
Abstract
Background
Psychiatric patients are susceptible to adverse mental health impacts during COVID-19, but complex interplays between psychopathology and pandemic-related variables remain elusive. This study aimed to investigate concomitant associations between psychopathological symptoms, psychological measures and COVID-19 related variables in Chinese psychiatric patients during the peak of fifth pandemic wave in Hong Kong.
Methods
We employed network analysis to investigate inter-relationships among psychopathological symptoms (including depression, anxiety, post-traumatic stress disorder-like [PTSD-like] symptoms, insomnia, psychotic symptoms), cognitive complaints, health-related quality of life, loneliness, resilience and selected pandemic-related factors in 415 psychiatric outpatients between 28 March and 8 April, 2022. Network comparisons between genders, diagnosis (common mental disorders [CMD] vs. severe mental disorders [SMD]), and history of contracting COVID-19 at fifth wave were performed as exploratory analyses.
Results
Our results showed that anxiety represented the most central node in the network, as indicated by its highest node strength and expected influence, followed by depression and quality of life. Three comparatively strong connections between COVID-19 and psychopathological variables were observed including: fear of contagion and PTSD-like symptoms, COVID-19 stressor burden and PTSD-like symptoms, and COVID-19 stressor burden and insomnia. Network comparison tests revealed significant network structural difference between participants with history of contracting COVID-19 and those without, but showed no significant difference between genders as well as between CMD and SMD patients.
Conclusions
Our findings suggest the pivotal role of anxiety in psychopathology network of psychiatric patients amidst COVID-19. Pandemic-related variables are critically associated with trauma/stress and insomnia symptoms. Future research is required to elucidate potential network structural changes between pandemic and post-COVID periods.
Similar content being viewed by others


Introduction
Literature has consistently shown the adverse effect of COVID-19 on individuals’ physical and mental health. Despite imposing public-health policies to contain the spread of COVID-19, the emergence of the Omicron-variant had led to the fifth pandemic wave in Hong Kong (HK) in 2022. It was the most severe outbreak of COVID-19 in HK, resulting in an estimated 60% of the population (approximately 4.4 million) having contracted the infection, with 3.73 deaths per thousand, the highest death rate worldwide at the time [1, 2]. People with pre-existing mental illness constitutes a vulnerable population during the pandemic, as they have higher risk of COVID-19 infection [3, 4] and related mortality [5], and experienced more pronounced psychological distress relative to the general population [6,7,8]. Notably, the complex interplay between psychopathological symptoms and pandemic-related variables among psychiatric patients are understudied and remain to be clarified. In this study, we employed network analysis to address this important question in the context of the fifth wave of COVID-19 in HK.
Network analysis approach conceptualizes psychopathology as a result of a complex, dynamic system of interconnections between symptoms [9], as opposed to previous notion of underlying common latent cause [10]. This method allows visualization of associations between variables in the form of a network while estimating relative importance of variables within the network. The resultant information not only facilitates identification of important variables in contributing to the genesis of psychopathology, but also variables that bridge between different psychopathologies [9]. In fact, network analysis has been increasingly applied to examine psychopathological network in the general population during COVID-19. For instance, a recent network-analytic study found that anxiety/fear about COVID-19 linked significantly with depression and anxiety symptoms [11]. Another report revealed depression as the most central node in the network during a lockdown period [12]. Relatively fewer network-analytic research has been conducted on psychiatric patients during the pandemic, and accumulating data have demonstrated strong connections between depression and anxiety symptoms [13, 14]. Longitudinal data and more recent cross-sectional research using data in the pandemic showed that anxiety had emerged as the core psychopathological symptom during the pandemic [15,16,17], and anxiety and COVID-19 related worries were significantly associated with other symptoms such as suicidal ideation in the network of clinical psychopathology [16, 18]. Nonetheless, these studies primarily focused on the associations among psychopathological items within one or two symptom scales, without taking into consideration potential influence of COVID-19 specific factors such as fear of contagion, pandemic-related stressors, distress due to social-distancing measures, to name a few. There is a paucity of network-analytic studies evaluating relationships across a more comprehensive array of psychopathological variables among individuals with mental disorders.
To this end, the current study employed a network analysis approach to investigate complex inter-relationships between psychopathological symptoms, psychological measures of resilience and loneliness, cognitive complaints, health-related quality-of-life, and COVID-19 related factors in a representative sample of Chinese psychiatric outpatients during the peak of fifth pandemic wave in Hong Kong (HK). Specifically, we aimed to: (1) examine the associations among the aforementioned array of variables, particularly those linked to COVID-19 related factors; (2) identify the most central variable in the network and clarify its associations with other variables; and (3) compare network difference between genders, diagnosis (common vs. severe mental disorders) and history of contracting COVID-19 infection.
Methods
Participants and setting
A total of 415 Chinese psychiatric patients aged 18–64 years were recruited from psychiatric outpatient clinics in HK West Cluster, a catchment area with a population of approximately 550,000, between 28 March and 8 April, 2022 (i.e., during the peak of the fifth COVID-19 wave in HK). Patients with learning disabilities, history of head trauma or neurological disease, or were unable to read Chinese language were excluded. Psychiatric diagnosis was based on ICD10 criteria and was ascertained by reviewing medical-records in public psychiatric services. Participants were further categorized into those with common-mental-disorders (CMD, including depressive and anxiety disorders) and severe-mental-disorders (SMD, including schizophrenia-spectrum disorders and bipolar disorder). The study was performed in accordance with the Declaration of Helsinki, and was approved by the local institutional review board (UW 22–202). Written informed consent was obtained from all participants before study assessment.
Study assessment
Self-rated questionnaire was administered in this cross-sectional study. Psychopathological symptom assessment included the following: Depressive and anxiety symptom severity were measured by Patient Health Questionnaire-9 (PHQ-9) [19] and Generalized Anxiety Disorder-7 scale (GAD-7) [20], respectively, with both scales using a 4-point Likert scale ranging from 0 (never) to 3 (nearly every day). Total score for depression ranged 0–27, whereas that for anxiety ranged 0–21. A modified version of Impact of Event Scale-Revised (IES-R) [21] specific to COVID-19 was administered to measure PTSD-like symptoms on a 5-point Likert scale (0 [never] to 4 [always]), with total score ranged 0–24. Insomnia symptoms were assessed using Insomnia Severity Index (ISI) [22]. Positive symptom subdomain items (4 items) of 15-item Community Assessment of Psychic Experiences Scale–Chinese version (CAPE-C15) [23] was employed to assess positive psychotic symptoms. Patients rated their symptom frequency on a 4-point Likert scale (1 [never] to 4 [nearly always]). For all symptom scales, higher scores indicated greater symptom severity. Cognitive impairment was measured by a self-report questionnaire, adapted from Cognitive Complaints in Bipolar Disorder Rating Assessment (COBRA) [24], which has been applied in a recent study on psychiatric patients during COVID-19 [25]. This adapted questionnaire comprised 5 items reflecting cognitive complaints manifested in everyday scenario including attention, processing speed, memory, learning and executive function (rated on frequency of cognitive complaints on a 4-point Likert scale, ranging from 0 [never] to 3 [nearly every day]) [25]. Health-related quality-of-life was assessed using the 8-item Short-Form Health Survey (SF-8) [26], with higher scores indicating better quality-of-life (item 1 score was reversed). We measured two psychological measures, namely loneliness and resilience. Loneliness was assessed by the UCLA 3-item Loneliness Scale [27] on a 3-point Likert scale (1 [hardly ever] to 3 [often]), with higher scores indicating greater loneliness. Resilience was assessed using the Brief Resilience Scale (BRS) [28] on a 5-point Likert scale (1 [strongly disagree] to 5 [strongly agree]), with higher scores indicating greater resilience. Selected COVID-19 related factors were evaluated, comprising history of contracting COVID-19 during fifth wave, fear of contagion, number of pandemic-related stressors and distress due to social-distancing measures. Details of COVID-19 related factors are summarized in Table 1.
Statistical analysis
Network analysis was performed including network estimation and network comparison tests, derivation of centrality indices, and evaluation of network stability and accuracy. All variables were standardized by centring before inclusion in network analysis. All statistical analyses were conducted using R4.2.2.
Network estimation
A total of 12 variables were included in network analysis. Each variable was represented by a node, whereas the associations between variables were represented by edges. The model was estimated using the bootnet R-package. ‘EBICglasso’ default set was called for network modelling. This model selection estimated the network using graphical Least-Absolute-Shrinkage-and-Selection-Operator (LASSO) and selected the optimal model using Extended Bayesian Information Criteria (EBIC), with the hyperparameter set as 0.5 [29]. Graphical LASSO minimised false-positive associations by assigning penalties to shrink weak association to exact zero, resulting in a less dense network for easier interpretation [30]. Correlation coefficients, also known as edge-weights, ranged from − 1 to 1 were also generated from network analysis. They indicated both the strength and direction of association between two nodes after controlling for all other information. Network structure was plotted using the Fruchterman-Reingold algorithm from the qgraph R-package. Exploratory analyses were conducted to compare the overall network structure and global strength between genders, diagnosis (CMD vs. SMD) and history of contracting COVID-19 infection at fifth wave (yes vs. no). Comparisons were made using the NetworkComparisonTest R-package, a resampling-based permutation test that assesses differences between two networks [31].
Centrality indices
Four centrality indices were computed: Node strength quantifies how well a node is connected to others directly by summing the edge-weights connected to the node; Closeness measures the indirect connection a node has with others, reflected by the inverse of the sum of the shortest paths from a node to all other nodes; Betweenness refers to the number of times a node lies on the shortest paths between two other nodes; and Expected influence reflects the level of connectivity of a given node with other nodes in the network. All indices were calculated and visualized using the qgraph package in R. Predictability estimates were also computed for all nodes in the network. The estimates reflect how well each node is predicted by other nodes in the network [32] and are represented as pie charts around each node.
Network stability and accuracy
To examine network stability and accuracy, bootstrapping was applied to assess centrality and edge-weight parameters using the bootnet R-package. It was first applied to evaluate the stability of centrality indices by case-dropping. The indices were repeatedly calculated with different subsets of data that consisted of different proportions of data dropped. Stability was evaluated by the correlation stability coefficient (CS-coefficient), which is the maximum proportion of cases that could be dropped with a 95% certainty. A CS-coefficient above 0.5 indicates good stability [33]. Second, edge-weight accuracy was assessed by calculating their confidence intervals derived from 1000 non-parametric bootstrap samples. Third, bootstrapped differences tests were conducted to test for significant differences in edge-weights and node strengths using a set of 1000 bootstrapped sample.
Results
Characteristics of the sample
In our sample, 144 (34.7%) were male, the mean age was 40.6 years old (SD = 12.6), and 236 (56.9%) achieved secondary educational level or below. Two-hundred forty-six (59.3%) patients were diagnosed with CMD, and 169 (40.7%) with SMD. Detailed characteristics of the sample are summarized in Table 2.
Network structure and analyses
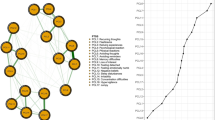
The resulting network model illustrated all nodes were interconnected across domains (Fig. 1). Nodes from COVID-19 related factors and psychological measures were overall highly interconnected within domain, compared to nodes from other domains. Within psychopathological symptom domain, depression and anxiety were strongly associated (r = 0.52), followed by the association between anxiety and PTSD-like symptoms (r = 0.32), and the link between depression and insomnia (r = 0.14). Notably, interconnection across domains were observed in all psychopathological symptom nodes except anxiety. For example, depression was correlated to subjective cognitive impairment (r = 0.20), PTSD-like symptoms were associated with cognitive impairment (r = 0.17), fear of contagion (r = 0.20) and number of stressors experienced (r = 0.14) in COVID-19 related domain, while positive symptoms were connected with cognitive impairment (r = 0.13) and loneliness (r = 0.16). Quality-of-life also showed connections with several domains. It was negatively associated with insomnia (r=-0.22) and s cognitive impairment (r=-0.22), and was moderately correlated with resilience (r = 0.21). Lastly, number of COVID-19 stressors was associated with insomnia (r = 0.16), while distress due to social-distancing measures was negatively correlated to resilience (r=-0.18) (Fig. 1).

Network of psychopathological symptom, cognition, quality of life, psychological, and COVID-related variables. This is a network structure of 12 study variables. Each node represents a study variable and each edge represents a significant association between two nodes. Edge thickness reflects the magnitude of the association, in which thicker lines denote stronger associations. Blue lines indicate positive association while red lines denote negative association. Predictability estimates are represented by the circle around each node
As shown in Fig. 2, centrality analyses revealed that anxiety showed the highest node strength, followed by depression and quality-of-life. Anxiety also had the highest expected influence value, and ranked second for the degrees of closeness and betweenness among all variables in the network. In COVID-19 related domain, the number of COVID-19 stressors experienced demonstrated the highest centrality, with the highest node strength, closeness, betweenness and expected influence among three COVID-19 related variables. Depression and resilience showed the highest closeness and betweenness, respectively, among all variables in the network. For predictability, anxiety had the highest predictability (R2 = 0.78), followed by depression (R2 = 0.77). The mean predictability of the resulting network was 0.48 (SD = 0.19).

Centrality indices of study variables within the network. Centrality indices of node strength, closeness, betweenness and expected influence are shown as standard z-scores
Network comparison between patients with versus without history of contracting COVID-19 revealed significant difference in structural invariance (M = 0.39, p = 0.002), but not in global strength (S = 0.78, p = 0.053). Specifically, the networks of infected and non-infected groups differed markedly in the association between fear of contagion and distress due to social-distancing measures (Supplementary Fig. S1). These two variables were negatively related to each other in the network of infected patients (r=-0.31), but were positively associated with each other in the network of non-infected counterparts (r = 0.07). Alternatively, network comparisons showed no significant differences between genders as well as between CMD and SMD patients in structural (gender: M = 0.25, p = 0.228; diagnosis: M = 0.18, p = 0.836) and global strength invariance (gender: S = 0.47, p = 0.215; diagnosis: S = 0.11, p = 0.767). The corresponding network per gender and diagnosis are depicted in Supplementary Figure S2 and S3, respectively.
Network stability and accuracy
CS-coefficients for centrality indices were 0.75 for node strength and expected influence, 0.52 for closeness and 0.21 for betweenness. These indicated that the network had a good stability in node strength and closeness, whereas the index of betweenness should be interpreted with caution. Bootstrapped 95% CIs showed a narrow curve, suggesting reliable and accurate edge-weight estimates (Supplementary Fig. S4). Results from bootstrapped difference tests (Supplementary Fig. S5 and S6) revealed that most edge-weights and node strengths were statistically different from one another in the resulted network.
Discussion
To our knowledge, the current study is the first to employ network analysis to examine complex inter-relationships among a comprehensive range of variables encompassing various psychopathological symptoms, cognitive complaints, loneliness and resilience, health-related quality-of-life and pandemic-related factors among psychiatric patients during COVID-19. Our results demonstrated that psychopathological symptoms and COVID-19 related factors were both highly connected within and between domains. Among the variables studied, anxiety played the most central role and had the strongest associations with other nodes. This indicates that emergence of anxiety symptoms in pandemic may lead to subsequent development of other psychopathological symptoms such as depression, PTSD-like symptoms and insomnia, with consequent deterioration of quality-of-life.
Three direct associations between the COVID-19 related factor domain and psychopathological symptom domain were observed from the constructed network. Number of COVID-19 stressors experienced was positively associated with PTSD-like symptoms and insomnia, whereas fear of contagion was solely linked to PTSD-like symptoms. Of these three connections, the last between-domain connection was the strongest. In line with COVID-19 literature on traumatic stress, our findings provided evidence that the pandemic itself can be inferred as a traumatic stressor [34]. For instance, fear of contagion could be regarded as an example of mind-wandering, in which individuals exhibit to cope with their distress but with deleterious effect on cognitive functioning [35]. Subsequently, frequent mind-wandering leads to poorer functioning in everyday life [36]. Alternatively, fear of contagion and economic hardship can constitute as subtypes of traumatic stress in COVID-19, which was found to predict PTSD, anxiety and depression in the general population [37]. Moreover, shortage of medical resources and health emergency are risk factors of developing PTSD-like symptoms during COVID-19 among healthcare professionals (HP) [38]. Although it could be argued that general population and psychiatric patients would be less likely to experience the same intensity of psychological distress compared to frontline HP at the COVID-19 outbreak, the aforementioned risk factors are still applicable to the former two groups. Indeed, studies conducted in HK at earlier pandemic stage indicated that worries of insufficient medical supplies and fear of contagion were associated with poorer mental-health outcomes [39, 40]. These suggest that COVID-19 may exert an indirect effect on individuals’ psychological distress by acting as continuous traumatic stressors in the fifth pandemic wave. Given their heightened susceptibility to stress, stronger associations between COVID-19 related factors and psychopathological symptoms may be more likely to emerge among psychiatric patients.
The COVID-19 stressor burden was also found to directly link with insomnia symptoms. Such relationship largely concurs with the literature on sleep research, including both conducted before and during the pandemic. According to the classic model of neuroendocrine stress response, exposure to stress activates the hypothalamic-pituitary-adrenal axis to release stress hormones, which subsequently modulate various physiological functions, including one’s sleep-wake cycle [41]. Prior studies have consistently reported higher prevalence of concomitant stress and insomnia symptoms experienced during the pandemic across different populations, such as general population, HP and psychiatric patients [42, 43]. Besides, a recent study demonstrated a longitudinal effect of increased stress on later perceived sleep disturbance during COVID-19 regardless of pre-existing sleep abnormalities [44]. This indicates a continuous effect of stress on individuals’ perceived sleep quality during the pandemic, in which sleep disturbance was positively associated with psychological distress [45]. Given the increased prevalence of sleep disturbance during pandemic [46] and its negative effect on quality-of-life, presentation of insomnia during pandemic should warrant attention and timely intervention is needed to minimize its adverse mental-health impacts.
Our exploratory analyses suggested network structural difference between psychiatric patients with versus without history of contracting COVID-19 during the fifth pandemic wave. Intriguingly, the resulting networks of infected and non-infected psychiatric patients differed markedly in the association between fear of contagion and distress due to social-distancing measures. These two variables were negatively related to each other among infected individuals but were positively associated with each other in non-infected counterparts. We speculate that such opposite directions of associations might partly be explained by potential differential psychological reaction toward COVID-19 between infected and non-infected individuals. A recent study indicated that individuals’ excessive fear reaction toward COVID-19 (or termed over-responses) was associated with heightened distress by self-isolation during the pandemic (e.g., social-distancing measures), whereas low fear reaction toward COVID-19 (or termed under-responses) was linked with increased tendency to disregard the social-distancing measures [47]. It might be possible that individuals with history of contracting COVID-19 (and recovered from the infection) perceived themselves as having low risk of infection, and hence exhibited under-responses toward COVID-19 with reduced fear of contagion compared to non-infected individuals. Consequently, participants in the infected group may experience greater distress due to social-distancing measures in the context of their diminished perceived threat against COVID-19. Nonetheless, owing to the scarcity of data examining network structural difference in relation to the history of COVID-19 infection, further investigation is required to verify our network comparison findings.
Anxiety symptoms and COVID-19 stressor burden play critical roles in leading to subsequent development of other psychopathological symptoms such as depression and insomnia. Future studies hence might consider to develop and evaluate effectiveness of interventions that target at reducing intensity of anxiety and stress level in different facets of daily life during pandemic so as to enhance the mental health and quality of life of psychiatric patients. For instance, a randomized controlled trial revealed that regular layperson-delivered telephone calls with empathetic conversational techniques could reduce anxiety, depression and loneliness, improving the general mental health during pandemic [48]). Another clinical trial showed that a single session of virtual reality with content to promote relaxation, distraction and stress relief demonstrated beneficial effect on reducing tiredness, shortness of breath, and anxiety, with an increase in the feeling of well-being during the pandemic [49]. Research like these ones can be extended to psychiatric patients to evaluate and maximize their clinical relevance.
There are several study limitations that warrant attention. First, the cross-sectional nature precludes us from investigating the change in psychopathological symptom severity among psychiatric patients prior to and during the pandemic. Second, causal relationships among variables could not be established. Third, our patient sample was recruited from outpatient clinics only and did not include those admitted to psychiatric inpatient units, and may therefore introduce selection bias towards patients with milder illness. Fourth, psychopathological symptom assessments were based on participants’ self-reporting (albeit well-validated and commonly used in mental-health surveys) which may not well align with the corresponding rating instruments administered by mental-health professionals.
In conclusion, this report is among the very few studies that comprehensively examined inter-relationships between psychopathological symptoms, cognitive complaints, health-related quality-of-life, loneliness, resilience and specific pandemic-related factors among psychiatric patients using network analysis. Our results indicate that anxiety is the most central node in the network, with a strong positive association with depression, and may represent a critical target of intervention to prevent further cascade of negative mental-health outcomes at times of pandemic. COVID-19 related variables including fear of contagion and stressor burden may exert influence on exacerbating psychopathological symptoms, especially insomnia and PTSD-like symptoms.
Data availability
The data that support the findings of this study and the analytic codes for data analysis are available from the corresponding author upon reasonable request.
References
Cheung PH, Chan CP, Jin DY. Lessons learned from the fifth wave of COVID-19 in Hong Kong in early 2022. Emerg Microbes Infect. 2022;11:1072–8.
Lee P. Covid-19 in data: 7 charts showing Hong Kong’s deadly Omicron outbreak, 2022. https://hongkongfp.com/2022/03/12/covid-19-in-data-6-charts-showing-hong-kongsdeadly-omicron-outbreak/. Accessed 2022 March 13.
Taquet M, Luciano S, Geddes JR, Harrison PJ. 2021. Bidirectional associations between COVID-19 and psychiatric disorder: retrospective cohort studies of 62 354 COVID-19 cases in the USA. Lancet Psychiatry. 2021;8:130–140.
Wang Q, Xu R, Volkow ND. 2021. Increased risk of COVID-19 infection and mortality in people with mental disorders: analysis from electronic health records in the United States. World Psychiatry. 2021;20:124–130.
Fond G, Nemani K, Etchecopar-Etchart D, et al. Association between mental health disorders and mortality among patients with COVID-19 in 7 countries: a systematic review and meta-analysis. JAMA Psychiatry. 2021;78:1208–17.
Iasevoli F, Fornaro M, D’Urso G, COVID-19 in Psychiatry Study Group. Psychological distress in patients with serious mental illness during the COVID-19 outbreak and one-month mass quarantine in Italy. Psychol Med. 2021;51:1054–6.
Solé B, Verdolini N, Amoretti S, et al. Effects of the COVID-19 pandemic and lockdown in Spain: comparison between community controls and patients with a psychiatric disorder. Preliminary results from the BRIS-MHC STUDY. J Affect Disord. 2021;281:13–23.
Vindegaard N, Benros ME. COVID-19 pandemic and mental health consequences: systematic review of the current evidence. Brain Behav Immun. 2020;89:531–42.
McNally RJ. Can network analysis transform psychopathology? Behav Res Ther. 2016;86:95–104.
Borsboom D, Cramer AO. Network analysis: an integrative approach to the structure of psychopathology. Annu Rev Clin Psychol. 2013;9:91–121.
Zavlis O, Butter S, Bennett K, et al. How does the COVID-19 pandemic impact on population mental health? A network analysis of COVID influences on depression, anxiety and traumatic stress in the UK population. Psychol Med. 2022;52:3825–33.
Di Blasi M, Gullo S, Mancinelli E, et al. Psychological distress associated with the COVID-19 lockdown: a two-wave network analysis. J Affect Disord. 2021;284:18–26.
Kim ST, Seo JH, Lee S et al. 2022. Dysfunctional coronavirus anxiety in nonpsychotic psychiatric outpatients during the COVID-19 pandemic: A network analysis. Depress Anxiety. 2022;39:556–563.
Li W, Zhao N, Yan X et al. 2022. Network analysis of depression, anxiety, posttraumatic stress symptoms, insomnia, pain, and fatigue in clinically stable older patients with psychiatric disorders during the COVID-19 outbreak. J Geriatr Psychiatry Neurol. 2022;35:196–205.
Fico G, Oliva V, De Prisco M, et al. Anxiety and depression played a central role in the COVID-19 mental distress: a network analysis. J Affect Disord. 2023;338:384–92.
Kim ST, Seo JH, Park CI, Kim SJ, Kang JI. COVID-19 pandemic’s impact on networks of depression and anxiety in naturalistic transdiagnostic sample of outpatients with non-psychotic mental illness. Front Psychiatry. 2023;14:1118942.
Li W, Zhao N, Yan X, et al. Network analysis of depression, anxiety, posttraumatic stress symptoms, insomnia, pain, and fatigue in clinically stable older patients with psychiatric disorders during the COVID-19 outbreak. J Geriatr Psychiatry Neurol. 2022;35(2):196–205.
Kim ST, Seo JH, Lee S, et al. Dysfunctional coronavirus anxiety in nonpsychotic psychiatric outpatients during the COVID-19 pandemic: a network analysis. Depress Anxiety. 2022;39(7):556–63.
Kroenke K, Spitzer RL, Williams JB. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med. 2001;16:606–13.
Spitzer RL, Kroenke K, Williams JB, Löwe B. A brief measure for assessing generalized anxiety disorder: the GAD-7. Arch Intern Med. 2006;166:1092–7.
Guo J, Yang L, Xu Y, et al. Prevalence and risk factors associated with insomnia symptoms among the Chinese general public after the coronavirus disease 2019 epidemic was initially controlled. Nat Sci Sleep. 2016;13:703.
Bastien CH, Vallières A, Morin CM. Validation of the Insomnia Severity Index as an outcome measure for insomnia research. Sleep Med. 2001;2:297–307.
Mark W, Toulopoulou T. Validation of the Chinese version of Community Assessment of psychic experiences (CAPE) in an adolescent general population. Asian J Psychiatry. 2017;26:58–65.
Rosa AR, Mercadé C, Sánchez-Moreno J, et al. Validity and reliability of a rating scale on subjective cognitive deficits in bipolar disorder (COBRA). J Affect Disord. 2013;150:29–36.
Montejo L, Solé B, Verdolini N, BRIS-MHC research group, et al. Self-reported neurocognitive symptoms during COVID-19 lockdown and its associated factors in a sample of psychiatric patients. Results from the BRIS-MHC study. Eur Neuropsychopharmacol. 2021;53:7–18.
Lang L, Zhang L, Zhang P, Li Q, Bian J, Guo Y. Evaluating the reliability and validity of SF-8 with a large representative sample of urban Chinese. Health Qual Life Outcomes. 2018;16:55.
Hughes ME, Waite LJ, Hawkley LC, Cacioppo JT. A short scale for measuring loneliness in large surveys: results from two population-based studies. Res Aging. 2004;26:655–72.
Smith BW, Dalen J, Wiggins K, Tooley E, Christopher P, Bernard J. The brief resilience scale: assessing the ability to bounce back. Int J Behav Med. 2008;15:194–200.
Foygel R, Drton M. Bayesian model choice and information criteria in sparse generalized linear models. arXiv. 2011;1112:5635.
Friedman J, Hastie T, Tibshirani R. Sparse inverse covariance estimation with the graphical lasso. Biostatistics. 2008;9:432–41.
van Borkulo CD, Boschloo L, Borsboom D, Penninx BWJH, Waldorp LJ, Schoevers RA. Association of symptom network structure with the course of depression. JAMA Psychiatry. 2015;72:1219–26.
Haslbeck JM, Fried EI. How predictable are symptoms in psychopathological networks? A reanalysis of 18 published datasets. Psychol Med. 2017;47:2767–76.
Epskamp S, Borsboom D, Fried EI. Estimating psychological networks and their accuracy: a tutorial paper. Behav Res Methods. 2018;50:195–212.
Bridgland VM, Moeck EK, Green DM, et al. Why the COVID-19 pandemic is a traumatic stressor. PLoS ONE. 2021;16:e0240146.
Boals A, Banks JB. Stress and cognitive functioning during a pandemic: thoughts from stress researchers. Psychol Trauma. 2020;12:S255.
McVay JC, Kane MJ, Kwapil TR. Tracking the train of thought from the laboratory into everyday life: an experience-sampling study of mind wandering across controlled and ecological contexts. Psychon Bull Rev. 2009;16:857–63.
Kira IA, Shuwiekh HAM, Ashby JS, et al. The impact of COVID-19 traumatic stressors on mental health: is COVID-19 a new trauma type. Int J Ment Health Addict. 2023;21:51–70.
Braquehais MD, Vargas-Cáceres S, Gómez-Durán E, et al. The impact of the COVID-19 pandemic on the mental health of healthcare professionals. QLM. 2020. https://doi.org/10.1093/qjmed/hcaa207. [Online ahead of print].
Choi EP, Hui BP, Wan EY. Depression and anxiety in Hong Kong during COVID-19. Int J Environ Res Public Health. 2020;17:3740.
Tso IF, Park S. Alarming levels of psychiatric symptoms and the role of loneliness during the COVID-19 epidemic: a case study of Hong Kong. Psychiatry Res. 2020;293:113423.
Martire VL, Caruso D, Palagini L, Zoccoli G, Bastianini S. Stress and sleep: a relationship lasting a lifetime. Neurosci Biobehav Rev. 2020;117:65–77.
Cénat JM, Blais-Rochette C, Kokou-Kpolou CK, et al. Prevalence of symptoms of depression, anxiety, insomnia, posttraumatic stress disorder, and psychological distress among populations affected by the COVID-19 pandemic: a systematic review and meta-analysis. Psychiatry Res. 2021;295:113599.
Cooke JE, Eirich R, Racine N, Madigan S. Prevalence of posttraumatic and general psychological stress during COVID-19: a rapid review and meta-analysis. Psychiatry Res. 2020;292:113347.
Ballesio A, Zagaria A, Musetti A, et al. Longitudinal associations between stress and sleep disturbances during COVID-19. Stress Health. 2022;38:919–26.
Alimoradi Z, Broström A, Tsang HWH, et al. Sleep problems during COVID-19 pandemic and its’ association to psychological distress: a systematic review and meta-analysis. EClinicalMedicine. 2021;36:100916.
Jahrami H, BaHammam AS, Bragazzi NL, Saif Z, Faris M, Vitiello MV. Sleep problems during the COVID-19 pandemic by population: a systematic review and meta-analysis. J Clin Sleep Med. 2021;17:299–313.
Taylor S, Landry CA, Paluszek MM, Asmundson GJ. Reactions to COVID-19: Differential predictors of distress, avoidance, and disregard for social distancing. J Affect Disord. 2020;277:94–8.
Kahlon MK, Aksan N, Aubrey R, et al. Effect of layperson-delivered, empathy-focused program of telephone calls on loneliness, depression, and anxiety among adults during the COVID-19 pandemic: a randomized clinical trial. JAMA Psychiatry. 2021;78:616–22.
Rodrigues IM, Lima AG, Santos AED, et al. A single session of virtual reality improved tiredness, shortness of breath, anxiety, depression and well-being in hospitalized individuals with COVID-19: a randomized clinical trial. J Pers Med. 2022;12:829.
Acknowledgements
We thank all the coordinating clinicians and staff from the psychiatric outpatient units (Western Psychiatric Centre and Psychiatric Outpatient Clinic in Queen Mary Hospital) for their kind assistance. We are also grateful to the individuals who participated in the study.
Funding
The study was supported by the Hong Kong Research Grants Council (grant number: 10617014). The funders had no role in study design, data collection, data analysis, interpretation of the data, manuscript preparation or journal submission.
Author information
Authors and Affiliations
Contributions
W.C.C., E.M.C.C. and C.S.M.W. designed and conceptualized the study. V.S.C.F., Y.K.S., J.M.T.C., J.K.N.C. and R.S.T.C. conducted data collection. V.S.C.F. conducted statistical analysis and wrote the first draft of the manuscript. W.C.C., V.S.C.F., E.M.C.C., C.S.M.W. and C.W.L. interpreted the study data. W.C.C. and V.S.C.F. revised and finalized the manuscript. All authors provided critical feedback to the manuscript and have approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was performed in accordance with the Declaration of Helsinki, and was approved by the Institutional Review Board of the University of Hong Kong/Hospital Authority Hong Kong West Cluster (HKU/HA HKW) and all participants provided written informed consent.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Fung, V.S.C., Chan, J.K.N., Chui, E.M.C. et al. Network analysis on psychopathological symptoms, psychological measures, quality of life and COVID-19 related factors in Chinese psychiatric patients in Hong Kong. BMC Psychiatry 24, 271 (2024). https://doi.org/10.1186/s12888-024-05690-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12888-024-05690-7