
Abstract
Background
Anxious depression, which is a common subtype of major depressive disorder, has distinct clinical features from nonanxious depression. However, little is known about the neurobiological characteristics of anxious depression. In this study, we explored resting-state regional brain activity changes between anxious depression and nonanxious depression.
Method
Resting-state functional magnetic resonance (rs-fMRI) imaging data were collected from 60 patients with anxious depression, 38 patients with nonanxious depression, and 60 matched healthy controls (HCs). One-way analysis of variance was performed to compare the whole-brain fractional amplitude of low-frequency fluctuation (fALFF) in the three groups. The correlation between the fALFF values and the clinical measures was examined.
Results
Compared with those of HCs, the fALFF values in the left superior temporal gyrus (STG) in patients with anxious depression were significantly increased, while the fALFF values in the left middle temporal gyrus (MTG), left STG, and right STG in patients with nonanxious depression were significantly increased. Patients with anxious depression showed reduced fALFF values in the right STG compared with patients with nonanxious depression (p < 0.001, corrected). Within the anxious depression group, fALFF value in the right STG was positively correlated with the cognitive disturbance score (r = 0.36, p = 0.005 corrected).
Conclusion
The bilateral STG and left MTG, which are related to the default mode network, appear to be key brain regions in nonanxious depression, while the right STG plays an essential role in the neuropathological mechanism of anxious depression.
Similar content being viewed by others

Background
Anxious depression is a clinical subtype of major depressive disorder (MDD) that presents with a high cooccurrence of anxiety-related symptoms [1]. It is estimated that approximately 50 − 80% of MDD patients have a comorbid anxiety disorder or syndromal anxiety symptoms [2,3,4].
Anxious depression is commonly defined using either syndromal criteria [5] (i.e., cooccurring MDD and at least one anxiety disorder diagnosis) or dimensional criteria [6, 7] (i.e., MDD diagnosis and anxiety/somatization factor score for 17 items on the Hamilton Rating Scale for Depression (HAMD-17) ≥ 7) [8]. In China, since MDD patients have a tendency have depression experiences with significant somatic symptoms [9], the dimensional criteria used to define anxious depression might be more suitable for clinical research in this particular subtype. In comparison with patients with nonanxious depression, patients with anxious depression have more severe somatic symptoms, a lower remission rate, a higher relapse rate or more recurrent episodes, more frequent suicidal ideations, a poorer response to antidepressants, more frequent and intense medication side effects, and a worse prognosis [10]. Although anxious depression is a common illness that leads to serious social and economic burdens [11, 12], there is less information regarding the neurobiological characteristics of anxious depression.
Previous neuroimaging studies have reported both structural and functional alterations in the cortical-limbic circuit, which are involved in emotional and cognitive regulation in patients with anxious depression [13,14,15]. A study that examined cortical and white matter alterations in MDD patients with comorbid generalized anxiety disorder (GAD) revealed thinning of the right medial orbitofrontal and fusiform gyri, left temporal pole, and lateral occipital cortices [13]. In a task-state functional magnetic resonance imaging (fMRI) study, patients with MDD and anxiety comorbidity who completed the parametric go/no-go (PGNG) test had higher activation in the anterior dorsolateral prefrontal cortex, hippocampus, and caudate within the cognitive control network than controls [14]. In a resting-state fMRI (rs-fMRI) study, Andreescu et al. found stronger functional connectivity (FC) in the posterior regions of the default mode network (DMN) and lower FC in the anterior regions of the DMN in patients with anxious depression than in patients with nonanxious depression [15]. Additionally, patients with anxious depression demonstrated reduced FC between the right centromedial/laterobasal part of the amygdala and right middle frontal gyrus relative to patients with nonanxious depression [16]. Although FC can be used to identify network and regional changes in anxious depression, it can not be used to explain the specific changes and regions that are involved in the primary deficits of the disease. Thus far, to our knowledge, there are only two rs-fMRI studies of brain activity in anxious depression [17, 18]. In the first study, it was observed that, compared to both remitted depression patients and healthy controls (HCs), patients with anxious depression exhibited an increase in the activity of the right dorsal anterior insula, while the activity of the bilateral lingual gyrus decreased [17]. However, the control group comprised remitted depression patients, and therefore, the results could not distinguish between patients with anxious depression and those with nonanxious depression. The second study previously reported that patients with anxious depression exhibited reduced amplitude of low-frequency fluctuation (ALFF) values in the right orbital part of the middle frontal gyrus relative to patients with nonanxious depression [18]. Nevertheless, the ALFF index is sensitive to physiological noise, which might reduce the sensitivity and specificity of spontaneous brain activity.
Fractional ALFF (fALFF) assessment is an advanced technique based on blood oxygen level-dependent (BOLD) fMRI signal intensity of a resting brain. fALFF examinations reduce nonspecific physiological artefacts in rs-fMRI and are thus highly sensitive and specific for detecting spontaneous neuronal activity [19]. In the past, the fALFF index was widely used to detect spontaneous neural activity in patients with depression [20, 21].
The DMN comprises the medial prefrontal cortex, posterior cingulate gyrus, praecuneus, bilateral inferior parietal lobule, middle temporal gyrus (MTG), superior temporal gyrus (STG), inferior temporal gyrus (ITG), and other brain regions [22, 23]. The DMN also participates in various psychological cognitive activities, such as spontaneous thinking, episodic memory, and emotional processing [24, 25]. A meta-analysis of fMRI studies of MDD patients found increased activity in brain regions related to the DMN [26]. However, patients with anxiety disorders exhibit contrasting brain activity patterns within the DMN relative to patients with MDD. For instance, individuals with anxiety disorders might display decreased or underactive functioning of the DMN [22].
Based on the different brain activity characteristics of anxiety disorder and MDD in the DMN, we hypothesized that brain activity would decrease in the regions related to the DMN in patients with anxious depression compared to that in patients with nonanxious depression.
Methods
Participants
One hundred and eleven treatment-naive patients with first-episode MDD were enrolled from Nanjing Brain Hospital and Nanjing Drum Tower Hospital. The inclusion criteria for all patients were as follows: (1) a diagnosis of MDD according to the Diagnostic and Statistical Manual of Mental Disorders, 4th edition (DSM-IV) [27]; (2) diagnosis of MDD confirmed by a psychiatrist using the Mini-International Neuropsychiatric Interview(MINI) [28]; (3) right-handed Han Chinese; (4) age range of 18 to 55 years; and (5) a total score greater than 17 on the 17-item Hamilton Depression Rating Scale (HAMD-17).
All patients were grouped into anxious depression and nonanxious depression groups according to the anxiety/somatization subscale items of the HAMD-17. Anxious depression was defined as a score of ≥ 7 on the anxiety/somatization factors and nonanxious depression was classified as a score of < 7 [6,7,8, 10]. The anxiety/somatization factors included general somatic symptoms, gastrointestinal somatic symptoms, hypochondriasis, insight, psychic anxiety, and somatic anxiety [8, 29]. To obtain more detailed clinical characteristics, all patients were evaluated with the Hamilton Anxiety Rating Scale (HAMA) [30].
Sixty-two HCs, matched for sex, age, and education years, were recruited via advertisements. The MINI was used to assess HCs to confirm that they had no history of mental illnesses. All HCs were right-handed Han Chinese.
The exclusion criteria for all participants were as follows: (1) a family history of mental disorders in first-degree relatives; (2) serious physical illness or organic brain diseases, such as nervous system diseases and traumatic brain injury; (3) a history of alcohol or substance abuse; (4) current pregnancy or breastfeeding; (5) contraindications of MRI; (6) use of antidepressants, psychotherapy, transcranial magnetic stimulation and/or electroconvulsive treatment; and (7) comorbidity with other neurological disorders and mental disorders, such as bipolar disorder, schizophrenia or substance addiction.
Psychological evaluation and magnetic resonance imaging were performed on all patients at Nanjing Brain Hospital. This study was approved by the Research Ethics Review Board of Nanjing Brain Hospital (grant number 2011-KY-027). All participants were informed about the details of the experiment, and informed consent was obtained.
MRI acquisition and preprocessing
MRI images were collected at the Nanjing Brain Hospital using a 3T Siemens Verio scanner with an eight-channel radio frequency coil. During the MRI scan, all participants were instructed to lie in the supine position and keep their eyes closed, to stay awake and to keep their heads still. Resting-state fMR images were acquired using gradient-recalled echo-planar imaging (GRE-EPI) with the following parameters: repetition time (TR) = 3000 ms, echo time (TE) = 40 ms, matrix = 64 × 64, field of view (FOV) = 240 mm×240 mm, flip angle (FA) = 90°, voxel size = 3.75 × 3.75 × 4 mm3, slice = 32, thickness = 4 mm, and volumes = 133. Structural MRI 3D T1-weighted images were acquired using a magnetization-prepared rapid acquisition gradient-echo sequence. The parameters for T1-weighted images were TR = 1900 ms, TE = 2.48 ms, matrix size = 256 × 256, FOV = 250 mm×250 mm2, FA = 9°, slice = 176, and thickness = 1 mm.
The processing of fMRI data was performed using MRIcroN (http://www.mricro.com) and the Data Processing Assistant for Resting-State fMRI (DPARSF)(http://www.restfmri.net/forum/DPARSF) toolbox. The raw MRI data were converted from DICOM format into NIFTI format using MRIcroN software. The first six functional volumes were discarded to remove the scanner start-up noise. Then, slice-timing correction and head-motion correction were performed on all the remaining images. Framewise displacement (FD) was calculated according to the work of Power et al. [31]. To minimize the influence of head displacement, ten patients with more than 2 mm movement in any direction and 2° of angular motion during the fMRI scan were excluded from the study. Images were then coregistered to the corresponding high-resolution T1 anatomical images, which were transformed into Montreal Neurological Institute (MNI) space. Afterwards, functional images were resampled to 3 × 3 × 3 mm3 voxels and smoothed with a 4-mm full-width, half-maximum Gaussian kernel. Linear detrending and temporal bandpass filtering (0.01–0.08 Hz) were performed. Five participants, including three patients and two HCs, were excluded because of abnormal brain signals.
fALFF analysis
To investigate regional activity, the grey matter template from the DPARSF toolbox was utilized to compute the whole-brain voxelwise fALFF. The whole brain comprised a total of 271,633 voxels (61 × 73 × 61 voxels). The fALFF maps for each individual were calculated using the DPARSF toolbox. The fALFF for each voxel was defined as the ratio of the power of low-frequency fluctuations (0.01–0.08 Hz) to that of the entire detectable frequency range. fALFF values were considered more sensitive for detecting spontaneous brain activity than ALFF values. The fast Fourier transform was applied to convert the time series into the frequency domain.
Statistical analysis
We evaluated the demographic characteristics among the three groups and clinical variables between patients with anxious depression and nonanxious depression and the distributions of all demographic and clinical variables were analysed. We used the chi-squared test to compare group differences in sex. For continuous variables, we used a one-way analysis of variance (ANOVA) or two-sample t test to compare variables whose variance was homogenous, while a nonparametric test was employed to compare the remaining variables.
ANOVA was used to compare fALFF values among the three groups while controlling for age, sex and education. Additionally, a post hoc t test was utilized to compare each pair of groups based on the observed significant clusters among the three groups. The corrected threshold was determined by AlphaSim correction with a threshold of p < 0.001. AlphaSim correction was performed using the Resting-State fMRI Data Analysis Toolkit (REST) toolbox. The minimal number of voxels (k) in a cluster was 13 for ANOVA, while k was 2 for post hoc analysis.
Relationships with clinical variables
To examine the correlation between brain functional abnormalities and clinical variabilities in the anxious depression group, we performed correlation analyses. The fALFF values involved in correlation analyses were the mean fALFF values within the 4-mm radius sphere centered at the peak of significantly different clusters between anxious depression and nonanxious depression patients. The clinical variables included the total HAMD score, HAMA score, duration of illness, and five-symptom factor scores. The five-symptom factor scores was defined as the total score for the corresponding items in the HAMD, including the anxiety/somatization factor, retardation factor, cognition disturbance factor, hopelessness factor, and sleep disturbance factor. The correlation between significant fALFF values and these clinical variables was examined using Pearson correlation analysis. The significance level was set at p < 0.0063(Bonferroni multiple comparisons correction p < 0.05/8).
Results
Demographic and clinical data
Sixty patients with anxious depression, 38 patients with nonanxious depression, and 60 HCs were selected for data analysis. The demographic characteristics and clinical variables of the participants are shown in Table 1. There were no significant differences in sex, age, years of education, or FD among the three groups. The duration of illness between the anxious depression and nonanxious depression groups did not differ significantly. The HAMD-17 score, anxiety/somatization factor score, and HAMA score of the anxious depression group were significantly higher than those of the nonanxious depression group, while the HAMD-17 score minus the anxiety/somatization factor score showed no difference between the two groups.
fALFF
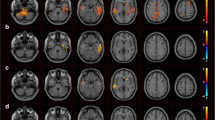
Group differences. There were five clusters with significant differences among the three groups. The observed clusters were named according to their peak coordinate locations: the right STG, the left STG, the left MTG, right cerebellar lobule 4 and 5, and right cerebellar lobule 7b (p < 0.001, k > 13, p < 0.05 corrected for multiple comparisons with AlphaSim)(see Table 2; Fig. 1A).

Clusters showing significantly differences. A: Clusters showing the significantly differences in the fALFF among the three groups. B: Clusters showing the significantly differences in the fALFF between AnD group and NAnD group. C: Clusters showing the differences in the fALFF between AnD group and HCs. D: Clusters showing the differences in the fALFF between NAnD and HCs. The color bar signifies the F or t value. Abbreviations: AnD, anxious depression; NAnD, nonanxious depression; HCs, healthy controls; ANOVA, analysis of variance; fALFF, fractional amplitude of low-frequency fluctuation
fALFF
Anxious depression patients vs. nonanxious depression patients. Relative to that of nonanxious depression patients, the fALFF value of the right STG was significantly lower in anxious depression patients (p < 0.001, k > 2, p < 0.05 corrected for multiple comparisons with AlphaSim)(see Table 2; Fig. 1B).
fALFF
Anxious depression patients vs. HCs. In contrast to those of HCs, the fALFF values of right cerebellar lobule 7b, right cerebellar lobule 8, right cerebellar lobule 9, and left cerebellar lobule 9 were significantly lower in patients with anxious depression, while the fALFF value of the left STG was significantly higher (p < 0.001, k > 2, p < 0.05 corrected for multiple comparisons with AlphaSim)(see Table 2; Fig. 1C).
fALFF
Nonanxious depression patients vs. HCs. Compared with HCs, the patients with nonanxious depression had higher fALFF values in right cerebellar lobule 4 and 5, the left MTG, the left STG, and the right STG(p < 0.001, k > 2, p < 0.05 corrected for multiple comparisons with AlphaSim)(see Table 2; Fig. 1D).
Correlational analysis between fALFF values and clinical data
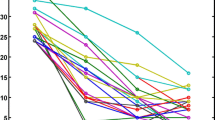
There was a significantly positive correlation between the fALFF value of the right STG and the cognitive disturbance factor score in the anxious depression group (r = 0.36, p = 0.005 corrected for multiple comparisons with Bonferroni correction)(see Fig. 2). All the corrected and uncorrected results are shown in Table 3.

Positive correlation between the fALFF values of STG in AnD group with cognitive disturbance factor scores. Abbreviations: fALFF, fractional amplitude of low-frequency fluctuation; AnD, anxious depression; STG, Superior Temporal Gyrus
Discussion
In the present study, patients with anxious depression exhibited significantly lower fALFF values in the right STG in contrast to patients with nonanxious depression and significantly higher fALFF values in the left STG compared to HCs. In addition, the fALFF values of the left MTG, left STG, and right STG were significantly higher in patients with nonanxious depression than in HCs. Furthermore, the fALFF values of the right STG positively correlated with the cognitive disturbance factor score in patients with anxious depression.
Our findings are in line with previous structural magnetic resonance studies that reported decreased grey matter volume in the STG and MTG in individuals with depression [32, 33]. Moreover, fMRI studies have identified brain activity alterations in the MTG and STG in patients with depression [34, 35]. Collectively, these results indicate that the MTG and STG play a role in the neuropathogenesis of depression. Both the MTG and STG are integral components of the DMN, which is particularly active during resting states [24] and is closely related to self-reference, rumination, spontaneous thinking, episodic memory, cognitive control, and emotional processing [36, 37]. Notably, the patients with depression exhibited more psychological activity of self-reference [38]. A meta-analysis of fMRI studies demonstrated increased activity in brain regions linked to the DMN in MDD patients [26]. Moreover, subtype analysis of depression further supported these findings, showing that the fALFF value in the STG of patients with anxious depression was significantly higher than that of HCs [39], which was consistent with our results.
The right STG participates in emotional and high-level cognitive functions such as emotional attention [40], social cognition [41], spatial perception [42], and exploration [43]. Previous structural MRI studies have confirmed the role of the right STG in the pathology of depression [44,45,46]. fMRI studies also revealed an association between the STG and depression [46,47,48]. Moreover, both current and remitted MDD patients exhibited morphologic changes in subregions of the STG [33]. Li et al. found that the regional homogeneity value of the right STG was significantly higher in patients with depression than in HCs [49]. In addition, the right STG is closely related to the generation of anxiety. Patients with social anxiety disorder and GAD had lower FC in the right and bilateral STG, respectively [50, 51]. Patients with severe anxiety disorder showed significantly reduced FC in regions of the DMN, including the right STG [23]. From these studies, it can be inferred that the function of the right STG increases in depression and decreases in anxiety. Anxious depression could be considered MDD with the presence of anxiety, which might explain why the fALFF value of the right STG was significantly lower in patients with anxious depression than in patients with nonanxious depression.
In our results, the fALFF value of the right STG had a positive correlation with the cognitive disturbances score in patients with anxious depression. Notably, the DMN is the most active network at rest in MDD patients and is related to negative rumination [52]. Furthermore, excessive self-referential processing, which plays a critical role in cognition, was activated in DMN structures, including the STG [53]. Therefore, higher a fALFF value in the right STG of patients with anxious depression might lead to increased self-reference and rumination activities, ultimately contributing to cognitive impairment.
In our study, the fALFF values of right cerebellar lobule 7b, right cerebellar lobule 8, and bilateral cerebellar lobule 9 decreased significantly in patients with anxious depression compared to those of HCs. Cerebellar lobules 7b, 8, and 9 are part of the visual network and are involved in advanced cognitive and emotional activities [54, 55]. In addition, cerebellar lobule 7b is part of the auditory network and salience network [55]. Cerebellar lobule 8 is a component of the sensorimotor network and is activated during pain-related processes, while cerebellar lobule 9 is related to the DMN [55]. Furthermore, there was strong rs-FC among cerebellar lobule 8, cerebellar lobule 9 and the amygdala [55]. Since the cerebellar lobules 7b, 8, and 9 are associated with the salience network, amygdala, and DMN, there is a possibility that reduced activity in these lobules might impair the ability to regulate anxiety.
There were several limitations in the study. First, the sample size was relatively small. Second, this study was cross-sectional study and did not consider the dynamic changes in brain activity during treatment. Future research should include a larger sample size and investigate the dynamic changes in brain activity before and after treatment. Finally, while we identified clusters in the cerebellum, it is essential to highlight the need for a closer examination of the pathology of MDD. Given the cerebellum’s unique physiological characteristics and anatomical location, the signals observed in this region are susceptible to potential confounding factors. Therefore, it is imperative to interpret the cerebellar results with caution, recognizing the complexities of this brain region in the context of MDD. Further investigations into the underlying nature of these signals are warranted in future research to provide a more comprehensive understanding of their significance and potential relevance to the disorder.
Conclusion
In summary, we used the fALFF index to explore the characteristics of resting-state brain activity in unmedicated patients with anxious depression. Our preliminary findings suggested that the bilateral STG and left MTG might be key brain regions in nonanxious depression. In addition, the right STG appears to play an essential role in the neural basis of anxious depression. The neural activity alterations within the STG might contribute to the emotional and cognitive aspects of anxious depression. Further research is needed to validate and corroborate the roles of these brain regions in nonanxious depression and anxious depression.
Data availability
The datasets used and/or analysed during the current study available from the corresponding author on reasonable request.
References
Rush AJ. The varied clinical presentations of major depressive disorder. J Clin Psychiatry. 2007;68(Suppl 8):4–10.
Gaspersz R, Nawijn L, Lamers F, Penninx BW. Patients with anxious depression: overview of prevalence, pathophysiology and impact on course and treatment outcome. Curr Opin Psychiatry. 2018;31(1):17–25. https://doi.org/10.1097/YCO.0000000000000376.
Bui E, Fava M. From depression to anxiety, and back. Acta Psychiatrica Scandinavica. 2017;136(4):341–2. https://doi.org/10.1111/acps.12801.
Ionescu DF, Niciu MJ, Mathews DC, Richards EM, Zarate CA Jr. Neurobiology of anxious depression: a review. Depress Anxiety. 2013;30(4):374–85. https://doi.org/10.1002/da.22095.
Rao S. Anxious depression: clinical features and treatment. Curr Psychiatry Rep. 2009;11(6):429–36. https://doi.org/10.1007/s11920-009-0065-2.
Fava M, Alpert JE, Carmin CN, Wisniewski SR, Trivedi MH, Biggs MM, Shores-Wilson K, Morgan D, Schwartz T, Balasubramani G. Clinical correlates and symptom patterns of anxious depression among patients with major depressive disorder in STAR* D. Psychol Med. 2004;34(7):1299–308. https://doi.org/10.1017/s0033291704002612.
Fava M, Rush AJ, Alpert JE, Carmin CN, Balasubramani G, Wisniewski SR, Trivedi MH, Biggs MM, Shores-Wilson K. What clinical and symptom features and comorbid disorders characterize outpatients with anxious major depressive disorder: a replication and extension. The Canon-anxious Depressionian Journal of Psychiatry. 2006;51(13):823–35. https://doi.org/10.1177/070674370605101304.
Ionescu DF, Niciu MJ, Henter ID, Zarate CA. Defining anxious depression: a review of the literature. CNS Spectr. 2013;18(5):252–60. https://doi.org/10.1017/S1092852913000114.
Parker G, Gladstone G, Chee KT. Depression in the planet’s largest ethnic group: the Chinese. Am J Psychiatry. 2001;158(6):857–64. https://doi.org/10.1176/appi.ajp.158.6.857.
Maurizio Fava AJR, Jonathan E, Alpert GK, Balasubramani SR, Wisniewski, Cheryl N, Carmin MM, Biggs S, Zisook A, Leuchter R, Howland. Diane Warden, Madhukar H Trivedi: difference in treatment outcome in outpatients with anxious versus nonanxious depression: a STAR*D report. Am J Psychiatry. 2008;165(3):342–51. https://doi.org/10.1176/appi.ajp.2007.06111868.
Kessler RC, Sampson NA, Berglund P, Gruber MJ, Wilcox MA. Anxious and non-anxious major depressive disorder in the World Health Organization World Mental Health Surveys. Epidemiol Psychiatric Sci. 2015;24(3):210–26. https://doi.org/10.1017/S2045796015000189.
Vos T, Flaxman AD, Naghavi M, Lozano R, Michaud C, Ezzati M, Shibuya K, Salomon JA, Abdalla S, Aboyans V, et al. Years lived with disability (YLDs) for 1160 sequelae of 289 Diseases and injuries 1990–2010: a systematic analysis for the global burden of Disease Study 2010. Lancet. 2012;380(9859):2163–96. https://doi.org/10.1016/S0140-6736(12)61729-2.
Canu E, Kostić M, Agosta F, Munjiza A, Ferraro PM, Pesic D, Copetti M, Peljto A, Tosevski DL, Filippi M. Brain structural abnormalities in patients with major depression with or without generalized anxiety disorder comorbidity. J Neurol. 2015;262(5):1255–65. https://doi.org/10.1007/s00415-015-7701-z.
Crane NA, Jenkins LM, Dion C, Meyers KK, Weldon AL, Gabriel LB, Walker SJ, Hsu DT, Noll DC, Klumpp H. Comorbid anxiety increases cognitive control activation in major depressive disorder. Depress Anxiety. 2016;33(10):967–77. https://doi.org/10.1002/da.22541.
Andreescu C, Wu M, Butters MA, Figurski J, Reynolds C, Aizenstein HJ. The default mode network in late-life anxious depression. Am J Geriatric Psychiatry. 2011;19(11):980–3. https://doi.org/10.1097/JGP.0b013e318227f4f9.
Jqa B, St A, Xwc D, Jsa E, Yu C, Shui T, Zya E, Qlc D. Brain functional abnormalities in the amygdala subregions is associated with anxious depression. J Affect Disord. 2020;276:653–9. https://doi.org/10.1016/j.jad.2020.06.077.
Liu CH, Ma X, Song LP, Fan J, Wang WD, Lv XY, Zhang Y, Li F, Wang L, Wang CY. Abnormal spontaneous neural activity in the anterior insular and anterior cingulate cortices in anxious depression. Behav Brain Res. 2015;281:339–47. https://doi.org/10.1016/j.bbr.2014.11.047.
Zhao P, Yan R, Wang X, Geng J, Lu Q. Reduced resting state neural activity in the right Orbital Part of Middle Frontal Gyrus in anxious depression. Front Psychiatry. 2020;10:994. https://doi.org/10.3389/fpsyt.2019.00994.
Zou QH, Zhu CZ, Yang Y, Zuo XN, Long XY, Cao QJ, Wang YF, Zang YF. An improved approach to detection of amplitude of low-frequency fluctuation (ALFF) for resting-state fMRI: fractional ALFF. J Neurosci Methods. 2008;172(1):137–41. https://doi.org/10.1016/j.jneumeth.2008.04.012.
Gao Y, Wang X, Xiong Z, Ren H, Liu R, Wei Y, Li D. Abnormal fractional amplitude of low-frequency fluctuation as a potential imaging biomarker for first-episode major depressive disorder: a resting-state fMRI study and support Vector Machine Analysis. Front Neurol. 2021;12:751400. https://doi.org/10.3389/fneur.2021.751400.
Huang M, Lu S, Yu L, Li L, Zhang P, Hu J, Zhou W, Hu S, Wei N, Huang J. Altered fractional amplitude of low frequency fluctuation associated with cognitive dysfunction in first-episode drug-nave major depressive disorder patients. BMC Psychiatry. 2017;17(1):11. https://doi.org/10.1186/s12888-016-1190-1.
Sylvester CM, Corbetta M, Raichle M, Rodebaugh T, Schlaggar B, Sheline Y, Zorumski C, Lenze E. Functional network dysfunction in anxiety and anxiety disorders. Trends Neurosci. 2012;35(9):527–35. https://doi.org/10.1016/j.tins.2012.04.012.
Modi S, Kumar M, Kumar P, Khushu S. Aberrant functional connectivity of resting state networks associated with trait anxiety. Psychiatry Res Neuroimaging. 2015;234(1):25–34. https://doi.org/10.1016/j.pscychresns.2015.07.006.
Raichle ME. The brain’s default mode network. Annu Rev Neurosci. 2015;38:433–47. https://doi.org/10.1146/annurev-neuro-071013-014030.
Buckner RL, Andrews-Hanna JR, Schacter DL. The brain’s default network: anatomy, function and relevance to Disease. Ann N Y Acad Sci. 2008;1124(1):1–38. https://doi.org/10.1196/annals.1440.011.
Kaiser RH, Andrews-Hanna JR, Wager TD, Pizzagalli DA. Large-Scale Network Dysfunction in Major Depressive disorder: a Meta-analysis of resting-state functional connectivity. Jama Psychiatry. 2015;72(6):603–11. https://doi.org/10.1001/jamapsychiatry.2015.0071.
Sartorius N, Kaelber CT, Cooper JE, Roper MT, Regier DA. Progress toward achieving a common language in psychiatry. Results from the field trial of the clinical guidelines accompanying the WHO classification of mental and behavioral disorders in ICD-10. Arch Gen Psychiatry. 1993;50(2):115–24. https://doi.org/10.1001/archpsyc.1993.01820140037004.
Sheehan DV, Lecrubier Y, Sheehan KH, Amorim PA, Dunbar GCL. The mini-international neuropsychiatric interview (M.I.N.I.): the development and validation of a structured diagnostic psychiatric interview for DSM-IV and ICD-10. J Clin Psychiatry. 1998;59(Suppl 20):22–33.
Farabaugh AH, Bitran S, Witte J, Alpert J, Chuzi S, Clain AJ, Baer L, Fava M, Mcgrath PJ, Dording C. Anxious depression and early changes in the HAMD-17 anxiety-somatization factor items and antidepressant treatment outcome. Int Clin Psychopharmacol. 2010;25(4):214–7. https://doi.org/10.1097/YIC.0b013e328339fbbd.
Thompson E. Hamilton rating scale for anxiety (HAM-A). Occup Med. 2015;65(7):601. https://doi.org/10.1093/occmed/kqv054.
Power JD, Barnes KA, Snyder AZ, Schlaggar BL, Petersen SE. Spurious but systematic correlations in functional connectivity MRI networks arise from subject motion. NeuroImage. 2012;59(3):2142–54. https://doi.org/10.1016/j.neuroimage.2011.10.018.
Kandilarova S, Stoyanov D, Sirakov N, Maes M, Specht K. Reduced grey matter volume in frontal and temporal areas in depression: contributions from voxel-based morphometry study. Acta Neuropsychiatrica. 2019;31(5):252–7. https://doi.org/10.1017/neu.2019.20.
Takahashi T, Yücel M, Lorenzetti V, Walterfang M, Kawasaki Y, Whittle S, Suzuki M, Pantelis C, Allen NB. An MRI study of the superior temporal subregions in patients with current and past major depression. Progress in Neuropsychopharmacology & Biological Psychiatry. 2010;34(1):98–103. https://doi.org/10.1016/j.pnpbp.2009.10.005.
Guo W, Liu F, Yu M, Zhang J, Zhang Z, Liu J, Xiao C, Zhao J. Functional and anatomical brain deficits in drug-naive major depressive disorder. Prog Neuropsychopharmacol Biol Psychiatry. 2014;54:1–6. https://doi.org/10.1016/j.pnpbp.2014.05.008.
Li N, Jin D, Wei J, Huang Y, Xu J. Functional brain abnormalities in major depressive disorder using a multiscale community detection approach. Neuroscience. 2022;501:1–10. https://doi.org/10.1016/j.neuroscience.2022.08.007.
Zhou HX, Chen X, Shen YQ, Li L, Yan CG. Rumination and the default mode network: Meta-analysis of brain imaging studies and implications for depression. NeuroImage. 2019;206:116287. https://doi.org/10.1016/j.neuroimage.2019.116287.
Davey CG, Pujol J, Harrison BJ. Mapping the self in the brain’s default mode network. NeuroImage. 2016;132:390–7. https://doi.org/10.1016/j.neuroimage.2016.02.022.
Whitfield-Gabrieli S, Ford JM. Default mode network activity and connectivity in psychopathology. Ann Rev Clin Psychol. 2012;8:49–76. https://doi.org/10.1146/annurev-clinpsy-032511-143049.
Yan H, Han Y, Shan X, Li H, Liu F, Xie G, Li P, Guo W. Common and exclusive spontaneous neural activity patterns underlying pure generalized anxiety disorder and comorbid generalized anxiety disorder and depression. J Affect Disord. 2023;331:82–91. https://doi.org/10.1016/j.jad.2023.03.047.
Jin N, Okada T, Sadato N, Fukui K, Yonekura Y. Attention to emotion modulates fMRI activity in human right superior temporal sulcus. Brain Res Cogn Brain Res. 2001;12(2):225–31. https://doi.org/10.1016/s0926-6410(01)00053-2.
Li R, Wang S, Zhu L, Guo J, Zeng L, Gong Q, He L, Chen H, Valdes-Sosa PA. Aberrant functional connectivity of resting state networks in transient ischemic Attack. PLoS ONE. 2013;8(8):e71009. https://doi.org/10.1371/journal.pone.0071009.
Amanda E, Igor S, Pattison LL, David MA. An exploration of the role of the superior temporal gyrus in visual search and spatial perception using TMS. Brain. 2004;102307–15. https://doi.org/10.1093/brain/awh244.
Hans-Otto. Karnath, Susanne, Ferber, Marc, Himmelbach: spatial awareness is a function of the temporal not the posterior parietal lobe. Nature. 2001;411(6840):950–3. https://doi.org/10.1038/35082075.
Quinn ML, Christopher WT, Rose S, Natalia J, Marie LL, Macmaster FP. History of Suicide attempt and right Superior temporal gyrus volume in youth with treatment-resistant major depressive disorder. J Affect Disord. 2018;239:291–4. https://doi.org/10.1016/j.jad.2018.07.030.
Pan LA, Ramos L, Segreti AM, Brent DA, Phillips ML. Right superior temporal gyrus volume in adolescents with a history of Suicide attempt. Br J Psychiatry. 2018;206(4):339–40. https://doi.org/10.1192/bjp.bp.114.151316.
Ali BF, Samia T, Ariel G, Philip G, John S, Nathan K, Gianfranco S, Vincenzo DL. Structural and functional alterations of the suicidal brain: an updated review of neuroimaging studies. Psychiatry Res Neuroimaging. 2018;278:77–9. https://doi.org/10.1016/j.pscychresns.2018.05.008.
Li M, Xu H, Lu S. Neural basis of Depression related to a Dominant Right Hemisphere: a resting-state fMRI study. Behav Neurol. 2018;2018:5024520. https://doi.org/10.1155/2018/5024520.
Fan T, Wu X, Yao L, Dong J. Abnormal baseline brain activity in suicidal and non-suicidal patients with major depressive disorder. Neuroence Lett. 2013;534(Complete):35–40. https://doi.org/10.1016/j.neulet.2012.11.032.
Burkhouse KL, Jacobs RH, Peters AT, Ajilore O, Langenecker SA. Neural correlates of rumination in adolescents with remitted major depressive disorder and healthy controls. Cogn Affect Behav Neurosci. 2016;17(2):1–12. https://doi.org/10.3758/s13415-016-0486-4.
Cui Q, Vanman EJ, Long Z, Pang Y, Chen Y, Wang Y, Duan X, Chen H, Gong Q, Zhang W. Social anxiety disorder exhibit impaired networks involved in self and theory of mind processing. Social Cogn Affect Neurosci. 2017;8:1284–95.
Cuevas EG, Rong W, Manning K, Wang L, Steffens MD. Functional brain networks of trait and state anxiety in late-life depression. Am J Geriatric Psychiatry. 2021;29(4):52–s53. https://doi.org/10.1016/j.jagp.2021.01.047.
Dutta A, Mckie S, Deakin J. Resting state networks in major depressive disorder. Psychiatry Res. 2014;224(3):139–51. https://doi.org/10.1016/j.pscychresns.2014.10.003.
Miller CH, Hamilton JP, Sacchet M, Gotlib IH. Meta-analysis of functional neuroimaging of major depressive disorder in Youth. Jama Psychiatry. 2015;72(10):1045–53. https://doi.org/10.1001/jamapsychiatry.2015.1376.
Depping MS, Schmitgen MM, Kubera KM, Wolf RC. Cerebellar contributions to Major Depression. Front Psychiatry. 2018;9:634. https://doi.org/10.3389/fpsyt.2018.00634.
Li S, Wen Q, Yong L, Wei H, Zhang Y, Jiang T, Yu C. Resting-state functional connectivity of the vermal and hemispheric subregions of the cerebellum with both the cerebral cortical networks and subcortical structures. NeuroImage. 2012;61(4):1213–25. https://doi.org/10.1016/j.neuroimage.2012.04.011.
Acknowledgements
We would like to express our gratitude to all the participants in Nanjing Brain Hospital and Nanjing Drum Tower Hospital.
Funding
This study was supported by grants of the National Natural Science Foundation of China (81871066); the Jiangsu Provincial key research and development program (BE2018609, BE2019675); the Jiangsu Provincial Medical Innovation Team of the Project of Invigorating Health Care through Science, Technology and Education (CXTDC2016004); the Key Project supported by Medical Science and Technology development Foundation, Jiangsu Commission of Health (K2019011).
Author information
Authors and Affiliations
Contributions
Peng Zhao designed the study and drafted of manuscript. Xinyi Wang analyzed the results. Qing Wang and Rui Yan collected the experimental data. Mohammad Ridwan Chattun proofread the article. Qing Lu and Zhijian Yao revised the paper. All authors contributed and approved the final manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
This study was approved by the Research Ethics Review Board of Nanjing Brain Hospital (grant number 2011-KY-027). Psychological evaluation and magnetic resonance imaging were performed on all patients in Nanjing Brain Hospital. All methods were carried out in accordance with relevant guidelines and regulations. All participants were informed about the details of the experiment and the informed consent was obtained.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Zhao, P., Wang, X., Wang, Q. et al. Altered fractional amplitude of low-frequency fluctuations in the superior temporal gyrus: a resting-state fMRI study in anxious depression. BMC Psychiatry 23, 847 (2023). https://doi.org/10.1186/s12888-023-05364-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12888-023-05364-w