
Abstract
Background
Childhood and peer experiences can influence adolescents’ perceptions of interpersonal relationships, which can, in turn, influence their emotional states and behavior patterns. Non-suicidal self-injury (NSSI) is now a common problem behavior among adolescents. The present study examined the role of childhood trauma and peer victimization in adolescents’ NSSI.
Methods
A cross-sectional survey was conducted among 1783 adolescents (1464 girls and 318 boys) in the psychiatric outpatient clinics or wards of 14 psychiatric hospitals or general hospitals in nine provinces in China. Data were collected using the Multidimensional Peer Victimization Scale (MPVS), Short-form Childhood Trauma Questionnaire(CTQ-SF), and Functional Assessment of Self-Mutilation (FASM). Structural equation modeling (SEM) with latent variables was used to demonstrate the mediating role of peer victimization in the association between childhoodtrauma and NSSI.
Results
The SEM analysis demonstrated that peer victimization plays a partial mediating role in the relationship between childhood trauma and NSSI. In addition, several covariates (such as age, gender, education level, and place of residence) effectively regulated the relationship between peer victimization and NSSI.
Conclusion
In future studies of NSSI among Chinese adolescents, attention should be paid to the roles of childhood trauma and peer bullying; there is a temporal sequence between these two variables and, to some extent, childhood trauma can have an impact on bullying during adolescence which, in turn, influences NSSI behavior.
Similar content being viewed by others

Introduction
Non-suicidal self-injury (NSSI) is defined as the deliberate direct destruction or alteration of body tissue without conscious suicidal intent [1]. In the Diagnostic and Statistical Manual of Mental Disorders, fifth edition (DSM-5), this diagnosis is denoted as a “ condition for further study” [2]. Globally, the lifetime prevalence of at least one episode of NSSI in adolescence is 17–18% [3]. As early as 2016, the prevalence of adolescent NSSI was found to be 15.0% in the sample of Chinese adolescent communities [4]. Besides, a large-scale sampling survey in 2021 showed that the prevalence of NSSI was 28.5% among 18,900 Chinese junior and senior high school students [5]. Besides, a recent study reported that 33.7–51% of community youths engage in self-injurious behavior [6]. Moreover, a meta-analysis showed that individuals with mood disorders (anxiety, depression, bipolar, and related disorders) are at higher risk of NSSI compared to normal controls [7]. In an adolescent psychiatric sample, the prevalence of one-time-only NSSI behavior was as high as 60%, and the incidence of recurrent NSSI was approximately 50% [8]. A better understanding of the underlying mechanisms and risk factors for adolescent NSSI is crucial to inform prevention and intervention efforts.
Childhood trauma includes abuse and neglect by family members, especially primary caregivers [9], and has been identified as an important risk factor for the occurrence of NSSI [10] [11]. Neglect can be divided into two categories [12]: (1) physical neglect, where the basic requirements for the child’s survival are not met, such as nutrition and shelter [13].; (2) emotional neglect, where the basic psychological needs of the child are neglected or diluted. Abuse can be divided into the following categories: (1) physical abuse, which is intentional and violent physical injury; (2) emotional abuse, which refers to verbal and other mental attacks that harm a child’s health, including attacks on self-confidence, insults, and other behaviors that hinder a child’s normal growth; (3) sexual abuse, defined as an adult using violence, inducement, or other methods to engage in any form of sexual behavior with a child [14].
The interdependent parent-child relationship is a unique feature of Chinese society and family relationships play an irreplaceable role in the lives of Chinese children [15]. According to attachment theory, children function best when in a safe environment created by their parents. However, if a child does not feel safe, a child’s mind attempts to reduce the threats and create safety by fighting, fleeing, or freezing [16]. When adolescents are exposed to danger, decisions are made instantaneously by the brain; this process primarily involves conditioned responses formed during early childhood rather than complex processes performed by higher-order parts of the brain that are not fully formed until early adulthood (i.e., the prefrontal and anterior cingulate cortex, the parts of the brain responsible for language, associative, and regulatory functions) [17]. That is, the early environment also affects adolescents’ coping styles and behaviors when facing risks [18]. To sum up, childhood experiences also have a fundamental role in subsequent development that cannot be ignored [15]. Importantly, a recent meta-analysis found that adverse childhood experiences have significant independent effects on self-harm [19]. Further, several studies have indicated that childhood trauma can directly [20] or indirectly lead to the development of NSSI [21]. Although there is a time lag, the association between childhood trauma and NSSI in adolescence is significant.
Peer victimization is when an individual is repeatedly and chronically bullied or victimized by one or more peers [22], including: (1) physical victimization, involving physical attacks by peers; (2) verbal victimization, involving verbal abuse by peers; (3) social victimization, involving bullying by peers in a personal relationship; and (4) property victimization, involving stealing or destruction of property by peers [23]. Individuals who have experienced peer victimization have a greater risk of NSSI [24]. In the highly developed modern society, the psychological growth of adolescents is inseparable from the establishment of social relationships with family members, peers, and teachers; peer relationships account for a large proportion of the life of adolescents [25]. The influence of peer relationships on adolescents should not be ignored. According to interpersonal suicide theory (ITS), the desire to die may increase if a sense of burden and frustrated belonging is perceived in core interpersonal interactions, and this desire then leads to self-injury and suicidal behavior Furthermore, integrative motivation-volition theory (IMV) suggests that negative life events, especially feelings that can be internalized as shame or frustration in interpersonal relationships, can lead to feelings of entrapment and subsequent suicidal thoughts and plans [26]. In a study of depressed adolescents, Vergara GA et al. reported that severe peer victimization and bullying led to NSSI [27]. Similarly, in another study, negative peer experiences were found to predict NSSI trajectories in depressed adolescents [28]. In summary, there is considerable evidence for a causal relationship between peer victimization and NSSI [29] [30].
In China, the saying goes ‘a single silk does not make a thread; a single tree does not make a forest’. Collectivism has always been a prominent characteristic of Chinese culture [31]. Even in modern society, there is a continuing cultural association between collectivism and some life domains [31]. In other words, Chinese people are more connected to the people around them, whether it is their family or friends. Several studies have reported that Chinese people have a higher level of dependency compared to people in Western countries [32]. Therefore, relationships between people are of extraordinary significance to the Chinese. Moreover, childhood trauma and peer victimization can be considered to be two different types of interpersonal trauma in adolescent life [33], both of which involve emotional and physical abuse [34]. Therefore, we hypothesized that childhood trauma and peer victimization may play significant roles in adolescent emotional and behavioral problems.
Although the correlation between childhood trauma and NSSI has been well confirmed in previous studies, to date, few studies have examined the mediating factors and underlying mechanisms of this relationship [35]. One of the existing studies found that adolescents who experienced more childhood abuse were also more likely to report peer victimization. In this prospective study, females who suffered childhood trauma (child sexual abuse) were at increased risk of peer victimization. Still, there is a need to explore in more depth the intrinsic links between childhood trauma, peer victimization, and NSSI. Further, at present, the majority of studies on family relationships, friendships, and NSSI are based on Western samples; these relationships have rarely been explored in the Chinese context. Due to the differences in the construction of society and the influence of traditional culture, there may be important differences between Chinese adolescents’ perceptions of interpersonal relationships and the importance they place on them, as compared to their Western counterparts.
In summary, although several risk factors for NSSI have been identified previously [36], there are few published studies on the effects of the external environment on adolescent NSSI. Further, most studies have measured childhood trauma and peer victimization as observable outcomes [37]; however, there are two types of variables: latent variables and observed variables. Latent variables are composed of a series of factor variables that constitute the latent variable, and if latent variables are treated as observed variables and processed directly, biased results may be obtained [38]. Thus, the mediation effect of peer victimization on the relationship between childhood trauma and NSSI was explored using (structural equation modelling) SEM in the current study to explore the influence of early family environment and peer relationships on the NSSI of Chinese adolescents.
Methods
Participants
The current study used data from the Chinese Adolescent Depression Cohort (CADC). Between December 2020 and December 2021, a total of 1783 adolescents (1464 girls and 318 boys) were recruited from the psychiatric outpatient clinics or wards of 14 psychiatric hospitals or general hospitals in nine provinces in China.
The inclusion criteria included: (1)aged 12–18 years; (2) ≥ 6 years of education; (3) the subjects in the NSSI group meet the criteria of NSSI according to the DSM-V, see Additional file 1; (4) patient and family members agree to participate in the project and provide written informed consent form;
The exclusion criteria included: (1) patients with comorbid severe physical, infectious, and immune system disorders; (2) patients with a history of traumatic brain injury, epilepsy, or other known severe neurological disorders or organic brain disorders; (3) patients with a previous history of severe mental disorders such as schizophrenia, mental retardation, autism spectrum, bipolar disorder were excluded, etc. (Fig. 1). (4) patients reported suicidal intent (i.e., self-injury that results in death) when they are engaged NSSI [39]. (5) researchers believed their self-injury behavior is life-threatening.
Procedure
All participants were evaluated by the psychiatric directors. The time of evaluation is about 15 min (some evaluation may take more time than other, which depend on the psychological status of the participants). After pass the evaluation, participants took the questionnaire test under the guidance of psychology or psychiatry graduate students. Prior to the official start of the study, all the researchers were trained to ensure they were familiar with the evaluation process. All tests are carried out in a quiet ward using a tablet computer and take approximately 30 min. The researchers introduce the project to the group of participants and legal guardians at the start of the study. Participants were asked to answer the questions truthfully. After completing the survey, the researcher presented the results to the participant and interpreted them accordingly. All participants provided written informed consent before taking part in the study. The study was approved by the Institutional Review Board (IRB) of Shenzhen Kangning Hospital, Ethics Approval No.: 2020-k021-02.

Sample flow chart. Note: NSSI Non-suicidal self-injury
Measures
Functional assessment of self-mutilation (FASM)
The FASM is a widely used tool to assess NSSI among adolescents. It is divided into 11 types of NSSI behavior and 22 functional domains of NSSI components [40]. The FASM was developed by Lloyd et al.[41]. In the current study, the Chinese version of the FASM was used [42], as this is more suitable for Chinese youth. The Cronbach’s α for the FASM in this study was 0.65.
Short-form childhood trauma questionnaire (CTQ-SF)
The CTQ scale was developed by Bernstein and Fink to detect experiences of child abuse and neglect [34]. It is divided into five subscales: emotional abuse, physical abuse, sexual abuse, emotional neglect, and physical neglect. There are 28 questions in total, and each question is scored on a five-point scale, with the total possible score ranging from 28 to 140; higher scores indicate higher levels of trauma exposure [12]. The scale has good reliability; the Cronbach’s α for the CTQ in this study was 0.84. Moreover, the α coefficients for the five sub-scales ranged from 0.70 (physical neglect) to 0.93(sexual abuse), indicating that the scale has good internal consistency.
Multidimensional peer victimization scale (MPVS)
The MPVS was developed by Mynard and Joseph. It is a 16-item self-report scale covering four dimensions of peer victimization: physical victimization, verbal victimization, social manipulation, and attacks on property [43]. Scores on each of the four dimensions range from 0 to 16, with higher scores indicating more incidents of peer victimization. The MPVS has good reliability and is suitable for measuring bullying victimization (internal consistency: Physical victimization = 0.85; Verbal victimization = 0.75; Social manipulation = 0.77; Property attacks = 0.73). The Cronbach’s α for the total MPVS score in this study was 0.89.
Analytic procedures
The descriptive statistics were compared between the two groups using Welch’s t-tests and Fisher’s exact tests. Preliminary data analyses were conducted using SPSS 22.0 (IBM, Armonk, NY, USA).
Latent variable structural equation modelling (SEM) was adopted to analyze the mediation effect of multidimensional peer victimization on the relationship between childhood trauma and adolescent NSSI. SEM is a data analysis tool that combines path analysis [44] and the common factor model [45]. It can verify a conceptual model and a study’s research hypotheses by specifying relations among observed entities and hypothesized latent constructs [46]. Latent variable models allow researchers to address research questions that directly compare the viability of dimensional, categorical, and hybrid conceptions of constructs and provide greater validity and generalizability by allowing for the correction of measurement error, as compared to methods based on observed variables [47]. In this model, childhood trauma and peer victimization were considered “latent” variables with five observed variables (emotional abuse, physical abuse, sexual abuse, emotional neglect, and physical neglect) [34] and four observed variables (physical victimization, verbal victimization, social manipulation, and attacks on property) [23], respectively. NSSI was estimated as an “observed” variable. A bootstrapping procedure was used to test the direct and indirect effects of the model. The demographic variables age, gender, education, and residence were used as covariates in this study. All modelling procedures were performed using Mplus 8.4.
The fit of the model was tested using chi-square statistic (CMIN), degrees of freedom (df), comparative fit index (CFI), adjusted goodness-of-fit index (AGFI), goodness-of-fit index (GFI), root mean square error of approximation (RMSEA), and Akaike’s Information Criterion [48].
Results
Descriptive statistics
As can be seen in Table 1, the study cohort comprised 318 males (17.8%) and 1464 females (82.2%), ranging in age from 12 to 18 years (mean ± SD = 14.85 ± 1.82). Overall, 66.4% of participants were from urban areas and 33.6% were from rural areas. Approximately half of the participants were in junior high school (55.8%), 4.3% were in primary school, and 39.9% were in senior high school or above. Most of the participants’ parents had a middle school education or above (father, 86.9%; mother, 77.1%).
The mean total CTQ, MPVS, and NSSI scores were 56.02 (± 13.32), 36.32(± 17.21), and 23.10 (± 9.12), respectively. Further, there were significant differences in NSSI, CTQ, and MPVS as a function of age, gender, residence, and education. Specifically, there were significant gender differences in NSSI, with women experiencing more NSSI behaviors than men; the significant differences in residence on PVQ and CTQ, with rural adolescents experiencing more peer bullying and childhood trauma than urban ones. Besides, there were significant Education level and age differences in NSSI, CTQ, MPVS and significant parental education differences in CTQ and MPVS.
Correlation analysis
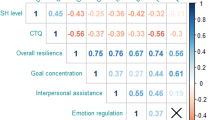
This study found that there was a significant positive correlation between NSSI and CTQ, MPVS; The age of demographic variables was negatively correlated with CTQ and MPVS; There is a significant positive correlation between gender and NSSI, but there is no significant correlation with total score of CTQ and MPVS, and there is a significant correlation with some factors of these two variables (CTQ, emotional abuse; MPVS, physical victimization, verbal victimization). Residence was not significantly associated with NSSI, but showed a significant association with CTQ, MPVS total score, and was not significantly associated with some of the factors of CTQ ( emotional abuse, sexual abuse, emotional neglect, physical neglect). Among demographic variables, age was negatively correlated with gender, and positively correlated with education level; There is a significant negative correlation between gender and education level; Other correlations were not significant(Table 2).
Regression analysis
On the various dimensions of CTQ, emotional abuse, physical abuse, emotional neglect, physical neglect have a significant impact on MPVS, and physical abuse and emotional neglect have a significant impact on NSSI; On the various dimensions of MPVS, physical victimization, verbal victimization and attacks on property have a significant impact on NSSI. In covariates, age, gender, education, resident had a significant impact on MPVS, while gender had no significant impact on MPVS; age and gender had a significant impact on NSSI, while the other covariates had no significant impact on NSSI; Those variables does not exist the serious multicollinearity. The results are shown in Tables 3 and 4.
Mediation analysis
Latent variable SEM was used to test the mediating role of peer victimization in the relationship between childhood trauma and NSSI (Fig. 2). The hypothetical model fit the data well (n = 1,783, CFI = 0.848, TLI = 0.801, RMSEA = 0.086, X2/df = 14.129). The standardized path coefficients from childhood trauma to peer victimization (β = 0.503, p < 0.001) and from peer victimization to NSSI (β = 0.215, p < 0.001) were statistically significant. Moreover, the direct effect of childhood trauma on NSSI was significant (β = 0.244, p < 0.001). The total effect in this model was 0.353, and the mediating effect was 0.109, which accounted for 30.9% of the total effect. The detailed effect sizes of all pathways in the model are presented in Table 2 It can be seen that peer victimization mediated the relationship between childhood trauma and NSSI and that childhood trauma still directly affected NSSI. Adolescents with traumatic experiences in childhood are more likely to experience greater peer victimization in adolescence, which may lead to increased NSSI. Besides, age has significant influences on MPVS, gender has significant influences on NSSI, residence has significant influences on MPVS.

Mediation effect of peer victimization on the link between childhood trauma and non-suicide self-injury. Note: Variables in the dashed box are covariates, included: age, age; gen, gender; edu, education; rsd, resident. CTQ, Childhood Trauma Questionnaire; c1, emotional abuse; c2, physical abuse; c3, sexual abuse; c4, emotional neglect; c5, physical neglect; MPVS, Multidimensional peer victimization Scale; p1, physical victimization; p2, verbal victimization; p3, social manipulation; p4, attacks on property
Besides, due to unbalanced ratio of gender and resident in the study, male subjects and rural subjects were separately selected to make further SEM analysis, the results were similar to the total results. However, the influence of covariates on the main variables is different from the overall research results. Residence has significant influences on MPVS and CTQ in the males subjects, and gender has significant influences on NSSI in rural subjects. This part of results is presented in the appendix.
Discussion
NSSI is a common and serious mental health problem among adolescents. With an increasing body of literature investigating the period of adolescence [49], the impact of early childhood experiences and peer relationship on adolescent problem behaviors is gaining more attention [50]. While several studies have explored the effects of childhood trauma and peer victimization on NSSI [51], the underlying relationships remain unclear. Thus, this study constructed a potential structural model to investigate how childhood trauma and peer victimization influence NSSI among Chinese adolescents. The results revealed that childhood trauma directly affected peer victimization as well as NSSI. Besides, peer victimization directly affected NSSI. And childhood trauma indirectly affected NSSI among Chinese adolescents through peer victimization. These results provide a basis for further exploration of the mechanism underlying NSSI in adolescents.
These findings are consistent with prior research indicating that trauma has a significant independent effect on NSSI [52]. The linear regression analysis shows that in childhood trauma, emotional abuse, physical abuse, emotional neglect and physical neglect both had significant effect on peer victimization. Consistent with previous findings, experiences of childhood emotional abuse and neglect can build maladaptive schemas for children, leading to the increase of the incidence of peer victimization [53]. Besides, people who were frequently victimized (including emotional abuse, physical abuse, etc. ) during childhood, they repeat and perpetuate an “aggressor-victim” interaction in their subsequent relationships [54]. In addition, some study thought that sexual abuse also play a important role in the relationship of early adolescent [55], which need to be estimated in future studies. Furthermore, physical abuse and emotional neglect had more effect on NSSI. The mental and psychological problems associated with physical abuse and neglect are varied. Research studies have found that physical abuse and neglect is associated with a large number of interpersonal, cognitive, emotional, behavioral, and substance abuse problems and psychiatric disorders [56]. In addition, Research shows physical abuse and emotional neglect had the strongest association with adult psychiatric disorders [57]. Therefore, the impact of physical abuse and emotional neglect should be given special attention during the growth of adolescents.
Different dimensions of childhood trauma may have different effects on NSSI. Child maltreatment [58], including emotional abuse [59], physical abuse, sexual abuse, physical neglect, and emotional neglect [60], have been confirmed to be significantly associated with NSSI [61], among which, physical and sexual abuse are more likely to increase the risk of suicide attempts [62]. In another study, emotional neglect and emotional abuse were identified as key factors in NSSI [63]. Childhood abuse affects the normal psychological development of adolescents and has been found to be associated with both depressive and NSSI behavior in adolescence [20]. Another study found that traumatic childhood experiences can lead to psychological dysfunction, which can trigger NSSI [64]. Several studies have also confirmed that a higher burden of adverse childhood experiences is associated with a higher risk of many adverse health, behavioral, psychological, and social outcomes [65]. Traumatic experiences in childhood not only have profound significance for individual psychological well-being and life quality, but also for the development of cognitive function. Several neurobiological studies have confirmed that individual exposure to childhood trauma may lead to a weakened hypothalamic-adrenal axis response [66], and NSSI has a moderating effect on the relationship between childhood trauma and hypothalamic-pituitary-adrenal axis function [67]. In summary, childhood trauma can cause psychological damage to individuals and can affect the structure and function of the brain, leading to long-lasting effects.
In the current study, the latent variable mediation model indicated that childhood trauma can further affect the NSSI of adolescents by influencing their experience of peer victimization. Similarly, our model has also been verified in the sample of individual male and rural subjects. In fact, several scholars have demonstrated that poor childhood experiences (bullying [68], Sexual victimization [69], Guardian incapacity [70], etc.) are among the strongest predictors of peer victimization outside the home during adolescence and later in adulthood [71]. The first potential explanation for this finding is that children who have experienced childhood trauma will repeat these patterns of interaction from their past family environment in their future interpersonal interactions [72]. D. W. Winnicott, a leading psychologist, argued that the formation and development of interpersonal relationships are largely affected by the relationship between the child and their main caregivers in early childhood [73]. Several recent studies have also reported that childhood trauma (maltreatment) in the family context is associated with later peer victimization [74]. Adolescents who have experienced childhood trauma may generalize the non-adaptive behaviors they learned from childhood to their extra-familial interactions, resulting in them being regarded as targets for bullying by peer groups [75]. It is worth noting that some children who have suffered childhood abuse are not only more likely to be bullied, but also to become bullies. Studies have found that these children exhibit higher levels of aggression and antisocial behavior [76], which makes them more likely to hurt others or themselves. Another explanation is that childhood trauma can affect adolescents’ perceptions of interpersonal relationships, resulting in inappropriate behavioral responses. The pioneer of object relation theory, Melanie Klein, found that childhood attachment to family not only affects post-adult relationships, but also alters the way an individual feels and reacts when in the presence of negativity [77]. Disorganized-disoriented parent-child attachment patterns shape an insecure avoidant attachment style; an individual with this attachment pattern tends to exhibit characteristics of jealousy, aggression, and sensitivity to negative stimuli in the process of interpersonal communications, which makes them feel unfulfilled and hurt in the relationship [78]. Certain characteristics, like indecisiveness, sensitivity, unconditional compliance, and so on can make a victimized children more likely to be the target of other forms of assault [75].
Peer victimization is a significant predictor of NSSI [79]. In all dimensions of peer victimization, physical victimization, verbal victimization and attacks on property had more effect on NSSI under controlling other related factors. Similar results have been found in previous studies. In a cross-lagged panel study, sleep problems may be a consequence of physical victimization [80]. And sleep problems is linked with NSSI, including NSSI history and intensity of urges to engage in NSSI [81]. Moreover, a study of juvenile offenders found that direct, indirect physical assault and verbal assault are common injuries to juvenile offenders [82]. The various forms of victimization experienced by these juvenile offenders affect their physical and psychological well-being and lead to various problematic behaviors. Although there are few studies on attacks on property, but it is also an important factor in victimization. It is pointed out in some researches that peer victimization is the most salient peer stressor to affect physical health outcomes in adolescence [83], could induce more NSSI [27].
In the general stress theory of Agnew, personal pressure or extra-personal stressors can lead to negative emotions and behaviors [84], and some teenagers could adopt dangerous behaviors such as NSSI in order to release these bad feelings [85]. Moreover, peer victimization is a major source of stress [84], and adolescents who have been bullied often have difficulty adjusting to school or society, which may increase the risk of them engaging in self-hurt behaviors. The interpersonal model proposes that NSSI can be used by teenagers as a negative coping strategy to reduce stress or tension caused by adverse interpersonal events [41]. However, as NSSI increases, peer bullying may be more prevalent and can lead to more subsequent NSSI [86].
Childhood trauma and peer victimization can be seen as injuries from the outside while NSSI, by definition, is a form of self-inflicted injury [87]. Actions play a key role in providing ‘meaning’ for the feelings [88]; in other words, self-injury behavior reflects, to some extent, the individual’s inner feelings after experiencing external abuse and harm. Hence, an understanding of the interaction between these three types of injury may have important implications for further understanding of the true psychological state of adolescents with NSSI, and thus, appropriate psychological interventions. Although there is still much room for further exploration of the internal mechanisms underlying the connections between the three concepts, several available studies offer potential explanations for the relationships observed in the current study. For example, several recent studies have demonstrated that adolescents who are exposed to negative parents may learn that they are inferior, have vulnerable self-esteem, and may become less able to express their true feelings [89]. Coupled with the experience of peer victimization, this can make it difficult for such adolescents to obtain sufficient social support for their psychological issues, resulting in the adoption of negative coping behaviors, such as NSSI, to express their anger [90]. Studies also indicate that both peer victimization [91]. and childhood trauma [92] are associated with negative long-term and short-term psychiatric, educational, and medical outcomes and increased risk of self-injurious behavior. In conclusion, childhood trauma and peer victimization are among the antecedent factors that contribute to the development of NSSI. Thus, it is important that both researchers and clinicians pay attention to the impact of the early environment and current circumstances on the mental health of adolescents. Timely interventions will be needed to shift the trajectory of development in a positive direction, providing beneficial effects on the physical and mental health of adolescents.
In the study, we also found that gender had a significant effect on NSSI. The finding is consistent with past researches, females report a higher prevalence of NSSI compared to males [93], in addition to literature reporting that NSSI behaviors are more common in females aged 16–19 years [94]. There is no gender difference in childhood trauma, which is different from previous studies. Some researches showed that women experienced more childhood trauma, especially with emotional abuse [95], compared to men. Possibly because of the development of the economy, the concept of “son preference” of out-dated ideas is changed by “gender equality”, girls also get better care [96]. And there was no significant gender difference in peer victimization. The similar results were found in previous study, and depressive symptoms and stressful life events mediate the association between peer victimization and NSSI in adolescents, [97]. Previous studies have noted significant gender differences in the effects of childhood trauma on peer victimization. A prospective study reported that females who suffered child sexual abuse were at increased risk of peer victimization compared to males [98]. However, some studies also found that there are no gender differences in physical violence in childhood trauma, i.e., both boys and girls who are physically abused in childhood are at increased risk of peer intimidation and physical assault in adolescence [99].This could be explored further in future studies.
Finally, there are several limitations of this study that should be noted. First, the demographic distribution of the same was uneven; the proportion of female subjects was much larger than that of male subjects, and the proportion of urban subjects was much larger than that of rural subjects. This may have had an impact on the findings and the effects of the covariates. Second, there is a long period of time between childhood and young adulthood, and during this time there are likely many other influences on the development of NSSI that have not been explored in this study. Third, given the samples were collected from the clinical, most of subjects are patients with emotional disorders, thus patients with depression are not completely excluded. Fourth, other demographic variables like family income were not collected in this study. We will consider to include more demographic variable in future study. Fifth, there are memory bias existed to impact the assessment of childhood trauma, and memory bias will also be affected by gender, age, residence, education level, etc. In future research, we can consider using longitudinal research or combining self-evaluation with other evaluation methods to reduce recall bias to improve the validity of the study. Nonetheless, this study provides an evidence base for further investigation of the risk factors for NSSI. In the future, longitudinal studies should explore the causal mechanisms underlying the influence of childhood trauma on NSSI and the potential roles of other important risk factors.
Conclusion
In conclusion, this study used SEM to model the relationship between the latent variables of childhood trauma (c1, emotional abuse; c2, physical abuse; c3, sexual abuse; c4, emotional neglect; c5, physical neglect) and peer victimization (p1, physical victimization; p2, verbal victimization; p3, social manipulation; p4, attacks on property). The SEM analysis demonstrated that peer victimization mediates the relationship between childhood trauma and NSSI. In addition, several covariates (such as age, gender, education level, and place of residence) regulated the relationship between peer victimization and NSSI. These results suggest that researchers and clinicians should pay attention to the associations between childhood trauma, peer victimization, and NSSI, as well as the influences of age, gender, education level, and place of residence on adolescent problem behaviors. This may help to inform the development of interventions for adolescent psychological and behavioral problems.
Data availability
The datasets generated and/or analyzed during the current study are not publicly available due to limitations of ethical approval involving the patient data and anonymity but are available from the corresponding author on reasonable request.
References
Whitlock J, Muehlenkamp J, Eckenrode J, Purington A, Baral Abrams G, Barreira P, Kress V. Nonsuicidal self-injury as a gateway to suicide in young adults. J Adolesc Health. 2013;52(4):486–92.
Kim H, Ryu JM, Kim HW. Characteristics and Trends of suicide attempt or non-suicidal self-injury in children and adolescents visiting Emergency Department. J Korean Med Sci. 2020;35(33):e276.
Muehlenkamp JJ, Claes L, Havertape L, Plener PL. International prevalence of adolescent non-suicidal self-injury and deliberate self-harm. Child Adolesc Psychiatry Ment Health. 2012;6:10.
Hilario BF, Roberto F-F, Laura C, Lourdes F, Rosa PB, Jose DL. The addictive model of self-harming (non-suicidal and suicidal) behavior. Front Psychiatry. 2016;7(4):8.
Zhao S, Hu J, Li D, Wan Y, Zhao L, Fang J, Zhang S. Associations of being bullied and non-suicidal self-injury with suicidal behaviors among Chinese adolescents. Curr Psychol 2021:1–9.
Liu Y, Xiao Y, Ran H, He X, Jiang L, Wang T, Yang RX, Xu X, Yang G, Lu J. Association between parenting and non-suicidal self-injury among adolescents in Yunnan, China: a cross-sectional survey. PeerJ. 2020;8:e10493.
Akram B, Batool M, Rafi Z, Akram A. Prevalence and predictors of Non-Suicidal Self-Injury among children with Autism Spectrum Disorder. Pak J Med Sci. 2017;33(5):1225–9.
Kaess M, Parzer P, Mattern M, Plener PL, Bifulco A, Resch F, Brunner R. Adverse childhood experiences and their impact on frequency, severity, and the individual function of nonsuicidal self-injury in youth. Psychiatry Res. 2013;206(2–3):265–72.
Bernstein DP, Fink L, Handelsman L, Foote J, Lovejoy M, Wenzel K, Sapareto E, Ruggiero J. Initial reliability and validity of a new retrospective measure of child abuse and neglect. Am J Psychiatry. 1994;151(8):1132–6.
Brown RC, Plener PL. Non-suicidal Self-Injury in Adolescence. Curr Psychiatry Rep. 2017;19(3):20.
Klonsky ED, Moyer A. Childhood sexual abuse and non-suicidal self-injury: meta-analysis. Br J Psychiatry. 2008;192(3):166–70.
Xiang Z, Liu Z, Cao H, Wu Z, Long Y. Evaluation on long-term test-retest reliability of the short-form Childhood Trauma Questionnaire in patients with Schizophrenia. Psychol Res Behav Manag. 2021;14:1033–40.
Rosenberg SD, Lu W, Mueser KT, Jankowski MK, Cournos F. Correlates of adverse childhood events among adults with schizophrenia spectrum disorders. Psychiatr Serv. 2007;58(2):245–53.
Arseneault L, Cannon M, Fisher HL, Polanczyk G, Moffitt TE, Caspi A. Childhood trauma and children’s emerging psychotic symptoms: a genetically sensitive longitudinal cohort study. Am J Psychiatry. 2011;168(1):65–72.
Dale LP, O’Hara EA, Keen J, Porges SW. Infant regulatory disorders: temperamental, physiological, and behavioral features. J Dev Behav Pediatr. 2011;32(3):216–24.
Blackman-Nandi J. Building the bonds of attachment: awakening love in deeply traumatized children. Therapy Today. 2018;29(8):17–7.
Schore AN. Attachment and the regulation of the right brain. Attach Hum Dev. 2000;2(1):23–47.
Yates TM, Carlson EA, Egeland B. A prospective study of child maltreatment and self-injurious behavior in a community sample. Dev Psychopathol. 2008;20(2):651–71.
Liu RT, Scopelliti KM, Pittman SK, Zamora AS. Childhood maltreatment and non-suicidal self-injury: a systematic review and meta-analysis. Lancet Psychiatry. 2018;5(1):51–64.
Wen Y, Zhang X, Xu Y, Qiao D, Guo S, Sun N, Yang C, Han M, Liu Z. Cognitive impairment in adolescent major depressive disorder with Nonsuicidal Self-Injury: evidence based on multi-indicator ERPs. Front Hum Neurosci. 2021;15:637407.
Taş Torun Y, Gul H, Yaylali FH, Gul A. Intra/interpersonal functions of non-suicidal self-injury in adolescents with major depressive disorder: the role of emotion regulation, Alexithymia, and Childhood Traumas. Psychiatry. 2022;85(1):86–99.
Wang Q. Association of Childhood Intrafamilial aggression and childhood peer bullying with adult depressive symptoms in China. JAMA Netw Open. 2020;3(8):e2012557.
Eastman ML, Moore AA, Cecilione J, Hettema JM, Roberson-Nay R. Confirmatory factor structure and psychometric properties of the multidimensional peer victimization scale. J Psychopathol Behav Assess. 2018;40(4):725–35.
Jantzer V, Haffner J, Parzer P, Resch F, Kaess M. Does parental monitoring moderate the relationship between bullying and adolescent nonsuicidal self-injury and suicidal behavior? A community-based self-report study of adolescents in Germany. BMC Public Health. 2015;15:583.
Demerval R, Cartierre N, Coulon N. The Effects of Family and School Disaffiliation on the Health of Adolescents. 2003.
O’Connor, Rory C, Kirtley, Olivia J. The integrated motivational-volitional model of suicidal behaviour. Philosophical Trans Royal Soc Lond Ser B Biol Sci 2018, 373(1754).
Vergara GA, Stewart JG, Cosby EA, Lincoln SH, Auerbach RP. Non-suicidal self-injury and suicide in depressed adolescents: impact of peer victimization and bullying. J Affect Disord. 2019;245:744–9.
Giletta M, Prinstein MJ, Abela JR, Gibb BE, Barrocas AL, Hankin BL. Trajectories of suicide ideation and nonsuicidal self-injury among adolescents in mainland China: peer predictors, joint development, and risk for suicide attempts. J Consult Clin Psychol. 2015;83(2):265–79.
Claes L, Luyckx K, Baetens I, Van de Ven M, Witteman C. Bullying and victimization, depressive Mood, and Non-Suicidal Self-Injury in Adolescents: the moderating role of parental support. J Child Fam stud. 2015;24(11):3363–71.
Moore SE, Norman RE, Suetani S, Thomas HJ, Sly PD, Scott JG. Consequences of bullying victimization in childhood and adolescence: a systematic review and meta-analysis. World J Psychiatry. 2017;7(1):60–76.
Hamamura T, Chen Z, Chan CS, Chen SX, Kobayashi T. Individualism with chinese characteristics? Discerning cultural shifts in China using 50 years of printed texts. Am Psychol. 2021;76(6):888–903.
Wei M, Su JC, Carrera S, Lin SP, Yi F. Suppression and interpersonal harmony: a cross-cultural comparison between chinese and european Americans. J Couns Psychol. 2013;60(4):625–33.
Yoo Y, Park HJ, Park S, Cho MJ, Cho SJ, Lee JY, Choi SH, Lee JY. Interpersonal trauma moderates the relationship between personality factors and suicidality of individuals with posttraumatic stress disorder. PLoS ONE. 2018;13(1):e0191198.
Petrikova M, Kascakova N, Furstova J, Hasto J, Tavel P. Validation and Adaptation of the Slovak Version of the Childhood Trauma Questionnaire (CTQ). Int J Environ Res Public Health 2021, 18(5).
Serafini G, Canepa G, Adavastro G, Nebbia J, Belvederi Murri M, Erbuto D, Pocai B, Fiorillo A, Pompili M, Flouri E, et al. The relationship between Childhood Maltreatment and Non-Suicidal Self-Injury: a systematic review. Front Psychiatry. 2017;8:149.
Ballard E, Bosk A, Pao M. Invited commentary: understanding brain mechanisms of pain processing in adolescents’ non-suicidal self-injury. J Youth Adolesc. 2010;39(4):327–34.
Zhang L, Ma X, Yu X, Ye M, Li N, Lu S, Wang J. Childhood Trauma and Psychological Distress: A Serial Mediation Model among Chinese Adolescents. Int J Environ Res Public Health 2021, 18(13).
Bollen KA. Latent variables in psychology and the social sciences. Annu Rev Psychol. 2002;53:605–34.
Nock MK. Self-Injury. Ann Rev Clin Psychol. 2010;6(1):339–63.
Young R, Sproeber N, Groschwitz RC, Preiss M, Plener PL. Why alternative teenagers self-harm: exploring the link between non-suicidal self-injury, attempted suicide and adolescent identity. BMC Psychiatry. 2014;14:137.
Lloyd-Richardson EE, Perrine N, Dierker L, Kelley ML. Characteristics and functions of non-suicidal self-injury in a community sample of adolescents. Psychol Med. 2007;37(8):1183–92.
Qu D, Wang Y, Zhang Z, Meng L, Zhu F, Zheng T, He K, Zhou Y, Li C, Bu H, et al. Psychometric Properties of the Chinese Version of the Functional Assessment of Self-Mutilation (FASM) in chinese clinical adolescents. Front Psychiatry. 2021;12:755857.
Mynard H, Joseph S. Development of the multidimensional peer-victimization scale. Aggressive Behav. 2000;26(2):169–78.
Wright S. The method of path coefficient analysis. 1934.
Sellbom M, Tellegen A. Factor analysis in psychological assessment research: common pitfalls and recommendations. Psychol Assess. 2019;31(12):1428–41.
Brandmaier AM, von Oertzen T, McArdle JJ, Lindenberger U. Structural equation model trees. Psychol Methods. 2013;18(1):71–86.
Miettunen J, Nordström T, Kaakinen M, Ahmed AO. Latent variable mixture modeling in psychiatric research–a review and application. Psychol Med. 2016;46(3):457–67.
Schermelleh-Engel K, Kerwer M, Klein AG. Evaluation of model fit in nonlinear multilevel structural equation modeling. Front Psychol. 2014;5:181.
Modrowski CA, Chaplo SD, Kerig PK, Mozley MM. Trauma exposure, posttraumatic overmodulation and undermodulation, and nonsuicidal self-injury in traumatized justice-involved adolescents. Psychol Trauma. 2019;11(7):743–50.
Wang X, Yang J, Wang P, Zhang Y, Li B, Xie X, Lei L. Deviant peer Affiliation and bullying perpetration in adolescents: the mediating role of Moral Disengagement and the moderating role of Moral Identity. J Psychol. 2020;154(3):199–213.
Stewart JG, Valeri L, Esposito EC, Auerbach RP. Peer victimization and suicidal thoughts and behaviors in depressed adolescents. J Abnorm Child Psychol. 2018;46(3):581–96.
Barbosa LP, Quevedo L, da Silva Gdel G, Jansen K, Pinheiro RT, Branco J, Lara D, Oses J, da Silva RA. Childhood trauma and suicide risk in a sample of young individuals aged 14–35 years in southern Brazil. Child Abuse Negl. 2014;38(7):1191–6.
May T, Younan R, Pilkington PD. Adolescent maladaptive schemas and childhood abuse and neglect: a systematic review and meta-analysis. Clin Psychol Psychother. 2022;29(4):1159–71.
Green AH. Child maltreatment and its victims. A comparison of physical and sexual abuse. Psychiatr Clin North Am. 1988;11(4):591–610.
Nagata JM, Trompeter N, Singh G, Raney J, Ganson KT, Testa A, Jackson DB, Murray SB, Baker FC. Adverse childhood experiences and early adolescent cyberbullying in the United States. J Adolesc 2022.
Kaplan SJ, Pelcovitz D, Labruna V. Child and adolescent abuse and neglect research: a review of the past 10 years. Part I: physical and emotional abuse and neglect. J Am Acad Child Adolesc Psychiatry. 1999;38(10):1214–22.
Salokangas RKR, Schultze-Lutter F, Schmidt SJ, Pesonen H, Luutonen S, Patterson P, von Graf H, Heinimaa M, From T, Hietala J. Childhood physical abuse and emotional neglect are specifically associated with adult mental disorders. J Ment Health. 2020;29(4):376–84.
Brown RC, Heines S, Witt A, Braehler E, Fegert JM, Harsch D, Plener PL. The impact of child maltreatment on non-suicidal self-injury: data from a representative sample of the general population. BMC Psychiatry. 2018;18(1):181.
Vieira AI, Machado BC, Moreira CS, Machado PPP, Brandão I, Roma-Torres A, Gonçalves S. Eating disorders and non-suicidal self-injury: structural equation modelling of a conceptual model. Eur Eat Disord Rev. 2018;26(5):431–7.
Paul E, Ortin A. Correlates of suicidal ideation and self-harm in early childhood in a cohort at risk for child abuse and neglect. Arch Suicide Res. 2019;23(1):134–50.
Martin J, Bureau JF, Yurkowski K, Fournier TR, Lafontaine MF, Cloutier P. Family-based risk factors for non-suicidal self-injury: considering influences of maltreatment, adverse family-life experiences, and parent-child relational risk. J Adolesc. 2016;49:170–80.
Guvendeger Doksat N, Zahmacioglu O, Ciftci Demirci A, Kocaman GM, Erdogan A. Association of suicide attempts and Non-Suicidal Self-Injury Behaviors with Substance Use and Family characteristics among children and adolescents seeking treatment for Substance Use Disorder. Subst Use Misuse. 2017;52(5):604–13.
Thomassin K, Shaffer A, Madden A, Londino DL. Specificity of childhood maltreatment and emotion deficit in nonsuicidal self-injury in an inpatient sample of youth. Psychiatry Res. 2016;244:103–8.
Huang C, Yuan Q, Ge M, Sheng X, Yang M, Shi S, Cao P, Ye M, Peng R, Zhou R, et al. Childhood Trauma and Non-suicidal Self-Injury among Chinese Adolescents: the mediating role of psychological sub-health. Front Psychiatry. 2022;13:798369.
Sonu S, Post S, Feinglass J. Adverse childhood experiences and the onset of chronic disease in young adulthood. Prev Med. 2019;123:163–70.
Klaassens ER, van Noorden MS, Giltay EJ, van Pelt J, van Veen T, Zitman FG. Effects of childhood trauma on HPA-axis reactivity in women free of lifetime psychopathology. Prog Neuropsychopharmacol Biol Psychiatry. 2009;33(5):889–94.
Reichl C, Heyer A, Brunner R, Parzer P, Völker JM, Resch F, Kaess M. Hypothalamic-pituitary-adrenal axis, childhood adversity and adolescent nonsuicidal self-injury. Psychoneuroendocrinology. 2016;74:203–11.
Bowes L, Maughan B, Ball H, Shakoor S, Ouellet-Morin I, Caspi A, Moffitt TE, Arseneault L. Chronic bullying victimization across school transitions: the role of genetic and environmental influences. Dev Psychopathol. 2013;25(2):333–46.
Classen CC, Palesh OG, Aggarwal R. Sexual revictimization: a review of the empirical literature. Trauma Violence Abuse. 2005;6(2):103–29.
Lereya ST, Wolke D. Prenatal family adversity and maternal mental health and vulnerability to peer victimisation at school. J Child Psychol Psychiatry. 2013;54(6):644–52.
Widom CS, Czaja SJ, Dutton MA. Childhood victimization and lifetime revictimization. Child Abuse Negl. 2008;32(8):785–96.
Cunningham S, Goff C, Bagby RM, Stewart JG, Larocque C, Mazurka R, Ravindran A, Harkness KL. Maternal- versus paternal-perpetrated maltreatment and risk for sexual and peer bullying revictimization in young women with depression. Child Abuse Negl. 2019;89:111–21.
Dell’Orto S, Caruso E. [W. D. Winnicott and the transitional object in infancy]. Pediatr Med Chir. 2003;25(2):106–12.
Martín-Babarro J, Toldos MP, Paredes-Becerra L, Abregu-Crespo R, Fernández-Sánchez J, Díaz-Caneja CM. Association of different forms of child maltreatment with peer victimization in Mexican Children and Adolescents. Front Psychol. 2021;12:662121.
Lereya ST, Samara M, Wolke D. Parenting behavior and the risk of becoming a victim and a bully/victim: a meta-analysis study. Child Abuse Negl. 2013;37(12):1091–108.
Wodarski JS, Kurtz PD, Gaudin JM Jr, Howing PT. Maltreatment and the school-age child: major academic, socioemotional, and adaptive outcomes. Soc Work. 1990;35(6):506–13.
Spanish AI. [Our adult world and its roots in childhood]. Rev Psicoanal 1961, 18.
KLEIN. : On the development of mental functioning. The International journal of psycho-analysis 2000.
Wolff J, Frazier EA, Esposito-Smythers C, Burke T, Sloan E, Spirito A. Cognitive and social factors associated with NSSI and suicide attempts in psychiatrically hospitalized adolescents. J Abnorm Child Psychol. 2013;41(6):1005–13.
Chen JK, Wu WC. Associations of sleep problems with non-physical bullying perpetration and victimization among adolescents: A cross-lagged panel study. Sleep Health 2022.
Burke TA, Hamilton JL, Seigel D, Kautz M, Liu RT, Alloy LB, Barker DH. Sleep irregularity and nonsuicidal self-injurious urges and behaviors. Sleep 2022, 45(6).
Owusu Ansah K, Atindanbila S, Osei Owusu J, Agyemang Duah C. Patterns of victimization in Ghana’s senior Correctional Center: the experiences of juvenile offenders. Int J Law Psychiatry. 2022;83:101808.
de Bruine M, Denissen JJA, Giletta M. Disentangling the effects of peer status and peer victimization on perceived physical health in adolescence. J Adolesc. 2022;94(3):435–47.
Jennings WG, Maldonado-Molina MM, Reingle J. General Strain Theory. In: Encyclopedia of Adolescence edn. Edited by Levesque RJR. New York, NY: Springer New York; 2011: 1158–1162.
Walters GD, Espelage DL. From victim to victimizer: hostility, anger, and depression as mediators of the bullying victimization-bullying perpetration association. J Sch Psychol. 2018;68:73–83.
Kim YS, Leventhal BL, Koh YJ, Boyce WT. Bullying increased suicide risk: prospective study of korean adolescents. Arch Suicide Res. 2009;13(1):15–30.
Wang Y, Zhou X, Cao B, Chen L, Wang R, Qi L, Meng L, Zeng L, Liu X, Wang W, et al. The psychological characteristics and risk factors of suicidal attempt among mood disorders adolescents accompany with non-suicidal self-injury: a multi-center study. J Affect Disord. 2022;298(Pt A):301–7.
Bernroider G, Panksepp J. Mirrors and feelings: have you seen the actors outside? Neurosci Biobehav Rev. 2011;35(9):2009–16.
Dong H, Zhang W. The Impact of Family on Bullies and Victims. J Shandong Normal University(Social Sci Ed) 2005.
Kim Y, Lee H, Park A. Patterns of adverse childhood experiences and depressive symptoms: self-esteem as a mediating mechanism. Soc Psychiatry Psychiatr Epidemiol. 2022;57(2):331–41.
Takizawa R, Maughan B, Arseneault L. Adult health outcomes of childhood bullying victimization: evidence from a five-decade longitudinal british birth cohort. Am J Psychiatry. 2014;171(7):777–84.
Green JG, McLaughlin KA, Berglund PA, Gruber MJ, Sampson NA, Zaslavsky AM, Kessler RC. Childhood adversities and adult psychiatric disorders in the national comorbidity survey replication I: associations with first onset of DSM-IV disorders. Arch Gen Psychiatry. 2010;67(2):113–23.
Sornberger MJ, Heath NL, Toste JR, McLouth R. Nonsuicidal self-injury and gender: patterns of prevalence, methods, and locations among adolescents. Suicide Life Threat Behav. 2012;42(3):266–78.
Wilkinson PO, Qiu T, Jesmont C, Neufeld SAS, Kaur SP, Jones PB, Goodyer IM. Age and gender effects on non-suicidal self-injury, and their interplay with psychological distress. J Affect Disord. 2022;306:240–5.
Bernegger A, Kienesberger K, Carlberg L, Swoboda P, Ludwig B, Koller R, Kapusta ND, Aigner M, Haslacher H, Schmöger M, et al. Influence of sex on suicidal phenotypes in affective disorder patients with traumatic childhood experiences. PLoS ONE. 2015;10(9):e0137763.
FangJia. The transformation of the concept of valuing men over women in rural China. Shaanxi Normal University; 2017.
Wang Q, Liu X. Peer victimization, depressive symptoms and non-suicidal self-injury behavior in Chinese migrant children: the roles of gender and stressful life events. Psychol Res Behav Manage 2019, 12.
Kennedy RS, Font SA, Haag AC, Noll JG. Childhood sexual abuse and exposure to peer bullying victimization. J Interpers Violence. 2022;37(19–20):Np18589–np18613.
Benedini KM, Fagan AA, Gibson CL. The cycle of victimization: the relationship between childhood maltreatment and adolescent peer victimization. Child Abuse Negl. 2016;59:111–21.
Acknowledgements
The authors would like to thank Shenzhen Kangning Hospital, the Affiliated Kangning Hospital of Wenzhou Medical University and other 12 psychiatric hospitals or general hospitals in nine provinces in China for their dedication in creating the Chinese Adolescent Depression Cohort (CADC). In addition, we are grateful to participants who actively cooperated with the researchers to collect data.
Funding
This study was supported by Zhejiang Provincial Natural Science Foundation of China (NO. LY22H090022), Shenzhen Fund for Guangdong Provincial High-level Clinical Key Specialties (No.SZGSP013), Shenzhen Science and technology research and Development Fund for Sustainable development project (No.KCXFZ20201221173613036), Zhejiang Provincial Medical health Project (NO. 2022RC256), Wenzhou Science and Technology Bureau project (NO. Y20210761, NO.S20180012).
Author information
Authors and Affiliations
Contributions
KZ and ST made great contributions to the conception, design, data acquisition, manuscript writing, and modification of this study. KY, TZ and KZ organized the database. ST conducted the statistical analysis. ST, LH, SY, WY, YX, ZF and JZ were responsible for collecting and pretreating the data. ST and SY wrote the first draft of the manuscript. All authors reviewed the final version of the manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
The study procedures were carried out in accordance with the Declaration of Helsinki. All methods were carried out in accordance with relevant guidelines and regulations. The study was approved by the Institutional Review Board (IRB) of Shenzhen Kangning Hospital, Ethics Approval No. 2020-k021-02. All subjects and/or their legal guardian(s) were informed about the study, and all provided informed consent.
Consent for publication
Not Applicable.
Competing interests
There are no conflicts of interest or competing interests associated to this study.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Zhao, K., Tong, S., Hong, L. et al. Childhood trauma, peer victimization, and non-suicidal self-injury among Chinese adolescents: a latent variable mediation analysis. BMC Psychiatry 23, 436 (2023). https://doi.org/10.1186/s12888-023-04848-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12888-023-04848-z