
Abstract
Background
Natural disasters cause long term psychological consequences, especially post-traumatic stress disorders. It has been regarded as the most prevalent of psychiatric disorders after a natural disaster. The purpose of this study is to estimate the prevalence of Post-Traumatic Stress Disorder (PTSD) and determine its associated factors in adult survivors three years after the 2015 Nepal earthquake.
Methods
A cross-sectional descriptive design was used where 1076 adults within the age range of 19–65 were randomly selected and interviewed from four adversely affected districts due to the 2015 earthquake. Instruments included a demographic questionnaire, an earthquake exposure questionnaire, the Oslo Social Support Scale (OSSS), and the Post-traumatic Stress Disorder Checklist-Civilian Version (PCL-C). Descriptive and inferential statistics were applied using Statistical Package for Social Science (SPSS) Version 16 for data analysis.
Results
The prevalence of PTSD among earthquake survivors was 18.9%. The multivariate logistic regression showed that gender, ethnicity, education, occupation, social support and severity of damage to house and property were significantly associated with PTSD. Odds of having PTSD was 1.6 times higher among females (AOR = 1.6, 95% CI: 1.1–2.3) and nearly 2 times higher amongst illiterate survivors (AOR = 1.9, 95% CI: 1.2–2.8). Participants from the Janajati ethnic group and those who had a business occupation had a 50% lower risk of having PTSD. Around 39% of the participants had moderate social support and had 60% lower odds of having PTSD compared to those with poor social support (AOR = 0.4, 95%CI: 0.2–0.5, p < 0.001). Participants with medium and very high-level damage to personal property were more likely to have PTSD.
Conclusion
Post-traumatic stress disorder remained prevalent amongst survivors three years after the 2015 Nepal Earthquake. It is important to provide psychological and social support for survivors to decrease the health burden from PTSD. Socio-demographic characteristics such as females, farmers, those survivors who endured significant personal property damage were at higher risk.
Similar content being viewed by others

Background
Nepal was hit by a devastating 7.8 magnitude earthquake with its epicenter in Barpak, Gorkha District, northwest of Kathmandu, at 11:55 a.m on April 25, 2015 (Nepal Standard Time). 17 days later, on May 12, 2015, another 6.8 magnitude aftershock caused further damage and suffering [1]. These two large earthquakes resulted in considerable property damage. In several districts, people's lives and infrastructure were in jeopardy [2]. The earthquake caused 8,896 fatalities and 22,303 seriously injured patients. More than 600,000 households were fully damaged leaving 300,000 partially damaged. Of these households, it is estimated that 450,000 people remained homeless [1, 3]. According to the World Health Organization (WHO), 20% of people in post-earthquake and other humanitarian situations experience psychological distress, with a lower minority (3–4%) experiencing severe mental disorders [4].
Earthquakes are one of the world’s major calamities. With very little warning, it destroys personal property and lives [5]. It may affect people physically as well as mentally, causing them to be more afraid of the earthquake due to its unpredictable and unforeseen nature [6].These experiences can be traumatic especially to the children, women and elderly [5]. Physical injuries can be treatable, as it can be viewed externally, but mental injury is often ignored as it is not visible [5].
More than two-thirds of the world's populations have experienced an earthquake at some point in their lives, resulting in a wide range of mental and physical health consequences [2]. Approximately two-thirds of the PTSD patients may improve over time, while for others, it may continue to damage their cognitive and behavioral functioning for years. As a result, it is necessary to give ancillary resources and social support in the aftermath of an earthquake to assist individuals in coping with stressful effects of an earthquake [5].
Numerous previous studies outside of Nepal have shown the prevalence rate of depression after earthquakes ranging from 16 to 28 percent, while PTSD prevalence rates range from 7 to 40 percent [7,8,9]. Similarly, a study done in China (Wenchuan, 2008) found that the prevalence of PTSD in earthquake survivors varied from 10.3 to 66%. Prevalence correlated with the level of trauma exposure and proximity to the epicenter of the earthquake [10]. Another study one year after the 2008 Wenchuan earthquake showed that the prevalence of PTSD was 40.1% in Wenchuan, China, over the four-year period following its 2008 [8]. According to a systematic review of mental health disorders following the Great East Japan Earthquake in 2011, the reported prevalence of PTSD ranged from 10 to 53.5%, while the prevalence of depression ranged from 3.0 to 43.7% [11].
Previous mental health research in Nepal has focused on heightened rates of psychological distress among a substantial proportion of the population affected by the 2015 Nepal earthquakes, with a smaller proportion reporting more severe mental health and psychosocial difficulties [3]. Research conducted in 2015 Dhadingdistrict earthquake survivors showed the prevalence of PTSD at 18.5% [5]. Another study amongstadolescents in Sindhupalchok and Kathmandu districts showed a PTSD prevalence of 39.5% and 10.7% three years after the earthquake [12]. The literature review retrieved PTSD measures immediately after earthquakes at 4, 9, 10 and 14 months in Nepal, concluding that PTSD remains for a long time [2, 5, 13, 14].
According to cross-sectional community-based research, 27.5 percent to 33.7 percent of individuals passed the Beck Depression Inventory criterion for depression, 22.9 percent to 27.7 percent for anxiety and 9.6 percent for PTSD [15, 16]. According to longitudinal follow-up, the frequency was higher among women and older age groups, as well as following armed conflict [16, 17].
In a quantitative survey of 513 community members, those with symptom scores suggesting depression (34.2 percent), anxiety (33.8 percent), and alcohol-use issues (20.4%) were in greater proportions than those with PTSD symptoms (5.2 percent) [3]. In the four months following the earthquake, the prevalence of suicidal ideation was alarmingly high, at 10.9 percent [3, 18].
According to a study by S. Sherchan et al., following the earthquake, mental health services were offered in the form of hospital-based clinical services, mobile health camps, and health worker training workshops to deliver basic mental health services [19].
Despite the fact that long-term psychological consequences of disasters are significant and common, little attention has been paid to the long-term psychological consequences of disasters [20]. More research on the long-term psychosocial consequences of disasters is neededespecially in Nepal as the country is at risk of major earthquakes in the future [21, 22]. To our knowledge, little research has been conducted in this area 3 years after the Nepal earthquake. Few studies have researched prevalence or quality of life in individuals with trauma/PTSD [23]. A systematic review revealed that most of the research was done 1 to 20 months after the 2015 earthquake in Nepal in limited earthquake affected areas only [24]. The finding of PTSD was mostly present among the earthquake survivors with rates varying from 4.9% to 51%. Gender and age were associated factors for this study. However, earthquake related variables weren't observed in this study [24]. Therefore, the goal of this study is to fill a gap in the literature by looking at the prevalence of PTSD and associated socio-demographic factors in adult survivors who are living in the most affected areas beyond 3 years after the 2015 earthquake. The identification of variables that are of influence in the 2015 earthquake in Nepal can educate and assist researchers in future exploration of the topic.
Methods
Study design, site and study population
The research was a descriptive cross-sectional study conducted in four earthquake-affected districts (Gorkha, Dolakha, Sindhupalchowk and Bhaktapur) in 2019, three years after the Nepal earthquake. The study population were young, middle and older adults who were the survivors of the devastating earthquake. Data was collected from 1076 randomly selected adults from the four adversely-affected districts. Participants aged between 19 and 65 years, who had experienced the earthquake, 2015 in Nepal and spoke Nepali were included in the study. Participants who had hearing problems, poor verbal communication, severe disease conditions, who were already identified or recorded in a health facility as intellectually disabled, dementia or any other major psychosis, and severe mental disorders under medication were excluded from the study.
Sampling strategy
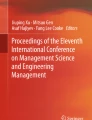
Sample size calculation was done (Fig. 1) for the four most earthquake affected districts (Gorkha, Dolakha, Sindhupalchowk and Bhaktapur). The sample size from Gorkha was 358, 182 from Dolakha, 256 from Sindhupalchowk and 280 from Bhaktapur to make the final sample size of 1076.

Flowchart of sampling strategy
Multi-stage random sampling was done. At the first stage (firstly), three rural municipalities (Gorkha, Dolakha, Sindhupalchowk) and one urban municipality (Bhaktapur) were selected randomly. The list of the total number of administrative wards in each of the four municipalities and the total number of houses destroyed in each of the wards was obtained from the ward offices. The household destruction percentage of each ward was calculated. On the basis of the household destruction percentage, the wards with over 50 percent household destruction were considered as the most affected. Secondly, one of the most affected wards was selected through simple random sampling (lottery method) from each four municipalities. Thirdly, systematic random sampling was done to select households. Due to the earthquake and internal migration, it was difficult to determine the population size and the list of people (age 19–65 years) in selected wards.
The total number of households and the sampling frame (list of households) in the selected wards were obtained from respective ward offices. The total number of present households in each ward was divided by the required sample size of the respective ward to determine the different kth intervals for each of the four wards.
The first household was selected through a lottery method. Then, every kth household was selected for the study from the list of households in each ward accordingly until the required sample size was met. Only one participant of age 19 to 65 years within a household was recruited for interview through lottery method to ensure independence of study subjects.
Ethical considerations
This study was approved by the Institutional Review Committee of Kathmandu University School of Medical Sciences at Dhulikhel, Nepal. All participants were informed about the purpose and procedures of the study. Participation in the study was voluntary. They were allowed to withdraw their consent and discontinue the research interview at any time. Before the interview began, written informed consent was taken from the participants. Anonymity and privacy of the participants were maintained during data collection.
Data collection tools
Face to face interview was conducted using a structured questionnaire. Before data collection, four enumerators with Bachelor’s degree in nursing were called together to review the questionnaire and each item was explained. They were also trained for face-to-face interview methods. The first part of the questionnaire included socio-demographic questionnaire such as age, gender, marital status, ethnicity, religion, occupation and literacy status. The second part included a questionnaire about earthquake exposure such as self-injury, loss of family or friends, loss of house and property, witness of burial, etc. Earthquake exposure was considered “Exposed” when participants answered “Yes” to any of these earthquake exposure related questionnaires.
In the third part, post-traumatic stress symptoms were assessed using the subscale of PTSD Checklist-Civilian Version (PCL-C) to assess PTSD prevalence. The PCL-C version is a commonly used instrument to assess PTSD. It has 17 items which measures three clusters of symptoms that record into diagnostic Criteria B (re-experiencing), C (avoidance/ numbing), and D (hyperarousal) for PTSD in the Diagnostic statistical manual for mental health (DSM-IV) was adopted (Ni et al., 2013) [25, 26]. This tool allows the participant to indicate the extent to which each symptom is correlated with the earthquake on a scale from 1 (not at all) to 5 (extremely). The Nepali translated version of the PCL-C was administered for measuring PTSD. The value of Cronbach alpha in this study for PCL-C was found to be 0.95, which possesses excellent internal consistency. All three clusters of symptoms were found to be acceptable in this study setting. The area under the curve for B, C and D groups of symptoms were 0.97, 0.98, and 0.96 respectively, which shows the tool is acceptable in Nepalese contests [5]. A provisional PTSD diagnosis can be made by adding up all items for a total severity score or treat response categories 3–5 (moderately or above) as symptomatic and responses 1–2 (below moderately) as non-symptomatic, then the DSM criteria is used for its diagnosis. The maximal total score for 17 items is 85. Participants with a score of 50 or greater were classified as having probable PTSD. With a PCL-C score of 50 as the diagnostic cut-off, the sensitivity was approximately 80% [23, 27,28,29,30,31,32,33,34]. According to a study done in Nepal, the value of Cronbach alpha of PCL-C was found to be 0.95, which possesses excellent internal consistency [5]. The PCL-C was previously validated in Nepal with total scores of 50 or above indicative of probable PTSD (Thapa&Hauff, 2005, Dhungana, 2021) [3, 23, 35]. Besides Nepal, a study done in 3372 pregnant women in Peru revealed the reliability of the PCL-C was excellent (α = 0.90). Receiver operating characteristics analysis showed that a cut-off score of 26 offered optimal discriminatory power, with sensitivity of 0.86 (95% CI: 0.78 – 0.92) and a specificity was found of 0.63 (95% CI: 0.62 – 0.65) [36].
The social support scale was the fourth section of the questionnaire. The Oslo 3-items Social Support Scale (OSSS-3) is one of the best indicators of mental health since it is a brief measure of social functioning. It assesses the number of persons with whom the respondent feels close, as well as the level of attention and care provided by others and the ease with which they can seek practical assistance. The Oslo Social Support scale scores ranged from 3–14, with 3–8 indicating low (poor) support, 9–11 indicating moderate support, and 12–14 indicating strong support [37]. Internal consistency for the Oslo Social Support Scale was found to be good with the Cronbach alpha of 0.82, which was also validated in Nepal [5].
Finally, data was collected from 1076 total adult survivors (one in each house) selected from four different districts.
Data analysis
All data were analyzed by statistical software SPSS 16.0. Descriptive analysis was done to report frequency, percentage, mean and standard deviation. Chi-square test was done to find association between PTSD and sociodemographic variables, earthquake exposure variables and social support. Binary logistic regression was used to determine the relationship between PTSD and socio-demographic variables, earthquake exposure variables and social support.
P value of < 0.05 was considered to be statistically significant.
Results
Table 1 depicts the distribution of socio-demographic variables, social support and their association with PTSD. The prevalence of PTSD was 18.9%. The socio demographic variables were associated with PTSD such as age (p = 0.003), gender (p = 0.001), ethnicity (p < 0.001), education (p < 0.001), marital status (p = 0.010) and occupation (p < 0.001). Social support was also associated with PTSD (p < 0.001).
In the study, most of the participants (88.4%) were young and middle adults where 17.6% of them had PTSD and 28.8% of older adults had PTSD. Again, more than half of the participants (56.3%) were females where 22.3% of females and 14.5% of males had PTSD. More than half of the participants (59.2) belonged to the Janajati ethnic group where 14.8% of them had PTSD. Majority (75.4%) of participants were Hindu and 18% of them had PTSD. Likewise, majority (79.6%) were literate and only 15% of them had PTSD. Most of the participants (82.3%) were married and among them 20% had PTSD. Agriculture was the most common (49.7%) occupation among the participants where 26% of them had PTSD.
Regarding social support scale, nearly half of the participants (46%) had poor social support. Among participants with poor social support, 26.3% of them had PTSD. In participants who had moderate social support, only 9.8% had PTSD and in people with strong social support, 19% had PTSD.
Earthquake exposure of the participants
Majority (87%) of the respondents were exposed to the earthquake characteristics. Regarding earthquake exposure of the participants, most of the exposure variables were associated with PTSD such as self-buried (p = 0.006), self-injured (p < 0.001), witness of injured in earthquake (p = 0.001), witness of buried in earthquake (p = 0.001), witness of death in earthquake (p = 0.002), family members being handicapped (p = 0.005), death of family members (p = 0.012), loss of house and property (p < 0.001) and severity of damage to house and property (p < 0.001). Other exposure variables such as self-handicapped and relatives and friends being handicapped were not associated with PTSD.
Majority of the participants (92.4%) had lost house or property in the earthquake. Among them, 20% had PTSD. Among the 82 participants who were self-buried, 30.5% had PTSD. Twenty two percent of the participants who had witnessed death in earthquake had PTSD. Again, among the participants who had death in their family, 26% of them had PTSD. The estimates related to earthquake exposure are not shown in tables.
Table 2 illustrates the relationship between PTSD and several associated factors. The multivariate logistic regression shows that gender, ethnicity, education, occupation, social support and severity of damage to house and property are significantly associated with PTSD. Odds of having PTSD is 1.6 times higher among females compared to males (AOR = 1.6, 95% CI: 1.1–2.3, p = 0.008). The people in Janajati ethnicity have 40% lower odds of having PTSD compared to Brahmin/Chhetri (AOR = 0.6, 95%CI: 0.4–0.9; p = 0.017). Participants who were illiterate are nearly 2 times more likely to have PTSD compared to literate (AOR = 1.9, 95%CI: 1.3–2.9, p = 0.001). Participants who did business had 60% lower risk of having PTSD compared to farmers (AOR = 0.4, 95% CI: 0.2–0.9, p = 0.028). The participants with moderate social support had 70% lower odds of having PTSD compared to those with poor social support (AOR = 0.3, 95%CI: 0.2–0.5, p < 0.001). Participants who had medium to very high level damage to house and property were nearly 5 times more likely to have PTSD compared to those who did not have any damage to house and property or very less damage (AOR = 4.9, 95%CI:2.3–10.5, p < 0.001).
Discussion
Earthquakes cause significant stress and affect a substantial number of people in the world. The 2015 earthquake in Nepal was a dreadful disaster with a painful impact on many survivors. Three years after the disaster, affected people have yet to fully recover. This cross-sectional study emerged within the four selected most affected districts. The PTSD prevalence assessed using PCL-C (DSM-IV) criteria was remarkably high three years after the disaster.
Prevalence of the PTSD
The present study found that the prevalence of PTSD three years after a devastating earthquake is 18.9% among earthquake-affected adult survivors, which is consistent with previous studies done in Nepal on mental health problems nine months after the 2015 Nepal earthquake [5].
A study containing forty-six eligible articles showed the combined incidence of PTSD among survivors who were diagnosed, at no more than nine months after the earthquake, was 28.76%, while for survivors who were diagnosed at over nine months after earthquake the combined incidence was 19.48% [38]. This result shows the prevalence of PTSD remains high years later. A study on 1355 adults from the 2010 Haiti earthquake after 30 months (about 2 and half years) found the prevalence rates of PTSD was 36.75%, which is higher than our study [39]. The PTSD was measured by the clinician using life events checklist subscale [39].
Similarly, our prevalence rates are lower than the 40% rate three years after the Turkey earthquake. The epicenter was predominantly government-constructed housing. The study used the Traumatic Stress Symptom Checklist (TSSC), which included 17 DSM IV PTSD, 55.2% female, 33.4% male reported eighteen months after the Kashmir earthquake those people were living in tents, 28.5% reported 11 months after the 2015 Nepal earthquake, 23% reported 14 months after the epicenter of Turkey earthquake, 22.1% reported 8 months after the 2008 Wenchuan earthquake in China [10, 40,41,42,43].
Most long-term studies of prevalence of PTSD in disaster exposed survivors show that the prevalence of PTSD decreases with time [44]. In contrast, some studies show that there might be a rise in the prevalence of PTSD. In the years following exposure to the 2001 World Trade Center disaster, the prevalence of PTSD among firefighters was shown to increase over time, from 9.8% in the first year (2002) to 10.6% in the 4th year (2005) (p = 0.0001), using the same scale as ours [45].
A literature review shows that most researchers who studied PTSD rates occurred around three months after the earthquake [10]. Even after powerful quakes (Wenchuan), the prevalence rate of PTSD was seen lower than other reports in the short term, however, our study focused on the potential long-term effects after an earthquake. These differences may be explained by factors such as the loss of family, loss of property, loss of job, self-injury/buried, gender, strength of coping, type of exposure, location of the disaster and diagnosis measure (tools) of PTSD. Compared with current study results of Nuwakot (2016) the prevalence (24.10%) was found to be higher in the Nepal earthquake after 10 months, it might be because of the short duration after an earthquake than ours [2]. This is also supported by a study done in China after 9 month of an earthquake which found PTSD 24.2% by using DSM IV criteria [46].
A study done in the Sichuan and Shaanxi provinces of China, 2 earthquake-stricken areas, showed that the 1 –year prevalence of PTSD amongst 2080 adult survivors was 40.1% [8]. Three years after the same earthquake it was found that 10.3% of the respondents had PTSD [47]. Similarly, a population survey done among 1756 respondents aged 16–98 in the 1991 earthquake in Yu-Chi, Taiwan found that at 6 months and 3 years, the estimated rate of Post-traumatic Stress Symptoms (PTSS) was 23.8% and 4.4% respectively [48]. Likewise, another study (Turkey) showed PTSD prevalence dropped by the length of time after the earthquake [43]. However, some other studies suggest the prevalence of PTSD has not decreased as time goes on [42, 47, 49].
After an extensive literature review and comparing our results we conclude that many factors contribute to the prevalence of PTSD symptoms amongst earthquake survivors. Further comparison is limited due to lack of studies measuring the prevalence of PTSD among survivors three years after the earthquake in Nepal. We can also assume that variation may exist between magnitude of earthquake, assessment tools, type of study (qualitative, quantitative) and coping strategies adopted by individuals after a traumatic event.
In our study, there was a significant association (p = 0.003) with age group and PTSD. In the age group of 60 and above, participants had the highest prevalence of PTSD (28.8%). These findings were consistent with a study done in Dhading Nepal, 9 months after the earthquake where adolescents and the elderly were associated with a higher incidence of PTSD [5, 50]. Similarly, another study done in Nepal (2019) and other countries (China, 2011, 2013 and 2014, Tehran, 2017), revealed that the elderly were more likely to have PTSD compared to younger adult survivors [2, 8, 51,52,53,54]. Our result is also consistent with a study done by Bhat W. et al. where age was one of the best predictors of PTSD prevalence [55].
Although our study is consistent with most other studies, it was inconsistent with the findings done in Wenchuan one month after the earthquake, which revealed the prevalence of PTSD as in young and middle age adult was 78.8% [56]. One probable reason is the ‘burden perspective hypotheses’, which suggests that middle-aged adults experience poorer coping capacity than others because of their responsibilities to society (e.g. working) and to the family (e.g. often providing support to both children and parents), which can render them more psychologically vulnerable in the aftermath of the disaster [57, 58]. Older adults have a high coping mechanism according to socio-cultural structure (potential spiritual, religious beliefs), which is consistent with a study done by Palgi. Y. [59, 60]. Moreover, older people were reported to learn coping mechanisms from experience; also, older age was associated with less sensitivity, fewer negative beliefs, and decreased mood symptoms [61].
Gender difference in prevalence of PTSD was also noted in our study. Females were found to have a 1.6 times higher odds ratio of developing PTSD compared to males. This is consistent with a study done by Lama et al. [54].
Gender differences are also supported from previous studies done in Nepal (2018) and other countries (China, 2015, Pakistan, 2011, 2013, and China, 2013) [5, 53, 61,62,63,64,65,66]. A study by Shrestha after the 2015 Nepal Earthquake also revealed higher PTSD amongst female medical personnel [67]. Higher PTSD risk among women may be due to their stronger perceptions of threat and loss of control [2]. In addition, it is possible that women are more susceptible to negative events and tend to express their emotions more than males [5]. Literature even explains gender differences in neuro-endocrine response that may lead to higher risk of PTSD in women [68].
In our study, illiterate survivors were nearly 2 times more likely to have PTSD compared to literate survivors. This is consistent with a study in Wenchuan (2012), where PTSD was found to be 52.6% among respondents with a low level of education (primary and secondary) compared with a university degree (master's and bachelor's degree). Another survey result revealed that in Nepal, the prevalence of PTSD was 13.9% among literate survivors, while illiterate accounted for 38.1% [2, 50]. A lower education level may contribute to patients being less informedwhich may decrease confidence in both physical and mental recovery [2].
The results of the present study differs from a study conducted in Haiti and other countries (China, Pakistan) which showed that higher education increases levels of PTSD [39, 62, 65]. Our study also disagrees with studies by Contractor, AA and Khodadadi-H. et al. which found that participants with a high school education were more likely to have PTSD [69]. Their hypothesis for these results is that due to their increased level of education they may be moreinclined to worry about future consequences regarding earthquake than illiterate respondents.
Our study found that ethnicity also had an association with PTSD symptoms. In the current literature, ethnicity has not been consistently described as a risk factor associated with PTSD [37, 68].
In our study, the profession of respondents was also found to have an association with PTSD. This is supported by a study conducted in China 5 years after the earthquake in 2013 [62]. The major occupation of the people residing in Wenchuan, China was fish farming (aquaculture). It was impacted or destroyed by the 2008 earthquake, and, as a result, their source of income was affected [62]. Similarly, a study revealed psychological health disturbances were more common in farmers and farmworkers, conducted by Daghagh Yazd S et al. [70].
People engaged in other occupations where less likely to develop PTSD when compared with farmers or those engaged in agriculture. Our result was consistent with a study done by Mitsuaki Katayanagi et al. which revealed that after the Great East Japan Earthquake in 2011 nearly half of the farmers who were engaged in agriculture and fishery reported decreased income [71]. It is possible that these survivors had fewer resources in coping with the stress from the economic burden than those of other occupations [62]. This may resulted in a higher PTSD rate amongst farmers [62].
In our study perceived social support was associated with PTSD in both univariate and multivariate analysis (p < 0.001). In this study, participants with moderate social support had 70% lower odds of having PTSD compared to those with poor social support (AOR = 0.3, 95%CI: 0.2–0.5, p < 0.001). These findings are similar to findings by Asnakew S. et al. who found that participants with poor social support were 3.6 times more likely to develop PTSD than those with strong social support (AOR = 3.6, 95% CI from 2.0 to 6.7) [72]. Other research has shown that there is a possible positive effect of social support for the prevention of PTSD. Social support will not benefit everyone equally. Numerous confounding variables, including gender, previous experiences of violent trauma, and self-efficacy, appear to play a role [73]. Another study by Dai W et al in 2016 found that strong social support can not only protect individuals from mental disorders but also facilitate psychological recovery from disaster [38]. This variation could be due to differences in the study population, assessment methods and posttraumatic period.
Earthquake related variables and PTSD related information
This study showed that there is a significant association between PTSD prevalence and factors such as getting buried after an earthquake, death of a family member, and witnessing others who have been buried, injured ordied. This finding is consistent with other previous studies [39, 74].These are all autonomous factors for developing PTSD. Similarly, survivors with family member loss may undertake more negative traumaand endure greater economic and psychological pressure,which may contribute to a higher PTSD prevalence rate [75].
Another factor that was associated with the PTSD prevalence was participant house and property damage. Those who had medium to very high level damage to house and property were 5 times more likely to have PTSD compared to those with no or very less damage. A study in Dhadhing showed participants who had house completely damaged and loss of property had between 4 and 9 times higher odds of having PTSD [5].
Our study is consistent with numerous previous studies [5, 7, 8, 62, 76, 77]. It is a common association that increases the prevalence rate of PTSD and likely was confounded by the fact that none of the respondents were living in their previous houses three years after the earthquake. Their current way of living and surrounding environment may have caused a constant reminder to the patient of the earthquake. The temporary accommodation of the respondents has likely made an impact on the prevalence of PTSD.
According to Galea and colleagues’ studies, loss of private property (e.g. house) and experiencing economic loss (e.g. loss of job) are major stressors after a disaster [44].This is consistent with our study. In our study sample, over ninety percent of houses were damaged during the earthquake. With loss of houses and property, many survivors were faced with financial and social problems/barriers three years later.
Similarly, consistent with our findings, a study (Kun P. et al. 2009 and 2013) of PTSD concluded that female gender, being married, ethnicity, death of family members, and damaged personal property are associated risk factors [53, 64]. Guo J. et al. and Zhou X. et al. revealed that risk factors for PTSD included advanced age, female gender, buried in the earthquake, injured in the earthquake, witnessing someone get injured in the earthquake, witnessing someone get buried in the earthquake, and witnessing someone die in the earthquake. These findings are consistent with our study findings [10, 75].
Strength of the study
The study included a large sample of communities most affected by the 2015 earthquake in 4 districts of Nepal. A standardized and validated PCL-C scale was used to assess PTSD symptoms. All interviews were conducted by trained researchers. There was, therefore, little missing data.
Limitations of the study
Our study has some limitations. Our design is a cross-sectional study with data collected at a single time reference point. To better study the effects of time, additional time points would be helpful. This study is quantitative in nature. The findings would be stronger if it had been triangulated by qualitative (study) interviews. Similarly, we also could not assure that all participants properly disclosed their mental illness. Participants were asked if they were suffering from mental illness and/or if they were under medication as exclusion criteria. It is possible that some participants who responded no had an underlying mental illness. We also did not inquire about our respondents’ family income. Family history of psychiatric illness was also not asked.
Ideally, the questionnaire should be completed by the respondents, but many of the respondents were illiterate. Researchers had to verbally ask questions and record their responses. This may have introduced bias into the study. Although the self-administration of the questionnaire would be more preferable, our data collector might have faced difficulties in explaining the PCL-C questionnaire during data collection due to its difficulty in comprehension. Recall bias may have also been a limitation. Although widely used around the world, PCL-C is a screening measure for PTSD, not a diagnostic tool. The current study participants with a score of 50 or above greater were classified as having probable PTSD without a clinical interview.
Conclusions
Our findings conclude those three years after the 2015 earthquake, adverse mental health impact still. PTSD remains a common mental health problem among survivors. Multivariate logistic regression shows that associated risk factors of survivors with persistent PTSD include gender, ethnicity, educational status, occupation, social support and severity to loss of house and property. To reduce psychiatric problems such as PTSD and to improve overall mental health and wellbeing in earthquake-affected communities, a community-based mental health and psychosocial support program should be implemented. We also recommend further mix method studies for triangulation between quantitative and qualitative information.
Availability of data and materials
The data is available from the corresponding authors upon reasonable request.
Abbreviations
- CI:
-
Confidence Interval
- DSM-IV:
-
Diagnostic and Statistical Manual of Mental Disorders 4th Edition
- DSM-5:
-
Diagnostic and Statistical Manual of Mental Disorders 5th Edition
- IRCKUSMS:
-
Institutional Review Committee of Kathmandu University School of Medical Sciences
- OR:
-
Odds Ratio
- OSSS:
-
Oslo Social Support Scale
- PCL-C:
-
PTSD (Post Traumatic Stress Disorder) Checklist—Civilian Version
- PTSD:
-
Post Traumatic Stress Disorder
- PTSS:
-
Post Traumatic Stress Symptoms
- SD:
-
Standard deviation
- SPSS:
-
Statistical Package for Social Sciences
- UGC:
-
University Grants Commission
- WHO:
-
World Health organization
References
The Government of Nepal - Ministry of Home Affairs (MoHA), Disaster Preparedness Network-Nepal (DPNet-Nepal). Nepal disaster report 2015. 2015. p. 270. Available from: http://reliefweb.int/sites/reliefweb.int/files/resources/1293600-World-Disasters-Report-2015_en.pdf.
AdhikariBaral I, KC B. Post traumatic stress disorder and coping strategies among adult survivors of earthquake, Nepal. BMC Psychiatry. 2019;19:118. https://doi.org/10.1186/s12888-019-2090-y.
Kane JC, Luitel NP, Jordans MJD, Kohrt BA, Weissbecker I, Tol WA. Mental health and psychosocial problems in the aftermath of the Nepal earthquakes: Findings from a representative cluster sample survey. EpidemiolPsychiatr Sci. 2018;27(3):301–10.
World Health Organization, United Nations High Commissioner for Refugees. Assessing Mental Health and Psychosocial Needs and Resources: Toolkit for Humanitarian Settings. Geneva: WHO; 2012.
Dahal HR, Kumar S, Thapa DK. Prevalence and risk factors of post-traumatic stress disorders among the survivors of 2015 Nepal earthquake, in Dhading. Nepal Sleep Hypn. 2018;20(2):128–39.
Devkota SP, Bagale S. Post-Traumatic Stress Disorder after Earthquake and Its Impact on Education in Nepal, Asia & the Pacific. 2016.
Cerdá M, Paczkowski M, Galea S, Nemethy K, Péan C, Desvarieux M. Psychopathology in the aftermath of the Haiti earthquake: A population-based study of post-traumatic stress disorder and major depression. Depress Anxiety. 2013;30(5):413–24.
Wu Z, Xu J, He L. Psychological consequences and associated risk factors among adult survivors of the 2008 Wenchuan earthquake. BMC Psychiatry. 2014;14(1):1–11.
Sakuma A, Takahashi Y, Ueda I, Sato H, Katsura M, Abe M, et al. Post-traumatic stress disorder and depression prevalence and associated risk factors among local disaster relief and reconstruction workers fourteen months after the Great East Japan Earthquake: A cross-sectional study. BMC Psychiatry. 2015;15(1):1–13.
Guo J, Wu P, Tian D, Wang X, Zhang W, Zhang X, et al. Post-traumatic stress disorder among adult survivors of the Wenchuan Earthquake in China: a repeated cross-sectional study. J Anxiety Disord. 2014;28(1):75–82. https://doi.org/10.1016/j.Janxdis.2013.12.001.
Ando S, Kuwabara H, Araki T, Kanehara A, Tanaka S, Morishima R, et al. Mental health problems in a community after the Great East Japan Earthquake in 2011: a systematic review. Harv Rev Psychiatry. 2017;25(1):15–28.
Silwal S, Dybdahl R, Chudal R, Sourander A, Lien L. Psychiatric symptoms experienced by adolescents in Nepal following the 2015 earthquakes. J Affect Disord. 2018;234:239–46. https://doi.org/10.1016/j.jad.2018.03.002.
Mishra D, Giri D, Marahatta SB. Post-traumatic stress disorder and associated factors among adolescents after 2015 Nepal earthquake. J ManmohanMemlInst Heal Sci. 2018;3(1):45–55.
Thapa P, Acharya L, Bhatta BD, Paneru SB, Khattri JB, Chakraborty PK, et al. Anxiety, depression and post-traumatic stress disorder after earthquake. J Nepal Health Res Counc. 2018;16(1):53–7.
Luitel NP, Jordans MJD, Sapkota RP, Tol WA, Kohrt BA, Thapa SB, et al. Conflict and mental health: a cross-sectional epidemiological study in Nepal. Soc Psychiatry PsychiatrEpidemiol. 2013;48(2):183–93.
Kohrt BA, Speckman RA, Kunz RD, Baldwin JL, Upadhaya N, Acharya NR, Sharma VD, Nepal MK, Worthman CM. Culture in Psychiatric Epidemiology: Using Ethnography and Multiple Mediator Models to Assess the Relationship of Caste with Depression and Anxiety in Nepal. 2009.
Kohrt BA, Hruschka DJ, Worthman CM, Kunz RD, Baldwin JL, Upadhaya N, et al. Political violence and mental health in Nepal: prospective study. Br J Psychiatry. 2012;201(4):268–75.
International Medical Corps. Exploring the Mental Health and Psychosocial Support Needs and Resources among Earthquake-Affected Communities in Nepal. 2016. p. 1–14. Available from: https://cdn1internationalmedicalcorps.org/wp-content/uploads/2017/07/International-Medical-Corps-2016-Nepal-Summary-Report.pdf.
Sherchan S, Samuel R, Marahatta K, Anwar N, Van Ommeren MH, Ofrin R. Post-disaster mental health and psychosocial support: experience from the 2015 Nepal earthquake. WHO South-East Asia J public Heal. 2017;6(1):22–9.
Rafiey H, Alipour F, LeBeau R, AminiRarani M, Salimi Y, Ahmadi S. Evaluating the psychometric properties of the Mental Health Continuum-Short Form (MHC-SF) in Iranian earthquake survivors. Int J Ment Health. 2017;46:1–9.
Xiao M, Li JA, Zhang X, Zhao ZE. Factors affecting functional outcome of Sichuan-earthquake survivors with tibial shaft fractures: a follow-up study. J Rehabil Med. 2011;43(6):515–20.
Sharma A, Kar N. Posttraumatic stress, depression, and coping following the 2015 Nepal earthquake: a study on adolescents. Disaster Med Public Health Prep. 2018;13(02):236–42.
Dhungana S, Koirala R, Ojha SP, Thapa SB. Quality of life and its association with psychiatric disorders in outpatients with trauma history in a tertiary hospital in Kathmandu, Nepal: a cross-sectional study. BMC Psychiatry. 2021;21(1):98. https://doi.org/10.1186/s12888-021-03104-6. PMID:33593325;PMCID:PMC7885479.
Gonzalez R, Regmi P, Aryal N, Akudjedu T. Mental health risk and associated factors in the aftermath of the 2015 earthquake in Nepal: a systematic literature review. J Manmohan Mem Inst Health Sci. 2021;7(1):93–105. https://doi.org/10.3126/jmmihs.v7i1.43155.
Ni J, Reinhardt JD, Zhang X, Xiao M, Li L, Jin H, et al. Dysfunction and post-traumatic stress disorder in fracture victims 50 months after the Sichuan earthquake. PLoS One. 2013;810:6–11.
Diagnostic E, Manual S, Disorders M. on DSM-III DSM-III-R these. 1995;(August): 1228–32
Yang X, Yang H, Liu Q, et al. Research on the Reliability and Validity of PCL-C and Influence Factors. China J Health Psychol. 2007;15:6–9.
Ge Y, Wu J, Sun X, Zhang K. Enhanced mismatch negativity in adolescents with post-traumatic stress disorder (PTSD). Int J Psychophysiol. 2011;79(2):231–5. https://doi.org/10.1016/j.ijpsycho.2010.10.012.
Forbes D, Creamer M, Biddle D. The validity of the PTSD checklist as a measure of symptomatic change in combat-related PTSD. Behav Res Ther. 2001;39(8):977–86.
Dell’Osso L, Carmassi C, Massimetti G, Daneluzzo E, Di Tommaso S, Rossi A. Full and partial PTSD among young adult survivors 10 months after the L’Aquila 2009 earthquake: Gender differences. J Affect Disord. 2011;131(1–3):79–83. https://doi.org/10.1016/j.jad.2010.11.023.
Zhang W, Jiang X, Ho KW, Wu D. The presence of post-traumatic stress disorder symptoms in adolescents three months after an 8.0 magnitude earthquake in southwest China. J ClinNurs. 2011;20(21–22):3057–69.
Zhang W, Liu H, Jiang X, Wu D, Tian Y. A longitudinal study of post-traumatic stress disorder symptoms and its relationship with coping skill and locus of control in adolescents after an earthquake in China. PLoS One. 2014;9(2):1–7.
Neria Y, Nandi A, Galea S. Post-traumatic stress disorder following disasters: a systematic review. Psychol Med. 2008;38(4):467–80.
Van Ommeren M, Sharma B, Thapa S, Makaju R, Prasain D, Bhattarai R, de Jong J. Preparing instruments for transcultural research: use of the translation monitoring form with Nepali-Speaking Bhutanese Refugees. Transcult Psychiatry. 1999;36(3):285–301. https://doi.org/10.1177/136346159903600304.
Thapa SB, Hauff E. Psychological distress among displaced persons during an armed conflict in Nepal. Soc Psychiatry PsychiatrEpidemiol. 2005;40(8):672–9.
Ben D, Scotti JR, Rabalais AE, Virginia W. Psychometric properties of the PTSD Checklist-Civilian Version. J Trauma Stress. 2003;16(5):495–502.
Bøen H, Dalgard OS, Bjertness E. The importance of social support in the associations between psychological distress and somatic health problems and socio-economic factors among older adults living at home: a cross sectional study. BMC Geriatr. 2012;12:27.
Dai W, Chen L, Lai Z, Li Y, Wang J, Liu A. The incidence of post-traumatic stress disorder among survivors after earthquakes: a systematic review and meta-analysis. BMC Psychiatry. 2016;16(1):1–11. https://doi.org/10.1186/s12888-016-0891-9.
Cénat JM, Derivois D. Assessment of prevalence and determinants of post-traumatic stress disorder and depression symptoms in adults survivors of earthquake in Haiti after 30 months. J Affect Disord. 2014;159:111–7. https://doi.org/10.1016/j.jad.2014.02.025.
Salcioglu E, Basoglu M, Livanou M. Post-traumatic stress disorder and comorbid depression among survivors of the 1999 earthquake in Turkey. Disasters. 2007;31(2):115–29. https://doi.org/10.1111/j.1467-7717.2007.01000.x.
Naeem F, Ayub M, Masood K, Gul H, Khalid M, Farrukh A, et al. Prevalence and psychosocial risk factors of PTSD: 18 months after the Kashmir earthquake in Pakistan. J Affect Disord. 2011;130(1–2):268–74. https://doi.org/10.1016/j.jad.2010.10.035.
Jha A, Shakya S, Zang Y, Pathak N, Pradhan PK, Bhatta KR, Sthapit S, Niraula S, Nehete R. Identification and treatment of Nepal 2015 earthquake survivors with post-traumatic stress disorder by non specialist volunteers: an exploratory cross-sectional study. Indian J Psychiatry. 2017;59(3):320.
Başoǧlu M, Kiliç C, Şalcioǧlu E, Livanou M. Prevalence of post-traumatic stress disorder and comorbid depression in earthquake survivors in Turkey: an epidemiological study. J Trauma Stress. 2004;17(2):133–41.
Galea S, Nandi A, Vlahov D. The epidemiology of post-traumatic stress disorder after disasters. Epidemiol Rev. 2005;27(July):78–91.
Berninger A, Webber MP, Cohen HW, Gustave J, Lee R, Niles JK, et al. Trends of elevated PTSD risk in firefighters exposed to the World Trade Center disaster: 2001–2005. Public Health Rep. 2010;125(4):556–66.
Wang X, Gao L, Shinfuku N, Zhang H, Zhao C, Shen Y. Longitudinal study of earthquake-related PTSD in a randomly selected community sample in North China. Am J Psychiatry. 2000;157:1260–6.
Zhang W, Duan G, Xu Q, Jia Z, Bai Z, Liu W, et al. A cross-sectional study on post-traumatic stress disorder and general psychiatric morbidity among adult survivors 3 years after the Wenchuan earthquake. China Asia-Pacific J Public Heal. 2015;27(8):860–70.
Tsai KY, Chou P, Chou FHC, Su TTP, Lin SC, Lu MK, et al. Three-year follow-up study of the relationship between post-traumatic stress symptoms and quality of life among earthquake survivors in Yu-Chi. Taiwan J Psychiatr Res. 2007;41(1–2):90–6.
Pietrzak RH, Tracy M, Galea S, Kilpatrick DG, Ruggiero KJ, Hamblen JL, et al. Resilience in the face of disaster: prevalence and longitudinal course of mental disorders following Hurricane Ike. PLoS One. 2012;7(6):1–14.
Xu J, He Y. Psychological health and coping strategy among survivors in the year following the 2008 Wenchuan earthquake. Psychiatry ClinNeurosci. 2012;66(3):210–9.
Zhang Y, Ho SMY. Risk factors of post-traumatic stress disorder among survivors after the 512 wenchuan earthquake in China. PLoS One. 2011;6(7):15–20.
Khodadadi-Hassankiadeh N, DehghanNayeri N, Shahsavari H, Yousefzadeh-Chabok S, Haghani H. Post-traumatic stress disorder in motor vehicle accidents Predictors of Post-Traumatic Stress Disorder among Victims of Serious Motor Vehicle Accidents. Vol. 5, IJCBNM October. 2017.
Kun P, Tong X, Liu Y, Pei X, Luo H. What are the determinants of post-traumatic stress disorder: age, gender, ethnicity or other? Evidence from the 2008 Wenchuan earthquake. Public Health. 2013;127(7):644–52. https://doi.org/10.1016/j.puhe.2013.04.018.
Lama PY, Ojha SP, Chapagai M, Tulachan P, Dhungana S. Post-Traumatic Stress Disorder in Displaced Population of Sindhupalchowk Following Earthquake. J KIST Med Coll. 2020;2(3):20–8.
Bhat W, Marlino S, Teoh V, Khan S, Khan U. Lower limb trauma and posttraumatic stress disorder: a single UK trauma unit's experience. J Plast Reconstr Aesthet Surg. 2014;67(4):555–60. https://doi.org/10.1016/j.bjps.2013.12.039.
Wang B, Ni C, Chen J, Liu X, Wang A, Shao Z, et al. Post-traumatic stress disorder 1 month after the 2008 earthquake in China: Wenchuan earthquake survey. Psychiatry Res. 2011;187(3):392–6. https://doi.org/10.1016/j.psychres.2009.07.001.
Karancian, Rüstemli A. Psychological Consequences of the 1992 Erzincan (Turkey) Earthquake. Disasters. 1995;19(1):8–18.
Tural U, Coşkun B, Onder E, Corapçioglu A, Yildiz M, Kesepara C, et al. Psychological consequences of the 1999 earthquake in Turkey. J Trauma Stress. 2004;17(6):451–9.
Palgi Y. Predictors of the new criteria for probable PTSD among older adults. Psychiatry Res. 2015;230(3):777–82.
Pearce M, Haynes K, Rivera NR, Koenig HG. Spiritually integrated cognitive processing therapy: a new treatment for post-traumatic stress disorder that targets moral injury. Glob Adv Health Med. 2018;7:216495611875993.
Feder A, Ahmad S, Lee EJ, Morgan JE, Singh R, Smith BW, et al. Coping and PTSD symptoms in Pakistani earthquake survivors: purpose in life, religious coping and social support. J Affect Disord. 2013;147(1–3):156–63. https://doi.org/10.1016/j.jad.2012.10.027.
Zhang LP, Zhao Q, Luo ZC, Lei YX, Wang Y, Wang PX. Prevalence and risk factors of post-traumatic stress disorder among survivors five years after the “Wenchuan” earthquake in China. Health Qual Life Outcomes. 2015;13(1):1–7. https://doi.org/10.1186/s12955-015-0247-z.
Anwar J, Mpofu E, Matthews LR, Shadoul AF, Brock KE. Reproductive health and access to healthcare facilities: risk factors for depression and anxiety in women with an earthquake experience. BMC Public Health. 2011;11:523.
Kun P, Chen X, Han S, Gong X, Chen M, Zhang W, et al. Prevalence of post-traumatic stress disorder in Sichuan Province, China after the 2008 Wenchuan earthquake. Public Health. 2009;123(11):703–7. https://doi.org/10.1016/j.puhe.2009.09.017.
Tian Y, Wong TKS, Li J, Jiang X. Post-traumatic stress disorder and its risk factors among adolescent survivors three years after an 8.0 magnitude earthquake in China. BMC Public Health. 2014;14(1):1073.
Solomon Z, Gelkopf M, Bleich A. Is terror gender-blind? Gender differences in reaction to terror events. Soc Psychiatry PsychiatrEpidemiol. 2005;40(12):947–54.
Shrestha R. Post-traumatic stress disorder among medical personnel after Nepal earthquake, 2015. J Nepal Health Res Counc. 2015;13(30):144–8.
Hu J, Feng B, Zhu Y, Wang W, Xie J, Zheng X. Gender Differences in PTSD: Susceptibility and Resilience. Gend Differ Differ Context. 2017.
Contractor AA, Durham TA, Brennan JA, Armour C, Wutrick HR, Christopher Frueh B, et al. DSM-5 PTSD’s symptom dimensions and relations with major depression’s symptom dimensions in a primary care sample. Psychiatry Res. 2014;215(1):146–53.
Yazd SD, Wheeler SA, Zuo A. Key risk factors affecting farmers’ mental health: a systematic review. Int J Environ Res Public Health. 2019;16(23):4849.
Katayanagi M, Seto M, Nakaya N, Nakamura T, Tsuchiya N, Narita A, et al. Impact of the great east Japan earthquake on the employment status and mental health conditions of affected coastal communities. Int J Environ Res Public Health. 2020;17(21):1–13.
Asnakew S, Shumet S, Ginbare W, et al. Prevalence of post-traumatic stress disorder and associated factors among Koshe landslide survivors, Addis Ababa, Ethiopia: a community-based, cross sectional study. BMJ Open. 2019;9:e028550. https://doi.org/10.1136/bmjopen-2018-028550.
Alipour F, Ahmadi S. Social support and Posttraumatic Stress Disorder (PTSD) in earthquake survivors: a systematic review. Soc Work Ment Health 2020:1–14. https://doi.org/10.1080/15332985.2020.1795045.
Kuo HW, Wu SJ, Ma TC, Chiu MC, Chou SY. Post-traumatic symptoms were worst among quake victims with injuries following the Chi-chi quake in Taiwan. J Psychosom Res. 2007;62(4):495–500.
Zhou X, Kang L, Sun X, Song H, Mao W, Huang X, et al. Prevalence and risk factors of post-traumatic stress disorder among adult survivors six months after the Wenchuan earthquake. Compr Psychiatry. 2013;54(5):493–9. https://doi.org/10.1016/j.comppsych.2012.12.010.
Cairo JB, Dutta S, Nawaz H, Hashmi S, Kasl S, Bellido E. The prevalence of post-traumatic stress disorder among adult earthquake survivors in Peru. Disaster Med Public Health Prep. 2010;4(1):39–46.
Wang L, Zhang Y, Shi Z, Wang W. Symptoms of post-traumatic stress disorder among adult survivors two months after the Wenchuan earthquake. Psychol Rep. 2009;105(3):879–85.
Acknowledgements
We would like to thank the University Grants Commission (UGC), Nepal, for the academic research grant, and Dhulikhel Hospital, Kathmandu University School of Medical Sciences, Dhulikhel, Kavre, Nepal, for the technical support. We would like to thank Alicia Khan (BMid, BDev, M.CHaM, IBCLC) and Ajay Bhatt (MD. Assistant Professor, University of Hawaii. Fulbright Scholar) for thorough proofreading, grammatical corrections and edits. We would also like to thank Dr. PranodanPoudel and Mr. HukumThapa (PhD scholar and Professor of English, Tribhuvan University) for editing the English language. We also extend our gratitude to data collectors and study participants for their time and effort.
Funding
This academic research proposal was funded by the University Grants Commission (UGC), Nepal (Faculty Research Grant; awarded No FRG-74/75- HS-10; Date 27 Sept, 2018). The funding body was not involved in the design of the study or in the collection, analysis, and interpretation of the data, or in the writing of the manuscript.
Author information
Authors and Affiliations
Contributions
R.A. and P.C. were involved in the conception and design of the study. R.A, P.C., S.K., B.M., B.C., J.P., J.N. and C.P. were responsible for the data acquisition. P.C. and J.N. were engaged in the data analysis and interpretation. R.A., J.P. and C.P. drafted the initial manuscript. P.C. was later involved in the necessary modifications and completion of the manuscript for publication. R.A., P.C. and J.N. revised manuscripts critically for intellectual content. S.K., B.M., B.C., J.P. and C.P. offered help in revising the manuscript. All authors reviewed and approved the submitted version of the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
All methods were performed in accordance with the relevant guidelines and regulations.
The Institutional Review Committee of Kathmandu University School of Medical Sciences (IRCKUSMS), Dhulikhel, Kavre, Nepal approved the study protocol (Approval Number: 88/17). Written informed consent was obtained from participants before data collection. For illiterate participants their immediate family members (brother, sister, son, daughter, son and daughter in law etc.) gave written informed consent for participation in the study. The ethics committee (IRCKUSMS) had approved the methods of giving consent.
Consent for publication
Not Applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Acharya Pandey, R., Chalise, P., Khadka, S. et al. Post-traumatic stress disorder and its associated factors among survivors of 2015 earthquake in Nepal. BMC Psychiatry 23, 340 (2023). https://doi.org/10.1186/s12888-023-04836-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12888-023-04836-3