 68]. Based on the Supportive Accountability Model [42], the provided human support by professional e-coaches was supposed to create perceived legitimacy and to be a requirement for positive effects of the monitoring part of AFG. Notably, it is assumed that the two elements of AFG (i.e., monitoring and feedback on demand) intertwine with each other in regard to their effects on adherence.
Self-help (SH)
Subjects in the SH-arm could contact the study administration and received support in case of technical issues.
Wait list control group (WLC)
The WLC-arm obtained access to the self-help intervention 6 months after randomisation. Priorly, they had full access to TAU through routine healthcare services.
Measures
Data was collected online between March 2014 and July 2015 with German self-report measures at successive assessments in time: screening for eligibility (T0), at baseline (T1), 7 weeks after randomisation (T2) and at a 6-month follow-up (T3). Further questionnaires used [35] will be taken into account in future publications.
Primary outcome measure
Primary outcome was the subjective stress level measured by the German version of the 10-item Perceived Stress Scale (PSS-10) [57, 69]. Since the PSS-10 was developed based on Lazarus’ transactional model of stress, it was assumed to be most suitable regarding the intervention’s content. The self-report items of this well-established questionnaire assess to what extent participants experienced their lives as stressful, i.e. as overstraining, unmanageable and unforeseeable in the past month. To avoid confounding with the training period (from T1 to T2), subjects in this study were asked to answer the questions against the background of their past week [69]. Respondents evaluate the items on a five-point Likert scale from 0 (never) to 4 (very often), resulting in sum score ranges from 0 to 40. Accordingly, the higher the sum score values, the more elevated stress levels are perceived. Sample item: “How often have you felt that you were unable to control the important things in your life?”. The scale was psychometrically evaluated in a German community sample and shown to have good internal consistency and construct validity [70]. For different samples, internal reliabilities (Cronbach’s α) were found to be .78 and .91 [71].
Secondary outcome measures
Health impairing and promoting mediators
Secondary outcomes included the examination of depression severity with the short version of the Centre for Epidemiological Studies’ Depression Scale (CES-D) [72, 73], with 15 items that are responded to on a four-point Likert scale from 0 to 3 (α = .95). Sample item: “I felt depressed”. The Connor-Davidson Resilience Scale (CD-RISC) [74] was used to examine resilience, measured with ten items on a five-point Likert scale from 0 to 4 (α = .85). Sample item: “Deal with whatever comes my way”. Emotional exhaustion was measured with the corresponding subscale of the Maslach Burnout Inventory (MBI-GS-D) [75, 76]. This scale is composed of five items that are rated from 1 to 6 (α = .85). Sample item: “I feel emotionally drained from my work”.
Work-related health
Work engagement was examined with the Utrecht Work Engagement Scale (UWES) [77, 78] that distinguishes between the three subcomponents dedication, vigour and absorption and consists of 9 items which are assessed on a 7-point Likert scale from 0 to 6 (α = .9). Sample item: “I am enthusiastic about my job”.
Work-related productivity
Presenteeism was assessed with the Work Limitations Questionnaire (WLQ) [79] and a single-item work ability question (WAI) [80]. Sample items: “Experience physical or mental problems speaking to others in person/on phone”, and “How would you rate your current ability to work?” respectively. In addition, the Effort Reward Imbalance Questionnaire – Short Form (ERI-SF) [81] was used with 10 items with a Likert-scale from 1 to 4 that compose the three scales effort, reward and overcommitment (αs = .77, .82 and .83, respectively). Sample item: “I have many interruptions and disturbances while performing my job”.
Client satisfaction and intervention usage
The Client Satisfaction Questionnaire adapted to Internet-based interventions (CSQ-I) [82] was used to investigate the participants’ satisfaction with the intervention. This comprises eight items with a range from 0 to 4. Reported values for the reliability indicated by McDonald omegas were .93–.95. Sample item: “I received the kind of training I wanted”. For an in-depth analysis, participants were required to answer questions about the different guidance formats (e.g. “What kind of guidance would you prefer if you would participate in a training of this kind again?”, “How often did you make use of the possibility to get in touch with an e-coach?”). In order to take these figures into account, the number of inquired feedbacks, as well as the amount of messages e-coaches sent to participants was checked for on the internal platform messaging system.
Other measures
For a description of the sample, we assessed various demographic variables such as sex, age, marital status, ethnicity, educational level, employment, work sector of employment, income and the previous use of health services.
Statistical analyses
The statistical analyses adhered to the pre-published study protocol [35]. They were carried out using IBM SPSS Statistics 25 [83] and according to the Consolidated Standards of Reporting Trials (CONSORT) guidelines [84, 85]. Consequently, analyses were conducted on the intention-to-treat (ITT) basis handling missing data with multiple imputations [86]. For this purpose, 10 estimates were calculated for each missing data point that were aggregated into a single overall value. To evaluate the efficacy of the intervention, analyses of covariance (ANCOVA) were conducted with respective outcome baseline values specified as covariates. Earlier simulation studies demonstrated the methodological robustness of ANCOVA for analysing experimental studies in terms of protecting against bias, higher precision and statistical power [87, 88]. For all analyses, a two-tailed significance level was set at P < .05. Deviating from the study protocol [35], Cohen’s d [89] was calculated by standardised deviations (SD) of the respective measurement points. Restricted variance in baseline scores would lead to smaller SD and the risk of an overestimation of effects. Therefore, effect sizes were calculated in a more conservative manner. Additionally, per protocol analyses (PPA) were performed for the primary outcome, including only satisfying protocol treatment and therefore solely subjects who completed at least six of the training modules.
Response analyses
To examine the clinical significance of a positive outcome, the reliable change index (RCI) defined by Jacobson and Truax was used [90]. In this manner, the SD of the norm population (6.2) and the reliability of the PSS-10 scale (α = .91) from samples in 2006 and 2009 were used in the respective formula [1.96*SD1*sqrt(2)*sqrt(1-rel)]. Eventually, an individual change over time was considered significantly reliable when the PSS-score differed more than ±5.16 points from T1 to T2 and T1 to T3. A cut-off value for symptom-free status was defined as more than 2 SDs below the mean (T1) value of the primary outcome (PSS-10 < 17.33). The number needed to treat (NNT) was calculated which indicates the average number of participants that need to be treated to achieve an additional response compared to the control condition and therefore prevent a non-response.
Mediation analysis
To explore how an effective stress reduction could lead to a prevention of depression, a mediation analysis based on a framework considering multiple pathways was conducted. Since depression can be preceded by stress, this was considered as potentially health impairing process as opposed to a health promoting process with resilience as a protective factor against the development or maintenance of depressive symptoms. Within this framework, perceived stress measured with PSS-10 [57, 69] was considered as potential risk factor to depression, hence to instigate a health impairing process. Resilience assessed with CD-RISC [55] on the other hand was assumed to be protective against the development of depressive symptoms as a result of work stress. A dual pathway with both factors mediating the efficacy in concert was also examined. For this purpose, a parallel mediation analysis was carried out using the PROCESS macro (v3.3) for SPSS (model 4) [91]. Temporal precedence was established by using T2-measurements of the mediators and the outcome values assessed at T3. In this model, baseline score for the potential mediators and the outcome were included as covariates [92]. Bias-corrected bootstrap with 10,000 samples was applied for indirect effects that were considered significant if 95% confidence intervals (CI) did not cover zero [91].
Results
Participants
The sample consisted of 404 participants (77% female), aged 18–62 years (M = 41.93, SD = 9.14) that were randomly allocated to the three study conditions AFG (n = 135), SH (n = 134) or WLC (n = 135). At enrolment, PSS-10 mean scores numbered in 26.44 for AFG (SD = 2.92), 26.82 for SH (SD = 3.44), and 26.36 for WLC (SD = 3.05). All assessed baseline characteristics are summarised in Table 2 and the study flow is depicted in Fig. 1. The study aimed to include 408 subjects at T1 for allocation but with four participants failing to fully meet employment requirement, they had to be excluded from the analysis at closer data inspection. At enrolment, 726 subjects were recruited of which 322 did not fulfil the inclusion criteria. Satisfying protocol treatment for PPA analysis (completion of at least six modules) was available for 101 subjects in AFG (75%) and 80 in SH (60%). Study dropout rates for the assessments were as follows: at T2, AFG n = 12 (9%), SH n = 7 (5%), WLC n = 3 (2%) and at T3, AFG n = 29 (21%), SH n = 22 (16%), WLC n = 15 (11%). For the primary outcome, data were missing for 5% at T2 and 16% at T3. To examine if data was missing completely at random (MCAR) Little’s test was applied. The null hypothesis for Little’s test is that data are MCAR, thus patterns of missing scores are not associated with observed and unobserved factors among the subjects’ values. Little’s test of randomness failed statistical significance (P = 0.16), indicating the hypothesis of data MCAR did not need to be rejected. Therefore, multiple imputations were conducted [86].

Study Flow
Primary outcome analysis
All three study groups showed an improvement in perceived stress levels from T1 to T2 and T3 (Fig. 2). At T2, analysis of covariance according to the study protocol [35] revealed a significant group effect (F2,400 = 36.08, P < .001) with large between group effect sizes for both AFG (d = 0.83; 95% CI 0.58–1.08) and SH (d = 0.88; 95% CI 0.63–1.13) in comparison to the control group (Table 3). A significant between group effect was also found for T3 (F2,400 = 37.04, P < .001) with large effect sizes for AFG (d = 0.85; 95% CI 0.60–1.10) and SH (d = 0.91; 95% CI 0.66–1.16) compared to WLC. No significant group differences were found between AFG and SH for the primary outcome. See Table 4 for means and standard deviations for all study groups on primary and secondary outcomes.

Comparison of adherence-focused guidance (AFG), self-help (SH) and waitlist control condition (WLC) on development of perceived stress measured with PSS-10 at T1 (baseline), T2 (after 7 weeks) and T3 (6-month follow-up)
Reliable change, symptom-free status, NNT
At T2, the majority of subjects in the intervention groups showed a reliable improvement on perceived stress assessed with PSS-10 (AFG: 84/123, 68%; SH: 80/127, 63%) compared to participants in WLC (39/131, 30%). Fewer symptom deterioration was found in the intervention groups (AFG: 3/123, 2%; SH: 3/127, 2%) than for WLC (7/131, 5%). These differences were statistically significant [χ2 = 4, (N = 381) = 45.11, P < .001].
At T3, a reliable improvement was present for both AFG (77/106, 73%) and SH (72/112, 64%) whereas this number was lower for WLC (26/119, 22%). Reliable deterioration again turned out lower for AFG (3/106, 3%) and SH (2/112, 2%) in comparison to WLC (7/119, 6%). Again, these differences were statistically significant [χ2 = 4, (N = 337) = 68.66, P < .001]. The NNT to achieve reliable improvement between T1 and T3 is 6, 95% CI [3.1, 26.7]. Furthermore, a significantly larger number of participants in the intervention groups could be considered as symptom-free (SH: 57, 43%; AFG: 69, 51%) compared to WLC (24, 18%) at T3 [χ2 = 2, (N = 404) = 34.64, P < .001].
Sensitivity analyses
In accordance with the study protocol [35], PPA including only subjects’ satisfying protocol treatment were conducted to test for the robustness of the main analyses (ITT) and revealed similar results. Significant between group effects were observed at T2 (F2,217 = 19.75, P < .001) with large effect sizes for AFG (d = 1.00, 95% CI 0.61–1.38) and SH (d = 1.11, 95% CI 0.71–1.52) compared to WLC. At T3, a significant group effect was found (F2,217 = 23.88, P < .001), again with large effect sizes for AFG (d = 1.22; 95% CI 0.83–1.62) and SH (d = 1.10; 95% CI 0.70–1.50). Again, the guided (AFG) and unguided (SH) conditions did not differ significantly from each other.
In addition, sensitivity analyses were performed to prevent bias due to the choice of the statistical approach. Therefore, all hypotheses were also tested applying repeated measures analysis of variance (ANOVA). All results could be replicated as indicated by the respective time x group effect.
Secondary outcome analyses
Results of the ITT-analyses for the secondary outcomes are shown in Table 3. For both T2 and T3, ANCOVAs resulted in highly significant between-group effects with significance levels of P < .001 for most of the outcomes. The only non-significant result was the between-group effect assessed for ERI-effort at T2 (P = 0.67). At T2, effect sizes ranged from small (e.g., ERI-reward with d = 0.21 for AFG and d = 0.19 for SH) to moderate (e.g., WAI with d = 0.40 for AFG and d = 0.43 for SH) to large (e.g., MBI-GS-D with d = 0.80 for AFG and d = 0.83 for SH). For T3, detected changes in the effect sizes were mixed with partly decreases of already low effect sizes (e.g., ERI-reward with d = 0.13 for AFG and d = 0.25 for SH) and partly enhancements of large effect sizes (e.g., MBI-GS-D with d = 0.84 for AFG and d = 0.91 for SH).
Training satisfaction and intervention usage
Client satisfaction assessed with CSQ-I did not significantly differ for the study arms, neither at T2 (F267,1 = 0.61, P = .437), nor at T3 (F267,1 = 0.47, P = .494). Frequencies for module completion differed significantly from each other (F267,1 = 35.31, P = .008). On average, subjects in the AFG group completed 5.9 modules (SD = 2.01) compared to 5.17 in the SH condition (SD = 2.38). As shown in Fig. 3, the majority in AFG completed the seven core modules (97/135, 72%) compared to SH (71/135, 53%).

Number (percentages) of participants who completed the module (based on log-data)
Frequencies of given feedback and reminders
Table 5 shows the frequency distribution of responses to the questionnaire used to gather feedback on the provided guidance format. In the AFG condition, 17 subjects stated they have made use of feedback on demand. However, the manual check for these numbers on the messaging platform showed that 37 participants attempted to establish contact to an e-coach. 60 feedbacks were inquired in total across all participants (per subject: M = 0.44, SD = 0.94, range 0–5). Additionally, 453 reminders were sent (per subject: M = 3.36, SD = 1.88, range 0–9). Hence, e-coaches spent most of the time rather on adherence monitoring than giving feedback.
Mediation analysis
As depicted in Fig. 4, perceived stress assessed with PSS-10 at T2 significantly mediated the intervention effect on depression (CES-D) at T3: a1b1 = − 0.77, 95% CI [− 1.26, − 0.34]. Resilience measured with CD-RISC at T2 also significantly mediated the intervention effect on depression (CES-D) at T3: a2b2 = − 0.62, 95% CI [− 1.05, − 0.26]. After these mediators were incorporated into the model, the direct effect of the intervention on depression remained significant: c’ = − 1.08 [− 1.95, − 0.21].

Parallel multiple mediation analysis with study condition as independent variable (coded 0 = waitlist control group, 1 = self-help, 2 = adherence-focused guidance), perceived stress (PSS-10) and resilience (CD-RISC) scores at post-intervention (T2) as mediators, 6-month follow-up depression values (T3) as outcome variable, and baseline values of mediators and outcome as covariates. Unstandardised beta coefficients are shown with 95% (bootstrapped biased corrected) CIs in parentheses
Discussion
This study aimed to investigate the comparative efficacy of different guidance formats on perceived stress within a web-based occupational SMI. Three arms were included in this trial to compare adherence-focused guidance, self-help and a wait list control group. With work stress being a major risk factor for the pathogenesis of depression which again is a leading cause for the contribution to the burden of disease [8], another objective was to reveal important insights into mechanisms of change to explore by which processes the SMI could have an impact on depressive symptoms. Understanding these mechanisms of change is of great interest and importance for health promotion, as offering SMI is a regarded strategy to prevent depression. To investigate potential mediators of the SMI’s efficacy on a reduction of depressive symptomatology, perceived stress was regarded as potentially health impairing mediator while resilience opposingly was considered a protective factor.
The results suggest that the intervention could effectively reduce perceived stress in employees, irrespective of the guidance format. Thus, the expected difference in efficacy between the two delivery modes AFG or SH was not found. For both intervention groups, the effect could be maintained at T3. Sensitivity analyses corroborated results of the ITT analyses and revealed even larger effect sizes.
The present study demonstrated higher effect sizes than a recent meta-analysis across 26 studies on web-based SMI with various guidance formats compared to different kinds of control groups (wait list control, attention control, alternative or no treatment) with an overall effect size of d = 0.43 for stress as primary outcome [15]. The yielded lower overall effect size compared to the higher effect sizes found in this study could be due to several reasons. It is important to note that heterogenous, not-specifically occupational interventions were included in this meta-analysis. Thus, study conditions, guidance formats, delivery mode or the length of these interventions could be various. This also accounts for the applied recruitment strategy which can vary between the studies and was shown to enhance treatment effects when open recruitment was used like in this trial [29]. The high levels of perceived stress subjects reported in this study at enrolment might indicate a high intrinsic motivation for the participation in this SMI and could have led to a greater benefit compared to subjects with lower baseline scores. Furthermore, higher levels of perceived stress at baseline might lead to a greater effect size due to the potential of improvement compared to lower scores at study enrolment.
Another potential explanation for the higher effect sizes found in this study might be found in the fact that the training comprises just two main components, namely emotion regulation and problem solving that are theoretically grounded in Lazarus’ transactional model of stress [60], comprising the two core components emotion regulation and problem solving. Research on traditional stress management programs suggests focussing on fewer components could be more effective than adding numerous modules [93]. This could possibly facilitate positive exercise effects and foster learning experiences due to the repeated revision of training contents. To the best of our knowledge, this is the first study on a web-based SMI investigating the comparative efficacy of different guidance formats within one trial, thus evidence for differential effects is limited and the present results can only be compared to heterogenous studies that each individually examined mostly only one type of guidance. Results of two individual trials investigating the same web-based SMI with each AFG [49] and SH [36] both also demonstrated comparably high effect sizes. In brief summary, this study is in line with previous research and adds to the hitherto missing evidence of the comparative efficacy of different guidance formats within one trial.
Concerning the non-significant differences between AFG and SH with regard to effects on the primary outcome, it should be noted that the intensity of guidance for AFG was per se low, and most resources were spent on adherence monitoring instead of providing feedback on demand. Albeit non-significant differences for the primary outcome, adherence in terms of completed modules was significantly higher for AFG than SH in this study. Another study investigated the comparative efficacy of AFG and SH under similar conditions within an Internet Intervention for problematic drinking in employees and also showed that despite missing between group differences, adherence was better for AFG [94]. Equally in the present trial, participants in the AFG condition completed significantly more modules (5.90) compared to SH (5.17). Additional to the monitoring, participants in the AFG condition could receive feedback on demand. 28% of the subjects in this group (37/134) made use of the latter and received 60 feedbacks in total, next to 453 reminders that were sent in sum. Similarly small numbers of participants demanding feedback were found before in trials on the same SMI, with e-coaches also spending more time on adherence monitoring [50]. In these trials, the amount of subjects making use of feedback on demand numbered 6% (8/132) [49] and 11% (15/102) [50]. In the aforementioned RCT on a web-based intervention for problematic drinking in employees, 10% (15/144) made use of feedback on demand [94].
At first glance, this could lead to the conclusion that guidance might not be conducive to the efficacy of web-based SMI. However, this needs to be considered cautiously. First, this would be a false conclusion since the utilisation rate of AFG was low, not only in the present trial but also previous ones [50, 94]. Second, reasons for this can be manifold. For example, results of the questionnaire on utilisation of and satisfaction with AFG indicated that the majority of this group was not even aware of their assigned condition. Instead, more than half of the AFG-subjects (53%) assumed receiving a pure SH-intervention. Moreover, 43% of the AFG-subjects (SH: 43%) stated they would have preferred regular feedback by an e-coach on their assignments which would furthermore be preferred by 48% (SH: 41%) if they would participate in a similar training again. In conclusion, it seems that the low utilisation rate of feedback on demand as part of AFG could possibly be due to a lack of awareness of what was offered. It can be speculated that information on the availability of personal feedback from the e-coach should have been presented more prominently and that such awareness-raising measures could have been helpful. In this way, e-coaches could for example contact participants more actively by encouraging them to make us of the AFG and offering their feedback. Another possibility to promote acceptance could be the use of educational videos to explain the delivery mode in more detail. To conclude, it seems that the monitoring component of AFG might promote adherence but might not be sufficient to enhance efficacy with such low utilisation rates of the offered feedback on demand. The superiority of AFG for adherence was not mirrored for the outcomes since results demonstrated high effect sizes for SH and adherence defined as the average amount of completed modules was satisfying for this group. On the one hand, this leads to the question if the usage of AFG is justifiable against the background of required resources. On the other hand, the level of guidance was per se low for AFG, thus differences compared to SH might be challenging to detect because they could be small by default.
Analyses of secondary measures demonstrated that the present web-based SMI came into effect on the majority of the outcomes such as depression, resilience, emotional exhaustion, work engagement, presenteeism and work ability. In more detail, effect sizes for the reduction of depressive symptoms were found to be high for each intervention group compared to WLC (at post-intervention, d = 0.62 for SH and d = 0.74 for AFG). These effect sizes are higher than those observed in a meta-analysis on the efficacy of SMI on depression (d = 0.34) [15]. Notably, earlier studies reported consistently higher effect sizes for guided Internet Interventions than unguided interventions [15, 39]. It seems interesting to note that all variables directly related to the subjects changed over time and that no significant effect was found for ERI-effort at T2 (P = .67) which from a conceptual point of view is a measure of the workplace situation. Comparable to the primary outcome, no significant differences were found between AFG and SH, although this should again be interpreted cautiously for already stated reasons.
Another important objective of this study was to examine mediating interventional effects on depressive symptoms. This is of great interest for practical and theoretical reasons and there is a growing need for such research [95, 96]. To date, research is limited to observational studies that identified stress as risk factor for the development of depression [6]. The use of SMI to prevent depression therefore seems reasonable, though interventional studies and more in-depth analyses of this relationship are missing yet. Beyond the reduction of perceived stress, the present SMI became efficacious on a pathological dimension by also reducing depressive symptoms. This result highlights the potential of the SMI in regard to the prevention of mental health disorders.
Results of the mediation analysis demonstrated the applicability of the proposed framework and showed that both considered paths mediated the intervention’s effect on depressive symptoms. On the one side, the intervention could positively affect perceived stress which again had a positive preventive effect on depressive symptoms. On the other side, the intervention also positively affected resilience which seemed conducive to a health promoting process and depressive symptoms eventually. These results reveal interesting insights into the question of how depressive symptoms could be reduced and prevented. Depressive symptomatology was less pronounced when participants on the one side perceived less stress and on the other side were more resilient. A similar pattern with interventional effects based on reducing negative factors on the one hand and building up positive ones on the other hand was also found in an earlier study on a web-based gratitude training which examined mediation analyses based on the same approach of a dual pathway [97].
Despite years of research on the effects of stress and resilience in an occupational context, mechanisms of change of SMI have not received attention yet. However, research not limited to interventional studies showed that resilience as a core protective factor can be developed at work and comes into effect especially in employees at a greater risk of experiencing high strain [98]. Taken together with the present results, important implications for practitioners and health intervention developers can be drawn. The present interventional study is in line with results of earlier observational studies and adds further evidence. Taken together, the findings suggest a contentual integration of both, the health impairing and health promoting processes. Participants should be supported in reducing risk factors such as stress and building up protective factors such as resilience.
Previous research has shown that Internet Interventions could be as effective as face-to-face settings [26,27,28]. However, evidence is only available on indirect comparisons; well designed and adequately powered head-to-head comparisons are yet missing [99]. Traditional face-to-face settings are characterised by certain features such as a group setting, a fixed venue or a pace depending on the training schedule which obviously are different to the typical characteristics of Internet Interventions (see [99] for a full comparison of both). The differences in the typical characteristics of both delivery modes can be an advantage for one participant (e.g. experiencing a motivating group atmosphere) and an obstacle for the other (e.g. high threshold to participate in group setting with social anxiety). Unfortunately, evidence for selective indication is missing. Interestingly, several studies on web-based SMI reported that the vast majority of participants have no experiences with previous face-to-face trainings [36, 49, 61], indicating that both delivery modes (traditional vs. online) reach their audience and thereby increase the overall reach and uptake of SMI.
This study had several limitations. First, the utilised SMI was for the indicated prevention of work stress related adverse health outcomes. This required an elevated stress level for participants to be included in the study. Therefore, resulting conclusions from this study cannot be generalised to populations showing lower stress levels or to a setting in universal prevention. However, from a methodological perspective, this allows for comparisons to studies with similar inclusion criteria. Second, limited generalisability of the results due to the recruitment strategy in this trial must be considered. This trial directly addressed subjects and therefore provides no insights with regard to an implementation into Corporate Health Management. In future research, it should therefore be considered offering SMI for employees in actual occupational setting, e.g. company health management programs. Third, only few participants in the AFG condition made use of the personalised feedback and many of them were not aware that their guidance comprised this opportunity. The low utilisation rate of the guidance suggests it would have been advisable to conduct a pre-test. This could ensure that participants who do not engage with the offered components of guidance (i.e. feedback on demand) deliberately decide against this but are aware of their options.
Finally, further research is needed to fully capture the comparative efficacy of different guidance formats. Participants should receive guidance facilitating and awareness-raising measures to know that and how they can make use of the accompanying guidance. Ideally, they could make an informed decision about the extent to which they would like to inquire feedbacks and determine the dose-response relationship. Other reasons for the low utilisation rate for AFG could also be considered and influencing factors examined, for example if and to what extent personal presence of e-coaches is necessary. Due to the low intensity of guidance for AFG, existing differences for the comparative efficacy could be difficult to detect compared to SH. Therefore, more heterogeneous trials on the impact of guidance are still necessary and could for example compare adherence-focused to content-focused guidance [38]. For future studies, it could also be an interesting approach to explore and disentangle the effects of the two single components of AFG, namely monitoring and giving feedback on demand.
Conclusions
The present study contributes to the scarce evidence on the comparative impact of guidance to the efficacy of SMI, next to mechanisms of change of depressive symptoms. To the best of our knowledge, no previous study has compared different guidance formats within a single trial on SMI. The results showed that the SMI was effective in reducing perceived stress as primary outcome, next to various other work- and mental health-related outcomes such as depression or burnout. However, no between group differences were found for the effect sizes when comparing AFG to SH. This supports a growing body of research showing that SMI with a limited amount of resources can be effective. Despite missing significant between group differences for the outcomes, it should be noted that adherence in terms of module completion was significantly better for AFG than SH. Due to the low utilisation rate of AFG, the results should furthermore be interpreted cautiously regarding the question of how much guidance is necessary for an efficacious and well-accepted SMI. Future studies should therefore focus on further capturing differences between different guidance formats and explore how the better adherence for AFG could also lead to better outcomes compared to SH. Guidance formats could for example be more distinguishable than AFG compared to SH to examine the incremental value of more intensive guidance. Another important conclusion for future studies is to attempt higher utilisation rates when guidance is offered, irrespective of its kind. Furthermore, the results showed that stress and resilience mediated the effects on depressive symptomatology. This interventional study therefore adds evidence to earlier observational studies on the relationships between stress and depression and resilience and depression. Important implications for practitioners and research can be derived to consider both pathways of a health impairing and health promoting process in designing such interventions.
Availability of data and materials
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- AFG:
-
Adherence-focused guidance
- ANCOVA:
-
Analysis of covariance
- ANOVA:
-
Analysis of variance
- BDI:
-
Beck depression inventory
- CD-RISC:
-
Connor-Davidson resilience scale
- CES-D:
-
Centre for epidemiological studies’ depression scale
- CI:
-
Confidence interval
- CONSORT:
-
Consolidated standards of reporting trials
- CSQ-I:
-
Client satisfaction questionnaire adapted to Internet-based interventions
- ERI-SF:
-
Effort reward imbalance questionnaire – short form
- GCP:
-
Good clinical practice
- ITT:
-
Intention-to-treat
- JD-R:
-
Job-demands-resources model
- MBI-GS-D:
-
Maslach burnout inventory
- MCAR:
-
Missing completely at random
- NNT:
-
Number needed to treat
- PPA:
-
Per protocol analysis
- PSS-10:
-
Perceived stress scale
- RCI:
-
Reliable change index
- RCT:
-
Randomised controlled trial
- SD:
-
Standard deviation
- SH:
-
Self-help
- SMI:
-
Stress management intervention
- TAU:
-
Treatment as usual
- UWES:
-
Utrecht work engagement scale
- WAI:
-
Work ability index
- WHO:
-
World health organization
- WLC:
-
Wait list control group
- WLQ:
-
Work limitations questionnaire
References
Kim H-G, Cheon E-J, Bai D-S, Lee YH, Koo B-H. Stress and heart rate variability: a meta-analysis and review of the literature. Psychiatry Investig. 2018;15:235–45. https://doi.org/10.30773/pi.2017.08.17.
Watanabe K, Sakuraya A, Kawakami N, Imamura K, Ando E, Asai Y, et al. Work-related psychosocial factors and metabolic syndrome onset among workers: a systematic review and meta-analysis. Obes Rev. 2018;19(11):1557–68. https://doi.org/10.1111/obr.12725.
Nixon AE, Mazzola JJ, Bauer J, Krueger JR, Spector PE. Can work make you sick? A meta-analysis of the relationships between job stressors and physical symptoms. Work Stress. 2011;25(1):1–22. https://doi.org/10.1080/02678373.2011.569175.
van der Molen HF, Nieuwenhuijsen K, Frings-Dresen MHW, de Groene G. Work-related psychosocial risk factors for stress-related mental disorders: an updated systematic review and meta-analysis. BMJ Open. 2020;10(7):e034849. https://doi.org/10.1136/bmjopen-2019-034849.
Duchaine CS, Aubé K, Gilbert-Ouimet M, Vézina M, Ndjaboué R, Massamba V, et al. Psychosocial stressors at work and the risk of sickness absence due to a diagnosed mental disorder. JAMA Psychiatry. 2020;77(8):842–51. https://doi.org/10.1001/jamapsychiatry.2020.0322.
Madsen IEH, Nyberg ST, Magnusson Hanson LL, Ferrie JE, Ahola K, Alfredsson L, et al. Job strain as a risk factor for clinical depression: systematic review and meta-analysis with additional individual participant data. Psychol Med. 2017;47(8):1342–56. https://doi.org/10.1017/S003329171600355X.
Andrea H, Bültmann U, van Amelsvoort LGPM, Kant Y. The incidence of anxiety and depression among employees-the role of psychosocial work characteristics. Depress Anxiety. 2009;26(11):1040–8. https://doi.org/10.1002/da.20516.
Mathers CD, Loncar D. Projections of global mortality and burden of disease from 2002 to 2030. PLoS Med. 2006;3(11):e442. https://doi.org/10.1371/journal.pmed.0030442.
World Health Organization. The global burden of disease: 2004 update. Geneva: World Health Organization; 2008. https://apps.who.int/iris/handle/10665/43942.
Hassard J, Teoh KRH, Visockaite G, Dewe P, Cox T. The cost of work-related stress to society: a systematic review. J Occup Health Psychol. 2018;23(1):1–17. https://doi.org/10.1037/ocp0000069.
Mitchell RJ, Bates P. Measuring health-related productivity loss. Popul Health Manag. 2011;14(2):93–8. https://doi.org/10.1089/pop.2010.0014.
Health and Safety Executive. Work related stress depression or anxiety statistics in Great Britain, 2018. 2018; October:1–10.
Siegrist J, Li J. Associations of extrinsic and intrinsic components of work stress with health: a systematic review of evidence on the effort-reward imbalance model. Int J Environ Res Public Health. 2016;13(4):432. https://doi.org/10.3390/ijerph13040432.
Sverke M, Hellgren J, Näswall K. No security: a meta-analysis and review of job insecurity and its consequences. J Occup Health Psychol. 2002;7(3):242–64. https://doi.org/10.1037/1076-8998.7.3.242.
Heber E, Ebert DD, Lehr D, Cuijpers P, Berking M, Nobis S, et al. The benefit of web- and computer-based interventions for stress: a systematic review and meta-analysis. J Med Internet Res. 2017;19(2):e32. https://doi.org/10.2196/jmir.5774.
Karyotaki E, Ebert DD, Donkin L, Riper H, Twisk J, Burger S, et al. Do guided internet-based interventions result in clinically relevant changes for patients with depression? An individual participant data meta-analysis. Clin Psychol Rev. 2018;63:80–92. https://doi.org/10.1016/j.cpr.2018.06.007.
Richards D, Richardson T. Computer-based psychological treatments for depression: a systematic review and meta-analysis. Clin Psychol Rev. 2012;32(4):329–42. https://doi.org/10.1016/j.cpr.2012.02.004.
Wind TR, Rijkeboer M, Andersson G, Riper H. The COVID-19 pandemic: The ‘black swan’ for mental health care and a turning point for e-health. Internet Interv. 2020;20 March:100317. https://doi.org/10.1016/j.invent.2020.100317.
Lehr D, Geraedts A, Asplund RP, Heber E, Bloom J De, Ebert DD, et al. Healthy at Work. 2016. https://doi.org/10.1007/978-3-319-32331-2.
Ebert DD, Kählke F, Buntrock C, Berking M, Smit F, Heber E, et al. A health economic outcome evaluation of an internet-based mobile-supported stress management intervention for employees. Scand J Work Environ Health. 2017;c:0–12. https://doi.org/10.5271/sjweh.3691.
Kählke F, Buntrock C, Smit F, Berking M, Lehr D, Heber E, et al. Economic evaluation of an internet-based stress management intervention alongside a randomized controlled trial. JMIR Ment Heal. 2019;6(5):e10866. https://doi.org/10.2196/10866.
Mack S, Jacobi F, Gerschler A, Strehle J, Höfler M, Busch MA, et al. Self-reported utilization of mental health services in the adult German population - evidence for unmet needs? Results of the DEGS1-mental health module (DEGS1-MH). Int J Methods Psychiatr Res. 2014;23(3):289–303. https://doi.org/10.1002/mpr.1438.
Griffiths F, Lindenmeyer A, Powell J, Lowe P, Thorogood M. Why are health care interventions delivered over the internet? a systematic review of the published literature. J Med Internet Res. 2006;8(2):e10. https://doi.org/10.2196/jmir.8.2.e10.
Corrigan P. How stigma interferes with mental health care. Am Psychol. 2004;59(7):614–25. https://doi.org/10.1037/0003-066X.59.7.614.
Rüsch N, Angermeyer MC, Corrigan PW. Mental illness stigma: concepts, consequences, and initiatives to reduce stigma. Eur Psychiatry. 2005;20(8):529–39. https://doi.org/10.1016/j.eurpsy.2005.04.004.
Andersson G, Cuijpers P, Carlbring P, Riper H, Hedman E. Guided internet-based vs. face-to-face cognitive behavior therapy for psychiatric and somatic disorders: a systematic review and meta-analysis. World Psychiatry. 2014;13(3):288–95. https://doi.org/10.1002/wps.20151.
Cuijpers P, Donker T, van Straten A, Li J, Andersson G. Is guided self-help as effective as face-to-face psychotherapy for depression and anxiety disorders? A systematic review and meta-analysis of comparative outcome studies. Psychol Med. 2010;40(12):1943–57. https://doi.org/10.1017/S0033291710000772.
Carlbring P, Andersson G, Cuijpers P, Riper H, Hedman-Lagerlöf E. Internet-based vs. face-to-face cognitive behavior therapy for psychiatric and somatic disorders: an updated systematic review and meta-analysis. Cogn Behav Ther. 2018;47(1):1–18. https://doi.org/10.1080/16506073.2017.1401115.
Phillips EA, Gordeev VS, Schreyögg J. Effectiveness of occupational e-mental health interventions: a systematic review and meta-analysis of randomized controlled trials. Scand J Work Environ Health. 2019;45(6):560–76. https://doi.org/10.5271/sjweh.3839.
Stratton E, Lampit A, Choi I, Calvo RA, Harvey SB, Glozier N. Effectiveness of eHealth interventions for reducing mental health conditions in employees: a systematic review and meta-analysis. PLoS One. 2017;12(12):e0189904. https://doi.org/10.1371/journal.pone.0189904.
Aronsson G, Theorell T, Grape T, Hammarström A, Hogstedt C, Marteinsdottir I, et al. A systematic review including meta-analysis of work environment and burnout symptoms. BMC Public Health. 2017;17(1):264. https://doi.org/10.1186/s12889-017-4153-7.
Siegrist J, Wege N. Adverse psychosocial work environments and depression–a narrative review of selected theoretical models. Front Psychiatry. 2020:1–10. https://doi.org/10.3389/fpsyt.2020.00066.
Deady M, Choi I, Calvo RA, Glozier N, Christensen H, Harvey SB. eHealth interventions for the prevention of depression and anxiety in the general population: a systematic review and meta-analysis. BMC Psychiatry. 2017;17(1):310. https://doi.org/10.1186/s12888-017-1473-1.
Tan L, Wang M-J, Modini M, Joyce S, Mykletun A, Christensen H, et al. Erratum to: preventing the development of depression at work: a systematic review and meta-analysis of universal interventions in the workplace. BMC Med. 2014;12(1):212. https://doi.org/10.1186/s12916-014-0212-4.
Ebert DD, Lehr D, Smit F, Zarski A-C, Riper H, Heber E, et al. Efficacy and cost-effectiveness of minimal guided and unguided internet-based mobile supported stress-management in employees with occupational stress: a three-armed randomised controlled trial. BMC Public Health. 2014;14(1):807. https://doi.org/10.1186/1471-2458-14-807.
Ebert DD, Heber E, Berking M, Riper H, Cuijpers P, Funk B, et al. Self-guided internet-based and mobile-based stress management for employees: results of a randomised controlled trial. Occup Environ Med. 2016;73(5):315–23. https://doi.org/10.1136/oemed-2015-103269.
Karyotaki E, Riper H, Twisk J, Hoogendoorn A, Kleiboer A, Mira A, et al. Efficacy of self-guided internet-based cognitive behavioral therapy in the treatment of depressive symptoms. JAMA Psychiatry. 2017;74(4):351–9. https://doi.org/10.1001/jamapsychiatry.2017.0044.
Zarski A-C, Lehr D, Berking M, Riper H, Cuijpers P, Ebert DD. Adherence to internet-based Mobile-supported stress management: a pooled analysis of individual participant data from three randomized controlled trials. J Med Internet Res. 2016;18(6):e146. https://doi.org/10.2196/jmir.4493.
Baumeister H, Reichler L, Munzinger M, Lin J. The impact of guidance on internet-based mental health interventions — a systematic review. Internet Interv. 2014;1(4):205–15. https://doi.org/10.1016/j.invent.2014.08.003.
Carolan S, Harris PR, Cavanagh K. Improving employee well-being and effectiveness: systematic review and meta-analysis of web-based psychological interventions delivered in the workplace. J Med Internet Res. 2017;19(7):e271. https://doi.org/10.2196/jmir.7583.
Schueller SM, Tomasino KN, Mohr DC. Integrating human support into behavioral intervention technologies: the efficiency model of support. Clin Psychol Sci Pract. 2017;24(1):27–45. https://doi.org/10.1111/cpsp.12173.
Mohr DC, Cuijpers P, Lehman K. Supportive accountability: a model for providing human support to enhance adherence to eHealth interventions. J Med Internet Res. 2011;13(1):e30. https://doi.org/10.2196/jmir.1602.
Andersson G, Titov N. Advantages and limitations of internet-based interventions for common mental disorders. World Psychiatry. 2014;13(1):4–11. https://doi.org/10.1002/wps.20083.
Donkin L, Christensen H, Naismith SL, Neal B, Hickie IB, Glozier N. A systematic review of the impact of adherence on the effectiveness of e-therapies. J Med Internet Res. 2011;13(3):e52. https://doi.org/10.2196/jmir.1772.
Lin J, Faust B, Ebert DD, Krämer L, Baumeister H. A web-based acceptance-facilitating intervention for identifying patients’ acceptance, uptake, and adherence of internet- and Mobile-based pain interventions: randomized controlled trial. J Med Internet Res. 2018;20(8):e244. https://doi.org/10.2196/jmir.9925.
Apolinário-Hagen J, Kemper J, Stürmer C. Public acceptability of E-mental health treatment Services for Psychological Problems: a scoping review. JMIR Ment Heal. 2017;4(2):e10. https://doi.org/10.2196/mental.6186.
Apolinário-Hagen J, Harrer M, Kählke F, Fritsche L, Salewski C, Ebert DD. Public attitudes toward guided internet-based therapies: web-based survey study. JMIR Ment Heal. 2018;5(2):e10735. https://doi.org/10.2196/10735.
Segal ZV, Dimidjian S, Beck A, Boggs JM, Vanderkruik R, Metcalf CA, et al. Outcomes of online mindfulness-based cognitive therapy for patients with residual depressive symptoms. JAMA Psychiatry. 2020;77(6):563–73. https://doi.org/10.1001/jamapsychiatry.2019.4693.
Ebert DD, Lehr D, Heber E, Riper H, Cuijpers P, Berking M. Internet- and mobile-based stress management for employees with adherence-focused guidance: efficacy and mechanism of change. Scand J Work Environ Health. 2016;42(5):382–94. https://doi.org/10.5271/sjweh.3573.
Ebert DD, Buntrock C, Lehr D, Smit F, Riper H, Baumeister H, et al. Effectiveness of web- and Mobile-based treatment of subthreshold depression with adherence-focused guidance: a single-blind randomized controlled trial. Behav Ther. 2018;49(1):71–83. https://doi.org/10.1016/j.beth.2017.05.004.
Christensen H, Griffiths KM, Farrer L. Adherence in internet interventions for anxiety and depression. J Med Internet Res. 2009;11(2):e13. https://doi.org/10.2196/jmir.1194.
Bakker AB, Demerouti E. The job demands-resources model: state of the art. J Manag Psychol. 2007;22(3):309–28. https://doi.org/10.1108/02683940710733115.
Demerouti E, Bakker AB, Nachreiner F, Schaufeli WB. The job demands-resources model of burnout. J Appl Psychol. 2001;86(3):499–512. https://doi.org/10.1037/0021-9010.86.3.499.
Bakker AB, Hakanen JJ, Demerouti E, Xanthopoulou D. Job resources boost work engagement, particularly when job demands are high. J Educ Psychol. 2007;99(2):274–84. https://doi.org/10.1037/0022-0663.99.2.274.
Connor KM, Davidson JRT. Development of a new resilience scale: the Connor-Davidson resilience scale (CD-RISC). Depress Anxiety. 2003;18(2):76–82. https://doi.org/10.1002/da.10113.
Van der Klink JJL, Blonk RWB, Schene AH, Van Dijk FJH. The benefits of interventions for work-related stress. Am J Public Health. 2001;91(2):270–6. https://doi.org/10.2105/AJPH.91.2.270.
Cohen S, Kamarck T, Mermelstein R. A global measure of perceived stress. J Health Soc Behav. 1983;24(4):385–96. https://doi.org/10.2307/2136404.
Lesage F-X, Berjot S, Deschamps F. Psychometric properties of the French versions of the perceived stress scale. Int J Occup Med Environ Health. 2012;25(2):178–84. https://doi.org/10.2478/s13382-012-0024-8.
Beck AT, Steer RA, Brown GK. Beck depression inventory manual. 2nd ed. San Antonio, TX: Psychological Corporation; 1996.
Lazarus RS, Folkman S. Stress, appraisal, and coping. New York: Springer; 1984.
Ebert DD, Lehr D, Boß L, Riper H, Cuijpers P, Andersson G, et al. Efficacy of an internet-based problem-solving training for teachers: results of a randomized controlled trial. Scand J Work Environ Health. 2014;40(6):582–96. https://doi.org/10.5271/sjweh.3449.
Junge MN, Lehr D, Bockting CLH, Berking M, Riper H, Cuijpers P, et al. For whom are internet-based occupational mental health interventions effective? Moderators of internet-based problem-solving training outcome. Internet Interv. 2015;2(1):39–47. https://doi.org/10.1016/j.invent.2014.11.007.
Berking M, Whitley B. Affect regulation training. New York: Springer New York; 2014. https://doi.org/10.1007/978-1-4939-1022-9.
Berking M, Ebert D, Cuijpers P, Hofmann SG. Emotion regulation skills training enhances the efficacy of inpatient cognitive behavioral therapy for major depressive disorder: a randomized controlled trial. Psychother Psychosom. 2013;82(4):234–45. https://doi.org/10.1159/000348448.
Titov N, Dear BF, Johnston L, Lorian C, Zou J, Wootton B, et al. Improving adherence and clinical outcomes in self-guided internet treatment for anxiety and depression: randomised controlled trial. PLoS One. 2013;8(7):e62873. https://doi.org/10.1371/journal.pone.0062873.
Titov N, Dear BF, Johnston L, McEvoy PM, Wootton B, Terides MD, et al. Improving adherence and clinical outcomes in self-guided internet treatment for anxiety and depression: a 12-month follow-up of a randomised controlled trial. PLoS One. 2014;9(2):e89591. https://doi.org/10.1371/journal.pone.0089591.
Fry JP, Neff RA. Periodic prompts and reminders in health promotion and health behavior interventions: systematic review. J Med Internet Res. 2009;11(2):e16. https://doi.org/10.2196/jmir.1138.
Tyler TR. Psychological perspectives on legitimacy and legitimation. Annu Rev Psychol. 2006;57(1):375–400. https://doi.org/10.1146/annurev.psych.57.102904.190038.
Michalsen A, Jeitler M, Brunnhuber S, Lüdtke R, Büssing A, Musial F, et al. Iyengar yoga for distressed women: a 3-armed randomized controlled trial. Evid Based Complement Altern Med. 2012;2012:1–9. https://doi.org/10.1155/2012/408727.
Klein EM, Brähler E, Dreier M, Reinecke L, Müller KW, Schmutzer G, et al. The German version of the perceived stress scale - psychometric characteristics in a representative German community sample. BMC Psychiatry. 2016;16(1):1–10. https://doi.org/10.1186/s12888-016-0875-9.
Cohen S, Janicki-Deverts D. Who’s stressed? Distributions of psychological stress in the United States in probability samples from 1983, 2006, and 20091. J Appl Soc Psychol. 2012;42(6):1320–34. https://doi.org/10.1111/j.1559-1816.2012.00900.x.
Hautzinger M, Bailer M. Allgemeine Depressions Skala: ADS. Manual. Göttingen: Beltz Test GmbH; 1993. http://www.psycontent.com/content/3x081j2m2732r345/.
Lehr D, Hillert A, Schmitz E, Sosnowsky N. Screening depressiver Störungen mittels Allgemeiner Depressions-Skala (ADS-K) und State-Trait Depressions Scales (STDS-T). Diagnostica. 2008;54(2):61–70. https://doi.org/10.1026/0012-1924.54.2.61.
Campbell-Sills L, Stein MB. Psychometric analysis and refinement of the connor–Davidson resilience scale (CD-RISC): validation of a 10-item measure of resilience. J Trauma Stress. 2007;20(6):1019–28. https://doi.org/10.1002/jts.20271.
Schaufeli W, Leiter MP, Maslach C, Jackson SE. Maslach burnout inventory - general survey (MI-GS). In: Maslach C, Jackson SE, Leiter MP, editors. Maslach burnout inventory manual. Palo Alto, CA: Consulting Psychologists Press; 1996.
Neubach B, Schmidt K-H. Gütekriterien einer deutschen Fassung des Maslach Burnout Inventory (MBI-D). Eine Replikationsstudie bei Altenpflegekräften. Zeitschrift Arbeits Organ. 2000;44(3):140–56. https://doi.org/10.1026//0932-4089.44.3.140.
Schaufeli W, Bakker A. Utrecht work engagement scale: test manual. Utrecht: The Netherlands Department of Pychology, Utrecht University; 2003.
Sautier L, Scherwath A, Weis J, Sarkar S, Bosbach M, Schendel M, et al. Assessment of work engagement in patients with hematological malignancies: psychometric properties of the German version of the Utrecht work engagement scale 9 (UWES-9). Rehabilitation (Stuttg). 2015;54(05):297–303. https://doi.org/10.1055/s-0035-1555912.
Lerner D, Amick BC, Rogers WH, Malspeis S, Bungay K, Cynn D. The work limitations questionnaire. Med Care. 2001;39(1):72–85. https://doi.org/10.1097/00005650-200101000-00009.
Ahlstrom L, Grimby-Ekman A, Hagberg M, Dellve L. The work ability index and single-item question: associations with sick leave, symptoms, and health – a prospective study of women on long-term sick leave. Scand J Work Environ Health. 2010;36(5):404–12. https://doi.org/10.5271/sjweh.2917.
Li J, Loerbroks A, Jarczok MN, Schöllgen I, Bosch JA, Mauss D, et al. Psychometric properties and differential explanation of a short measure of effort-reward imbalance at work: a study of industrial workers in Germany. Am J Ind Med. 2012;55(9):808–15. https://doi.org/10.1002/ajim.22018.
Boß L, Lehr D, Reis D, Vis C, Riper H, Berking M, et al. Reliability and validity of assessing user satisfaction with web-based health interventions. J Med Internet Res. 2016;18(8):e234. https://doi.org/10.2196/jmir.5952.
IBM Corp. IBM SPSS Statistics for Windows, Version 25.0. Armonk: IBM Corp.; 2017.
Altman DG. Better reporting of randomised controlled trials: the CONSORT statement. BMJ. 1996;313(7057):570–1. https://doi.org/10.1136/bmj.313.7057.570.
Schulz KF, Altman DG, Moher D, Jüni P, Altman D, Egger M, et al. CONSORT 2010 statement: updated guidelines for reporting parallel group randomised trials. BMC Med. 2010;8(1):18. https://doi.org/10.1186/1741-7015-8-18.
Schafer JL, Graham JW. Missing data: our view of the state of the art. Psychol Methods. 2002;7(2):147–77. https://doi.org/10.1037/1082-989X.7.2.147.
Egbewale BE, Lewis M, Sim J. Bias, precision and statistical power of analysis of covariance in the analysis of randomized trials with baseline imbalance: a simulation study. BMC Med Res Methodol. 2014;14(1):49. https://doi.org/10.1186/1471-2288-14-49.
O’Connell NS, Dai L, Jiang Y, Speiser JL, Ward R, Wei W, et al. Methods for analysis of pre-post data in clinical research: a comparison of five common methods. J Biom Biostat. 2017;08:1–8. https://doi.org/10.4172/2155-6180.1000334.
Cohen J. Statistical power analysis for the behavioral sciences. 2nd ed. Hillsdale, N. J: Lawrence Erlbaum Associates; 1988.
Jacobson NS, Truax P. Clinical significance: a statistical approach to defining meaningful change in psychotherapy research. J Consult Clin Psychol. 1991;59(1):12–9. https://doi.org/10.1037/0022-006X.59.1.12.
Hayes AF. Introduction to mediation, moderation and conditional process analysis. A regression-based approach. Second. New York: The Guilford Press; 2018.
Hayes AF, Rockwood NJ. Regression-based statistical mediation and moderation analysis in clinical research: observations, recommendations, and implementation. Behav Res Ther. 2017;98:39–57. https://doi.org/10.1016/j.brat.2016.11.001.
Richardson KM, Rothstein HR. Effects of occupational stress management intervention programs: a meta-analysis. J Occup Health Psychol. 2008;13(1):69–93. https://doi.org/10.1037/1076-8998.13.1.69.
Boß L, Lehr D, Schaub MP, Paz Castro R, Riper H, Berking M, et al. Efficacy of a web-based intervention with and without guidance for employees with risky drinking: results of a three-arm randomized controlled trial. Addiction. 2018;113(4):635–46. https://doi.org/10.1111/add.14085.
van der Velden AM, Kuyken W, Wattar U, Crane C, Pallesen KJ, Dahlgaard J, et al. A systematic review of mechanisms of change in mindfulness-based cognitive therapy in the treatment of recurrent major depressive disorder. Clin Psychol Rev. 2015;37:26–39. https://doi.org/10.1016/j.cpr.2015.02.001.
Kazdin AE. Evidence-based treatment research: advances, limitations, and next steps. Am Psychol. 2011;66(8):685–98. https://doi.org/10.1037/a0024975.
Heckendorf H, Lehr D, Daniel D, Freund H. Efficacy of an internet and app-based gratitude intervention in reducing repetitive negative thinking and mechanisms of change in the intervention’s effect on anxiety and depression: results from a randomized controll. Behav Res Ther. 2019;119:103415. https://doi.org/10.1016/j.brat.2019.103415.
Vanhove AJ, Herian MN, Perez ALU, Harms PD, Lester PB. Can resilience be developed at work? A meta-analytic review of resilience-building programme effectiveness. J Occup Organ Psychol. 2016;89(2):278–307. https://doi.org/10.1111/joop.12123.
Lehr D, Geraedts A, Asplund RP, Khadjesari Z, Heber E, de Bloom J, et al. Occupational e-mental health: current approaches and promising perspectives for promoting mental health in workers. In: Wiencke M, Cacace M, Fischer S, editors. Healthy at work. Cham: Springer International Publishing; 2016. p. 257–81. https://doi.org/10.1007/978-3-319-32331-2.
Acknowledgements
The authors thank Angelina Scheel and Torsten Tarnowski for contributing to the study administration.
Funding
This study is funded by the European Union (EFRE: ZW6–80119999, CCI 2007DE161PR001) and the BARMER GEK. Open Access funding enabled and organized by Projekt DEAL.
Author information
Authors and Affiliations
Contributions
DE and DL obtained funding for this study. EH, DE and DL contributed to the development of the GET.ON Stress training. DE was responsible for the initial study-design draft, EH, DL and LB contributed to the final study design. EH, DE, DL and LB oversaw the conduct of the study and data collection. PN conducted data analyses. DL, LB oversaw data analyses, DL contributed to interpretation of data and supervised the writing process. PN drafted the manuscript that was revised by EH, DE, DL and LB. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The University of Marburg ethics committee approved of this study (No. 2014-5 K). All participants gave informed written consent. The trial was registered in the German Clinical Trials Register on 06/06/2014 (DRKS00005687).
Consent for publication
Not applicable.
Competing interests
DE, DL and EH are stakeholders in the Institute for Online Health Training which aims to transfer scientific knowledge related to the present research into routine health care. LB and PN do not have any conflicts of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Nixon, P., Boß, L., Heber, E. et al. A three-armed randomised controlled trial investigating the comparative impact of guidance on the efficacy of a web-based stress management intervention and health impairing and promoting mechanisms of prevention. BMC Public Health 21, 1511 (2021). https://doi.org/10.1186/s12889-021-11504-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12889-021-11504-2