
Abstract
Background
The dramatic rise in Noncommunicable Diseases (NCD) in the oil-producing countries of the Arabian Peninsula is driven in part by insufficient physical activity, one of the five main contributors to health risk in the region. The aim of this paper is to review the available evidence on physical activity and sedentary behaviour for this region. Based on the findings, we prioritize an agenda for research that could inform policy initiatives with regional relevance.
Methods
We reviewed regional evidence on physical activity and sedentary behaviour to identify the needs for prevention and policy-related research. A literature search of peer-reviewed publications in the English language was conducted in May 2016 using PubMed, Web of Science and Google Scholar. 100 studies were identified and classified using the Behavioural Epidemiology Framework.
Results
Review findings demonstrate that research relevant to NCD prevention is underdeveloped in the region. A majority of the studies were epidemiological in approach with few being large-scale population-based studies using standardised measures. Correlates demonstrated expected associations with health outcomes, low levels of physical activity (particularly among young people), high levels of sedentary behaviour (particularly among men and young people) and expected associations of known correlates (e.g. gender, age, education, time, self-motivation, social support, and access). Very few studies offered recommendations for translating research findings into practice.
Conclusions
Further research on the determinants of physical activity and sedentary behaviour in the Arabian Peninsula using standard assessment tools is urgently needed. Priority research includes examining these behaviours across the four domains (household, work, transport and leisure). Intervention research focusing on the sectors of education, health and sports sectors is recommended. Furthermore, adapting and testing international examples to the local context would help identify culturally relevant policy and programmatic interventions for the region.
Similar content being viewed by others


Background
Noncommunicable disease (NCD) accounts for a large portion of mortality and morbidity in the oil-producing countries of the Arabian Peninsula (Bahrain, Kuwait, Oman, Qatar, Saudi Arabia and United Arab Emirates; UAE) [1, 2]. A large majority of NCD mortality is due to cardiovascular disease. For example, more than a quarter of the adult population has high blood pressure and high blood glucose [3]. More than half of adults in the region are currently overweight or obese [3]. In the context of the links between maternal obesity and gestational diabetes and the health of unborn children globally [4], these regional prevalences combined with a high rate of congenital anomalies [2, 5] have far reaching implications for the health of future generations.
Insufficient physical activity (defined as less than 150 min of moderate physical activity per week) is one of the main contributors to health risk globally [3]. Sedentary behaviour (any waking behaviour characterized by an energy expenditure ≤1.5 METs while in a sitting or reclining posture [6, 7]) is a newer area of research; it has associations with all-cause and cardiovascular disease mortality, diabetes, and obesity when controlling for the influence of moderate-vigorous physical activity [8, 9]. The latest research indicates that a high level of moderate physical activity attenuates, but does not eliminate, the risk of high sitting time [10]. Despite the growing research confirming these associations, there is insufficient research documenting their relevance for the six oil-producing countries of the Arabian Peninsula.
The rapid socio-economic development of the region has contributed to a rise in urbanization, motorisation, trade liberalization and “western” dietary patterns [1, 11] which are widely recognized as key contributors to the rise of NCDs globally [12–14]. Although the radical changes in the food environment and consumption patterns in the region have been documented [1, 11], there is less evidence about the relationship between physical activity and sedentary behaviour and NCDs [15, 16]. There is also limited documentation of the shifts in occupational and transport (car-dependent) patterns in the region and their impact on physical activity [1]. Evidence that would help identify the social and cultural contexts that may limit people’s mobility, especially women, is sparse [15, 17]. The role of the hot arid climate has yet to be adequately specified [17, 18]. Thus, more thorough documentation of physical activity and sedentary behaviour in the region is an important priority, particularly as it relates to NCD prevention.
Research establishing patterns of physical activity and sedentary behaviour is well-documented in most other regions globally [14, 19–21]. The Behavioural Epidemiology Framework was developed as a simple approach to understand these patterns and build the evidence needed to inform public health action on physical activity and sedentary behaviour [22, 23]. It organizes research into the following phases:
-
Phase 1. Identifying relationships of physical activity and sedentary behaviour with health outcomes
-
Phase 2. Measuring physical activity and sedentary behaviour
-
Phase 3. Characterizing prevalence and variations of physical activity and sedentary behaviour in populations
-
Phase 4. Identifying the determinants of physical activity and sedentary behaviour
-
Phase 5. Developing and testing interventions to influence physical activity and sedentary behaviour
-
Phase 6. Using evidence to inform public health guidelines and policy
As a research framework, it helps identify research gaps and systemizes the development of a research agenda to inform and guide public health policy and practice. To be effective, regional evidence is needed to understand the contextual determinants of these behaviours and introduce regionally relevant policies to address them [1, 24]. We review the available evidence on physical activity and sedentary behaviour for the oil-producing countries of the Arabian Peninsula. Based on the findings, we prioritize an agenda for research that could inform policy initiatives in the region.
Methods
Search strategy
A literature search was conducted in May 2016 with PubMed, Web of Science and Google Scholar using the following search terms: active living; exercise; lifestyle; physical activity; walking; screen time; sedentary; sitting or television viewing; and the name of each country in the Region (Bahrain, Kuwait, Oman, Qatar, Saudi Arabia and United Arab Emirates) or Arab. The search was limited to peer-reviewed publications in the English language from any time period through April 2016. All articles were imported in an Endnote file to facilitate deduplication, screening and selection.
Selection process
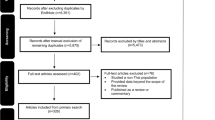
The initial search produced 3,560 articles, after deduplication. All articles were screened independently by two authors (RMM and MJK). Screening was conducted in two steps. In the first step, original English language articles on related disciplines published in peer-reviewed journals through April 2016 were included by judging from the title and source of articles. Publications in other languages, conference proceedings and theses as well as articles in unrelated disciplines were removed. By the end of this step, 347 articles remained.
In the second step, the abstracts and full texts were examined. The primary inclusion criteria were country specific studies which gathered original data, fit into any phase of the Behavioural Epidemiology framework [22, 23], and full-texts were available. Additional secondary inclusion criteria were used for the first three phases to facilitate within and cross-country comparison:
-
Phase 1: Cross-sectional studies used a clearly described measure for physical activity/sedentary behaviour and prospective studies involved a physical activity intervention
-
Phase 3: Studies clearly defined physical activity as meeting the recommendation of 150 min/week for adults or 60 min/day for children/adolescents.
-
Phase 4: For demographic correlates, studies used a clearly described measure for physical activity/sedentary. The secondary inclusion criteria were not used for the studies examining the non-demographic articles to ensure a comprehensive review of available research in the region.
This resulted in a total of 100 articles. The flow diagram for article inclusion following PRISMA guidelines can be seen in Fig. 1 [25]. Since this was a systematic review of published research, rather than a study involving the collection of primary data, ethical clearance was not obtained.

PRISMA 2009 Flow diagram
Data extraction, analysis and synthesis
Once the list of selected studies were identified, RMM extracted and MJK cross-checked the following for each: authors, country in which study was conduct, sample characteristics (number, size, gender, age), and physical activity/sedentary behaviour measurement tools. Key findings of each study were extracted and organized according to the Behavioural Epidemiology Framework. Differences in opinion in data extracted and placement within the framework were discussed to reach consensus. An ecological model that helps to classify potential multiple levels of influence on physical activity and sedentary behaviours-intrapersonal, social cultural, environmental [26, 27], was used to further organize the evidence for Phase 4 (the determinants of physical activity and sedentary behaviour).
Risk of bias assessment
Two authors (RMM and MJK) independently assessed quality of studies included in the review. Studies were assessed for risk of bias using criteria adapted from the Cochrane risk of bias tool [28] and a tool for qualitative research studies [29]. All studies, except qualitative studies, were given a score of ‵1′ if they had an adequate description for each of five criteria: eligibility, randomization of participant selection or assignment for case–control studies, study sample (including number/size, age and gender), measurement of physical activity or sedentary behaviour appropriate for the aim of the study, and co-variates included in the data analysis. Qualitative studies were assessed for a clear description of eligibility, sample selection, study sample (including number/size, age and gender), utilization of standard definition for physical activity and/or sedentary behaviour, and analysis/interpretation.
Results
Fourteen prospective studies and 29 cross-cross-sectional studies utilizing a clearly defined measure of physical activity and sedentary behaviour (such as the Global Physical Activity Questionnaire-GPAQ [30] or International Physical Activity Questionnaire-IPAQ [31]) were included in Phase 1, associations with health outcome (Table 1). Only 3 studies focused solely on measurement and adapted and/or validated a tool (Phase 2) [32–34]. Twenty-six population-based cross-sectional studies reporting on prevalence of these behaviours were included in Phase 3. Studies in Phase 4 included 10 population-based cross-sectional studies utilizing standard measures for physical activity and sedentary behaviour to examine the demographic risk factors influencing these behaviours as well as 25 studies examining a diversity of factors using various study methodologies. Only six studies that reported testing physical activity interventions were included in Phase 5 and none identified in Phase 6. Eleven studies were included in more than one phase (Additional file 1: Table S1).
The review showed a relatively short history of research being conducted on physical activity in this region. All studies were published after the year 2000 with half (52) published in 2013 or later. Examining physical activity and/or sedentary behaviour was explicitly mentioned in the objectives of half (55) of the articles; the remaining focused more broadly on “risk factors” or “lifestyles”. Over half of the studies focused on populations in Saudi Arabia (57) and the UAE (16) with 8 or less articles about populations in each of the other countries of the region (Kuwait: 8; Oman: 7; Qatar: 6 and Bahrain: 5, not shown); the target populations were citizens of each country except for one study where the sample was South Asian immigrants [35].
A majority (86) focused on physical activity with only a few reporting on domain specific physical activity; work (2) [16, 36], transport (4) [16, 35–37], and/or leisure physical activity (5) [16, 37–39]. One-third (34) examined sedentary behaviour in the first 3 phases; all reported on TV viewing and/or computer time except for 8 studies reporting on total sitting time. Most studies focused on adults (62) and/or adolescents (28) with only 7 involving children less than 10 years. Very few studies (6) focused on translating knowledge into practice (Phases 5); these were only in adult populations. A majority (74) were cross-sectional descriptive epidemiology studies. The remaining were short-term (less than 1 year) intervention studies (18), long-term (6 or more years) prospective studies (2) [38, 40] or qualitative studies (6) focusing on physical activity.
Findings of studies organized within the behavioural epidemiology framework
Phase 1 (Identifying relationships with health outcomes)
The review identified 14 prospective studies involving a physical activity intervention and 29 cross-sectional population-based studies utilizing a clear definition of physical activity to examine the association of physical activity with a health outcome (Table 2). Thirty studies sampled adult populations; the remaining studies were among young people, with only three including children under the age of 10 years [41–43]. The most common health outcome studied was obesity (21 studies) using BMI, waist circumference, waist-hip ratio and/or total body fat as the outcome measure. Most reported an inverse association of obesity with physical activity; one reported a positive association with total body fat [44] and two reported no significant association [41, 42]. The remaining studies identified associations with various clinical indicators like high blood pressure [35, 38, 45–49], diabetes [46, 50–52], bone health [37, 40, 53], the metabolic syndrome [16, 54], and Vitamin D deficiency [55, 56].
Twenty-one articles examined associations of sedentary behaviour with a health outcome. Associations of obesity with sedentary behaviour were less conclusive than with physical activity: four studies reported a positive association with different types of sedentary behaviour [42, 57–59], two found no association [60, 61], two reported an inverse association [36, 62] and one reported a positive association with computer time among boys but an inverse association among girls [41]. Another key health outcome studied was the metabolic syndrome; two found a positive association with total sitting time [16, 54] but one reported that this association did not remain after further adjustment for physical activity [16].
Phase 2 (Measuring physical activity and sedentary behavior)
Three studies tested the validity and reliability of Arabic physical activity questionnaires. Two measured physical activity behaviour: the Arabic version of the Questionnaire l’ Activite Physique en Altitude Chez les Enfants for children under the age of 10 years [34] and the tool for the Arab Teens Lifestyle Study (ATLS) [33]. The third tested the psychometric properties of the Arabic Version of the Physical Activity Self-Efficacy Scale for Adolescents [32]. All were identified as valid physical activity instruments for young people in the Arab world.
Across all remaining studies the definitions and measures used for both physical activity and sedentary behaviour varied widely across studies. Several different tools were used to measure physical activity and sedentary behaviour (Additional file 1: Table S1). Self-report was the most common form of reporting (73). Only seven studies used objective measures for physical activity (pedometers and accelerometers); four studies used them as the only measure of behaviour [63–66]. None used objective measures for sedentary behaviour.
Most studies (75) examined self-report derived measures of total physical activity. TV/computer use and/or screen time was the most common proxy measure for sedentary behaviour (32); only six studies reported total sitting time. Some studies used reliable and validated instruments like the IPAQ/IPAQ-short (physical activity-12 studies; sedentary behaviour-5 studies [41, 49, 56, 67, 68]), GPAQ (physical activity-11 studies, sedentary behaviour-4 studies [16, 54, 69, 70]) and the ATLS (physical activity-16 studies, sedentary behaviour-15 studies). Many studies developed their own tools (29 studies examining physical activity and 8 studying sedentary behaviour), eleven provided very limited description of the tools in terms of measuring frequency, intensity and duration of physical activity. Seven studies developed/adapted tools for gathering cognitive and psychosocial data relevant to physical activity such as perceived barriers [71–75], stages of change [73, 75] and self-efficacy [73, 75]. None of the studies in this review used tools concerning the physical environment and physical activity.
Phase 3 (Characterizing Prevalence and variation in populations)
Of the 27 studies reporting on the prevalence of physical activity (Table 3), 11 were on the adult population in four countries: Oman, Qatar, Saudi Arabia and the United Arab Emirates. Four were population-based with three gathering data nationally through household interviews [39, 54, 69] and one by telephone in one city [76]. Two studies were conducted in Saudi Arabia with large differences in the prevalence of physical activity; for a national study the prevalence was very low (Men: 6.1 %, Women: 1.9 %) [39] while in the telephone-based study in Riyadh reported that more than half were met physical activity recommendations (Men: 56.3 %; Women: 65.7 %) [76]. The national study in Oman reported higher prevalence rates than the national household study in Saudi Arabia and Qatar (Women: 44.2 %) with similar rates as in Riyadh (Men: 68.0 %, Women: 59.5 %) [54].
Sixteen country-specific studies from all six countries except Qatar reported on the prevalence of physical activity in the adolescent population. Eight school-based studies utilized the ATLS; among them, the lowest and highest reported prevalence of physical activity (doing at least 60 min moderate physical activity on 7 days a week) were 43.8 to 70.5 % for boys and 4 to 39.2 % for girls in Saudi Arabia and Kuwait respectively [57, 58, 77–82]. Prevalence rates across all studies showed consistently higher rates among boys than girls.
Sedentary behaviour was reported across 18 studies. Only three were national surveys among adult populations in Oman and Qatar; each study presented their data differently. Two studies were secondary analyses of the same survey conducted in Oman; one reported that a quarter of adults (23.7 %) sat 6 or more hours/day [54] and the other reported that nearly half (45.3 %) sat for at least 3 h/day [70]. The third study reported that the mean total sitting time was 183.6 min/day (SD: 168.3 min/day) for women in Qatar [69].
All 15 studies conducted with child and adolescents reported on computer, TV and/or total screen time. Like the adult studies, data were presented differently: mean TV and/or computer time or a prevalence of computer and/or TV of greater than 2 or 3 hours per day. Two studies reported mean computer/TV times with higher rates in girls (Oman: 3.70 ± 2.9 h/day; Saudi Arabia: 5.89 ± 3.3 h/day) than boys (Oman: 2.86 ± 2.3 h/day; Saudi Arabia 5.31 ± 3.1 h/day) [80, 82]. Four studies from Saudi [83–85] and Oman [74] reported on the prevalence of watching 3 or more hours of TV; the highest percentage were girls (60.9 %) in Jeddah, Saudi Arabia [85] and boys (38.0 %) in Abha, Saudi Arabia [84]. These rates were higher than seen in Oman; girls: 25.3 % and boys: 21.1 % [74]. The only study among preschool students reported a mean TV time of 154.8 ± 66.1 min/day [65].
Phase 4 (Identifying the determinants)
Thirty-five studies examined the correlates of physical activity (Table 4). Population-based surveys conducted in Oman and Saudi Arabia consistently reported that gender and education were associated with physical activity with men being more physically active than women [39, 76, 86–90] and people with lower education were more active than their more educated counterpart [70, 76, 90, 91]. All studies reported an association of physical activity with age with younger people being more active than older people [39, 70, 76, 87, 89, 90], except for Oman, where one study reported a direct correlation of age and physical activity among men [70].
In addition to the demographic correlates, the studies explored other factors associated with participation in physical activity, including intrapersonal, social/cultural, physical environment and policy level correlates. The most frequently identified barriers (negative association) of physical activity identified included: time, self-motivation, perceived health, norms limiting women’s mobility or prioritizing her care-taking role, social support, availability of facilities, limited capacity within health institutions and weather. Positive support for participation in physical activity mentioned in more than one study was the knowledge that physical activity is important [92, 93] and desire to enhance one’s appearance [94, 95]. Healthy diet, such as the consumption of fruits and vegetables, were also reported as positive correlates several studies [66, 86–88].
Only one study examined the correlates of sedentary behaviour [70]. It reported that younger women have higher sitting times than older women and more-educated men have higher sitting times than those less educated. Other correlates reported included employment status, smoking and obesity.
Phase 5 (Developing and testing interventions)
Only six studies reported on interventions conducted in Bahrain, Saudi Arabia and UAE; three reported increases in physical activity [96–98] (Table 5). The duration for all studies was less than one year. Four were 6 months or less [96, 97, 99, 100]. Only one study included a post-intervention follow-up [99]. The target group varied with three involving university students [96, 97, 101], two addressing adults with chronic disease [99, 100] and only one targeting the general adult population [98]. Two supplemented awareness raising activities; one involved Instagram motivational messages to encourage the use of an exercise workout video [96] and the other encouraged participants to keep a 1 week log on physical activity [97]. The former was the only one of the six studies that followed a case–control methodology.
Risk of Bias
The two reviewers independently reviewed the methodological quality of the studies included in the review. Quality ratings ranged between 1 and 5; discrepancies in ratings were discussed to reach agreement (Additional file 1: Table S1). For the quantitative studies (n = 94), the mean score was 3.6 with only a quarter (25.5 %) rated 5, the highest score (Additional file 1: Table S1). A vast majority (90 studies or 95.7 %) provided an adequate description of the study sample, 78 studies (83.0 %) provided an adequate description of random sampling, 62 studies (66.0 %) provided a clear description of the eligibility criteria, 61 studies (64.9 %) utilized a valid measure of physical activity and/or sedentary behaviour and 45 studies (47.9 %) adjusted for co-variates. For the six qualitative studies, the mean score was 4.2. All studies provided an adequate description of the eligibility criteria, study sample and the analysis and interpretation and five (83.3 %) provided an adequate description of the sample selection process. However, only two (33.3 %) adhered to the broad definition of physical activity vs the terminology of “exercise” or “sport.” When looking at the studies according to the five phases, the mean score was markedly lower for Phase 5 (2.3) and Phase 2 (3.0) studies which had fewer number of studies compared to those assigned to the other phases (Phase 1: 3.9, Phase 2: 3.7 and Phase 4: 3.6).
Discussion
The findings of this review have identified relevant evidence and some of the limitations in understanding physical activity, sedentary behaviours and public health, an emerging area of knowledge in the Arabian Peninsula. Although 100 publications were identified since 2000, over half of these were published since 2013. This research was spread unevenly across the behavioural epidemiology phases used to structure our review of the evidence [22, 23]. The majority of published studies focussed on assessing health outcomes (Phase 1 n = 43), prevalence (phase 3, n = 26) or identifying the correlates of physical activity and sedentary behaviours (phase 4 n = 35).
Far fewer published studies addressed the measurement of physical activity and sedentary behaviours (phase 2, n = 3) [32–34] or the testing of interventions (phase 5, n = 6). Publications were found from all six countries in the study area, although were mostly focused on adults rather than on children. The sedentary behaviour research identified in this review was much more limited than that related to physical activity and covered only the first three of the five phases of the Behavioural Epidemiology Framework.
Research Implications
The findings points towards the need for more and higher quality research. The following paragraphs describe the research required closely following the Behavioural Epidemiology Framework. Overall, the body of evidence included only a small number of prospective and cross-sectional studies which reported generally consistent associations between physical activity and sedentary behaviours and various health outcomes (Behavioural Epidemiology, Phase 1). Globally, there is extensive evidence on physical activity and life expectancy, cardiovascular disease, diabetes, cancer, mental health and bone health, but it largely originates from countries outside this study region [102, 103]. Examining the associations between patterns of physical activity and sedentary behaviours with various health outcomes in Arab populations should continue to address the knowledge gaps but future studies should employ rigorous methodologies including prospective study design and use objective measures of exposure to increase the quality of evidence available from this region (Behavioural Epidemiology, Phase 2).
Studies found in our review revealed overall low levels of participation in physical activity (particularly among young people), and high levels of sedentary behaviour (particularly among men and young people-Behavioural Epidemiology, Phase 3). Although the prevalence of physical activity among adolescent was generally higher than in adults, a large percentage of both adults and adolescents did not engage in sufficient amounts. Similar findings were observed in a global study of 34 countries [104]; however, the gender differences in the prevalence of physical activity, up to 40 percentage points more in boys than girls, is much larger in this review. Further studies using standardized methods of nationally representative samples are needed to monitor trends as well as to identify population variations and vulnerable groups. This point is particularly important since countries are expected to report on physical activity levels for both adult and adolescent populations as part of the WHO Global Plan of Action [105]. In addition, research on domain-specific physical activity for different populations groups is urgently needed to guide the development of targeted regionally appropriate interventions in light of regional trends like motorization and shifts in occupational patterns.
Studies exploring factors associated with physical activity (Behavioural Epidemiology, Phase 4) reported consistent associations with known correlates. Gender and age were consistently association with physical activity. Men were found to be more active than women and younger people more active than older people which is consistent with other countries [106, 107]. Only one study found that it was the older people more physical active [70]. Four studies in this review reported an inverse association of physical activity with education [70, 76, 90, 91], however, when findings from multiple countries are considered, the inconsistent evidence points to this correlate likely being more context and/or culture-specific [70]. A majority of the studies reporting on the individual-level correlates of physical activity were not guided by a formal conceptual model that could inform subsequent public-health approaches to behavioural change. While this might be construed as a limitation of the evidence that is available, addressing the need for more-basic descriptive data in the region should be a higher priority.
Few studies assessed the physical and policy environments across the four domains of active living (household, occupational, transport and recreation) [108]. Evidence on potential multiple levels of influence on physical activity (intrapersonal, perceived, social cultural, information, natural and policy environments) [108] exists for several Western countries; however, evidence for countries in this region is needed to understand the particular influences that may operate in Arab populations and their social and environmental contexts so as to inform policy and practice.
Only six studies reported the testing of population-based physical activity interventions [96–101] (Behavioural Epidemiology, Phase 5). Three studies reported positive results across different settings [96–98]. Given the importance of increasing physical activity and reducing sedentary behaviours as part of a comprehensive population based approach to the prevention of non-communicable disease [105], greater priority should be given to encouraging an increase in multidisciplinary intervention research to guide national policy and programs.
Measurement of physical activity and sedentary behaviour
Underpinning the development of a strong body of research evidence on physical activity and sedentary behaviours is robust measurement of the exposure variables (Behavioral Epidemiology, Phase 2). This review revealed that many of the studies to date have employed a narrow understanding of physical activity behaviour, with their focus on “exercise” where this is a formal and structured activity. This is in contrast to the broader field of physical activity and public health which has adopted a wider view and includes all types of physical movement (such as walking, recreation, play, cycling to work, etc.) consistent with the WHO Global Recommendations [109].
Of particular concern this review revealed is the wide variability and quality in the measurement instruments used and the presentation of outcomes variables of exposure which severely limits within-and between-country comparisons. Except for those studies reporting use of two well established international measures (IPAQ and GPAQ), there was limited adoption of other valid and reliable tools to assess physical activity and sedentary behaviours, measures of the physical environment, self-reported cognitive, psychosocial measures and domain-specific measures [110]. There was one example of a formal multi-country initiative to develop, validate and utilize a specific physical activity measure for Arab populations [33]. It was the first collaborative project that assessed lifestyle-related variables in a large sample of adolescents from the nine countries of the Arab world. Most studies depended on self-report instruments with only a limited number employing objective instruments to assess either behaviours. Instruments such as accelerometers, pedometers, mobile phones or other electronic devices are increasingly being used across the international literature to address the limitations of self-report measures and are strongly recommended, especially in studies with children [111–113]. Accurate measurement is critical for policy development and necessary for population monitoring of trends over time and differences between populations. It is also essential for research aimed at programme evaluation of individual-based and population-based actions [110].
Policy-relevant research
Although there were no studies that fit into the policy-related phase of the Behavioural Epidemiology Framework, we propose policy-relevant research though a critical review of our findings through the lens of international guidelines. To guide international efforts, recommendations on effective and feasible interventions have been provided on physical activity by the WHO in the Global Action Plan 2013–2020 [105]. Consistent with the 2011 report is the “Seven Investments to Promote Physical Activity” produced by Global Advocacy for Physical Activity (GAPA) [114–116]; intervention strategies are identified across seven key settings (school, transport, urban design, health services, mass media, sports and the community). Sustained public education campaigns using mass media to promote physical activity is a “best investment” recommended by both WHO [105] as well as GAPA [116, 117]. Based on the findings of this review, social marketing intervention efforts in the Arab Peninsular should be gender specific and target youth, especially girls and young women [17]. Campaigns should address the identified common barriers (i.e., limited time, lack of social support) [17, 18, 71–75, 86, 90, 92, 94, 95, 118–123] and cultural norms that place a low value on physical activity [17, 72, 119] and restrict women’s and girls’ participation in physical activity (i.e., cultural norm that limits women from walking/running on their own, or limited space within which to walk within the home compound) [17, 90, 93, 120]. Conducting the necessary formative and pilot research would help identify the promising strategies to then test in larger scale rigorous trials, including those integrating new media and community-based approaches [124].
A quarter of the population in these six countries are under 25 years of age [125, 126]. In addition, the prevalence of physical activity in adolescent populations is low, especially among girls, [57, 58, 65, 77–81]. Thus, interventions in the schools setting and implementation of a “whole of school” programme is a high priority for this region. The Health Promoting Schools (HPS) and Alharaka Baraka programmes [114, 117] provide a basis for developing and testing interventions as well as accelerating school-based action.
Limited capacity within health services to promote physical activity was identified as a key barrier [119, 127, 128]. Two interventions highlighted in this review provide some guidance on possible health services initiatives [98, 101]. Conducting research on how best to integrate promoting physical activity in health services should address gaps already identified. Suggestions have included intensive behaviour change interventions, training of healthcare workers and expanding preventive health services [119, 127–130].
Internationally there is increasing focus on the role of the physical environment [131–133] and consistent with other research, poor access was an identified barrier in this review [18, 71, 92, 119, 129, 134]. Better understanding the distribution, use and opportunities for improving the provision of sports programs and facilities more accessible to the general population, particularly girls and women is a priority for future research in this region. This should include better understanding of the role of informal recreational and sporting opportunities and facilities (such as hiking, biking, group exercise/aerobics, dance and martial arts).
Initiating research to examine the impact of urban planning and transport policy and practice in countries in the Arabian Peninsula is of importance. Research from elsewhere has identified that patterns of land-use, population density as well as the provision of adequate infrastructure to support ‘active transport’ (that is walking cycling and public transport) and optimal green and nature spaces are associated with higher levels of physical activity [131, 133, 135]. Given the rapid urban growth in this region as well as increasing levels of urban sprawl and motorization [136–138], research is needed to inform planning policy that is tailored to the culture and regional specific contexts. For example, encouraging more active transport and recreation needs to be understood within the context of the hot arid climate of the Arabian Peninsula [17, 18, 90, 93, 119, 120, 122, 139]. Research should explore the influence of climate, including seasonal variability (a known factor in other parts of the world) [140–142] and dust storms (a common event throughout the year) [143] on physical activity in the region. Initiating these lines of research may benefit from international collaborations which can build local research skills and capacity and benefit from extensive experience and protocols developed elsewhere [144, 145].
Sedentary behaviour: an emerging field of research
The study of sedentary behaviour, relatively new globally, is only now beginning to receive the attention of researchers in the countries of the Arabian Peninsula. Only a third examined sedentary behaviour and the research was limited to phases 1, 2 and 3 of the Behavioural Epidemiology Framework. The proposed research agenda would be similar to that outlined globally; an ecological model of four domains of sedentary behaviour focusing specifically on domestic screen time, extended sitting time in workplaces and schools, and time spent sitting in cars -- not only to better understand their determinants but also in designing appropriate interventions [26].
Strengths and Limitations
This is the first systematic review of physical activity and sedentary behaviour for this region and complements an earlier review of the prevalence of physical activity [146]. Adherence to the PRISMA statement and the use of three different search engines identified a substantial number of relevant studies. However, there were some limitations. First, our review was restricted to published studies in the English language. It is likely that additional studies such as government reports and scientific papers published in Arabic journals do exist but were not included. Second, the search was limited to only three multidisciplinary literature databases it is possible that additional databases may have identified more studies. Third, the variation in tools and methodologies as well as methodological quality limited within and cross-country comparability. These limitations may bias our view of the gaps in evidence and potential solutions. Nevertheless, the evidence that we have identified in this review is informative. Many evidence gaps remain in understanding how most appropriately to address physical activity and sedentary behaviour in the context of the increasing rates of NCDs in this unique region of the world.
Conclusions
The epidemiological transition, including increasing life expectancy and changing mortality patterns, in the oil-producing countries of the Arabian Peninsula has taken only 50 years; a timeframe much more rapid than for many other high-income countries. The rapidly rising prevalence of NCDs and increased susceptibility of the population to these diseases have dire consequences to future generations. The predicted trends and future burden on health care systems demands that public health action be more interventionist than those in developed countries (James PT: WHO Mission Report: Nutrition Planning for Health in 2050, unpublished). Given the low levels of physical activity in the Arabian Peninsula and high levels of sedentary behaviour, a much stronger evidence base is needed to guide action than is currently available.
Policy relevant research should be undertaken by interdisciplinary teams of policy makers and researchers [26, 108]. Guided by the Behavioural Epidemiology Framework, priority research includes examining these behaviours across the four domains (household, work, transport and leisure). Following the ecological model and using standard assessment tools will improve the quality of research. For the short-term, the most feasible and priority intervention research is in the education, health and sports sectors, especially targeting women and young people. Adapting and testing international models and assessing some of the positive examples in the Arabian Peninsula [114, 115], can help guide and/or refine current policy and practice [147].
References
Studies included in the review are starred (*)
Rahim HF, Sibai A, Khader Y, Hwalla N, Fadhil I, Alsiyabi H, Mataria A, Mendis S, Mokdad AH, Husseini A. Non-communicable diseases in the Arab world. Lancet. 2014;383(9914):356–67.
Mokdad AH, Jaber S, Aziz MI, AlBuhairan F, AlGhaithi A, AlHamad NM, Al-Hooti SN, Al-Jasari A, AlMazroa MA, AlQasmi AM, et al. The state of health in the Arab world, 1990–2010: an analysis of the burden of diseases, injuries, and risk factors. Lancet. 2014;383(9914):309–20.
World Health Organization. Global Status Report on noncommunicable diseases 2014. Geneva: World Health Organization; 2014.
Poston L, Harthoorn LF, Van Der Beek EM. Obesity in pregnancy: implications for the mother and lifelong health of the child. A consensus statement. Pediatr Res. 2010;69(2):175–80.
Al-Gazali L, Hamamy H, Al-Arrayad S. Genetic disorders in the Arab world. BMJ. 2006;333(7573):831–4.
Gibbs BB, Hergenroeder AL, Katzmarzyk PT, Lee IM, Jakicic JM. Definition, measurement, and health risks associated with sedentary behavior. Med Sci Sports Exerc. 2015;47(6):1295–300.
Pate RR, O’Neill JR, Lobelo F. The evolving definition of “sedentary”. Exerc Sport Sci Rev. 2008;36(4):173–8.
Owen N, Salmon J, Koohsari MJ, Turrell G, Giles-Corti B. Sedentary behaviour and health: mapping environmental and social contexts to underpin chronic disease prevention. Br J Sports Med. 2014;48(3):174–7.
Owen N, Sparling PB, Healy GN, Dunstan DW, Matthews CE. Sedentary behavior: emerging evidence for a new health risk. Mayo Clin Proc. 2010;85(12):1138–41.
Ekelund U, Steene-Johannessen J, Brown WJ, Fagerland MW, Owen N, Powell KE, Bauman A, Lee IM, Lancet Physical Activity Series 2 Executive C, Lancet Sedentary Behaviour Working G: Does physical activity attenuate, or even eliminate, the detrimental association of sitting time with mortality? A harmonised meta-analysis of data from more than 1 million men and women. Lancet 2016.
Musaiger AO, Hassan AS, Obeid O. The paradox of nutrition-related diseases in the Arab countries: the need for action. Int J Environ Res Public Health. 2011;8(9):3637–71.
Swinburn BA, Sacks G, Hall KD, McPherson K, Finegood DT, Moodie ML, Gortmaker SL. The global obesity pandemic: shaped by global drivers and local environments. Lancet. 2011;378(9793):804–14.
Popkin BM, Adair LS, Ng SW. Global nutrition transition and the pandemic of obesity in developing countries. Nutr Rev. 2012;70(1):3–21.
Ng SW, Popkin BM. Time use and physical activity: a shift away from movement across the globe. Obes Rev. 2012;13(8):659–80.
Ng SW, Zaghloul S, Ali HI, Harrison G, Popkin BM. The prevalence and trends of overweight, obesity and nutrition-related non-communicable diseases in the Arabian Gulf States. Obes Rev. 2010;12(1):1–13.
*Mabry RM, Winkler EA, Reeves MM, Eakin EG, Owen N. Associations of physical activity and sitting time with the metabolic syndrome among Omani adults. Obesity (Silver Spring). 2012;20(11):2290–5.
*Mabry RM, Al-Busaidi ZQ, Reeves MM, Owen N, Eakin EG. Addressing physical inactivity in Omani adults: perceptions of public health managers. Public Health Nutr. 2013;1:8.
*Ali HI, Baynouna LM, Bernsen RM. Barriers and facilitators of weight management: perspectives of Arab women at risk for type 2 diabetes. Health Soc Care Community. 2010;18(2):219–28.
Bell AC, Ge K, Popkin BM. The road to obesity or the path to prevention: motorized transportation and obesity in China. Obes Res. 2002;10(4):277–83.
Ng SW, Norton EC, Popkin BM. Why have physical activity levels declined among Chinese adults? Findings from the 1991–2006 China Health and Nutrition Surveys. Soc Sci Med. 2009;68(7):1305–14.
Monda KL, Gordon-Larsen P, Stevens J, Popkin BM. China’s transition: the effect of rapid urbanization on adult occupational physical activity. Soc Sci Med. 2007;64(4):858–70.
Owen N, Healy GN, Matthews CE, Dunstan DW. Too much sitting: the population health science of sedentary behavior. Exerc Sport Sci Rev. 2010;38(3):105–13.
Sallis JF, Owen N, Fotheringham MJ. Behavioral epidemiology: a systematic framework to classify phases of research on health promotion and disease prevention. Ann Behav Med. 2000;22(4):294–8.
World Health Organization (Regional Office of the Eastern Mediterranean Region). Promoting physical activity in the Eastern Mediterranean Region, a call for action. 2014.
Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. 2009;6(7), e1000097.
Owen N, Sugiyama T, Eakin EE, Gardiner PA, Tremblay MS, Sallis JF. Adults’ sedentary behavior determinants and interventions. Am J Prev Med. 2011;41(2):189–96.
Sallis JF, Owen N, Fisher EB. Ecological models of health behavior. In: Glanz K, Rimer K, Viswanath K, editors. Health Behavior and Health Education: Theory, Research, and Practice. Fourthth ed. San Francisco: Jossey-Bass; 2008. p. 465–82.
Higgins JP, Altman DG, Gotzsche PC, Juni P, Moher D, Oxman AD, Savovic J, Schulz KF, Weeks L, Sterne JA, et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ. 2011;343:d5928.
Long AF, Godfrey M. An evaluation tool to assess the quality of qualitative research studies. Int J Soc Res Methodol Theory Pract. 2004;7(2):181–96.
Armstrong T, Bull F. Development of the World Health Organization Global Physical Activity Questionnaire (GPAQ). J Public Health. 2006;14:66–70.
Craig CL, Marshall AL, Sjostrom M, Bauman AE, Booth ML, Ainsworth BE, Pratt M, Ekelund U, Yngve A, Sallis JF, et al. International physical activity questionnaire: 12-country reliability and validity. Med Sci Sports Exerc. 2003;35(8):1381–95.
*Abd-El-Fattah SM. Rasch Rating Scale Analysis of the Arabic Version of the Physical Activity Self-Efficacy Scale for Adolescents: A Social Cognitive Perspective. Psychology. 2015;06(16):2161–80.
*Al-Hazzaa HM, Al-Sobayel HI, Musaiger AO. Convergent validity of the Arab Teens Lifestyle Study (ATLS) physical activity questionnaire. Int J Environ Res Public Health. 2011;8(9):3810–20.
*Platat C, Jarrar A. Reliability and validity of a physical activity questionnaire in children. Int J Food Sci Nutr. 2011;63(6):637–44.
*Shah SM, Loney T, Sheek-Hussein M, El Sadig M, Al Dhaheri S, El Barazi I, Al Marzouqi L, Aw TC, Ali R. Hypertension prevalence, awareness, treatment, and control, in male South Asian immigrants in the United Arab Emirates: a cross-sectional study. BMC Cardiovasc Disord. 2015;15:30.
*Al-Mahroos F, Al-Roomi K. Obesity among adult Bahraini population: impact of physical activity and educational level. Ann Saudi Med. 2001;21(3–4):183–7.
*Ardawi MS, Rouzi AA, Qari MH. Physical activity in relation to serum sclerostin, insulin-like growth factor-1, and bone turnover markers in healthy premenopausal women: a cross-sectional and a longitudinal study. J Clin Endocrinol Metab. 2012;97(10):3691–9.
*Salman RA, Al-Rubeaan KA. Incidence and risk factors of hypertension among Saudi type 2 diabetes adult patients: an 11-year prospective randomized study. J Diabetes Complications. 2009;23(2):95–101.
Al-Nozha MM, Al-Hazzaa HM, Arafah MR, Al-Khadra A, Al-Mazrou YY, Al-Maatouq MA, Khan NB, Al-Marzouki K, Al-Harthi SS, Abdullah M, et al. Prevalence of physical activity and inactivity among Saudis aged 30–70 years. A population-based cross-sectional study. Saudi Med J. 2007;28(4):559–68.
*Rouzi AA, Al-Sibiani SA, Al-Senani NS, Radaddi RM, Ardawi MS. Independent predictors of all osteoporosis-related fractures among healthy Saudi postmenopausal women: the CEOR Study. Bone. 2011;50(3):713–22.
*Al Junaibi A, Abdulle A, Sabri S, Hag-Ali M, Nagelkerke N. The prevalence and potential determinants of obesity among school children and adolescents in Abu Dhabi, United Arab Emirates. Int J Obes (Lond). 2012;37(1):68–74.
Kerkadi A, Abo-Elnaga N, Ibrahim W. Prevalence of overweight and associated risk factors among primary female school children in Al-Ain city United Arab Emirates. Emirates J Food Agric. 2005;17:1.
*Yousef S, Eapen V, Zoubeidi T, Mabrouk A. Behavioral Correlation with Television Viewing and Videogame Use among Children in the United Arab Emirates. Int J Psychiatry Clin Pract. 2013;18:203–7.
*Al-Kilani H, Waly M, Yousef R. Trends of Obesity and Overweight among College Students in Oman: A cross sectional study. Sultan Qaboos Univ Med J. 2012;12(1):69–76.
*Al Saif A, Alsenany S. Aerobic and anaerobic exercise training in obese adults. J Phys Ther Sci. 2015;27(6):1697–700.
*Al-Ghimlas F, Subbramaniam K, Al-Owaish O, Bilas MT, Behbehani K. The Effects of Supervised Exercise Program on Health-Related Physical Fitness in Kuwait. British J Med Med Res. 2014;4(32):5083.
*Kneffel Z, Goebel R, Alkhatib A. Car-diovascular risk factors and their re-sponses to a 10 weeks training pro-gram in young Qatari adults. Obes Res Open J. 2015;2(2):57–63.
*Al-Hamdan NA, Al-Zalabani AH, Saeed AA. Comparative study of physical activity of hypertensives and normotensives: A cross-sectional study of adults in Saudi Arabia. J Family Community Med. 2012;19(3):162–6.
*El Bcheraoui C, Memish ZA, Tuffaha M, Daoud F, Robinson M, Jaber S, Mikhitarian S, Al Saeedi M, AlMazroa MA, Mokdad AH, et al. Hypertension and its associated risk factors in the kingdom of saudi arabia, 2013: a national survey. Int J Hypertens. 2014;2014:564679.
*Abdi S, Sadiya A, Ali S, Varghese S, Abusnana S. Behavioural Lifestyle Intervention Study (BLIS) in patients with type 2 diabetes in the United Arab Emirates: A randomized controlled trial. BMC Nutrition. 2015;1(1):1.
*Sadiya A, Abdi S, Abusnana S. Lifestyle Intervention for Weight Loss: a group-based program for Emiratis in Ajman, United Arab Emirates. Diabetes Metab Syndr Obes. 2016;9:101–8.
*Tomar RH, Hashim MH, Al-Qahtani MH. Effects of a 12-week aerobic training on glycemic control in type 2 diabetes mellitus male patients. Saudi Med J. 2013;34(7):757–9.
*Alghadir AH, Gabr SA, Al-Eisa ES, Alghadir MH. Correlation between bone mineral density and serum trace elements in response to supervised aerobic training in older adults. Clin Interv Aging. 2016;11:265–73.
*El-Aty MA, Mabry R, Morsi M, Al-Lawati J, Al-Riyami A, El-Sayed M. Metabolic Syndrome and Its Components: Secondary analysis of the World Health Survey, Oman. Sultan Qaboos University medical journal. 2014;14(4):e460–467.
*Tuffaha M, El Bcheraoui C, Daoud F, Al Hussaini HA, Alamri F, Al Saeedi M, Basulaiman M, Memish ZA, AlMazroa MA, Al Rabeeah AA, et al. Deficiencies Under Plenty of Sun: Vitamin D Status among Adults in the Kingdom of Saudi Arabia, 2013. N Am J Med Sci. 2015;7(10):467–75.
*Muhairi SJ, Mehairi AE, Khouri AA, Naqbi MM, Maskari FA, Al Kaabi J, Al Dhaheri AS, Nagelkerke N, Shah SM. Vitamin D deficiency among healthy adolescents in Al Ain. United Arab Emirates BMC Public Health. 2013;13:33.
*Al-Nakeeb Y, Lyons M, Collins P, Al-Nuaim A, Al-Hazzaa H, Duncan MJ, Nevill A. Obesity, physical activity and sedentary behavior amongst British and Saudi youth: a cross-cultural study. Int J Environ Res Public Health. 2012;9(4):1490–506.
*Al-Nuaim AA, Al-Nakeeb Y, Lyons M, Al-Hazzaa HM, Nevill A, Collins P, Duncan MJ. The Prevalence of Physical Activity and Sedentary Behaviours Relative to Obesity among Adolescents from Al-Ahsa, Saudi Arabia: Rural versus Urban Variations. J Nutr Metab. 2012;2012:417589.
*Alrashidi M, Shahwan-Akl L, James J, Jones L. Contributing factors to childhood overweight and obesity in Kuwait. International Journal of Health Sciences. 2015;3(1):133–55.
*Al-Haifi AR, Al-Fayez MA, Al-Athari BI, Al-Ajmi FA, Allafi AR, Al-Hazzaa HM, Musaiger AO. Relative contribution of physical activity, sedentary behaviors, and dietary habits to the prevalence of obesity among Kuwaiti adolescents. Food Nutr Bull. 2013;34(1):6–13.
*Al-Hazzaa HM, Abahussain NA, Al-Sobayel HI, Qahwaji DM, Musaiger AO. Lifestyle factors associated with overweight and obesity among Saudi adolescents. BMC Public Health. 2012;12:354.
*Alqahtani N, Scott J. S U: Physical Activity and Sedentary Behaviors as Risk Factors of Obesity among Rural Adolescents. Journal of Child and Adolescent Behaviour. 2015;42:13.
*Al-Eisa ES, Al-Sobayel HI. Physical Activity and Health Beliefs among Saudi Women. J Nutr Metab. 2012;2012:642187.
*Al-Eisa E, Buragadda S, Melam GR. Association between physical activity and psychological status among Saudi female students. BMC Psychiatry. 2014;14:238.
*Al-Hazzaa HM, Al-Rasheedi AA. Adiposity and physical activity levels among preschool children in Jeddah. Saudi Arabia Saudi Med J. 2007;28(5):766–73.
*Alkahtani SA, Elkilany AM, Al-Mohannadi AS, AlDuhIshy AM. Relationship Between Self-Reported Dietary Intake and Measured Physical Activity among Male Students in the Preparatory Year in University of Dammam in Saudi Arabia. Curr Res Nutr Food Sci J. 2015;3(2):130–9.
*Basulaiman M, El Bcheraoui C, Tuffaha M, Robinson M, Daoud F, Jaber S, Mikhitarian S, Wilson S, Memish ZA, Al Saeedi M, et al. Hypercholesterolemia and its associated risk factors-Kingdom of Saudi Arabia, 2013. Ann Epidemiol. 2014;24(11):801–8.
*Moradi-Lakeh M, El Bcheraoui C, Tuffaha M, Daoud F, Al Saeedi M, Basulaiman M, Memish ZA, AlMazroa MA, Al Rabeeah AA, Mokdad AH. Self-Rated Health Among Saudi Adults: Findings from a National Survey, 2013. J Community Health. 2015;40(5):920–6.
*Al Thani M, Al Thani A, Al-Chetachi W, Al Malki B, Khalifa SAH, Bakri AH, Hwalla N, Nasreddine L, Naja F. Lifestyle Patterns Are Associated with Elevated Blood Pressure among Qatari Women of Reproductive Age: A Cross-Sectional National Study. Nutrients. 2015;7(9):7593–615.
*Mabry RM, Winkler EA, Reeves MM, Eakin EG, Owen N. Correlates of Omani adults’ physical inactivity and sitting time. Public Health Nutr. 2012;16(1):65–72.
*AlQuaiz AM, Tayel SA. Barriers to a healthy lifestyle among patients attending primary care clinics at a university hospital in Riyadh. Ann Saudi Med. 2009;29(1):30–5.
*Awadalla NJ, Aboelyazed AE, Hassanein MA, Khalil SN, Aftab R, Gaballa II, Mahfouz AA. Assessment of physical inactivity and perceived barriers to physical activity among health college students, south-western Saudi Arabia. East Mediterr Health J. 2014;20(10):596–604.
*Gawwad ES. Stages of change in physical activity, self efficacy and decisional balance among saudi university students. J Family Community Med. 2008;15(3):107–15.
*Youssef RM, Al Shafie K, Al-Mukhaini M, Al-Balushi H. Physical activity and perceived barriers among high-school students in Muscat. Oman East Mediterr Health J. 2013;19(9):759–68.
*Al-Otaibi HH. Measuring Stages of Change, Perceived Barriers and Self efficacy for Physical Activity in Saudi Arabia. Asian Pac J Cancer Prev. 2013;14(2):1009–16.
*Al-Hazzaa HM. Health-enhancing physical activity among Saudi adults using the International Physical Activity Questionnaire (IPAQ). Public Health Nutr. 2007;10(1):59–64.
*Allafi A, Al-Haifi AR, Al-Fayez MA, Al-Athari BI, Al-Ajmi FA, Al-Hazzaa HM, Musaiger AO, Ahmed F. Physical activity, sedentary behaviours and dietary habits among Kuwaiti adolescents: gender differences. Public Health Nutr. 2013;1:8.
*Al-Hazzaa HM, Abahussain NA, Al-Sobayel HI, Qahwaji DM, Musaiger AO. Physical activity, sedentary behaviors and dietary habits among Saudi adolescents relative to age, gender and region. Int J Behav Nutr Phys Act. 2011;8:140.
Al-Hazzaa HM, Alahmadi MA, Al-Sobayel HI, Abahussain NA, Qahwaji DM, Musaiger AO. Patterns and Determinants of Physical Activity Among Saudi Adolescents. J Phys Act Health. 2013;11:1202–11.
*Al-Hazzaa HM, Al-Nakeeb Y, Duncan MJ, Al-Sobayel HI, Abahussain NA, Musaiger AO, Lyons M, Collins P, Nevill A. A cross-cultural comparison of health behaviors between Saudi and British adolescents living in urban areas: gender by country analyses. Int J Environ Res Public Health. 2013;10(12):6701–20.
*Al-Hazzaa HM, Al-Sobayel HI, Abahussain NA, Qahwaji DM, Alahmadi MA, Musaiger AO. Association of dietary habits with levels of physical activity and screen time among adolescents living in Saudi Arabia. J Hum Nutr Diet. 2013;27:204–13.
Kilani H, Al-Hazzaa H, Waly MI, Musaiger A. Lifestyle Habits: Diet, physical activity and sleep duration among Omani adolescents. Sultan Qaboos Univ Med J. 2013;13(4):510–9.
*Mahfouz AA, Abdelmoneim I, Khan MY, Daffalla AA, Diab MM, Al-Gelban KS, Moussa H. Obesity and related behaviors among adolescent school boys in Abha City. Southwestern Saudi Arabia J Trop Pediatr. 2008;54(2):120–4.
*Mahfouz AA, Shatoor AS, Khan MY, Daffalla AA, Mostafa OA, Hassanein MA. Nutrition, physical activity, and gender risks for adolescent obesity in Southwestern Saudi Arabia. Saudi J Gastroenterol. 2011;17(5):318–22.
*Musaiger AO, Zagzoog N. Dietary and lifestyle habits among adolescent girls in Saudi Arabia: A comparison between private and government schools. Nutrition & Food Science. 2013;43(6):605–10.
*Al-Hazzaa HM, Alahmadi MA, Al-Sobayel HI, Abahussain NA, Qahwaji DM, Musaiger AO. Patterns and determinants of physical activity among saudi adolescents. J Phys Act Health. 2014;11(6):1202–11.
*Al-Sobayel H, Al-Hazzaa HM, Abahussain NA, Qahwaji DM, Musaiger AO. Gender differences in leisure-time versus non-leisure-time physical activity among Saudi adolescents. Ann Agric Environ Med. 2015;22(2):344–8.
*Duncan MJ, Al-Hazzaa HM, Al-Nakeeb Y, Al-Sobayel HI, Abahussain NA, Musaiger AO, Lyons M, Collins P, Nevill A. Anthropometric and lifestyle characteristics of active and inactive Saudi and British adolescents. Am J Hum Biol. 2014;26(5):635–42.
*Amin TT, Al Khoudair AS, Al Harbi MA, Al Ali AR. Leisure time physical activity in Saudi Arabia: prevalence, pattern and determining factors. Asian Pac J Cancer Prev. 2012;13(1):351–60.
*Amin TT, Suleman W, Ali A, Gamal A, Al Wehedy A. Pattern, prevalence, and perceived personal barriers toward physical activity among adult Saudis in Al-Hassa. KSA J Phys Act Health. 2011;8(6):775–84.
*Almajwal AM. Correlations of Physical Activity, Body Mass Index, Shift Duty, and Selected Eating Habits among Nurses in Riyadh. Saudi Arabia Ecol Food Nutr. 2015;54(4):397–417.
*Donnelly TT, Al Suwaidi J, Al Enazi NR, Idris Z, Albulushi AM, Yassin K, Rehman AM, Hassan AH. Qatari women living with cardiovascular diseases-challenges and opportunities to engage in healthy lifestyles. Health Care Women Int. 2012;33(12):1114–34.
*Sulaiman N, Hamdan A, Al-Bedri DAM, Young D. Diabetes knowledge and attitudes towards prevention and health promotion: qualitative study in Sharjah, United Arab Emirates. IntJFood Safety, Nutrition and Public Health. 2009;2(1):78–88.
*Alsubaie AS, Omer EO. Physical Activity Behavior Predictors, Reasons and Barriers among Male Adolescents in Riyadh, Saudi Arabia: Evidence for Obesogenic Environment. Int J Health Sci (Qassim). 2015;9(4):400–8.
*Daradkeh G, Al Muhannadi A, Chandra P, Al Hajr M, Al Muhannadi H. Physical Activity Profile of Adolescence in the State of Qatar. International Journal of Nutrition and Growth. 2015;1(1):1–7.
*Al-Eisa E, Al-Rushud A, Alghadir A, Anwer S, Al-Harbi B, Al-Sughaier N, Al-Yoseef N, Al-Otaibi R, Al-Muhaysin HA. Effect of Motivation by “Instagram” on Adherence to Physical Activity among Female College Students. Biomed Res Int. 2016;2016:1546013.
*Barss P, Grivna M, Al-Maskari F, Kershaw G. Strengthening public health medicine training for medical students: development and evaluation of a lifestyle curriculum. Med Teach. 2008;30(9–10):e196–218.
*Midhet FM, Sharaf FK. Impact of health education on lifestyles in central Saudi Arabia. Saudi Med J. 2011;32(1):71–6.
*Abduelkarem A, Sackville M. Changes of some Health Indicators in Patients with Type 2 Diabetes: A Prospective Study in three Community Pharmacies in Sharjah. United Arab Emirates Libyan J Med. 2009;4(1):31–6.
*Sharaf F. Impact of health education on compliance among patients of chronic diseases in Al Qassim, Saudi Arabia. Int J Health Sci (Qassim). 2011;4(2):139–48.
*Grant N, Gibbs T, Naseeb TA, Al-Garf A. Medical students as family-health advocates: Arabian Gulf University experience. Med Teach. 2007;29(5):e117–121.
Physical Activity Guidelines Advisory Committee. Physical activity guidelines advisory committee report. Washington: US Department of Health and Human Services; 2008.
World Health Organization. Reducing Risks, Promoting Healthy Life. World Health Report 2002. Geneva: World Health Organization; 2002.
Guthold R, Cowan MJ, Autenrieth CS, Kann L, Riley LM. Physical activity and sedentary behavior among schoolchildren: a 34-country comparison. J Pediatr. 2010;157(1):43–9. e41.
World Health Organization. Global Action Plan for the Prevention and Control of Noncommunicable Diseases, 2013–2020 [Resolution WHA66.10]. Geneva: World Health Organization; 2013.
Bauman A, Bull F, Chey T, Craig CL, Ainsworth BE, Sallis JF, Bowles HR, Hagstromer M, Sjostrom M, Pratt M, et al. The International Prevalence Study on Physical Activity: results from 20 countries. Int J Behav Nutr Phys Act. 2009;6(1):21.
Trost SG, Owen N, Bauman AE, Sallis JF, Brown W. Correlates of adults’ participation in physical activity: review and update. Med Sci Sports Exerc. 2002;34(12):1996–2001.
Sallis JF, Cervero RB, Ascher W, Henderson KA, Kraft MK, Kerr J. An ecological approach to creating active living communities. Annu Rev Public Health. 2006;27:297–322.
World Health Organization. Global Recommendations for Physical Activity for Health. Geneva: World Health Organization; 2010.
Bauman A, Phongsavan P, Schoeppe S, Owen N. Physical activity measurement--a primer for health promotion. Promot Educ. 2006;13(2):92–103.
Hallal PC, Andersen LB, Bull FC, Guthold R, Haskell W, Ekelund U. Global physical activity levels: surveillance progress, pitfalls, and prospects. Lancet. 2012;380(9838):247–57.
Freedson P, Bowles HR, Troiano R, Haskell W. Assessment of physical activity using wearable monitors: recommendations for monitor calibration and use in the field. Med Sci Sports Exerc. 2012;44(1):S1–4.
Cain KL, Sallis JF, Conway TL, Van Dyck D, Calhoon L. Using accelerometers in youth physical activity studies: a review of methods. J Phys Act Health. 2013;10(3):437–50.
Bull F. Global advocacy for physical activity-Development and progress of the Toronto Charter for Physical Activity: A global call for action. Res Exerc Epidemiol. 2011;13(1):1–10.
World Health Organization (Regional Office of the Eastern Mediterranean Region). Promoting physical activity in the Eastern Mediterranean Region through a life-course approach. 2014.
The Toronto charter for physical activity. a call to action [http://www.globalpa.org.uk/charter/]. Accessed 11 Apr 2012.
Non communicable disease prevention: Investments that work for physical activity [http://www.globalpa.org.uk/investments/].
*Al-Rafaee SA, Al-Hazzaa HM. Physical activity profile of adult males in Riyadh City. Saudi Med J. 2001;22(9):784–9.
*Ali HI, Bernsen RM, Baynouna LM. Barriers to weight management among Emirati women: a qualitative investigation of health professionals’ perspectives. Int Q Community Health Educ. 2008;29(2):143–59.
*Berger G, Peerson A. Giving young Emirati women a voice: participatory action research on physical activity. Health Place. 2009;15(1):117–24.
*Hashim R, Al-Ali K. Health of dentists in United Arab Emirates. Int Dent J. 2013;63(1):26–9.
*Musaiger AO, Al-Kandari FI, Al-Mannai M, Al-Faraj AM, Bouriki FA, Shehab FS, Al-Dabous LA, Al-Qalaf WB. Perceived barriers to weight maintenance among university students in Kuwait: the role of gender and obesity. Environ Health Prev Med. 2014;19:207–14.
*Serour M, Alqhenaei H, Al-Saqabi S, Mustafa AR, Ben-Nakhi A. Cultural factors and patients’ adherence to lifestyle measures. Br J Gen Pract. 2007;57(537):291–5.
Leavy JE, Bull FC, Rosenberg M, Bauman A. Physical activity mass media campaigns and their evaluation: a systematic review of the literature 2003–2010. Health Educ Res. 2011;26(6):1060–85.
Al-Khouri AM. Population growth and government modernisation efforts. International Journal of Research in Management and Technology. 2012;2(1):1–8.
World Health Organization (Regional Office of the Eastern Mediterranean Region). Demographic, social and health indicators for countries of the Eastern Mediterranean Region. Cairo: World Health Organization (Regional Office of the Eastern Mediterranean Region); 2013.
*Al-Doghether M, Al-Tuwijri A, Khan A. Obstacles to preventive intervention. Do physicians’ health habits and mind-set towards preventive care play any role? Saudi Med J. 2007;28(8):1269–74.
*Al-Ghawi A, Uauy R. Study of the knowledge, attitudes and practices of physicians towards obesity management in primary health care in Bahrain. Public Health Nutr. 2009;12(10):1791–8.
Mabry R, Owen N, Eakin E. A National Strategy for Promoting Physical Activity in Oman: A call for action. Sultan Qaboos Univ Med J. 2014;14(2):e170–175.
Cobiac LJ, Vos T, Barendregt JJ. Cost-effectiveness of interventions to promote physical activity: a modelling study. PLoS Med. 2009;6(7), e1000110.
Trowbridge MJ, Schmid TL. Built environment and physical activity promotion: place-based obesity prevention strategies. J Law Med Ethics. 2013;41(2):46–51.
Sallis JF, Floyd MF, Rodriguez DA, Saelens BE. Role of built environments in physical activity, obesity, and cardiovascular disease. Circulation. 2012;125(5):729–37.
Durand CP, Andalib M, Dunton GF, Wolch J, Pentz MA. A systematic review of built environment factors related to physical activity and obesity risk: implications for smart growth urban planning. Obes Rev. 2011;12(5):e173–182.
Differences in prevalence of obesity among black, white, and Hispanic adults-United States, 2006–2008. MMWR Morb Mortal Wkly Rep. 2009;58(27):740–4.
Koohsari MJ, Sugiyama T, Lamb KE, Villanueva K, Owen N. Street connectivity and walking for transport: role of neighborhood destinations. Prev Med. 2014;66:118–22.
UN-Habitat. The State of Arab Cities, 2012, Challenges of Urban Transition. Secondth ed. Nairobi: UN-Habitat; 2012.
Mohammad R, Sidaway J. Spectacular urbanization amidst variegated geographies of globalization: learning from Abu Dhabi’s Trajectory through the lives of South Asian Men. International Journal of Urban and Regional Research. 2012;363:606–27.
Mohareb NI. Land use as a sustainability indicator for Arab cities. Urban Design and Planning. 2009;163:105–66.
Musaiger AO, Al-Mannai M, Tayyem R, Al-Lalla O, Ali EY, Kalam F, Benhamed MM, Saghir S, Halahleh I, Djoudi Z, et al. Perceived barriers to healthy eating and physical activity among adolescents in seven Arab countries: a cross-cultural study. ScientificWorldJournal. 2013;2013:232164.
Chan CB, Ryan DA, Tudor-Locke C. Relationship between objective measures of physical activity and weather: a longitudinal study. Int J Behav Nutr Phys Act. 2006;3:21.
Carson V, Spence JC. Seasonal variation in physical activity among children and adolescents: a review. Pediatr Exerc Sci. 2010;22(1):81–92.
Tucker P, Gilliland J. The effect of season and weather on physical activity: a systematic review. Public Health. 2007;121(12):909–22.
Prakash PJ, Stenchikov G, Kalenderski S, Oslpov S, Bangalath H. The impact of dust storms on the Arabian Peninsula and the Red Sea. Atmospheric, Chemistry, Physics Discussions. 2014;14:19181–245.
Cerin E, Conway TL, Cain KL, Kerr J, De Bourdeaudhuij I, Owen N, Reis RS, Sarmiento OL, Hinckson EA, Salvo D, et al. Sharing good NEWS across the world: developing comparable scores across 12 countries for the Neighborhood Environment Walkability Scale (NEWS). BMC Public Health. 2013;13:309.
Sugiyama T, Cerin E, Owen N, Oyeyemi AL, Conway TL, Van Dyck D, Schipperijn J, Macfarlane DJ, Salvo D, Reis RS, et al. Perceived neighbourhood environmental attributes associated with adults recreational walking: IPEN Adult study in 12 countries. Health Place. 2013;28:22–30.
Mabry RM, Reeves MM, Eakin EG, Owen N. Evidence of physical activity participation among men and women in the countries of the Gulf Cooperation Council: a review. Obes Rev. 2010;11:457–64.
Giles-Corti B, Sallis JF, Sugiyama T, Frank LD, Lowe M, Owen N. Translating active living research into policy and practice: One important pathway to chronic disease prevention. J Public Health Policy. 2015;36(2):231–43.
*Al-Eisa E, Alghadir AH, Gabr SA, Iqbal ZA. Exercise intervention as a protective modulator against metabolic disorders in cigarette smokers. J Phys Ther Sci. 2016;28(3):983–91.
*Alghadir AH, Gabr SA, Aly FA. The effects of 4 weeks aerobic training on saliva cortisol and testosterone in young healthy persons. J Phys Ther Sci. 2015;27(7):2029–33.
*Al-Daghri NM, Alokail MS, Rahman S, Amer OE, Al-Attas OS, Alfawaz H, Tripathi G, Sabico S, Chrousos GP, McTernan PG, et al. Habitual physical activity is associated with circulating irisin in healthy controls but not in subjects with diabetes mellitus type 2. Eur J Clin Invest. 2015;45(8):775–81.
*Al-Thani MH, Al-Thani AA, Al-Chetachi WF, Khalifa SAH, Akram H, Poovelil BV, Almalki BA, Bakri AH, Arora P, Badawi A. Dietary and Nutritional Factors Influencing Obesity in Qatari Adults and the Modifying Effect of Physical Activity. J Obes Weight-Loss Medic. 2015;1:007.
*El-Ghazali S, Ibrahim JM, Kanari BM, Ismail NA. The relationship between lifestyle and body mass index among university students in Kuwait. Egyptian Journal of Community Medicine. 2010;28:1.
*Hegazy AM, Salama BM, Elgaml AM, Alzyat AR. Association of low back pain with vitamin D deficiency and other common risk factors: A hospital based case–control study. European Journal of Preventive Medicine. 2015;3:1–5.
*Memish ZA, El Bcheraoui C, Tuffaha M, Robinson M, Daoud F, Jaber S, Mikhitarian S, Al Saeedi M, AlMazroa MA, Mokdad AH, et al. Obesity and associated factors--Kingdom of Saudi Arabia, 2013. Prev Chronic Dis. 2014;11:E174.
*Al Saweer A, Salehi S, Al Tiho M, Al Saffar B, Al Amer M. Interventional Program for Teenagers’ Obesity. Bahrain Medical Bulletin. 2015;37(2):109.
*Al-Haifi AA, AlMajed HT, Al-Hazzaa HM, Musaiger AO, Arab MA, Hasan RA. Relative Contribution of Obesity, Sedentary Behaviors and Dietary Habits to Sleep Duration Among Kuwaiti Adolescents. Glob J Health Sci. 2016;8(1):107–17.
*Al-Hazzaa HM, Musaiger AO, Abahussain NA, Al-Sobayel HI, Qahwaji DM. Lifestyle correlates of self-reported sleep duration among Saudi adolescents: a multicentre school-based cross-sectional study. Child Care Health Dev. 2013;40:533–42.
*Allam AR, Taha IM, Al-Nozha OM, Sultan IE. Nutritional and health status of medical students at a university in Northwestern Saudi Arabia. Saudi Med J. 2012;33(12):1296–303.
*Banday AH, Want FA, Alris FF, Alrayes MF, Alenzi MJ. A Cross-sectional Study on the Prevalence of Physical Activity Among Primary Health Care Physicians in Aljouf Region of Saudi Arabia. Mater Sociomed. 2015;27(4):263–6.
*Carter AO, Elzubeir M, Abdulrazzaq YM, Revel AD, Townsend A. Health and lifestyle needs assessment of medical students in the United Arab Emirates. Med Teach. 2003;25(5):492–6.
*Khalaf A, Ekblom O, Kowalski J, Berggren V, Westergren A, Al-Hazzaa H. Female university students’ physical activity levels and associated factors--a cross-sectional study in southwestern Saudi Arabia. Int J Environ Res Public Health. 2013;10(8):3502–17.
*Koura MR, Al-Dabal BK, Rasheed P, Al-Sowielem LS, Makki SM, Koura MR, Al-Dabal BK, Rasheed P, Al-Sowielem LS, Makki SM. Prehypertension among young adult females in Dammam, Saudi Arabia. East Mediterr Health J. 2013;19(10):899–900.
*Farghaly NF, Ghazali BM, Al-Wabel HM, Sadek AA, Abbag FI. Life style and nutrition and their impact on health of Saudi school students in Abha, Southwestern region of Saudi Arabia. Saudi Med J. 2007;28(3):415–21.
*Gharib NM, Rasheed P. Obesity Among Bahraini Children and Adolescents: Prevalence And Associated Factors. Journal of the Bahrain Medical Society. 2008;20:3.
*AboZaid HA, Farahat FM. Physical activity profile among patients attending family medicine clinics in western Saudi Arabia. Saudi Med J. 2010;31(4):428–33.
*Taha AZ. Self-reported knowledge and pattern of physical activity among school students in Al Khobar, Saudi Arabia. East Mediterr Health J. 2008;14(2):344–55.
*Faris MA, Epuru S, Al-Shimmari S, Al-Shimmari E. Alarming High Levels of Energy Drinks Consumption among School Children in Hail, Northern of Saudi Arabia. International Journal of Child Health and Nutrition. 2015;4:1–13.
Acknowledgements
Not applicable.
Funding
No funding was provided for this study.
Availability of data and material
Summary information of articles reviewed are provided in Tables and Supplementary materials. Endnote file is available on request.
Authors’ contributions
RMM conceived the study, conducted the literature review, drafted and finalized the manuscript, MJK assisted with the literature review, data extraction/synthesis and quality assessment. FB assisted in drafting the manuscript, and NO supervised the project. All authors critically reviewed the manuscript and approved the final version. The views expressed in this paper are those of the authors and do not necessarily reflect those of the WHO. All authors read and approved the final manuscript.
Competing interests
The authors declare that they have no competing interests.
Consent for publication
None since individual person’s data was not included.
Ethics approval and consent to participate
None since this was a review.
Author information
Authors and Affiliations
Corresponding author
Additional file
Additional file 1:
Quality Assessment of Studies on Physical Activity and Sedentary Behaviour in the Arabian Peninsula. (DOCX 124 kb)
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Mabry, R., Koohsari, M.J., Bull, F. et al. A systematic review of physical activity and sedentary behaviour research in the oil-producing countries of the Arabian Peninsula. BMC Public Health 16, 1003 (2016). https://doi.org/10.1186/s12889-016-3642-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12889-016-3642-4