
Abstract
Background
The present study aimed to explore changes in depression and posttraumatic stress disorder (PTSD) among the general population during the prolonged COVID-19 pandemic and to investigate risk factors and adaptive/nonadaptive strategies.
Methods
A web-based longitudinal survey was conducted across five timepoints from 2020 to 2022 in Japan. Depressive symptoms were measured using the Patient Health Questionnaire-9 (PHQ-9), PTSD was measured using Impact of Event Scale-Revised (IESR), and coping strategies were measured using Brief Coping Orientation to Problems Experienced (Brief COPE). Higher scores of PHQ-9 and IESR indicate more symptoms and Higher score of Brief COPE indicate that these means of coping are used very frequently.
Results
A total of 1,366 participants (mean age = 52.76, SD = 15.57) were analyzed. Regarding levels of depression, PHQ-9 scores in 2022 were lower than in 2020 and 2021 (all p < 0.01). Regarding levels of PTSD, IESR scores in 2022 were lower than in 2021 among females (p < 0.001). Being younger (β = -0.08 and − 0.13, both p < 0.01) and engaging in self-blame (β = 0.12 and 0.18, both p < 0.01) increased PHQ-9 scores regardless of sex. For males, not working (β = 0.09, p = 0.004) and having suffered an economic impact (β = 0.07, p = 0.003) were risk factors for depressive symptoms, and active coping (β = -0.10, p = 0.005) was associated with decreased depressive symptoms. For females, substance use (β = 0.07, p = 0.032) and behavioral disengagement (β = 0.10, p = 0.006) increased depressive symptoms, and females did not show strategies that decreased the symptoms.
Conclusions
Levels of depression might have increased in the early stages of the pandemic and decreased in January 2022. Although males need to improve their economic situation to decrease depressive symptoms, adaptive strategies might be difficult to identify due to the prolonged pandemic among both sexes. In addition, the pandemic might be a depressive event but not a traumatic event among the general population, at least in Japan.
Similar content being viewed by others


Background
The Coronavirus disease 2019 (COVID-19) has spread worldwide and the pandemic has led to social restrictions for the general population. During the early stages of the pandemic, meta-analyses showed levels of depression [1,2,3,4,5,6,7] and posttraumatic stress disorder (PTSD) [3, 8,9,10,11,12] increased among the general population. A previous study showed that age, social status, and economic impact of the pandemic were risk factors for depression and PTSD [1, 5, 13, 14]. On the other hand, some research that surveyed mental health between January and March 2020 reported that mental health sometimes improved during the stable period of the pandemic [15, 16]. Although much previous research investigated mental health in the early stage of infection, it is necessary to investigate levels of depression and PTSD and risk factors during the prolonged pandemic.
Moreover, previous research pointed out that mental health vulnerability varies by sex: females were found to have worse mental health than males before the pandemic [17] and to be more influenced by social restrictions due to the pandemic [18, 19]. Some coping strategies have been shown to be useful for maintaining mental health [20, 21]; however, the effect of coping strategies on mental health might differ by sex [22].
The present study aimed to explore the changes in depressive and PTSD symptoms from 2020 to 2022 in Japan. In addition, this study examined risk factors and adaptive/nonadaptive strategies associated with mental health by sex and provided ways of identifying individuals who need professional support in the context of the chronic stress associated with the pandemic. In Japan, strict lockdowns have never been implemented, but mild lockdowns have been implemented intermittently because the pandemic has exhibited a repeated pattern of expansion and contraction. Previous research conducted in 2020 and 2021 reported that the prevalences of depressive symptoms in Japan were 18.35% and 43.4%, respectively, and the rate might have increased before the pandemic [23,24,25]. Additionally, the rate of suicide in 2020 increased by 4.5% compared to that in 2019 [26]. Regarding sex, although the number of male suicides was 2 times as high as that of females in 2020 and 2021, the number of male suicides in 2020 and 2021 decreased from that in 2019; on the other hand, the number of female suicides in 2020 and 2021 increased from that in 2019 [26].
Methods
Study design and participants
We conducted a longitudinal survey that consisted of 5 web-based surveys administered by an online research company, Macromill, Inc., in Japan. Macromill, Inc. primarily conducts online market research for other companies. Macromill, Inc. and their partner companies have 10 million individuals registered as potential participants, from whom Macromill, Inc. can choose participants who meet the selection criteria for research. The 1st survey (T1) was conducted from 17 to 22 July 2020, the 2nd survey (T2) was conducted from 18 to 23 September 2020, the 3rd survey (T3) was conducted from 22 to 27 January 2021, the 4th survey (T4) was conducted from 17 to 21 September, and the 5th survey (T5) was conducted from 21 to 26 January 2022. The T1 survey was conducted on the earliest date that the Ethics Review Committee approved this study, and the deadline of the T1 survey was set to reach the target number of participants, as follows. The T2 to T5 surveys were conducted at regular intervals, and the deadline for each survey was set at 6 days.
From a pool of approximately 10 million individuals registered with Macromill, Inc. and their partner companies, we recruited participants who were between 20 and 79 years old and who lived in 13 out of the 47 prefectures in Japan. The 13 prefectures included those where COVID-19 had spread in April 2020, which was the first wave of the COVID-19 pandemic in Japan, and where the Government of Japan had implemented special measures. A quota sampling method was used to obtain age groups of equal size (i.e., groups of individuals in their 20s, 30s, 40s, 50s, 60s, and 70s), participants of both sexes (male and female), and participants with different employment statuses (full-time worker; no regular employment; and unemployed, including homemaker, retired, and jobless). All the participants received Macromill points for their participation; Macromill points are associated with the original point service provided by Macromill, Inc., and participants can trade these points for prizes or cash.
Sample size and effect size
We planned to recruit 2,700 participants at T1 based on a calculation of the appropriate sample size [24]; however, the present study was a longitudinal study, and so it was difficult to control its sample sizes. We calculated effect sizes as follows: Cohen’s D (d) for the t test, Phi (φ) and Cramer’s V (V) for the chi-square test, and partial η2 (ηp2). With respect to d, 0.80 indicates a large effect size, 0.50 a medium effect size, and 0.20 a small effect size. Regarding φ and V, 0.50 represents a large effect size, 0.30 a medium effect size, and 0.10 a small effect size. Although no clear criteria are associated with ηp2, the higher the value of this measure is, the larger the effect size. For adjusted R2, 0.26 designates a large effect size, 0.13 a medium effect size, and 0.02 a small effect size.
Measurements
The present study collected participants’ sociodemographic characteristics and included 3 questionnaires pertaining to depressive symptoms, PTSD symptoms, and coping strategies. PTSD symptoms were measured as part of the T2 survey, and all other sociodemographic characteristics and questionnaires were measured at all 5 time points.
The sociodemographic characteristics investigated included age, sex, the presence or absence of chronic illnesses, marital status, the presence or absence of children, employment status, household income (< 4 million JPY, 4–8 million JPY, and > 8 million JPY), and the economic impact for the COVID-19 pandemic. One million JPY was 9,400 USD in 2020 and, in Japan, the average annual household income was 5.52 million JPY, and the median income was 4.37 million JPY [27]. The economic impact of the COVID-19 pandemic was assessed by asking whether the participant perceived economic impacts of the pandemic.
Depressive symptoms were measured using the Japanese version of the Patient Health Questionnaire-9 (PHQ-9) [28, 29]. Participants were asked to indicate the frequency with which they had experienced depressive symptoms over the past 2 weeks. The PHQ-9 consists of 9 items scored on a four-point scale (0 to 3); the total score can range from 0 to 27, with higher scores indicating more depressive symptoms. The Japanese version of the PHQ-9 has been validated for depression in primary care, and the relationship with the mental component summary of the SF-8 was significant [29].
PTSD was measured using the Japanese version of the Impact of Event Scale-Revised (IESR) [30,31,32]. Participants were asked to indicate the frequency with which they had experienced PTSD symptoms over the past week. The IESR consists of 22 items scored on a five-point scale (0 to 4); the total score can range from 0 to 88, with higher scores indicating more PTSD symptoms. The Japanese version of the IESR has been validated for PTSD among nonsurvivors and survivors of traumatic events: high Cronbach’s alpha coefficients of the whole scale were shown, and participants with PTSD had significantly higher scores than those without PTSD [30].
Coping strategies were measured using the Japanese version of the Brief Coping Orientation to Problems Experienced (Brief COPE) [33, 34]. Participants were asked about the frequency with which they used various coping styles to deal with the social changes and inconveniences resulting from the COVID-19 pandemic at the time of completing the survey. The scale consists of 28 items and assesses 14 coping styles: self-distraction (e.g., “I turn to work or other activities to take my mind off things”); active coping (e.g., “I take action to try to make the situation better”); denial (e.g., “I refuse to believe that it has happened”); substance use (e.g., “I use alcohol or other drugs to make myself feel better”); use of emotional support (e.g., “I get emotional support from others”); use of instrumental support (e.g., “I get help and advice from other people”); behavioral disengagement (e.g., “I give up trying to deal with it”); venting (e.g., “I express my negative feelings”); positive reframing (e.g., “I try to find comfort in what is happening”); planning (e.g., “I think hard about what steps to take”); humor (e.g., “I make jokes about it”); acceptance (e.g., “I accept the reality of the fact that it happened”); and religion (e.g., “I try to find comfort in my religion or spirituality”). Each coping style is evaluated by reference to two items that are scored on a four-point scale (1 to 4); the total scores for each coping style can range from 2 to 8. Higher scores indicate that these means of coping are used very frequently. The Japanese version of the Brief COPE has been validated among Japanese workers: the relationships between coping styles and negative emotions, fatigue, concentration, and activity levels were significant [34].
Statistical analysis
The present study analyzed participants who completed all 5 surveys. First, we compared the demographic characteristics of the analyzed participants and to those of participants who were excluded from the analysis. Sociodemographic characteristics at T1, mean PHQ-9 scores at T1 and mean IESR scores at T2 were compared using the chi-square test and two-sample t test. Subsequently, to compare the sociodemographic characteristics and coping strategies of the analyzed participants by sex, two-sample t tests and chi-square tests were conducted to explore their sociodemographic characteristics at T5 and mean Brief COPE scores at T5.
Thereafter, to examine changes in the level of depressive and PTSD symptoms across the timepoints of the survey, a mixed-model analysis of variance (ANOVA) was conducted with respect to the mean PHQ-9 and IESR scores including survey time as a within-subject factor and sex as a between-subjects factor.
Finally, to examine the influences of sociodemographic characteristics and coping strategies on depressive and PTSD symptoms, multiple linear regression analyses were conducted by sex using PHQ-9 and IESR scores at T5 as the dependent variables and sociodemographic characteristics and Brief COPE scores at T5 as the predictor variables.
The statistical significance level was set at p < 0.05, and effect sizes, Cohen’s D (d) for the t test, Phi (φ) and Cramer’s V (V) for the chi-square test, partial η2 (ηp2) for ANOVAs, and adjusted R2 were used for multiple linear regression, as mentioned previously. All statistical analyses were conducted using IBM SPSS statistical software (Version 28).
Results
Comparison between participants and members of the drop-out group
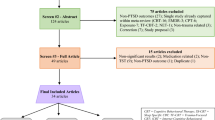
A detailed description of study participant inclusion is shown in Fig. 1. A total of 2,708 participants were included in the 1st survey, of whom 1,342 were excluded from the analysis because they did not participate in the longitudinal survey (N = 1,332) or because they were missing responses (N = 10). Following these exclusions, a total of 1,366 participants were analyzed in the present study (for a valid response rate of 50.4%), of whom 776 were male and 600 were female.

Flow chart of this study showing participant inclusion
A comparison between the final participants and the participants who were excluded from the analysis at T1 showed that the participants analyzed in the study were older (p < 0.001, d = 0.46) and included a large percentage of males (p < 0.001, φ = 0.12) and a large percentage of individuals with children (p = 0.007, φ = 0.05). Regarding employment status, a low percentage of participants were homemakers, and a large percentage did not work (p < 0.001, Cramer’s V = 0.09). Regarding household income, a large percentage of participants had a household income of more than 8 million JPY, and the participants included in the final analysis were less likely to provide no answer or an answer of “unknown” for household income (p < 0.001, Cramer’s V = 0.09). The participants included in the final analysis suffered a greater economic impact from the pandemic than participants who were excluded from the analysis (p = 0.001, d = 0.06). Regarding mental health, the analyzed group exhibited low PHQ-9 scores at T1 (p = 0.001, d = 0.13); however, there were no significant differences in PTSD symptoms at T2. The effect size of age difference was medium, those of employment status and household income were small, and other differences were very small.
Participants’ sociodemographic characteristics and variables at T5 by sex
Sociodemographic characteristics and Brief COPE scores at T5 are shown according to sex in Table 1. The mean age among males was 53.73 ± 16.08 years, and that among females was 54.95 ± 14.89 years. Among the male, large percentages had chronic illnesses, were single, were not working, and had household income of less than 4 million JPY; on the other hand, low percentages did not have children and were homemakers. The effect size of employment status was medium, and those of chronic illnesses, marital status, children, and household income were small. Regarding Brief COPE, males used the strategies of self-distraction, active coping, emotional support, instrumental support, venting, positive reframing, planning, and acceptance less frequently and employed denial, substance use, and self-blame more frequently than females. The effect sizes of self-distraction, active coping, substance use, emotional support, instrumental support, and venting were small, and those of other coping strategies were very small.
Mean scores and prevalence of depressive and PTSD symptoms by sex
Mean PHQ-9 scores by sex are shown in Fig. 2. The interaction between survey times and sex was nonsignificant (p = 0.577, ηp2 = 0.001). The main effect of sex was significant (p = 0.012, ηp2 = 0.005), and the mean score among males was higher than that among females. The main effect of survey time was significant (p < 0.001, ηp2 = 0.006), and the mean score at T5 was lower than that at T1 (p < 0.001), T2 (p = 0.001), T3 (p = 0.003), and T4 (p < 0.001).

Mean PHQ-9 scores by sex from T1 to T5. Error bars show the standard error. The mean score of males was higher than that of females, and mean scores at T5 were lower than those at T1 to T4
Mean scores of PTSD symptoms by sex between T2 and T5 are shown in Fig. 3. The interaction between survey times and sex was significant (p = 0.003, ηp2 = 0.003); males scored higher than females at T4 (p = 0.012) and T5 (p = 0.003), and the mean score at T5 among females was lower than that at T3 (p < 0.001). The main effects of sex were significant (p = 0.027, ηp2 = 0.004), and males scored higher than females. The main effect of survey time was nonsignificant (p = 0.057, ηp2 = 0.002).

Mean IESR scores by sex from T2 to T5. Error bars show the standard error. The mean score of males was higher than that of females at T4 and T5. Among females, the mean score at T5 was lower than that at T3
Risk factors and coping strategies for depressive and PTSD symptoms
The results of multiple linear regression analysis by sex concerning the prediction of depressive symptoms (PHQ-9) at T5 are shown in Table 2. Adjusted R2 scores were 0.64 in male and 0.56 in female and significant (p < 0.001 in both cases). Regarding risk factors for depressive symptoms, being younger was a risk factor for both males and females, and not working and having suffered an economic impact from the pandemic were risk factors for males. Regarding coping strategies, self-blame increased depressive symptoms for both males and females. Among males, active coping decreased symptoms, and venting increased symptoms. Among females, substance use and behavioral disengagement increased symptoms.
The results of multiple linear regression analysis by sex concerning the prediction of PTSD symptoms (IESR) at T5 are shown in Table 3. Adjusted R2 scores were 0.57 in male and 0.48 in female and significant (p < 0.001 in both cases). Economic impact was a risk factor for both males and females, and being younger was a risk factor for females. Regarding coping strategies, self-blame increased PTSD symptoms among males and females. Among males, self-distraction, behavioral disengagement, and venting increased symptoms, and the use of emotional support decreased symptoms. Among females, denial increased symptoms, and the use of instrumental support decreased symptoms.
Discussion
The present study investigated depressive and PTSD symptoms, related factors, and coping strategies between 2020 and 2022. A total of 1,366 participants were analyzed, and the results showed that the level of depressive symptoms in 2022 was lower than that in 2020 and 2021. For both depressive and PTSD symptoms, males reported more symptoms than females. Risk factors and coping strategies related to depressive and PTSD symptoms are shown by sex.
Characteristics of participants in the present study
Some sociodemographic characteristics of the participants in the present study were similar to those of the Japanese population in general [27, 35], such as the percentages of homemakers and jobless individuals females and household incomes among males and females. However, the percentage of males who were not working and that of single individuals among both males and females were larger than that the corresponding percentages among the Japanese population in general. Some studies have noted that being jobless and single might be risk factors for mental illness during the COVID-19 pandemic [36,37,38]. Thus, some degree of bias might have resulted from the quota sampling method. The excluded groups showed higher depressive levels than the included group. Consequently, it is possible that individuals with high levels of depressive symptoms might have been excluded from the analysis in the present study, and the participants in the present study might have included a large number of individuals who had some risk factors.
Changes in levels of depressive and PTSD symptoms
Levels of depression might have increased due to the pandemic and subsequently decreased slightly in 2022. Because, the present study showed that levels of depressive symptoms in January 2022 were lower than in 2020 and 2021, and these scores in January 2022 were nearly the same as scores obtained before the pandemic [39, 40] rather than during the pandemic [23]. The same result was found for the number of suicides in Japan: the rate of suicides increased from July 2020 to June 2021, but the rate decreased from July 2021 to February 2022 [26]. Accordingly, the general population experienced depression during the pandemic, but it improved in 2022. However, it is possible that this decrease in depressive symptoms is temporary due to the increase in the number of suicides in March 2022 in Japan [26]; therefore, it is necessary to conduct a follow-up survey concerning mental health during and after the pandemic.
Regarding PTSD symptoms, although the symptoms of females decreased beginning in late 2021, IESR scores did not seem to decrease compared with the same scores before the pandemic [30]. Brunet, et al. [41] conducted a survey to investigate PTSD during the COVID-19 pandemic across countries, which indicated few participants met the clinical threshold for PTSD; accordingly, these authors noted that PTSD was not a common symptom associated with the COVID-19 pandemic. On the other hand, some studies concerning China, the Philippines, northern Iran, Poland, and Italy found high levels of PTSD symptoms during the pandemic [42,43,44,45,46,47]. Therefore, because PHQ scores increased in the early stages of the pandemic and decreased in the prolonged pandemic while IESR scores remained the same as before the pandemic, the pandemic might be a depressive event but not a traumatic event for the general population, at least in Japan, which has not conducted a strict lockdown but has conducted several mild lockdowns.
Additionally, the present study found that males exhibited higher levels of depression and PTSD than females; however, many studies have reported that being female is a risk factor for mental illness [17, 30, 48,49,50,51]. One potential reason for this difference is sampling bias, which is discussed in the limitations; thus, the conclusions of this study must be considered in combination with other studies.
Sociodemographic characteristics and coping strategies for depressive and PTSD symptoms
Regarding depressive symptoms, the present study found that risk factors and nonadaptive strategies, that is, strategies that increased depressive symptoms, regardless of sex, were being young and engaging in self-blame, which is consistent with previous studies [1, 5, 13, 14, 24, 25]. Not working and perceiving an economic impact of the pandemic were risk factors among males; however, these economic factors were not related to symptoms among females. In addition, females employed only nonadaptive strategies; that is, these strategies decreased their symptoms, which is discussed below. On the other hand, males employed both nonadaptive strategies and adaptive strategies: males needed to take some action to improve their situation to decrease depressive symptoms. Additionally, although some previous studies have reported household income to be a risk factor [5], the present study did not find any relationship between household income and mental health; accordingly, people who were not working or who faced economic impacts might require mental health care regardless of their income.
Regarding PTSD symptoms, regardless of sex, risk factors and nonadaptive strategies included perceiving an economic impact of the pandemic and engaging in self-blame, respectively. To decrease PTSD symptoms, males need to receive emotional support from others, and females need help and advice from others.
However, the present study found that more nonadaptive strategies were used than adaptive strategies: blaming oneself for the pandemic was related to depression and PTSD regardless of sex, and becoming immersed, denying the situation, drinking alcohol and using drugs, behavioral disengagement, expressing negative feelings, and relying on religion as a distraction from negative feelings or a means of escaping the situation might lead to an increase in the symptoms of depression or PTSD.
Although some research conducted during the early stages of the pandemic showed that exercise and social support were effective in improving mental health [19, 52, 53], G Maggi, I Baldassarre, A Barbaro, ND Cavallo, M Cropano, R Nappo and G Santangelo [54] noted that it is difficult to discover adaptive strategies due to the prolonged nature of this stressful situation. Additionally, some of these nonadaptive strategies, that is denying the situation, drinking alcohol and using drugs, behavioral disengagement, and relying on religion, were identified as nonadaptive strategies before the pandemic [34]; accordingly, these strategies might be general nonadaptive strategies used to deal with daily stress, which is relevant since the pandemic has led to notable daily stressors for the general population.
Limitation
The participants analyzed in the present study might have exhibited bias because the present study employed the quota sampling method, and a total of 50% of the participants were excluded from the analysis. Participants’ depressive and PTSD symptoms might not be reflective of the general population of Japan; in particular, young participants were excluded from the analysis more frequently, and previous studies have reported that being young is a risk factor related to mental health [20, 37, 52, 55,56,57,58,59,60].
As responses to the survey were self-reported, the mental health, behaviors and cognition of the participants were not observed. In particular, the measures of depressive and PTSD symptoms reported in the present study were not identical with diagnoses. In addition, it was difficult to examine certain sociodemographic factors, such as not working and not having regular employment, in detail in the present study.
Additional limitations of the study included the following: the study analyzed coping strategies cross-sectionally; the survey times could not be controlled; and the study used an online survey with incentives, which may have resulted in the inclusion of participants who felt compelled to participate to earn the economic incentive.
Conclusion
The present study showed that levels of depression among the general population increased in the early stages of the pandemic and decreased in 2022. Regarding depressive symptoms, the risk factor among males was economic factors; efforts should be made to improve this situation to decrease depressive symptoms. However, especially for females, adaptive strategies might be more difficult to identify than they were during the early stages of the pandemic due to the prolonged pandemic and the diversity of perceptions of this stressful situation. Finally, PTSD symptoms were at the same level as before the pandemic, so the pandemic might be a depressive event but not a traumatic event among the general population, at least in Japan. However, because the potential remains for levels of especially depressive symptoms to increase at some point in the future, there is a need for long-term follow-up survey.
Data Availability
The datasets used during the current study are available from the corresponding author on reasonable request.
Abbreviations
- COVID-19:
-
Coronavirus disease 2019
- PHQ-9:
-
Patient Health Questionnaire-9
- IESR:
-
Impact of Event Scale-Revised
- Brief COPE:
-
Brief Coping Orientation to Problems Experienced
- ANOVA:
-
Analysis of variance
References
Balakrishnan V, Ng KS, Kaur W, Govaichelvan K, Lee ZL. COVID-19 depression and its risk factors in Asia Pacific - a systematic review and meta-analysis. J Affect Disord. 2022;298:47–56.
Castaldelli-Maia JM, Marziali ME, Lu Z, Martins SS. Investigating the effect of national government physical distancing measures on depression and anxiety during the COVID-19 pandemic through meta-analysis and meta-regression. Psychol Med. 2021;51:881–93.
Cenat JM, Blais-Rochette C, Kokou-Kpolou CK, Noorishad PG, Mukunzi JN, McIntee SE, et al. Prevalence of symptoms of depression, anxiety, insomnia, posttraumatic stress disorder, and psychological distress among populations affected by the COVID-19 pandemic: a systematic review and meta-analysis. Psychiatry Res. 2021;295:113599.
Deng Y, Chen Y, Zhang B. Different prevalence trend of depression and anxiety among healthcare workers and general public before and after the peak of COVID-19 occurred in China: a meta-analysis. Asian J Psychiatr. 2021;56:102547.
Hosen I, Al-Mamun F, Mamun MA. Prevalence and risk factors of the symptoms of depression, anxiety, and stress during the COVID-19 pandemic in Bangladesh: a systematic review and meta-analysis. Glob Ment Health (Camb). 2021;8:e47.
Hossain MM, Rahman M, Trisha NF, Tasnim S, Nuzhath T, Hasan NT, et al. Prevalence of anxiety and depression in South Asia during COVID-19: a systematic review and meta-analysis. Heliyon. 2021;7:e06677.
Lee Y, Lui LMW, Chen-Li D, Liao Y, Mansur RB, Brietzke E, et al. Government response moderates the mental health impact of COVID-19: a systematic review and meta-analysis of depression outcomes across countries. J Affect Disord. 2021;290:364–77.
Arora T, Grey I, Ostlundh L, Lam KBH, Omar OM, Arnone D. The prevalence of psychological consequences of COVID-19: a systematic review and meta-analysis of observational studies. J Health Psychol. 2022;27:805–24.
Liu X, Zhu M, Zhang R, Zhang J, Zhang C, Liu P, et al. Public mental health problems during COVID-19 pandemic: a large-scale meta-analysis of the evidence. Transl Psychiatry. 2021;11:384.
Yuan K, Gong YM, Liu L, Sun YK, Tian SS, Wang YJ, et al. Prevalence of posttraumatic stress disorder after infectious disease pandemics in the twenty-first century, including COVID-19: a meta-analysis and systematic review. Mol Psychiatry. 2021;26:4982–98.
Yunitri N, Chu H, Kang XL, Jen HJ, Pien LC, Tsai HT, et al. Global prevalence and associated risk factors of posttraumatic stress disorder during COVID-19 pandemic: a meta-analysis. Int J Nurs Stud. 2022;126:104136.
Zhang L, Pan R, Cai Y, Pan J. The prevalence of post-traumatic stress disorder in the general population during the COVID-19 pandemic: a systematic review and single-arm meta-analysis. Psychiatry Investig. 2021;18:426–33.
Chen Q, Li W, Xiong J, Zheng X. Prevalence and risk factors associated with postpartum depression during the COVID-19 pandemic: a literature review and meta-analysis. Int J Environ Res Public Health. 2022;19:2219.
Yuan K, Zheng YB, Wang YJ, Sun YK, Gong YM, Huang YT, et al. A systematic review and meta-analysis on prevalence of and risk factors associated with depression, anxiety and insomnia in infectious diseases, including COVID-19: a call to action. Mol Psychiatry. 2022;27:3214–22.
Cai Z, Cui Q, Liu Z, Li J, Gong X, Liu J, et al. Nurses endured high risks of psychological problems under the epidemic of COVID-19 in a longitudinal study in Wuhan China. J Psychiatr Res. 2020;131:132–7.
Zhu Z, Liu Q, Jiang X, Manandhar U, Luo Z, Zheng X, et al. The psychological status of people affected by the COVID-19 outbreak in China. J Psychiatr Res. 2020;129:1–7.
American Psychiatric Association. Diagnostic and statistical Manual of Mental Disorders, Fifth Edition (DSM-5). American Psychiatric Publication; 2013.
Moore HE, Siriwardena AN, Gussy M, Hill B, Tanser F, Spaight R. Exploring the impact of the COVID-19 pandemic on male Mental Health Emergencies attended by Ambulances during the First National “Lockdown” in the East Midlands of the United Kingdom. Am J Mens Health. 2022;16:15579883221082428.
Jacques-Avino C, Lopez-Jimenez T, Medina-Perucha L, de Bont J, Goncalves AQ, Duarte-Salles T, et al. Gender-based approach on the social impact and mental health in Spain during COVID-19 lockdown: a cross-sectional study. BMJ Open. 2020;10:e044617.
Shechory Bitton M, Laufer A. Mental health and coping in the shadow of the COVID-19 pandemic: the israeli case. Front Public Health. 2020;8:568016.
Umucu E, Lee B. Examining the impact of COVID-19 on stress and coping strategies in individuals with disabilities and chronic conditions. Rehabil Psychol. 2020;65:193–8.
Rana IA, Bhatti SS, Aslam AB, Jamshed A, Ahmad J, Shah AA. COVID-19 risk perception and coping mechanisms: does gender make a difference? Int J Disaster Risk Reduct. 2021;55:102096.
Deguchi Y, Iwasaki S, Niki A, Kadowaki A, Hirota T, Shirahama Y, et al. Relationships between occupational stress, change in work environment during the COVID-19 pandemic, and depressive and anxiety symptoms among non-healthcare workers in Japan: a cross-sectional study. Int J Environ Res Public Health. 2022;19:983.
Fukase Y, Ichikura K, Murase H, Tagaya H. Depression, risk factors, and coping strategies in the context of social dislocations resulting from the second wave of COVID-19 in Japan. BMC Psychiatry. 2021;21:33.
Fukase Y, Ichikura K, Murase H, Tagaya H. Age-related differences in depressive symptoms and coping strategies during the COVID-19 pandemic in Japan: a longitudinal study. J Psychosom Res. 2022;155:110737.
National Police Agency. The number of suicides in Japan. 2022. https://www.npa.go.jp/publications/statistics/safetylife/jisatsu.html. Accessed 3 June 2022.
Ministry of Health Labor and Welfare. Comprehensive survey of living conditions in 2019. 2020. https://www.mhlw.go.jp/toukei/saikin/hw/k-tyosa/k-tyosa19/index.html.
Kroenke K, Spitzer RL, Williams JB. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med. 2001;16:606–13.
Muramatsu K, Miyaoka H, Kamijima K, Muramatsu Y, Tanaka Y, Hosaka M, et al. Performance of the japanese version of the patient health questionnaire-9 (J-PHQ-9) for depression in primary care. Gen Hosp Psychiatry. 2018;52:64–9.
Asukai N, Kato H, Kawamura N, Kim Y, Yamamoto K, Kishimoto J, et al. Reliabiligy and validity of the japanese-language version of the impact of event scale-revised (Ies-RJ): four studies of different traumatic events. J Nerv Ment Dis. 2002;190:175–82.
Weiss DS. The impact of event scale-revised. In: Assessing Psychological Trauma and PTSD edn. Edited by Wilson JP, Keane TM. New York, NY, US: The Guilford Press; 2004: 168–89.
Weiss DS. The impact of event scale: revised. In: Cross-Cultural Assessment of Psychological Trauma and PTSD edn. Edited by Wilson JP, Tang CS. New York, NY, US: Springer Science + Business Media; 2007: 219–238.
Carver CS. You want to measure coping but your protocol’too long: consider the brief cope. Int J Behav Med. 1997;4:92–100.
Otsuka Y, Sasaki T, Iwasaki K, Mori I. Working hours, coping skills, and psychological health in japanese daytime workers. Ind Health. 2009;47:22–32.
Ministry of Internal Affairs and Communications Statistic Bureau. Labour force survey. 2021. https://www.stat.go.jp/data/roudou/index.html. Accessed 5 May 2022.
Cao Y, Siu JY, Shek DTL, Shum DHK. COVID-19 one year on: identification of at-risk groups for psychological trauma and poor health-protective behaviour using a telephone survey. BMC Psychiatry. 2022;22:252.
Rodríguez-Rey R, Garrido-Hernansaiz H, Collado S. Psychological impact and associated factors during the initial stage of the coronavirus (COVID-19) pandemic among the general population in Spain. Front Psychol. 2020;11:1540.
Zhang L, Cai H, Bai W, Zou SY, Feng KX, Li YC, et al. Prevalence of suicidality in clinically stable patients with major depressive disorder during the COVID-19 pandemic. J Affect Disord. 2022;307:142–8.
Nakata K, Tsuji T, Vietri J, Jaffe DH. Work impairment, osteoarthritis, and health-related quality of life among employees in Japan. Health Qual Life Outcomes. 2018;16:64.
Toyoshima K, Inoue T, Masuya J, Fujimura Y, Higashi S, Kusumi I. Affective temperaments moderate the effect of insomnia on depressive symptoms in adult community volunteers. J Affect Disord. 2021;282:726–31.
Brunet A, Rivest-Beauregard M, Lonergan M, Cipolletta S, Rasmussen A, Meng X, et al. PTSD is not the emblematic disorder of the COVID-19 pandemic; adjustment disorder is. BMC Psychiatry. 2022;22:300.
Bonichini S, Tremolada M. Quality of life and symptoms of PTSD during the COVID-19 lockdown in Italy. Int J Environ Res Public Health. 2021;18:4385.
Li Q. Psychosocial and coping responses towards 2019 coronavirus diseases (COVID-19): a cross-sectional study within the chinese general population. QJM. 2020;113:731–8.
Reskati MH, Shafizad M, Aarabi M, Hedayatizadeh-Omran A, Khosravi S, Elyasi F. Mental health status and psychosocial issues during nationwide COVID-19 quarantine in Iran in 2020: a cross-sectional study in Mazandaran Province. Curr Psychol. 2021;1–17. https://doi.org/10.1007/s12144-021-02011-z.
Shah T, Shah Z, Yasmeen N, Ma ZR. Psychological impact of the COVID-19 pandemic on chinese population: an online survey. World J Clin Cases. 2021;9:9500–8.
Tee M, Wang C, Tee C, Pan R, Reyes PW, Wan X, et al. Impact of the COVID-19 pandemic on physical and mental health in lower and upper middle-income asian countries: a comparison between the Philippines and China. Front Psychiatry. 2020;11:568929.
Wang C, Chudzicka-Czupala A, Grabowski D, Pan R, Adamus K, Wan X, et al. The association between physical and mental health and face mask use during the COVID-19 pandemic: a comparison of two countries with different views and practices. Front Psychiatry. 2020;11:569981.
Bello UM, Kannan P, Chutiyami M, Salihu D, Cheong AMY, Miller T, et al. Prevalence of anxiety and depression among the general population in Africa during the COVID-19 pandemic: a systematic review and meta-analysis. Front Public Health. 2022;10:814981.
Gomez-Salgado J, Andres-Villas M, Dominguez-Salas S, Diaz-Milanes D, Ruiz-Frutos C. Related health factors of psychological distress during the COVID-19 pandemic in Spain. Int J Environ Res Public Health. 2020;17:3947.
Vindegaard N, Eriksen Benros M. COVID-19 pandemic and mental health consequences: systematic review of the current evidence. Brain Behav Immun. 2020;89:531–42.
Wang C, Pan R, Wan X, Tan Y, Xu L, Ho CS, et al. Immediate psychological responses and associated factors during the initial stage of the 2019 coronavirus disease (COVID-19) epidemic among the general population in China. Int J Environ Res Public Health. 2020;17:1729.
Hossain MM, Tasnim S, Sultana A, Faizah F, Mazumder H, Zou L, et al. Epidemiology of mental health problems in COVID-19: a review. F1000Research. 2020;9:636.
Ni MY, Yang L, Leung CMC, Li N, Yao XI, Wang Y, et al. Mental health, risk factors, and social media use during the COVID-19 epidemic and cordon sanitaire among the community and health professionals in Wuhan, China: cross-sectional survey. JMIR Ment Health. 2020;7:e19009.
Maggi G, Baldassarre I, Barbaro A, Cavallo ND, Cropano M, Nappo R, et al. Age- and gender-related differences in the evolution of psychological and cognitive status after the lockdown for the COVID-19 outbreak: a follow-up study. Neurol Sci. 2022;43:1521–32.
Fitzpatrick KM, Harris C, Drawve G. How bad is it? Suicidality in the middle of the COVID-19 pandemic. Suicide Life Threat Behav. 2020;50:1241–9.
Lin LY, Wang J, Ou-Yang XY, Miao Q, Chen R, Liang FX, et al. The immediate impact of the 2019 novel coronavirus (COVID-19) outbreak on subjective sleep status. Sleep Med. 2020;77:348–54.
Solomou I, Constantinidou F. Prevalence and predictors of anxiety and depression symptoms during the COVID-19 pandemic and compliance with precautionary measures: age and sex matter. Int J Environ Res Public Health. 2020;17:4924.
Varshney M, Parel JT, Raizada N, Sarin SK. Initial psychological impact of COVID-19 and its correlates in Indian Community: an online (FEEL-COVID) survey. PLoS ONE. 2020;15:e0233874.
Wang H, Xia Q, Xiong Z, Li Z, Xiang W, Yuan Y, et al. The psychological distress and coping styles in the early stages of the 2019 coronavirus disease (COVID-19) epidemic in the general mainland chinese population: a web-based survey. PLoS ONE. 2020;15:e0233410.
Yamamoto T, Uchiumi C, Suzuki N, Yoshimoto J, Murillo-Rodriguez E. The psychological impact of ‘mild lockdown’ in Japan during the COVID-19 pandemic: a nationwide survey under a declared state of emergency. Int J Environ Res Public Health. 2020;17:9382.
Acknowledgements
Not applicable.
Funding
This work was supported by Japan Society for the Promotion of Science KAKENHI Grant Number 20H01771, Murata Science Foundation, and Kitasato University School of Allied Health Sciences (Grant-in-Aid for Research Project, Nos. 2020–1029, 2021–1025, and 2022–1025).
Author information
Authors and Affiliations
Contributions
Y.F., K.I., and H.T. designed the study and conducted the statistical analyses. Y.F. collected the data and drafted the manuscript. Y.F. and K.I. contributed to the scientific discussion of the data. All authors read and approved the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The Research Ethics Review Committee of Kitasato University School of Allied Health Sciences approved this study (the approval numbers were 2020–011 and 2020–023). All participants were informed of the aims of the present study and their right to cease participating in the survey prior to their participation. For participants, checking a box indicating “I agree to participate in the study” was considered to be an indication of consent, and informed consent was obtained from all participants. This study was conducted in accordance with the 1964 Declaration of Helsinki and its later amendments.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Fukase, Y., Ichikura, K. & Tagaya, H. Symptoms and risk factors of depression and PTSD in the prolonged COVID-19 pandemic: a longitudinal survey conducted from 2020 to 2022 in Japan. BMC Psychiatry 23, 180 (2023). https://doi.org/10.1186/s12888-023-04670-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12888-023-04670-7