
Abstract
Background
The non-medical use of prescription drugs is a growing public health problem worldwide. Recent trends in Cameroon show that the use of psychoactive substances, among which are prescription drugs by adolescents is becoming a public health issue and is linked to juvenile delinquency and violence in schools. However, there is a paucity of data on the burden of this phenomenon among adolescent secondary school students in the country. The aim of this study was to determine the prevalence and factors associated with the use of non-prescription drugs in secondary schools in Buea, South West region of Cameroon.
Methods
We conducted a cross-sectional study from 1st February 2021 to 30th April 2021. Secondary school students were recruited using a multistage stratified cluster sampling. A modified and standardized version of the World Health Organization student drug-use survey model questionnaire was used. Ethical approval was obtained from the Institutional Review Board of the Faculty of Health Sciences, University of Buea (No. 2021/1273–02/UB/SG/IRB/FHS). The Statistical Package for Social Sciences, IBM SPSS Statistics for Windows, Version 25.0. was used for data analysis. Descriptive statistics were used to describe the sociodemographic characteristics of participants. Univariate and multivariate logistic regression models were used to explore associated factors of non-medical use of prescription drugs.
Results
A total of 570 participants were enrolled for the study, and 510 participants responded giving a response rate of 89.5%. The prevalence of non-medical use of prescription drugs was 15.3%, tramadol being the most used. Motivators for non-medical use of prescription drugs were “to work longer”, “to be courageous”, and “curiosity”. Logistic regression results showed that alcohol consumption [OR 3.68; 95% CI: 2.24–6.06; p < 0.001], smoking [OR 6.00; 95% CI: 3.07–11.75; p < 0.001] and use of illicit drugs [OR 10.85; 95% CI: 5.48–21.48; p < 0.001] were independent factors associated with non-medical use of prescription drugs.
Conclusion
Non-medical use of prescription drugs was prevalent among adolescent secondary school students in Buea, Cameroon. Tramadol is the main drug of prescription involved. Our results can guide policymakers on strategies to screen, prevent and control non-medical use of prescription drugs among secondary school students in Cameroon.
Similar content being viewed by others

Background
Non-medical use of prescription drugs (NMUPD), defined as the use of prescription drugs that is not prescribed to a user, or other than in the manner, for reasons, or time period prescribed, is a growing health problem [1, 2]. Young people are more vulnerable to drug use, and the misuse of prescriptions drugs, particularly opioids, benzodiazepines and synthetic stimulants is generally higher among adolescents than among the general population in all regions of the world [3,4,5,6].
Globally, about 296 million people 5.8 percent of the global population aged 15 – 64 are estimated to have used drugs in 2021, representing about a 23 per cent increase over the last 10 years [2]. According to data from the United Nations Office on Drugs and Crime (UNODC), there is an increased availability of substances in the drug markets, with NMUPDs ranking second after cannabis [7]. The problematic non-medical use of pharmaceutical opioids, especially tramadol affects many countries worldwide, and is the main driver of non-medical use of prescription drugs in North, West and Central Africa [7,8,9]. Non-medical use of tramadol is an emerging public health crisis with serious public health consequences in Africa [8,9,10]. Emerging trends on non-medical use of prescription drugs in Kenya showed that the problem is more prevalent among adolescents and data indicated a lifetime usage of 10.4% among primary school students, with antidepressants, antipsychotics, anticholinergics, opioid analgesics, antihistamines and anaesthetics identified as the main drug classes involved [11]. In Nigeria, a study on substance use among secondary school students revealed that up to 35 per cent of them had taken tramadol, and 18 per cent had taken Refnol in their lifetime for non-medical purposes [12]. Another recent study in Parakou, Benin, reported 13.5% prevalence amongst secondary school students with a lifetime non-medical use of any prescription drugs, mostly among those aged 20 to 24 years [13].
In Cameroon, psychoactive substance use among adolescents and young adults in schools is becoming a public health problem, and is associated with juvenile violence and delinquency [14]. Few studies have been done in tertiary institutions and in street children on recreational drugs and other substance abuse in Cameroon [15,16,17,18]. Furthermore, due to conflict and stressors related to internal displacements, there has been an increase in the use of recreational drugs in the country [19]. However, to our knowledge, there has been no investigation on the non-medical use of prescription drugs among adolescents and young people in Cameroon. The aim of the current study was to determine the prevalence and predictors of NMUPD among adolescents in secondary schools in Buea. The data will help in the design of school-based interventions for the prevention and control of non-medical use of prescription drugs among adolescents in secondary schools.
Methods
Study design
A cross-sectional study was undertaken in order to determine the prevalence and predictors of non-medical use of prescription drugs in some secondary schools in Buea from 1st February 2021 to 30th April 2021.
Study area and setting
The secondary schools in Buea have an estimated population of 17,852 students. The city has noticed an increased in its population over the past four years following a socio-political crisis in the anglophone regions of Cameroon that has led to internally displaced persons fleeing from conflicts zones in rural areas to the major city of Buea [19, 20].
Study population
Adolescent students from seven randomly selected public, mission and lay private secondary schools in the Buea municipality were included.
Inclusion criteria
All students who accepted to participate in the study and signed a consent/assent form.
Exclusion criteria
Students aged less than 13 years or greater than 20 years.
Sample size
The sample size was calculated using the Cochran formula [21]. as shown below;
Z = standard normal variate (1.96) at 95% confidence interval.
P = estimate of prevalence of NMUPD was taken as 50% due to paucity of the prevalence study in this population in Cameroon at the time of our study.
e = sampling error that can be tolerated (5%)
Taking a non-response rate of 10%, 10/100(384) = 39.
Therefore, the least estimated sample size was 423 students, and we recruited an actual sample of 510 students.
Multistage sampling technique was used to obtain study participants. In the first stage, seven secondary schools were conveniently selected out of a total 15 using convenience sampling method in order to include public, lay private and mission schools. Secondly, probability proportionate to size was used to select the number of students from each secondary school. Lastly, simple random sampling (balloting) was used to select students from the individual schools.
Data collection
Data was collected using a standardized questionnaire, adapted version of the World Health Organization student drug-use survey model questionnaire [22]. This tool has been tested and shown to be reliable and valid among students in a neighbouring country in Nigeria [23]. The questionnaire was pretested among 30 students from secondary schools not selected for the study. Three data collectors were trained on proper data collection steps for a period of four days, and they pretested 10 students each. Following the training, the principal investigator and the 03 data collectors then moved to the various selected schools for data collection. All participants in the study received a participant information sheet. Following clear explanation of the information sheet, the voluntary participants were required to sign an informed consent form or assent form. Schools were visited days before the study and consent/assent forms were presented to administrators who later obtained a verbal consent from the students’ parents/guardians. A self-administered questionnaire was then used to collect the data. After random sampling, students were given about 15 min to fill the questionnaire.
Ethical approval
Ethical approval was obtained from the Institutional Review Board of the Faculty of Health Sciences, University of Buea (2021/1273–02/UB/SG/IRB/FHS). This was then followed by administrative authorization from the South West regional delegations of public health and of Secondary education respectively. Authorization was also gotten from the various principals of the selected schools. Written consent was obtained from the parents of individual students by the school administration, while in each class, the investigators obtained oral consent from the students in the presence of their class teachers. Participants were informed on the importance of the study and confidentiality and privacy were respected.
Data management and analysis
Data collection was coded to ensure confidentiality. Data were entered into a computer using the Excel spreadsheet and exported to Statistical package for Social Science (SPSS) version 25 for statistical analysis. Descriptive summary measures were expressed as means ± standard deviation for normally distributed data, or median [interquartile range] for non-normally distributed data and number (percentages) for qualitative variables. Categorical comparisons were performed by Chi-square test. Odds ratios (ORs) and nominal 95% confidence intervals (CIs) were presented. A logistic regression model (multivariate analysis) was used to estimate the association between baseline demographics and predictors for drug use. Statistical significance was set at p < 0.05.
Results
Five hundred and ten out of the five hundred and seventy invited adolescents secondary school students accepted to participate in the study, giving a response rate of 89.5%.
General characteristics of participants
Most of the participants were form five and upper sixth students, 219 (42.9%) and 201(39.4%) respectively. The majority of the participants were female, 262 (51.4%), and there was an even ratio of 1:1. The mean age (SD) was 17.3 (1.9) years, and the age group most represented was that of adolescent school students between 17 and 20 years (62.4%). The socio-demographic characteristics of the participants are shown on Table 1. Most of the adolescent school students, 325(63.7%) had an estimated monthly allowance of less than 5,000 FCFA, and were mostly living in same homes with their parents or guardians (68.6%).
Prevalence of non-medical use of prescription drugs among adolescent secondary school students
Seventy-eight participants admitted usage of prescription drugs, giving a prevalence of non-medical use of prescription drugs among adolescents in secondary schools in Buea of 15.3%.
The most frequently misused drugs were opioid analgesics, with a prevalence of lifetime usage of 10.58%, followed by stimulants (3.1%), and sleep medication (diazepam) (1.7%). Tramadol was reported to be the commonly used prescription drug (Fig. 1).

Frequency of common NMUPDs by adolescent secondary school students
Twenty-seven (33.3%) of the students reported a daily usage of prescription drugs for non-medical reasons and 25.9% used them occasionally. More than half of the students [45 (53.6%)] started using the drugs between the ages of 15 and 17 years. These drugs are consumed by students mostly before sexual intercourse [36 (36.7%)], before sporting activities [21 (21.2%)], at parties [19 (19.2%)] and before exams [15 (15.2%)]. These drugs were mostly purchased from roadside vendors (31.7%), local drugstores (23.3%), clubs (18.3%), and approved pharmacies (11.7%).
Non-medical use of prescription drugs were associated with other concurrent substance misuse. Alcohol usage was the most reported substance utilized by the secondary school students 167 (32.8%), followed by tobacco and illicit drug use in 41(8.0%) each. Cannabis was the most common form of illicit substance used by secondary school students, and was reported in 6.07% of the students.
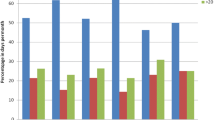
The factors motivating the non-medical use of prescription drugs were mainly due to personal reasons, or influence from the family, peers or the neighborhood. The motivators for NMUPDs are reported in Fig. 2.

Motivators for NMUPDs among adolescent secondary school students
Predicting factors of NMUPD among secondary school students in Buea
On bivariate analysis, alcohol use (OR 3.68; 95% CI 2.24, 6.06; P < 0.000), tobacco smoking (OR 6.00; 95% CI 3.07, 11.75; P < 0.000), and use of illicit drugs (OR 10.85; 95% CI 5.48, 21.48; P < 0.000), were strongly associated with non-medical use of prescription drugs (Table 2).
On multivariable analysis, the use of alcohol (aOR 2.23; 95% CI 1.26, 3.95; P = 0.006), and illicit drugs (OR 5.60; 95% CI 2.41, 12.97; P < 0.000), were shown to be independently associated with the use of prescription drugs for non-medical purposes among the secondary school students in Buea (Table 3).
Discussion
The aim of our study was to determine the prevalence and factors associated with non-medical use of prescription drugs among adolescents in secondary schools in Buea. This is one of the first studies that evaluates the prevalence and correlates of non-medical use of prescription drugs among secondary school students in Cameroon.
Prevalence of non- medical use of prescription drugs
We found that the prevalence of non-medical use of prescription drugs was 15.3%. Most of the students concerned with NMUPDs were adolescents in the age group between 15 and 17 years (53.6%). Our results indicate that opioid analgesics, specifically tramadol is the most frequently used prescription drug among adolescent secondary school students, followed by stimulants and benzodiazepines. Up to 10.58% of the school students were using opioids, mainly tramadol, followed by stimulants (3.1%), and sleep medication(diazepam) (1.7%).
The use of drugs for non-medical purposes is on the rise among school-age population in Cameroon. Our observation is in keeping with previous findings from tertiary settings in the country, whereby the use of opioid analgesics and other substances such as cannabis and alcohol for recreational purposes is common among youth [15, 18, 19]. Metuge et al. [18] in a study on substance use among students in tertiary institutions in Buea, Cameroon found that the commonest substances used were alcohol (98.4%), tobacco (28.3%), tramadol (7.5%) and 6.8% of cannabis [18]. Their findings are similar to those of Mbanga et al. [15] who also confirmed the association of opioid use with the consumption of other substances as alcohol and tobacco.
Non-medical use of prescription drugs has increased globally over the past decades, and is driven mainly by the increased availability of substances on the drug market [2]. In West, Central, East, and North Africa and the Middle East, although cannabis is the main drug among people with drug use disorders, opioid analgesics remain the main drug involved with non-medical use [24]. Our study findings of tramadol as the main non-prescription drug misused agree with these international trends. Bio-Sya et al. [13] in a cross-sectional study of 384 secondary students within the age group of 10–24 years in Benin, found a lifetime prevalence of non-medical use of tramadol of 9.6%. These findings are similar to the 10.58% of our secondary school students who were using tramadol, although we did not perform urinary toxicological tests for the detection of tramadol and its metabolites as they did. Other authors from Nigeria have reported similar prevalence of non-medical prescription use of tramadol among secondary school students [25,26,27,28]. However, our findings are in contradiction with the emerging trends on non-medical use of prescription drugs in Kenya by Kamenderi et al. [11], who reported that the most prevalent prescription drug for non-medical use was diazepam in 35.2% of 68 confirmed samples, followed by flunitrazepam and amitriptyline, while tramadol represented only 1.5% of their samples. We think that the reason for this discrepancy may be that the study in Kenya was a national survey covering up to eight regions, and was not focused only on school students.
Associated factors of non-medical use of prescription drugs
Most sociodemographic and behavioural factors showed a weak association with non-medical use of prescription drugs. In comparison with other studies [29, 30], we found that the use of alcohol and other illicit drugs such as cannabis were independently associated with the non-medical use of prescription drugs among secondary school students. In Cameroon, alcohol misuse has been shown be accompanied by the use other illicit drugs such as cannabis and tobacco, and is responsible for indiscipline, violence and other harmful effects among adolescents and youth in school settings [31,32,33]. There is need for further studies to explore the burden of alcohol and other illicit drugs consumption as drivers for the tramadol epidemic that is common in Africa [9, 10], especially among adolescents in secondary school settings. The link between alcohol usage, illicit drug use and other non-medical prescription drugs, especially tramadol is not limited to our setting, it is a global phenomenom, reported in both high-income and low-income countries alike, and most persons who use prescription drugs for non-medical purpose seem to be polysubstance abuses [5, 6, 30, 34, 35].
Like other studies, we found that the desire to achieve emotional feelings of happiness and joy, courage to talk in public, curiosity, peer pressure and the need to improve school performance where the main reasons adolescent school students were engaging in the non-medical use of prescription drugs (Fig. 2). In a systematic review of motivations for the non-medical use of prescription drugs in young adults aged 18 to 25 years, Tess et al. [4], found that most of them are motivated to take prescription drugs such as stimulants, opioids and antidepressants non-medically to experience the cognitive enhancement effects, and to help them study, improve focus, stay alert and to increase energy among other reasons [4]. The few studies done among students in tertiary institutions and other settings in Cameroon have focused only on the use of drugs for recreational purposes [36] and none has explored the motivations behind the non-medical use of prescription drugs, and none of them has focused on the secondary school students despite the violence and delinquency related to their use in these settings [33]. We also found that some of the students had become addicted to the opioids following chronic use for painful medical conditions, for example, recurrent treatment of acute vaso-occlusive crisis pain in sickle cell disease has been associated with subsequent addiction and non-prescription drug usage [37, 38].
Implication of the findings
This study has made a number of important contributions to the study of non-medical use of prescription drugs among adolescents in secondary schools in Cameroon. Firstly, our study highlights specifically the high prevalence of tramadol misuse in the school setting, which calls for regular screening and monitoring of students. These findings fall in line with the opioid crisis and its impact in Africa [8, 9]. Secondly, our findings have shown some of the factors associated with the non-medical use of prescription drugs in school settings in Cameroon. These findings could help in the design of selective and specific school-based interventions for the prevention and control of the usage non-medical prescription drugs and other illicit drugs in secondary schools. This will contribute to curbing the problem of violence and indiscipline [14], among adolescent secondary school students.
Strengths and limitations
Our study has the strength of being one of the first studies on the non-medical use of prescription drugs among adolescents, and involves a large sample size from several private and public secondary schools in Cameroon. However, it has some limitations that we must acknowledge. First, the cross-sectional design of our study could not allow us to establish any causal relationship. Secondly, our findings are based on self-reporting by the school students and are therefore subject to recall and information bias. Furthermore, we did not study the impact of conflict and internal displacements of secondary students on non-medical use of prescription drugs in schools. Atabong et al. [19], have shown the use of recreational drugs to be related to conflict in the region and this could be a confounding factor that we did not explore. In spite of these limitations, our findings provide baseline information that could be used in the design of further studies for more evidence that would inform policy in this setting.
Conclusion
In conclusion, one out of six secondary school students in Buea, South West region of Cameroon, is involved with the non-medical use of prescription drugs. Opioid analgesics, mainly tramadol are the main type of prescription drugs concerned, and alcohol use, tobacco smoking and other illicit drugs are independently associated with non-medical use of prescription drugs. Parents, school authorities and healthcare policymakers need to be aware of the high prevalence of non-medical use of prescription drugs. Our findings can helpful in developing and implementing screening, prevention and targeted school-based interventions among adolescent secondary school students in Cameroon.
Availability of data and materials
The datasets generated during and/or analysed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- NMUPD:
-
Non-Medical Use of Prescription Drug
References
United Nations Office on Drugs and Crime (UNODC). The non-medical use of prescription drugs: Policy direction issues. 2011.
United Nations Office on Drugs and Crime (UNODC). World Drug Report. 2022. UNODC, World Drug Report 2022 (United Nations publication, 2022). Available from: https://www.unodc.org/unodc/en/data-and-analysis/world-drug-report-2022.html. Cited 2023 Jan 19.
Martins SS, Ghandour LA. Nonmedical use of prescription drugs in adolescents and young adults: not just a Western phenomenon. World Psychiatry. 2017;16(1):102–4.
Drazdowski TK. A systematic review of the motivations for the non-medical use of prescription drugs in young adults. Drug and Alcohol Dependence Elsevier Ireland Ltd. 2016;162:3–25.
Novak SP, Håkansson A, Martinez-Raga J, Reimer J, Krotki K, Varughese S. Nonmedical use of prescription drugs in the European Union. BMC Psychiatry. 2016;16(1):1–2.
Iwanicki JL, Schwarz J, May KP, Black JC, Dart RC. Tramadol non-medical use in Four European countries: A comparative analysis. Drug Alcohol Depend. 2020;1:217.
UNODC, World Drug Report 2022 (United Nations publication, 2022).
Kurth AE, Cherutich P, Conover R, Chhun N, Bruce RD, Lambdin BH. The Opioid Epidemic in Africa and Its Impact. Curr Addict Rep Springer. 2018;5:428–53.
Salm-Reifferscheidt L. Tramadol: Africa's opioid crisis. Lancet. 2018;391(10134):1982–3.https://doi.org/10.1016/S0140-6736(18)31073-0. Epub 2018 May 17.
Boun SS, Omonaiye O, Yaya S. Protocol for a scoping review study on the prevalence and public health consequences of non-medical use (NMU) of tramadol in Africa. PLoS One. 2023;18(5):e0285809.
Morris Kamenderi JMVO, JK, WMKL and SK. African Journal of Alcohol & Drug Abuse : Volume 5. 2021. p. 41–55 Emerging Trends on Non-Medical Use of Prescription Drugs in Kenya. Available from: https://nacada.go.ke/sites/default/files/2022-03/Emerging%20Trends%20on%20Non-Medical%20Use%20of%20Prescription%20Drugs%20in%20Kenya%20Ajada%20Vol%205.pdf. Cited 2023 Jan 19.
Onigbogi O, Ojo O, Babalola O. Prevalence of Substance Abuse among Secondary School Students in Lagos State of Nigeria. ESJ [Internet]. 2023;19(15):67. [cited 2023 Sep. 2]. Available from: https://eujournal.org/index.php/esj/article/view/16818.
Bio-Sya A, Onzo PJ, Klikpo ETE, Allabi AC. Nonmedical Use of Prescription Psychotropic Drugs among Secondary School Students in Parakou, northern Benin. Res J Drug Abuse. 2023;10(1):1.
Oshodi OY, Aina OF, Onajole AT. Substance use among secondary school students in an urban setting in Nigeria: prevalence and associated factors. Afr J Psychiatry. 2010;13(1):52–7.
Mbanga CM, Efie DT, Aroke D, Njim T. Prevalence and predictors of recreational drug use among medical and nursing students in Cameroon: A cross sectional analysis. BMC Res Notes. 2018;11(1):1–7.
Mabouopda V, Guy Toguem M, Domngang Noche C, Fotso Djemo JB. Substance use and substance abuse among street children in the city of Yaounde, Cameroon. 2022; Available from: https://doi.org/10.21203/rs.3.rs-1180441/v2.
Cumber S, Tsoka-Gwegweni J. Pattern and practice of psychoactive substance abuse and risky behaviours among street children in Cameroon. SAJCH. 2016;10(3):166–70.
Metuge CE, Dzudie A, Ebasone PV, Assob JCN, Ngowe MN, Njang E, et al. Prevalence and factors associated with substance use among students in tertiary institutions in Buea, Cameroon. Pan Afr Med J. 2022;1:41.
Atabong EN, Fombo EJ, Nyuydzedze SS, Nembulefac DK, Ayongi ENS. Prevalence and predictors of recreational drug use in a conflict affected area in the Southwest region of Cameroon: A cross-sectional study. J Public Health Epidemiol. 2022;14(2):107–15.
Tande K, Patrick M. An appraisal on the predicament of internally displaced persons (idps) and refugees of the anglophone armed conflict in Cameroon. GPH-Int J Educ Res. 2021;4(07):01–13.
Charan J, Kaur R, Bhardwaj P, Singh K, Ambwani SR, Misra S. Sample Size Calculation in Medical Research: A Primer. Ann Natl Acad Med Sci. 2021;57(02):074–80.
United Nations Office on Drugs and Crime. Conducting school surveys on drug abuse. Global Assessment Programme on Drug Abuse Toolkit Module 3. United Nations; 2003. 95.
Adelekan ML, Odejide OA. The reliability and validity of the WHO student drug-use questionnaire among Nigerian students. Drug Alcohol Depend. 1989;24(3):245–9.
United Nations Office for Drugs and Crime. United Nations Publications . 2023. World Drug Report 2023. Available from: https://www.unodc.org/unodc/en/data-and-analysis/world-drug-report-2023.html. Cited 2023 Aug 9.
Nabofa OE. New trend of drugs abused by secondary school students in nigeria. Afr Health Sci. 2021;21(3):1460–6.
Idowu A, Aremu AO, Olumide A, Ogunlaja AO. Substance abuse among students in selected secondary schools of an urban community of Oyo-state, South West Nigeria: Implication for policy action. Afr Health Sci. 2018;18(3):776–85.
Soremekun RO, Folorunso BO, Adeyemi OC. Prevalence and perception of drug use amongst secondary school students in two local government areas of lagos state, nigeria. S Afr J Psychiatry. 2020;26:1–6.
Dumbili EW, Odeigah OW. Prescription Opioids and New Psychoactive Substances Use in Nigeria: A Systematic Review and Policy Implications. Available from: http://orcid.org/0000-0002-3563-1617.
Papazisis G, Tsakiridis I, Siafis S. Nonmedical use of prescription drugs among medical students and the relationship with illicit drug, tobacco, and alcohol use. Subst Abuse: Res Treat. 2018;12:1178221818802298.
Piispa I, Karjalainen K, Karttunen N. Nonmedical use of prescription drugs: A comparison between intoxication-oriented and other nonmedical users. NAD Nordic Studies Alcohol Drugs. 2022;39(1):64–75.
Afumbom DA. Youth Alcoholism among Campus Undergraduates in Cameroon: Implications for Indiscipline in University Neighbourhoods. Print) International Journal of Social Science and Humanities Research.;10:136–50. Available fromhttps://doi.org/10.5281/zenodo.6873450. Cited 2023 Aug 11.
Tarkang EE, Pencille LB, Lutala P. Addressing adolescent´s binge drinking in Cameroon using the five key areas of the Ottawa charter for health promotion: implication for the spread of HIV - a commentary. PAMJ-OH 2020; 1:2. 2020 Mar 19;1(2). Available from: https://www.one-health.panafrican-med-journal.com/content/article/1/2/full. Cited 2023 Aug 11.
Kingsley TA*, Asangbeng TE, Acha AE, Longdoh NA, Shey ND. Factors Influencing Psychoactive Substance Use Among Students; Why Juvenile Violence and Delinquency Within Schools in Cameroon. Scope of the Evidence. Annal Pub Health Epidemiol. 2022;2(1):APHE.MS.ID.000527. https://doi.org/10.33552/APHE.2022.02.000527.
Weidberg S, Aonso-Diego G, García-Fernández G, Secades-Villa R. Prevalence and Correlates of Prescription Drug Misuse Among Spanish Adolescents. Psicothema. 2022;34(2):275–82.
Chen LY, Chen YL, Tsay WI, Wu SC, Chen YT, Hsiao PC, et al. Nonmedical prescription drug use of analgesics and sedatives/hypnotics in Taiwan: Results from the 2014 National Survey of Substance Use. Prev Med Rep. 2019;1:15.
Njingu AE, Jabbossung FE, Eyong S, Ayongi N. Health-Related Quality Of Life And Its Determinants Among Recreational Drug Users In A Rural Area In Cameroon: A Cross-Sectional Study. 2021; Available from: https://doi.org/10.21203/rs.3.rs-907905/v1.
Mo G, Jang T, Stewart C, Khoury L, Ferguson N, Egini O, et al. Chronic opioid use in patients with sickle cell disease. Hematology (United Kingdom). 2021;26:415–6 Taylor and Francis Ltd.
Arzoun H, Srinivasan M, Sahib I, Fondeur J, Mendez LE, Hamouda RK, Mohammed L, Hamouda R. Opioid use in patients with sickle cell disease during a vaso-occlusive crisis: a systematic review. Cureus. 2022;14(1).
Acknowledgements
We appreciate the support of the study participants (students) and the principals of the various secondary schools within Buea municipality for being collaborative in the data collection. We are also grateful to Dr. Tanue Elvis for logistical assistance in the work.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Author information
Authors and Affiliations
Contributions
This study was conceived and designed by NC and AKN; conducted by SIN and NC under the supervision of AKN. SIN analysed the data and wrote the first draft of the manuscript. All authors have been involved in the acquisition and interpretation of the data as well as revision of the manuscript. All authors have contributed to writing the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Participants received detailed written and informed consent and oral study information on the study. Written informed consent was obtained from all participants and for children under 16 informed consent was obtained from their parent or guardian. The study was approved by the Institutional Review Board of the Faculty of Health Sciences, University of Buea, Cameroon (No. 1273–02 2021/1273–02/UB/SG/IRB/FHS)) and was conducted in accordance with the Declarations of Helsinki-Ethical Principles for Medical Research Involving Human Subjects.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Nkouonlack, C., Shifu, I.N., Atchou, J.G.B. et al. Prevalence and associated factors of non-medical use of prescription drugs among adolescents in secondary schools in Buea, Cameroon: a cross-sectional study. BMC Psychiatry 23, 695 (2023). https://doi.org/10.1186/s12888-023-05120-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12888-023-05120-0