
Abstract
Background
To analyze the trend of lower extremity major amputations (MA) among patients with type 2 diabetes mellitus (T2DM) in the Regions of Spain from year 2001 until 2015.
Methods
Descriptive study of 40,392 MA. Data were obtained from the national hospital discharge database in patients with T2DM. The incidence rate was calculated in each Region, in addition to the incidence ratios (IR) between annual incidence and incidence of the year 2001. The length of hospital stay and mortality risks were analyzed using regression models adjusted for sex, age and smoking.
Results
The major amputations incidence rate per 100,000 person-years was 0.48 in Spain; Canary Islands showed the highest incidence (0.81). The trend was a slight decrease or stability of the incidence in all Regions except in the Canary Islands (IR2015 = 2.0 [CI95% = 1.5, 2.6]) and in Madrid (IR2015 = 0.1 [CI95% = 0.1, 0.2]). Mortality after major amputations was 10% in Spain; Cantabria suffered the highest risk of death [1.7 (CI95% = 1.4; 2.1), p < 0.001] and La Rioja the lowest risk (0.5 [CI95% = 0.2; 0.9]; p = 0.026). The longest hospital stay was registered in the Canary Islands [(CI95% = 11.4;13.3], p < 0.001)], and the shortest in the Valencian Community [(CI95% = − 7.3; − 5.8), p < 0.001)].
Conclusion
MA in T2DM followed a growing trend in the Canary Islands, which diverged from the downward trend in Spain. The variability of mortality and hospital stay, suggest to review the clinical management in some Regions. Sudden incidence decrease in Madrid suggests checking the record procedures of hospital discharges.
Similar content being viewed by others


Background
More than a half of the non-traumatic amputations of limbs occur in patients with type 2 diabetes (T2DM), although during the twenty-first century the incidence of these amputations has been decreasing in Europe, USA, and Asia [1,2,3]. Despite this decrease, major lower extremity amputations (MA) still remain a cause of high mortality and loss of quality of life with a significant increase in health costs associated to diabetes [2]. In recent decades there has been an improvement in the early detection and control of T2DM complications and, since the Saint Vincent Declaration in 1990, diabetic foot care has been intensified to reduce the incidence of major amputations. However, the increase in life expectancy of patients diagnosed with T2DM has also increased the associated morbidity [4]. Advanced age, African ethnicity and male sex are associated with an increased risk of amputations in patients with T2DM, while other factors such as female gender, kidney failure and congestive heart failure increase the risk of death during hospitalization [5]. In addition, undergoing a MA is a significant risk factor for long term mortality among T2DM patients [6].
The overall incidence of amputations due to diabetes increased by 4.29% in Spain between 2001 and 2004, followed by a downward trend until 2012, around 2% [7]. In-hospital mortality due to amputations remained stable between 2001 and 2012, around 10%, resulting in an economic cost of 33% of the total cost spent in hospital treatment of T2DM complications [8]. Although there are several published works in relation to non-traumatic amputations in Spain [5,6,7,8], they account for the major and minor procedures globally in the analysis, or do not differentiate the type of diabetes. To our knowledge, there are no publications that have compared MA incidence in patients with T2DM in the seventeen Autonomous Communities (AACC) or Regions of Spain, nor analyzed possible regional heterogeneity in MA mortality or days of hospital stay.
We conducted the present study in order to analyze the trend of major amputations incidence in patients with T2DM during the period 2001–2015 in all the AACC of Spain, as well as mortality and hospital stay in each of them.
Methods
Design and subjects
This is a retrospective observational study of the Spanish National Hospital Discharges of 40,392 hospital admissions for major amputations (defined as through, or proximal to, the tarsometatarsal joint) in patients with T2DM in the seventeen AACC of Spain, during the period 2001–2015. Data were collected from the Minimum Basic Data Set (CMBD, in Spanish) obtained from public and private hospitals. CMBD is a record of clinical-administrative data integrated into the health information system of the national health system, and contains the information at discharge of all episodes of hospitalization in the country. The database for this study was produced by the Ministry of Health with aggregated fully anonymized data, so neither individual written consent by patients nor ethical approval was required because in Spain the use of the CMBD does not require prior approval of an ethics committee (under the Spanish Organic Law 3/2018 on the protection of personal data and digital rights, which transcribe the European Union General Data Protection Regulation 2016/679).
The information was obtained from the principal and secondary diagnoses for each episode of admission in addition to age, sex and hospital code, current consumption of tobacco, admission date and causes for hospital discharge (including death). The database did not include other socio-economic or lifestyle data. The length in days of hospital stay in each AACC was also analyzed, and its difference was calculated with respect to the average stay in Spain.
Inclusion and exclusion criteria
Only cases of MA in patients with T2DM were selected (ICD9-CM codes ranging from 250.00 to 250.92, except codes for type 1 diabetes). The records of patients under 15 years of age were excluded because there were not MA patients with T2DM under this age. We also excluded those cases in which sex or geographical area had not been recorded, as well as episodes recorded in the North-African cities of Ceuta and Melilla.
Statistical analysis
The scale variables were summarized according to their mean and standard deviation, or by percentiles. The categorical variables were presented by the observed frequency (%) and the 95% Confidence Interval (CI95%).
The MA incidence rates during the period 2001–2015 were computed for the population in each Region and in the whole of Spain; for each geographical area the numerator was the sum of cases in this period in patients of 15 or more years of age, and the denominator was the sum of all the resident annual populations with that same age, obtained from the National Institute of Statistics (Spain). These regional MA rates were age-standardized by the direct method, taking as a reference the population of Spain.
In addition, in each Region the ratio between the annual incidence of MA respect to the incidence of 2001 was calculated, and the Open-Epi package was used to obtain the CI95% of these incidence ratios (IR). The trend of the IR was analyzed with a sequence chart to plot time series.
Linear regression models were used to adjust for age, sex and smoking the differences in the length of hospital stay. Regression coefficients and their confidence intervals are offered with a CI95%. To estimate the risk of mortality after MA, logistic regression models were adjusted for sex, age and active smoking; Odds ratios (OR) and their CI95% were obtained in this way.
Statistical analyses were performed using the statistical package SPSS 21.0, in Spanish.
Results
The study included 40,392 non-traumatic MA in patients with T2DM in the seventeen AACC of Spain (Fig. 1) during the period 2001–2015.

The seventeen Autonomous Communities or Regions of Spain (free distribution under Creative Commons license. https://commons.wikimedia.org/wiki/File:Ccaa-spain.png)
Table 1 shows the number of cases in each Region, as well as their age, proportion of women, active smokers, days of hospital stay and mortality derived from MA procedures. The average age of patients who underwent MA was above 72.5 years in all the AACC, except in the Balearic and Canary Islands. Among them, the prevalence of active smokers varied between 12% in Navarra and 5% in the Basque Country or La Rioja. The Regions with the longest hospital stay for MA were Aragon, Asturias and The Canaries; by contrast, the Balearic Islands, the Valencian Community and Murcia were the Regions with the shortest stay. Regarding mortality after MA, Cantabria showed the highest rate (17%) and La Rioja the lowest one (5%).
Table 2 presents the ratios between the annual incidence of MA and the incidence for the initial year (2001), showing a strong increase in the Canary Islands ratio (IR = 2.0 at the end of the 15 years period), compared to the moderate decrease in the whole country (IR = 0.8). The greatest decrease occurred in the Region of Madrid (IR = 0.1 at the end of the period [CI95% = 0.08; 0.17]), but it should be noted that the incidence of this Community experienced a very sharp fall (greater than 80%) between 2009 and 2010. This table also shows the MA incidence rates in the AACC for the entire period; the Canarian rate (0.81 / 100,000 people-year) was almost double that of Spain incidence rate (0.48 / 100,000 people- year) and triple that of Madrid (0.24 / 100,000 people-year).
Table 3 shows the multivariate adjustment of the length of hospital stay between each community and the total of Spain, as well as the risk of death in each Region compared to the overall mortality in Spain. Both models were adjusted for sex, age and smoking; they corroborated that the longest hospital stay by MA occurred in the Canary Islands, being 12 days longer than the average of the country and 19 days longer than the Region with the shortest stay (Valencian Community). However, the risk of in-hospital death after MA was higher in Cantabria, which exceeded the overall risk in Spain by 70%, while in La Rioja there was a 50% reduction in the risk of death with respect to the country.
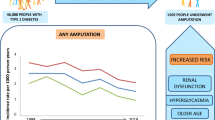
Figure 2 represents the trend of the annual incidence ratios compared to 2001 for two AACC of similar population size (The Canary Islands and the Basque Country) and for the global of Spain.

Trend of the incidence ratio of major amputation in patients with T2DM in Spain, Canary Islands and the Basque Country for each year of the period in relation to 2001
Discussion
The study of 40,392 hospital admissions for nontraumatic major amputations occurred in patients with T2DM in Spain during the period 2001–2015 showed a high variability among AACC, both in incidence and length of hospital stay and mortality. The trend of the incidence has been moderately decreasing in the whole of the country, but more accentuated in the Community of Madrid; however, the exception was the Canarian Community, that has worsened until doubling its incidence in respect to the initial years of the data reviewing period.
Although T2DM mortality has declined in these islands significantly in the last five years, [9] the severity of this disease in the Canary Islands is known; its current population suffers the highest incidence and prevalence [10, 11] in Spain, as well as high mortality rates due to this disease [12]. It is also known the high incidence of MA in Canarian population [13] but the trends with respect to the other Regions had not been studied. We have corroborated that, far from approaching the improvement experienced in the whole of the country, the trend of the MA in the Canary Islands diverged from the other AACC during this century. At the opposite extreme is the Community of Madrid, which is known to have the lowest prevalence and mortality by T2DM in Spain [10] and for which we have now found the best trend in the country for MA incidence; nevertheless, we want to draw attention to the sudden decline of MA in this Region as of 2009, which could be attributed to an error in the record procedures of hospital discharges.
Looking at the population size, the most similar Region to the Canaries is the Basque Country, whose MA prevalence in T2DM had been previously studied [14]. In both AACC the population aged over 15 years (1,804,000 inhabitants) represented 4.7% of the Spanish population in 2015 [15], but for the studied period their cases of MA were 5.8% in the Canary Islands (that is, 23% more than expected) and 4.3% in the Basque Country (that is, 9% less than expected); so, the divergent trend produced a ratio of 4.5 between their incidence rates for 2015/2001. In addition, according to previous publications [2, 4, 7] the general profile of MA patients, in order to age and gender, corresponded to a 74-year-old male; but in the Canary Islands the average age of the patients had underwent a MA was 1.5 years younger than in Spain. This increases the burden of T2DM in Canarian population in terms of lost years of potential life free of disability.
In European and North-American countries there has been a decrease in the incidence of nontraumatic amputations in the last decades, [16] especially at the expense of MA in patients with T2DM [17] and particularly more evident for major amputations above the knee [18]; this has been attributed to the healthcare offered to the patient with T2DM, specially the diabetic foot care programmes [4]. This decreasing trend was also reported in Spain [7, 19]. However, most studies do not analyze regional differences, as our study does. Our analysis questions the homogeneity of the Spanish health system and suggests the need for further research on the causes of the detected variability. Some aspects like the identification of access barriers, and the provision of early revascularization services must be taken into account to improve the diabetic foot care programmes [20].
The great variability that our study detected in the length of hospital stay due to MA reveals an important heterogeneity of clinical management within the National Spanish Health System. The Canarian and Valencian Communities presented the extreme data points, with 19 days of difference between them for an average hospital stay. We have not used in this article the costs provided by the CMBD because they are estimates for the entire health system and its disaggregation by AACC would not represent the real costs. Undoubtedly, further duration of the hospital stay increases the costs of the procedures and, in addition, negatively affects the beds availability and increases the risk of nosocomial infections too. According to this, we believe that length of hospital stay management should be reviewed, especially in the Regions with the longest hospital stay, pointing out after Canary Islands the cases of Aragon and, at some distance, Cantabria.
Looking at mortality during hospitalization for MA, we have found another important difference among Regions, where the highest mortality risk (Cantabria) tripled the lowest risk (La Rioja and Basque Country). These results were not modified when the Community of residence was used instead of the Community of hospitalization, nor when they were adjusted for length of stay, age, sex or smoking. It could be speculated that MA criteria in T2DM could be more conservative in some AACC than in others; in fact, the seven AACC with the highest risk of death had a lower incidence of MA than the average of the country. Once again, we believe that Regions with the highest mortality risks should review the clinical management of MA.
The prevalence of smoking in the studied population exceeded 10% in some AACC. Certainly, smoking was higher in the general adult population of Spain, [21] but it should be noted that this 10% refers to active smoking in patients with T2DM admitted for severe macrovascular complications. We cannot demonstrate that these patients had been informed that tobacco increases the risk of amputations and, in addition, suffering an amputation does not implies smoking cessation [22]. New approaches are needed to ensure the effectiveness of tobacco control policies.
The main limitation of our study is that data came from clinical-administrative hospital records and there is a possibility of under-registration of T2DM as well as an underestimation of incidence of non-traumatic amputations in those cases. In addition, it remains difficult to establish a causal relationship that explains the differences detected regarding mortality in the Regions due to the lack of relevant information such as the number of years having T2DM, concomitant treatments or disease control status. Systematic reviews of studies on the incidence of amputations indicate that the variability detected could be explained by aspects related to the design, statistical methods used or the heterogeneity in the definition of the variables [23]. Despite this, the CMBD has shown a confident quality of data and a valid exploitation for health research [24]. In contrast, the main strength of our study is the large sample size, which includes patients admitted to hospitals for MA in whole of Spain.
Conclusions
We conclude that the trend of MA incidence was moderately favorable for the global of Spain during the first fifteen years of this century with the only exception of the Canary Islands, which increased its incidence. The great variability in mortality and length of hospital stay due to MA questions the homogeneity of the healthcare provided by the National Spanish Health System. The Regions with worse outcomes should make efforts to identify the reasons for the observed differences and improve the healthcare quality. The abrupt decline of MA in the Community of Madrid after 2009, advises to revise the record procedures of its hospital discharges. More national and regional studies monitoring nontraumatic amputations in patients with T2DM are needed.
Availability of data and materials
All raw data on which our study is based can be accessed from the Ministry of Health (icmbd@msssi.es).
Abbreviations
- AACC:
-
Autonomous Communities
- IR:
-
Incidence ratio
- MA:
-
Lower extremity major amputations
- T2DM:
-
Type 2 diabetes mellitus
References
Moxey PW, Gogalniceanu P, Hinchliffe RJ, et al. Lower extremity amputations: a review of global variability in incidence. Diabet Med. 2011;28:1144–53.
Claessen H, Narres M, Haastert B, Arend W, Hoffman H, Morbach S, et al. Lower-extremity amputations in people with and without diabetes in Germany, 2008-2012- an analysis of more than 30 million inhabitants. Clin Epidemiol. 2018;10:475–88.
Lin CW, Armstrong DG, Lin CH, Liu PH, Hung SY, Lee SR, Huang CH, Huang YY. Nationwide trends in the epidemiology of diabetic foot complications and lower-extremity amputation over an 8-year period. BMJ Open Diabetes Res Care. 2019;7:e000795.
Yashkin AP, Picone G, Sloan F. Causes of the Change in the Rates of Mortality and Severe Complications of Diabetes Mellitus: 1992–2012. Med Care. 2015;53:268–75.
Lopez-de-Andres A, Hernandez-Barrera V, Lopez R, Martin-Junco P, Jimenez-Trujillo I, Alvarez-Mecca A, et al. Predictors of in-hospital mortality following major lower extremity amputations in type 2 diabetic patients using artificial neural networks. BMC Med Res Methodol. 2016;16:160.
López-de-Andrés A, Jiménez-García R, Esteban-Vasallo MD, Hernández-Barrera V, Aragon-Sánchez J, Jiménez-Trujillo I, de Miguel-Diez J, Palomar-Gallego MA, Romero-Maroto M, Perez-Farinos N. Time Trends in the Incidence of Long-Term Mortality in T2DM Patients Who Have Undergone a Lower Extremity Amputation. Results of a Descriptive and Retrospective Cohort Study. J Clin Med. 2019; 8. pii: E1597.
López-de Andrés A, Jiménez-García R, Aragón-Sánchez J. National trends in incidence and outcomes in lower extremity amputations in people with and without diabetes in Spain, 2001–2012. Diab Res Clin Pract. 2015;108:499–507.
Crespo C, Brosa M, Soria-Juanc A, Lopez-Alba A, Lopez-Martinez N, Soria B. Direct costs of diabetes mellitus and its complications in Spain (SECCAID study: Spain estimated cost Ciberdem-Cabimer in diabetes). Av Diabetol. 2013;29:182–9.
Carlos III Health Institute (Spanish Government). National Center of Epidemiology, http://raziel.cne.isciii.es/maps/fMap.php ; 2019 [].
de Leon AC, Coello SD, González DA, Diaz BB, Castillo JC, Hernández AG, et al. Impaired fasting glucose, ancestry and waist-to-height ratio: main predictors of diabetes in the Canary Islands. Diabet Med. 2012;29:399–403.
Grau M, Elosua R, Cabrera de León A, Guembe MJ, Baena-Díez JM, Vega Alonso T, et al. Cardiovascular Risk Factors in Spain in the First Decade of the 21st Century, a Pooled Analysis with Individual Data from 11 Population-Based Studies: the DARIOS Study. Rev Esp Cardiol. 2011;64:295–304.
Marcelino I, Elosua R, Perez Mdel C, Fernandez-Berges D, Guembe MJ, Alonso TV, et al. On the problem of diabetes mortality in the Canary Islands, Spain. The DARIOS study. Diabetes Res Clin Pract. 2016;111:74–82.
Aragón-Sánchez J, García-Rojas A, Lázaro-Martínez JL, Quintana-Marrero Y, Maynar-Moliner M, Rabellino M, et al. Epidemiology of diabetes-related lower extremity amputations in gran Canaria, Canary Islands (Spain). Diabetes Res Clin Pract. 2009;86:e6–8.
Alonso-Morán E, Orueta JF, Fraile Esteban JI, Arteagoitia Axpe JM, Marqués González ML, Toro Polanco N, Ezkurra Loiola P, Gaztambide S, Nuño-Solinis R. The prevalence of diabetes-related complications and multimorbidity in the population with type 2 diabetes mellitus in the Basque Country. BMC Public Health. 2014;14:1059.
Spanish National Institute of Statistics, http://www.ine.es/jaxiT3/Tabla.htm?t=9681&L=1 [accessed December 2, 2019].
Lombardo FL, Maggini M, De Bellis A. Lower extremity amputations in persons with and without diabetes in Italy: 2001-2010. PLoS One. 2014;9:e86405.
Kennon B, Leese G, Cochrane L, et al. Reduced incidence of lower extremity amputations in people with diabetes in Scotland. Diabetes Care. 2012;35:2588–90.
Claessen H, Avalosse H, Guillaume J, Narres M, Kvitkina T, Arend W, et al. Decreasing rates of major lower-extremity amputation in people with diabetes but not in those without: a nationwide study in Belgium. Diabetologia. 2018;61:1966–77.
Alcalá Martínez-Gómez D, Moreno-Carrillo MA, Campillo-Soto A. Reduction in diabetic amputations over 15 years in a defined Spain population. Benefits of a critical pathway approach and multidisciplinary team work. Rev Esp Quimioter. 2014;27:170–9.
Schaper NC. Apelqvist J, Bakker K (2012). Reducing lower leg amputations in diabetes: a challenge for patients, healthcare providers and the healthcare system. Diabetologia. 2012;55:1869–72.
Spanish National Health Survey of 2017, https://www.mscbs.gob.es/en/estadEstudios/estadisticas/encuestaNacional/encuesta2017.htm. ; 2019 [accessed 2 December 2019].
Anderson JJ, Boone J, Hansen M, Spencer L, Fowler Z. A comparison of diabetic smokers and non-smokers who undergo lower extremity amputation: a retrospective review of 112 patients. Diabetic Foot Ankle. 2012;3:19178.
Narres M, Kvitkina T, Claessen H. Incidence of lower extremity amputations in the diabetic compared with the non-diabetic population : a systematic review. PLoS One. 2017;12:e0182081.
Ribera A, Marsal J, Ferreira-González I, et al. Predicting in-hospital mortality with coronary bypass surgery using hospital discharge data: comparison with a prospective observational study. Rev Esp Cardiol. 2008;61:843–52.
Acknowledgements
To the Institute for Health Information (Ministry of Health, Consumption and Social Welfare), for the development of the database. To Dr. Geraldine Quintero Platt for her reading and her advice on the translation of our text into English.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Author information
Authors and Affiliations
Contributions
MCRP and ACL contributed to the study conception and design, data acquisition, analysis and interpretation of data, and decided the final version of the manuscript. CC and DS participated on the study conception, updated the bibliographic search and participated in the writing of the introduction and methods chapters. AGP, FJCF, IMR and SDC contributed to the interpretation of results and critical review providing feedback on the entire manuscript. All authors read and approved the final manuscript. MCRP and ACL are the guarantors of this manuscript and they are responsible for the integrity of work as a whole.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The database for this study was produced by the Ministry of Health with aggregated fully anonymized data. The Ministry did not require prior approval of an ethics committee, but a commitment to confidentiality that the authors signed (under the Spanish Organic Law 3/2018 on the protection of personal data and digital rights, which transcribe the European Union General Data Protection Regulation 2016/679).
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

{kind=link}
Cite this article
Rodríguez Pérez, M.d.C., Chines, C., Pedrero García, A.J. et al. Major amputations in type 2 diabetes between 2001 and 2015 in Spain: regional differences. BMC Public Health 20, 54 (2020). https://doi.org/10.1186/s12889-019-8137-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12889-019-8137-7