
Abstract
Background
The inclusion of biomarkers could improve diagnostic accuracy of attention-deficit/hyperactivity disorder (ADHD). One potential biomarker is the ADHD polygenic score (PGS), a measure of genetic liability for ADHD. This study aimed to investigate if the ADHD PGS can provide additional information alongside ADHD rating scales and examination of family history of ADHD to distinguish between ADHD cases and controls.
Methods
Polygenic scores were calculated for 576 adults with ADHD and 530 ethnically matched controls. ADHD PGS was used alongside scores from the Wender-Utah Rating Scale (WURS) and the Adult ADHD Self-Report Scale (ASRS) as predictors of ADHD diagnosis in a set of nested logistic regression models. These models were compared by likelihood ratio (LR) tests, Akaike information criterion corrected for small samples (AICc), and Lee R². These analyses were repeated with family history of ADHD as a covariate in all models.
Results
The ADHD PGS increased the variance explained of the ASRS by 0.58% points (pp) (R2ASRS = 61.11%, R2ASRS + PGS=61.69%), the WURS by 0.61pp (R2WURS = 77.33%, R2WURS + PGS= 77.94%), of ASRS and WURS together by 0.57pp (R2ASRS + WURS=80.84%, R2ASRS + WURS+PGS=81.40%), and of self-reported family history by 1.40pp (R2family = 28.06%, R2family + PGS=29.46%). These increases were statistically significant, as measured by LR tests and AICc.
Conclusion
We found that the ADHD PGS contributed additional information to common diagnostic aids. However, the increase in variance explained was small, suggesting that the ADHD PGS is currently not a clinically useful diagnostic aid. Future studies should examine the utility of ADHD PGS in ADHD prediction alongside non-genetic risk factors, and the diagnostic utility of the ADHD PGS should be evaluated as more genetic data is accumulated and computational tools are further refined.
Similar content being viewed by others


Introduction
A clinical diagnosis of attention-deficit/hyperactivity disorder (ADHD) relies on a detailed assessment of symptoms and patient history by a trained professional [1]. Structured interviews and rating scales of ADHD symptoms are effective aids in the diagnosis of ADHD and are commonly employed in both primary care and specialist treatment settings [1, 2]. Rating scales are cost-effective, provide standardized information on symptom severity, and allow for ADHD symptoms to be followed up to monitor clinical course and treatment efficacy [3].
ADHD has a high heritability, and genome-wide association studies (GWASs) have identified common genetic markers associated with the condition [4, 5]. A polygenic score (PGS) is a measure of an individual’s genetic liability for a trait [6]. It is calculated by summing up an individual’s common risk alleles weighed by their effect sizes given by a GWAS [6]. The ADHD PGS has several potential clinical applications, such as in screening, risk stratification, treatment optimization, and disease prediction [7,8,9,10]. The inclusion of the ADHD PGS in the diagnostic process could make the diagnosis of ADHD more precise.
This study aimed to investigate whether the ADHD PGS has potential as a diagnostic aid in ADHD diagnostics by providing additional information to self-report rating scales commonly used in clinical practice, as well as self-reported ADHD family history.
Method
Participants
Participants were recruited as part of the “ADHD in Norwegian Adults” project launched in 2004, and all participants provided a signed informed consent [11]. Data collection was performed with questionnaires mailed to participants between 2005 and 2008.
The case sample consists of a well-characterized group of patients, mainly recruited from a national registry of adults diagnosed with ADHD in Norway between 1997 and 2005. Inclusion criteria were a clinical diagnosis of ADHD and age greater than 18 years, and there were no formal exclusion criteria.
The controls were recruited from the general adult Norwegian population and were recruited from several sources. The majority (79%) were randomly selected individuals between 18 and 40 years of age from the Medical Birth Registry of Norway, which includes all individuals born in Norway after January 1st 1967 [12]. The remainder were recruited from friends of cases and from students attending the University of Bergen between 2005 and 2007. The inclusion criterium was age older than 18 years, and there were no exclusion criteria. For a more detailed description of the sample, see Johansson et al. 2008 [11].
Genetic data
DNA was collected via kits for collecting saliva mailed to the participants. DNA from saliva samples were genotyped in two batches: one at the Broad Institute (Boston, MA, USA), genotyped on the Human OmniExpress-12v1-1_B (Illumina, San Diego, CA, USA) platform, and one at deCODE (Reykjavik, Iceland), genotyped on the Human OmniExpress-12v1_H (Illumina, San Diego, CA, USA) platform. Genotypes were assigned according to the standard Illumina protocol in GenomeStudio software, version V2011.1 [13]. Quality control and imputation were performed using Ricopili [14]. The batches were merged with PLINK [15].
Rating scales
Adult ADHD self-report scale
The Adult ADHD Self-Report Scale (ASRS) was developed as a screening tool to assess symptoms of ADHD in adults [16]. It includes 18 items rating symptoms of inattention, hyperactivity, and impulsivity during the past six months, based on the Diagnostic and Statistical Manual of Mental Disorders 4th edition (DSM-4) criteria for ADHD [16]. Symptom severity is reported on a 5-point Likert-type scale from 0 (never) to 4 (very often), with a range of 0–72 points.
A shorter version, the ASRS-screener, was later developed. This version has six items with a range of 0–24 points and is the official ADHD-screening tool of the World Health Organization [16]. Both the English and Norwegian translations have internal consistency and convergent validity [3, 16, 17].
In our main analyses we employed the full ASRS as a predictor, whereas in the sensitivity analyses we used the ASRS-screener as a predictor.
The wender utah rating scale
The Wender Utah Rating Scale (WURS) retrospectively rates the frequency and severity of ADHD symptoms in childhood [18]. The WURS is based on the Utah criteria, which has a broader perspective on ADHD symptomatology than the DSM-4 criteria, including items addressing emotional regulation and conduct problems [19]. It originally included 61 items, but was condensed to the 25 items that best distinguished between cases and controls [18]. For this study we used the 25 item-version.
Participants responded to the 25 items on a Likert-type 5-point scale on a scale from 0 (not at all/very slightly) to 4 (very much), with a range of 0-100 points. Both the original English version and the Norwegian translation of the WURS have been shown to have greater diagnostic accuracy than the ASRS [3, 17].
Calculation of polygenic scores
Polygenic scores (PGSs) were calculated using summary statistics from the 2023 ADHD Working Group of the Psychiatric Genomics Consortium GWAS meta-analysis, with the Bergen sample excluded [5]. Genotypes and GWAS summary statistics underwent quality control (QC) as outlined in Choi et al. 2022, with the additional steps described by the QC protocol for PRS-CS [6, 20]. Variants with minor allele frequency greater than 0.01, less than 5% missingness and Hardy Weinberg equilibrium of p > 10− 10 were included in the analyses. The European reference panel from the 1000 Genomes Project and default settings were used to run PRS-CS [21]. Next, ADHD PGSs were calculated with the score function in PLINK, using weights generated by PRS-CS [5, 15, 20]. The scores were residualized on the first five principal components (PCs) and batch, and standardized.
Family history
To investigate the family history of ADHD, participants were asked whether they had first degree family members with a diagnosis of ADHD, with possible answers being “yes”, “no” and “uncertain”. Participants who responded with “uncertain” were coded as “no”, while participants with missing data were excluded from this sub-analysis.
Statistical analyses
Eight multivariable logistic regression models were constructed with ADHD diagnosis as the outcome and different combinations of WURS-score, ASRS-score, and ADHD PGS as predictors. The base model included sex and age as predictors.
Likelihood Ratio (LR) tests were performed for the hierarchical models with and without ADHD PGS, to investigate if the ADHD PGS contributed additional information alongside the rating scales. The entire nonhierarchical set of models was also compared by their Akaike Information Criterion (AIC) and Lee R2 to determine whether the PGS provided the models with better model fit and phenotypic variance explained [22, 23].
AIC compares nonhierarchical models by their model fit and number of predictors to select the optimal model which best describes the data [22]. It penalizes additional predictors and prioritizes simpler models if the difference in model fit between simple and complex models is small. We used the AIC corrected for small sample sizes (AICc) [22].
The Lee R2 is a better coefficient of determination for genetic profile analysis with binary outcomes than pseudo-R2 measures based on the likelihood function, as these do not give appropriate interpretations when measuring goodness-of-fit of linear predictors of models on the scale of liability [23,24,25]. We elected to calculate the weighted R2 on the logit liability scale with a population prevalence of 2.58% [26].
As the ASRS screener is commonly used to screen for ADHD, we wanted to investigate whether the ADHD PGS contributed additional information to the ASRS-screener. We therefore repeated the analyses with the ASRS screener score as a predictor in a supplementary analysis.
In clinical interviews, patients are routinely asked for family history of ADHD, which captures some genetic liability for ADHD, and we wanted to investigate whether the ADHD PGS contributed additional information to self-reported ADHD family history. We therefore repeated the analyses with self-reported ADHD family history as a covariate as a supplementary analysis.
We also performed sensitivity analyses to investigate whether the ADHD PGS was associated with the other predictors of interest. For these analyses, we constructed three linear regression models with ASRS-score, ASRS screener-score and WURS-score as continuous outcomes with the ADHD PGS as predictor and a logistic regression model with ADHD family history as a binary outcome, with the ADHD PGS as a predictor. Sex and age were included as covariates in all models.
Analyses were conducted in GenomeStudio and R version 4.3.0 [27]. The AICcmodavg package was used to perform the AIC analysis, and the lmtest package was used to perform LR tests [28, 29]. An R Markdown document with the code used in this analysis can be found in Additional File 1.
Results
The sample included 576 cases (51.2% female) and 530 controls (61.9% female), for a total sample size of 1106 participants (56.3% female). Demographic and clinical information for this sample is presented in Table 1. The control sample contained significantly more females than the case sample, and ADHD cases were significantly older than the controls (Table 1). Mean ASRS score, WURS score, and ADHD PGS Z-score were significantly higher in the ADHD group (Table 1).
For a more detailed table of clinical information in men and women, and in those with and without family history of ADHD, see Table S1 and Table S2 respectively in Additional File 2.
Likelihood ratio test
When testing each nested pair of models with and without ADHD PGS using LR tests, we found that the PGS contributed significantly better model fit to the base model (p < 0.0001), the ASRS-only model (p = 0.0381), the WURS-only model (p = 0.0048), and the full model (p = 0.0103). The results of the LR tests for all nested pairs of models are presented in Table 2.
The ADHD PGS also provided significantly better model fit to the ASRS-screener-model (p = 0.016), see Table S3 in Additional file 2. When self-reported ADHD family history was included in the models, we found that the PGS contributed significantly better model fit to all models, except for the ASRS only model (as well as the ASRS-screener model as assessed in the sensitivity analyses).
For the full results of likelihood ratio tests when family history of ADHD was included in the base model see Table S4 in Additional file 2.
Akaike information criterion
When comparing the AICc of the different models, we found that the models that included the ADHD PGS had better model fit compared to the corresponding models without the ADHD PGS. For the full list of AICc, see Table 3. For a comparison of each pair of hierarchical models with and without PGS, see Tables S5, S6, S7 and S8 in the Additional File 2.
The ADHD PGS also contributed with better model fit to the ASRS screener (ΔAICc = 3.78), as can be seen in Table S9 in Additional file 2. When including family history in the models, we found that inclusion of the PGS only gave a better model fit compared to an examination of family history (ΔAICc = 10.02) and the WURS-only model (ΔAICc = 2.45). For the full results of AICc analyses when family history was included in the base model, see Table S10 in Additional File 2.
Lee R2
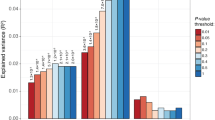
We found that the ADHD PGS increased the Lee R2 of all the models. The model with the highest R2 was the model that included the ADHD PGS and both rating scales with an R2 of 81.402%. The PGS increased the R2 of the base model by 1.518% points (pp), of the ASRS model by 0.577pp, of the WURS model by 0.610pp, and of both rating scales together by 0.565pp. See Table 4 for the full list of Lee R2.
We found that the ADHD PGS increased the variance explained of the ASRS screener model by 0.662pp, as seen in Table S11 in Additional file 2. Inclusion of family history of ADHD in the models attenuated the PGS’ contribution to all the diagnostic aids, with the PGS contributing 1.395pp to the base model. For the full list of R2 by different models when family history was included, see Table S12 in Additional file 2.
Sensitivity analyses
In the sensitivity analyses of the ADHD PGS’ association with the predictors of interest, we found that the ADHD PGS was significantly associated with ASRS (p < 0.001), ASRS-screener (p < 0.001), WURS (p < 0.001), and self-reported family history of ADHD (p = 0.039). For the full summary of the sensitivity analyses, see Table S13 in Additional file 2.
Discussion
Here we aimed to investigate whether an ADHD PGS could provide additional information to commonly used diagnostic aids of ADHD in distinguishing between individuals with and without ADHD. We found that the ADHD PGS contributed with additional information to self-report rating scales and family history in a clinically representative sample of adults diagnosed with ADHD. However, the PGS’ contribution to variance explained was low, suggesting that its clinical utility in diagnostics remains limited.
We also found that the WURS performed better than the ASRS, as measured by R2 and AICc, as has previously been reported [3, 17]. This may be because the WURS is addressing a broader range of ADHD symptoms than ASRS.
To our knowledge, this is the first study examining the contribution of the ADHD PGS to commonly used diagnostic aids for the purpose of distinguishing between individuals with and without ADHD. Previous studies have found that ADHD PGS is associated with ADHD diagnosis in adults and children, without investigating the PGS’ potential in diagnostics alongside other diagnostic tools [30, 31]. Evidence from psychiatric genetics suggests that familial risk for psychopathology and PGS for psychiatric conditions capture slightly different genetic domains and have unique predictive powers [32]. Our findings support this, as the ADHD PGS provided supplemental information to self-reported family history of ADHD in distinguishing between cases and controls. However, our findings suggest that an interrogation of family history provides more information to identify individuals with ADHD than the ADHD PGS currently does.
While our findings suggest that the current ADHD PGS is too imprecise to have practical utility in routine diagnostics, it may be useful in predicting ADHD in combination with other screening tools. PGSs for other conditions have been used alongside other information in prediction models, such as for prediction of coronary artery disease, type 2 diabetes, and depression onset in Alzheimer’s disease [33,34,35]. Such models demonstrate that a PGS can provide supplementary information to other clinical instruments and biomarkers, resulting in improved prediction accuracy. In addition to being used in diagnostics, a PGS could potentially be a prognostic tool and to explore genetic liability of treatment response in psychiatric disorders [36].
Prediction models have also been developed for ADHD, employing other known risk factors such as depressive symptoms, socio-economic status, and prematurity [37, 38]. One recent study aimed to include the ADHD PGS in a prediction model of ADHD in adults and found that it increased the variance explained, without significantly improving prediction [38]. However, this PGS was based on the 2019 ADHD GWAS meta-analysis, which is less accurate than the 2023 ADHD GWAS meta-analysis used in our study [5, 38, 39]. Another recent study on the prediction of the developmental trajectory of ADHD in children found that the ADHD PGS provided information independent of other ADHD risk factors (e.g. low parental education and low birth weight) [40]. While our findings show that the ADHD PGS is limited in how much additional variance it can explain alongside commonly employed diagnostic aids, it may be more useful to investigate its utility in prediction models of ADHD alongside other risk factors, such as family environment and maternal smoking during pregnancy [7, 40,41,42]. Notably, all of these established risk factors have a polygenic genetic risk component that partially overlaps with ADHD genetic risk [5, 43, 44]. Future studies should investigate the ADHD PGS’ contribution to prediction models of ADHD using multiple sources of information.
Our findings must be understood in the context of certain limitations. Firstly, our sample included only Norwegians, and our results may not be generalizable to other ancestries or clinical contexts. Secondly, our participants were adults, with all cases being diagnosed with persistent, childhood onset ADHD and there were no exclusion criteria. Although children and adults with ADHD share many common genetic risk variants, the results may not be generalizable to children or adolescents, and comorbidities among the patients may have affected the association of the ADHD PGS with our ADHD diagnosis outcome [45]. However, a strength of this sample is that it consists of real-life ADHD patients, who often have diverse comorbidities [46].
Thirdly, we contrasted the utility of the PGS with the utility of the ASRS and WURS, which are useful aids in the diagnosis of ADHD, but are not necessary or sufficient to diagnose ADHD. Additionally, both the ASRS and WURS have been demonstrated to have factor structures that are more accurate in discriminating between ADHD and controls. However, in this study we decided not to use these factor structures, as the full scores are more representative of how these tools are commonly used in the clinic [16,17,18, 47, 48]. Finally, our study was not designed to test the utility of the ADHD PGS in a clinical diagnostic setting. However, since our results indicate only a small contribution to total variance explained, it is reasonable to believe that the ADHD PGS does not currently have clinical utility in diagnostics, despite its statistical significance.
Conclusions
We found that the ADHD PGS contributed with additional information to commonly used self-reported clinical rating scales and self-reported family history of ADHD in distinguishing between ADHD cases and controls. However, the increase in variance explained was small and the current ADHD PGS is unlikely to have diagnostic value compared to well-established rating scales. Still, the ADHD PGS could prove useful in prediction models in combination with other types of information. Future studies should examine the utility of ADHD PGS in prediction of ADHD, and the diagnostic utility of ADHD PGS should be continually investigated as larger ADHD GWAS meta-analyses are published and new computational tools are developed.
Data availability
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- ASRS:
-
Adult ADHD Self-Report Scale
- AIC:
-
Akaike information criterion
- AICc:
-
Akaike information criterion corrected for small sample sizes
- ADHD:
-
Attention-deficit/hyperactivity disorder
- DSM-4:
-
Diagnostic and Statistical Manual of Mental Disorders 4th edition
- GWAS:
-
Genome-Wide Association Study
- LR:
-
Likelihood Ratio
- Pp:
-
Percentage Points
- PGS:
-
Polygenic Score
- QC:
-
Quality control
- WURS:
-
Wender Utah Rating Scale
References
Haavik J, Halmøy A, Lundervold AJ, Fasmer OB. Clinical assessment and diagnosis of adults with attention-deficit/hyperactivity disorder. Expert Rev Neurother. 2010;10(10):1569–80.
Leffa DT, Caye A, Rohde LA. ADHD in children and adults: diagnosis and prognosis. Springer International Publishing; 2022. pp. 1–18.
Rösler M, Retz W, Thome J, Schneider M, Stieglitz RD, Falkai* P. Psychopathological rating scales for diagnostic use in adults with attention-deficit/hyperactivity disorder (ADHD). Eur Arch Psychiatry Clin Neuro Sci. 2006;256(S1):i3–11.
Taylor MJ, Martin J, Butwicka A, Lichtenstein P, D’Onofrio B, Lundström S et al. A twin study of genetic and environmental contributions to attention-deficit/hyperactivity disorder over time. J Child Psychol Psychiatry. 2023.
Demontis D, Walters GB, Athanasiadis G, Walters R, Therrien K, Nielsen TT et al. Genome-wide analyses of ADHD identify 27 risk loci, refine the genetic architecture and implicate several cognitive domains. Nat Genet. 2023.
Choi SW, Mak TS-H, O’Reilly PF. Tutorial: a guide to performing polygenic risk score analyses. Nat Protoc. 2020;15(9):2759–72.
Lewis CM, Vassos E. Polygenic risk scores: from research tools to clinical instruments. Genome Med. 2020;12(1).
Lambert SA, Abraham G, Inouye M. Towards clinical utility of polygenic risk scores. Hum Mol Genet. 2019;28(R2):R133–42.
Torkamani A, Wineinger NE, Topol EJ. The personal and clinical utility of polygenic risk scores. Nat Rev Genet. 2018;19(9):581–90.
Ronald A, De Bode N, Polderman TJC. Systematic review: how the Attention-Deficit/Hyperactivity disorder polygenic risk score adds to our understanding of ADHD and Associated traits. J Am Acad Child Adolesc Psychiatry. 2021;60(10):1234–77.
Johansson S, Halleland H, Halmøy A, Jacobsen KK, Landaas ET, Dramsdahl M, et al. Genetic analyses of dopamine related genes in adult ADHD patients suggest an association with the DRD5-microsatellite repeat, but not with DRD4 or SLC6A3 VNTRs. Am J Med Genet Part B: Neuropsychiatric Genet. 2008;147B(8):1470–5.
Irgens LM. The Medical Birth Registry of Norway. Epidemiological research and surveillance throughout 30 years. Acta Obstet Gynecol Scand. 2000;79(6):435–9.
GenomeStudio S. [ https://emea.illumina.com/techniques/microarrays/array-data-analysis-experimental-design/genomestudio.html.
Lam M, Awasthi S, Watson HJ, Goldstein J, Panagiotaropoulou G, Trubetskoy V, et al. RICOPILI: Rapid Imputation for COnsortias PIpeLIne. Bioinformatics. 2020;36(3):930–3.
Purcell S, Neale B, Todd-Brown K, Thomas L, Ferreira MAR, Bender D, et al. PLINK: a Tool Set for whole-genome Association and Population-based linkage analyses. Am J Hum Genet. 2007;81(3):559–75.
Kessler RC, Adler L, Ames M, Demler O, Faraone S, Hiripi E, et al. The World Health Organization adult ADHD self-report scale (ASRS): a short screening scale for use in the general population. Psychol Med. 2005;35(2):245–56.
Brevik EJ, Lundervold AJ, Haavik J, Posserud MB. Validity and accuracy of the adult Attention-Deficit/Hyperactivity disorder (ADHD) self‐report scale (ASRS) and the Wender Utah rating scale (WURS) symptom checklists in discriminating between adults with and without ADHD. Brain Behav. 2020;10(6):e01605.
Ward MF, Wender PH, Reimherr FW. The Wender Utah rating scale: an aid in the retrospective diagnosis of childhood attention deficit hyperactivity disorder. Am J Psychiatry. 1993;150(6):885–90.
Wender PH. Attention-deficit hyperactivity disorder in adults. New York, NY: Oxford University Press; 1995.
Ge T, Chen C-Y, Ni Y, Feng Y-CA, Smoller JW. Polygenic prediction via bayesian regression and continuous shrinkage priors. Nat Commun. 2019;10(1).
Fairley S, Lowy-Gallego E, Perry E, Flicek P. The International Genome Sample Resource (IGSR) collection of open human genomic variation resources. Nucleic Acids Res. 2019;48(D1):D941–7.
Cavanaugh JE, Neath AA. The Akaike information criterion: background, derivation, properties, application, interpretation, and refinements. WIRE Comput Stat. 2019;11(3):e1460.
Lee SH, Goddard ME, Wray NR, Visscher PM. A Better Coefficient of Determination for Genetic Profile Analysis. Genet Epidemiol. 2012;36(3):214–24.
Nagelkerke NJ. A note on a general definition of the coefficient of determination. Biometrika. 1991;78(3):691–2.
Cox DR. Analysis of binary data. Routledge; 2018.
Song P, Zha M, Yang Q, Zhang Y, Li X, Rudan I. The prevalence of adult attention-deficit hyperactivity disorder: a global systematic review and meta-analysis. J Glob Health. 2021;11:04009.
Team RC. R: a Language and Environment for Statistical Computing. R Foundation for Statistical Computing; 2022.
Mazerolle MJ, Mazerolle MMJ. Package ‘AICcmodavg’. R Package. 2017;281.
Zeileis A, Hothorn T. Diagnostic checking in regression relationships: na; 2002.
Jansen AG, Dieleman GC, Jansen PR, Verhulst FC, Posthuma D, Polderman TJC. Psychiatric Polygenic Risk scores as Predictor for attention Deficit/Hyperactivity Disorder and Autism Spectrum Disorder in a clinical child and adolescent sample. Behav Genet. 2020;50(4):203–12.
Hermosillo RJM, Mooney MA, Fezcko E, Earl E, Marr M, Sturgeon D, et al. Polygenic risk score-derived subcortical connectivity mediates Attention-Deficit/Hyperactivity disorder diagnosis. Biol Psychiatry Cogn Neurosci Neuroimaging. 2020;5(3):330–41.
Loughnan RJ, Palmer CE, Makowski C, Thompson WK, Barch DM, Jernigan TL, et al. Unique prediction of developmental psychopathology from genetic and familial risk. J Child Psychol Psychiatry. 2022;63(12):1631–43.
Läll K, Mägi R, Morris A, Metspalu A, Fischer K. Personalized risk prediction for type 2 diabetes: the potential of genetic risk scores. Genet Sci. 2017;19(3):322–9.
Upadhya S, Liu H, Luo S, Lutz MW, Chiba-Falek O. Polygenic risk score effectively predicts Depression Onset in Alzheimer’s Disease based on major depressive disorder risk variants. Front Neurosci. 2022;16:827447.
Abraham G, Havulinna AS, Bhalala OG, Byars SG, De Livera AM, Yetukuri L, et al. Genomic prediction of coronary heart disease. Eur Heart J. 2016;37(43):3267–78.
Meerman JJ, Ter Hark SE, Janzing JGE, Coenen MJH. The potential of polygenic risk scores to predict antidepressant treatment response in Major Depression: a systematic review. J Affect Disord. 2022;304:1–11.
Caye A, Agnew-Blais J, Arseneault L, Gonçalves H, Kieling C, Langley K et al. A risk calculator to predict adult attention-deficit/hyperactivity disorder: generation and external validation in three birth cohorts and one clinical sample. Epidemiol Psychiatric Sci. 2020;29.
Lorenzi CH, Teixeira Leffa D, Bressan R, Belangero S, Gadelha A, Santoro ML, et al. Replication of a predictive model for youth < scp > ADHD in an independent sample from a developing country. J Child Psychol Psychiatry. 2023;64(1):167–74.
Demontis D, Walters RK, Martin J, Mattheisen M, Als TD, Agerbo E, et al. Discovery of the first genome-wide significant risk loci for attention deficit/hyperactivity disorder. Nat Genet. 2019;51(1):63–75.
Brikell I, Wimberley T, Albiñana C, Vilhjálmsson BJ, Agerbo E, Børglum AD, et al. Interplay of ADHD polygenic liability with Birth-Related, somatic, and psychosocial factors in ADHD: a Nationwide Study. Am J Psychiatry. 2023;180(1):73–88.
He Y, Chen J, Zhu LH, Hua LL, Ke FF. Maternal smoking during pregnancy and ADHD: results from a systematic review and Meta-analysis of prospective cohort studies. J Atten Disord. 2020;24(12):1637–47.
Claussen AH, Holbrook JR, Hutchins HJ, Robinson LR, Bloomfield J, Meng L et al. All in the family? A systematic review and Meta-analysis of parenting and family environment as risk factors for Attention-Deficit/Hyperactivity disorder (ADHD) in children. Prev Sci. 2022.
Shadrin AA, Smeland OB, Zayats T, Schork AJ, Frei O, Bettella F, et al. Novel loci Associated with Attention-Deficit/Hyperactivity disorder are revealed by leveraging Polygenic Overlap with Educational Attainment. J Am Acad Child Adolesc Psychiatry. 2018;57(2):86–95.
Franke B, Michelini G, Asherson P, Banaschewski T, Bilbow A, Buitelaar JK, et al. Live fast, die young? A review on the developmental trajectories of ADHD across the lifespan. Eur Neuropsychopharmacol. 2018;28(10):1059–88.
Rovira P, Demontis D, Sánchez-Mora C, Zayats T, Klein M, Mota NR, et al. Shared genetic background between children and adults with attention deficit/hyperactivity disorder. Neuropsychopharmacology. 2020;45(10):1617–26.
Katzman MA, Bilkey TS, Chokka PR, Fallu A, Klassen LJ. Adult ADHD and comorbid disorders: clinical implications of a dimensional approach. BMC Psychiatry. 2017;17(1).
Kouros I, Hörberg N, Ekselius L, Ramklint M. Wender Utah rating Scale-25 (WURS-25): psychometric properties and diagnostic accuracy of the Swedish translation. Ups J Med Sci. 2018;123(4):230–6.
Adler LA, Spencer T, Faraone SV, Kessler RC, Howes MJ, Biederman J, Secnik K. Validity of pilot adult ADHD self- report scale (ASRS) to rate adult ADHD symptoms. Ann Clin Psychiatry. 2006;18(3):145–8.
Acknowledgements
The authors would like to thank Dr. Tetyana Zayats for her contribution to the study design and assistance with the statistical analysis, and Dr. Ditte Demontis for supplying GWAS summary statistics without sample overlap.
Funding
This work was supported by grants from Stiftelsen Kristian Gerhard Jebsen (SKGJ-MED-02), The Regional Health Authority of Western Norway (912264), The Research Council of Norway (Project 331725), the European Union’s Horizon 2020 research and innovation program and The Norwegian ADHD Research Network (Project 51379).
Open access funding provided by University of Bergen.
Author information
Authors and Affiliations
Contributions
A.H. and J.H. conceptualized the study. A.H. designed the study, conducted data management and statistical analyses, and wrote the main manuscript text. All authors contributed to the interpretation of the results, provided intellectual contributions, drafted the manuscript, and approved the final version of the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The Norwegian Regional Committee for Medical and Health Research Ethics approved the study, REC West [IRB #3 (FWA00009490, IRB00001872)]. Participants provided signed informed consent.
Consent for publication
Not applicable.
Competing interests
BSS and JH have received honoraria as part of medical education programs sponsored by Takeda and Medice, all outside the submitted work. TAH and AH declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Høberg, A., Solberg, B.S., Hegvik, TA. et al. Using polygenic scores in combination with symptom rating scales to identify attention-deficit/hyperactivity disorder. BMC Psychiatry 24, 471 (2024). https://doi.org/10.1186/s12888-024-05925-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12888-024-05925-7