
Abstract
Background
Literature has typically associated delusional disorder with a poorer prognosis relative to schizophrenia, without considering the confounding effect of age despite the differential age of onset. This study therefore aims to investigate the diagnostic stability, clinical, functional, and neurocognitive differences of Chinese first-episode psychosis age-matched patients with delusional disorder and schizophrenia at four years.
Methods
71 delusional disorder and 71 age-matched schizophrenia patients were followed up for four years after their initial episode. Their symptoms, insight in psychosis, side effects of medication, medication compliance, functioning, and neurocognitive performance were assessed at four years.
Results
At four years, 65% of DD patients maintained the same diagnosis, while the rest shifted to SZ. Only those without a diagnostic shift were included in the analysis. Delusional disorder patients (n = 46) experienced greater general psychopathology and poorer insight, but better attitude towards medication than schizophrenia patients (n = 71). Social and occupational functioning, quality of life, and cognitive functioning, however, were similar in delusional disorder and schizophrenia patients.
Conclusions
Results indicate that delusional disorder is less diagnostically stable than schizophrenia. Their outcomes in a Chinese population were largely similar at four years after removing the confounding age factor, implying that delusional disorder and schizophrenia may not be as distinct as previously thought.
Similar content being viewed by others


Introduction
Delusions can be defined as strongly-held abnormal beliefs that are bizarre and impervious to evidence, and which may be categorised according to their contents [1]. In the past, delusional disorder (DD) was differentiated from schizophrenia (SZ) by the requirement of non-bizarre delusions without hallucinations [2,3,4]. However, the DSM-V [5] now allows for bizarre delusions or relevant non-prominent hallucinations to co-occur with delusion(s). With the boundaries becoming less distinct, it is important to clarify the differences between DD and SZ for diagnostic accuracy and the optimisation of clinical treatment and management of patients.
Previous research have suggested that compared to SZ, DD is associated with a greater predominance of jealousy and somatic delusions [6], little or non-existent hallucinations [7], and less cognitive and negative symptoms [8]. These findings generally indicate DD as a milder psychotic disorder than SZ, supporting the idea of a psychosis spectrum that may encompass DD, SZ, and schizoaffective disorder in escalating severity [8].
In terms of longitudinal stability, only 59% of DD patients maintained the same diagnosis at follow-up, with approximately one-third later diagnosed with SZ [9]. In fact, 93% of diagnostic changes within the SZ spectrum occurred towards SZ. Therefore, refining their longitudinal clinical characterisation and profiling may contribute towards the debate of a categorical or a dimensional descriptive approach, where DD may be better subsumed under SZ [10].
Comparisons between DD and SZ cohorts
Few studies have compared DD with other psychoses due to recruitment difficulties. On top of its low prevalence, DD is often associated with relatively better functioning and a poorer insight which may prevent help seeking behaviour. Methodological constraints and mixed findings further prevent a conclusion from being drawn.
One relevant seminal review of 17 Western studies suggested that DD patients were more likely to be females, married, an immigrant, socially disadvantaged, and have an older age of onset and shorter hospitalisation [11]. However, the included studies dated before the standardisation of DD diagnostic criteria, and therefore lacked appreciation for the different manifestations of the disorder. Other studies suggest a comparable co-morbidity rate with affective disorders and suicidal behaviour between DD and SZ [12, 13], though DD demonstrates a greater susceptibility to physical conditions [14] than SZ [15].
From a functioning perspective however, later studies indicate DD patients to display better social functioning than those with SZ. A longitudinal German study concluded great dissimilarity between DD and paranoid SZ in family history for mental disorders, age of onset, illness course, symptoms, and outcomes [16]. However, only inpatients were included which may have introduced sampling bias with patients who are females and experienced a later onset with more severe symptoms. Another comparative study of DD, paranoid SZ, and non-paranoid SZ in Spain has also indicated DD to be associated with an older age of onset and at index admission, better premorbid adjustment, poorer antipsychotic response, greater likelihood of being married, fewer hospitalisations, and better overall functioning [6].
Adjusting for age in the exploration of DD vs. SZ differences
Evidence presenting DD and SZ as distinct entities often fails to consider a potentially important confounder – age. Age represents a key prognostic factor in psychosis [17], as older adults are more likely to have established social networks and occupational achievements. Given DD’s older age of onset, comparative studies to other psychoses without adjusting for age may be more inclined to find better premorbid adjustment and functioning in DD.
Indeed, no significant differences in symptom severity, functioning, or neurocognitive performance were found between age-matched DD and SZ patients, except that the former was more likely to be married and have less premorbid schizoid and schizotypal traits [18]. However, another cross-sectional study reports better global functioning in DD than SZ despite age adjustments [7]. With such inconsistent findings, there is a need to further investigate if DD is distinct from SZ in age-matched studies, or whether an extension of the psychosis spectrum is more appropriate. The diagnostic instability of DD further compels the necessity of such research [9], especially given the almost exclusive focus on Western samples thus far. This study aims to investigate the diagnostic stability and the differences in clinical, functional, and neurocognitive outcomes between age-matched DD and SZ cohorts in Hong Kong from Hui et al.’s study [18] at four years.
Methods
Study design and participants
Participants were recruited from a population-based, territory-wide Jockey Club Early Psychosis (JCEP) study involving 360 adult patients with first-episode psychosis (FEP), where they were randomized to receive either two or four years of early intervention, or four years of standard care treatment in Hong Kong [19, 20]. Participants were included in the JCEP study if they had received antipsychotic treatment for no longer than 12 months since their first episode; were aged 26–55; were ethnically Chinese and spoke Cantonese; and met the DSM-IV [3] diagnostic criteria for schizophrenia, schizophreniform disorder, schizoaffective disorder, delusional disorder, brief psychotic disorder, psychotic disorder not otherwise specified, or manic episodes with psychotic features. Exclusion criteria include organic brain conditions, substance-induced psychoses, a known history of intellectual disability, and suicidal/violent risks.
As part of this 4-year trial, the baseline characteristics between age-matched patients with DD (N = 71) and SZ (N = 71) were analyzed in a previous study [18]. The current analysis further examines the four-year outcomes of these DD and SZ patients (Fig. 1). Diagnostic ascertainment was achieved using the validated Chinese version of the Structured Clinical Interview for DSM-IV [21], medical records, and illness history taken from informants and JCEP case workers. Two experienced psychiatrists further confirmed the diagnosis by using the best-estimate consensus approach [22]. Diagnosis of DD and SZ was similarly reassessed at 4 years by psychiatrists.

Flow diagram of patients at each phase of the study
The ethics of the study were approved by the Institutional Review Board at each study site and was carried out in accordance with Good Clinical Practice as well as the Declaration of Helsinki. All participants provided written informed consent.
Assessments
Demographic information was sampled from baseline. The following clinical and functioning measures were also evaluated at baseline and at four years.
Symptoms of psychosis were assessed using the Positive and Negative Syndrome Scale (PANSS) [23]. Depressive and mania symptoms were assessed using the Calgary Depression Scale for Schizophrenia (CDSS) [24] and the Young Mania Rating Scale (YMRS) [25].
Insight was measured using the shortened Scale to assess Unawareness of Mental Disorder (SUMD) [26]. Medication side effects and adherence were assessed by the Simpson-Angus Scale (SAS) [27], the Abnormal Involuntary Movement Scale (AIMS) [28], the Barnes Akathisia Rating Scale (BARNS) [29], the Udvalg for Kliniske Undersøgelser (UKU) [30], and the Medication Compliance Questionnaire, a modified Cantonese version of the Medication Adherence Rating Scale [31].
Functioning and quality of life were indicated using the Social Occupational Functioning Assessment Scale (SOFAS) [32], the Role Functioning Scale (RFS) [33], and the 12-item Short Form health survey (SF-12) [34]. Neurocognitive performance was assessed using the Digit Symbol Substitution, Logical Memory, Verbal Fluency and Visual Patterns, and Wisconsin Card Sorting tests.
Statistical analysis
Analysis was carried out using IBM® SPSS® Version 24.0. Patients with a diagnostic change at four-year were excluded from analysis.
Baseline comparisons between the DD and SZ cohorts were conducted using independent sample t-tests and Mann-Whitney U tests for continuous variables, and Chi-Squared tests for categorical variables. Significant variables (i.e., years of intervention received) were statistically controlled for in subsequent analyses.
Outcome differences were evaluated using binary logistic regression for categorical variables and linear regression for continuous variables. In total, 10 patients (n = 5 DD; n = 5 SZ) were lost to follow-up at four years due to death (n = 6), withdrawal of consent (n = 2), or other reasons (n = 2) (Fig. 1). Their outcomes were therefore excluded from the four-year comparative analysis. Analysis was repeated to compare pure DD and SZ patients from the JCEP cohort at baseline and at 4-year, without matching for age [20]. To reduce the probability of falsely rejecting a null hypothesis during multiple testing, a false discovery rate (q-value) of 10% with the Benjamini-Hochberg procedure was used [35].
Results
Baseline comparisons
There were no statistical baseline differences in age, sex, employment status, years of education, duration of untreated psychosis (DUP), and medication intake between DD and SZ, nor in clinical symptoms or functioning at baseline (Table 1). However, patients with DD received more years of JCEP intervention.
Diagnostic stability
Only patients with a pure diagnosis across the four years were included in the outcome analyses (Fig. 1). Patients who were diagnosed with SZ at baseline all remained as such at four years. Amongst the 71 DD patients, 46 (65%) maintained the same diagnosis while 25 (35%) shifted to a SZ diagnosis at four years. There was no statistical difference in the demographics, DUP, or clinical symptoms at baseline between patients with and without a diagnostic shift (see Additional File 1).
Clinical outcomes
DD patients had significantly higher PANSS general psychopathology sub-scores at four years (Table 2). No significant differences were found between the two groups in positive, negative, depressive, and mania symptoms. Although there were no differences between the two groups in total antipsychotics intake dosage and side effects, DD patients exhibited better attitude towards medication (Table 3). DD patients also had significantly higher SUMD total and item scores indicating a more impaired insight than SZ patients.
Functioning and neurocognitive outcomes
At four years, DD and SZ patients showed no statistical differences in occupational status, functioning, neurocognitive performance, and quality of life (Table 4).
Overall, aside from attitude towards medication, group differences remained significant for general psychopathology and insight in mental disorder after corrections using the Benjamini-Hochberg procedure [35].
In order to evaluate whether matched and non-matched samples would yield differential outcomes, analyses were repeated for all DD (n = 72) and SZ (n = 157) patients from the JCEP cohort [20] without matching for age (see Additional File 2). As expected, DD and SZ cohorts showed significant baseline differences in age and employment status. Attitude towards medication did not differ in non-matched patients after controlling for employment status. However, differences relating to general psychopathology and insight remained significant.
Discussion
Previous studies comparing the outcomes of DD and SZ patients have either only included inpatients or neglected to match for a crucial prognostic factor in schizophrenia – age. Continuing from an earlier cross-sectional study on Chinese patients [18], this was the first prospective study investigating the diagnostic stability and clinical, functional, and neurocognitive differences between age-matched DD and SZ Chinese cohorts at four years.
Notably, few studies have explored DD and SZ in non-Western populations despite potential cultural differences. For instance, familial support may be more accessible in Hong Kong considering that 87% of FEP patients live in a family household [36]. Such support may be especially important given that 42% of patients require medication reminders by family members or carers [37], Indeed, only 26% of patients with SZ demonstrate non-adherence to medication in Hong Kong [38] in comparison to 50% in Western countries [39]. However, the stigmatisation of psychosis in Hong Kong [40] may lead to poorer social and occupational functioning due to exclusion from employers [41]. Other differences include local substance abuse, as the prevalence in Hong Kong [42] is less than one-tenth of Denmark [43]. Substance abuse not only poses a clinical challenge for diagnostic ascertainment, but is also associated with poorer functioning [44]. Therefore, the current study provides a unique insight into DD and SZ beyond a Western perspective in Hong Kong.
Diagnostic stability
In line with previous evidence of the diagnostic instability [9], a large proportion of our DD patients (35%) underwent a diagnostic reassignment to SZ by the fourth year. The diagnostic stability of SZ may be related to its stringent diagnostic requirement, such that symptoms should be present for at least six months while no such specification exists for DD. Alternatively, the distinction between DD and SZ may be arbitrary in reality – the diagnostic conversion may reflect a natural course of illness rather than an actual diagnostic change [45, 46].
Clinical outcomes
Our study showed that pure DD is associated with more general psychopathology symptoms compared to SZ, even after accounting for the poorer insight reported in DD. A post hoc analysis of PANSS general psychopathology found significant results even after removing item G12 (insight; b = -1.632, p = .037, CI -3.160 to -0.104). The significant difference may therefore be driven by a collective range of symptoms such as depression, anxiety, and other behavioural symptoms. Our findings may thus pave the path for an enhanced characterisation of DD that moves beyond the content of delusions to the underlying psychopathological structure of the disorder.
Medication side effects, compliance, and insight
Our findings revealed that DD patients had more impaired insight, particularly in their awareness of the mental illness and its consequences. With delusions being its defining symptom, it is perhaps unsurprising that DD patients were unable to differentiate between the creations of their own mind and reality, thus failing to recognise their mental illness. There may also be an underlying tendency for DD patients to make erroneous inferences with high conviction. Greater over-confidence in judgement has been associated with the presence of delusions in psychotic disorders [47]. Not only may the lack of insight hinder help-seeking and treatment adherence, but it may also impede development of therapeutic relationships [48].
Despite no difference in side effects, DD patients displayed a better attitude towards medication. These findings are rather contentious considering that both side effects and insight have been shown to predict medication attitude [49]. However, studies of medication attitude often neglect to consider other moderating factors (e.g., cognitive impairments) [50] and its multidimensionality. This includes the dimensions of necessity and concerns about medication, of which only the former relates to illness awareness [51]. Although speculative, the smaller dosage of medication taken by the DD cohort (Table 3) may have also influenced their medication attitudes in the current study.
Furthermore, the dimensions of SUMD may be differentially related to medication attitude and therefore should be considered individually. An earlier study suggested that amongst the three aspects of insight, only awareness of medication impact was important for medication attitude [52]. Given that DD patients only demonstrated an impaired insight towards the presence of their mental illness and its consequences, that they also express better attitudes to medication may not be as contradictory as first assumed. Regardless, the difference in medication attitude failed to remain significant after a false discovery rate correction which suggests that findings should be interpreted with caution.
Functioning, neurocognitive performance, and quality of life
At four years, social and occupational functioning were comparable between the cohorts. Matching the two groups for age, sex, and years of education may account for why the present findings contradict previous studies [11]. In a secondary analysis that was conducted as part of our baseline study [18], level of functioning did differ between the two groups when age-matching was omitted.
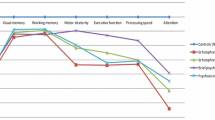
Neurocognitive functions were also found to be similar between the DD and SZ groups in our study. This finding resonates with that of the baseline study [18] and other relevant studies. For example, an earlier age-matched comparison of DD and SZ patients found comparable attention level, verbal and motor skills, cognitive flexibility, abstract thinking, memory, and psychomotricity [53]. A similar study that matched for age and years of education found no differences between DD and paranoid SZ patients in verbal learning, general memory, and sustained attention [54]. However, DD patients displayed better overall functioning than SZ patients when not matched for age [16]. The discrepancy in findings may be attributed to the potentially confounding effects of age on functioning, which may have resulted in the illusion that DD is associated with better functioning when it is not controlled for. Another interpretation is that age may have a stronger bearing on neurocognitive functions in DD relative SZ.
Limitations
This study had the following limitations. Firstly, this prospective follow-up study was conducted as a part of an intervention study [20], with a predetermined duration of treatment that can only be statistically controlled for. Secondly, only FEP patients aged 26–55 were included; the scarcity of adolescent cases made it difficult to recruit a sizable younger sample. The finding that DD and SZ are not as different as previously thought may therefore not apply to the adolescent population.
While it may have been preferable to only compare patients with more acute symptoms at study entry, patients were often only referred to the JCEP early intervention service four months after treatment. As a result, their clinical presentation may have already reduced in severity at study entry. In addition, statistical power may have been undermined by the removal of patients with a diagnostic shift at 4 years. Therefore, findings should be replicated in a larger sample with more acute presentations to provide further support for the lack of differences between DD and SZ.
Although age-matching removes a critical confounding variable, it also simultaneously hinders the exploration of the effects of age on outcomes. Age could be indicative of the impact of long-term illness or the cumulated use of antipsychotics on brain tissue atrophy over time [55]. Nevertheless, repeating the analysis without matching for age yielded similar results except that medication attitude failed to reach significance. This further reinforces the notion that DD and SZ may truly share similar longitudinal outcomes.
Conclusion
By comparing the four-year outcomes of age-matched DD and SZ patients, we found that the main differences laid in clinical factors. DD patients experienced more general psychopathology symptoms with a poorer illness insight and a better medication attitude. However, the two groups were largely similar in terms of social and occupational functioning, neurocognitive outcomes, and quality of life. Therefore, the two cohorts may not be as distinct as previously thought when the effects of potential confounders such as age, sex, and years of education are minimised. We believe that these findings will be useful in the characterisation of DD as a continuum of SZ, as well as in the advocacy for a dimensional approach to psychosis spectrum disorders.
Data Availability
The data that support the findings of this study are available from the corresponding author, CLMH, upon reasonable request.
Abbreviations
- AIMS:
-
Abnormal Involuntary Movement Scale
- BARNS:
-
Barnes Akathisia Rating Scale
- CDSS:
-
Calgary Depression Scale for Schizophrenia
- DD:
-
Delusional Disorder
- DUP:
-
Duration of Untreated Psychosis
- EI:
-
Early Intervention
- FEP:
-
First Episode Psychosis
- JCEP:
-
Jockey Club Early Psychosis
- PANSS:
-
Positive and Negative Syndrome Scale
- RFS:
-
Role Functioning Scale
- SAS:
-
Simpson-Angus Scale
- SF-12:
-
12-item Short Form health survey
- SOFAS:
-
Social Occupational Functioning Assessment Scale
- SUMD:
-
Scale to assess Unawareness of Mental Disorder
- SZ:
-
Schizophrenia
- UKU:
-
Udvalg for Kliniske Unders?gelser
- YMRS:
-
Young Mania Rating Scale
References
Spitzer RL, First MB, Kendler KS, et al. The reliability of three definitions of bizarre delusions. Am J Psychiatry. 1993;150(6):880–4.
American Psychiatric Association, Washington. Diagnostic and statistical manual of mental disorders: DSM-III-R. District of Columbia: American Psychiatric Association Press; 1988.
American Psychiatric Association. Diagnostic and statistical manual of mental disorders: DSM-IV. Washington, District of Columbia: American Psychiatric Association Press; 1994.
World Health Organisation. The ICD-10 classification of mental and behavioural disorders: clinical descriptions and diagnostic guidelines. Geneva: World Health Organization; 1992.
American Psychiatric Association. Diagnostic and statistical manual of mental disorders: DSM-V. Washington, District of Columbia: American Psychiatric Association Press; 2013.
Peralta V, Cuesta MJ. Delusional disorder and schizophrenia: a comparative study across multiple domains. Psychol Med. 2016;46(13):2829–39.
Muñoz-Negro JE, Ibáñez-Casas I, de Portugal E, et al. A psychopathological comparison between delusional disorder and schizophrenia. Can J Psychiatry. 2018;63(1):12–9.
Muñoz-Negro JE, Ibanez-Casas I, de Portugal E, et al. A dimensional comparison between delusional disorder, schizophrenia and schizoaffective disorder. Schizophr Res. 2015;169(1–3):248–54.
Fusar-Poli P, Cappucciati M, Rutigliano G, et al. Diagnostic stability of ICD/DSM first episode psychosis diagnoses: meta-analysis. Schizophr Bull. 2016;42(6):1395–406.
Allardyce J, Suppes T, Van Os J. Dimensions and the psychosis phenotype. Int J Methods Psychiatr Res. 2007;16(S1):34–S40.
Kendler KS. Demography of paranoid psychosis (delusional disorder): a review and comparison with schizophrenia and affective illness. Arch Gen Psychiatry. 1982;39(8):890–902.
Grover S, Biswas P, Avasthi A. Delusional disorder: study from North India. Psychiatry Clin Neurosci. 2007;61(5):462–70.
de Portugal E, González N, Del Amo V, et al. Empirical redefinition of delusional disorder and its phenomenology: the DELIREMP study. Compr Psychiatry. 2013;54(3):243–55.
Segovia AP, Jimenez MG, de Albornoz Calahorro CC, Ballesteros JC. Comorbidity between delusional disorder and sensory deficits. Results from the deliranda case register. Eur Psychiatry. 2016;33(S1):144.
Sim K, Chan YH, Chua TH, Mahendran R, Chong SA, McGorry P. Physical comorbidity, insight, quality of life and global functioning in first episode schizophrenia: a 24-month, longitudinal outcome study. Schizophr Res. 2006;88(1–3):82–9.
Marneros A, Pillmann F, Wustmann T. Delusional disorders—are they simply paranoid schizophrenia? Schizophr Bull. 2012;38(3):561–8.
Malla A, Norman R, Schmitz N, et al. Predictors of rate and time to remission in first-episode psychosis: a two-year outcome study. Psychol Med. 2006;36(5):649–58.
Hui CLM, Lee EHM, Chang WC, et al. Delusional disorder and schizophrenia: a comparison of the neurocognitive and clinical characteristics in first-episode patients. Psychol Med. 2015;45(14):3085–95.
Hui CLM, Wong AKH, Ho ECN et al. Effectiveness and optimal duration of early intervention treatment in adult-onset psychosis: a randomized clinical trial. Psycholog Med. 2022;1–13.
Hui CLM, Chang WC, Chan SKW, et al. Early intervention and evaluation for adult-onset psychosis: the JCEP study rationale and design. Early Interv Psychiatry. 2014;8(3):261–8.
So E, Kam I, Leung C, et al. The chinese-bilingual SCID-I/P project: stage 1–reliability for mood disorders and schizophrenia. Hong Kong J Psychiatry. 2003;13(1):7–19.
Leckman JF, Sholomskas D, Thompson WD, et al. Best estimate of lifetime psychiatric diagnosis: a methodological study. Arch Gen Psychiatry. 1982;39(8):879–83.
Kay SR, Fiszbein A, Opler LA. The positive and negative syndrome scale (PANSS) for schizophrenia. Schizophr Bull. 1987;13(2):261–76.
Addington D, Addington J, Schissel B. A depression rating scale for schizophrenics. Schizophr Res. 1990;3(4):247–51.
Young RC, Biggs JT, Ziegler VE, et al. A rating scale for mania: reliability, validity and sensitivity. Br J Psychiatry. 1978;133:429–35.
Amador XF, Strauss DH, Yale SA, et al. Assessment of insight in psychosis. Am J Psychiatry. 1993;150(6):873–9.
Simpson GM, Angus JW. A rating scale for extrapyramidal side effects. Acta Psychiatri Scand. 1970;45(S212):11–9.
Guy W. Abnormal involuntary movement scale (AIMS). ECDEU assessment manual for psychopharmacology: revised. Rockville: U.S. Dept. of Health, Education, and Welfare, Public Health Service, Alcohol, drug abuse, and Mental Health Administration, National Institute of Mental Health, Psychopharmacology Research Branch, Division of Extramural Research Programs; 1976. 534–7.
Barnes TR. A rating scale for drug-induced akathisia. Br J Psychiatry. 1989;154(5):672–6.
Lingjaerde O, Ahlfors W, Bech P, et al. The UKU (Udvalg for Kliniske Undersogelser) side effect rating scale. Acta Psychiatri Scand. 1987;76:85–94.
Thompson K, Kulkarni J, Sergejew AA. Reliability and validity of a new Medication Adherence Rating Scale (MARS) for the psychoses. Schizophr Res. 2000;42(3):241–7.
Goldman HH, Skodol AE, Lave TR. Revising axis V for DSM-IV: a review of measures of social functioning. Am J Psychiatry. 1992;149(9):1148–56.
Goodman SH, Sewell DR, Cooley EL, et al. Assessing levels of adaptive functioning: the Role Functioning Scale. Community Ment Health J. 1993;29(2):119–31.
Ware J, Kosinski M, Keller S. A 12-Item short-form Health Survey: construction of scales and preliminary tests of reliability and validity. Med Care. 1996;34(3):220–33.
Benjamini Y, Hochberg Y. Controlling the false discovery rate: a practical and powerful approach to multiple testing. J R Stat Soc Series B Methodol. 1995;57(1):289–300.
Hui CLM, Tang JYM, Wong GHY, Chang WC, Chan SKW, Lee EHM, Chen EYH. Predictors of help-seeking duration in adult-onset psychosis in Hong Kong. Soc Psychiatry Psychiatr Epidemiol. 2013;48:1819–28.
Olivares JM, Thirunavukarasu M, Kulkarni J, Zhang HY, Zhang M, Zhang F. Psychiatrists’ awareness of partial and nonadherence to antipsychotic medication in schizophrenia: results from an Asia–Pacific survey. Neuropsychiatr Dis Treat. 2013 Aug;12:1163–70.
Hui CLM, Chen EYH, Yip KC, Law CW, Chiu CP. Anti-psychotics adherence among out-patients with schizophrenia in Hong Kong. Keio J Med. 2006;55(1):9–14.
Lacro JP, Dunn LB, Dolder CR, Jeste DV. Prevalence of and risk factors for medication nonadherence in patients with schizophrenia: a comprehensive review of recent literature. J Clin Psychiatry. 2002;63(10):15489.
Lam TP, Sun KS. Stigmatizing opinions of chinese toward different types of mental illnesses: a qualitative study in Hong Kong. Int J Psychiatry Med. 2014;48(3):217–28.
Tsang HW, Angell B, Corrigan PW, Lee YT, Shi K, Lam CS, Jin S, Fung KM. A cross-cultural study of employers’ concerns about hiring people with psychotic disorder: implications for recovery. Soc Psychiatry Psychiatr Epidemiol. 2007;42:723–33.
Chen EY, Hui CL, Lam MM, Chiu CP, Law CW, Chung DW, Tso S, Pang EP, Chan KT, Wong YC, Mo FY. Maintenance treatment with quetiapine versus discontinuation after one year of treatment in patients with remitted first episode psychosis: randomised controlled trial. BMJ. 2010;341.
Wunderink L, Nienhuis FJ, Sytema S, Slooff CJ, Knegtering R, Wiersma D. Guided discontinuation versus maintenance treatment in remitted first-episode psychosis: relapse rates and functional outcome. J Clin Psychiatry. 2007;68(5):654.
Carey KB, Carey MP, Simons JS. Correlates of substance use disorder among psychiatric outpatients: focus on cognition, social role functioning and psychiatric status. J Nerv Ment Dis. 2003;191(5):300–8.
Amin S, Singh SP, Brewin J, et al. Diagnostic stability of first-episode psychosis: comparison of ICD–10 and DSM–III–R systems. Br J Psychiatry. 1999;175(6):537–43.
Whitty P, Clarke M, McTigue O, et al. Diagnostic stability four years after a first episode of psychosis. Psychiatr Serv. 2005;56(9):1084–8.
Warman DM, Lysaker PH, Martin JM. Cognitive insight and psychotic disorder: the impact of active delusions. Schizophr Res. 2007;90(1–3):325–33.
Roudsari MJ, Chun J, Manschreck TC. Current treatments for delusional disorder. Curr Treat Options Psychiatry. 2015;2(2):151–67.
Kampman O, Laippala P, Väänänen J, et al. Indicators of medication compliance in first-episode psychosis. Psychiatry Res. 2002;110(1):39–48.
Staring AB, van der Gaag M, Duivenvoorden HJ, et al. Why do patients with schizophrenia who have poor insight still take antipsychotics? Memory deficits as moderators between adherence belief and behavior. J Psychiatr Pract. 2011;17(5):320–9.
Beck EM, Cavelti M, Kvrgic S, et al. Are we addressing the ‘right stuff’ to enhance adherence in schizophrenia? Understanding the role of insight and attitudes towards medication. Schizophr Res. 2011;132(1):42–9.
Dassa D, Boyer L, Benoit M, Bourcet S, Raymondet P, Bottai T. Factors associated with medication non-adherence in patients suffering from schizophrenia: a cross-sectional study in a universal coverage health-care system. Australian & New Zealand Journal of Psychiatry. 2010;44(10):921–8.
Evans JD, Paulsen JS, Harris MJ, et al. A clinical and neuropsychological comparison of delusional disorder and schizophrenia. J Neuropsychiatry Clin Neurosci. 1996;8(3):281–6.
Lapcin S, Guler J, Ceylan E, et al. Attention impairment in patients with paranoid schizophrenia and delusional disorder: a controlled study. Int J Neuropsychopharmaco. 2008;11:251.
Tordesillas-Gutierrez D, Koutsouleris N, Roiz-Santiañez R, et al. Grey matter volume differences in non-affective psychosis and the effects of age of onset on grey matter volumes: a voxelwise study. Schizophr Res. 2015;164(1–3):74–82.
Acknowledgements
We thank our collaborating partners, the Hong Kong Hospital Authority, Caritas Hong Kong (Social Work Services), and the Mental Health Association of Hong Kong, for their valuable contribution to facilitate the JCEP project. We also thank all the patients for their participation, without which this study could not have been completed.
Funding
The study was funded by the Hong Kong Jockey Club Charities Trust (grant number 21009144).
Author information
Authors and Affiliations
Contributions
EYHC and CLMH conceptualised the study and formulated the study design. CLMH, EHML, WCC, SKWC, and EYHC collected the data. CLMH, PWMH, ECNH, and BSTL analysed the data and drafted the manuscript. All authors contributed to the interpretation of the findings and critical revisions of the manuscript, and approved of the final version for publication.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the Institutional Review Boards at each study site (University of Hong Kong/Hospital Authority Hong Kong West Cluster: UW09-123, UW16-125 and UW16-004; Hong Kong East Cluster: HKEC-2009-040; Kowloon Central/Kowloon East: KC/KE-09-0068/ER-3; New Territories West Cluster: NTWC/CREC/716/09; Kowloon West Cluster: KW/EX/09–058; and New Territories East Cluster: CREC Ref. No. 2009.256-T). Written informed consent was obtained from all patients or legally authorized representatives prior to participation.
Consent for publication
No applicable.
Competing interests
EYHC reports having received speaker honoraria from Otsuka and DSK BioPharma; received research funding from Otsuka; participated in paid advisory boards for Jansen and DSK BioPharma; received funding to attend conferences from Otsuka and DSK BioPharma. All other authors have nothing to declare.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Supplementary Material 1.
BMC_additional file 1. Title: “Supplementary data on diagnostic stability”.. Contains a table to show the baseline comparison of demographic and psychopathology variables between delusional disorder patients with and without a diagnostic shift to schizophrenia after four years.
Supplementary Material 2.
BMC_additional file 2. Title: “Supplementary data on non-matched comparative analysis”.. The file provides detailed descriptions of the non-matched comparative analysis among 72 patients with delusional disorder and 157 patients with schizophrenia from the original cohort that has not been matched for age. Four tables are included to show the baseline and 4-year outcome comparisons between patients with delusional disorders and schizophrenia.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Hui, C.L.M., Chan, E.W.T., Hui, P.W.M. et al. Functional and clinical outcomes of delusional disorder and schizophrenia patients after first episode psychosis: a 4-year follow-up study. BMC Psychiatry 23, 676 (2023). https://doi.org/10.1186/s12888-023-05175-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12888-023-05175-z