
Abstract
Background
Assessing inequities in health services utilization contributes to build effective strategies for health equity promotion. This study aimed to evaluate the socioeconomic inequalities and inequities in health services utilization among hypertensive patients and explore the changes between 2015 and 2019 in Pearl River Delta of China.
Methods
The cross-sectional surveys were conducted using the questionnaire. Eight hundred thirty and one thousand one hundred sixty-six hypertensive patients in 2015 and 2019 were interviewed, respectively. The concentration index (CI) and the horizontal inequity index (HI) were used to access the socioeconomic inequalities and horizontal inequities in outpatient and inpatient health services use. The contribution of influential factors to the overall inequalities was estimated via the concentration index decomposition. Oaxaca-type decomposition technique was utilized to measure the changes in socioeconomic inequalities between the observation periods.
Results
In 2015 and 2019, the CIs for outpatient and inpatient utilization decreased from 0.1498 to 0.1198, 0.1982 to 0.1648, respectively, and the HIs for outpatient and inpatient utilization decreased from 0.1478 to 0.1078, 0.1956 to 0.1390, respectively. Economic status contributed the maximum ratio of the socioeconomic inequalities in the use of outpatient service (81.05% in 2015, 112.89% in 2019) and inpatient service (82.46% in 2015, 114.68% in 2019) in these 2 years. Oaxaca decomposition revealed that educational level (78.30% in outpatient, 53.79% in inpatient) and time to the nearest health facilities (66.78% in outpatient, 31.06% in inpatient) made the main positive contributions to decline the inequalities. While the main factor pushing the equalities toward deterioration was economic status (− 46.11% in outpatient, −76.56% in inpatient).
Conclusion
There were certain declines in the socioeconomic inequalities and inequities in health services utilization by hypertensive patients in Pearl River Delta of China over time. The widening economic gap was the largest contribution to the observed inequalities. Interventions to protect the vulnerable group deserve further concern from policy makers.
Similar content being viewed by others

Background
In the past few decades, reducing inequity in the utilization of health care has been a major goal of health systems [1]. However, it is still being observed globally [2,3,4], even exists in nations that are considered as “more equitable”, such as Norway [5]. China, as the greatest developing country, is no exception. In the report issued by the World Health Organization in 2000, China ranked 188th out of 191 countries in health performance [6].
Indeed, since China began its economic reform in 1978, the gap between the rich and poor has widened and health insurance coverage was small. The sick had to pay a high medical expense, while the poor could not support themselves due to financial difficulty [7]. Fortunately, the seriousness of the issue has drawn the attentions of the Chinese government, and the government had carried out some relevant policies, such as the launch of a new health system reform in 2009. Measures to promote a more equitable health system were implemented in the reform, including strengthening the primary health care system, expanding health insurance coverage, and subsidizing the funding of public health services in poor areas [8]. The number of practicing (assistant) physicians per thousand population increased by 65% from 2009 (1.7) to 2019 (2.8) [9], which was one result of this reform. Universal health coverage is another outstanding achievement. The coverage increased from 56% in urban and 21% in rural in 2003 to almost 90% in 2015 [10, 11]. However, there are strong pieces of evidence of pro-rich inequities in the utilization of health services [12, 13]. Equity of access to health service in the Chinese health care system still a serious concern.
Previous studies have been carried out worldwide on the inequity in the utilization of health services. A study conducted in Norway showed that low-income and less educated individuals as a vulnerable group in the process of seeking hospital outpatient care [5]. Another report observed that the utilization of health care showed a pro-rich inequity in the slum areas, whereas horizontal equity was achieved among the non-slum areas [14]. Terraneo found that compared with the less educated elderly, the more educated make more use of health services because they have more resources, such as cognition, communication, and relationships, which enable them to make more informed choices [15]. It also showed that the poor is facing worse health situations and they require more urgent health services than the rich [16]. Barbosa used the multivariate inequity to analyze the utilization of physician service in Brazil, and found that health insurance coverage and urban location both contribute more to the pro-rich inequity than income [17].
At present, the inequity in health services utilization studies in China are mainly focused in a specific area such as the rural region [13], and special communities such as the middle-aged and elderly [18]. However, there is still a lack of comparative studies on the inequities of outpatient and inpatient services for individuals with chronic non-communicable diseases (NCDs) [19], especially among those with hypertension. Hypertension was ranked the 1st in the number of two-week illnesses and chronic diseases in China according to the 2013 National Health Services Survey [20], and 6.6% of health-care costs are directly related to hypertension [21]. More seriously, compared with other diseases, patients with hypertension often require more frequencies and long-term connecting to health facilities. It has been considered as one significant financial burden to the lower socioeconomic groups which tend to use fewer health services, and it will exacerbate the inequities in the utilization of health services. Therefore, it is important and urgent to pay close attention to the socioeconomic inequality and horizontal inequity of outpatient and inpatient services utilization in patients with hypertension.
The Pearl River Delta, as a major part of Guangdong-Hong Kong-Macao Great Bay Area, is one of the most open and economically dynamic regions in China. At the same time, the medical and health services system in this region is booming. For example, the number of health care institutions increased by 14% from 2009 (17,433) to 2015 (19,870). Of note, the number increased to 25,023 in 2019, which was up 26% from 2015 [22]. However, this area has a heavy burden on NCDs. It is noted that more than one-fifth of middle-aged and elderly residents suffer from two or more chronic diseases [23]. As the development of this region, it attracts not only many domestic migrants from other provinces, but also residents from Hong Kong and Macao. Recent policy has proposed that residents of Hong Kong and Macao who living in Guangdong Province could share the same treatment as mainland residents in education, medical care and old-age care, etc. [24]. This new requirement means that cooperation between the region will no longer be restricted in the economy, but will also focus on society and livelihood issues. A society should grant its citizens equal access to health care for equal need. Under the special circumstances of “one country, two systems”, it is especially crucial to explore the inequities in the utilization of health services and promote the harmonious development of the Great Bay Area.
In such context, this study is to measure socioeconomic inequalities and inequities in health services utilization by hypertensive patients in Pearl River Delta in 2015 and 2019 and to explore whether the condition have been changed. Using decomposition analysis, this study also provides further evidence on the contribution of socioeconomic variables to the distribution of health services utilization among hypertensive individuals.
Methods
Study design and subjects
A data from the cross-sectional study based on a community health survey conducted in Pearl River Delta of China in 2019 was used. Moreover, the data from the same survey we conducted in this region in 2015 was used for comparison. The two study samples were selected by a multistage and stratified random sampling method. The primary sampling units were designated as street communities and the second-stage sampling units were nominated as communities according to the economic level. All information was collected by trained staff through face-to-face household questionnaire interviews, including demographics, socioeconomic variables, and health services utilization. A total of 6153 and 6426 individuals aged 15 and above were sampled from 138 communities or villages in 2015 and 2019, respectively. After excluding data with relevant variables missing and logic error answers, complete data were available for 5507 individuals in 2015, and 5867 individuals in 2019. Overall, 830 and 1166 residents suffered from hypertension in 2015 (15.1%) and 2019 (19.9%) were selected for further analysis.
Measurements
Dependent variables
Two binary outcome variables of health services utilization by hypertensive patients were employed. The following questions of the hypertensive patients were asked: (1) Have you visited a doctor for outpatient care because of hypertension in the past 2 weeks? (2) Have you visited a doctor for inpatient care as a result of hypertension in the past year? The answers to the questions were either “yes” or “no”.
Independent and control variables
In our study, age, sex, and years of hypertension were classified as the need variables. Age was categorized into three-year groups within 65 years old and years of hypertension was also divided into three groups: 1–4, 5–9, and 10 or above.
Economic status, educational level, employment status, marital status, residential location, registration, health insurance, and time to the nearest health facilities were considered as socioeconomic variables (non-need variables).
Household income can directly summarize an individual’s social position and possession of resources that are important for health [25], so we measured economic status by the per capita household income, which was calculated by dividing the total income last year by household size. Total income refers to the income of the household for final expenditure and savings, including cash receipts and in-kind receipts. Then we divided per capita household income into five quintiles, which meant that the lowest and the highest quintile represent the poorest and the richest wealthy quintiles, respectively. In this study, the per capita house income data were inflated to 2019. Finally, the per capita household income in the participants in 2015 was grouped as follows: ≤8738 RMB; 8739 ~ 18,022 RMB; 18,023 ~ 26,947 RMB; 26,948 ~ 34,909 RMB and ≥ 34,910 RMB. The per capita household income in the participants in 2019 was ordered as follows: ≤11,484 RMB; 11,485 ~ 23,760 RMB; 23,761 ~ 40,764 RMB; 40,765 ~ 55,932 RMB and ≥ 55,933 RMB.
Educational levels were grouped into four groups: primary or below education, middle school, high school, and college or above education. Two employment categories and marital categories were employment and unemployment, married and single, respectively. The single includes unmarried, divorced, widowed and separated. Residential location was classified as rural and urban depending on whether the participant resided in an administrative community or village within the last 6 months. The registration was divided into migrants and locals according to whether their domicile is in Guangdong province. Health insurance is based on whether the respondent is covered by the social health insurances. The time to get to the nearest health facilities as fast as possible was divided into two groups: ≤15 min and > 15 min.
Concentration index (CI)
The measurement of socioeconomic inequality in the use of health services is based on a widely accepted index, appointed as CI. CI ranges from − 1 to 1, with the positive value indicating the concentration of the health inequality among the rich and vice versa [26]. The index can be calculated by employing the equation as follows, and the definition of each variable in eq. (1) has been described elsewhere [27].
Decomposition of inequality
To analyze the contribution of independent variables of the inequality, we followed the method proposed by Wagstaff et al. to decompose CI [28]. Probit regressions were employed to calculate the partial effects [27]. The outcome variable (y) is established as the eq. (2):
In eq. (2), where xji is the need variable (e.g. age, sex, and health need), zki is the non-need or socioeconomic variable (e.g. economic status, educational level, and employment status); βj and γk are the marginal effects (dy/dx) of xj and zk; εi indicates the error term. Then, CI for y can be calculated as the eq. (3):
In eq. (3), where \( \overline{\chi_{\mathrm{j}}} \) and \( \overline{Z_k} \) are the means of xj and zk; Cj and Ck are the concentration indexes of xj and zk; μ is the mean of y and GCε is the concentration index of the error term ε. This equation reveals the total concentration index is made up of two components. One of them is the residual, another one is the determinant part [29]. Then we calculated the absolute and the percentage contribution of each regressor. Details of the contribution have been described elsewhere [27].
Horizontal inequity index (HI)
HI is the concentration index that measures the need-standardized health service utilization. It reflects socioeconomic inequality in the use of health services after controlling for the impacts of biological needs, such as age and sex [30]. HI can be computed as follows:
In eq. (4), similar to CI, HI ranges from − 1 to 1. A positive HI suggests that the health service is more concentrated among the richer groups and vice versa.
Decomposition changes in inequality
At this stage, the Oaxaca-type decomposition method was used to decompose the change in inequality [31]. The decomposition formula is as follows and the details of the definition of each variable in eq. (5) have been described elsewhere [32].
All analyses were performed on STATA 14.0. Statistical significance level was set as 0.05.
Results
Social demographic characteristics of respondents
The characteristics of the study population are displayed in Table 1. In 2015 and 2019, the utilization of inpatient service due to hypertension increased greatly, with the growth rate at 34.20%, whereas, a slight rise in the utilization of outpatient service, with a growth rate of 10.64%. Nearly half of the patients were aged 65 or above. More than half of the patients were suffering from hypertension for less than 5 years. Most of the respondents finished middle school. Over half of the participants were unemployed and married. Most of the respondents with hypertension were urban and local residents. The health insurance coverage increased from 97.71 to 99.94% during this period. In terms of access to care, it took most of them less than 15 min to get to the nearest health facilities.
Socioeconomic inequalities and inequities
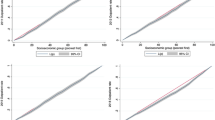
Table 1 also presents CIs and HIs for health services utilization by hypertensive patients. The CIs for outpatient and inpatient utilization, although all of them were positive, decreased from 0.1498 to 0.1198, 0.1982 to 0.1648, respectively, which meant that there were existed pro-rich inequalities in utilization of health services by hypertensive patients, but the inequalities shrank over time (Fig.1). However, as the health services requirement have not been taken into account, inequality is not equivalent to real inequity [18]. Then we calculated the HI. The HIs for outpatient and inpatient utilization decreased from 0.1478 to 0.1078, 0.1956 to 0.1390, respectively, which provides evidence of pro-rich inequities in utilization of health services. In other words, the rich could utilize more health services than the poor even after controlling for their different demands. Compared with the inequities in outpatient utilization, those in inpatient utilization were higher during 2015–2019.

Concentration curves for use of health services, 2015 versus 2019. a. Concentration curves for use of outpatient services. b. Concentration curves for use of inpatient services
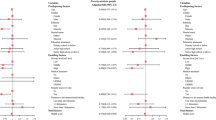
Decomposition of the inequalities
A positive contribution to socioeconomic inequality means that the considered variable increases inequality. Tables 2 and 3 reported the detailed decomposition of CIs for the health services utilization by hypertensive patients in the two survey-years. As can be seen from the results, the need variables of 65 years or above and years of hypertension more than 10 years displayed contribution in favor of the affluent. Among socioeconomic variables, economic status played the greatest contributory role to the inequalities favoring the rich in the utilization of health services.
Notably, the percentage contribution of educational level to the uneven distribution of health services was positive in 2015. Nonetheless, it was negative in 2019, especially in hypertensive patients who completed college or above. In other words, the change of this factor reduced such pro-rich inequalities considerably. Furthermore, the positive contributions of the factors such as registration and time to the nearest health facilities declined to varying degrees over time, which also reduced the observed inequalities. For other remained variables such as employment status, residential location and health insurance, their contributions were relatively small during the observation period.
Decomposition changes in inequalities between 2015 and 2019
As shown in Table 1, the CIs of outpatient and inpatient utilization by hypertensive patients reduced by 0.0300(20.03%) and 0.0334 (16.85%) in 2015 and 2019. Then, the reductions were decomposed to seek contributing factors following by Oaxaca-type decomposition in Table 4. It displayed changes in the amount of inequality in determinants in the second and fourth columns; and the third and seventh columns show changes in elasticities of determinants.
From the changed CIs and elasticities for utilization of health services, we found that the three major contributors to reducing the decrease inequalities, including the educational level, registration, and time to the nearest health facilities. What’s more, changes in employment status, residential location, and health insurance could explain the reduction of CIs to some extent.
However, the changes in economic status accounted for the biggest contributor to the pro-rich inequalities. Also, the need variables of age and years of hypertension pushed these inequalities into deterioration, especially in the utilization of inpatient.
Discussion
Our study explored the socioeconomic inequalities and inequities in the health services utilization by hypertensive patients in Pearl River Delta of China between 2015 and 2019, and further quantifies the contribution of selected factors toward the inequalities. Besides, we also assessed the changes in the inequalities and inequities during the survey-period. The main findings were as follows: 1) Obvious pro-rich inequalities and inequities in utilization of health services by hypertensive patients existed in Pearl River Delta in both periods, but they declined over time. 2) The changes in such inequalities were caused by the alteration in the interaction among the relevant determinants, including economic status, educational level, employment status, residential location, registration, health insurance and time to the nearest health facilities.
The horizontal inequity indexes in 2015 and 2019 showed that there existed pro-rich inequities in utilization of health services by hypertensive patients in Pearl River Delta, which indicated that more health resources were utilized by the wealthier even after controlling people’s different needs. These findings were consistent with the previous studies [33, 34]. However, the study displayed an exciting sign that the degrees of inequities in the use of health services have decreased over time. It could be explained by the measures taken by the Chinese government to ensure equity to health access [35, 36]. The funding subsidy for basic public health services increased from 15 to 40 RMB per capita from 2009 to 2015, even increased to 69 RMB per capita in 2019 [37,38,39]. For hypertensive patients, the Chinese government provides at least one free follow-up visit every 3 months including health evaluation, syndrome surveillance, behavioral intervention, guidance on the use of medicines, and health education [40]. Naturally, these initiatives are supposed to help reduce the disease burden and improve the equities in health services utilization.
In line with other studies [16, 41], HIs also revealed greater inequities in inpatient utilization compared to outpatient utilization in both 2015 and 2019. As the national report showed, financial difficulty is the main reason why low-income people refuse or avoid hospitalization [20]. The price of inpatient service may be much more expensive than the outpatient, and hypertension patients from lower economic status are easier to fall into poverty [16].What’s worse, many low-income people are located in rural areas, which have poor access to hospitals [42]. Compared with the urban patients, rural patients will incur additional costs during hospitalization, such as accommodation and transportation costs, which greatly increase the indirect hospitalization costs. They are more likely to enter a vicious circle of “poverty from illness and disease from poverty”. Besides, the reimbursement rate of hypertensive patients attending basic medical insurance is as high as more than 50%, when they use outpatient services in secondary and lower designated primary medical institutions [43],with no doubt that low-income patients are more likely to choose the outpatient service at an affordable cost than inpatient service by Chinese medical service policy.
Previous literature showed that the pro-rich inequity in the inpatient service in Canada was decreasing over time, while such inequity in outpatient was increasing [1]. However, our survey indicated that the pro-rich inequities in inpatient and outpatient services in the Pearl River Delta of China were gradually reduced over time. Based on an ongoing nationally longitudinal data in China by Xu’s report, it also showed that the inequity of preventive service use in China was alleviating [32]. Findings from some developing countries, such as Mongolia and Mexico [3, 44], indicated the same trend in the inequity in health service utility as ours. Brazil was a bit different, where inpatient service was always in favor of the poor between 1998 and 2008, although the inequity was declining [4]. Affordability and accessibility are the two main components of equal access to qualified health services. The affordability is primarily related to health insurance reimbursement rates and income-related factors; and the availability is primarily related to the allocation of health resources and government policies [42]. As we can see, so great efforts on the two components were made by the Chinese government in the past few years, that the inequalities from 2015 to 2019 were gradually reduced. Notably, despite the inequity in the inpatient service in the Pearl River Delta has decreased in 2019, HI was still higher than that of Mongolia and Mexico [3, 44]. It follows that horizontal equity in health care remains a challenge for this region of China and the government still needs to focus more on this issue.
The decomposition analysis presented that economic status had the most significant association with inequalities in the use of health services by hypertensive patients in Pearl River Delta of China during 2015–2019, furthermore, the positive contribution was increased in 2019. Actually, many studies have proved that the economic status was associated with health services utilization owing to high payment capacity for care by high incomes [45, 46]. It also found that the rich with NCDs tended to overuse the health services, in contrast, the poor with NCDs tended to underuse the health services [41]. However, as Fu’s study showed, people in lower income are generally in poorer health and they have a greater demand for health services [12]. Clearly, the contribution of the economic status was not conducive to the equitable and rational utilization of health services by individuals.
In addition, other socioeconomic variables such as educational level, employment status, residential location, registration and time to the nearest health facilities also can help to explain the uneven distribution of health services utilization over this period [42, 47,48,49]. Generally, a variety of social factors related to an individual’s socioeconomic status have an impact on a person’s health beliefs, which in turn influence one’s health-seeking behavior [48].
Oaxaca decomposition revealed that the changes in inequalities arise from the alteration in the interaction among the related determinants, including economic status, educational level, employment status, residential location, registration, health insurance and time to the nearest health facilities. Changes in the residential location, registration, and time to the nearest health facilities pushed the inequalities towards equality line. These findings were likely to reflect the successful outcome of China’s new health reform and the implementation of recent policies, which aimed at establishing a public health system covering both urban and rural residents and a universal health insurance system through affordable and equitable primary health care [50]. The number of health facilities nationwide reached 1.014 million in 2019, an increase of 24,000 over 2015 [11, 51], even hypertensive patients living in townships and counties can easily get a variety of antihypertensive drugs at a zero profit mark-up from primary care facilities [52]. A “15-minute medical treatment circle” has basically been formed, greatly reducing the distance and time for residents to obtain health services [53]. Significantly, the government of Guangdong Province has taken the lead in implementing the project of a direct settlement of out-of-town medical treatment to ensure the migrants can obtain timely reimbursement [54]. These measures greatly reduced the burden of the migrants suffered from hypertension and bridged urban-rural disparity in health services utilization.
Moreover, the development of employment status and educational attainment have also contributed to reducing there inequalities. A series of employment policies delivered by the government, such as increasing employment opportunities among the economically disadvantaged groups [55], played a role in promoting this trend. For the changes in educational level, a possible explanation may be that the proportion of young hypertensive individuals substantially increased in China [56], leading to an overall increase in patients’ education. It is well-known that health insurance can help to reduce the inequality in health services use [57, 58]. Our study also showed the same result, but the contribution was really limited. The insurance coverage in China exceeded 90% in 2015 and reached 96% in 2019 [11, 51], and the change in the coverage is only about 6% which may explain why health insurance did not contribute largely.
However, we found that the change in economic status has pushed the inequalities in health services usage towards deterioration, which is consistent with another study in China [32]. It may be related to the growing income gap in China. According to the lasted national data, China’s gross domestic product (GDP) per capita increased from 50,237 yuan in 2015 to 70,581 yuan in 2019 [59]. However, rapid growth has brought increased income inequality over the past few years, with the individual income Gini coefficient rising from 0.462 in 2015 to 0.465 in 2019 [60]. There is no doubt that the inequality of income in China ultimately widened the gap in purchasing healthcare services between the rich and poor.
Also, our findings revealed that changes in the need variable of age and years of hypertension made negative contributions to the reduction in such inequalities, particularly in the utilization of inpatient. High blood pressure can reduce the elasticity of the vascular wall and aggravate atherosclerosis with the development of the disease, causing a variety of heart, brain, kidney and other target organ damage. Hypertensive patients who are older or had a long year of hypertension may have high demands for health services, especially for inpatient service. Thereby, more health services were biased toward those people.
This study has some limitations that must be mentioned. Firstly, recall biases could not be avoided in questionnaire-based surveys, especially the self-reported utilization of health services. Secondly, the supply-side variables used in the decomposition only include the time accessibility of health facilities, but lack of other factors, such as the price of health services. Finally, since the decomposition analysis is a descriptive statistic, we were not able to carry out a causality analysis and the results should be interpreted with care. Despite the above limitations, this study has important policy implications for China towards reducing socioeconomic inequalities and inequities in health services utilization among patients suffered from NCDs.
Conclusion
Monitoring of the inequities in health services for people with NCDs can help design effective strategies to improve health equity. Overall, our results indicated that the pro-rich inequities persist in health services utilization by hypertensive patients in Pearl River Delta from 2015 to 2019 and the horizontal inequity in the utilization of inpatient service is higher than that of outpatient service, although there is a reduction of the inequities. The Oaxaca decomposition analysis revealed that the widening income gap is the main factor to exacerbate such inequalities. Health policies alone are not enough to tackle the inequities and more comprehensive social policies are needed to protect the disadvantaged groups, particularly the individuals who suffered from chronic diseases.
Availability of data and materials
The data used during the current study available from the corresponding author (peixi001@163.com) on reasonable request.
Abbreviations
- CI:
-
Concentration index
- HI:
-
Horizontal inequity
- NCDs:
-
Non-communicable diseases
- GDP:
-
Gross domestic product
References
Penning MJ, Zheng C. Income inequities in health care utilization among adults aged 50 and older. Can J Aging. 2016;35(1):55–69. https://doi.org/10.1017/S0714980815000562.
Devaux M. Income-related inequalities and inequities in health care services utilisation in 18 selected OECD countries. Eur J Health Econ. 2015;16(1):21–33. https://doi.org/10.1007/s10198-013-0546-4.
Dorjdagva J, Batbaatar E, Dorjsuren B, Kauhanen J. Income-related inequalities in health care utilization in Mongolia, 2007/2008-2012. Int J Equity Health. 2015;14(1):57. https://doi.org/10.1186/s12939-015-0185-8.
Macinko J, Lima-Costa MF. Horizontal equity in health care utilization in Brazil, 1998-2008. Int J Equity Health. 2012;11(1):33. https://doi.org/10.1186/1475-9276-11-33.
Vikum E, Krokstad S, Westin S. Socioeconomic inequalities in health care utilisation in Norway: the population-based HUNT3 survey. Int J Equity Health. 2012;11(1):48. https://doi.org/10.1186/1475-9276-11-48.
WHO. The World Health Report 2000 (Chinese version). Geneva: People's Medical Publishing House; 2000.
Tang S, Meng Q, Chen L, Bekedam H, Evans T, Whitehead M. Tackling the challenges to health equity in China. Lancet. 2008;372(9648):1493–501. https://doi.org/10.1016/S0140-6736(08)61364-1.
Chen R, Zhao Y, Du J, Wu T, Huang Y, Guo A. Health Workforce Equity in Urban Community Health Service of China. Plos One. 2014;9:e11598812.
National health data; Available from: https://data.stats.gov.cn/easyquery.htm?cn=C01. Accessed 22 Mar 2021.
Yip WC, Hsiao WC, Chen W, Hu S, Ma J, Maynard A. Early appraisal of China's huge and complex health-care reforms. Lancet. 2012;379(9818):833–42. https://doi.org/10.1016/S0140-6736(11)61880-1.
Statistical Bulletin of the People's Republic of China on National Economic and Social Development in 2015; Available from: http://www.stats.gov.cn/tjsj/zxfb/201602/t20160229_1323991.html. Accessed 29 Feb 2016.
Fu X, Sun N, Xu F, Li J, Tang Q, He J, et al. Influencing factors of inequity in health services utilization among the elderly in China. Int J Equity Health. 2018;17(1):144. https://doi.org/10.1186/s12939-018-0861-6.
Song S, Yuan B, Zhang L, Cheng G, Zhu W, Hou Z, et al. Increased inequalities in health resource and access to health care in rural China. Int J Environ Res Public Health. 2019;16(1):49.
Duy KV, Van Minh H, Bao GK, Weinehall L, Ng N. Horizontal inequity in public health care service utilization for non-communicable diseases in urban Vietnam. Glob Health Action. 2014;7:24919.
Terraneo M. Inequities in health care utilization by people aged 50+: evidence from 12 European countries. Soc Sci Med. 2015;126:154–63. https://doi.org/10.1016/j.socscimed.2014.12.028.
Sun X, Zhang H, Hu X, Gu S, Zhen X, Gu Y, et al. Measurement and analysis of equity in health: a case study conducted in Zhejiang Province, China. Int J Equity Health. 2018;17(1):36. https://doi.org/10.1186/s12939-018-0746-8.
Barbosa EC, Cookson R. Multiple inequity in health care: an example from Brazil. Soc Sci Med. 2019;228:1–8. https://doi.org/10.1016/j.socscimed.2019.02.034.
Li C, Dou L, Wang H, Jing S, Yin A. Horizontal inequity in health care utilization among the middle-aged and elderly in China. Int J Environ Res Public Health. 2017;14(8):842.
Fu X, Wang L, Sun C, Wang D, He J, Tang Q, et al. Inequity in inpatient services utilization: a longitudinal comparative analysis of middle-aged and elderly patients with the chronic non-communicable diseases in China. Int J Equity Health. 2020;19(1):6. https://doi.org/10.1186/s12939-019-1117-9.
Center For Health Statistics and Information of NHFPC. An analysis report of 2013 National Health Services Survey in China. Beijing: China Union Medical University Press; 2015.
Chen W, Gao R, Liu L, Zhu M, Wang W, Wang Y, et al. China cardiovascular diseases report 2015: a summary. J Geriatr Cardiol. 2017;14(1):1–10. https://doi.org/10.11909/j.issn.1671-5411.2017.01.012.
A compendium of Health statistics of Guangdong Province in 2019; Available from: http://wsjkw.gd.gov.cn/zd_ylfwxxgk/content/post_3002828.html. Accessed on 27 May 2020.
Bao XY, Xie YX, Zhang XX, Peng X, Huang JX, Du QF, et al. The association between multimorbidity and health-related quality of life: a cross-sectional survey among community middle-aged and elderly residents in southern China. Health Qual Life Outcomes. 2019;17(1):107. https://doi.org/10.1186/s12955-019-1175-0.
The CPC Central Committee and the State Council issued the Outline of the Development Plan for the Guangdong-Hong Kong-Macao Greater Bay Area; Available from: http://www.gov.cn/zhengce/2019-02/18/content_5366593.htm#1. Accessed 18 Feb 2019.
Pampel FC, Krueger PM, Denney JT. Socioeconomic disparities in health behaviors. Annu Rev Sociol. 2010;36(1):349–70. https://doi.org/10.1146/annurev.soc.012809.102529.
Wagstaff A, van Doorslaer E, Paci P. On the measurement of horizontal inequity in the delivery of health care. J Health Econ. 1991;10(2):169-205, 247-9, 251-6–205. https://doi.org/10.1016/0167-6296(91)90003-6.
Lai S, Shen C, Yang X, Zhang X, Xu Y, Li Q, et al. Socioeconomic inequalities in the prevalence of chronic diseases and preventive care among adults aged 45 and older in Shaanxi Province, China. BMC Public Health. 2019;19(1):1460.
Wagstaf A, van Doorslaer E, Watanabe N. On decomposing the causes of health sector inequalities with an application to malnutrition inequalities in Vietnam. J Econ. 2003;112(1):207–23. https://doi.org/10.1016/S0304-4076(02)00161-6.
Shin H, Kim J. Differences in income-related inequality and horizontal inequity in ambulatory care use between rural and non-rural areas: using the 1998–2001 U.S. National Health Interview Survey data. Int J Equity Health. 2010;9:17.
van Doorslaer E, Wagstaff A, van der Burg H, Christiansen T, De Graeve D, Duchesne I, et al. Equity in the delivery of health care in Europe and the US. J Health Econ. 2000;19(5):553–83. https://doi.org/10.1016/S0167-6296(00)00050-3.
Oaxaca R. Male-female wage differentials in urban labor markets. Int Econ Rev. 1973;14(3):693–709. https://doi.org/10.2307/2525981.
Xu Y, Zhang T, Wang D. Changes in inequality in utilization of preventive care services: evidence on China's 2009 and 2015 health system reform. Int J Equity Health. 2019;18(1):172. https://doi.org/10.1186/s12939-019-1078-z.
Zhao Y, Mahal AS, Haregu TN, Katar A, Oldenburg B, Zhang L. Trends and inequalities in the health care and hypertension outcomes in China, 2011 to 2015. Int J Environ Res Public Health. 2019;16(22):4578.
Firmo JO, Barreto SM, Lima-Costa MF. The Bambui health and aging study (BHAS): factors associated with the treatment of hypertension in older adults in the community. Cad Saude Publica. 2003;19(3):817–27. https://doi.org/10.1590/S0102-311X2003000300014.
Xiao N, Long Q, Tang X, Tang S. A community-based approach to non-communicable chronic disease management within a context of advancing universal health coverage in China: progress and challenges. BMC Public Health. 2014;14(Suppl 2):S2.
Zhang D, Pan X, Li S, Liang D, Hou Z, Li Y, et al. Impact of the National Essential Public Health Services Policy on hypertension control in China. Am J Hypertens. 2017;31(1):115–23. https://doi.org/10.1093/ajh/hpx139.
Notice on Doing a Good Job of the National Basic Public Health Service Project in 2019; Available from: http://www.nhc.gov.cn/jws/s7881/201909/83012210b4564f26a163408599072379.shtml. Accessed 4 Sep 2019.
Notice on Doing a Good Job of the National Basic Public Health Service Project in 2015; Available from: http://www.nhc.gov.cn/jws/s3577/201506/61340494c00e4ae4bca0ad8411a724a9.shtml. Accessed on 11 June 2015.
China has launched and deployed nine national basic public health services; Available from: http://www.gov.cn/jrzg/2009-07/10/content_1362010.htm. Accessed on 10 July 2009.
The Three Departments Issued a Notice on Doing a Good Job in the National Basic Public Health Service Project in 2017; Available from: http://www.gov.cn/xinwen/2017-09/10/content_5223957.htm. Accessed 10 Sept 2017.
Xie X, Wu Q, Xu L, Liu C, Li Y, Kang Z, et al. Identifying determinants of socioeconomic inequality in health service utilization among patients with chronic non-communicable diseases in China. PLoS One. 2014;9(6):e100231. https://doi.org/10.1371/journal.pone.0100231.
Zhu D, Guo N, Wang J, Nicholas S, Chen L. Socioeconomic inequalities of outpatient and inpatient service utilization in China: personal and regional perspectives. Int J Equity Health. 2017;16(1):210. https://doi.org/10.1186/s12939-017-0706-8.
Interpretation of guiding opinions and policies on improving the mechanism of medication guarantee for hypertension and diabetes in urban and rural residents; Available from: http://www.nhsa.gov.cn/art/2019/10/10/art_38_1844.html. Accessed on 10 Oct 2019.
Barraza-Llorens M, Panopoulou G, Diaz BY. Income-related inequalities and inequities in health and health care utilization in Mexico, 2000-2006. Rev Panam Salud Publica. 2013;33(2):122–9. https://doi.org/10.1590/S1020-49892013000200007.
Huang C, Liu CJ, Pan XF, Liu X, Li NX. Correlates of unequal access to preventive care in China: a multilevel analysis of national data from the 2011 China health and nutrition survey. BMC Health Serv Res. 2016;16(1):177. https://doi.org/10.1186/s12913-016-1426-2.
Fan L, Liu J, Habibov NN. A multilevel Logit estimation on the determinants of utilization of preventive health care and healthy lifestyle practice in China. World Med Health Policy. 2015;7(4):309–28. https://doi.org/10.1002/wmh3.160.
Yang W. China's new cooperative medical scheme and equity in access to health care: evidence from a longitudinal household survey. Int J Equity Health. 2013;12(1):20. https://doi.org/10.1186/1475-9276-12-20.
Huang M, Zhang H, Gu Y, Wei J. Outpatient health-seeking behavior of residents in Zhejiang and Qinghai Province, China. BMC Public Health. 2019;19(1):967. https://doi.org/10.1186/s12889-019-7305-0.
Li H, Wu Z, Hui X, Hu Y. Impact of local health insurance schemes on primary care management and control of hypertension: a cross-sectional study in Shenzhen, China. BMJ Open. 2019;9(10):e31098.
Chen Z. Launch of the health-care reform plan in China. Lancet. 2009;373(9672):1322–4. https://doi.org/10.1016/S0140-6736(09)60753-4.
Statistical Bulletin of the People's Republic of China on National Economic and Social Development in 2019; Available from: http://www.stats.gov.cn/tjsj/zxfb/202002/t20200228_1728913.html. Accessed 28 Feb 2020.
Liu GG, Vortherms SA, Hong X. China's health reform update. Annu Rev Public Health. 2017;38(1):431–48. https://doi.org/10.1146/annurev-publhealth-031816-044247.
Yip W, Fu H, Chen AT, Zhai T, Jian W, Xu R, et al. 10 years of health-care reform in China: progress and gaps in universal health coverage. Lancet. 2019;394(10204):1192–204. https://doi.org/10.1016/S0140-6736(19)32136-1.
The Provincial Medical Insurance Bureau Comprehensively Promotes the "One-stop" Settlement of Medical Assistance and Direct Settlement of Medical Treatment in Other Places has Reached a New Level; Available from: http://hsa.gd.gov.cn/gkmlpt/content/2/2590/post_2590453.html#464. Accessed 27 Aug 2019.
Notice of the People's Government of Guangdong Province on the Issuance of Certain Policies and Measures for Further Promoting Employment in Guangdong Province; Available from: http://www.gd.gov.cn/zwgk/wjk/qbwj/yf/content/post_164461.html. Accessed 03 Dec 2018.
Li D, Zeng X, Huang Y, Lei H, Li G, Zhang N, et al. Increased risk of hypertension in young adults in Southwest China: impact of the 2017 ACC/AHA high blood pressure guideline. Curr Hypertens Rep. 2019;21(3):21. https://doi.org/10.1007/s11906-019-0926-y.
van Doorslaer E, Koolman X, Jones AM. Explaining income-related inequalities in doctor utilisation in Europe. Health Econ. 2004;13(7):629–47. https://doi.org/10.1002/hec.919.
Zhou Z, Zhu L, Zhou Z, Li Z, Gao J, Chen G. The effects of China's urban basic medical insurance schemes on the equity of health service utilisation: evidence from Shaanxi Province. Int J Equity Health. 2014;13(1):23. https://doi.org/10.1186/1475-9276-13-23.
China NBOS. China statistical yearbook 2020 (Chinese-English edition). Beijing: China Statistics Press; 2020.
Chinese Gini coefficient; Available from: https://www.ceicdata.com/zh-hans/china/resident-income-distribution/gini-coefficient. Accessed on 1 Feb 2020.
Acknowledgements
Not applicable.
Funding
This study was supported by research grants from the National Natural Science Foundation of China (81872584 and 81472941) and the Natural Science Foundation of Guangdong Province (2016A030313138). The funder had role in data collection, data analysis and preparation of the manuscript.
Author information
Authors and Affiliations
Contributions
YL, PW and JM conceived and designed the study. YL, MC, XP JH and NL contributed to collection of data, and analyzed the data and interpretation of the results. YL wrote the draft manuscript. NL, JM and PW critically commented the paper. NL, JM, PW and YL finalized the manuscript with inputs from all authors. All of the authors approved the final version submitted for publication.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
The study was approved by the ethics committee of Health Research Specialty Committee of Guangdong Sociological Society. Written informed consent was obtained from each study participant before investigation. When the participant is a child (under 16 years of age), written informed consent was obtained from the parent or guardian.
Consent for publication
Not Applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1:
The questionnaire used in this study. Table 1. Questionnaire on Family General Situation (excerpt). Table 2. Questionnaire on Personal Situation of Family Members (excerpt).
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Liu, Y., Liu, N., Cheng, M. et al. The changes in socioeconomic inequalities and inequities in health services utilization among patients with hypertension in Pearl River Delta of China, 2015 and 2019. BMC Public Health 21, 903 (2021). https://doi.org/10.1186/s12889-021-10879-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12889-021-10879-6