
Abstract
Background
Whether and how psychotherapies change brain structure and function is unknown. Its study is of great importance for contemporary psychotherapy, as it may lead to discovery of neurobiological mechanisms that predict and mediate lasting changes in psychotherapy, particularly in severely mentally ill patients, such as those with chronic depression. Previous studies have shown that psychoanalytic psychotherapies produce robust and enduring improvements in not only symptom severity but also personality organization in patients who have chronic depression and early life trauma, especially if therapy is delivered at a high weekly frequency.
Methods/design
Patients with chronic major depression and a history of early life trauma will be recruited, assessed, and treated across 3 international sites: Germany, Switzerland, and the United States. They will be randomized to one of two treatment arms: either (1) once weekly psychoanalytic psychotherapies, or (2) 3–4 times weekly psychoanalytic psychotherapies. They will have full clinical characterization as well as undergo MRI scanning at study baseline prior to randomization and again one year later. A group of matched healthy controls will undergo similar assessments and MRI scanning at the same time points to help discern whether study treatments induce brain changes toward or away from normal values. Primary study outcomes will include anatomical MRI, functional MRI, and Diffusion Tensor Imaging measures. Study hypotheses will be tested using the treatment-by-time interaction assessed in multiple general linear models with repeated measures analyses in an intent-to-treat analysis.
Discussion
MODE may allow the identification of brain-based biomarkers that may be more sensitive than traditional behavioral and clinical measures in discriminating, predicting, and mediating treatment response. These findings could help to personalize care for patients who have chronic depression patients and early life trauma, and they will provide new therapeutic targets for both psychological and biological treatments for major depressive illness.
Similar content being viewed by others


Introduction
Chronic depression and psychoanalytic psychotherapy research
Chronic depression is a common disorder. Population lifetime prevalence estimates are 3–15% for major depression [1,2,3,4,5,6] and 3–4% for dysthymia [7,8,9,10], with 20–33% of all depressive illness becoming chronic [3, 11]. Persons whose depression is chronic tend to have more severe symptoms, more frequent recurrences, lower remission rates, longer courses of medication treatment [12, 13], and higher rates of psychiatric and physical co-morbidities [2, 3, 12, 14] compared with depressive episodes of shorter duration. Recent epidemiological findings suggest that chronic depression is associated with a series of potentially modifiable risk factors, such as increase in suicidal ideation/attempts during the most severe episode, higher levels of neuroticism, lower levels of extraversion and lower levels of informal help-seeking behavior compared to nonchronic MDD, that are accessible via psychotherapies that can improve the course of chronic depression [15]. Chronic depression entails enormous direct and indirect costs for health care systems (see e.g. [16]).
Patients with chronic depression require tailored psychotherapeutic treatments that address their specific clinical needs [17]. Meta-analyses show that various forms of short-term therapy are similarly successful in reducing symptom severity but do not significantly reduce relapse rates [11, 18,19,20,21,22,23,24,25,26,27]. Increasing evidence suggests that these patients require more intensive and longer treatments to achieve sustained symptomatic and functional improvement [17, 28,29,30,31].
Only a small number of studies, however, have assessed the effectiveness of long-term therapies for chronic depression [24, 25, 32,33,34,35,36,37,38,39,40]. We refer to two more recent studies that assessed the effectiveness of long-term psychoanalytic psychotherapy for chronic depression in particular. One was The Tavistock Adult Depression Study (TADS), which was a randomized controlled trial of 129 patients with chronic depression of at least 2 years duration. It assessed the effectiveness of 18 months of long-term psychoanalytic psychotherapy (LTPP) as an adjunct to treatment-as-usual (TAU), compared to TAU alone. The TAU group was treated with interventions as directed by the referring practitioner, which could include referral to other specialists in accordance with UK guidelines of the National Institute for Clinical Excellence (National Institute for Health and Clinical Excellence [41]. Both clinician- and self-reported depression severity, as well as measures of social adjustment, showed significantly greater improvement in the LTPP group [39].
The second was the LAC Study (Langzeitbehandlungen chronisch depressiver Patienten), which compared the effectiveness of long-term cognitive-behavioral therapy (CBT) vs long-term psychoanalytic therapy (PAT) in 252 chronically depressed patients. The study also considered the effects of preferential or randomized allocation [42]. As is the practice of the two forms of psychotherapeutic interventions in Germany, the number of sessions offered to the patient varied. During the first year of treatment, CBT patients received a mean (SD) of 32.5 (9.0) therapy sessions while PAT participants received a mean (SD) of 80.4 (27.8) sessions. Both psychotherapies and both allocation conditions showed a clinically relevant and highly significant reduction of depressive symptoms over 1, 2, and 3 years. After 3 years, self-rated full remission rates were 45% (BDI ≤ 12), and clinician-rated full remission rates were 61% (QIDS-C ≤ 5). The effect sizes were very large (d = 1.78 for the BDI); d = 2.12 for the QIDS-C). These effect sizes and full remission rates were better compared to other studies [11, 29, 34]. As in other studies, researchers found no significant difference between PAT and CBT for symptom reduction 3 years after beginning treatment.
In contrast to the original hypotheses PAT produced a statistically significant reduction in depressive symptoms already after one year of treatment. In addition, three years after the start of treatment, significantly more patients in psychoanalytic treatment showed increased awareness of unconscious fantasies and conflicts, so-called “structural changes, in personality organization compared to patients in cognitive-behavioral treatments [30]. Clinical observations confirmed that these changes were more pronounced in high-frequency treatments than in low-frequency treatments.
Early trauma, frequency of sessions, and treatment effects in chronic depression
An unexpected, post hoc finding of the LAC study was that more than 80% of chronically depressed patients participating in the study suffered from early trauma, and that these patients responded especially well to high frequency psychoanalytic psychotherapy, often achieving sustained, structural changes in personality organization. A review of clinical observations revealed that patients in high-frequency psychoanalytic treatments were more likely to be successful in therapeutically regaining the primal trust in a helping Other and their own self agency that had collapsed as a result of traumatization than in low frequent treatments (see e.g. [43,44,45,46]; or “epistemic trust” – see [47]. These clinical effects were connected to some extent to "structural changes" in personality organization as assessed using the Operationalized Psychodynamic Diagnosis (OPD) [29, 30, 47,48,49]. This clinical finding was consistent with a previous study showing that chronically depressed patients who had a history of early childhood trauma achieved significantly higher remission rates with psychotherapy monotherapy than with nefazodone monotherapy [50], leading to the conclusion of the study investigators that chronically depressed patients who have a history of early trauma may differ in some fundamental yet undefined way from those without a history of early trauma [50]. A meta-analysis [51] also showed that neglect and emotional abuse are correlated with adult depression. In the LAC Study emotional neglect, as measured by the CTQ, was the most frequent form of childhood trauma of the chronic depressed patients and influenced the severity of the depression in this group of patients (see e.g. [52]).
A meta-analysis of including a variety of psychotherapies for chronic depression reported a strong association for symptomatic improvement with the number of treatment sessions [53]. Moreover, both a higher number of weekly psychoanalytic sessions, as well as a more pronounced application of psychoanalytic treatment techniques, increased the effectiveness of psychotherapy in patients with major depression [54]. Session frequency has also been identified as an important factor in the efficacy of psychotherapy in general. An overview focusing on the difference between psychoanalysis and psychoanalytic psychotherapy suggested that the success of therapy does not correlate most with the duration of the treatment, but with the frequency of sessions [31]. These findings suggest that a higher treatment frequency is more effective than lower treatment frequency in reducing symptoms. In sum, findings suggest that higher session frequency may offer an advantage that goes beyond the total number of sessions in the psychoanalytic psychotherapy of depression. Still unknown is whether a similar frequency effect is present in the psychoanalytic treatment of depression that is chronic.
Psychotherapy research in depression using brain imaging
Several investigators have used brain imaging technologies to study the associations of psychotherapies with measures of brain structure and function [55], including in depressed patients [56,57,58,59,60,61,62,63,64,65,66]. Lueken & Hahn [67] describe two general approaches that have been employed thus far: 1) the longitudinal study of brain changes, comparing pre- to post-treatment brain measures, associating those changes with measures of treatment response to psychotherapy; and 2) associating pre-treatment brain measures with treatment outcomes, such as depressive symptom reduction, to identify brain predictors of treatment response. Most of these studies have been naturalistic (without employing randomization between treatment arms) and they often have been uncontrolled (without a comparison group). Three meta-analyses summarized studies on treatment effects on clinical and brain-based predictors [68,69,70]. Cristea et al. [71] combined a meta-analysis with a review of biological markers for psychotherapy in treating depression. They found limited evidence that the benefits of psychological treatments for depression translate to biological outcomes, in that only neuroimaging markers showed promise in predicting treatment response. Two neuroimaging studies are particularly important for MODE: The Hanse-Neuro-Psychoanalysis Study investigated unmedicated outpatients with recurrent depression (n = 16) and healthy controls (n = 17) before and after 15 months of 2 or more sessions of weekly psychoanalytic psychotherapy. In the fMRI study, neural activity associated with the processing of personalized attachment material changed in patients from baseline to endpoint, but not in healthy controls. The Frankfurt fMRI/EEG Depression Study (FRED) studied a subsample of participants in the LAC Depression study (see 2.1.2, n = 24 and 24 controls) using the Operationalized Psychodynamic Diagnosis (in analogy to the Hanse-Neuro-Psychoanalysis Study) and dream words taken from a significant dream elicited in a dream interview. Measurements were obtained at three different time points, each one a minimum of 8 months apart. Results of the dream experiment revealed that dream words, in contrast to neutral words, showed a differential activation of medial orbitofrontal areas, functionally related to the self and self-agency. Results of the OPD Experiment – using the OPD-sentences collected previously – yielded similar conclusions (see Fischmann et al. [72,73,74,75]).
Objectives
Although considerable evidence supports the clinical effectiveness of psychoanalytic therapies, we do not yet understand the mechanisms through which they improve symptoms and reduce functional impairments – knowledge that can further enhance treatment effectiveness, especially in the highest risk and most complex clinical populations. This mechanistic clinical trial will identify the mediators of psychoanalytic therapy treatment response in depressed patients. These neurobiological as well as clinical mediators, once identified, will allow their targeting in the development of new therapies and in improving existing ones. Using these mediators as surrogate endpoints will facilitate smaller and more cost-effective future clinical trials of psychoanalysis than those that have only clinical measures as endpoints [76]. These aims are consistent with the NIMH experimental therapeutics initiative to identify mechanistic targets for clinical trials development [77,78,79].
In addition to identifying mediators of treatment response, this mechanistic clinical trial will identify baseline predictors of psychoanalytic treatment response in chronic, severely depressed patients. In future studies, we will be able to use the predictors we discover here to determine, for example, whether we can screen depressed patients for these predictive biomarkers and thereby significantly improve treatment response rates. Identifying these markers will provide a framework for developing personalized care in depressed patients.
The prototypical study design in modern medicine for inferring causation is the Randomized Controlled Trial (RCT), which assesses the effects of an experimentally manipulated intervention on the dependent (outcome) variable, usually illness severity. RCTs studying the efficacy and effectiveness of psychotherapy traditionally use clinical measures of symptom change as their primary outcome measure. Many cognitive, behavioral, and neural systems influence symptom severity, however, making these outcome measures very noisy, which in turn reduces the statistical power to detect real change that the therapies produce. Low statistical power in turn necessitates large numbers of participants to detect significant effects of the intervention, thereby increasing the size, duration, and cost of RCTs. Instead of employing change in symptom severity as the usual clinical outcome measure, MODE will use the change in brain imaging measures from the study baseline to study endpoint as the primary study outcome, providing strong causal inference that the treatment causes the changes in brain measures and depressive symptoms observed [80]. In our prior studies using these technologies, brain measures compared with traditional clinical measures provided much more sensitive and robust markers for treatment response, because brain measures are direct reports that the treatments have on the brain, which in turn underlie the change in symptom severity. MODE will be therefore identifying the biomarkers that predict and mediate change in symptoms and other clinical outcomes in high vs low frequency of psychoanalytic therapy in severely and chronically depressed patients.
Specific aims and hypotheses
AIM 1
Identify how long-term psychoanalytic therapies change brain structure and function in chronically depressed patients with a history of early trauma and to assess how those changes differ in patients assigned randomly to either high or low frequency weekly sessions.
AIM 2
Assess whether these brain changes significantly mediate clinical improvement over 1 year of treatment.
Primary hypotheses
High compared with low frequency treatment will normalize brain structure and function.
Brain structure
Based on prior findings in chronic depression patients in an RCT of medication therapy vs placebo [81], changes in cortical thickness, representing therapy-induced, neuroplastic compensatory changes in brain structure, will normalize during 1 year of treatment – i.e., baseline abnormalities relative to healthy control values will change more during high frequency treatment compared with low frequency treatment, and 1 year after beginning treatment will be statistically indistinguishable from healthy control values. Change in cortical thickness will correlate significantly with the magnitude of clinical improvement after 1 year of treatment.
Brain activation
High compared with low frequency treatment will produce greater change in brain activity (a greater degree of normalization relative to healthy control values) in ventral medial brain regions during the functional MRI (fMRI) Cyberball paradigm for social exclusion, and the changes in brain activity will significantly mediate clinical improvement during the 1-year duration of treatment.
Functional connectivity
High compared with low frequency treatment will produce a greater change in measures of functional brain connectivity after 1 year of treatment during resting state fMRI, particularly in the default mode network (DMN), which likely subserves the capacity for free association. Based on prior findings in chronically depressed patients in an RCT of medication therapy vs placebo [82], we expect high compared with low frequency treatment to produce a greater degree of normalization in DMN activity relative to activity in healthy control participants.
Tissue microstructure
High compared with low frequency treatment will produce a more pronounced normalization of indices of tissue microstructure in white matter (increasing fractional anisotropy and decreasing mean diffusivity) measured with diffusion tensor imaging (DTI).
Secondary hypotheses
Psychopathology
Although high and low frequency treatments will both produce clinical improvement, improvement will be significantly greater for high frequency treatment in structural integration (measured with the Operationalized Psychodynamic Diagnosis Structure Questionnaire (OPD-SQ)), depressive symptoms (measured with the BDI-2), and in the manifest dreams (measured with DREams Assessment Scale for measuring Changes in manifest dream (DREAMS-C). Improvement in these clinical measures will associate significantly with the regional changes in MRI measures that change in response to high vs low frequency treatment.
Metabolic profile (only for a subgroup in Frankfurt)
Proton MR Spectroscopy (1H-MRS) measures brain metabolites N-acetyl-aspartate (NAA), choline (Cho) and creatine (Cr) as potential in vivo biomarker of the integrity of neurons (NAA), membranes (Cho) and glia (Cr) [83, 84]. High compared with low frequency treatment will produce a more pronounced changes of metabolite concentration in N-Acetylaspartate (NAA/Cr, respectively), indicating normalization of neuronal integrity measured with MR spectroscopy (1H MRS). Change in NAA (NAA/Cr) will correlate significantly with the magnitude of clinical improvement after 1 year of treatment.
Methods/Design
Study design
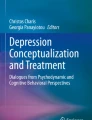
MODE is a randomized, parallel, superiority and single blinded controlled trial comparing the effectiveness of two active interventions – high frequency (n = 30) vs low frequency (n = 30) psychoanalyses – in modifying brain structure and function over one year of treatment chronic depression patients who have a history of early life trauma (Fig. 1).

Flow chart of the study
This study design will overcome many of the limitations of prior psychotherapy effectiveness studies. It will include an active control condition rather than a mere wait list, thereby controlling for the effects of interpersonal attention and interaction. Randomization and statistical evaluation will be performed by independent teams. Moreover, the active comparator condition, low frequency psychoanalysis, will help to control for the “allegiance” effects that confound most psychotherapy trials [85]. Finally, comparing high vs low frequency psychoanalyses will inherently provide an assessment of dose–response effects of psychoanalytic therapy on brain structure and function. Establishing dose–response associations will further improve causal inference in our study design.
In addition to randomization of depressed patients, we will include a group of healthy control participants (n = 30) who are free of psychiatric illness. They will not undergo treatment and therefore will not be randomized. They will undergo similar assessments and MRI scanning at one-year intervals. Their measures will serve as reference points to help discern whether study treatments induce brain changes toward or away from normal values.
Inclusion and exclusion criteria
Patients
Patients between 21 and 60 years of age of all genders suffering from chronic depression will be included in the study. Patients must be continuously depressed for more than one year and currently meet a diagnosis of major depression or dysthymia. The SCID interview will confirm a yearlong history of depression. Only patients without antidepressant (AD) medication at study onset will be included. Only patients with early trauma on at least one of the subscales of the CTQ will be included (Table 1).
Healthy control participants
Inclusion criteria are: (1) no history of prior or current psychiatric diagnoses (Structured Clinical Interview for DSM-SCID); (2) no prior history of trauma on any of the CTQ subscales; (3) 21–60 years of age; and (4) sufficient knowledge of the local language to undergo assessments. Exclusion criteria are: (1) serious physical illness; and (2) any current psychotherapeutic or psychotropic treatment. Healthy controls will be group-matched on age and gender to participants in the treatment groups (Table 2).
All participants
Standard MRI exclusion criteria will apply (metallic tattoos, pacemakers, or other metallic implants).
Intervention and comparator
Study intervention will be comprised of low frequency psychoanalytic psychotherapy (1 session a week) for early traumatized, chronically depressed patients and high frequency psychoanalytic psychotherapy (3–4 weekly sessions). The active comparator condition, low frequency psychoanalysis, delivered by study therapists who are experts in delivering both frequencies, and with the same overall manual based theoretical framework and technical interventions [86], will ensure that they will be equally aligned to both high and low frequency therapies. A group of healthy controls will be needed for brain imaging comparison purposes. A control group will allow to measure cortical thickness in patients with chronic depression in comparison to healthy control participants. Therapy sessions (45–50’ each) will be delivered in the private practice rooms or rooms of the outpatient clinics of the local psychotherapeutic institutions. Patients who will require a combination therapy of medication and psychotherapy during treatment will not be excluded but form a special subgroup that will be treated separately during data analyses. Patients who will require a change in psychotherapy setting during treatment according to patient and therapist decision will be analyzed as randomized. MODE study duration will be one year, but after 1 year of treatment initiation, treatment may continue according to patient and therapist decision. Treatments will be financed in the usual way in the participating countries (in Germany by the health insurance companies, in the US and Switzerland partly by the health insurance companies, partly by the patients themselves).
Outcome measures
Study participants will be assessed as detailed below and in Table 3, for primary and secondary outcome measures. Patients will be assessed by independent and trained clinicians who are blind to treatment conditions.
Primary outcomes: MRI brain measures
Assessment will comprise the following MRI brain measures. Anatomical MRI: measures of cortical thickness at all points across the cerebrum. Resting State Functional MRI (rsfMRI): measures of functional connectivity throughout the brain. Cyberball Task-Related Functional MRI (fMRI): measures of brain activation throughout the brain in response to trust, mistrust (social exclusion), and rebuilding of trust (social re-inclusion). Diffusion Tensor Imaging (DTI): measures of fractional anisotropy and average diffusion coefficient.
What these outcomes tell us about the brain MRI is an entirely safe way of imaging the brain at any age. It is routinely performed in unsedated people at multiple time points, including multiple time points within an RCT, and without the need for exposure to any radioactivity. MRI scanning can be performed in different modes, with each modality providing unique information probing different aspects of the brain’s structural and functional organization. Anatomical MRI provides information about brain structure, most commonly the volumes and shapes of particular brain regions. Diffusion Tensor Imaging (DTI) provides information about tissue organization within the brain, especially white matter fibers that connect one brain region to another. At each voxel, Fractional Anisotropy (FA) measures the directional diffusion of water, Mean Diffusivity (MD) measures the overall diffusion of water, Axial Diffusivity (AD) measures diffusion along the long axis of diffusion, which is presumed to be along the long axis of the fiber bundle, and Radial Diffusivity (RD) measures diffusion perpendicular to the long axis of diffusion or fiber bundle. Functional MRI (fMRI) provides measures of time-dependent changes in the relative concentration of deoxyhemoglobin within each voxel, which itself is driven largely by changes in oxygen use and the underlying changes in neuronal activity within the voxel [87, 88]. Measures of resting state connectivity (rsfMRI) are in essence measures of cross-correlation for the fMRI series of two different voxels (i.e., two different points in the brain), which assesses how strongly those two regions communicate with one another over time.
MRI Scanning
All scans will be acquired on 3.0 T scanners: Siemens Prisma (Frankfurt, Lausanne), Philips Achieva (CHLA). Signal-to-noise and contrast-to-noise was determined to be comparable across all scanning platforms (Tables 4, 5, 6 and 7).
Theoretical basis for the fMRI task used in MODE
Chronically depressed patients need to experience an intensive, professional, reliable, holding, and containing therapeutic relationship in order to both regain confidence in a "helping object" in the form of the therapist and develop a basic feeling of self-agency. According to psychoanalytic theory, severe early life trauma produces a defensive withdrawal of the self from outside objects into a depressed inner world. Metaphorically speaking, the self is encapsulated in an inner crypt [89]. Therefore, as a first indispensable step in a therapeutic relationship, the withdrawn, depressed patient must regain confidence in an external object (i.e. the therapist) to dare to confront himself with the traumatic experiences in the transference relationship, in the hope of making alternative, "healing" experiences. The fMRI task we have selected and adapted for use in MODE is intended to index the development of this basic trust in others in response to the therapeutic interventions.
Task-based fMRI ‘Cyberball’ paradigm
MODE will study the neurobiological mechanisms that subserve this evolving sense of interpersonal trust within patients over the first year of psychoanalytic therapy. We have adapted a task that participants perform while in the MRI scanner so as to identify the brain systems that support the cognitive, emotional, and behavioral requirements of the task. This fMRI task, called “Cyberball” [90], is a computer game in which participants believe they are playing with real people in another room of the building. It is designed to manipulate the independent variable of social exclusion, via including and then suddenly excluding the participant in the ball-tossing. The game begins with the participant and two other “players” throwing a ball to one another, each of the three players receiving it an equal number of times. Without warning, the other two players then stop throwing the ball to the study participant, an experience that has been shown to produce feelings of betrayal and social exclusion. After some time, they once again throw the ball to the study participant, which produces feelings of relief upon re-inclusion. Brain activity during each of the three phases of this fMRI task will be measured at study baseline and after one year of psychoanalytic therapy [91,92,93]. Our aim is to identify the neural systems that support the expression of trust, mistrust, and social exclusion, and then reintegration of trust in interpersonal relationships, how activity in these systems change over the year in depressed patients compared with the change observed in healthy controls, and how high vs low frequency of PA therapy modifies activity in these systems over time.
Secondary outcome measures
MODE will investigate whether and how brain changes are associated with common measures of change for patients with chronic depression and early trauma after one year of treatment. To achieve this aim and as recommended in meta-analytic reviews, various broad areas of patient’s functioning are assessed including (1) psychopathology, (2) personality, social and work functioning, and (3) dynamic functioning which may underlie impaired functioning and contribute to vulnerability to psychiatric disorders [94]. Due to their depressive symptomatology, patients may face some difficulties with self-report questionnaires. Therefore, we have restricted the total number of items included in the assessment battery (Table 8).
Assessment of psychopathology
Diagnosis
The Structured Clinical Interview for DSM (SCID, [95]) is used to collect diagnostic information. This instrument enables the collection of extensive information on psychiatric conditions including mood and anxiety disorders.
Depression
Depressive symptoms will be assessed using three instruments: (1) The Inventory of Depressive Symptom (QIDS; [96]), a clinician rating measure (QIDS-C16); (2) the self-rated version of the QIDS (QIDS-SR16), 16-item measures of depressive symptoms; and (3) the Berg -Depression Inventory (BDI-II; [97]). The Depressive Experience Questionnaire (DEQ; [98]), which assesses a wide range of life experiences often reported by depressed individuals but not considered symptoms of depression.
Distress
The Symptom Check-List (SCL-90-R; [99]) is a widely used self-report measure of distress and psychiatric symptoms.
Early life trauma
Early childhood trauma is recognized as one of the best predictors of response to psychotherapy for severely depressed patients ( [100]). The Childhood Trauma Questionnaire Short-Form (CTQ-SF; [101]) provides a quick, multidimensional, retrospective measure of childhood trauma with good reliability and validity.
Patient trauma narratives
Patients will be asked to send a written trauma narrative to the study center with 5 keywords. After the year of study, the research team will send again the keywords to the participant and will ask them to write again their memories on trauma. The trauma narrative will be written freely, with the instruction to write about their deepest thoughts and feelings about the most disturbing aspects of their childhood. Participants will be asked to write during 15 to 20 min once started. The Linguistic Inquiry Word Count (LIWC; [102]) will be applied to patient trauma narratives to investigate patient narratives about their central early trauma as well as to their dream diaries [103, 104].
Dynamic personality functioning
Psychodynamic functioning and change
The Operationalized Psychodynamic Diagnosis (OPD) is a form of multiaxial diagnostic system based on five axes: I = experience of illness and prerequisites for treatment, II = interpersonal relations, III = conflict, IV = structure and V = mental and psychosomatic disorders ( [105]). To measure change in the domain of psychodynamic functioning, we will use the short-form of this questionnaire (OPD-SF, [106]).
Dream diary
Dreams will be collected in dream diaries ideally at each follow-up points and latest at study termination with the intent to examine dream characteristics in participants with chronic depression and early trauma. Participants can write freely about their dreams. To help participants document their dreams, an exemplary table will be provided where they can write a description of their dream(s) and report on the feelings they experienced in the dream(s) as well as elements of real life associated to the dream(s). Dream characteristics and changes of the manifest content of dreams as reported in the dream diaries will be assessed using the Social Cognition and Object Relations Scale-Global Rating Method (SCORS-G; [107]) as well as the LIWC (see above).
Psychosocial functioning
Interpersonal problems
The Inventory of Interpersonal Problems (IIP; [108]) is a self-report measure of problems in interpersonal relationships. It is widely used in psychotherapy research.
Interpersonal trust
Primal trust in a helping Other has been proposed as an important feature of therapeutic interaction [47]. We will use the Trust game to measure trust and reciprocity in participants [109]. This is a paradigm drawn from behavioral economics that tests how much money a person would give to a stranger in order to potentially receive a higher amount [110].
Therapeutic Alliance
Alliance plays an important role in effective psychotherapy [111]. Alliance with the individual therapist will be assessed using the patient self-rated Working Alliance Inventory Short-Form (WAI-SR; [112]).
The Global Assessment of Functioning (GAF)
Is a numeric scale (0 through 100) used by an independent coder to rate the social, occupational and psychological level of functioning [113].
Work Ability Index (WAI-SR)
A previous study found that short- and long-term psychodynamic psychotherapy were differentially effective in improving work ability [114]. We will use the WAI to assess work ability, a questionnaire used in occupation health and research [115].
MRI Scanning MR spectroscopy (1H MRS)
Scans are acquired on 3.0 T scanners, Siemens Prisma in Frankfurt subgroup only. Spectroscopy was performed at the end of the MRI examination. An axial slice was recorded with 2D MRSI using an acquisition weighted circular phase encoding scheme on a 20 × 20 matrix, FOV of 240 × 240 mm2, 12 mm slice thickness, nominal voxel size of 12 × 12x12 mm3, TR 2000 ms, TE 40 ms, and 2 acquisitions. The volume of interest (VOI), which was selected by using the sLASER sequence from the vendor and outer volume suppression, was adjusted to contain GM and WM. Spectra were analyzed using LCModel [116]. The basis data set contained simulated spectra from Alanine, Creatine, GABA, Glucose, Glutamine, Glutamate, Glycine, Choline, Glutathion, Lactate, Mio-Inositol, N-acetyl-aspapartate-glutamate and N-Acetyl-Aspapartate.
Procedures
Data collection sites
Recruitment and treatment sites will be located in one center in the US (Los Angeles) and six centers in Europe (Germany: Frankfurt a.M., Cologne, Leipzig, Giessen, Mainz; and Switzerland: Lausanne). MRI scanning occurs in Los Angeles, Frankfurt a.M., and Lausanne. MRI data are processed in Los Angeles (CHLA). A clinical agreement has been signed and approved by each participating site.
Patient recruitment
Patients will be recruited in private psychotherapeutic and psychiatric practices, in outpatient clinics for mood disorders in hospitals. Patient flyers describing study aims and procedures will be available to potential participants with a likely diagnosis of chronic depression. Healthy controls will be recruited through informal networks. Patients with a likely diagnosis of chronic depression (BDI-II > 17) and interested healthy volunteers will be referred to the respective study center in each country and thereafter interviewed for eligibility by a research assistant.
Presentation of the study and informed consent procedures
The study will be presented to potential participants. Documents explaining the study, with its aims, procedures, benefits and risks for the participants will be provided to the participants. Interested subjects will be given a period to consider whether they would like to participate and the research team will be at their disposal to answer their eventual questions on their participation. Subjects confirming their interest in participating will then be asked to provide their informed consent to be randomly assigned to one of the treatment settings, to participate in the diagnostic, MRI, and psychometric procedures, to agree that some psychotherapy sessions are audio recorded, and agree to participate in the follow-up measurements). Participants with chronic depression and early life trauma will then be randomized in one of the two intervention groups.
Randomization
The randomization procedure will consist of a computer-generated sequence of random numbers using SPSS (SPSS Statistics, version 28), which will then be used to allocate patients to either of the 2 treatment arms. The randomization sequence will be generated and maintained by an independent study administrator in Frankfurt. Once the patient is included the ID number is communicated to the study administration in Frankfurt. On the same day, the randomization arm will be communicated to the local team and applied to the participant included.
Blinding
All the members of the investigating team (SCID /LIFE interviewers, MRI team etc.) will be blinded (they do neither know the treatment arm nor the names of the study therapists).
Rater training
SCID interviewers will be masters-level psychologists, previously trained on administration of SCID and supervised be a senior study investigators.
Manualized psychotherapeutic interventions
In the LAC study, therapists were trained in the specific treatment technique of psychoanalysis using the Tavistock Manual [117, 118], which we have modified and extended for the MODE study [119]. The MODE manual was developed by leading clinical experts of all participating sites of the study. It integrates various psychoanalytic traditions and cultures for treating chronically depressed, traumatized patients and describes high- and low-treatments. French and English translations are available.
Therapist selection and training
Both interventions will be delivered by board certified psychoanalytic therapists which have trainings and clinical experiences in low frequent and high frequent psychoanalytic therapies. Trained therapists will deliver both treatments, depending on their availability and vacancies at the time of participant enrollment. All MODE therapists are trained in the Manual [119]. Most of the study therapists in Germany have already been trained and worked in the LAC Study. Additional training will be offered for them and the new MODE study therapists of all centers in several workshops. It will include theoretical presentations, group discussion of exemplary cases, and individual case presentations. Training will be conducted by expert trainers who are qualified psychoanalysts and authors or collaborators in developing the Manual.
Clinical supervision
All study therapists will participate in monthly group supervisions or in one of the monthly “Clinical Conferences” (chairs in Germany: Marianne Leuzinger-Bohleber, Tamara Fischmann, in Lausanne: Gilles Ambresin, in SF/LA: Cheryl Goodrich), where therapists present their ongoing psychoanalyses with study patients.
Recording and transcription
A random selection of therapy sessions will be audiotaped. Adherence to the treatment protocol will be assessed by independent members of the research teams using the Comparative Psychotherapy Process Scale (CPPS; [120], see also [29]).
Power calculation
Power analyses using MRI measures from prior RCTs of medication therapy for the treatment of chronic depression [81, 82] indicated that a sample size of N = 30 participants for each of the 3 arms of the study would afford us a power of 80% to detect a moderate-to-large effect size (Cohen d = 0.5) with an α = 0.05 in each imaging modality (anatomical, task-based fMRI, resting state fMRI, and DTI).
Data analysis
Analyses will follow an intent-to-treat strategy comparing patients in the groups to which they were originally randomized.
All data will be scored and rescored by separate staff members and checked for accuracy prior to double entry into a REDCap database. Before conducting inferential statistics, we will explore data using descriptive analyses, data visualization, and examining the distributions of all imaging and clinical data. When necessary for continuous variables used as dependent variables, appropriate transformations to obtain approximate normality will be performed.
We will test a priori Primary Hypotheses in the 60 depressed participants by assessing a treatment-by-time interaction in multiple general linear models with repeated measures analyses in an intent-to-treat analysis applied to our various brain measures as dependent variables, including cortical thickness, task-based fMRI activation, resting state connectivity, and FA & ADC measures. Treatment (high vs low frequency) will be the independent variable. When testing hypotheses, we will account appropriately for the correlation of repeated measures across the two time points of measurement (baseline and 1 year) and the spatial correlation within each of our imaging measures. Covariates will include age and sex of the participants. We will examine parameter estimates and 95% confidence intervals, approximate the p-values of component terms, and estimate effect sizes in our final models. Least squares estimates (or maximum likelihood estimates) and their standard errors will be calculated for all models and plotted to assist in interpretation of significant main effects and their interactions. We will ensure that overall, study-wide Type I error-rate is maintained, correcting for multiple comparisons using False Discovery Rate (FDR). FDR-corrected p-values < 0.05 will be color-coded and displayed on a template brain.
The 30 healthy controls will be used to estimate the mean and variance of brain measures in the healthy population quantify the effects of high and low frequency psychoanalysis on brain measures and to aid their interpretation as either normalizing a previously abnormal brain measure or introducing a new brain difference that attenuates symptoms.
Missing data
We will model missing responses/covariates in our longitudinal models. We will consider missing data mechanisms, including missing completely at random, missing at random, or missing not at random, to handle missing data due to a missed assessment time point, study dropout, or unusable MRIs. The full information maximum likelihood estimation (FIML) method will be used in fitting statistical models including LMM and LVM, which allow incomplete data (i.e., cases with missing data will contribute to the analysis).
Discussion
The findings of MODE will be relevant for both clinical and basic research in identifying the brain-based mechanisms whereby psychotherapy exerts its therapeutic effects. MODE is, to our knowledge, the first study to investigate the neurobiological changes in response the effects of intensive psychoanalytic psychotherapy. MODE will thus contribute to the methodology of using MRI studies in translational psychotherapy. MODE may be the first in a series of studies combining neurobiological, psychological, and psychoanalytical approaches. It will allow us to establish outcome measures on a neural level that are perhaps more sensitive in distinguishing the differential effects of therapeutic dosing than established behavioral and clinical markers of symptom severity and change can provide.
MODE can also offer an answer to the question of why a relatively large group of patients with major depression respond poorly to treatment. Our initial studies suggest that these are patients who often suffered severe trauma before the age of 7 [51, 121]. MODE may help chronic depression patients with early trauma access a tailored treatment that addresses their specific needs. Because of the extremely high prevalence of depression in populations with early trauma, the development of effective and sustainable therapies for these difficult-to-treat patients is among the most urgent medical imperatives.
This research has a notable strength in its randomized controlled design. Yoking MRI to RCTs can identify neurobiological mechanisms predicting and causally mediating treatment response [80]. Most imaging study designs are associational and performed in samples of convenience. They therefore cannot support causal inferences for identifying disease etiology or treatment effects [80]. We hope to use the predictors that we discover to determine whether we can screen depressed patients for those biomarkers and thereby significantly improve treatment response rates in this highly treatment-resistant population. Identifying these markers will provide a framework for developing personalized care in depressed patients. Identifying the brain-based mediators of therapeutic response will support future efforts to enhance manipulation of those mediators to improve treatment response.
Availability of data and materials
The datasets generated and/or analysed during the current study will be available on reasonable request to the PIs, via the corresponding author (gilles.ambresin@chuv.ch).
Abbreviations
- BDI-II:
-
Beck Depression Inventory-II
- CTQ:
-
Childhood Trauma Questionnaire
- HF:
-
High Frequent treatment
- IIP:
-
Inventory of Interpersonal Problems
- LAC:
-
Langzeitbehandlungen chronisch Depressiver
- LF:
-
Low Frequent Treatment
- MDE:
-
Major Depressive Episode
- MDD:
-
Major Depressive Disorder
- MODE:
-
Multi-level Outcome study of psychoanalyses of therapy-refractory, chronically Depressed patients with Early trauma
- MRI:
-
Magnetic Resonance Imaging
- NT:
-
No Treatment
- OPD:
-
Operationalized Psychodynamic Diagnostics
- PAT:
-
Psycho-Analytic Treatments
- QIDS:
-
Quick Inventory of Depressive Symptoms
- RCT:
-
Randomized Controlled Trial
- SCL:
-
Symptom Checklist – 90
- SCID:
-
Structured Clinical Interview for DSM Disorders
- WAI:
-
Working Alliance Inventory
- WAIx:
-
Working Ability Index
References
Bromet E, Andrade LH, Hwang I, Sampson NA, Alonso J, De Girolamo G, De Graaf R, Demyttenaere K, Hu C, Iwata N. Cross-national epidemiology of DSM-IV major depressive episode. BMC Med. 2011;9(1):1–16.
Vandeleur CL, Fassassi S, Castelao E, Glaus J, Strippoli M-PF, Lasserre AM, Rudaz D, Gebreab S, Pistis G, Aubry J-M. Prevalence and correlates of DSM-5 major depressive and related disorders in the community. Psychiatry Res. 2017;250:50–8.
Murphy JA, Byrne GJ. Prevalence and correlates of the proposed DSM-5 diagnosis of chronic depressive disorder. J Affect Disord. 2012;139(2):172–80.
Satyanarayana S, Enns MW, Cox BJ, Sareen J. Prevalence and correlates of chronic depression in the canadian community health survey: mental health and well-being. Can J Psychiatry. 2009;54(6):389–98.
World Health O. Depression and other common mental disorders: global health estimates. Geneva: World Health Organization; 2017.
World Health Organization. Mental Health action plan 2013–2020. Geneva: World Health Organisation; 2013.
Weissman MM, Leaf PJ, Bruce ML, Florio L. The epidemiology of dysthymia in five communities: rates, risks, comorbidity, and treatment. Am J Psychiatry. 1988;145(7):815–9.
Spijker J, De Graaf R, Bijl RV, Beekman ATF, Ormel J, Nolen WA. Duration of major depressive episodes in the general population: results from the Netherlands Mental Health Survey and Incidence Study (NEMESIS). Br J Psychiatry. 2002;181(3):208–13.
Rush AJ, Trivedi MH, Wisniewski SR, Nierenberg AA, Stewart JW, Warden D, Niederehe G, Thase ME, Lavori PW, Lebowitz BD, et al. Acute and longer-term outcomes in depressed outpatients requiring one or several treatment steps: a STAR*D report. Am J Psychiatry. 2006;163(11):1905–17.
Vandeleur CL, Fassassi S, Castelao E, Glaus J, Strippoli M-PF, Lasserre AM, Rudaz D, Gebreab S, Pistis G, Aubry J-M, et al. Prevalence and correlates of DSM-5 major depressive and related disorders in the community. Psychiatry Res. 2017;250:50–8.
Steinert C, Hofmann M, Kruse J, Leichsenring F. Relapse rates after psychotherapy for depression – stable long-term effects? A meta-analysis. J Affect Disord. 2014;168:107–18.
Hung C-I, Liu C-Y, Yang C-H. Persistent depressive disorder has long-term negative impacts on depression, anxiety, and somatic symptoms at 10-year follow-up among patients with major depressive disorder. J Affect Disord. 2019;243:255–61.
Carvalho AF, Berk M, Hyphantis TN, McIntyre RS. The integrative management of treatment-resistant depression: a comprehensive review and perspectives. Psychother Psychosom. 2014;83(2):70–88.
Klein DN, Shankman SA, Rose S. Ten-year prospective follow-up study of the naturalistic course of dysthymic disorder and double depression. Am J Psychiatry. 2006;163(5):872–80.
Ambresin G, Strippoli M-PF, Vandeleur CL, de Roten Y, Despland J-N, Preisig M. Correlates of chronic depression in the general population: results from the CoLaus|PsyCoLaus study. Soc Psychiatry Psychiatr Epidemiol. 2023;58(8):1179–91.
Laezer KL, Tischer I, Gaertner B, Leuzinger-Bohleber M. Aufwendige Langzeit-Psychotherapie und kostengünstige medikamentengestützte Verhaltenstherapie im Vergleich. Gesundheitsökonomie & Qualitätsmanagement. 2015;20(04):178–85.
Jobst A, Brakemeier E-L, Buchheim A, Caspar F, Cuijpers P, Ebmeier K, Falkai P, van der Gaag RJ, Gaebel W, Herpertz S. European Psychiatric Association Guidance on psychotherapy in chronic depression across Europe. Eur Psychiatry. 2016;33:18–36.
Ambresin G, Despland J-N, Preisig M, de Roten Y. Efficacy of an adjunctive brief psychodynamic psychotherapy to usual inpatient treatment of depression: rationale and design of a randomized controlled trial. BMC Psychiatry. 2012;12(1):1–9.
Ambresin G, De Coulon N, De Roten Y, Despland J-N. Brief psychodynamic psychotherapy for patients hospitalized for depression. Psychothérapies. 2009;29(2):75–84.
Cuijpers P. Four decades of outcome research on psychotherapies for adult depression: an overview of a series of meta-analyses. Can Psychol. 2017;58(1):7.
Cuijpers P, Huibers MJ, Furukawa TA. The need for research on treatments of chronic depression. JAMA Psychiat. 2017;74(3):242–3.
Cuijpers P, Noma H, Karyotaki E, Vinkers CH, Cipriani A, Furukawa TA. A network meta-analysis of the effects of psychotherapies, pharmacotherapies and their combination in the treatment of adult depression. World Psychiatry. 2020;19(1):92–107.
Driessen E, Cuijpers P, de Maat SC, Abbass AA, de Jonghe F, Dekker JJ. The efficacy of short-term psychodynamic psychotherapy for depression: a meta-analysis. Clin Psychol Rev. 2010;30(1):25–36.
Leichsenring F, Rabung S. Effectiveness of long-term psychodynamic psychotherapy: a meta-analysis. JAMA. 2008;300(13):1551–65.
Leichsenring F, Abbass A, Luyten P, Hilsenroth M, Rabung S. The emerging evidence for long-term psychodynamic therapy. Psychodyn Psychiatry. 2013;41(3):361–84.
Solomonov N, Barber JP. What we know, what we do not know, and where are we heading? Efficacy and acceptability of psychological interventions for depression. Epidemiol Psychiatric Sci. 2016;25(4):301–8.
Caligor E, Kernberg OF, Clarkin JF, Yeomans FE. Psychodynamic therapy for personality pathology: Treating self and interpersonal functioning. Washington D.C.: American Psychiatric Association Publishing; 2018.
Luyten P, Blatt SJ. Psychodynamic treatment of depression. Psychiatric Clin. 2012;35(1):111–29.
Leuzinger-Bohleber M, Hautzinger M, Fiedler G, Keller W, Bahrke U, Kallenbach L, Kaufhold J, Ernst M, Negele A, Schoett M. Outcome of psychoanalytic and cognitive-behavioural long-term therapy with chronically depressed patients: a controlled trial with preferential and randomized allocation. Can J Psychiatry. 2019;64(1):47–58.
Leuzinger-Bohleber M, Kaufhold J, Kallenbach L, Negele A, Ernst M, Keller W, Fiedler G, Hautzinger M, Bahrke U, Beutel M. How to measure sustained psychic transformations in long-term treatments of chronically depressed patients: symptomatic and structural changes in the LAC depression study of the outcome of cognitive-behavioural and psychoanalytic long-term treatments. Int J Psychoanal. 2019;100(1):99–127.
Rössler-Schülein H, Löffler-Stastka H. Methoden Psychoanalyse und psychoanalytische psychotherapie – Unterschiede und Gemeinsamkeiten. Neuropsychiatr. 2013;27(4):180–7.
Blomberg J, Lazar A, Sandell R. Long-term outcome of long-term psychoanalytically oriented therapies: first findings of the Stockholm outcome of psychotherapy and psychoanalysis study. Psychother Res. 2001;11(4):361–82.
Leichsenring F, Schauenburg H. Empirically supported methods of short-term psychodynamic therapy in depression – towards an evidence-based unified protocol. J Affect Disord. 2014;169:128–43.
Huber D, Zimmermann J, Henrich G, Klug G. Comparison of cognitive-behaviour therapy with psychoanalytic and psychodynamic therapy for depressed patients–a three-year follow-up study. Z Psychosom Med Psychother. 2012;58(3):299–316.
Huber TJ. Stationäre Depressionsbehandlung. Soll man Psychotherapie und Medikamente kombinieren? Der Nervenarzt. 2005;76(3):270–7.
Knekt P, Lindfors O, Laaksonen MA, Renlund C, Haaramo P, Härkänen T, Virtala E, Group HPS. Quasi-experimental study on the effectiveness of psychoanalysis, long-term and short-term psychotherapy on psychiatric symptoms, work ability and functional capacity during a 5-year follow-up. J Affect Disord. 2011;132(1–2):37–47.
Knekt P, Lindfors O, Renlund C, Sares-Jäske L, Laaksonen MA, Virtala E. Use of auxiliary psychiatric treatment during a 5-year follow-up among patients receiving short-or long-term psychotherapy. J Affect Disord. 2011;135(1–3):221–30.
Knekt P, Virtala E, Härkänen T, Vaarama M, Lehtonen J, Lindfors O. The outcome of short-and long-term psychotherapy 10 years after start of treatment. Psychol Med. 2016;46(6):1175–88.
Fonagy P. The effectiveness of psychodynamic psychotherapies: an update. World Psychiatry. 2015;14(2):137–50.
Leuzinger-Bohleber M, Kächele H. An open door review of outcome and process studies in psychoanalysis. London: International Psychoanalytical Association; 2015.
National Institute for Health and Clinical Excellence. Depression: the treatment and management of depression in adults. In: Edited by NHS. London: NHS; 2009. (Updated 2016).
Beutel ME, Leuzinger-Bohleber M, Rüger B, Bahrke U, Negele A, Haselbacher A, Fiedler G, Keller W, Hautzinger M. Psychoanalytic and cognitive-behavior therapy of chronic depression: study protocol for a randomized controlled trial. Trials. 2012;13(1):1–8.
Leuzinger-Bohleber M. Working with severely traumatized, chronically depressed analysands. Int J Psychoanal. 2015;96(3):611–36.
Leuzinger-Bohleber M, Grabhorn A, Bahrke U. Was nur erzählt und nicht gemessen werden kann: Einblicke in psychoanalytische Langzeitbehandlungen chronischer depressionen. Giessen: Psychosozial-Verlag; 2020.
Bleichmar H. Rethinking pathological mourning: multiple types and therapeutic approaches. Psychoanal Q. 2010;79(1):71–94.
Leuzinger-Bohleber M. ‘... I Feel Very Alien and Forever Alien in This World...’ (Susan Taubes) Depression – An Illness of Ideals and Trauma. Bulletin of the European Psychoanalytical Federation. 2022;76:23.
Fonagy P, Luyten P, Allison E, Campbell C. Mentalizing, epistemic trust and the phenomenology of psychotherapy. Psychopathology. 2019;52(2):94–103.
Bohleber W, Leuzinger-Bohleber M. The special problem of interpretation in the treatment of traumatized patients. Psychoanal Inq. 2016;36(1):60–76.
Selous C, Kelly-Irving M, Maughan B, Eyre O, Rice F, Collishaw S. Adverse childhood experiences and adult mood problems: evidence from a five-decade prospective birth cohort. Psychol Med. 2020;50(14):2444–51.
Nemeroff CB, Heim CM, Thase ME, Klein DN, Rush AJ, Schatzberg AF, Ninan PT, McCullough JP, Weiss PM, Dunner DL. Differential responses to psychotherapy versus pharmacotherapy in patients with chronic forms of major depression and childhood trauma. Proc Natl Acad Sci. 2003;100:14293.
Mandelli L, Petrelli C, Serretti A. The role of specific early trauma in adult depression: a meta-analysis of published literature. Childhood trauma and adult depression. Eur Psychiatry. 2015;30(6):665–80.
Negele A, Kaufhold J, Kallenbach L, Leuzinger-Bohleber M. Childhood trauma and its relation to chronic depression in adulthood. Depress Res Treat. 2015;2015:650804.
Cuijpers P, van Straten A, Schuurmans J, van Oppen P, Hollon SD, Andersson G. Psychotherapy for chronic major depression and dysthymia: a meta-analysis. Clin Psychol Rev. 2010;30(1):51–62.
Zimmermann J, Löffler-Stastka H, Huber D, Klug G, Alhabbo S, Bock A, Benecke C. Is it all about the higher dose? Why psychoanalytic therapy is an effective treatment for major depression. Clin Psychol Psychother. 2015;22(6):469–87.
Wade-Bohleber LM, Boeker H, Grimm S, Gärtner M, Ernst J, Recher DA, Buergi N, Seifritz E, Richter A. Depression is associated with hyperconnectivity of an introspective socio-affective network during the recall of formative relationship episodes. J Affect Disord. 2020;274:522–34.
Buchheim A, Kächele H. Psychoanalyse im Spannungsfeld neurowissenschaftlicher Forschung. Zeitschrift für Psychiatrie, Psychologie und Psychotherapie. 2015;63(2):89–96.
Buchheim A, Viviani R, Kessler H, Kächele H, Cierpka M, Roth G, George C, Kernberg OF, Bruns G, Taubner S. Changes in prefrontal-limbic function in major depression after 15 months of long-term psychotherapy. PLoS One. 2012;7(3):e33745.
Boeker H, Richter A, Himmighoffen H, Ernst J, Bohleber L, Hofmann E, Vetter J, Northoff G. Essentials of psychoanalytic process and change: how can we investigate the neural effects of psychodynamic psychotherapy in individualized neuro-imaging? Front Hum Neurosci. 2013;7:355.
Boeker H, Kraehenmann R. Neuropsychodynamic approach to depression: integrating resting state dysfunctions of the brain and disturbed self-related processes. Front Hum Neurosci. 2018;12:247.
Boeker H, Northoff G. Psychotherapy Research in the Context of Neuroscience. In: Neuropsychodynamic Psychiatry. edn. Edited by Boeker H, Hartwich P, Northoff G. Cham: Springer International Publishing; 2018. p. 531–62.
Huang X, Huang P, Li D, Zhang Y, Wang T, Mu J, Li Q, Xie P. Early brain changes associated with psychotherapy in major depressive disorder revealed by resting-state fMRI: evidence for the top-down regulation theory. Int J Psychophysiol. 2014;94(3):437–44.
Klein JP, Becker B, Hurlemann R, Scheibe C, Colla M, Heuser I. Effect of specific psychotherapy for chronic depression on neural responses to emotional faces. J Affect Disord. 2014;166:93–7.
Sankar A, Scott J, Paszkiewicz A, Giampietro VP, Steiner H, Fu CHY. Neural effects of cognitive–behavioural therapy on dysfunctional attitudes in depression. Psychol Med. 2015;45(7):1425–33.
Straub J, Metzger CD, Plener PL, Koelch MG, Groen G, Abler B. Successful group psychotherapy of depression in adolescents alters fronto-limbic resting-state connectivity. J Affect Disord. 2017;209:135–9.
Wiswede D, Taubner S, Buchheim A, Münte TF, Stasch M, Cierpka M, Kächele H, Roth G, Erhard P, Kessler H. Tracking functional brain changes in patients with depression under psychodynamic psychotherapy using individualized stimuli. PLoS One. 2014;9(10):e109037.
Yoshimura S, Okamoto Y, Onoda K, Matsunaga M, Okada G, Kunisato Y, Yoshino A, Ueda K, Suzuki S-I, Yamawaki S. Cognitive behavioral therapy for depression changes medial prefrontal and ventral anterior cingulate cortex activity associated with self-referential processing. Soc Cogn Affect Neurosci. 2014;9(4):487–93.
Lueken U, Hahn T. Functional neuroimaging of psychotherapeutic processes in anxiety and depression: from mechanisms to predictions. Curr Opin Psychiatry. 2016;29(1):25–31.
Fu CH, Steiner H, Costafreda SG. Predictive neural biomarkers of clinical response in depression: a meta-analysis of functional and structural neuroimaging studies of pharmacological and psychological therapies. Neurobiol Dis. 2013;52:75–83.
Marwood L, Wise T, Perkins AM, Cleare AJ. Meta-analyses of the neural mechanisms and predictors of response to psychotherapy in depression and anxiety. Neurosci Biobehav Rev. 2018;95:61–72.
Messina I, Sambin M, Palmieri A, Viviani R. Neural correlates of psychotherapy in anxiety and depression: a meta-analysis. PLoS One. 2013;8(9):e74657.
Cristea IA, Karyotaki E, Hollon SD, Cuijpers P, Gentili C. Biological markers evaluated in randomized trials of psychological treatments for depression: a systematic review and meta-analysis. Neurosci Biobehav Rev. 2019;101:32–44.
Fischmann T, Russ MO, Baehr T, Stirn A, Singer W. Veränderungen der Gehirnfunktion bei chronisch Depressiven nach psychoanalytischen und kognitiv-behavioralen Langzeitbehandlungen. In: Depression und Neuroplastizität: psychoanalytische Klinik und Forschung edn. Edited by Leuzinger-Bohleber M (Ed.) Frankfurt a. M.: Brandes & Apsel Verlag; 2010. p. 162–85.
Fischmann T, Ambresin G, Leuzinger-Bohleber M. Dreams and trauma changes in the manifest dreams in psychoanalytic treatments–a psychoanalytic outcome measure. Front Psychol. 2021;12:678440.
Fischmann T, Russ M, Baehr T, Stirn A, Leuzinger-Bohleber M. Changes in dreams of chronic depressed patients: the Frankfurt fMRI/EEG study (FRED). In: The Significance of Dreams Bridging Clinical and Extraclinical Research in Psychoanalysis. edn. Edited by P. Fonagy HK, M. Leuzinger-Bohleber, & D. Taylor (Eds.). London: Routledge; 2012. p. 159–84.
Fischmann T, Russ MO, Leuzinger-Bohleber M. Trauma, dream, and psychic change in psychoanalyses: a dialog between psychoanalysis and the neurosciences. Front Hum Neurosci. 2013;7:877.
Selleck MJ, Senthil M, Wall NR. Making meaningful clinical use of biomarkers. Biomark Insights. 2017;12:1177271917715236.
Insel TR. The NIMH experimental medicine initiative. World Psychiatry. 2015;14(2):151.
Insel TR, Gogtay N. National Institute of Mental Health clinical trials: new opportunities, new expectations. JAMA Psychiat. 2014;71(7):745–6.
Gordon JA. From neurobiology to novel medications: a principled approach to translation. Am J Psychiatry. 2019;176(6):425–7.
Horga G, Kaur T, Peterson BS. Annual research review: current limitations and future directions in MRI studies of child- and adult-onset developmental psychopathologies. J Child Psychol Psychiatry. 2014;55(6):659–80.
Bansal R, Hellerstein DJ, Peterson BS. Evidence for neuroplastic compensation in the cerebral cortex of persons with depressive illness. Mol Psychiatry. 2018;23(2):375–83.
Posner J, Hellerstein DJ, Gat I, Mechling A, Klahr K, Wang Z, McGrath PJ, Stewart JW, Peterson BS. Antidepressants normalize the default mode network in patients with dysthymia. JAMA Psychiat. 2013;70(4):373–82.
Bertholdo D, Watcharakorn A, Castillo M. Brain proton magnetic resonance spectroscopy: introduction and overview. Neuroimaging Clinics. 2013;23(3):359–80.
Rae CD. A guide to the metabolic pathways and function of metabolites observed in human brain 1 H magnetic resonance spectra. Neurochem Res. 2014;39:1–36.
Munder T, Brütsch O, Leonhart R, Gerger H, Barth J. Researcher allegiance in psychotherapy outcome research: an overview of reviews. Clin Psychol Rev. 2013;33(4):501–11.
Leuzinger-Bohleber M, Ambresin G, Fischmann T, Solms M. On the Dark Side of Chronic Depression: Psychoanalytic, Social-cultural and Research Approaches: Taylor & Francis; 2022.
Ogawa S, Tank DW, Menon R, Ellermann JM, Kim SG, Merkle H, Ugurbil K. Intrinsic signal changes accompanying sensory stimulation: functional brain mapping with magnetic resonance imaging. Proc Natl Acad Sci. 1992;89(13):5951–5.
Heeger DJ, Huk AC, Geisler WS, Albrecht DG. Spikes versus BOLD: what does neuroimaging tell us about neuronal activity? Nat Neurosci. 2000;3(7):631–3.
Abraham N, Torok M. Mourning or melancholia: introjection versus incorporation. In: The Shell and the Kernel: renewals of psychoanalysis. Volume 1, edn.: University of Chicago Press; 1994. p. 125–138.
Eisenberger NI, Lieberman MD, Williams KD. Does rejection hurt? An fMRI study of social exclusion. Science. 2003;302(5643):290–2.
Cacioppo S, Frum C, Asp E, Weiss RM, Lewis JW, Cacioppo JT. A quantitative meta-analysis of functional imaging studies of social rejection. Sci Rep. 2013;3(1):2027.
Rotge J-Y, Lemogne C, Hinfray S, Huguet P, Grynszpan O, Tartour E, George N, Fossati P. A meta-analysis of the anterior cingulate contribution to social pain. Soc Cogn Affect Neurosci. 2015;10(1):19–27.
Wang H, Braun C, Enck P. How the brain reacts to social stress (exclusion)–a scoping review. Neurosci Biobehav Rev. 2017;80:80–8.
Perry JC, Banon E, Ianni F. Effectiveness of psychotherapy for personality disorders. Am J Psychiatry. 1999;156(9):1312–21.
First MB, Gibbon M. The structured clinical interview for DSM-IV axis I disorders (SCID-I) and the structured clinical interview for DSM-IV axis II disorders (SCID-II). 2004.
Rush AJ, Trivedi MH, Ibrahim HM, Carmody TJ, Arnow B, Klein DN, et al. The 16-Item Quick Inventory of Depressive Symptomatology (QIDS), clinician rating (QIDS-C), and self-report (QIDS-SR): a psychometric evaluation in patients with chronic major depression. Biol Psychiatry. 2003;54(5):573–83.
Beck AT, Steer RA, Ball RA, Ranieri WF. Comparison of Beck depression inventories IA and –II in psychiatric outpatients. Journal of Psychological Assessment. 1996;67(3):588–97.
Blatt SJ, DA J, Quinlan DM. Depressive Experiences QuestionnaireBlatt SJ, D’Afflitti J, Quinlan DM. Yale University; 1979.
Derogatis LR, Rickels K, Rock AF. The SCL-90 and the MMPI: a step in the validation of a new self-report scale. Br J Psychiatry. 1976;128(3):280–9.
Nemeroff CB, Heim CM, Thase ME, Klein DN, Rush AJ, Schatzberg AF, et al. Differential responses to psychotherapy versus pharmacotherapy in patients with chronic forms of major depression and childhood trauma. Proc Natl Acad Sci USA. 2003;100(24):14293–6.
Bernstein DP, Stein JA, Newcomb MD, Walker E, Pogge D, Ahluvalia T, Stokes J, Handelsman L, Medrano M, Desmond D. Development and validation of a brief screening version of the childhood trauma questionnaire. Child Abuse Negl. 2003;27.
Hawkins RC II, Boyd RL. Such stuff as dreams are made on: dream language, LIWC norms, and personality correlates. Dreaming. 2017;27(2):102.
Pennebaker JW. Writing about emotional experiences as a therapeutic process. Psychol Sci. 1997;8(3):162–6.
Pennebaker JW. The secret life of pronouns: What our words say about us. New York: Bloomsbury Press; 2011.
Ehrenthal JC, Benecke C: Tailored treatment planning for individuals with personality disorders: the operationalized psychodynamic diagnosis (OPD) approach. In: Case formulation for personality disorders. edn.: Elsevier; 2019. p. 291–314.
Ehrenthal JC, Dinger U, Horsch L, Komo-Lang M, Klinkerfuss M, Grande T, et al. The OPD Structure Questionnaire (OPD-SQ): first results on reliability and validity. Psychother Psychosom Med Psychol. 2012;62(1):25–32.
Stein M, Slavin-Mulford J. The Social Cognition and Object Relations Scale-Global rating method (SCORS-G): A comprehensive guide for clinicians and researchers. London: Routledge; 2017.
Horowitz LM, Rosenberg SE, Baer BA, Ureno G, Villasenor VS. Inventory of interpersonal problems: psychometric properties and clinical applications. J Consult Clin Psychol. 1988;56.
Robson SE, Repetto L, Gountouna V-E, Nicodemus KK. A review of neuroeconomic gameplay in psychiatric disorders. Mol Psychiatry. 2020;25(1):67–81.
Berg J, Dickhaut J, McCabe K. Trust, reciprocity, and social history. Games Econom Behav. 1995;10(1):122–42.
Baier AL, Kline AC, Feeny NC. Therapeutic alliance as a mediator of change: a systematic review and evaluation of research. Clin Psychol Rev. 2020;82:101921.
Hatcher RL, Gillaspy JA. Development and validation of a revised short version of the working alliance inventory. Psychother Res. 2006;16(1):12–25.
Piersma HL, Boes JL. The GAF and psychiatric outcome: a descriptive report. Community Ment Health J. 1997;33:35–41.
Knekt P, Lindfors O, Laaksonen MA, Raitasalo R, Haaramo P, Järvikoski A, Group HPS. Effectiveness of short-term and long-term psychotherapy on work ability and functional capacity—a randomized clinical trial on depressive and anxiety disorders. J Affect Disord. 2008;107(1–3):95–106.
Tuomi K, Ilmarinen J, Jahkola A, Tulkki A. Work Ability Index. Helsinki: The Finnish Institute of Occupational Health; 1998.
Provencher SW. Estimation of metabolite concentrations from localized in vivo proton NMR spectra. Magn Reson Med. 1993;30(6):672–9.
Taylor D. Das Tavistock-Manual der psychoanalytischen Psychotherapie – unter besonderer Berücksichtigung der chronischen Depression. Psyche (Stuttg). 2010;64:833–61.
Taylor D. Treatment manuals and the advancement of psychoanalytic knowledge: The treatment manual of the tavistock adult depression study. Int J Psychoanal. 2015;96(3):845–75.
Leuzinger-Bohleber M, Fischmann T, Beutel ME: Chronische Depression: Analytische Langzeitpsychotherapie, vol. 12: Hogrefe Verlag GmbH & Company KG; 2022.
Hilsenroth MJ, Blagys MD, Ackerman SJ, Bonge DR, Blais MA. Measuring psychodynamic-interpersonal and cognitive-behavioral techniques: development of the comparative psychotherapy process scale. Psychother Theory Res Pract Train. 2005;42(3):340.
Williams LM, Debattista C, Duchemin A, Schatzberg AF, Nemeroff CB. Childhood trauma predicts antidepressant response in adults with major depression: data from the randomized international study to predict optimized treatment for depression. Transl Psychiatry. 2016;6(5):e799–e799.
Acknowledgements
We thank Mark Solms, Charles Fischer, Harriet Wolfe, Cheryl Goodrich, Linda Goodman, Bart Blinder, Jean Nicolas Despland, Nicolas de Coulon, Erwin Sturm, Lisa Kallenbach-Kaminski, Andju Labuhn, Elisabeth Imhorst, Christine Huth, Serge Croes, Silvia Janko-Milch, Manfred Beutel as well as 72 psychoanalysts in our different sites which are supporting MODE as study therapists. Thanks also to our research and administrative team, Suzanne Badan, Maria Jose Gonzalez, Anne Schorr, Sun Bernice, Nicoletta Zuccarini, Siddhant Sawardekar, and our PhD students Nadine Montigny, Julia Wichelmann, Marielle Donié, Terry Meyer.
Study registration
DRKS-ID: DRKS00016872.
Date of Registration in DRKS: 2019/03/12 Last update 2023/01/30.
Universal Trial Number (UTN): U1111-1229-2321.
Funding
Open access funding provided by University of Lausanne This study is funded by grants of the International Psychoanalytic Association, the American Psychoanalytic Association, the Alfred Berman Foundation for Medical Research, and the Wallerstein foundation (The Robert S. Wallerstein Fellowship in Psychoanalytic Research) and the German Psychoanalytic Association. No funding body had a role in study design; the collection, analysis, and interpretation of data; the preparation, review, or approval of the manuscript; or the decision to submit this manuscript for publication.
Author information
Authors and Affiliations
Contributions
MLB and BSP both international principal investigators and sponsors for the study conceived the study. MLB, BSP, GA, RB, NA, EH and TF developed the design of the study. GA, MLB, and BSP were major contributors in writing the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Ethics approval For the main study (current protocol), the ethics committee in Frankfurt gave its approval on August 14th, 2023. In Los Angeles, the original protocol was amended to correspond to the German main study protocol and has been accepted by the local ethics committee on June 6th, 2023. In Lausanne, the ethic committee from the Canton de Vaud gave its approval for the similarly amended protocol on September 5th, 2023. As regards, the feasibility study, in Frankfurt, the ethics committee gave its approval for the pilot study on March 16th, 2020 and for the main study August 14th, 2023. In Los Angeles, the protocol has been accepted by the local ethics committee on June 10th, 2020. In Lausanne, the ethic committee from the Canton de Vaud gave its approval on February 18th, 2021.
Consent to participate Patients and healthy controls signed an informed consent form in accordance with local law requirements.
In the US site, the participant will also be given a copy of HIPAA, and Experimental Bill of Rights to read and sign in accordance with California State Law.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: Supplementary Table 1.
MODE study. Trial registration data.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Ambresin, G., Leuzinger-Bohleber, M., Fischmann, T. et al. The multi-level outcome study of psychoanalysis for chronically depressed patients with early trauma (MODE): rationale and design of an international multicenter randomized controlled trial. BMC Psychiatry 23, 844 (2023). https://doi.org/10.1186/s12888-023-05287-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12888-023-05287-6